-
7/30/2019 Questions and Answers on Pandemic Influenza.24
1/7
50 AJN MJuly 2007 M Vol. 107, No. 7
http://www.nursingcenter.com
ing to local disasters such asfloods or hurricanesin
whichcommunities provide support to astricken area and immediate
aid isexpected from regional, state, ornational entitiescould be
greatly
curtailed in a pandemic because ofits potentially global scope.
Andthe weeks- or months-long dura-tion of a pandemic could result
inthe exhaustion of essential person-nel and supplies that would
needrepeated replenishing. But becausea pandemic makes every
commu-nity vulnerable, little outside helpmight be available to
those copingwith mass illness and death.Communities not yet
affectedwould undoubtedly feel the need to
reserve resources to protect them-selves against the threat,
while those recoveringwould be too overwhelmed and depleted to
assist.
On the other hand, a pandemic with a nonviru-lent strain could
be a very manageable event.Overreacting to a disease outbreak (by
unnecessar-ily closing schools or limiting travel, for example)can
also cause harm. The challenge in pandemicinfluenza planning is to
find a balance between riskand preparedness that realistically
estimates the conse-quences of a pandemic and doesnt rob resources
fromthe many everyday health care and social challenges.Planners
should be aware of preparations being madeat local, state, and
federal levels; proceed logicallywith their own planning; and be
able to interpretevidence that indicates an influenza pandemic
isunfolding. Also, it should be noted, every month thatgoes by
without an outbreak is an opportunity tostockpile antiviral drugs
and protective equipmentand to develop plans for continuing to
deliver healthcare and essential services in the event of a
pan-demic outbreak.
SEASONAL OR PANDEMIC INFLUENZA?Influenza outbreaks occur every
year. Called sea-
sonal, or interpandemic, influenza, the illness iscaused by
viral strains that have circulated in
I
nfluenza killed more people in a year thanthe Black Death of the
Middle Ages killedin a century; it killed more people intwenty-four
weeks than AIDS has killedin twenty-four years. So writes John
M.
Barry in his bestselling account of the horrificSpanish flu
pandemic of 191820, The GreatInfluenza.1 Today, such knowledge of
history is guid-ing disaster planners as they consider equally
stag-gering scenarios among their forecasts for aninfluenza
pandemic (see Table 1, page 52).
The prospect of an influenza pandemic causedby a lethal viral
subtype is of great concern tonurses, who understand the impact
such an eventcould have, and it poses unaccustomed challengesto
disaster planners. The typical model for respond-
Questions and Answers on Pandemic InfluenzaStriking a balance
between risk and preparedness.
Victoria J. Davey is deputy chief officer for public health
andenvironmental hazards at the Department of Veterans Affairsin
Washington, DC, and a doctoral student at UniformedServices
University of the Health Sciences, Bethesda, MD.Contact author:
[email protected]. Disaster Care is coordi-nated by Mary
Chaffee, MS, RN, FAAN: [email protected] author of this article
has no significant ties, financial orotherwise, to any company that
might have an interest in the
publication of this educational activity.The views expressed in
this article are those of the author
and are not necessarily those of the U.S. government,
theDepartment of Veterans Affairs, or the Department of
Defense.
Continuing Education2HOURS
Overview: Disaster planning based on events such asfloods or
hurricanes, which are local or regional in scale,may be inadequate
for responding to a lethal influenza pan-demic that has the
potential to overwhelm existing publichealth infrastructures.
However, if a mild strain of the virus
achieves pandemic proportions, the current public health sys-tem
may be able to manage the outbreak relatively easily.Therefore, the
challenge in pandemic influenza planning is tofind a balance
between risk and preparedness. Planners andpolicy makers must make
realistic estimates of the conse-quences of a pandemic and allocate
limited resources wisely,so that everyday health care and social
needs arent short-changed. This article examines what weve learned
from pastinfluenza pandemics and answers some frequently
askedquestions about pandemics and how to prepare for them.
-
7/30/2019 Questions and Answers on Pandemic Influenza.24
2/7
[email protected] AJN MJuly 2007 M Vol. 107, No. 7 51
humans previously (thus, some peo-ple are immune) and for which
thereare effective vaccines. Most peopleexperience seasonal
influenza as amiserable week of fever, fatigue,aching muscles, and
hacking cough.Yet in the United States, more than200,000 excess
hospitalizations andperhaps 40,000 deaths occur annu-ally from
complications of influenza,mostly among the very young andold.2,
3
The predominant mode of influ-enza transmission is probably
virus-containing respiratory droplets (largerthan 10 microns in
diameter). Aninfected person releases dropletswhen sneezing,
coughing, or speak-ing, and a nearby person then inhalesthem into
the respiratory tract, or thevirus is deposited on mucous
mem-branes such as the eyes, nose, ormouth. Transmission may also
occurvia inhalation of smaller airborneviral particles (smaller
than 5 microns
in diameter) that can remain sus-pended in the air for minutes
tohours, or by picking up virus fromsurfaces like countertops and
thentouching the mucous membranes.4, 5
Efficient transmission is characteristic of influenza:infected
people may shed virus for half a day beforethey feel symptoms.
Influenzas brief incubationperiod (the time between infection and
the develop-ment of symptoms) averages just two days. Theviruss
reproduction ratio (the number of personsinfected by one source
person) depends on the strainand subtype, the quantity and type of
contactsamong people, and the susceptibility of the unin-fected
person. An infected person will, on average,transmit the virus to
one to two other people in aninfluenza outbreak, potentially
resulting in rapidpropagation of the virus in a population.4, 6,
7
Minor genetic changes that accumulate in sea-sonal influenza
viruses (a process known as anti-genic drift) make it necessary to
reformulate andreadminister the influenza vaccine each season.8,
9
With its easy transmissibility and mutability,influenza poses
constant challenges that nursesknow all too wellfrom teeming
wintertime EDs
and pediatric waiting rooms to illness-relatedabsences that
strain remaining staff.
Major viral-gene mutations or recombination oftwo different
viral strains of human and animalinfluenza strains can create a new
viral subtype (aprocess called antigenic shift) thats easily
trans-mitted to and among humans.8-10 Isolation and iden-tification
of new viral subtypes is necessary forvaccine development, which is
itself a complexmanufacturing process that currently does not
beginto produce doses in quantity for at least sixmonths.11 When a
virus for which there is no vaccinebecomes easily transmissible
among nonimmunepeople, the opportunity for a pandemic is
created.
The historical record shows many accounts of dis-ease outbreaks
that may have been influenza epi-demics or pandemics. Although the
scale of theoutbreaks and their causative agents are not
preciselyknown in many cases, most historians agree that anoutbreak
that began in Asia in 1580 was an influenzapandemic.12 In the past
300 years, there have been atleast 10 influenza pandemics,13, 14
which, by defini-
tion, result in moderate to dramatic spikes in illnessesand
deaths above average annual levels.15, 16
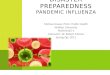
In this 1918 photograph, influenza victims crowd into an
emergency hospital atCamp Funston, a subdivision of Fort Riley in
Kansas. The flu, which some expertsbelieve originated in Kansas,
killed at least 20 million people worldwide.
By Victoria J. Davey, MPH, RN
AssociatedPress/NationalMuseumofHealthandM
edicine,
ArmedForcesInstituteofPathology
-
7/30/2019 Questions and Answers on Pandemic Influenza.24
3/7
52 AJN MJuly 2007 M Vol. 107, No. 7
http://www.nursingcenter.com
During the 20th century three pandemicsoccurred: in 191820,
195758, and 196869 (afourth worldwide outbreak that began in 1977
isnot accepted by all authorities as a true pandemic).The most
fearsome of these, the 191820 pandemic(see Figure 1, page 53),
sickened 25% of the U.S.population in several six-to-eight-week
waves andrapidly killed an estimated 2.5% of its victims
(thepercentage of ill people who die, known as the casefatality
ratio, is an important indicator of the sever-ity of the outbreak;
in 1918, some populations out-side the United States had much
higher case fatalityratios).17 Communities were paralyzed for
weeks,with hospitals and mortuaries filled beyond capac-ity, public
services severely disrupted, and schools
and businesses shuttered. This experience wasechoed around the
world, and estimates of theglobal loss of human life range between
30 millionand 50 million.18, 19 In contrast, the 195758 and196869
pandemics were clinically milder, thoughthey still resulted in
worldwide death tolls of 1 mil-lion to 2 million, and they are
remembered less asdisasters than as epidemiologic curiosities in
whicha single influenza strain was tracked around theworld.15 Since
the last influenza pandemic a newnetwork of global laboratories and
surveillance sys-tems can speed the recognition of an emerging
pan-demic and the identification of its cause, but
influenza pandemics remain difficult to predict.20
WHY WORRY NOW?Worldwide social and ecologic changes, including
agrowing human population, crowded living condi-tions, and rising
global mobility, have raised the riskthat a virulent influenza
strain could spark a partic-ularly devastating pandemic. Larger
populationshave resulted in higher numbers of food animals,leading
to more humananimal interaction andtherefore to opportunities for
viral-gene recombi-nation and transmission.21 Once a virus adapts
tohumans, global air travel can greatly accelerate itsspread. Since
2003, a pathogenic avian influenzastrain, A (H5N1), has caused a
pandemic in domes-tic poultry and wild birds in much of the
world,as well as more than 300 laboratory-confirmedhuman cases,
with a 60% case fatality ratio.20
Presently, avian A (H5N1) influenza is not readilytransmitted to
humansmost of the people whohave fallen ill from A (H5N1) had
direct exposure topoultry. It is not known whether the A (H5N1)
viruswill cause a human pandemic.
Prototype vaccines for A (H5N1) are being testedin clinical
trials, and small quantities have been stock-
piled.22
But a pandemic could be caused by an entirelydifferent influenza
subtype, one for which a vaccine
Table 1. Estimated Rates of Health Care Use, Illness, andDeath
in Moderate and Severe Influenza Pandemics
* The estimates presume that the same percentages of the
populationwill be infected in a moderate and a severe pandemic; the
virulenceof the influenza strain will determine the severity of
illness.U.S. Department of Health and Human Services. HHS pandemic
influenza plan part 1: strategicplan. The pandemic influenza
threat. U.S. Department of Health and Human Services. 2005.
Characteristic Number of people affected*
Moderate pandemic(similar to 1958 and1968 outbreaks)
Severe pandemic(similar to 1918outbreak)
Illness 90 million (30% of population)
90 million (30% ofpopulation)
Outpatient med-ical care
45 million (50% ofthose who fall ill)
45 million (50% ofthose who fall ill)
Hospitalization 865,000 9,900,000
ICU care 128,750 1,485,000
Mechanicalventilation
64,875 742,500
Deaths 209,000 1,903,000
Personal Pandemic PlanningPreparing for a disease outbreak is
similar to generalemergency preparedness.
Keep essential supplies on hand: nonperishable foods,
bottledwater, medications, and personal hygiene products.
Keep your familys health information up-to-date, organized,and
accessible.
Make sure you can communicate from your home by severalmethods
(such as telephone and e-mail) and that you canget information from
the outside world (including by battery-powered radio).
Get an annual seasonal influenza vaccination; it protects youand
your contacts from seasonal influenza strains now andfrom any that
might circulate later with a pandemic strain.
Participate in your facilitys emergency planning; get trainingin
the implementation of the plans.
In case you cant work because of your own or a family mem-bers
illness, be prepared to spend an extended period oftime at home;
have supplies on hand to keep yourself busy.
Explore the possibility of telecommuting (for example,
byassisting with telephone health care advice).
Contribute to your communitys preparedness (for example,
byorganizing local response planning and being available tohelp in
the event of an outbreak).
-
7/30/2019 Questions and Answers on Pandemic Influenza.24
4/7
[email protected] AJN MJuly 2007 M Vol. 107, No. 7 53
wont be available in large enough quantities until atleast six
months after the strain is isolated.11
Potentially effective antiviral medications are avail-able for
treatment, postexposure prophylaxis, orlonger-term prophylaxis, and
stockpiles are increas-ing. But the effectiveness of current
antivirals againsta specific pandemic influenza strain is
uncertain, andthe medications would need to be
administeredswiftlywithin 48 hours of symptoms appearingwhich is a
daunting challenge for distribution sys-tems.15 Experience from
past influenza pandemicsand the ability to monitor for specific
pathogens suchas the avian A (H5N1) subtype should help informour
nations readiness for the next pandemic.
In addition to the emergence and spread of the A(H5N1) virus,
disasters that have occurred in recentyears have made clear the
advisability of planning foran influenza pandemic. The outbreak of
severe acuterespiratory syndrome (SARS) in 2003 startled the
global public health community with its virulence,efficient
transcontinental transmission, and signifi-
cant economic effects. Then the devastation causedby Hurricanes
Katrina and Rita demonstrated thata large-scale disaster can
overwhelm existing emer-gency response systems. Also, its only in
the pasthalf decade that new information about the 1918influenza
virus and reexamination of the long-lasting effects of that
pandemic have returned it togeneral awareness.10, 15
HOW CAN WE PREPARE?In both the private and public sectors, and
at thefederal, regional, state, and local levels, prepara-tions and
planning are taking place.
Government strategy. On November 1, 2005,President Bush unveiled
the National Strategy forPandemic Influenza, a document that
outlines bothgovernment and private sector responsibilities inthree
areas: preparedness and communications, sur-veillance and
detection, and response and contain-
ment.23
A detailed national implementation plandeveloped from this
document charged cabinet-level
Figure 1. Transmission of Influenza Around the World, 191820
Nicholson GK, et al., editors. Textbook of influenza. 1998.
Adapted with permission of the authors and published with
permission ofBlackwell Publishing, Oxford.
-
7/30/2019 Questions and Answers on Pandemic Influenza.24
5/7
federal agencies with devising plans to maintainoperations,
protect employees, communicate withstakeholders, and support
federal efforts during apandemic.11 The plan culminates in a list
of actionitems and performance measures that require fed-eral
agencies to work together and with state agen-cies and private
groups, including businesses andfaith-based organizations, to
prepare for aninfluenza pandemic (see Table 2, above, for a sam-ple
action item that focuses on communications, anarea of special
concern in large-scale events). A goalof the national strategy and
implementation plan isto create and test disaster response and
emergencymanagement systems to ensure that a well-pre-pared,
communicative, and operational responsewill be in place if we are
faced with an influenza pan-demic of any severity. Already under
way are newvaccine development24; federal stockpiling of antivi-ral
medications, personal protective equipment,and health care
materiel22; modeling studies to fore-
cast potential outcomes of pandemic interven-tions25, 26; and a
host of detailed plans drafted by
54 AJN MJuly 2007 M Vol. 107, No. 7
http://www.nursingcenter.com
federal agencies, states, businesses, schools, andhealth care
systems and facilities.
In February, the Centers for Disease Control andPrevention, in
collaboration with numerous publicand private agencies, issued
planning guidance forcommunity mitigation measures during a
pan-demic. These are specific actions that a communitycould take to
minimize the diseases spread, limit ill-ness and death, and keep
essential services operat-ing. The measures would be applied
according tothe severity of the pandemic and could includetreating
those who had fallen ill with antiviral med-ications and providing
prophylactic antivirals to
their household members, voluntary isolation of theill and
quarantine of household members, schoolclosures and cancellation of
public gatherings, andusing social distancing measures in the
workplace.27
Other planning efforts. The federal govern-ments emphasis on
pandemic planning as well as fed-eral funding of states pandemic
planning havespurred planning efforts by regions, states,
commu-nities, and the private sector. Nearly all states haveplans
posted on the Internet. Details vary widely,but state plans include
actions they would take inpandemic surveillance, management, and
contain-ment, including distribution of antivirals and vac-
cines.28, 29 Checklists to help businesses, schools,colleges and
universities, faith-based organizations,and health care settings
with pandemic planningare available at www.pandemicflu.gov. (A
quicksearch of the Internet reveals an abundance of pan-demic plans
posted from a wide array of sources.) Toaddress concerns about
allocating scarce resourcesduring a pandemic, federal agencies have
initiatedpublic and private sector collaborations charged
withdeveloping prioritization plans for distributing vac-cine and
antiviral medications.30
WHATS THE RIGHT BALANCE?At every level, from the presidents
cabinet to ruralhospitals, pandemic influenza planning takes
timeand resources. Preparations are costly and compli-cated. If
youve served in a hospital or communityplanning group, you may have
estimated howmany N95 respirators or doses of antiviral
medica-tions might be needed in a severe influenza pan-demicand
been daunted by the cost and storagerequirements. Or perhaps youve
faced the adminis-trative conundrum of how to quickly train
retirednurses to replace those absent because of illness.And you
may have questioned the worth of planning,
and the cost of stockpiling resources, when your facil-ity has
so many present needs.
Ensuring Effective Risk Communication
6.3.8 Ensure that timely, clear, coordinated messages are
deliv-ered to the American public from authoritative sources at all
lev-els of government and assist the governments of affected
nationsto do the same.
6.3.8.1 HHS, in coordination with DHS, DOD, and VA, shalldevelop
and disseminate a risk communication strategy within6 months,
updating it as required. Measure of performance: imple-mentation of
risk communication strategy on www.pandemicflu.gov
and elsewhere.6.3.8.2 DOD and VA, in coordination with HHS,
shalldevelop and disseminate educational materials, coordinatedwith
and complementary to messages developed by HHS buttailored for
their respective departments, within 6 months.Measure of
performance: up-to-date risk communication materialpublished on DOD
and VA pandemic influenza websites, HHSwebsite www.pandemicflu.gov,
and in other venues.
HHS = Department of Health and Human Services, DHS =Department
of Homeland Security, DOD = Department ofDefense, VA = Department
of Veterans Affairs.
Table 2. Sample Action Item from the National Strategy
forPandemic Influenza: Implementation Plan
White House Homeland Security Council. National strategy for
pandemic influenza: implemen-tation plan. Washington, DC; 2006 May.
http://www.whitehouse.gov/homeland/pandemic-influenza-implementation.html.
-
7/30/2019 Questions and Answers on Pandemic Influenza.24
6/7
[email protected] AJN MJuly 2007 M Vol. 107, No. 7 55
But as you grapple with these difficult questions,consider the
fact that influenza pandemics will hap-pen because we cannot
prevent them. A renownedhistorian of the 191820 pandemic, Alfred
W.Crosby, said, I know how not to get AIDS. I dontknow how not to
get the flu.31
Perhaps the 1918 pandemic was a once-in-a-
millennium event, or maybe a pandemic caused bya similarly
lethal influenza A (H5N1) strain will
strike in the next five years. Its wise to plan,
alwaysconsidering how the resources might be useful forother
situations. All hazards emergency plans aredesigned to be of use in
managing nearly any kindof disaster or emergency. Harking back to
the SARSepidemic, every all hazards emergency planshould include
measures for dealing with any infec-tious disease outbreak. Your
list of retired nurseswilling to return to work might prove useful
in theaftermath of an earthquake. Immunization clinicsfor seasonal
influenza can help you plan how youwill distribute vaccine or
antivirals in a pandemic(see Emerging Infections, Using Seasonal
Influenza
Clinics for Public Health Preparedness Exercises,October 2006).
The search for an A (H5N1)influenza vaccine has stimulated research
that willimprove vaccine production in general.24 Finally,think of
pandemic planning the way you think ofcar insuranceas something you
must have buthope never to have to use.M
REFERENCES
1.Barry JM. The great influenza: the epic story of the
dead-liest plague in history. New York: Viking; 2004.
2.Dushoff J, et al. Mortality due to influenza in the
UnitedStatesan annualized regression approach using multiple-
cause mortality data. Am J Epidemiol2006;163(2):181-7.3.Harper
SA, et al. Prevention and control of influenza.
Recommendations of the Advisory Committee onImmunization
Practices (ACIP). MMWR Recomm Rep2005;54(RR-8):1-40.
4.Bridges CB, et al. Transmission of influenza: implicationsfor
control in health care settings. Clin Infect Dis
2003;37(8):1094-101.
5.Goldmann DA. Transmission of viral respiratory infectionsin
the home. Pediatr Infect Dis J2000;19(10 Suppl):S97-S102.
6.Weiss RA. The Leeuwenhoek Lecture 2001. Animal originsof human
infectious disease. Philos Trans R Soc Lond B BiolSci
2001;356(1410):957-77.
7.Longini IM, Jr., et al. Containing pandemic influenza at
thesource. Science 2005;309(5737):1083-7.
8.Gabriel G, et al. The viral polymerase mediates adaptationof
an avian influenza virus to a mammalian host. Proc NatlAcad Sci USA
2005;102(51):18590-5.
9.Kilbourne ED. Influenza pandemics: can we prepare for
theunpredictable? Viral Immunol2004;17(3):350-7.
10.Taubenberger JK, et al. Characterization of the 1918influenza
virus polymerase genes. Nature 2005;437(7060):889-93.
11.White House Homeland Security Council. National strategyfor
pandemic influenza: implementation plan. Washington,DC; 2006 May.
http://www.whitehouse.gov/homeland/pandemic-influenza-implementation.html.
12.Potter CW. A history of influenza.J Appl
Microbiol2001;91(4):572-9.
13.Hope-Simpson RE. Recognition of historic influenza epi-demics
from parish burial records: a test of prediction from
a new hypothesis of influenzal epidemiology.J Hyg
(Lond)1983;91(2):293-308.
Face Masks or Respirators?
Apress release on May 3 from the Centersfor Disease Control and
Prevention (CDC)
introduced interim guidance for the use of facemasks and
respirators in public settings duringan influenza pandemic, which
is summarized atwww.pandemicflu.gov/vaccine/maskguidance.html. Here
are the three main recommendationsin the summary. Whenever
possible, rather than relying on
the use of masks or respirators, close contactand crowded
conditions should be avoidedduring an influenza pandemic.
Facemasks should be considered for use byindividuals who enter
crowded settings, bothto protect their nose and mouth from
otherpeoples coughs and to reduce the wearerslikelihood of coughing
on others; the timespent in crowded settings should be as shortas
possible.
Respirators should be considered for use byindividuals for whom
close contact with aninfectious person is unavoidable. This
caninclude selected individuals who must care for
a sick person ([for example, a] family memberwith a respiratory
infection) at home.In the press release, Dr. Michael Bell,
associ-
ate director for infection control in the Division ofHealthcare
Quality Promotion at the CDC, said,Facemasks are not designed to
protect peoplefrom breathing in very small particles, such
asviruses. . . . Rather, facemasks help stop poten-tially
infectious droplets from being spread bythe person wearing them. .
. . Respirators aredesigned to protect people from breathingin very
small particles, which might containviruses. Thus, if you are
caring for someone
who is ill with pandemic flu, proper use of awell-fitted
respirator may be a reasonablechoice.Dana Carey, associate
editor
-
7/30/2019 Questions and Answers on Pandemic Influenza.24
7/7
14.Patterson KD. Pandemic influenza, 17001900: a study
inhistorical epidemiology. Totowa, NJ: Rowman andLittlefield;
1986.
15.Knobler SL, et al., editors. The threat of pandemicinfluenza:
are we ready? Washington, DC: NationalAcademies Press; 2005.
16.Osterholm MT. Preparing for the next pandemic. N Engl
JMed2005;352(18):1839-42.
17.Schoch-Spana M. Hospitals full-up: the 1918
influenzapandemic. Public Health Rep 2001;116 Suppl 2:32-3.
18.Gostin LO. Pandemic influenza: public health preparednessfor
the next global health emergency.J Law Med
Ethics2004;32(4):565-73.
19. Patterson KD, Pyle GF. The geography and mortality of
the1918 influenza pandemic. Bull Hist Med1991;65(1):4-21.
20.World Health Organization. Epidemic and pandemic alert
and response (EPR): avian influenza. World HealthOrganization.
2007.
http://www.who.int/csr/disease/avian_influenza/en/index.html.
21.Wilson ME. The traveler and emerging infections:
sentinel,courier, transmitter.J Appl Microbiol2003;94
Suppl:1S-11S.
22.U.S. Department of Health and Human Services.
Pandemicplanning update II. Washington, DC; 2006 Jun 29.
http://www.pandemicflu.gov/plan/pdf/PanfluReport2.pdf.
23.White House Homeland Security Council. National strategyfor
pandemic influenza. Washington, DC; 2005
Nov.http://www.whitehouse.gov/homeland/nspi.pdf.
24.U.S. Department of Health and Human Services. HHSawards
contracts totaling more than $1 billion to developcell-based
influenza vaccine. 2006.
http://www.hhs.gov/news/press/2006pres/20060504.html.
25.Germann TC, et al. Mitigation strategies for
pandemicinfluenza in the United States. Proc Natl Acad Sci
USA2006;103(15):5935-40.
26.Committee on Modeling Community Containment forPandemic
Influenza. Board on Population Health and PublicHealth Practice.
Modeling community containment for pan-demic influenza: a letter
report. Washington, DC: Institute ofMedicine of the National
Academies; 2006. http://www.nap.edu/catalog/11800.html.
27.Centers for Disease Control and Prevention. Interim
pre-pandemic planning guidance: community strategy for pan-demic
influenza mitigation in the United Statesearlytargeted, layered use
of nonpharmaceutical interventions.Atlanta: U.S. Department of
Health and Human Services;2007 Feb.
http://www.pandemicflu.gov/plan/community/community_mitigation.pdf.
28.Holmberg SD, et al. State plans for containment of pan-
demic influenza. Emerg Infect Dis 2006;12(9):1414-7.29.U.S.
Department of Health and Human Services. State pan-
demic plans. 2007.
http://www.pandemicflu.gov/plan/states/stateplans.html.
30.U.S. Department of Health and Human Services. Tests,vaccines,
medications, and masks: vaccine prioritization.2006.
http://www.pandemicflu.gov/vaccine/index.html#vprioritization.
31.Kolata GB. Flu: the story of the great influenza pandemic
of1918 and the search for the virus that caused it. New
York:Farrar, Straus and Giroux; 1999.
56 AJN MJuly 2007 M Vol. 107, No. 7
http://www.nursingcenter.com
GENERAL PURPOSES: To provide registered professionalnurses with
current information about influenza andguidelines for preparing for
an influenza pandemic.
LEARNING OBJECTIVES: After reading this article and takingthe
test on the next page, you will be able to discuss the history,
outcomes, and virulence of influenza.
describe the transmission and management of influenza. outline
the key factors to consider when planning for aninfluenza
pandemic.
TEST INSTRUCTIONSTo take the test online, go to our secure Web
site at www.nursingcenter.com/CE/ajn .
To use the form provided in this issue, record your answers in
the test answer section of the CE
enrollment form between pages 56 and 57. Each ques-tion has only
one correct answer. You may make copiesof the form.
complete the registration information and course evalua-tion.
Mail the completed enrollment form and registrationfee of $19.95 to
Lippincott Williams and Wilkins CEGroup, 2710 Yorktowne Blvd.,
Brick, NJ 08723, by
July 31, 2009. You will receive your certificate in four to
sixweeks. For faster service, include a fax number and we willfax
your certificate within two business days of receiving
your enrollment form. You will receive your CE certificate
ofearned contact hours and an answer key to review yourresults.
There is no minimum passing grade.
DISCOUNTS and CUSTOMER SERVICE Send two or more tests in any
nursing journal published by
Lippincott Williams and Wilkins (LWW) together, anddeduct $0.95
from the price of each test.
We also offer CE accounts for hospitals and other healthcare
facilities online at www.nursingcenter.com. Call(800) 787-8985 for
details.
PROVIDER ACCREDITATIONLWW, publisher ofAJN, will award 2 contact
hours for
this continuing nursing education activity.LWW is accredited as
a provider of continuing nursing
education by the American Nurses Credentialing CentersCommission
on Accreditation.
LWW is also an approved provider of continuing nurs-ing
education by the American Association of Critical-Care Nurses
#00012278 (CERP category A), District ofColumbia, Florida #FBN2454,
and Iowa #75. LWWhome study activities are classified for Texas
nursing con-tinuing education requirements as Type 1. This
activityis also provider approved by the California Board
ofRegistered Nursing, provider number CEP 11749, for2 contact
hours.
Your certificate is valid in all states.
TEST CODE: AJN1407
Continuing Education2HOURS
EARN CE CREDIT ONLINEGo to www.nursingcenter.com/CE/ajnand
receive a certificate within minutes.