Embed Size (px)
Citation preview

Quality Culture 1
QUALITY CULTURE AND INTEGRATED COMMUNICATIONS: An exploratory case study in a Thai health care setting
Karinrat Srismith School of Professional Communication
University of Canberra Canberra Australia
.
Presented at
The Annual Meeting of the Australian and New Zealand Communication Association
Christchurch, New Zealand
4-7 July 2005

Quality Control 2

Quality Control 3
Abstract This paper reports some preliminary findings from a research project on Integrated Communications (IC). This study approached IC from an organisational culture perspective. It took the view that organisations must have an organisational culture that allows staff from different departments within an organisation to coordinate and collaborate in their communication efforts. This will enable organisations to fully adopt and practice IC to its potential. This study tested the proposition that an organisation with a ‘Quality Culture’ (deriving from successfully adopting quality management concepts) is likely to have a type of organisational culture facilitating IC. A case study approach was used to understand the contributing role of Total Quality Management (TQM) in IC practice. This study also sought to understand the appropriateness of adopting Western concepts in a Thai context. Data was collected through in-depth interviews and was analysed based on a study framework drawn from the concepts of Competing Values Framework (CVF), Communication Climate, TQM, and IC. The results of this study supported the study’s proposition and revealed the interrelated relationships between CVF cultural type of clan, TQM principles, and communication climate and practice. Responses received also suggested that some aspects of Thai cultural behaviour may benefit IC practice. Introduction The concept of Integrated Communications (IC) has been discussed since the 1960s. Argyis (1960), Levitt (1960), and Nickel (1976) shared a similar view on IC. They agreed on the need for a company to unify its messages, sent through various communication channels, in order to maintain a unified image of the company. The crucial development period of the Integrated Communications concept was in the 1990s when the concept of Integrated Marketing Communications (IMC) was introduced by US academics Schultz, Tannenbaum and Lauterborn (1994). Although the concept has received considerable attention from academics and practitioners on a worldwide scale, many organisations have yet to fully implement the fundamental ideas contained in IMC. This study suggests the easy-to-interpret name, ‘Integrated Marketing Communications’, has led practitioners to perceive IMC as a concept of integrating various marketing communication channels and activities (i.e., advertising, sales promotion, public relations) to create a marketing communication synergy. With this limited view of IMC, other dimensions of IMC such as customer databases, organisational structure, organisational culture, and the mindset of the staff tend to be ignored. This study argues that to successfully implement the concept of communication integration, an organisation needs to take the organisational issues such as organisational culture and structure into consideration. A number of academics and researchers have also claimed that organisational issues are the main barrier to integration (Drobis, 1997; Duncan, 2002; Eagle, Kitchen, Hayde, Fourie, & Padisetti, 1999; Kliatchko, 2005; Prensky, McDarty, & Lucus 1996; Schultz & Kitchen, 1997; Schultz, Tannenbaum & Lauterborn, 1994). Therefore, in this study, the term, Integrated Communications (IC) is used rather than IMC because it offers a broad and unrestricted name that allows viewing integration of communication activities from an organisation-wide level, not just the communication activities being integrated at a marketing department level. Given that this study has approached IC from the organisational context perspective and that no IC definition has been given from this perspective, in this study, the definition of IC is based on the concept of IMC (Schultz et al., 1994), IC (Gronstedt, 1996), and

Quality Control 4
organisational communication (Cheney & Christensen, 2001; Miller, 2003). Accordingly, IC is:
The coordination and collaborative efforts achieved through vertical, horizontal, and simultaneous communication of staffs across departments within an organisation regarding its internal and external communication activities to produce clear and consistent messages.
The Study Research Questions The research questions of this study were derived from reviewing the interplay between IC and its relevant concepts of the Competing Value Framework (CVF), communication climate and Total Quality Management (TQM). Competing Values Framework (CVF) CVF is based on the view that organisational culture is composed of the shared values and beliefs of its members (Hofstede, 1998). This study adopted Cameron and Quinn’s (1999) CVF as a sense-making device to categorise the qualitative findings of organisational culture. According to Cameron and Quinn (1999), an organisation is likely to exhibit some characteristics of all four types: • Clan: culture based on norms and values associated with affiliation and teamwork • Adhocracy: culture based on assumptions of change and risk taking • Hierarchical: culture reflecting the values and norms associated with bureaucracy
such as control, stability, and security • Market: culture emphasising productivity and efficiency However, one type is likely to dominate the organisation’s value system. The work of the researchers using CVF suggested that some cultures have higher effectiveness than others (Cameron & Freeman, 1991; Rogers & Hildebrandt, 1993; Zammuto & Krakower, 1991). In this study, a cultural type of ‘clan’ was assumed to be one of the most appropriate organisational cultures for IC because ‘clan’ is based on norms and values associated with affiliation and teamwork, which are believed to be the key success factor for IC’s context of companywide integration. As a consequence of this investigation, the first research question of this study is: What is the organisational culture at the organisation investigated? Communication Climate The communication climate frameworks of Tukiainen (2001) and Gibb (1961) were used as the study framework. Tukiainen (2001) proposed three dimensions of superior communication and ways of conduct (i.e., the ways to conduct communication; organisational structure and the rules of communication); horizontal face-to-face communication (i.e., peer communication, the general willingness to communicate); and functioning of the communication process (i.e., general functioning of communication flow, quality and quantity of communication flow). Gibb (1961) grouped communication climate based on superiors’ communication attitude and behaviour. According to Gibb (1961), there are two opposite types of communication climates in organisations: defensive climate and supportive climate and, within each type, there are six categories of behavioural characteristics.

Quality Control 5
Table 1: Gibb’s (1961) Defensive and Supportive Communication Climate
Defensive Communication Climate
Supportive Communication Climate
1. Evaluation 1. Description 2. Control orientation 2. Problem orientation 3. Strategy 3. Spontaneity 4. Neutrality 4. Empathy 5. Superiority 5. Equality 6. Certainty 6. Provisionalism
In this study, a supportive communication climate was viewed as positively related to IC practice, particularly for communication in the integration and coordination process. Thus, the second research question is: What is the communication climate at the organisation investigated? Total Quality Management (TQM) According to the TQM literature, an organisation that has been successfully implementing TQM and continuing to improve its quality is likely to have a ‘Quality Culture’. Experts in IC/IMC observed an interplay between IC and TQM (Gronstedt, 1996; Gronstedt & Thorsoon, 1996; Moriarty & Duncan, 1998). Despite having different schools of thought, this study identified eight principles that are commonly viewed as reflecting the notion of TQM (Crosby, 1980; Deming, 1986; Juran, 1988). These principles included: customer focus, common vision, supportive leadership, teamwork, empowerment, continuous improvement, problem solving, and process focus. The fact that TQM principles are built on a fully integrative management effort with a great emphasis on the processes of inter-departmental cooperation (Deming, 1986; Juran, 1988) indicates that TQM is likely to be supportive of IC, particularly for communication in the integration and coordination process. The third research question, is thus, how have TQM principles interacted with the way the studied organisation and its staff communicate? Research Methodology This exploratory case study used in-depth interviews for data collection. In-depth interviews allowed the researcher to investigate the issues comprehensively and in an insightful manner (Cresswell, 1998). The case selected for study was a private, accredited hospital in Bangkok, Thailand. The hospital selected, passed the case selection criteria because the hospital has been accredited nationally and internationally for the commitment to its Total Quality Management program. The respondents of this study included non-medical provider staff from the hospital’s back office (Executive management, TQM, Human resources, Marketing, Education and Training, and Employee relations) and front office (Customer services, Support service, and International centre).

Quality Control 6
Sample Achieved A total of 36 respondents were interviewed. The respondents represented two types of categories: the working section (back office or front office) and working level (management or operation). Table 2. Sample achieved for in-depth interview
Back office (n=18)
Front office (n=18)
Management (n=18) 10 9 Operation (n=18) 8 9
Data Analysis Interview transcripts were stored, organised, and retrieved using the Nvivo qualitative analysis software package (QSR international Pty Ltd, Doncaster, Victoria, Australia). This allowed the researcher to explore and code the interview transcripts to identify themes and patterns systematically. Through this approach, responses were grouped and interpreted according to the theoretical elements contained in the analytical framework. The researcher also recorded the frequency of responses. Since the frequency of the coding was obtained every time the keyword appeared, ‘frequency’ was not used to represent the ‘number of people commenting on the issues’. Rather, the frequency was treated as an indicator of the issue’s significance. In addition to this, the data of this study was analysed from a cross-cultural point of view because the researcher herself is Thai and was studying for a postgraduate degree in a western country for five years before she went back to Thailand to conduct this research project. The findings Some of the following preliminary findings are chosen to be discussed:
Organisational culture of the hospital studied The hospital’s organisational culture appeared to be dominated by the ‘clan’ cultural profile. The coding for ‘clan’ was far greater than the second dominant sub-culture of ‘hierarchy’. The sub-culture of ‘adhocracy’ and ‘market’ arrived at the third and fourth place with similar frequencies. Table 3. Frequency of responses on CVF Dominant
characters Leadership Management Social
glue Strategic emphases
Criteria for
success
TOTAL
CLAN 46 52 153 14 11 84 360 ADHOCRACY 19 9 9 6 7 6 56 HIERARCHY 24 35 72 62 0 2 195 MARKET 13 6 5 28 0 0 52 According to the table, the ‘clan’ dimension dominates in five out of six dimensions of CVF: dominate characteristics, leadership, management, strategic emphases and criteria for success. There is only one social glue dimension that is dominated by ‘hierarchy’. As a result, it seems that the ‘clan’-dominant culture is manifested by the hospital’s way of
Section Level

Quality Control 7
management as well as staff members’ ways of work. Overall, the hospital placed a high value on teamwork. Leaders seemed to play an important role in fostering a collective effort and building teamwork. They also encouraged discussion for ideas and problem solving. Responses received from managerial and operational staff also suggested that the hospital’s managerial staff acted as mentors to their subordinates. According to the findings, managerial staff appeared to be helping, supporting, listening to their subordinates, as well as empowering them by providing training opportunities. The ‘flexible’ value of the ‘adhocracy’ culture profile was found in a context of delivering service to satisfy the customer—not in a context of managing the hospital. Responses on management suggested a ‘hierarchy’ archetype. Members from all groups’ descriptions emphasized the presence of hierarchical value in information management, process, policies, procedures, control, standardization, rules, and documentation. These values indicate a high level of formality and documentation. Interestingly, staff members seemed to have no difficulties with this control mechanism. They felt having a well- structured organisation chart and line of command provided a better direction for job processing as well as communication. The ‘clan’ value of caring about the need of their customers and encouraging loyalty from the customer was very evident in the hospital. In fact, this value attribute received, by far, the highest frequency of all CVF attributes. The customer oriented value governed the hospital’s goal, mission, vision, and strategy towards providing a quality service and keeping the customers satisfied. Therefore, despite a few responses associated with the ‘market’ archetype value of determination to commit with the hospital’s vision and mission and to accomplish goal setting, all of the hospital’s visions, missions, and goals were deliberately set toward satisfying customers. Communication climate of the hospital studied Overall, data suggested that the studied hospital appeared to have a supportive communication climate, especially in its functions of communication process. Nevertheless, responses suggesting a defensive communication climate were also found, and many of them related to staff members’ attitudes and ways of communication. 1. Supportive Communication Climate There was a consistent agreement among the respondents that the hospital had the supportive functions of the communication process that included: • a clear organisational chart, clear line of command, and well-stated job description
that allowed their messages to go though the right channel and be handled efficiently by an authorised person;
• a well established, advanced Information Communication and Technology (ICT) system with a variety of communication channels and tools for both online communication (Internet, intranet, online message board) and offline communication (wireless phones, pagers, SMS on mobiles) that allowed communication messages from inside and outside the hospital to flow simultaneously and quickly. The hospital also integrated its ICT system and customer databases to increase the communication effectiveness of the customer service. For instance, they set up an ‘internal code’ on the customer databases to inform staff about the customer’s special classification (i.e.,

Quality Control 8
VIP, special service requested, or unsatisfied customers) so that the staff could approach a particular customer appropriately;
• clear written rules, policies and procedures regarding internal and external communication activities that allowed staff to work on the same format and in the same direction. For instance, a new or revised policy that needed to be updated online within 72 hours or, an investigation regarding customer complaint needed to follow certain steps and had to be done within a certain period of time. Interestingly, despite having to follow working policies and procedure, many respondents, especially those from the operational level seemed to be satisfied with it. Some staff reported that when they followed the procedure, they felt reassured knowing that they were doing things correctly;
• all communication directions, top-down, horizontal, and bottom up, were found to be positively related to communication supportiveness. Evidence received suggested that the hospital’s management attempted to set up communication mechanisms to encourage more horizontal (i.e., meetings, morning briefings, and group discussions) and bottom up communication (i.e., ‘feedback gathering’ report forms, incident reports). They also attempted to improve the effectiveness of top-down communication (i.e., monthly reports, monitoring work progress). One interesting finding was on the horizontal communication form of ‘meeting’. The meeting seemed to be the place where messages from the top and the bottom level were brought in for discussion at the horizontal level before being sent back to its original source. This facilitated communication flow in all directions. Another interesting finding was that the majority of the operational staff viewed top-down messages as supportive, not defensive. They found top-down messages were clear-cut; they knew exactly what they had to do. This reduced disputes or disagreements which sometimes occurred when tasks were delegated or assigned at their level.
In terms of communication attitude and behaviour, based on Gibb’s (1961) ‘supportive and defensive communication climate’, responses related to supportive communication were rated far higher than those related to defensive communication. Within Gibb’s (1961) supportive attitude and behaviour categories, ‘empathy’ received the highest responses, followed closely by ‘equality’ and ‘problem orientation’ with similar frequencies. Empathetic words indicated that the superior staff were responsive to the subordinate staff’s feelings and thoughts. Words, such as understanding, concern, and interest, were often mentioned by both operational and managerial respondents. As for ‘equality’, the superior staff seemed to act in forms of listening, sharing information, and asking for inputs; whereas the ‘problem orientation’ was often approached in a form of seeking solutions by inviting staff to come together and share ideas. 2. Defensive communication climate Responses for a defensive communication climate were mostly related to bottom up communication and, interestingly, it was mostly related to employees’ communication attitude and behaviour, not the hospital’s functions of communication process. The superior staff were reported to demonstrate Gibb’s (1961) defensive attitude and behaviour categories of ‘superiority’. Some managers made their own decisions and asked their subordinates to follow the decisions made without any explanation. Or,

Quality Control 9
despite listening to subordinate employees’ ideas or problems, some managers did not take any further action. The lack of action caused misunderstandings among some operational staff members; they suspected their upward messages were delayed or lost in the line of command. It was also found that the lack of communication or explanation from the senior staff discouraged subordinate staff from expressing ideas and they tended to think that they were ignored. In fact, in some cases, it was found that some superiors used their ‘superiority’ with ‘empathy’—some managers made a decision in consideration of what should be best for their subordinate staff without a discussion with the subordinate. This caused misunderstandings between the two parties. Besides managerial employees’ defensive communication behaviour, this study found that the defensive behaviour also came from employees at the operational level. Many respondents revealed they felt uncomfortable sending a message upward despite having opportunities to do so. It seemed that they preferred to talk or discuss with someone at their level, and let that person talk with someone at a higher up level. This kind of attitude is commonly related to a Thai attitude called, ‘Kreng Jai’ which is described as extreme reluctance to impose on anyone or disturb his/her personal equilibrium by direct criticism, challenge or confrontation (Sriussadaporn-Charoenngam & Jablin, 1999).
TQM and communication Overall, the majority of the respondents agreed that after the successful implementation of TQM, the hospital’s communication had improved, especially in the hospital’s communication process and system. Respondents found the communication system and process to be better organised, more formalised and well structured which in turn, allowed them to work more effectively and efficiently. The respondents also found that communication in the form of meetings and group discussions were practiced extensively, especially for the purpose of problem solving. The respondents were asked what TQM principles have you found to be related to effective organisational communication within the hospital? Overall, TQM seemed to positively interact with respondents’ communication performance. Responses concerning TQM principles were grouped based on their direct and indirect impact on the hospital and its staff’s communication practices.
Indirect impact on communication practice Three TQM principles: customer focus, continuous improvement and common vision had indirectly affected the hospital employees’ attitude towards their communication practice. 1. Customer focus Almost all respondents spoke confidently about their focus on the hospital’s customers. Responses received showed that the alignment of customer focus had a positive impact on both the hospital’s internal and external communication activities. When communicating internally, staff with a customer focus attitude tended to focus on customers’ interest, not their own interest. By sharing the same focus, staff tended to (1) be more able to compromise with team members; (2) put more effort into coordinating tasks; and (3) be able to reach a consensus in decision making. As for external communication, responses suggested that staff, especially those in the frontline, put more effort in communicating with customers while staff involved in planning marketing

Quality Control 10
communication strategies ensured that their marketing communication activities and messages were ethically conducted. 2. Continuous improvement Responses received, indicate that the continuous improvement principle facilitated communication practices, in terms of the hospital’s, and its staff’s, commitment to provide a better service for its customers. In doing so, it was found that continuous improvement activities included: (1) setting up more ‘customer feedback gathering’ mechanisms; (2) upgrading the hospital’s communication system and facilities; and (3) updating new information, policies, and working procedures on its ‘online document’. In addition to this, improving the hospital’s staff competency through the Service Excellence workshop was found to be positively related to staff’s acknowledgment of the important role of communication in keeping their customers happy. The staff who attended the workshop appeared to be more active in providing useful information for customers. More importantly, they seemed to be more receptive for the hospital communication messages and other useful information so that they could handle customers’ inquiries efficiently. 3. Common vision This principle seemed to interact with communication practice, in terms of creating a shared understanding about the hospital’s vision and mission. It was found that the hospital attempted to repeatedly communicate its vision and mission through various forms of communication channels—from written documents such as a pocket-sized cards containing the hospital’s visions and missions and the hospital’s newsletters to verbal communications such as staff orientations, workshops, and training programs. By reinforcing the hospital’s visions and missions, a shared understanding among staff was created. Respondents reported that they became aware of the hospital’s vision and direction, and this, allowed them to understand their role of contribution in accomplishing the organisational goal. As a result, they tended to be more receptive to the hospital’s messages and communication activities related to the hospital’s vision and mission, as well as more cooperative with the hospital’s organised activities.
Direct impact on communication practice 1. Process focus The majority of the respondents seemed to agree that this principle created the most significant impact on the hospital’s communication practices. According to the respondents, they found the hospital developed a well-structured and integrated information technology system; a formalised documenting system; and well-written organisational rules, policies, and working processes. By having these systems and processes, the respondents reported that they were clear about their roles and responsibilities (through a well-written job description) as well as their working procedure. This resulted in a reduction of confusion and communication errors in the working processes. More importantly, the hospital’s communication seemed to flow better through the generation of the ‘set-up-working-process’, and this allowed managers to constantly monitor and follow up their staff’s working progress.

Quality Control 11
2. Leadership support It was found that the hospital’s managerial staff supported their subordinate staff in several ways. This was achieved through: (1) providing communication facilities and organising a well-structured communication process and system; (2) demonstrating supportive communication attitudes and characteristics. The most frequently mentioned communication attitudes were ‘open-mindedness’, ‘trust’, and ‘respect other ideas’; (3) financially supporting working projects as well as employee’s incentives, rewards, and recognition program, through budget allocation; and, (4) empowering staff through workshops and training programs. Some operational staff who felt they were supported by their superiors expressed enthusiasm for their work. 3. Problem Solving & Teamwork The focus on solving problems brought staff from various working levels and units together in an attempt to find solutions to the problem. The majority of the respondents agreed that working in teams had increased significantly after the hospital’s adoption of TQM. The hospital placed a great emphasis on solving problems—problems should never go unattended. This new working attitude brought in a simultaneous, horizontal communication form of meetings and group discussions. Respondents indicated some positive impacts that resulted from teamwork: (1) sped up working processes (2) better solutions through multi-disciplinary team effort (3) communication flowed in all directions (4) staff were allowed to work in the same direction and in a collaborative manner and; (5) better interpersonal relationships. This latter benefit was often mentioned and was indicated by some respondents as the key to accomplishing their tasks. According to them, when a good personal relationship had developed, each party tended to have more understanding and was more readily prepared to compromise with each other. 4. Empowerment The hospital seemed to empower its staff in two ways: staff competency programs and decision-making. There were a lot of training programs, workshops and classes. Staff reported that they felt equipped with information and knowledge and, that they were more ready and confident in communicating with customers. As for empowerment though decision-making, the management level tended to have the authority to make decisions on important issues such as changing working processes and procedures; whereas staff at the operational level, tended to have authority for tasks related to keeping customers happy.
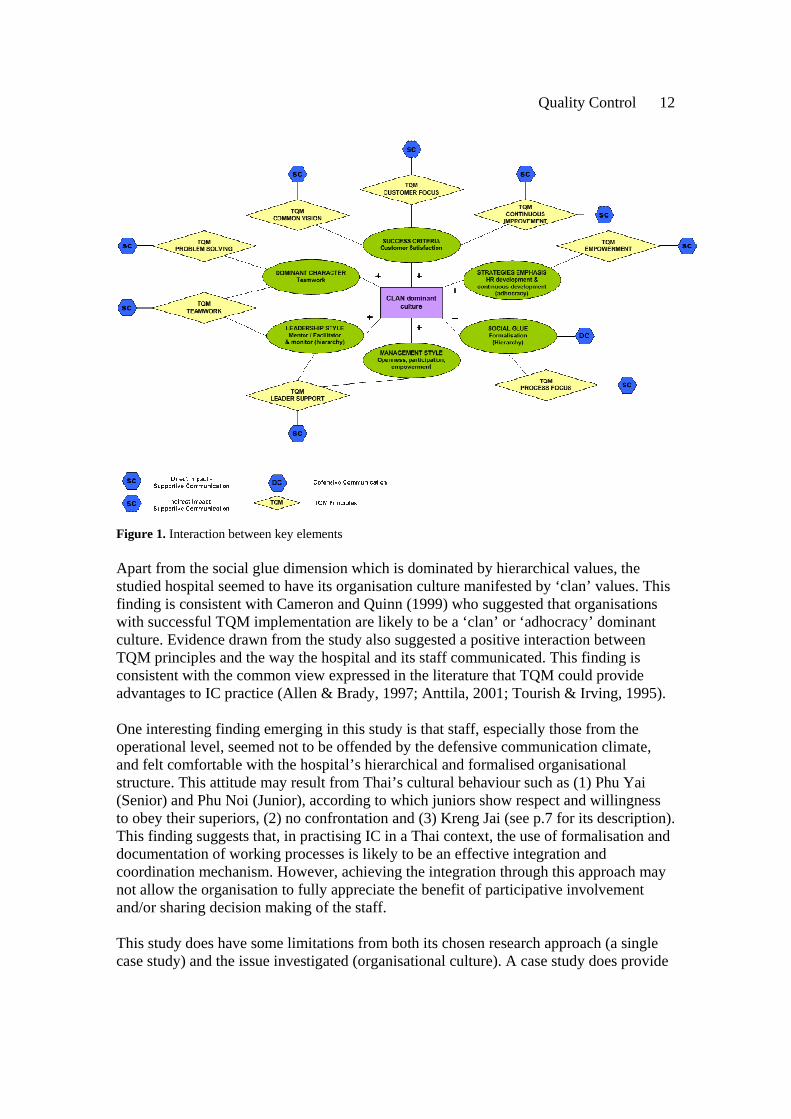
Discussion and Conclusion The results suggest that there is a positive interaction between a culture dominated by a clan profile, TQM principles, and communication attitudes and behaviour, as shown in Figure 1.
Quality Control 12
Figure 1. Interaction between key elements Apart from the social glue dimension which is dominated by hierarchical values, the studied hospital seemed to have its organisation culture manifested by ‘clan’ values. This finding is consistent with Cameron and Quinn (1999) who suggested that organisations with successful TQM implementation are likely to be a ‘clan’ or ‘adhocracy’ dominant culture. Evidence drawn from the study also suggested a positive interaction between TQM principles and the way the hospital and its staff communicated. This finding is consistent with the common view expressed in the literature that TQM could provide advantages to IC practice (Allen & Brady, 1997; Anttila, 2001; Tourish & Irving, 1995). One interesting finding emerging in this study is that staff, especially those from the operational level, seemed not to be offended by the defensive communication climate, and felt comfortable with the hospital’s hierarchical and formalised organisational structure. This attitude may result from Thai’s cultural behaviour such as (1) Phu Yai (Senior) and Phu Noi (Junior), according to which juniors show respect and willingness to obey their superiors, (2) no confrontation and (3) Kreng Jai (see p.7 for its description). This finding suggests that, in practising IC in a Thai context, the use of formalisation and documentation of working processes is likely to be an effective integration and coordination mechanism. However, achieving the integration through this approach may not allow the organisation to fully appreciate the benefit of participative involvement and/or sharing decision making of the staff. This study does have some limitations from both its chosen research approach (a single case study) and the issue investigated (organisational culture). A case study does provide

Quality Control 13
an in-depth understanding of the issue investigated; however, it does not allow generalisations. This is especially the case in a study of organisational culture. Each organisation has its own ways of operating; the same concept may be approached differently and yield a different outcome. More importantly, other factors such as national culture, types of business, and leadership styles may impede or facilitate IC practice. References Allen, M., & Brady, R. (1997). Total quality management, organisational commitment, perceived organisational support, and intraorganisational communication. Management Communication Quarterly, 10 (3), 316-341. Anttila, J. (2001). Effective Quality Communication. Saint Petersburg, FL: The 6th TQM
World Congress. Argyis, C. (1960). Understanding organisational behavior. London: Tavistock. Brannan, T. (1995). The practical guide to integrated marketing communications. London: Kogan Page Limited. Cameron, K. S., & Freeman, S. J. (1991). Cultural congruence, strength, and type: Relationships to effectiveness. In R. W. Woodman & W. A. Passmore (Eds.), Research in organization change and development. Greenwich, CT: JAI Press. Cameron, K., & Quinn, R. E. (1999). Diagnosing and changing organisational culture: Based on the Competing Values Framework. Reading, MA: Addison-Wesley. Cheney, G., & Christensen, L. (2001). Organisational identity: Linkages between
internal and external communication. In F. Jablin & Putnum, L. (Eds.), The new handbook of organisational communication: Advances in theory, research, and methods. Thousand Oaks, CA: Sage Publication.
Cresswell, J. W. (1998). Research design: qualitative & quantitative approaches. Thousand Oaks, CA: Sage. Crosby, P.B. (1980). Quality is free. New York: Penguin Books. Deming, W.E. (1986). Out of crisis. Cambridge, MA: Massachusetts Institute of Technology. Drobis, D. (1997). Integrated marketing communication redefined. Journal of Integrated Marketing Communications, 8, 6-10. Duncan, T. (2002). IMC: Using advertising and promotion to build brands (International Edition). New York: McGraw-Hill. Duncan, T., & Caywood, C. (1996). The concept, process, and evolution of integrated marketing communications. Mahwah, NJ: Lawrence Erbaum Associates. Duncan, T., & Everett, S. (1993).Client perceptions of integrated marketing communications. Journal of Advertising Research, 33(3), 30-39. Eagle, L., Kitchen, P., Hayde, K., Fourie, W. & Padisetti, M. (1999). Perceptions of integrated marketing communications among marketers and ad agency executives in New Zealand. International Journal of Advertising Research, 18(1), 89-119. Gibb, J. R. (1961). Defensive communication. Journal of Communication, 11(3), 141-148. Gronstedt, A. (1996). Integrated communications at America's leading total quality management corporations. Public Relations Review, 22(1), 25- 43. Gronstedt, A., & Thorsoon. E., (1996). Five approaches to organise an integrated

Quality Control 14
marketing communication agency. Journal of Advertising Research, 36(2), 48-58. Hofstede, G. (1998). Identifying organizational subcultures: An empirical approach. Journal of Management Studies, 35(1), 1-12. Juran, J.M. (1988). Juran on Planning for Quality. New York: The Free Press. Kliatchko, J. (2005). Towards a new definition of integrated marketing communications. International Journal of Advertising, 24(1), 7-34. Levitt, T. (1960). Marketing Myopia. Harvard Business Review, 38(4), 45-56. McArthur, D., & Griffin, T., (1997). A marketing management view of integrated marketing communications. Journal of Advertising Research, 37(5), 19-26. Moriarty, S., & Duncan, T. (1998). A communication-based marketing model for managing relationships. Journal of Marketing, 62(2). Miller, K. (2003). Organisational communication: Approaches and processes. Belmont,
CA: Wadsworth Publishing Co. Nickels, W. (1976). Marketing communications and promotion. Ohio: Grid, INC. Prensky, D., McCarty, J.A. & Lucus, J. (1996). Integrated marketing communication:
An organizational perspective. In E.Thorson & Moore, J. (Eds.), Integrated communication: Synergy of persuasive voices (pp.167-183), Lawrence, NJ: Lawrence Erlbaum Associates.
Rogers, P. S., & Hildebrandt W. (1993). Competing values instruments for analyzing written and spoken management messages. Human Resource Management, 32(1), 121-143. Schultz, D., & Kitchen, P. (1997). Integrated marketing communications in U.S. advertising agencies: An exploratory study. Journal of Advertising Research, 37(5), 7-18. Schultz, D., Tannenbaum, S., & Lauterborn, R. (1994). The new marketing paradigm: Integrated marketing communications. Illinois: NTC Publishing Group. Sriussadaporn-Charoenngam, N., & Jablin, F. (1999). An exploratory study of communication competence in Thai organisations. The Journal of Business Communication, 36(4), 382-418. Tourish, D., & Irving, P. (1995). Integrated communications perspectives and the practice of total quality management. International Journal of Health Care Quality Assurance, 8(3). Tukiainen, T. (2001). An agenda model of organisational communication. Corporate Communications: An International Journal, 6(1), 47-52. Zammuto, R. F., & J. Y. Krakower. (1991). Quantitative and qualitative studies of organizational culture. In R. W. Woodman & Passmore, W. A. (Eds.), Research in organizational change and development (pp. 83-114), Greenwich, CF: JAI Press.
Address for correspondence Karinrat Srismith
School of Professional Communication
Division of Communication and Education
University of Canberra, Canberra, Australia





























