Embed Size (px)
Citation preview

Pathology International 2006; 56: 309–314 doi:10.1111/j.1440-1827.2006.01965.x
Blackwell Publishing AsiaMelbourne, AustraliaPINPathology International1320-54632006 Japanese Society of PathologyJune 2006566309314Original ArticlePrognostic factors of phyllodes tumorJ. C. Roa
et al
.
Correspondence: Juan Carlos Roa, MD, Department of Pathology,Faculty of Medicine, Universidad de la Frontera, Manuel Montt 112,Temuco 478-1176, Chile. Email: [email protected]
Received 26 September 2005. Accepted for publication 7February 2006.
Original Article
Prognostic factors of phyllodes tumor of the breast
Juan Carlos Roa,1 Oscar Tapia,1 Paula Carrasco,1 Enrique Contreras,2 Juan Carlos Araya,1 Sergio Muñoz3 and Iván Roa1–4
Departments of 1Pathology and 3Public Health, Universidad de la Frontera, 2Department of Surgery, Hernan Henriquez Aravena Hospital and 4Department of Pathology, Clínica Alemana de Temuco, Temuco, Chile
The phyllodes tumor is characterized by its tendency torecur locally and occasionally to metastasize. The purposeof the present paper was to assess the prognostic value ofclinical–morphological characteristics in patients with phyl-lodes tumor. Forty-seven cases of phyllodes tumors wasstudied; the World Health Organization classification wasused and follow up was obtained. A total of 51%, 28% and21% of the tumors were classified as benign, borderlineand malignant, respectively. The adherence (P = 0.01), size>10 cm (P = 0.001), high mitotic activity (P = 0.03), infiltra-tive tumor margin (P = 0.0002) and type of surgery in malig-nant tumors (P = 0.02) proved to be good predictors ofrelapse. The presence of pain (P = 0.03), postmenopausalstatus (P < 0.04), heavy cellular pleomorphism (P = 0.007),high mitotic activity (P = 0.002), tumoral grade (P = 0.006)and metastasis (P < 0.00001) were prognostic factors ofpoor survival. Tumoral grade and some clinical–morpholog-ical characteristics of patients with phyllodes tumors havea significant impact on the prediction of its biologicalbehavior.
Key words: phyllodes tumor, prognostic factors, tumoral grade
The phyllodes tumor, also known as cystosarcoma phyllodes,is a fibroepithelial tumor first described in 1838 by JohannesMüller1 and it represents between 0.3 and 0.5% of all breastneoplasias.2–8 It is a rare disease that affects women almostexclusively, generally in the third to fourth decade of life,although cases in adolescence have been reported.4,9–12
Factors that predispose to the development of a phyllodestumor have not been identified; but morphological and cyto-genic studies have demonstrated similar characteristicsbetween this tumor and fibrodenomas, suggesting progres-sion to a cystosarcoma phyllodes.3,9,13–15
Clinically they correspond to a large, solid, painful, well-circumscribed, movable mass, not having a characteristicpattern in mammography or breast ultrasound.9,16
One of the main characteristics of this tumor is the ten-dency to recur locally and also to metastasize, with a localrelapse rate of up to 20% after surgical resection.3,6,9,10,12,16,17
This unpredictable behavior can be explained in part by thetumor histological characteristics, which have led to variousclassification systems.3–6
In order to establish a diagnosis, most patients undergo anexcisional biopsy or mastectomy because a fine-needlebiopsy is generally insufficient to obtain adequate numbersof stromal cells for analysis.9,16,18
Controversies exist regarding the surgical procedure uti-lized for the management of these patients, as well as thechoice of adjuvant treatment in the case of local relapse ormetastasis.3,4,7,19–21
Some authors have concluded that there are no gross orhistological findings that enable reliable separation of benignfrom malignant phyllodes tumors,22,23 while others dis-agree.22–25 Some have defined a third borderline category.26
The objective of the present study was to analyze clinicaland morphological characteristics in order to assess thevalidity of parameters and/or classification that should beused to predict the biological behavior of this neoplasia.
MATERIALS AND METHODS
Forty-seven patients with a phyllodes tumor diagnosis wereregistered in the files of the Surgical Pathology unit ofthe Hernán Henriquez Aravena Hospital in Temuco, Chilebetween January 1966 and December 2003. Access wasgranted to the file materials, the clinical records and followup in all cases. The La Frontera University Ethics committeeapproved the study.
Demographic variables and clinical records such as sex,age, race, age of menarche, age of first child, number of

310 J. C. Roa et al.
children, duration of lactation and chief complaint wereanalyzed. Postmenopausal and premenopausal status wasregistered. The tumor’s characteristics upon physical exami-nation included location, presence of pain, changes in theskin and nipple, size (measured by the pathologist in at leasttwo dimensions), consistency and adherence. Also consid-ered in the analysis were the type of treatment carried out,as well as local relapse and metastasis.
For the analysis of the morphological variables, a qualita-tive estimation was performed of the extent of cellular atipiaand pleomorphism, the number of mitoses, tumor margin(compressive–infiltrative), stromal pattern and heterologousstromal differentiation according to the criteria proposed bythe World Health Organization (WHO).27 The tumor grade wasclassified into three groups (benign, borderline and malig-nant) depending on the following elements: (i) stromal cellu-larity: low, intermediate or high; (ii) cellular pleomorphism:light, moderate or heavy (Fig. 1); (iii) number of mitoses: >10mitoses per 10 high-power fields (HPF), malign, or ≤4,benign; (iv) tumor margin (microscopically determined): com-pressive or infiltrative; and (v) stromal pattern: with homoge-neous, heterogeneous distribution or with overgrowth.
In accordance with these variables, a malignant or high-grade tumor was defined as that which presented a maximumgrade of at least four variables. A benign tumor complied withthree or more of these characteristics at lowest grade andhad a maximum of two variables at intermediate grade. Finallyan intermediate or borderline tumor corresponded to thosethat did not fall into the aforementioned categories.
Statistical analysis
The analysis of categorical variables such as sex, race andhistological type was performed using Fisher’s exact test. Forcontinuous variables, the Student’s t-test was used. Kaplan–Meier estimates and curves were used to analyze time todeath variables, and the comparison was done by applyinglog–rank.
RESULTS
Clinical data
All 47 cases corresponded to female patients with an averageage of 42.5 years at the time of diagnosis, 16.6% belongedto the Mapuche amerindian ethnic group. Most patients werepremenopausal (74%). The chief complaint was the discov-ery of a tumor upon self-examination in 73% of cases.
The mean age of the patients at the time of first child birthwas 26.7 years and the average parity was 1.7, with anaverage lactation period of 15 months.
Upon physical examination a large solid, movable masswas detected. It was painful in one-third of cases (Table 1).The presence of pain proved to be a statistically significantprognostic factor in the survival time of these patients(P = 0.03), as was the fixation to neighboring tissues.
Morphological data
The frequency of benign, borderline and malignant phyllodestumor was 51%, 28% and 21%, respectively. The variablesthat best correlated to tumor relapse were: >4 mitoses per10 HPF (P = 0.03) and infiltrative tumor margin (P = 0.0002;Table 2). Other variables important in tumor relapse that arenot part of the WHO classification were adherence (definedas tumor fixed to deeper tissues; P = 0.01), and tumor size>10 cm (P = 0.001).
Treatment
Conservative surgical treatment (lumpectomy) was carriedout in two-thirds of cases. Patients with lower grade tumor,averaging 8.6 cm in diameter relapsed less frequently. Incontrast, patients with high-grade tumors averaging 12 cm indiameter (Fig. 2) relapsed in 60% of cases, independent ofthe treatment given (lumpectomy vs mastectomy; Table 3).Adjuvant treatment (radiotherapy/chemotherapy) was per-formed in three cases. In these three cases the surgicaltreatment performed was a total mastectomy: two patientshad high-grade malignant tumors and one had metastasis.The third patient had an 18 cm, low-grade tumor and a neg-ative surgical resection margin. Mastectomy produced better
Table 1 Relapse and survival association with clinical character-istics (n = 47)
VariableRelapse
n (%)Deathn (%) Relapse Survival
Skin lesionsYes 2/8 (25) 2/8 (25) NS NSNo 7/39 (18) 2/39 (5)
Nipple lesionYes 1/2 (50) 0/2 (0) NS NSNo 8/45 (18) 4/45 (9)
PainYes 5/16 (31) 4/16 (25) NS P = 0.003No 4/31 (13) 0/31 (0)
AdherenceYes 4/8 (50) 2/8 (25) P = 0.01 NSNo 5/39 (13) 2/39 (5)
Size ≥ 10 cmYes 9/25 (36) 2/25 (8) P = 0.001 NSNo 0/22 (0) 2/22 (9)
PostmenopausalYes 4/12 (33) 3/12 (25) P = 0.01 NSNo 5/35 (14) 1/35 (3)
Prognostic factors of phyllodes tumor 311
results than lumpectomy in malignant cases with regard torelapse status (P = 0.02).
One patient with benign tumor relapsed. For the borderlineand malignant tumors a non-statistically significant greaterrelapse rate was observed (histological features andrelapse). At the time of relapse, all the cases catalogued asmalignant had a high mitotic count with a sarcomatoid com-ponent in the tumoral stroma. The case classified as benigndid not have any significant morphological difference with
respect to the original biopsy sample. Of the two casescatalogued as borderline, only one had a high cellularity ofthe stroma and a high mitotic count.
Survival
The median survival time for the group was 96 months. Sta-tistically significant poorer survival rates were associatedwith cellular pleomorphism (P = 0.007), the presence of >10mitoses per 10 HPF (P = 0.002), tumor grade (P = 0.006)and the presence of metastasis (P < 0.000001; Fig. 3) Ofthe nine patients who relapsed, four presented multiplemetastases (predominantly pulmonary), and died a shorttime later. In the rest, the disease was controlled with acombination of radical surgery and chemotherapy and/orradiotherapy.
DISCUSSION
Numerous classifications have attempted to predict the bio-logical behavior of this tumor. All of them include the samemorphological variables such as hypercellularity, number ofmitoses, tumor margin, stromal pattern, cellular atypia andtumor size. Most authors recognize the existence of threetumor grades of phyllodes tumor: benign, borderline andmalignant neoplasias.4,5,10,12,19,28–31
Mangi et al. find no correlation between histological gradeand tumor behavior.9 In the present series, in agreement withother publications, the criteria proposed by the WHO weregood indicators of survival time as well as tumorrelapse.4,5,10,31
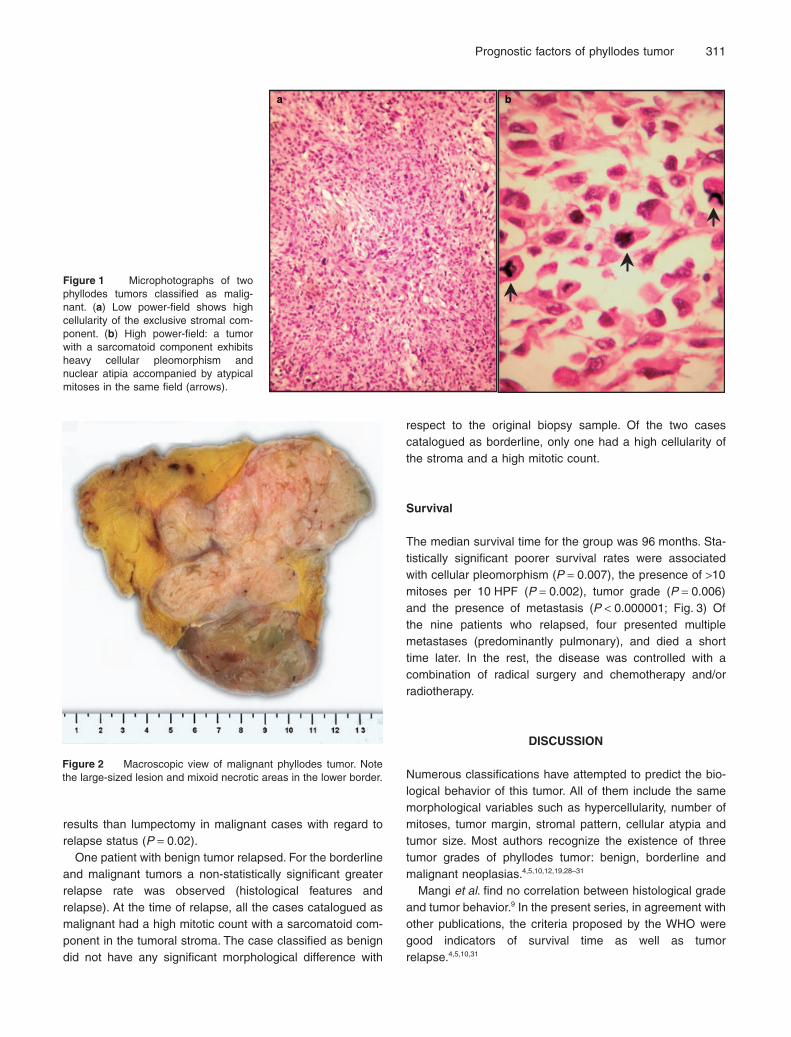
Figure 1 Microphotographs of twophyllodes tumors classified as malig-nant. (a) Low power-field shows highcellularity of the exclusive stromal com-ponent. (b) High power-field: a tumorwith a sarcomatoid component exhibitsheavy cellular pleomorphism andnuclear atipia accompanied by atypicalmitoses in the same field (arrows).
a b
Figure 2 Macroscopic view of malignant phyllodes tumor. Notethe large-sized lesion and mixoid necrotic areas in the lower border.

312 J. C. Roa et al.
In agreement with other studies, the univariate analysisdemonstrated that cellular pleomorphism and the number ofmitosis were useful to estimate overall survival time and localrelapse (P < 0.05). Moreover, involvement of tumor marginswas correlated with local relapse, these findings coincidewith results of other studies.5,9,10,21,32,33 In the present series,three of the variables suggested by the WHO (mitotic index,tumors margin and pleomorphism) turned out to be predic-tors of survival and/or relapse; in addition, the value of themitotic count was more statistically significant than the com-bined use of the variables in predicting poor survival. Tworecent publications of series of patients with phyllodestumors that assess morphological characteristics and biolog-ical behavior obtained results similar to ours using the samevariables, thereby reinforcing the importance of using stan-dardized criteria for the classification of these tumors.31,34
Although the size of the tumor is not included in the WHOcriteria, it should be considered because it has proved to bea prognostic factor in survival time and tumor relapse, assuggested by de Roos et al.10 and Rowell et al.3 Most pub-lished series indicate that this pathology is exclusive to
female patients, as do all of the present cases. However,there are reports of isolated cases of phyllodes tumor inmale patients.35
The average age of presentation in the current serieswas 42.5 years, which coincides with that of publishedseries, which vary between 39 and 44 years.4,9–11,13 Thistumor is characterized by its clinical presentation in themajority of cases as large, solid, unilateral masses.4,10 Uponphysical examination, changes to the skin or nipple couldbe verified in 16% and 3%, respectively, and presentingpain in one-third of the cases, which is similar to otherreported series.5,9 Pain proved to be a prognostic factor oflesser survival time in the present series (P < 0.05). Theimportance of determining the fixation of the tumor to softtissues during physical examination becomes importantbecause this parameter proved to be related to localrelapse (P = 0.01).
One of the main problems with this tumor is its tendencyto recur locally and occasionally to metastasize, the latteroccurring in two patients in the present series (4%), with bothtumors being high-grade malignant ones. In one of these
Table 2 Histological variables
Variable
Tumoral grade
SurvivalP = 0.006
RelapseNS
Benign Borderline Malignant
No relapse(n = 23)n (%)
Relapse(n = 1)n (%)
No relapse(n = 11)n (%)
Relapse(n = 2)n (%)
No relapse(n = 4)n (%)
Relapse (n = 6)n (%)
MarginCompressive 20 (87) 1 (100) 9 (82) 1 (50) 3 (75) 4 (67) NS P = 0.0002Infiltrative 3 (13) 2 (18) 1 (50) 1 (25) 2 (33)
CellularityLow 13 (57) 2 (18) NS NSIntermediate 7 (30) 1 (100) 6 (55)High 3 (13) 3 (27) 2 (100) 4 (100) 6 (100)
StromaHomogeneous 19 (83) 1 (100) 6 (55) NS NSHeterogeneous 3 (13) 3 (27) 2 (100)Overgrowth 1 (4) 2 (18) 4 (100) 6 (100)
PleomorphismLow 10 (43) 1 (100) 2 (18) 1 (50) P = 0.007 NSIntermediate 13 (57) 7 (64) 1 (50) 1 (25)High 2 (18) 3 (75) 6 (100)
Mitosis (X 10 HPF)<10 20 (83) 0 (0) 6 (46) 1 (8) 0 (0) 2 (20) P = 0.002 P = 0.03≥10 3 (13) 1 (4) 5 (38) 1 (8) 4 (40) 4 (40)Average 0.8 (0–5) 3 4.1 (0–10) 7 (4–10) 13.3 (10–20) 15 (8–20)
HPF, high-power field.
Table 3 Surgical treatment performed
Histologicalgrade
Averagesize
(mm)
Lumpectomy Mastectomy
Follow up(months) P †
Relapsen (%)
No relapsen (%)
Relapsen (%)
No relapsen (%)
Benign (n = 24) 86 1 (6) 14 (94) 0 (0) 9 (100) 95 (9–206) NSBorderline (n = 13) 85 2 (22) 7 (78) 0 (0) 4 (100) 107 (12–196) NSMalignant (n = 10) 120 5 (100) 0 (0) 1 (20) 4 (80) 90 (7–230) 0.02
†Fisher’s exact test.

Prognostic factors of phyllodes tumor 313
cases a lumpectomy was performed with no subsequentcomplementary treatment, with a survival time of 7 months.In the other patient a total mastectomy was performed withsubsequent chemotherapy and radiotherapy, presenting asurvival time of 22 months. In both patients metastatic com-promise affected the lung and in one of them there was alsohepatic involvement. This is coincident with the Reinfusset al. series of 170 cases, in which the most frequentlyaffected organ was the lung.5
Presently it is still difficult to predict the clinical course ofthe patients, the final result appearing to be determinedmore by the biology of the tumor than by changes in localsurgical treatment. It would be important to discover prog-nostic factors of a genetic–molecular nature to identifypatients with a more aggressive disease, with greater localrelapse and eventual metastasis. Furthermore subsequentstudies are required to evaluate the real impact of adjuvanttherapy.
ACKNOWLEDGMENTS
This study was supported in part by Research Division, Uni-versidad de la Frontera (DIUFRO Grant). The authors thankHelen Lowry PhD for translation.
REFERENCES
1 Fiks A. Cystosarcoma phyllodes of the mammary gland:Muller’s tumor. For birthday of Johannes Muller. Virchows ArchA Pathol Anat Histol 1981; 392: 1–6.
2 Matar N, Soumani A, Noun M et al. Phyllodes tumors of thebreast. Forty one cases. J Gynecol Obstet Biol Reprod (Paris)1997; 26: 32–6 (in French).
3 Rowell MD, Perry RR, Hsiu JG et al. Phyllodes tumors. Am JSurg 1993; 165: 376–9.
4 Chaney AW, Pollack A, McNeese MD et al. Primary treatmentof cystosarcoma phyllodes of the breast. Cancer 2000; 89:1502–11.
Figure 3 Predictive factors of survival (Kaplan–Meier curves). Four survival charts that show marked differences in survival for differentdegrees of (a) cellular pleomorphism (P = 0.007), (b) mitotic index (P = 0.002), (c) tumoral grade (P = 0.006), and (d) presence of metastasis(P < 0.00001).
0.2
0.4
0.6
0.8
1
0
1.2
0.2
0.4
0.6
0.8
1
0
1.2
Pro
bab
ility
240180120600 240180120600
Survival (months)
Low
Intermediate
Severe≥ 10 mitoses X 10 HPF
< 10 mitoses X 10 HPF
Malignant
Benign–borderline
(a) (b)
(c)
(d)
Metastasis
No metastasis

314 J. C. Roa et al.
5 Reinfuss M, Mitus J, Duda K et al. The treatment and prognosisof patients with phyllodes tumor of the breast: An analysis of170 cases. Cancer 1996; 77: 910–16.
6 Sallusti E, Simonelli I, Marzullo A et al. The breast phyllodestumor: Surgical therapy following report. G Chir 2004; 25: 95–7 (in Italian).
7 Khan SA, Badve S. Phyllodes tumors of the breast. Curr TreatOptions Oncol 2001; 2: 139–47.
8 Mezi S, Pallotta M, Filippini A et al. Diagnosis, prognosis andtherapy of phyllodes tumor of the breast. G Chir 1992; 13: 413–17 (in Italian).
9 Mangi AA, Smith BL, Gadd MA et al. Surgical management ofphyllodes tumors. Arch Surg 1999; 134: 487–92;discussion492–3.
10 de Roos WK, Kaye P, Dent DM. Factors leading to local recur-rence or death after surgical phyllodes tumours of the breast.Br J Surg 1999; 86: 396–9.
11 Stebbing JF, Nash AG. Diagnosis and management of phyl-lodes tumour of the breast: 33 cases at a specialist centre. AnnR Coll Surg Engl 1995; 77: 181–4.
12 Gabriele R, Borghese M, Corigliano N et al. Phyllodes tumorof the breast. Personal contribution of 21 cases. G Chir 2000;21: 453–6 (in Italian).
13 de Aretxabala X, Roa I, Contreras E et al. Cystosarcoma phyl-lodes of the breast: Clinical and morphological 17 cases. RevMed Chil 1987; 115: 952–5 (in Spanish).
14 Rosen PP. Neoplasias fibroepiteliales. In: Rosen PP, ed.Patología Mamaria de Rosen. Madrid: AMOLCA, 2005; 163–200 (in Spanish).
15 Michaud P, Chave B, Lemaire B et al. Phyllodes breast tumors.Rev Fr Gynecol Obstet 1989; 84: 944–9 (in French).
16 Vos DI, Mastboom WJ, de Vos RA. Phyllodes tumor in thebreast. Ned Tijdschr Geneeskd 1998; 142: 716–21 (in Dutch).
17 Haberthur F, Torhorst J, Feichter GE. Rare breast tumors. TherUmsch 1993; 50: 359–65 (in German).
18 Iau PT, Lim TC, Png DJ et al. Phyllodes tumour: An update of40 cases. Ann Acad Med Singapore 1998; 27: 200–203.
19 Salvadori B, Cusumano F, Del Bo R et al. Surgical treat-ment of phyllodes tumors of the breast. Cancer 1989; 63:2532–6.
20 Barth RJ Jr. Histologic features predict local recurrence afterbreast therapy of phyllodes tumors. Breast Cancer Res Treat1999; 57: 291–5.
21 Bennett IC, Khan A, De Freitas R et al. Phyllodes tumours: Aclinicopathological review of 30 cases. Aust NZ J Surg 1992;62: 628–33.
22 Blichert-Toft M, Hansen JP, Hansen OH et al. Clinical courseof cystosarcoma phyllodes related to histologic appearance.Surg Gynecol Obstet 1975; 140: 929–32.
23 Blumencranz PW, Gray GF. Cystosarcoma phyllodes. Clinicaland pathologic study. NY State J Med 1978; 78: 623–7.
24 Hart WR, Bauer RC, Oberman HA. Cystosarcoma phyllodes.A clinicopathologic study of twenty-six hypercellular periductalstromal tumors of the breast. Am J Clin Pathol 1978; 70: 211–16.
25 McDivitt RW, Urban JA, Farrow JH. Cystosarcoma phyllodes.Johns Hopkins Med J 1967; 120: 33–45.
26 Pietruszka M, Barnes L. Cystosarcoma phyllodes: A clinico-pathologic analysis of 42 cases. Cancer 1978; 41: 1974–83.
27 Bellocq J, Magro G. Fibroepithelial tumors. In: Tavassoli F,Devilee P, eds. World Health Organization Classification ofTumours. Pathology and Genetics of Tumours of the Breast andFemale Genital Organs. Lyon: IARC Press, 2003; 99–103.
28 Reinfuss M, Mitus J, Stelmach A. Phyllodes tumor of the breast.Strahlenther Onkol 1995; 171: 5–11.
29 Trifonov D, Aleksiev B, Sedloev T et al. Phyllodes tumors of thebreast. Khirurgiia (Sofiia) 1998; 51: 14–16 (in Bulgarian).
30 Ciatto S, Bonardi R, Cataliotti L et al. Phyllodes tumor of thebreast: A multicenter series of 59 cases. Coordinating Centerand Writing Committee of FONCAM (National Task for BreastCancer), Italy. Eur J Surg Oncol 1992; 18: 545–9.
31 Tan PH, Jayabaskar T, Chuah KL et al. Phyllodes tumors of thebreast: The role of pathologic parameters. Am J Clin Pathol2005; 123: 1–12.
32 Kapiris I, Nasiri N, A’Hern R et al. Outcome and predictivefactors of local recurrence and distant metastases followingprimary surgical treatment of high-grade malignant tumours ofthe breast. Eur J Surg Oncol 2001; 27: 723–30.
33 Hart J, Layfield LJ, Trumbull WE et al. Practical aspects in thediagnosis and management of cystosarcoma phyllodes. ArchSurg 1988; 123: 1079–83.
34 Chen WH, Cheng SP, Tzen CY et al. Surgical treatment ofphyllodes tumors of the breast: Retrospective review of 172cases. J Surg Oncol 2005; 91: 185–94.
35 Konstantakos AK, Graham DJ. Cystosarcoma phyllodes tumorsin men. Am Surg 2003; 69: 808–11.

![Aggressive malignant phyllodes tumor€¦ · phyllodes tumor was classically known as cystosarcoma phyllodes becauseoftheleaf-likeprojections[3,4].Renamedphyllodestumor in the early](https://img.dokumen.tips/doc/110x75/5f0251577e708231d403ac91/aggressive-malignant-phyllodes-tumor-phyllodes-tumor-was-classically-known-as-cystosarcoma.jpg)



























