-
7/28/2019 Pleno.scenario 3 urogenital
1/40
PLENARY DISCUSSION
ASIHS PATIENT
GROUP 2
ANATHARAO A/L SUBRAMANIAM
DIAN PRATIWI BURNAMA FAJAR SATRIA PRATAMA
KHALIDAH
KEVIN MAULANDA
MEIVITA WULANDARI
SONYA VIESKA TIARA RAHMA ZAIN
VEGGY PRATAMA ANANDA PUTRA
WIDYATUL AINA
-
7/28/2019 Pleno.scenario 3 urogenital
2/40
Scenario 3 ;Asihs Patient
Asih is a medical school student who are undergoing their
clinical pediatrics section. One day, he gets a patient, a
boy
aged 5 years who were admitted to hospital because of a
loss of consciousness. Typical symptoms in children are
kussmaul respiratory and growth retardation. Blood gas
analysis showed a significant decrease in the levels of
bicarbonate and anion gap within normal limits. laboratory
results of urine showed the pH of the urines is alkaline.
Doctors suspect the child is suffering kidney disease. basedon
this, Asih try to analyze what happened to the child.
How do you explain what happened to the child?
-
7/28/2019 Pleno.scenario 3 urogenital
3/40
Learning objective1. Regulation of acid-base balance
2. Factors affecting the acid-base balance as well as water
and electrolyte
3. Buffer mechanism in maintaining acid-base balance
4. Regulation of fluid-electrolyte
5. Acid-base balance disorders as well as water
andelectrolytes
-
7/28/2019 Pleno.scenario 3 urogenital
4/40
1. BODY REGULATION OF ACID-BASE BALANCE
Refers to precise regulation of free H+ concentration in
bodyfluids
Acids
Group of H+ containing substances that dissociate in
solution to release free H
+
and anions(H2CO3)Bases
Substance that can combine with free H+ and remove it
fromsolution(HCO3)
pH
Designation used to express the concentration of H+ pH 7
neutral
pH less than 7 acidic
pH greater than 7 basic
-
7/28/2019 Pleno.scenario 3 urogenital
5/40
BUFFER SYSTEM
The fastest performer, works in seconds
Bicarbonate ions combine with excess hydrogenions to form
carbonic acid in a dynamic
relationship HCO3 + H+ H2CO3
For every molecule of carbonic acid, there are 20molecules of
bicarbonate
Any change in the this 20:1 ratio is immediatelycorrected to
maintain pH
An increase H+ causes an increase in H2CO3
A decrease in H+ causes a decrease in H2CO3
-
7/28/2019 Pleno.scenario 3 urogenital
6/40
BUFFER SYSTEM
Carbonic acid is a weak, volatile acid which must be eliminated
The enzyme carbonic anhydrase causes the carbonic acid to
convert to carbon dioxide and water
The CO2 and the H2O are easily eliminated by the lungs
andkidneys
Buffers system in the bodyBicarbonate: most important ECF
buffer
Phosphate: important ICF and renal tubular buffer
HPO4-- + H+ H2PO4
-
Ammonia: important renal tubular bufferNH3 + H
+ NH4+
Proteins: important ICF and ECF buffers
Largest buffer store in the body
Albumins and globulins, such as Hb
-
7/28/2019 Pleno.scenario 3 urogenital
7/40
-
7/28/2019 Pleno.scenario 3 urogenital
8/40
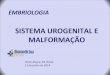
The respiratory system can activate changes in pHwithin 1 to 3
minutes and can eliminate or conserve Co2. As
discussed, when a strong acid is present in the body,
thebicarbonate, carbonic acid buffer pair is activated to buffer
theacid. This results in a net increase of carbonic acid,
whichdissociates into Co2 and H2O. Carbon dioxide is theneliminated
by the lungs. An increase in H+ concentration inthe blood
stimulates the breathing center in the medulla to
increase the respiratory rate, which facilitates CO2elimination.
If, on the other hand, pH is elevated secondary toan increase in
HCO3-, the respiratory center is inhibited, andthe respiratory rate
decreases.
This results in CO2 retention, which then becomesavailable to
form carbonic acid, which buffers the excess
bicarbonate. The respiratory system is thus able tocompensate
for changes in pH related to metabolic disordersby regulating Pc02,
which alters the bicarbonatecarbonic acidratio. The respiratory
system cannot, however, produce anyloss or gain of hydrogen ions.
Respiratory compensation isactivated within minutes and is usually
fully functional within I
to 2 days.
Respiratory System
-
7/28/2019 Pleno.scenario 3 urogenital
9/40
9
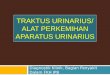
RENAL SYSTEM
Can take hours to days to workKidneys can retain bicarbonate
ion, causing
a decrease in H+ and an increase in pH
Kidneys can excrete bicarbonate ion,
causing an increase in H+ and a decreasein pH
-
7/28/2019 Pleno.scenario 3 urogenital
10/40
Renal compensation is a slower process, requiring Ito 2 days for
complete activation. The kidneys react tochanges in pH by
regulating the excretion orconservation of HC03-
A low pH stimulates excretion of H+ into the urine.
As H+ enters the urine, it displaces another positive
ion,usually Na+. At the same time, HC03- is reabsorbed inexchange
for the H+. The Na+ is then reabsorbed intothe tubule cell, where
it combines with HC03- to formNaHC03 which is then available to
buffer other H+ in theblood. The rale of H+ excretion, and
therefore the rate ofHC03- reabsorption, is proportionate to
arterial Pc02.This reaction is reversed for increases in pH.
Renal System
-
7/28/2019 Pleno.scenario 3 urogenital
11/40
The transport of H+ in the renal tubules is facilitated by
thebuffer's phosphate and ammonia, which is classified as a
base.
Most ammonia is converted to urea by the liver and is
eliminatedfrom the body in urine. The remaining ammonia combines
with H+to form the ammonium ion (NH4+) in the renal tubules. NH4+
alsodisplaces Na+ and is eliminated in the urine. The Na+ is
thenreabsorbed into the tubule cells, where it combines with HC03-
toform NaHC03, which is absorbed into the blood to buffer
excessH+.
The amount of H+ excreted in the urine can be measuredby
determining the amount of alkali required to neutralize theurine
and is called titratable acidity. As a result of H+ and
NH4+excretion, urine usually has an acidic pH of 6. In the
clinicalsetting, checking urine pH can be a useful indicator of
the
degree of renal compensation when assessing acid-basestatus. For
example, a low or acidic blood pH will beaccompanied a few days
later by a low or acidic urine pH whenrenal compensatory mechanisms
are active. The reverse is truein alkalotic states.
-
7/28/2019 Pleno.scenario 3 urogenital
12/40
2. FACTORS THAT AFFECT THEEQUILIBRIUM LIQUID ELECTROLYTE
AND ACID BASE
1.age
fluid composition in adult women in about 50% of the body
weight
fluid composition in adult men 60% of body weight
on children's body fluid composition 75% of body weight
in the elderly komposis 40-50% of body fluid loss dsri Berst2.
Climate
the colder the climate, the less caitan that ekskresikan by the
body,and vice versa.
-
7/28/2019 Pleno.scenario 3 urogenital
13/40
3.diet
diet affect fluid and electrolyte intake, when nutrient intake
is not strong,
the body will burn fat prtotein and, thus serum albumin and
protein
reserves will decline.
4.stress
stress will lead to increased cell metabolism, thereby
increasing the
levels of sodium and water retention in the body
5. ill
sunburnthis will lead to a lot of liquid which is excreted in
the body surface.
cardiovascular-renal disease
-
7/28/2019 Pleno.scenario 3 urogenital
14/40
FACTORS THAT AFFECT ACID-BASE BALANCE
1. Hydrogen ion concentration in the body
2.konsentrasi bicarbonate ions in the body3.Partial pressure
carbon dioxide in the body
-
7/28/2019 Pleno.scenario 3 urogenital
15/40
1. Bicarbonate Buffer SystemConsist of a weak acid H2CO3 and
bicarbonate salt NaHCO3.
When a strong acid such as HCl is added to a solution of
bicarbonate buffer, an increase in H ions released by the HCl
will
be supported by HCO3.
H + HCO3 H2CO3 CO2 + H2O
When strong bases such as NaOH is added to a solution of
bicarbonate buffer, ion OH from NaOH joined H2CO3 to form
HCO3 extra.
NaOH + H2CO3 NaHCO3 + H2O
3. Buffer System on Acid-Base Balance
-
7/28/2019 Pleno.scenario 3 urogenital
16/40
Henderson-Hasselbalch equation
Increasing the concentration of bicarbonate ions causes the pH
to
rise, shifting the acid-base balance toward alkalosis.Increasing
the concentration of H2CO3 cause decreased pH, acid-
base balance shifts toward acidosis.
pH= pKa + log [HCO3] / [H2CO3]
-
7/28/2019 Pleno.scenario 3 urogenital
17/40
2. Phosphate buffer system
Plays an important role in supporting the renal tubular fluid
andintracellular fluid. The main elements of phosphate buffer
system is
H2PO4 and HPO4.
When a strong acid such as HCl is added to the phosphate
buffersolution, hydrogen accepted by HPO4 converted to H2PO4.
When strong bases such as NaOH is added to the phosphate
buffer system, OH supported by H2PO4 to form a number of
additions HPO4 + H2O
HCl + Na2HPO4 NaH2PO4 + NaCl
NaOH + NaH2PO4 Na2HPO4 + H2O
-
7/28/2019 Pleno.scenario 3 urogenital
18/40
3. Protein
Is an important intracellular buffer.
Diffusion elements of bicarbonate buffer system causing pH
in
intracellular fluid change when there is a change of
extracellularfluid pH.
60-70% of total chemical buffering fluid inside the cells
and
mostly produced by the intracellular protein.
The slow movement of hydrogen ions and bicarbonate ions
through the cell membrane often slow intracellular protein
maximum capacity up to several hours to buffer acid-base
disturbances.
4. The Ammonia Buffer System
This ammonia buffer system occurs in 3 steps:1) synthesis
ofNH4
+ from glutamine, an amino acid in the proximal tubule,
thick ascending loop of Henle & distal tubules
2) recycling & reabsorption ofNH3 in the kidneys medulla,
&
3) buffering of H+ ions by NH3 in the collecting tubules
http://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://medical-dictionary.thefreedictionary.com/proximal+tubulehttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://medical-dictionary.thefreedictionary.com/proximal+tubulehttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppthttp://localhost/var/www/apps/conversion/tmp/scratch_2/Acid%20Base%20Tutorial.ppt
-
7/28/2019 Pleno.scenario 3 urogenital
19/40
4. Fluid Electrolyte Balance
Distribution of Body FluidsIntracellular = inside the cell; 42%
of body weight
Extracellular = outside the cell, 17% of body weight
Interstitial = contains lymph; fluid between cells and outside
blood
vessels
Intravascular = blood plasma found inside blood vessels
Transcellular = fluid that is separated by cellular barrier,
Body fluids contain ElectrolytesAnions negative charge
Cl, HCO3, SO4
Cations positive charge
Na, K, Ca Electrolytes are measured in mEq
Minerals are ingested as compounds and are constituents ofall
body tissues and fluids
Minerals act as catalysts
-
7/28/2019 Pleno.scenario 3 urogenital
20/40
Electrolytes in Body Fluids
Normal Values Sodium (Na+) 35 145 mEq/L
Potassium (K+) 3.5 5.0 mEq/L
Ionized Calcium (Ca++) 4.5 5.5 mg/dL
Calcium (Ca++) 8.5 10.5 mg/dL
Bicarbonate (HCO3) 24 30 mEq/L
Chloride (Cl--) 95 105 mEq/L
Magnesium (Mg++) 1.5 2.5 mEq/L
Phosphate (PO4---
) 2.8 4.5 mg/dL
-
7/28/2019 Pleno.scenario 3 urogenital
21/40
Regulation of Body Fluids
Homeostasis is maintained through Fluid intake Hormonal
regulation
Fluid output regulation
-
7/28/2019 Pleno.scenario 3 urogenital
22/40
Fluid Intake Thirst control center located in the
hypothalamus
Osmoreceptors monitor the serum osmotic pressureWhen osmolarity
increases (blood becomes more
concentrated), the hypothalamus is stimulated resulting inthirst
sensation Salt increases serum osmolarity
Hypovolemia occurs when excess fluid is lostAverage adult intake
2200 2700 mL per day Oral intake accounts for 1100 1400 mL per
day
Solid foods about 800 1000 mL per day
Oxidative metabolism 300 mL per day
Those unable to respond to the thirst mechanism areat risk for
dehydration Infants, patients with neuro or psych problems, and
older
adults
-
7/28/2019 Pleno.scenario 3 urogenital
23/40
Hormonal Regulation
ADH (Antidiuretic hormone)Stored in the posterior pituitary and
released in response to
serum osmolarity
Pain, stress, circulating blood volume effect the release ofADH
Increase in ADH = Decrease in urine output = Body saves water
Makes renal tubules and ducts more permeable to water
Renin-angiotensin-aldosterone mechanismChanges in renal
perfusion initiates this mechanismRenin responds to decrease in
renal perfusion secondary to
decrease in extracellular volumeRenin acts to produce
angiotensin I which converts to
angiotensin II which causes vasoconstriction, increasingrenal
perfusionAngiotensin II stimulates the release of aldosterone
when
sodium concentration is low
-
7/28/2019 Pleno.scenario 3 urogenital
24/40
Hormonal Regulation
AldosteroneReleased in response to increased plasma potassium
levels
or as part of the renin-angiotensin-aldosterone mechanism
tocounteract hypovolemia
Acts on the distal portion of the renal tubules to increase
the
reabsorption of sodium and the secretion and excretion
ofpotassium and hydrogen
Water is retained because sodium is retained
Volume regulator resulting in restoration of blood volume
Atrial Natriuretic Peptide (ANP) ANP is a hormone secreted from
atrial cells of the heart in response to atrial
stretching and an increase in circulating blood volume
ANP acts like a diuretic that causes sodium loss and inhibits
the thirstmechanism
Monitored in CHF
-
7/28/2019 Pleno.scenario 3 urogenital
25/40
Fluid Output Regulation
Organs of water loss Kidneys Lungs
Skin
GI tract
-
7/28/2019 Pleno.scenario 3 urogenital
26/40
Fluid Output RegulationKidneys are major regulatory organ of
fluid balance Receive about 180 liters of plasma to filter
daily
1200 1500 mL of urine produced daily
Urine volume changes related to variation in the amount and
typeof fluid ingested
Skin Insensible Water Loss
Continuous and occurs through the skin and lungs
Can significantly increase with fever or burns
Sensible Water Loss occurs through excess perspiration
Can be sensible or insensible via diffusion or perspiration
500 600 mL of insensible and sensible fluid lost through
skineach day
-
7/28/2019 Pleno.scenario 3 urogenital
27/40
Fluid Output RegulationLungs
Expire approx 500 mL of water daily
Insensible water loss increases in response to changes in
resp rate and depth and oxygen administration
GI Tract
3 6 liters of isotonic fluid moves into the GI tract and
thenreturns to the ECF
200 mL of fluid is lost in the feces each day Diarrhea can
increase this loss significantly
-
7/28/2019 Pleno.scenario 3 urogenital
28/40
Regulation of Electrolytes Major Cations in body fluids
Sodium (Na+)
Potassium (K+)
Calcium (Ca++)
Magnesium (Mg++)
-
7/28/2019 Pleno.scenario 3 urogenital
29/40
Sodium RegulationMost abundant cation in the extracellular
fluid
Major contributor to maintaining water balance Nerve
transmission Regulation of acid-base balance
Contributes to cellular chemical reactions
Sodium is taken in via food and balance is
maintained through aldosterone
-
7/28/2019 Pleno.scenario 3 urogenital
30/40
Potassium Regulation
Major electrolyte and principle cation in the
extracellular fluid
Regulates metabolic activities
Required for glycogen deposits in the liver andskeletal
muscle
Required for transmission of nerve impulses, normal
cardiac conduction and normal smooth and skeletal
muscle contractionRegulated by dietary intake and renal
excretion
-
7/28/2019 Pleno.scenario 3 urogenital
31/40
Calcium Regulation Stored in the bone, plasma and body cells
99% of calcium is in the bones and teeth
1% is in ECF
50% of calcium in the ECF is bound to protein (albumin) 40% is
free ionized calcium
Is necessary for Bone and teeth formation
Blood clotting
Hormone secretion
Cell membrane integrity
Cardiac conduction
Transmission of nerve impulses
Muscle contraction
-
7/28/2019 Pleno.scenario 3 urogenital
32/40
Magnesium RegulationEssential for enzyme activities
Neurochemical activities
Cardiac and skeletal muscle excitability
RegulationDietary
Renal mechanisms
Parathyroid hormone action
50 60% of magnesium contained in bones 1% in ECF
Minimal amount in cell
-
7/28/2019 Pleno.scenario 3 urogenital
33/40
-
7/28/2019 Pleno.scenario 3 urogenital
34/40
5. Acid-base balance disorders as well as water
and electrolytes
Acid-Base Imbalance
-
7/28/2019 Pleno.scenario 3 urogenital
35/40
PaCO2 & pHA primary disorder where the first change is an
elevation ofPaCO2,resulting in decreased pH.
Compensation (bringing pH back up toward normal) is a
secondary
retention ofHCO3 by the kidneys; this elevation of HCO3- is
notmetabolic alkalosis since it is not a primary process.
Primary Event Compensatory Event
HCO3- HCO3- pH ~ --------- pH ~ ---------
PaCO2 PaCO2
RESPIRATORY ACIDOSIS
-
7/28/2019 Pleno.scenario 3 urogenital
36/40
A primary acid-base disorder where the first change isa lowering
ofHCO3-, resulting in decreased pH.
Compensation (bringing pH back up toward normal) isa secondary
hyperventilation; this lowering ofPaCO2,
Renal excretion of hydrogen ions & K+ exchangesPrimary Event
Compensatory Event
HCO3- HCO3-
pH ~ ------------ pH ~ ------------PaCO2 PaCO2
Metabolic acidosis
-
7/28/2019 Pleno.scenario 3 urogenital
37/40
Metabolic Alkalosis
A primary acid-base disorder where the first change is
anelevation ofHCO3-, resulting in increased pH.
Compensation is a secondary hypoventilation (increasedPaCO2),
Compensation for metabolic alkalosis is less predictablethan for
the other three acid-base disorders.
Primary Event Compensatory Event
HCO3- HCO3- pH ~ ------------ pH ~ ---------
PaCO2 PaCO2
-
7/28/2019 Pleno.scenario 3 urogenital
38/40
Respiratory Alkalosis
A primary disorder where the first change is a lowering ofPaCO2,
resulting in an elevated pH.
Compensation is a secondary lowering(excreting)HCO3 by
the kidneys.
Primary Event Compensatory Event
HCO3- HCO3- pH ~ ------- pH ~ --------
PaCO2 PaCO2
-
7/28/2019 Pleno.scenario 3 urogenital
39/40
Water Electrolyte Disorders
Hipovolemia is a diminution of the circulating volume of
Blooddue to multiple factors like Hemorrhage, dehydration,
burns,
among others.
Dehydrationis the loss of water and salts essential for normal
bodyfunction. Dehydration occurs when the body loses more fluid
than
it takes in.
Hyponatremiais a medical term which refers to a dangerously
lowlevel of sodium in the body.
-
7/28/2019 Pleno.scenario 3 urogenital
40/40
Edemais swelling that is caused by fluid trapped inyour bodys
tissues. Edema happens most often in the
feet, ankles, and legs, but can affect other parts of the
body, such as the face, hands, and abdomen. It can
also involve the entire body.
Hyperkalemia is defined as a condition in which the
serum potassium level is greater than 5.3 mEq/L. Any
of 3 pathogenetic mechanisms can cause
hyperkalemia: excessive intake, decreased excretion,
d hif f i ll l ll l
Water Electrolyte Disorders