Embed Size (px)
Citation preview

RED EYEASMPH LEC Group 6
Abad and Imperial
Ophthalmology Clerkship Rotation: TMC

Outline
Pathophysiology Evaluation Common Causes of Red Eye
Subconjunctival Hemorrhage Blepharitis Conjunctivitis Pterygium Phylctenulosis Episcleratis Keratitis Corneal Abrasion Acute Angle Glaucoma Uveitis
Reference

Pathophysiology
Dilatation of blood vessels in the eye conjunctival (superficial)
ciliary (deeper)

Evaluation
Chief complaint: RED EYE HPI Past Ocular History Past Medical History Ocular Exam

Common Causes of Red Eye

Subconjunctival hemorrhage
Causes: Idiopathic, Trauma, Valsalva, Bleeding
disorders, Drugs: Blood-thinners, steroids,
contraceptives, Severe febrile systemic disease: Dengue, typhoid, malaria,
etc.
Usually benign and self- limiting
Usually without pain and discharge; unilateral

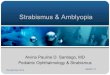
Blepharitis
Condition Clinical Findings Treatment
1) Anterior Blepharitis
Lid margin erythema,
ulceration, fibrin, collarettes (fibrin coating lashes), crusts at base of
lashes, sty (pustules forming at the base of hair
follicles)
Lid hygiene, warm compresses,
bactericidal ointment, anti-staphylococcal
antibiotics
2) Posterior Blepharitis
Chronic burning, foreign body sensation,
conjunctival redness, filmy vision, tearing,
crusting of eyelids
Warm compress, oral tetracycline,
doxycycline or erythromycin, topical
corticosteroids

Anterior Blepharitis

Posterior Blepharitis

Conjunctivitis
inflammation of the conjunctiva dilatation of the superficial conjunctival
blood vessels hyperemia and edema with discharge

Clinical Findings
and Cytology
Viral Bacterial Chlamydial
Allergic
Itching Minimal Minimal Minimal Severe
Hyperemia Generalized Generalized Generalized Generalized
Tearing Profuse Moderate Moderate Moderate
Exudation Minimal Profuse Profuse Minimal
In- stained scrapings
and exudates
Monocytes Bacteria, PMNs
PMNs, plasma cells,
inclusion bodies
Eosinophils
Associated sore
throat and fever
Occasional Occasionally
Never Never
Common Types of Conjunctivitis

Adenoviral Conjunctivitis
Usually self- limiting
The common sore eye

Epidemic keratoconjunctivitis
Treatment: artificial tears, cold compress, topical corticosteroids
(controversial)
Common sequelae of adenoviral conjunctivitis.
Serotypes 8, 11, 19 most common

Gonococcal keratoconjunctivitisNeisseria gonorrhoeae: Hyper-acute, purulent conjunctivitis
Rapid progression, copious purulent
discharge, chemosis, lid edema
Systemic IV/IM ceftriaxone (Cephalosporin)
Topical antibiotics

Chlamydial (Inclusion) keratoconjunctivitis
Chlamydia oculogenitalis
Most common form of neonatal conjunctivitis
and adult STD conjunctivitis
Treatment: Oral doxycycline, topical erythromycin

Allergic conjunctivitis
Hallmark: Itching!
Type I hypersensitivity reaction (IgE-mediated)
Treatment: Topical antihistamines, mast cell stabilizers and
avoidance of allergen

Vernal conjunctivitisCommon profile: Male, brown skin, under
20, lives at equatorial region.
accumulation of eosinophil
Treatment: Topical antihistamines, mast cell stabilizers, corticosteroids
FOR SHORT TERM; self-limiting
On palpebral conjunctiva, especially upper
conjunctiva; Diffuse papillary hypertrophy:
Giant (cobblestone) papillae

Giant Papillary Conjunctivitis
Usually occurs in soft contact lens wearers: Contact lens material, solution, debris
Treatment: Discontinuation of contact lens, topical
antihistamine, mast cell stabilizers, shift to disposable
lenses.

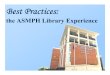
Pterygium
Benign fibrovascular proliferation covered by conjunctival-like epithelium extending into peripheral cornea
Location: Within or Above Bowman’s Line
Treatment: Surgery, Excision with ancillary procedure
The redness is confined largely to a raised, yellowish, fleshy lesion that is usually located on the nasal side of the bulbar conjunctiva

Phylctenulosis
Focal, translucent lymphocytic nodules generally located at limbus
Cause: Delayed Cell-Mediated Hypersensitivity (IV)
Symptoms: tearing, ocular irritation, mild to severe photophobia and a history of similar episodes
Treatment: Improve Eyelid Hygiene,Topical Corticosteroids

Episcleritis
Inflammatory condition affecting the episcleral tissue
Symptoms: Rapid onset of redness, dull ache, and tenderness on palpation
Simple: intermittent bouts of moderate-to-severe inflammation that often recur at 1- to 3-month intervalsNodular: prolonged attacks of inflammation that are typically more painful than simple episcleritis
Treatment: Topical Vasoconstrictors, Mild Corticosteroids

Bacterial Keratitis
Inflammation of the cornea due to infection
Symptoms Pain and foreign body
sensation due to mechanical effects of lids
Watering from the eye due to reflex hyperlacrimation
Photophobia from stimulation of nerve endings
Blurred vision from corneal haze
Redness of eyes due to congestion of circumcorneal vessels

Bacterial KeratitisStreptococcus pneumoniae
Serpiginous, gray-white stromal infiltrate and hypopyon characteristic of Gram-positive bacteria
Suppuration does not usually extend over entire corneal surface
Very painful!
Treatment: Topical erythromycin, chloramphenicol, 4th generation fluoroquinolones (moxiflocxcin, gatifloxacin), Oral cephalosporin, erythromycin, Cypoplegics

Bacterial KeratitisPseudomonas aeruginosa
Typical Gram-negative corneal ulcer: Rapid evolution, marked tendency to spread.
Can perforate in 48 hours.
Common in immunocompromised patients, contact lens wearers with faulty hygiene
Treatment: Topical tobramycin, ciprofloxacin, moxifloxacin, gatifloxacin

Fungal Keratitis
Intense suppuration, progressive hypopyon
Modes of infection:
Injury by vegetative material such as crop, leaf, branch of tree, straw, hay or decaying vegetable matter. Common sufferers are field workers especially during harvest season
Therapeutic problem: No effective topical agent
Debridement: Scrape it off and reduce load of organism or perform keratectomy.
Candida: Natamycin; ketoconazole, voriconazole, amphotericin B

Fungal Keratitis
Yeast Fungi Filamentous Fungi

Herpes simplex keratitis
Mode of infection:HSV1 - Through kissing or coming in close contact with patient suffering from herpes labialis.HSV2 - Transmitted to eyes of neonates through infected genitalia of the mother.
Coalesces in a few days into branching or dendritic lesion
Treatment: Self limited but recurrent.Topical/systemic acyclovir, ganciclovir, debridement
Symptoms: Injection, Irritation, Mucoid discharge, Pain, Mild photophobia

Corneal abrasion
Follows Occular Trauma
May be superficial or deep
Symptoms: Acute pain after ocular traumaPhotophobia, excessive tearing,blepharospasm, foreign body sensation,blurred vision
Treatment: Patching, Topical Antibiotics, Cycloplegics

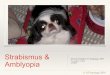
Acute Angle Closure Glaucoma

Acute Angle Closure Glaucoma
ocular pain, headache unilateral blurring of
vision "iridescent" vision: haloes
around lights nausea and vomiting
Elevated intraocular pressure (>40 mmHg)
deep circumlimbal conjunctival and episcleral injection: "ciliary flush"
fixed, mid-dilated pupil edematous or steamy
cornea shallow anterior
chamber
Symptoms Signs

Acute Angle Closure Glaucoma Treatment: Lower IOP
Carbonic anhydrase inhibitors Hyperosmotic agents Pilocarpine Supportive: steroids and analgesics
Laser Iridotomy

Acute anterior uveitis
Uveitis: Inflammation of one or all parts of the uveal tract
Hallmark: Cells and Flare
Symptoms• Deep, dull pain ofinvolved eye and surrounding orbit• Photophobia• Tearing• Difficulty in reading
Signs• Ciliary flush• Sterile hypopyon (severe)• Cells and flares• Keratic precipitates• Posterior synechiae• Granulomatous nodules

Acute anterior uveitis
Keratic precipitates Posterior synechiae
Granulomatous nodules
Koeppe (pupil) Brusacca

Acute anterior uveitis
Ankylosing spondylitis Bechet’s disease Chronic granulomatous
disease Enthisitis Inflammatory bowel disease Kawasaki’s disease Multiple sclerosis Polyarteritis nodosa Psoriatic arthritis SLE Vogt-Koyanagi-Harada
syndrome
Brucellosis Herpes simplex Herpes zoster Leptospirosis Lyme disease Syphilis Toxoplasmosis Tuberculosis
Systemic causes Infectious causes

Acute anterior uveitis
Treatment Immobilize iris, ciliary body to relieve pain
(ie. atropine, cyclopentolate) Reduce inflammation (ie. topical steroids) Treat underlying ocular, systemic disease


References
Vaughan & Asbury’s General Ophthalmology 17th ed.
ASMPH Ophthalmology Lecture Notes on “Common Causes of Red Eye” by Dr. Victor L. Caparas. January 2010.
The Red Eye. The New England Journal of Medicine. Volume 343 Number 5. December 2007.

Thank You =)