Embed Size (px)
Citation preview

Preventive Ophthalmology
Melissa A. Dator & Jay Grace U. HernandezASMPH 2013
Blindness and Visual Impairment: Global Facts 284 million people are visually impaired
worldwide – 39 million are blind 80% of visual impairment can be prevented,
treated or cured!
Blindness in the Philippines one hundred children lose their sight every
week Almost half of these cases are either treatable
or preventable. Poor nutrition, measles, and premature birth are
among the leading causes of preventable blindness in children.
Early detection and treatment are the keys to saving the sight of these children.
Individuals at risk should be easily identified
Population screening should be easy to perform, accurate and reliable
Preventive measures should be effective and acceptable to the target population
Needs cooperation among all members of society
Prevention of OCULAR injuries
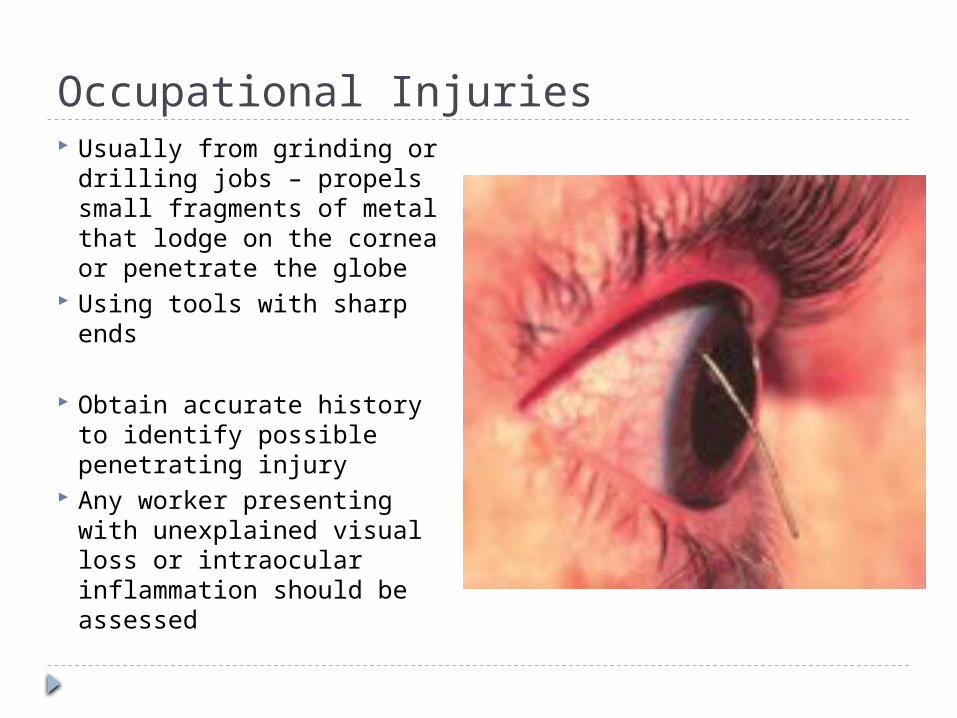
Occupational Injuries Usually from grinding or
drilling jobs – propels small fragments of metal that lodge on the cornea or penetrate the globe
Using tools with sharp ends
Obtain accurate history to identify possible penetrating injury
Any worker presenting with unexplained visual loss or intraocular inflammation should be assessed
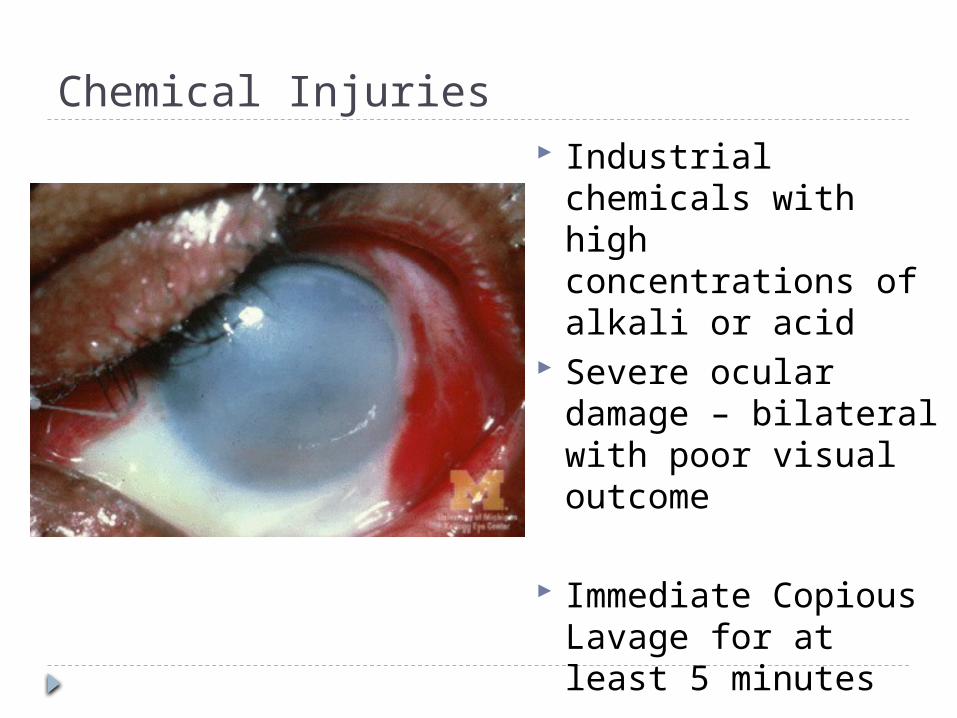
Chemical Injuries Industrial chemicals
with high concentrations of alkali or acid
Severe ocular damage – bilateral with poor visual outcome
Immediate Copious Lavage for at least 5 minutes
Protective Equipment Workers must be
properly trained in the use of tools, machinery, chemicals
Safety goggles must be worn at all times
Educate
Non-Occupational Injuries
Non-Occupational Injuries High incidence of
severe injuries in various sports #1 cause of eye
injuries in children under 16
Corneal abrasions, lid hematomas, retinal detachments, internal bleeding
Availability of toughened plastic protective glasses with refractive correction
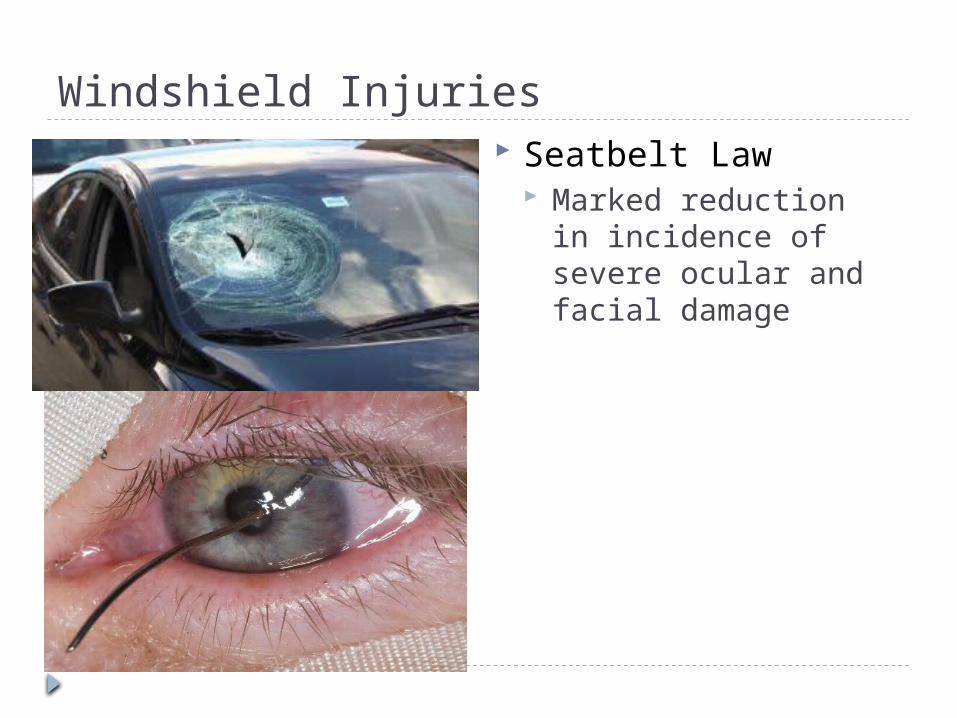
Windshield Injuries Seatbelt Law
Marked reduction in incidence of severe ocular and facial damage
Bottle Cork Injury
Violent Assaults Unexploded Bombs and Land mines – major
cause of corneal blindness in children in countries at war
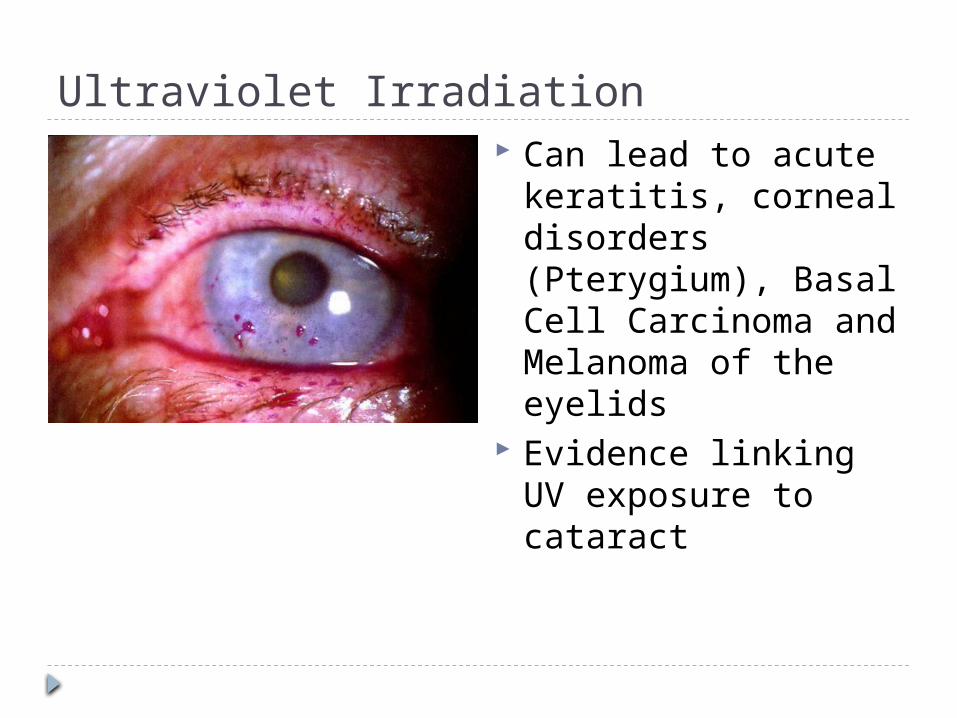
Ultraviolet Irradiation Can lead to acute
keratitis, corneal disorders (Pterygium), Basal Cell Carcinoma and Melanoma of the eyelids
Evidence linking UV exposure to cataract
Sunglasses = NOT protective
Exposure to UV light happens at birth
Not advisable to put sunblock on the eyes
Educate public of dangers of prolonged sun exposure
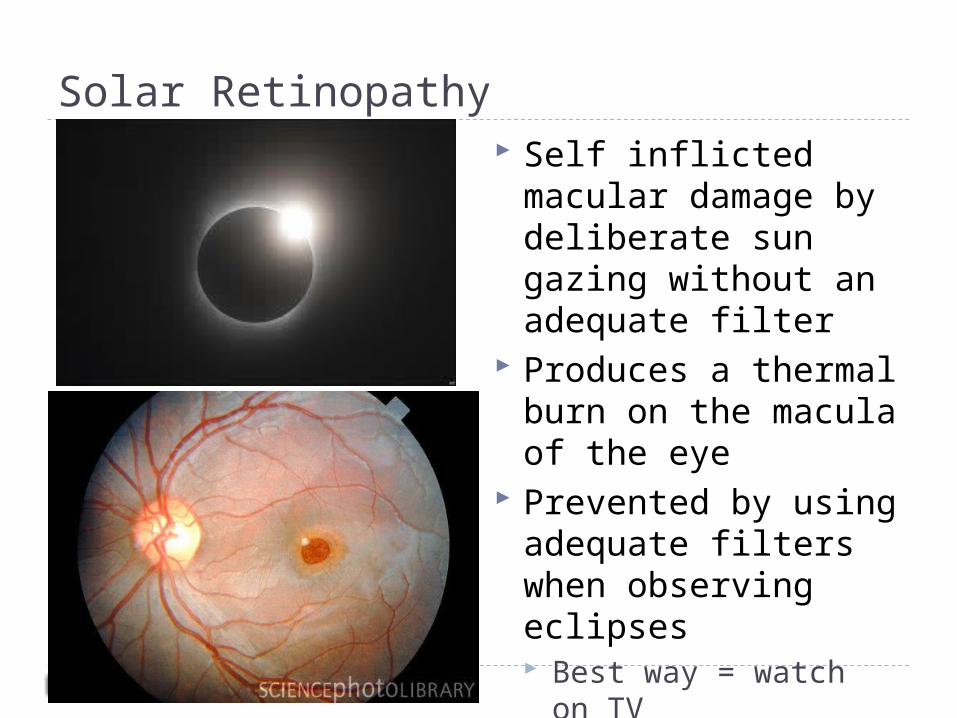
Solar Retinopathy Self inflicted macular
damage by deliberate sun gazing without an adequate filter
Produces a thermal burn on the macula of the eye
Prevented by using adequate filters when observing eclipses Best way = watch on
TV
Prevention of Acquired Ocular Infections
Prevention of Acquired Ocular Infections Infections – major cause of preventable ocular
morbidity Major barrier to infection – epithelium of the cornea
and conjunctiva Can be damaged directly by trauma (surgical or contact
lens) or secondary effects of abnormalities of the outer eye (lid abnormalities or tear deficiency)
Corneal or Conjunctival Epithelial Defect (trauma or surgery) – use prophylactic antibiotic therapy
Avoid accidental epithelial injury in compromised eyes
Comatose patients are at risk for corneal exposure – prophylactic eyelid taping

Preoperative and Perioperative Prophylaxis Ocular environment must be assessed pre-op
to identify and treat any sources of pathogenic organisms
Pre-op instillation of Povidone-Iodine into conjunctival sac has shown to be beneficial
S. epidermidis – major cause of endophtalmitis after cataract surgery; colonizes the eyelids
Sterility must be ensured in the operative field
Contact Lens Wear and Suppurative Keratitis
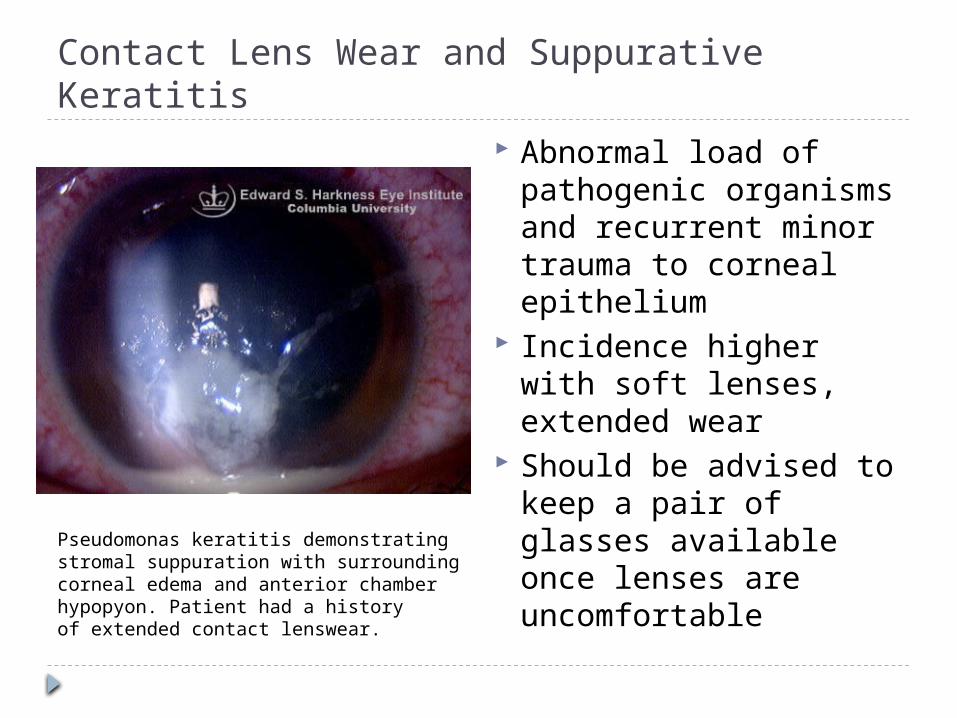
Pseudomonas keratitis demonstrating stromal suppuration with surrounding corneal edema and anterior chamber hypopyon. Patient had a history of extended contact lenswear.
Abnormal load of pathogenic organisms and recurrent minor trauma to corneal epithelium
Incidence higher with soft lenses, extended wear
Should be advised to keep a pair of glasses available once lenses are uncomfortable
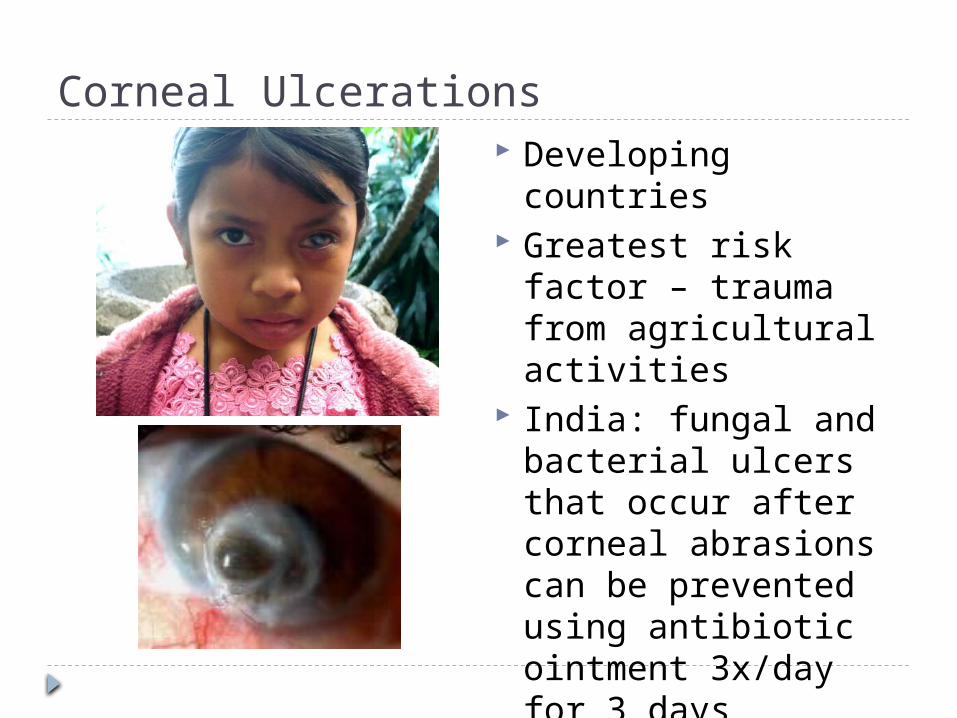
Corneal Ulcerations Developing countries Greatest risk factor –
trauma from agricultural activities
India: fungal and bacterial ulcers that occur after corneal abrasions can be prevented using antibiotic ointment 3x/day for 3 days
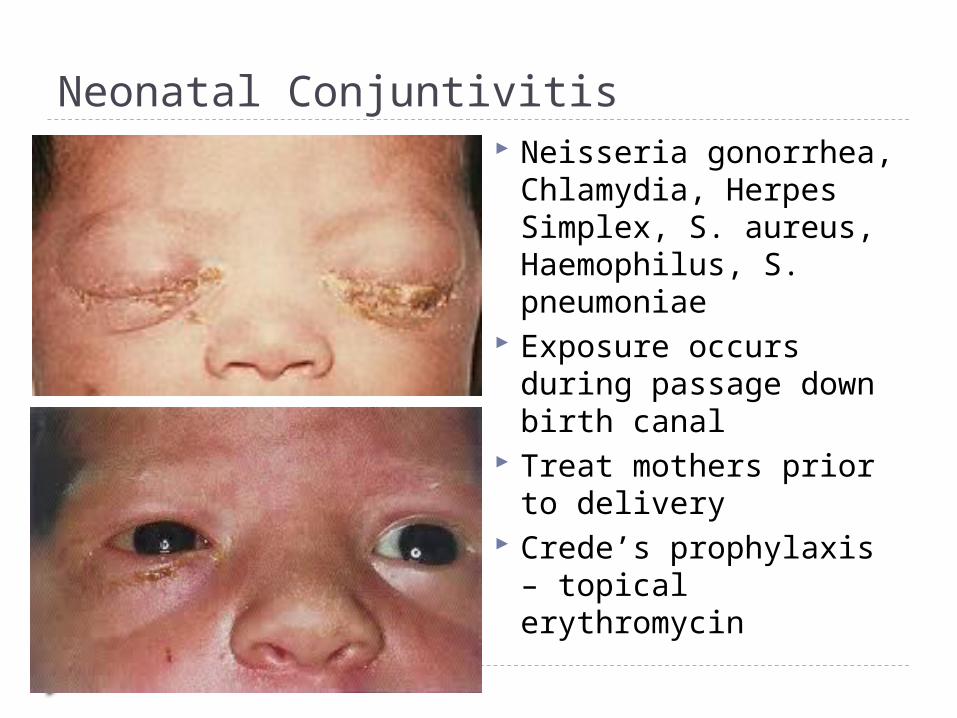
Neonatal Conjuntivitis Neisseria gonorrhea,
Chlamydia, Herpes Simplex, S. aureus, Haemophilus, S. pneumoniae
Exposure occurs during passage down birth canal
Treat mothers prior to delivery
Crede’s prophylaxis – topical erythromycin
Prevention of Iatrogenic Ocular Infection
Epidemic Keratoconjunctivitis Adenovirus – hands, tonometer, droppers that
rubbed against infected eyes Pseudomonas aeruginosa – ophthalmic
solutions Sterilize tonometer by wiping with 70%
isopropyl alcohol swabs then allow to dry before use Immerse in disinfectant at the end of each working
day
HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHINGHAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHINGHAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHINGHAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHINGHAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHING HAND WASHINGHAND WASHING HAND WASHING HAND WASHING HAND WASHING
Prevention of Ocular Damage due to Congenital Infections

Rubella and CMV – most damaging to the infant
Rubella can be prevented by vaccination
Infantile Glaucoma
Toxoplasmosis May lead to
Chorioretinitis Cerebral or Cerebellar Calcification Hydrocephalus CNS Abnormalities
Prevention: eating meat that is well cooked, washing fruits and vegetables, wearing gloves when disposing cat litter
Prevention of Genetic Diseases with Ocular Involvement
Prevention of Genetic Diseases with Ocular Involvement Genetic counseling
childhood diabetes retinitis pigmentosa consanguineous mating Retinoblastoma Neurofibromatosis
Amniocentesis Down syndrome
Early Detection of Treatable Ocular Disease
Age-Related Macular Degeneration leading cause of permanent visual loss in the
elderly in industrialized countries >50 yo Types:
atrophic ("dry") degeneration exudative ("wet") degeneration
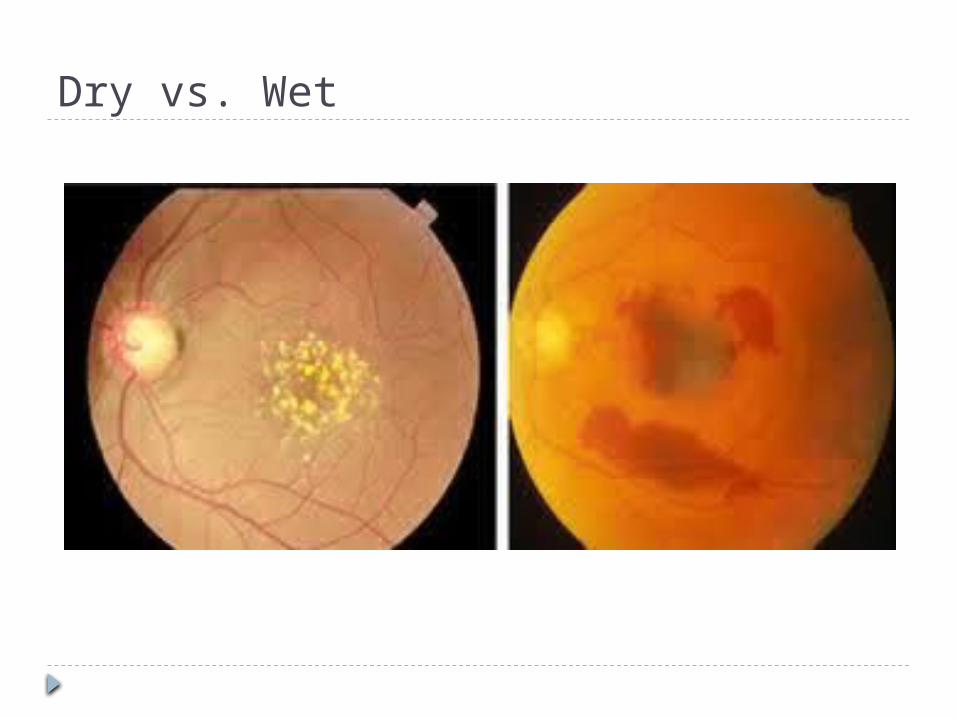
Dry vs. Wet
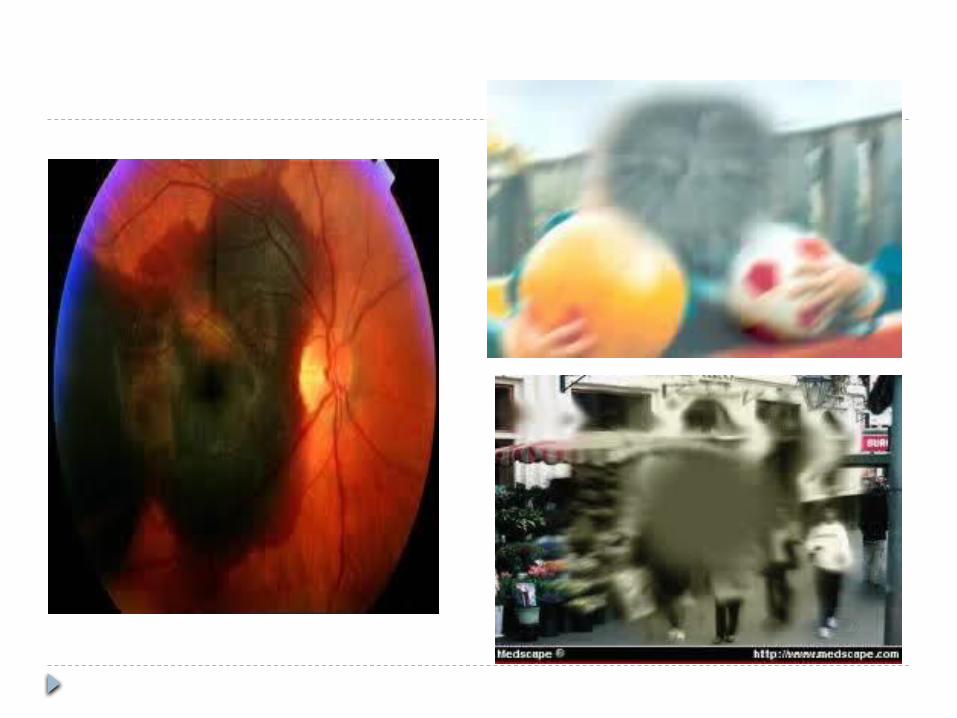
Delaying Onset of Central Visual Loss
Treatment: Medical
Laser photocoagulation of subretinal neovascular membranes
photodynamic therapy following IV verteporfin Surgical:
translocation of the macula intravitreal vascular endothelial growth factor
inhibitors ranibizumab (Lucentis), bevacizumab (Avastin) repeated intravitreal injection
Primary Open-Angle Glaucoma major cause of preventable blindness
worldwide 2M Americans, half undiagnosed Prevalence
0.1% for aged 40-49 to 3% for over age 70 Effective tx: detection on earlier stage
Ophthalmic Assessment fluorescein angiography
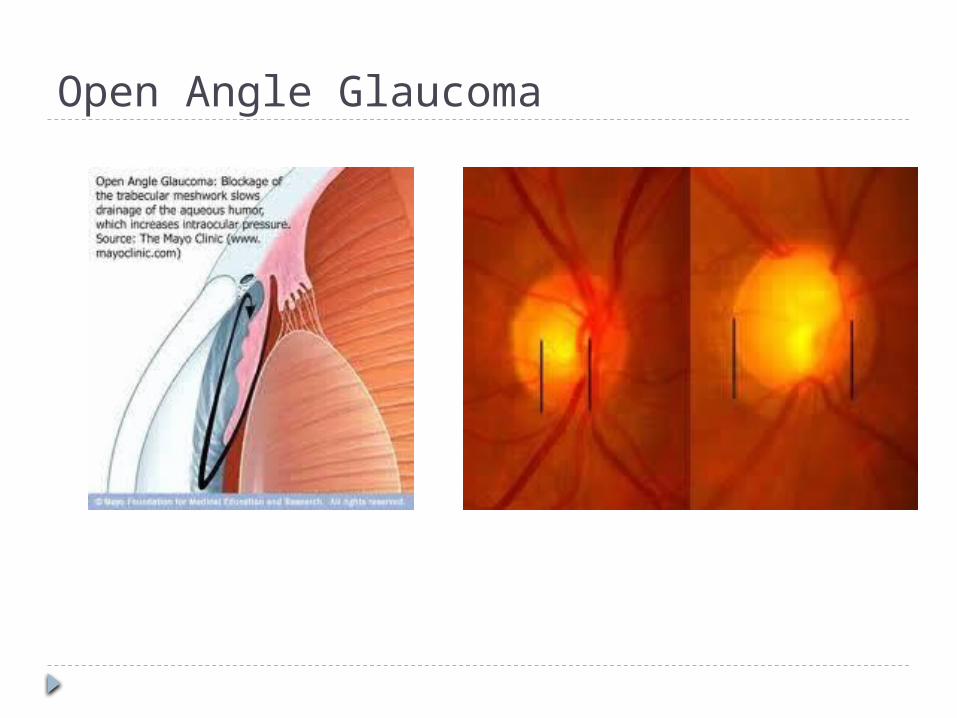
Open Angle Glaucoma
Latest Asia-Pacific Glaucoma Guidelines case detection: conducting a comprehensive
ophthalmologic examination on pt >35 yo seek ophthalmic attention for any reason
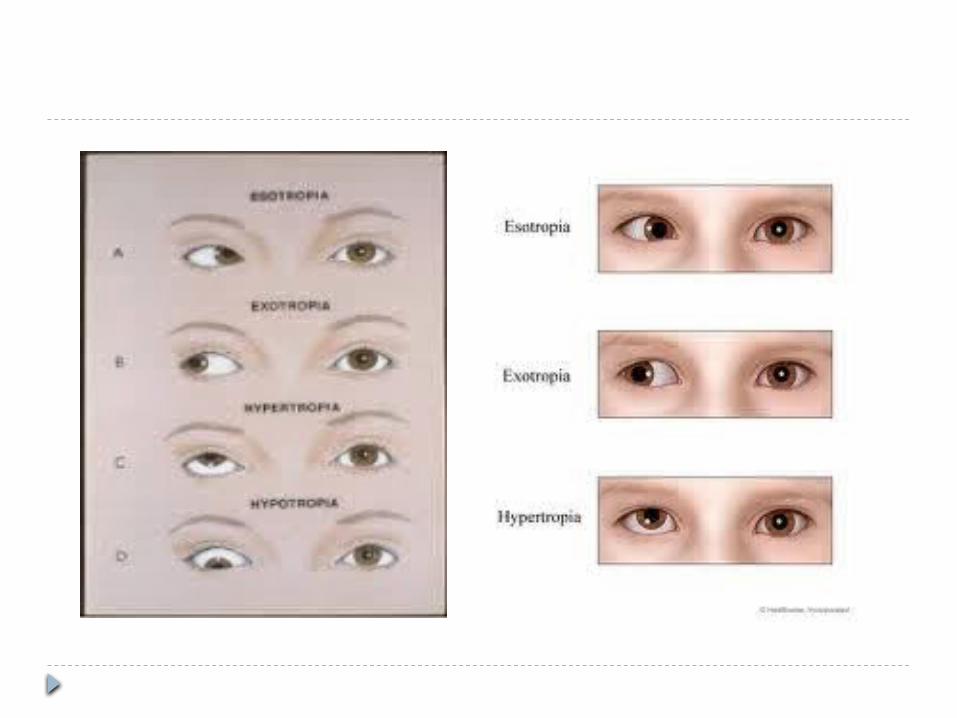
Prevention of Amblyopia "Lazy Eye" diminished visual acuity in one eye in the
absence of organic eye disease Central vision: 0-6 or 7 y/o 2 main abnormalities
Strabismus Anisometropia
Prevention of Amblyopia
Strabismus Esotropia or exotropia double vision unused eye- not developed, unless the good
eye is patched No functional connection with the visual centers of
the brain.
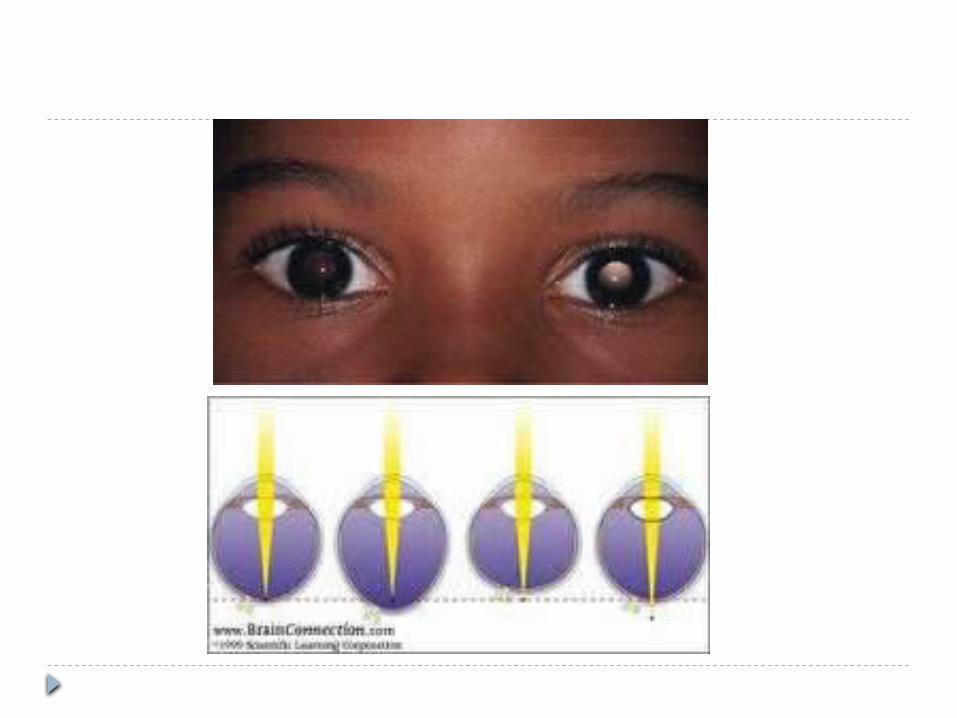
Anisometropia Young children are more concerned with the
perception of near objects than with those at a distance
favors the nearsighted eye monocular blindness due to failure of visual
development in an unused eye incidence of anisometropia is about 0.75-1%
Prevention: Early diagnosis Test VA of all preschool children
occlusion therapy Illiterate "E" chart / "Home Eye Test" Pediatricians: VA test = <4yo Photorefraction
screening for anisometropia, ametropia, astigmatism, and strabismus in preschool children
Prevention of Ocular Damage Due to Systemic Diseases
Prevention of Ocular Damage Due to Systemic Diseases Diabetic retinopathy
diabetics- regular fundal examination Blood sugar control Proper diet
Juvenile rheumatoid arthritis Uveitis
severe loss of vision due to glaucoma, cataract, or band keratopathy has already occurred
Regular ophthalmic screening
• Vitamin A deficiency disease large intramuscular doses of vitamin A followed by
corrective diet
Prevention of Visual Loss due to Drugs

Prevention of Visual Loss Due to Drugs Ophthalmic drugs:
packaged and labelled
color-labelling
Medication history to avoid
duplication and possible overdosage
Atropine and scopolamine: dilate the pupil in iridocyclitis may precipitate acute glaucoma in pt with
narrow anterior chamber angles. prolonged use: conjunctivitis and allergic
eczema of the eyelids. Preservatives in eye drops: allergic reactions,
cicatrizing conjunctivitis (cicatricial pemphigoid)
Topical anesthetics Avoid prescribing or avoid long-term use severe corneal ulceration and scarring

Corticosteroids depress the local defense mechanisms: corneal
infection worsen herpetic keratitis prolonged use: open-angle glaucoma, posterior
subcapsular cataract unwise use of topical corticosteroids: severity of
herpes simplex virus and varicella-zoster virus corneal infections
• Systemic drugs: keratopathy, retrobulbar neuritis, retinopathy, and
Stevens-Johnson syndrome (erythema multiforme) A MUST:
take a careful history of the patient's use of drugs as part of the initial examination.