Embed Size (px)
Citation preview

Planetary Confusion: Where is Captain Kirk when we need him?
Edmonton May 7th 2011 Building Partnerships With Women, their
Families and Care Providers based on what providers and women believe about childbirth
How can evidence shape a new relationship?
Michael C. KleinEmeritus Professor of Family Practice UBC and
Child and Family Research Institute

Maternity Care Attitudes & Beliefs Study
Funded By:
Four-YearNational
Study
In Association With:
Supported by:
•College Family Physicians of Canada (CFPC)•Society of Obstetricians and Gynaecologists of Canada • Association of Obstetricians and Gynecologists of Quebec (AOGQ)•The Canadian Association of Midwives (CAM)•Association des omnipraticiens en périnatalité du Québec (AOPQ) --Various Provincial & National Nurses Associations
--DONA International

Maternity Care Research GroupMichael C. Klein, MD, CCFP, FAAP (Neonatal/Perinatal), FCFP, ABFP,
Principal Investigator, UBCJanusz Kaczorowski, PhD, Co-Principal Investigator –
Medical Sociology, UBCWilliam Donald Fraser, MD, MA, FRCSC, Co-Principal Investigator -
Obstetrics, University of MontrealRobert Liston, MB ChB, FRCSC, FRCOG, FACOG,
Co-Investigator – Obstetrics, UBCSharon Dore, RN, PhD, Co-Investigator – Nursing, McMasterWendy Hall, RN, PhD, Co-Investigator – Nursing, UBCPatricia McNiven, RM, PhD, Co-Investigator – Midwifery, McMasterLee Saxell, RM, MA, Co-Investigator – Midwifery, UBCKathleen A. Lindstrom, CD, Doula Educator, Co-Investigator - Doula,
Douglas CollegeJalana Grant, CD, Co-Investigator – Doula, DONA Western Canada
Director Rollin Brant, PhD,Co-Investigator – Statistics, UBCSahba Eftekhary MD, MPH, MHA, Co-InvestigatorJude Kornelsen,PhD, Co-Investigator - Medical Sociologist, UBCJocelyn Tomkinson, MPH, Project Manager Jessica Rosinski MA,Research AssistantAndrea Procyk, BA, Research AssistantNazli Baradaran, MD, Research AssistantOralia Gómez-Ramírez MA, Research AssistantAoife Chamberlaine, BA, Research Assistant
Gestation Self-Portrait © Rae Maté, 1988
www.maternitycare.ca

National Study Background:
•Differences in beliefs and attitudes toward birth among different maternity care providers doing similar work can be a source of conflict and confusion in the workplace
•And can create inter-professional difficulties and problems for pregnant and laboring women to build partnerships with their provider.
•As well as creating confusion for undergraduate and postgraduate trainees

The Ground is Shifting
• The profession of OB/GYN is changing—aging and feminizing
• Demographics of the other maternity care providers are changing
• Demographics of the childbearing population are changing—older, heavier etc
• Birth technology is changing, ?? improving • EBM approach is changing—more EBM in maternity
care• Hence, every reason to expect changes in attitudes of
providers and women in the new generation of each

• 553 Obstetricians• 894 Family Physicians
• 495 Provide Intrapartum Care• 399 Provide Antepartum Care Only
• 381 Midwives• 541 Nurses• 130 Doulas• 1350 Nulliparous Women
2499 Maternity Care Providers Across Canada Responded Both Languages
The responses for each group represented every region in Canada, Rural and Urban and paralleled actual distribution providers, with the exception of some weakness in Quebec for nurses, midwives, doulas and women
Midwifery and Home Birth

Post-Term Pregnancy Beliefs

In-Depth Study of Obstetricians
This generational analysis encapsulates many of these changes and was most revealing and predictive of the future of maternity care
•Areas of Agreement and disagreement between Obstetricians <=40 and >40

Demographics OBs <=40 and >40 age
• Female: 81% younger vs 40% older
• Generation NOT gender
• Regional, Level, and type of practice similar
• Mean deliveries/year: – 169 younger vs 109 older

Some areas of intergenerational agreement
Could consider them core values

20 21.7
70.9
21.717.2
21.3
70.6
22.7
0
10
20
30
40
50
60
70
80
90
100
is safer for the baby than vaginal birth
is as safe as vaginal birth for women
costs more for the health system than
vaginal birth
Women who want C/S in the absence of
medical indication should have to pay
for it
% A
gree
men
tCesarean Section:
40 and Under
Over 40
Some ways to reduce the Cesarean section
rate

25.921.7
27.5
21.3
0
10
20
30
40
50
60
70
80
90
100
Providing more midwifery services Encouraging more family physicians to provide intrapartum maternity care
% A
gree
men
tApproaches to reducing Cesarean Section rate:
40 and Under
Over 40
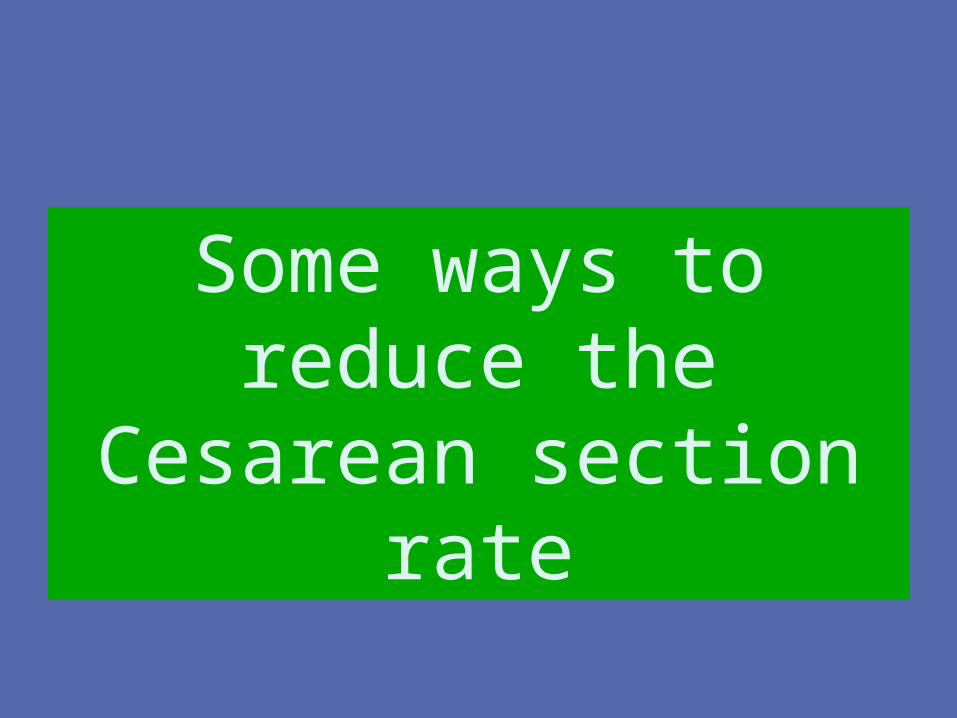
7.5 9.1
44.3
5.4 7.1
49.2
0
10
20
30
40
50
60
70
80
90
100
Because of the unpredictability of vaginal
birth, I would prefer a scheduled C/S for myself or
partner
If my partner or I were pregnant with an apparently normal pregnancy, I would
prefer an elective C/S instead of a vaginal birth
For single term frank breech, women should be
offered the choice of vaginal birth
% A
gree
men
tChoosing Cesarean:
40 and Under
Over 40

70.3 71.5
0
10
20
30
40
50
60
70
80
90
100
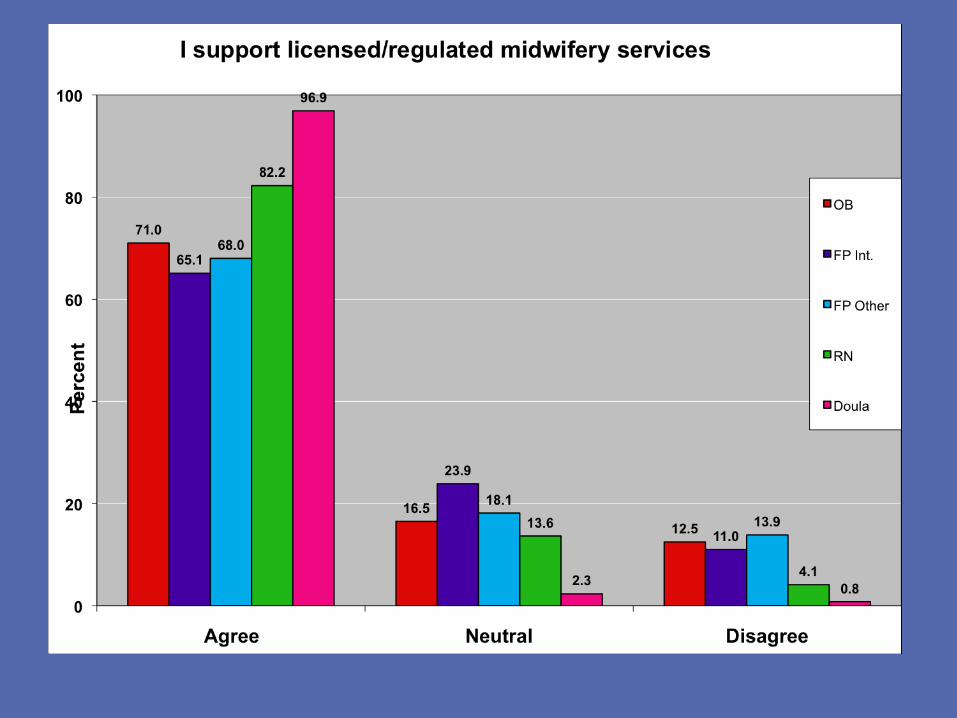
I support licensed/regulated midwifery services
% A
gree
men
tRegulated Midwifery:
40 and Under
Over 40

Positive attitudes toward doulas
Strongly Agree
Neutral
Strongly Disagree

29.5
52.6
28.528.1
60.1
34.9
0
10
20
30
40
50
60
70
80
90
100
There is a need for doula services in maternity care
In my practice, doulas are welcome
Doulas improve birth outcomes
% A
gree
men
tDoulas:
40 and Under
Over 40

In-Depth Study of Obstetricians
Areas of Disagreement between Obstetricians
<=40 and >40
All statistically significant at p <.05 or usually <.01 to <.001
But keep in mind areas or zones of interdisciplinary agreement
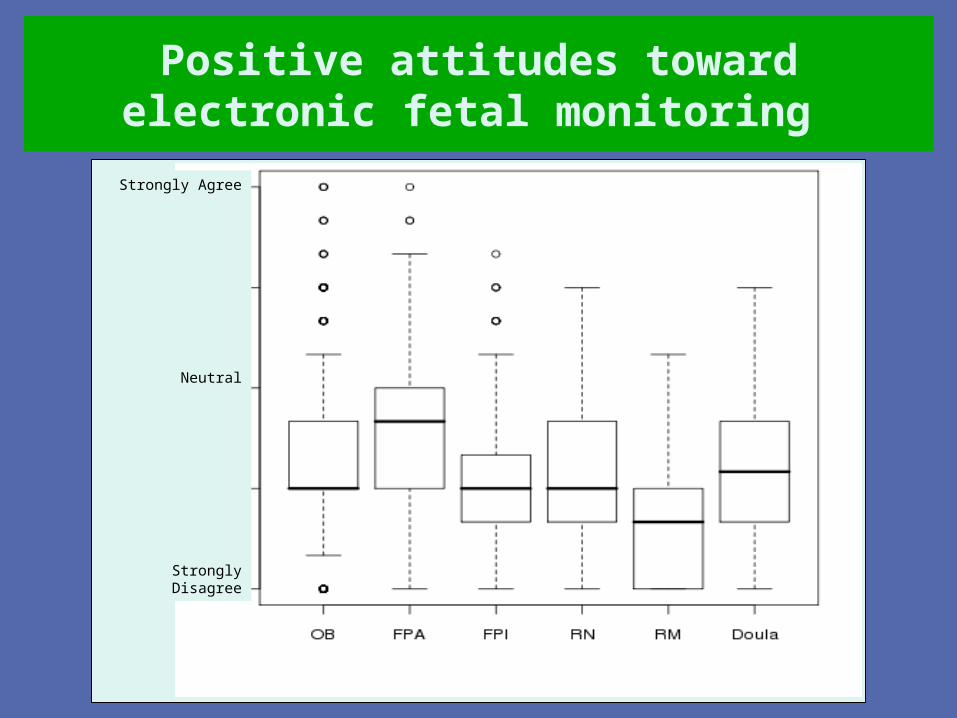
Positive attitudes toward electronic fetal monitoring
Strongly Agree
Neutral
Strongly Disagree
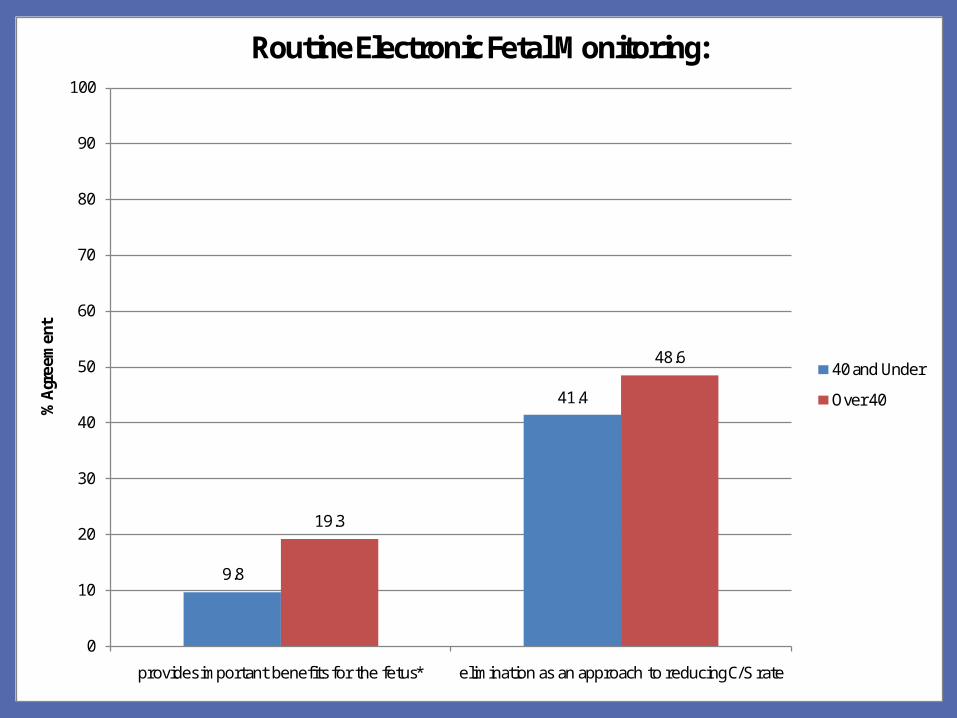
9.8
41.4
19.3
48.6
0
10
20
30
40
50
60
70
80
90
100
provides important benefits for the fetus* elimination as an approach to reducing C/S rate
% A
gree
men
tRoutine Electronic Fetal Monitoring:
40 and Under
Over 40

Positive attitudes regarding epidural analgesia
Strongly Agree
Neutral
Strongly Disagree

21.1
41.0
72.6
31.4
53.7
60.1
0
10
20
30
40
50
60
70
80
90
100
interferes with the normal progress of labour*
increases the incidence of instrumental birth*
should be administered whenever a patient requests
it*
% A
gree
men
tEpidural Analgesia:
40 and Under
Over 40

Positive attitudes regarding routine episiotomy
Strongly Agree
Neutral
Strongly Disagree

0.6
7.4
92.0
6.3
15.6
73.8
0
10
20
30
40
50
60
70
80
90
100
if done routinely, can prevent pelvic floor
relaxation*
should be used for all instrumental vaginal births*
if done routinely, leads to more harm than good*
% A
gree
men
tEpisiotomy:
40 and Under
Over 40


93.7
33.1
86.7
21.3
0
10
20
30
40
50
60
70
80
90
100
Home birth is more dangerous than hospital birth, even in an uncomplicated
pregnancy*
If a woman has had a previous C/S, a scheduled repeat C/S can improve
newborn outcomes*
% A
gree
men
tSafety by place and mode of birth:
40 and Under
Over 40
Woman’s role in her own birth

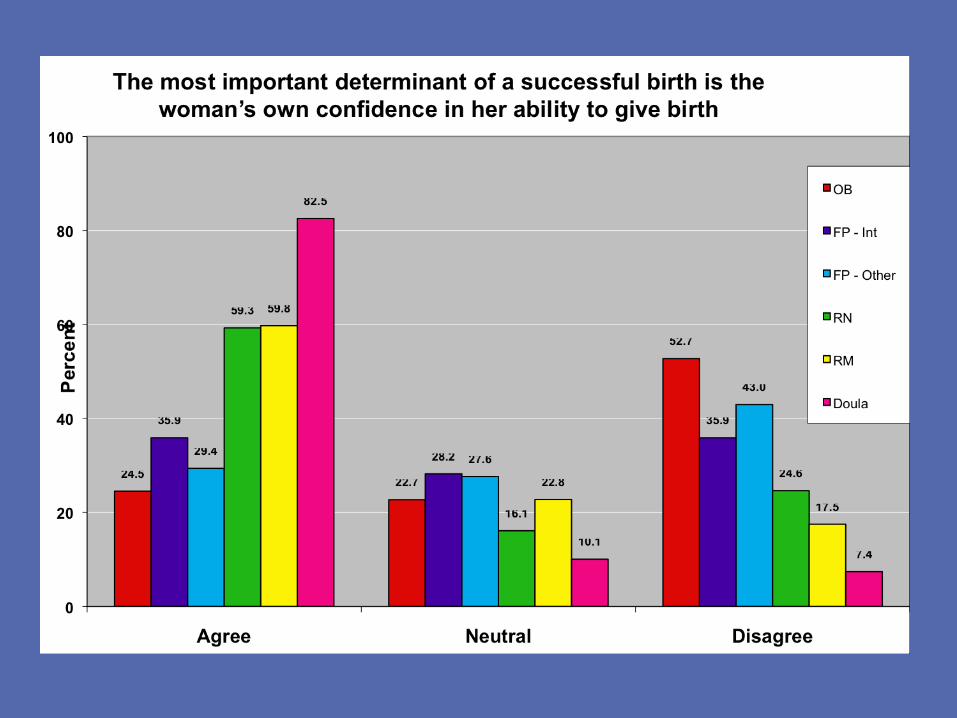
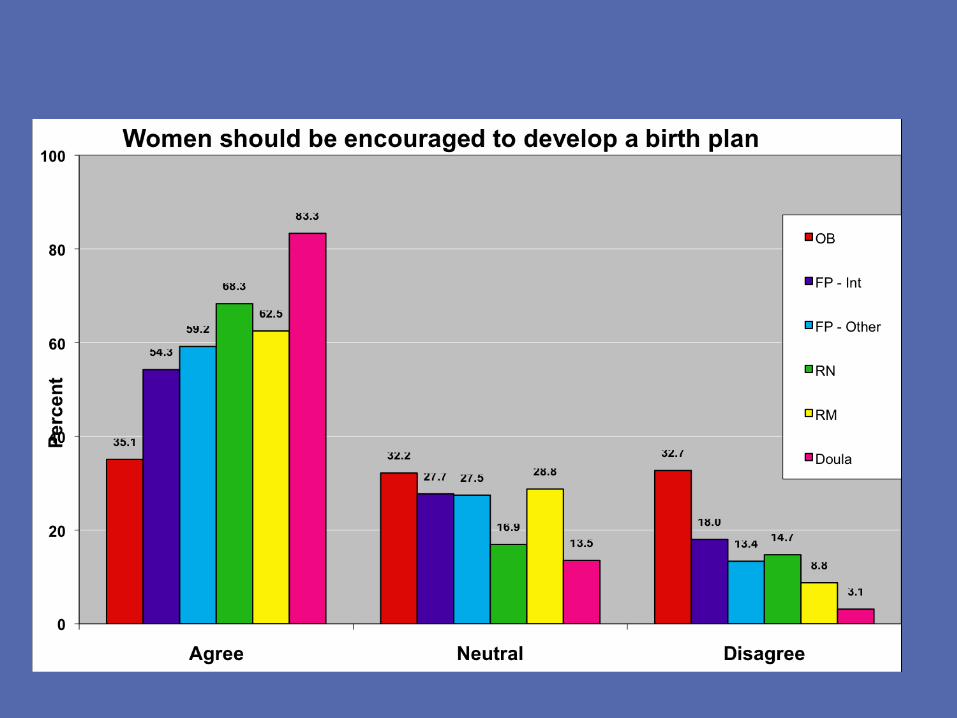
Positive attitudes toward the importance of maternal choices and the role played by the mother in her own
birth Strongly Agree
Neutral
Strongly Disagree

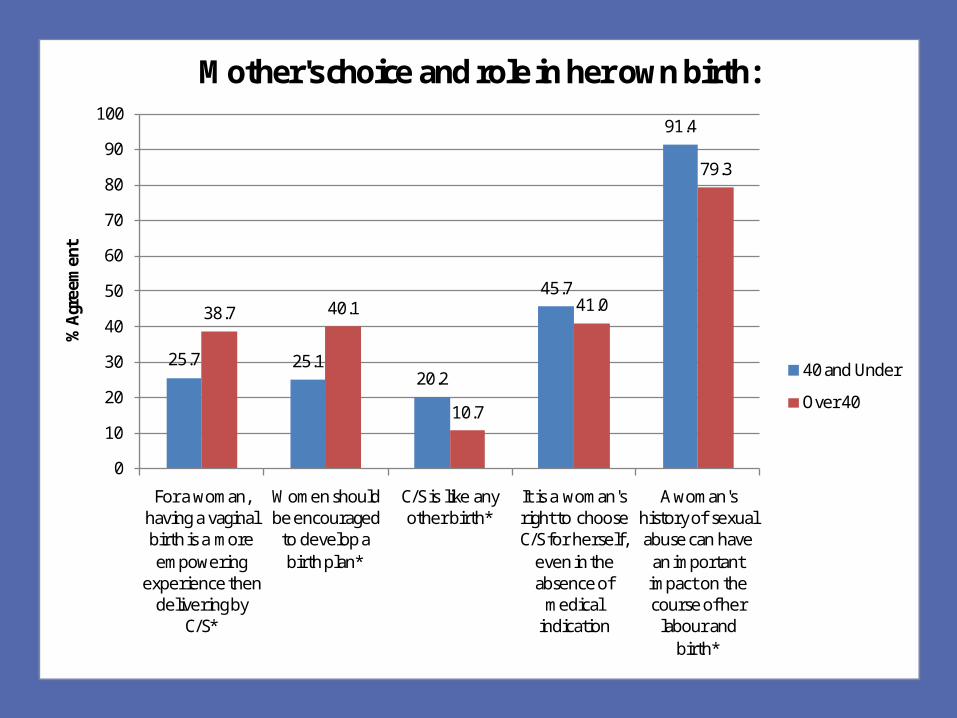
25.7 25.120.2
45.7
91.4
38.7 40.1
10.7
41.0
79.3
0
10
20
30
40
50
60
70
80
90
100
For a woman, having a vaginal birth is a more empowering
experience then delivering by
C/S*
Women should be encouraged
to develop a birth plan*
C/S is like any other birth*
It is a woman's right to choose C/S for herself,
even in the absence of
medical indication
A woman's history of sexual abuse can have
an important impact on the course of her
labour and birth*
% A
gree
men
tMother's choice and role in her own birth:
40 and Under
Over 40
Fear/Concern about vaginal birth compared with Cesarean

Positive attitudes toward provider/spouse fears about birth mode
Strongly Agree
Neutral
Strongly Disagree

21.1
12.6
22.3 24.3
12.6
5.49.0 10.9
0
10
20
30
40
50
60
70
80
90
100
may lead to urinary incontinence*
may comprimise sexual functioning*
may lead to fecal or flatal incontinence*
could lead to perineal and/or
pelvic floor damage*
% A
gree
men
tI fear vaginal birth for myself or my partner as it:
40 and Under
Over 40

The Attitudes of Family Physicians Providing Intrapartum Care vs. Those That Do Not:

• More than 50% of antenatal care in Canada provided by FPs who do not provide intrpartum care
• Only 11% of Canadian FPs attend births
• Yet 1/3 Canadian births attended by FPs
• Canadian FPs important providers of maternity care and influential on women’s perceptions and expectations about birth
897 Family Physicians
503 Provide Intrapartum Care
394 Provide Antepartum Care Only

Cesarean Section as preventive strategy strategy
p<.001 p=.011

Woman’s Role in her own birth
p=.042










Summary Summary
• Intrapartum FPs consistently hold more positive views about normal vaginal birth than FPP and especially FFN.
• Many antepartum only FPs seem to have a technological view of birth and potentially influence their patients to that view before transfer usually to OBs, and less likely FPs and occasionally to midwives. They decide when and to whom to refer their patients
• Therefore, we can’t neglect them as they provide more than 50% of the antenatal care in Canada

Summary:
• Many antepartum only FPs seem to distrust birth and likely influence their patients to that view. Therefore, we can’t neglect them as they provide 50% of the antenatal care in Canada
• Our postgraduate FP curriculum and CME activities for FPs need to acknowledge this problem and adjust accordingly.
• We need to encourage antenatal only FPs to refer to other FPs attending births and to engage in evidence-based counselling of their patients.
• Regardless of whether FPs attend births or not, we as a discipline need to engage in a national discussion about evidence-based, optimal birth.

And the Women Approaching Their First
Birth—what do they believe and know?---stratified by type of maternity provider
Some outcomes from the women’s study
•1355 Nulliparous women attending three types of providers•By demographics•And by trimester

Theme A:Woman’s Role in Her Own Birth
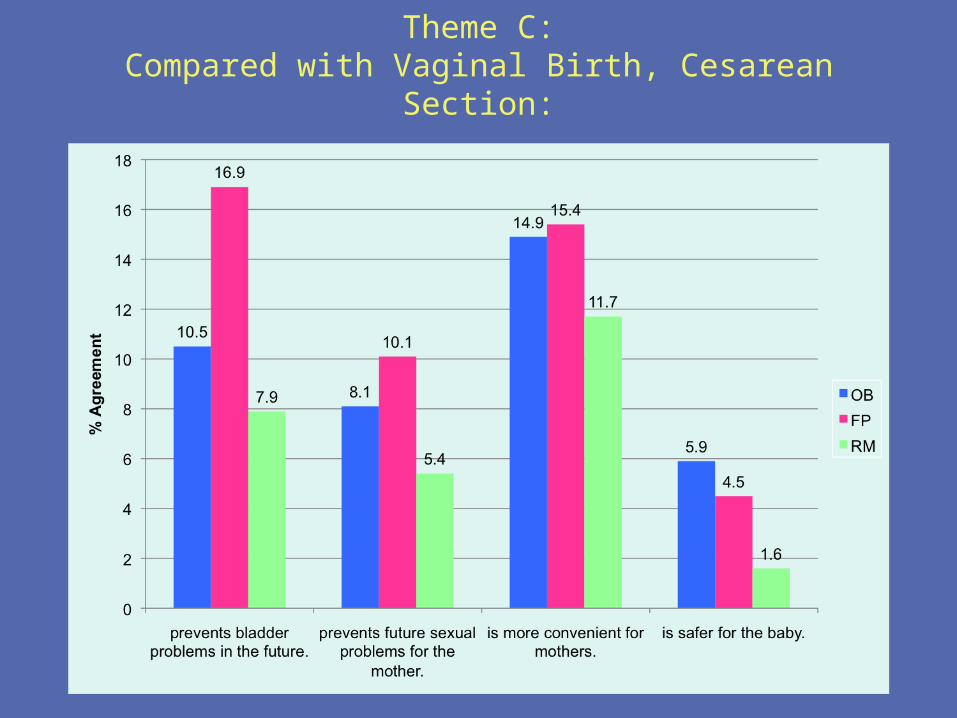
Theme C:Compared with Vaginal Birth, Cesarean Section:

Theme C:Cesarean Section (cont).

0.1 1 10
PROVIDER TYPEOB
*FP*RM
REGIONBC/AB
*SK/MBOntario
*Quebec*Atlantic
Territories
INCOMELess than 40K
40 to 60K60 to 100KOver 100K
*Prefer not to say
PLAN TO GIVE BIRTHCity
Small townRural/remote region
TRIMESTER12
*3
Evidence-Based Knowledge(10 items, KR20 = .822)
* indicates significance, p<.05
(Ordinal Logistic Regression Odds Ratios & 95% C.I.)
More Knowledgeable | . | Less Knowledgeable
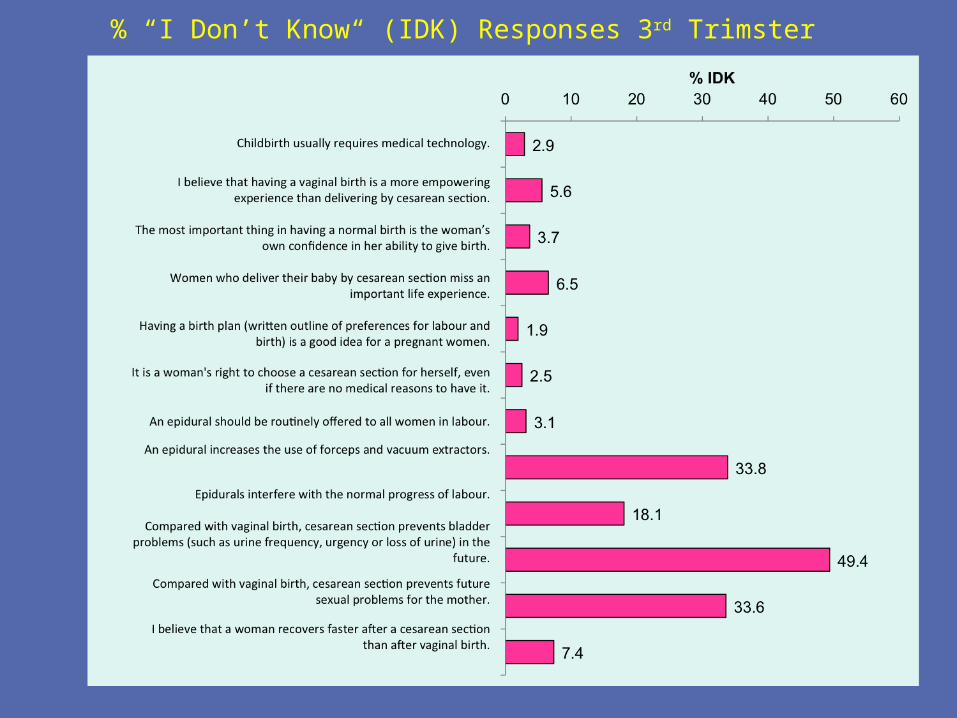
% “I Don’t Know“ (IDK) Responses 3rd Trimster
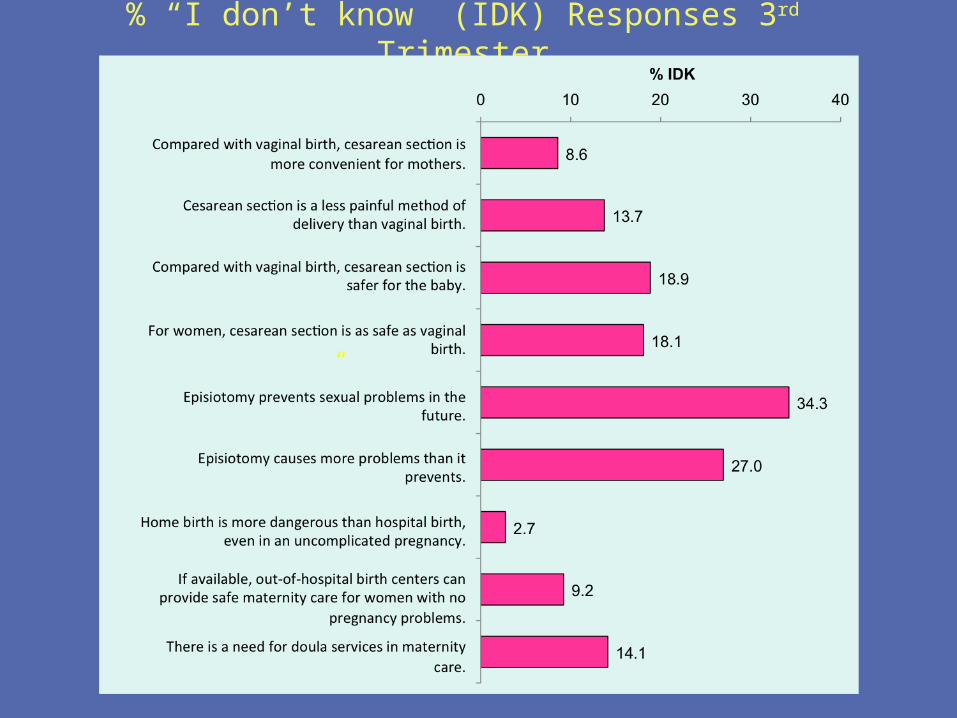
% “I don’t know” (IDK) Responses 3rd Trimester
“

Proportion of IDK Responses Stratified by Trimester and Provider

Meaning
• It appears that three different populations of women are attending the three provider groups
• Women attending midwives have a greater fund of evidence-based knowledge even before their first visit with a midwife
• Many women even late in pregnancy are lacking information that they should know

Overall Summary:
• Younger Canadian obstetricians <40, 81%who are women, more fearful/concerned about vaginal childbirth than older usually male colleagues
• Younger are sometimes evidence-based in their attitudes, sometimes not
• But it is about generation not gender• 30% of OBs do or would consider limiting their practice
to consultation not primary care
Summary• While great similarities within the OB discipline as a
group, – Some important differences amongst Obstericians—not only
by generation• More importantly, on most issues (even contentious
ones), 15-20% of OBs align with midwives (BOXPLOTS)• We need to know more about the underlying issues that divide
the disciplines. • We need to put ourselves in the shoes of each discipline—to
appreciate the why the differences

TOWARD BETTER CARE• Grow regulated midwifery in Canada• Rebuild FP Maternity Care• Encourage further doula development and
availability• If change is to happen, we need to understand
where each discipline is coming from and…• We need to appreciate the different value
systems in operation for each provider group—and why!
• Better is also cheaper

Summary: All Providers
• 71% of OBs support regulated/licensed midwifery, but 89% of OBs believe that home birth is more dangerous than hospital birth
• The majority of OBs are in disagreement with most beliefs held by RMs
• This dissonance has importance for the SOGC’s position on collaborative and team practice and Normal Birth
Summary: All Providers• RNs vary according to the issue, aligning with OBs or
Midwives or FPs—or independent.– Nurses have to adapt to the attitudes/beliefs of the other
providers• Doulas align with midwives• Many providers have strongly held beliefs that
may not be evidence-based• Truly informed consent cannot take place in
such an environment—especially for nulliparous women who are frightened and confused

WHAT DOES THIS TELL US?• We need to know more about the underlying issues that divide
the disciplines and motivate women• This requires attentive listening and the acquisition of deep
understanding of the underlying motivations of both providers and women.
• Small interventions and fixes are not likely to lead to enhanced partnerships.
• The care system and the education for truly collaborative care and true partnerships between maternity care providers and women will require development of trust and reciprocal understanding
• This a huge and long-term commitment between educators, professional organizations consumers and government

TOWARD BETTER CARE ?
• Inter-professional Education?• Redesign maternity care curriculum for OBs and FPs, Nurses
and Midwives too• Collaborative Practice/collaborative education? New Models of
Care?????– South Health only real model in Canada
• Altered Remuneration?• We must engage with antepartum FPs who do not do
intrapartum maternity! • We need to recognize the power imbalance that exists in
maternity care and do something to reduce it.

TOWARD BETTER CARE ?• Informed choice is a right• It is about acknowledging that women loose control when they
come to the hospital and doing something about it.• It is about paying attention to the woman’s value systems and
integrating them into the plan• It is about acknowledging that doing all this takes time—so we
have to design systems that provide the time• COMPASSION and understanding is at the core of any
contemplated change