Embed Size (px)
Citation preview

8/18/2019 Pilates Method for Women’s Health
http://slidepdf.com/reader/full/pilates-method-for-womens-health 1/12
REVIEW ARTICLE
Pilates Method for Women’s Health: Systematic
Review of Randomized Controlled Trials
Melissa Mazzarino, MCMid,a Debra Kerr, PhD,a Henry Wajswelner, DPhysio,b
Meg E. Morris, PhDb
From the aCenter for Chronic Disease Prevention and Management, College of Health & Biomedicine, Victoria University, Melbourne; and bCollege of Science, Health and Engineering, Department of Physiotherapy, La Trobe University, Melbourne, Australia.
Abstract
Objective: To critically analyze the benefits of Pilates on health outcomes in women.
Data Sources: CINAHL, MEDLINE, PubMed, Science Direct, SPORTDiscus, Physiotherapy Evidence Database (PEDro), Cochrane Central
Register of Controlled Trials, and Web of Science.
Study Selection: Databases were searched using the terms Pilates and Pilates Method. Published randomized controlled trials (RCTs) were
included if they comprised female participants with a health condition and a health outcome was measured, Pilates needed to be
administered, and the article was published in English in a peer-reviewed journal from 1980 to July 2014.
Data Extraction: Two authors independently applied the inclusion criteria to potential studies. Methodological quality was assessed using the
PEDro scale. A best-evidence grading system was used to determine the strength of the evidence.
Data Synthesis: Thirteen studies met the inclusion criteria. PEDro scale values ranged from 3 to 7 (mean, 4.5; median, 4.0), indicating a
relatively low quality overall. In this sample, Pilates for breast cancer was most often trialed (nZ2). The most frequent health outcomes
investigated were pain (nZ4), quality of life (nZ4), and lower extremity endurance (nZ2), with mixed results. Emerging evidence was found for
reducing pain and improving quality of life and lower extremity endurance.
Conclusions: There is a paucity of evidence on Pilates for improving women’s health during pregnancy or for conditions including breast cancer,obesity, or low back pain. Further high-quality RCTs are warranted to determine the effectiveness of Pilates for improving women’s health
outcomes.
Archives of Physical Medicine and Rehabilitation 2015;96:2231-42
ª 2015 by the American Congress of Rehabilitation Medicine
Pilates is a form of exercise based on movement principles
including whole-body movement, breathing, concentration,
centering, precision, and rhythm.1-5 Pilates is a mindful approach
to exercise, stimulating awareness of body structure, muscle
recruitment, and body alignment during movement.1,2 Joseph
Pilates2,3 claimed that this set of corrective exercises promoted
voluntary control over the body and effective posture, stabilizing
core muscles during dynamic movement, and promoted physical
and mental vitality.4,6 Pilates may be practiced on the mat using
one’s body weight or using Pilates equipment,7,8 which has
resistant springs to stabilize and strengthen deep muscle groups.2
Internationally, Pilates has appealed to women as a mainstream
form of exercise9 for improving physical health (muscular
strength, endurance, core stability, breathing), psychological
health (mood, motivation, body awareness), and motor functions
(muscle control, dynamic postural control, balance and
coordination).1,4
Recent systematic reviews have investigated the effectiveness
of Pilates on health outcomes related to body composition,10
breast cancer rehabilitation,11 physical fitness and fall prevention
in seniors,12-14 and pelvic floor muscle function.15 Aladro-
Gonzalvo et al10 reported on 7 studies and concluded that there
was poor empirical evidence supporting Pilates having a positive
effect on body composition. Alternatively, another review11 of 3
studies that applied Pilates for breast cancer rehabilitation found
trends in enhanced quality of life (QOL), mood, body image, and
aerobic capacity; however, sample sizes were small. GranacherDisclosures: none.
0003-9993/15/$36 - see front matter ª 2015 by the American Congress of Rehabilitation Medicine
http://dx.doi.org/10.1016/j.apmr.2015.04.005
Archives of Physical Medicine and Rehabilitation journal homepage: www.archives-pmr.org
Archives of Physical Medicine and Rehabilitation 2015;96:2231-42

8/18/2019 Pilates Method for Women’s Health
http://slidepdf.com/reader/full/pilates-method-for-womens-health 2/12
et al12 reviewed 20 studies and found improvement in trunk
muscle strength, functional performance, and balance in healthy
seniors. A similar review13 of 17 experimental studies found
improvement in static and dynamic balance in elderly people.
Currently, there is limited evidence to support Pilates’ effective-
ness to reduce stress urinary incontinence.15
Most studies examining Pilates have investigated individuals
with chronic low back pain.16-23 La Touche17 and Lim19 and
colleagues found evidence that Pilates reduced pain. A review22
of 5 systematic reviews concluded that there is inconclusive evidence
to support Pilates in reducing pain in people with chronic low back
pain, and cautioned against the use of findings because of con-
cerns about the heterogeneity of pooled studies and scienti-
fic rigor.
While several studies have investigated the effectiveness of
Pilates for health conditions (eg, breast cancer,9 postmenopausal
osteoporosis)24 and in promoting health (eg, strengthening pelvic
floor muscles,25 preventing falls),26,27 a synthesis and evaluation
of the evidence has not been conducted in the form of a systematic
review. Although there is emerging evidence that Pilates may
reduce chronic low back pain,18-21,23 these investigations were
from samples of men and women. The specific effects on women’s
health are difficult to ascertain in these mixed samples, and the
benefits are not clear. Therefore, the aim of this systematic review
was to evaluate the evidence for the effectiveness of Pilates for
improving health outcomes in women.
Methods
Data sources and searches
A joint search was conducted by 2 authors (M.M., H.W.). Studies
were selected for review up to November 2014 by searching the
following search engines: CINAHL, MEDLINE, PubMed, Sci-
ence Direct, SPORTDiscus, Physiotherapy Evidence Database(PEDro), Cochrane Central Register of Controlled Trials, and Web
of Science. The search strategy used the terms Pilates and
Pilates Method .
Study selection
Retrieved studies were reviewed for inclusion if they met the
following criteria: (1) published in a peer-reviewed journal in the
period 1980 to July 2014; (2) written in the English language; and
(3) the methodology included a randomized controlled trial (RCT)
design, Pilates administered as the intervention, female partici-
pants with a health condition, and an evaluation that included
measurement of a health outcome. The researchers adopted theWorld Health Organization (WHO)28 definition for a health con-
dition, which includes disease (acute or chronic), disorder, injury
or trauma, and other circumstances such as pregnancy, aging,
stress, congenital anomaly, or genetic predisposition. The re-
searchers used the WHO International Statistical Classification of
Diseases and Related Health Problems29 to identify health prob-
lems or diseases, as well as health conditions for individuals in a
general health situation or human life cycle including pregnancy,
childbirth, and aging. For high-resourced countries, the WHO30
defines an older person as 60 years of age, and the researchers
used this criteria to classify an aging population.
The WHO International Classification of Functioning,
Disability and Health28 was used to define health outcomes. It is a
2-level classification system for (1) body structures and functions,and (2) activities and participation. It was used as a framework to
categorize health outcome metrics with health conditions. For
example, pelvic floor muscle strength (eg, health outcome metric)
assessment may be used to investigate stress incontinence (eg, the
health condition). The following domains were used: structure
related to movement; neuromuscular and movement functions;
sensory functions and pain; mental functions; digestive, meta-
bolic, and endocrine functions; functions of the cardiovascular
system; and activities and participation.
For the first phase of the article selection process, 2 reviewers
(M.M., H.W.) assessed all retrieved abstracts for possible inclu-
sion. Discrepancies were resolved through discussion between the
2 reviewers. A third reviewer (D.K.) was consulted if consensus
could not be reached.
Full articles were then retrieved for the second phase of the
selection process to assess eligibility for inclusion in the review.
Two reviewers (M.M., H.W.) individually reviewed the articles to
confirm eligibility criteria. Articles that were identified as eligible
for inclusion were reexamined for accuracy and consistency by the
third reviewer (D.K.), who also arbitrated on discrepancies.
Rating the quality of articles
For each eligible RCT, methodological quality was assessed by 2
reviewers (M.M., H.W.) using the PEDro scale.31 The PEDro
scale, based on the Delphi list,32 is commonly used to assess the
quality of clinical trials in physiotherapy.31 It consists of 10
items: random allocation, concealed allocation, similarity at
baseline, subject blinding, therapist blinding, assessor blinding,
adequate follow-up (>85% follow-up for at least 1 key
outcome), intention-to-treat analysis, between-group compari-
sons for at least 1 key outcome, point estimates and variability
measures.32 These 10 items are each allocated a score of 1 point
if the criteria satisfy the standardized score. The PEDro score
ranges from 1 to 10, with higher PEDro scores corresponding to
a higher quality in methodology.33 A PEDro score 4 has been
evaluated to be of lower quality.31 The interrater reliability has
been evaluated previously31 and appears to be a valid measure of
methodological quality for clinical physical therapy trials.33,34
Disagreements in PEDro scoring between the 2 reviewers(M.M., H.W.) were resolved by the third reviewer (D.K.). All
PEDro scores were entered into an individual spread-
sheet (table 1).
Data synthesis
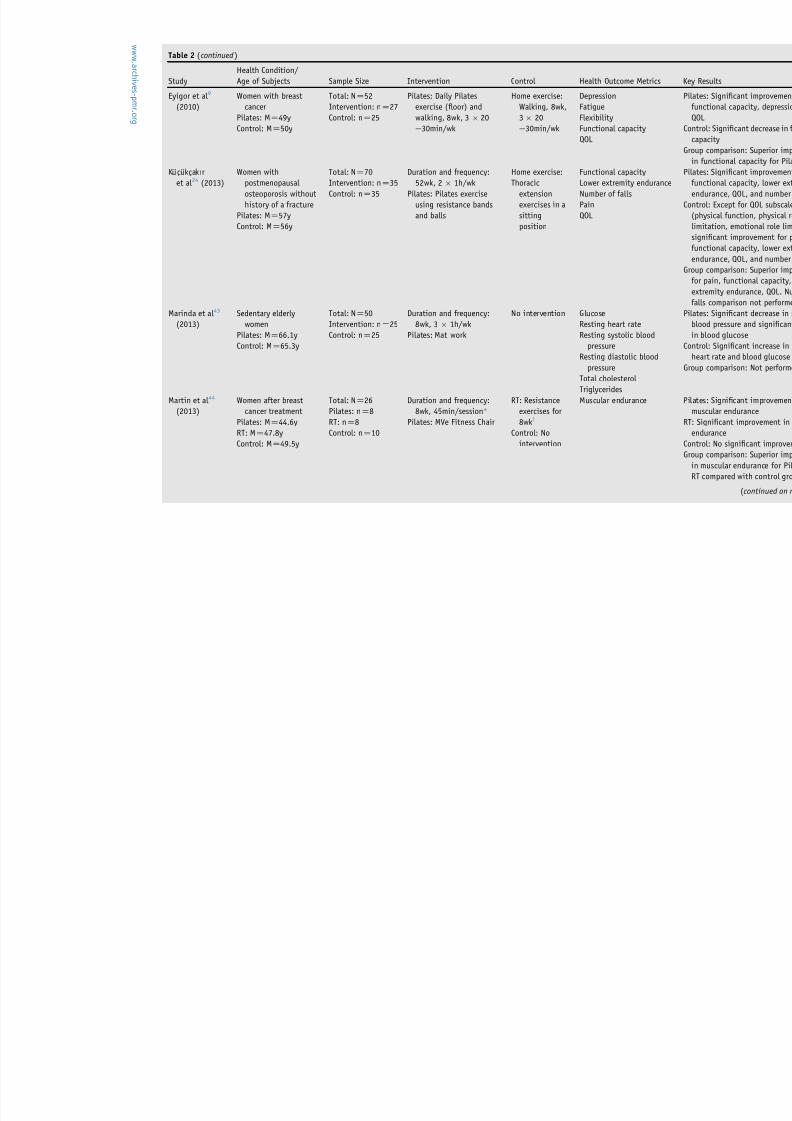
For articles that met the eligibility criteria, the following data were
extracted and reported in an evidence table (table 2): author/year,
health condition, age, sample size, intervention, health outcome
metrics, and results. Only statistically significant improvements in
health outcomes, evidenced by P<.05, were included. Table en-
tries were checked for accuracy and consistency by a second
List of abbreviations:
BES best-evidence synthesis
PEDro Physiotherapy Evidence Database
QOL quality of life
RCT randomized controlled trial
WHO World Health Organization
2232 M. Mazzarino et al
www.archives-pmr.org
8/18/2019 Pilates Method for Women’s Health
http://slidepdf.com/reader/full/pilates-method-for-womens-health 3/12
author (D.K.). Any disagreements concerning the information
reported in the evidence table were reconciled among the
research team.
The best-evidence synthesis (BES) approach35,36 was used to
measure the strength of the evidence. BES incorporates processes
of the meta-analysis including systematic literature searches and
quantification with a detailed analysis of study characteristics. The
BES approach is an alternative to a meta-analysis when the
number of eligible studies and power is low.35-38
BES provides astrategy for prioritizing evidence37 and has been used in a previous
review6 on the effects of Pilates in healthy people. The researchers
adopted the method of Cruz-Ferreira et al6 in allocating strength
of evidence to findings as follows: strong evidence allocated to
health outcomes where >1 high-quality (PEDRO score >4) RCT
is available; moderate evidence allocated to health outcomes
where 1 high-quality RCT with >1 low-quality RCT is available;
limited evidence allocated to health outcomes where 1 high-
quality or >1 low-quality RCT is available; and no evidence
allocated where 1 low-quality RCT or contradictory outcomes
were found between group comparisons.
Results
Study selection
The initial search located a total of 362 citations. After review of
the title and abstract, 59 full articles were retrieved for further
assessment of eligibility. After article review and identification of
duplicates, 13 RCTs9,24,39-49 were included in the review. Figure 1
illustrates the process for selection of articles.
Method quality
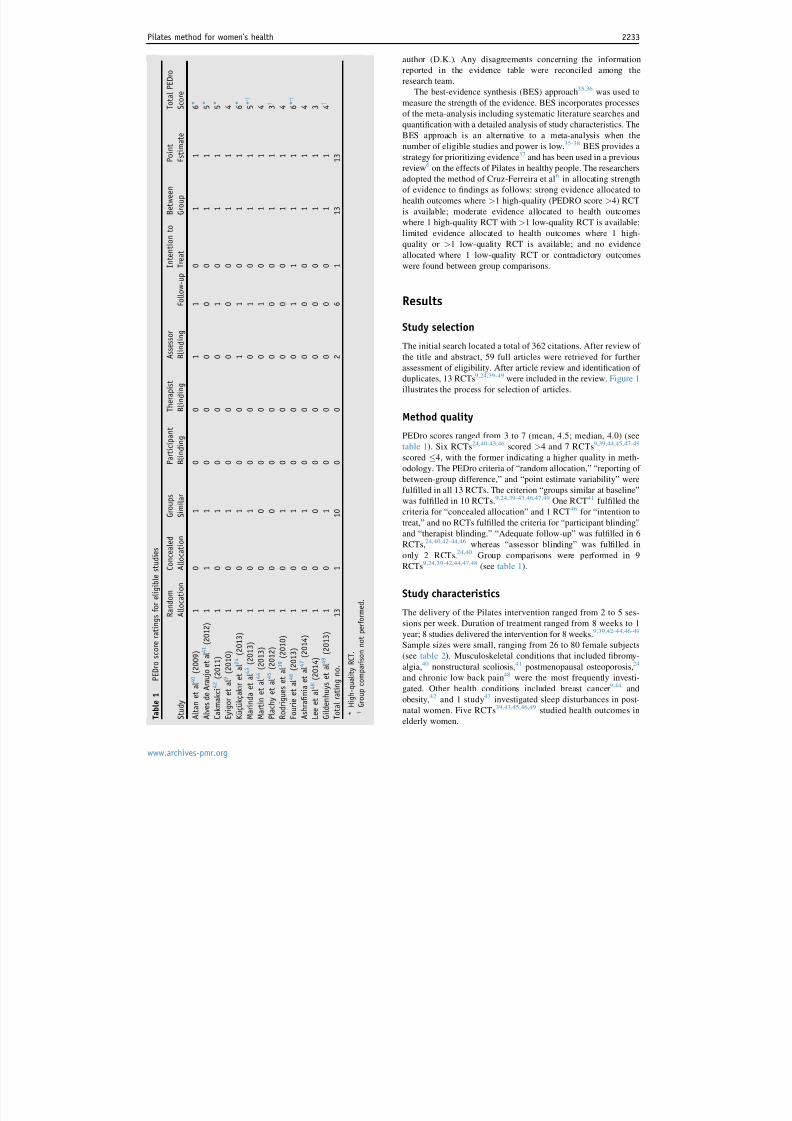
PEDro scores ranged from 3 to 7 (mean, 4.5; median, 4.0) (see
table 1). Six RCTs24,40-43,46 scored >4 and 7 RCTs9,39,44,45,47-49
scored 4, with the former indicating a higher quality in meth-
odology. The PEDro criteria of “random allocation,” “reporting of
between-group difference,” and “point estimate variability” were
fulfilled in all 13 RCTs. The criterion “groups similar at baseline”
was fulfilled in 10 RCTs.9,24,39-43,46,47,49 One RCT41 fulfilled the
criteria for “concealed allocation” and 1 RCT46 for “intention to
treat,” and no RCTs fulfilled the criteria for “participant blinding”
and “therapist blinding.” “Adequate follow-up” was fulfilled in 6
RCTs,24,40,42-44,46 whereas “assessor blinding” was fulfilled in
only 2 RCTs.24,40 Group comparisons were performed in 9
RCTs9,24,39-42,44,47,48 (see table 1).
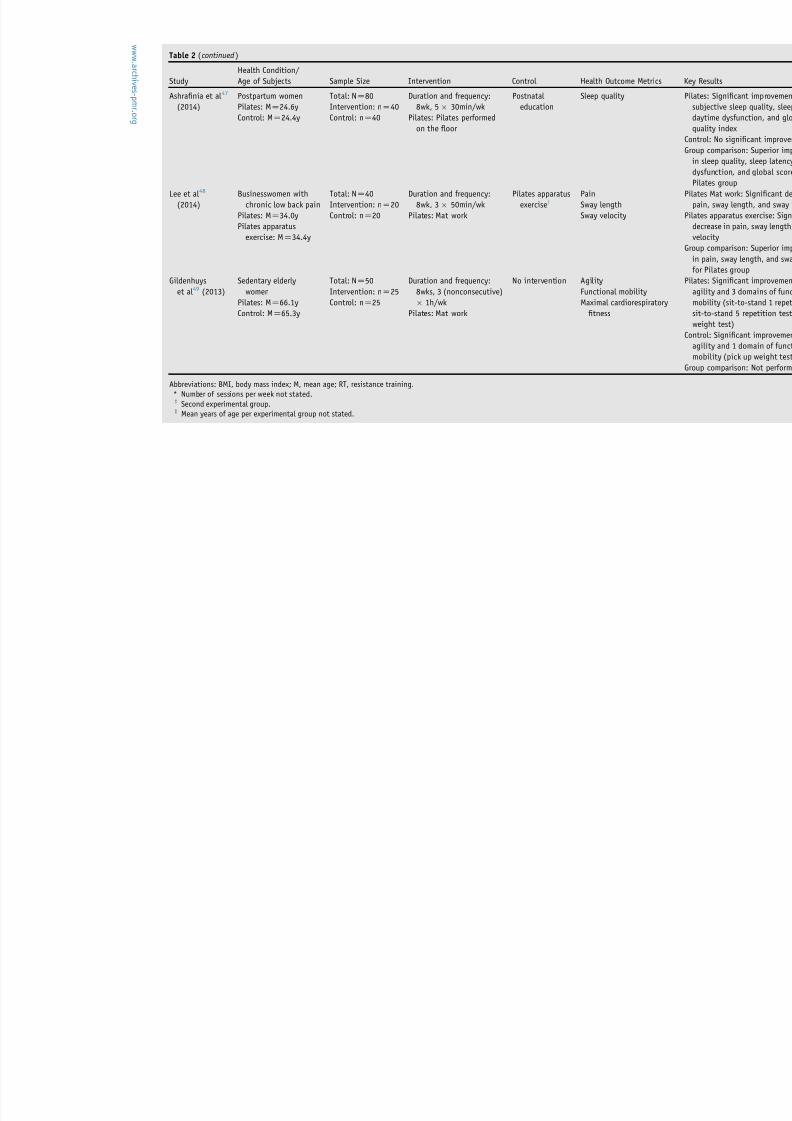
Study characteristics
The delivery of the Pilates intervention ranged from 2 to 5 ses-
sions per week. Duration of treatment ranged from 8 weeks to 1
year; 8 studies delivered the intervention for 8 weeks.9,39,42-44,46-49
Sample sizes were small, ranging from 26 to 80 female subjects
(see table 2). Musculoskeletal conditions that included fibromy-
algia,40 nonstructural scoliosis,41 postmenopausal osteoporosis,24
and chronic low back pain48 were the most frequently investi-
gated. Other health conditions included breast cancer9,44 and
obesity,42 and 1 study47 investigated sleep disturbances in post-
natal women. Five RCTs39,43,45,46,49 studied health outcomes in
elderly women. T a b l e
1
P E D r o s c o r e r a t i n g s f o r e l i g i b l e s t u d i e s
S t u d y
R a n d o m
A l l o c a t i o n
C o n c e a l e d
A l l o c a t i o n
G r o u p s
S i m i l a r
P a r t i c i p
a n t
B l i n d i n g
T h e r a p i s t
B l i n d i n g
A s s e s s o r
B l i n d i n g
F o l l o
w - u p
I n t e n t i o n t o
T r e a t
B e t w e e n
G r o u p
P o i n t
E s t i m
a t e
T o t a l P E D r o
S c o r e
A l t a n e t a l 4 0
( 2 0 0 9 )
1
0
1
0
0
1
1
0
1
1
6 *
A l v e s d e A r a u j o e t a l 4 1
( 2 0 1 2 )
1
1
1
0
0
0
0
0
1
1
5 *
C a k m a k c i 4 2
( 2 0 1 1 )
1
0
1
0
0
0
1
0
1
1
5 *
E y i g o r e t a l 9
( 2 0 1 0 )
1
0
1
0
0
0
0
0
1
1
4
K u ¨ c ¸ u ¨ k c ¸ a k ı r e t a l 2 4
( 2 0 1 3 )
1
0
1
0
0
1
1
0
1
1
6 *
M a r i n d a e t a l 4 3
( 2 0 1 3 )
1
0
1
0
0
0
1
0
1
1
5 * , y
M a r t i n e t a l 4 4
( 2 0 1 3 )
1
0
0
0
0
0
1
0
1
1
4
P l a c h y e t a l 4 5
( 2 0 1 2 )
1
0
0
0
0
0
0
0
1
1
3 y
R o d r i g u e s e t a l 3 9
( 2 0 1 0 )
1
0
1
0
0
0
0
0
1
1
4
F o u r i e e t a l 4 6
( 2 0 1 3 )
1
0
1
0
0
0
1
1
1
1
6 * , y
A s h r a fi n i a e t a l 4 7
( 2 0 1 4 )
1
0
1
0
0
0
0
0
1
1
4
L e e e t a l 4 8
( 2 0 1 4 )
1
0
0
0
0
0
0
0
1
1
3
G i l d e n h u y s e t a l 4 9
( 2 0 1 3 )
1
0
1
0
0
0
0
0
1
1
4 y
T o t a l r a t i n g n o .
1 3
1
1 0
0
0
2
6
1
1 3
1 3
*
H i g h - q u a l i t y R C T .
y
G r o u p c o m p a r i s o n n o t p e r f o r m e d .
Pilates method for women’s health 2233
www.archives-pmr.org

8/18/2019 Pilates Method for Women’s Health
http://slidepdf.com/reader/full/pilates-method-for-womens-health 4/12
Table 2 Description of eligible studies
Study
Health Condition/
Age of Subjects Sample Size Intervention Control Health Outcome Metrics
Altan et al 40
(2009)
Women with
fibromyalgia
syndrome
Pilates: MZ48.2y
Control: MZ
50.0y
Total: NZ50
Intervention: nZ25
Control: nZ25
Duration and frequency:
12wk, 3 1h/wk
Pilates: Pilates using props
(balls and resistance
bands)
Home exercise
(relaxation/
stretching)
Algometric score for tende
points
Fibromyalgia impact
Lower extremity endurance
PainQOL
Alves de Araujo
et al 41 (2012)
Sedentary women with
nonstructural
scoliosis
Range: 18e25y
Total: NZ31
Intervention: nZ20
Control: nZ11
Duration and frequency:
12wk, 2 1h/wk
Pilates: Pilates performed
with Swiss balls, flexball
quarks, and apparatus
(Cadillac, Reformer, Step
chair, and Ladder-barrel)
No intervention Degree of scoliosis
Pain
Range of motion for trunk
flexion
Cakmakci42
(2011)
Sedentary, obese women
Pilates: MZ36y
Control MZ39y
Total: NZ61
Intervention: nZ34
Control: nZ27
Duration and frequency:
8wk, 4 1h/wk
Pilates: Mat work with balls
No intervention Basal metabolic rate
BMI
Fat percentage
Flexibility
Lean body mass
Metabolic
Waist circumference
Skinfold thickness (biceps,
iliac, subscapula, triceps
Waist-hip ratio
Weight
w w w . a r c h i v
e s -
pmr
. or
g
8/18/2019 Pilates Method for Women’s Health
http://slidepdf.com/reader/full/pilates-method-for-womens-health 5/12
Table 2 (continued )
Study
Health Condition/
Age of Subjects Sample Size Intervention Control Health Outcome Metrics
Eyigor et al 9
(2010)
Women with breast
cancer
Pilates: MZ49y
Control: MZ50y
Total: NZ52
Intervention: nZ27
Control: nZ25
Pilates: Daily Pilates
exercise (floor) and
walking, 8wk, 3 20
e30min/wk
Home exercise:
Walking, 8wk,
3 20
e30min/wk
Depression
Fatigue
Flexibility
Functional capacity
QOL
Ku cukcakır
et al 24 (2013)
Women with
postmenopausal
osteoporosis without
history of a fracture
Pilates: MZ57y
Control: MZ56y
Total: NZ70
Intervention: nZ35
Control: nZ35
Duration and frequency:
52wk, 2 1h/wk
Pilates: Pilates exercise
using resistance bands
and balls
Home exercise:
Thoracic
extension
exercises in a
sitting
position
Functional capacity
Lower extremity endurance
Number of falls
Pain
QOL
Marinda et al 43
(2013)
Sedentary elderly
women
Pilates: MZ66.1y
Control: MZ65.3y
Total: NZ50
Intervention: nZ25
Control: nZ25
Duration and frequency:
8wk, 3 1h/wk
Pilates: Mat work
No intervention Glucose
Resting heart rate
Resting systolic blood
pressure
Resting diastolic blood
pressure
Total cholesterol
Triglycerides
Martin et al 44
(2013)
Women after breast
cancer treatment
Pilates: MZ44.6y
RT: MZ47.8y
Control: MZ49.5y
Total: NZ26
Pilates: nZ8
RT: nZ8
Control: nZ10
Duration and frequency:
8wk, 45min/session*
Pilates: MVe Fitness Chair
RT: Resistance
exercises for
8wky
Control: No
intervention
Muscular endurance
w w w . a r c h i v
e s -
pmr . or
g

8/18/2019 Pilates Method for Women’s Health
http://slidepdf.com/reader/full/pilates-method-for-womens-health 6/12
Table 2 (continued )
Study
Health Condition/
Age of Subjects Sample Size Intervention Control Health Outcome Metrics
Plachy et al 45
(2012)
Elderly women
Pilates: MZ66.2y
Aqua/Pilates: MZ67.1y
Control: MZ68.2y
Total: NZ42
Intervention: nZ15
Aqua/Pilates: nZ15
Control: nZ12
Frequency: 24wk
Pilates: Pilates exercises,
3 1h/wk
Aqua/Pilates: 2 1h/wk
(Aqua) and Pilates 1 1h/wk
Aqua fitness/
Pilatesy
No intervention
Aerobic endurance
Endurance and low body
strength
Flexion of right shoulder
Flexion of right hipLumbar spine flexion
Thoracolumbar spine flexion
Trunk lateral flexion
Rodrigues et al 39
(2010)
Elderly women
MZ66yzTotal: NZ52
Intervention: nZ27
Control: nZ25
Duration and frequency:
8wk, 2 1h/wk
Pilates: Pilates exercises
used with Bobath ball,
Cadillac, Wall Unit,
Combo chair, and
Reformer devices
No intervention Personal autonomy
QOL
Static balance
Fourie et al 46
(2013)
Elderly sedentary
women
Pilates: MZ66.1y
Control: MZ65.3y
Total: NZ50
Intervention: nZ25
Control: nZ25
Duration and frequency:
8wk, 3 1h/wk
Pilates: Mat work
No intervention Body fat
Body mass
BMI
Fat massLean body mass
w w w . a r c h i v
e s -
pmr
. or
g
8/18/2019 Pilates Method for Women’s Health
http://slidepdf.com/reader/full/pilates-method-for-womens-health 7/12
Table 2 (continued )
Study
Health Condition/
Age of Subjects Sample Size Intervention Control Health Outcome Metrics
Ashrafinia et al 47
(2014)
Postpartum women
Pilates: MZ24.6y
Control: MZ24.4y
Total: NZ80
Intervention: nZ40
Control: nZ40
Duration and frequency:
8wk, 5 30min/wk
Pilates: Pilates performed
on the floor
Postnatal
education
Sleep quality
Lee et al 48
(2014)
Businesswomen with
chronic low back pain
Pilates: MZ34.0y
Pilates apparatus
exercise: MZ34.4y
Total: NZ40
Intervention: nZ20
Control: nZ20
Duration and frequency:
8wk, 3 50min/wk
Pilates: Mat work
Pilates apparatus
exerciseyPain
Sway length
Sway velocity
Gildenhuys
et al 49
(2013)
Sedentary elderly
womenPilates: MZ66.1y
Control: MZ65.3y
Total: NZ50
Intervention: nZ
25Control: nZ25
Duration and frequency:
8wks, 3 (nonconsecutive) 1h/wk
Pilates: Mat work
No intervention Agility
Functional mobilityMaximal cardiorespiratory
fitness
Abbreviations: BMI, body mass index; M, mean age; RT, resistance training.
* Number of sessions per week not stated.y Second experimental group.z Mean years of age per experimental group not stated.
w w w . a r c h i v
e s -
pmr . or
g

8/18/2019 Pilates Method for Women’s Health
http://slidepdf.com/reader/full/pilates-method-for-womens-health 8/12
Different approaches for Pilates were used as the intervention.
In 6 RCTs,9,43,46-49
Pilates was performed on a mat or floor, and insome studies assistive equipment (ie, Pilates balls, resistance
bands) was also used.24,40,42 Three RCTs39,41,44 used at least 1
apparatus (ie, Cadillac, Reformer, Step chair, Ladder-barrel,
Combo chair, MVe Fitness Chair). The form of Pilates was not
specified for 1 study.45 In 1 RCT,9 the Pilates intervention was
delivered in addition to home exercises and walking exercise.
For 8 RCTs,39,41-46,49 the control condition did not include any
specific exercise. In 3 RCTs, the control group performed ho me
exercises that included relaxation and stretching exercises,40
walking,9 and thoracic extension exercise,24 and in 1 RCT47
women were provided with postnatal care education.
Ten studies9,24,39-43,46,47,49 had 1 intervention group and 1
control group as part of the methodology. Two studies44,45 had 2
intervention groups and a control group. The study by Martin
et al44 had 1 intervention group that performed Pilates on the MVe
Fitness Chair, and the other intervention group received resistance
training. The study by Plachy et al45 included a Pilates interven-
tion group and an aqua fitness/Pilates class intervention group.
Lee et al48 included 2 experimental Pilates groups only (mat
Pilates group and an apparatus Pilates group). In the study by
Altan et al40 there were 25 participants in a single large group,
whereas the other studies did not clarify group size. The primary
discipline of the instructor was reported in 8
studies9,39,41,42,44,46,47,49: Pilates instructor certified (nZ3),42,46,49
physiotherapist certified in Pilates instruction (nZ2),9,39 physio-
therapist (Pilates certification not reported) (nZ1),41 and exercise
and sport science clinician (Pilates certification not reported)
(nZ2).44,47 No studies described the style of Pilates or origin of
Pilates exercises.
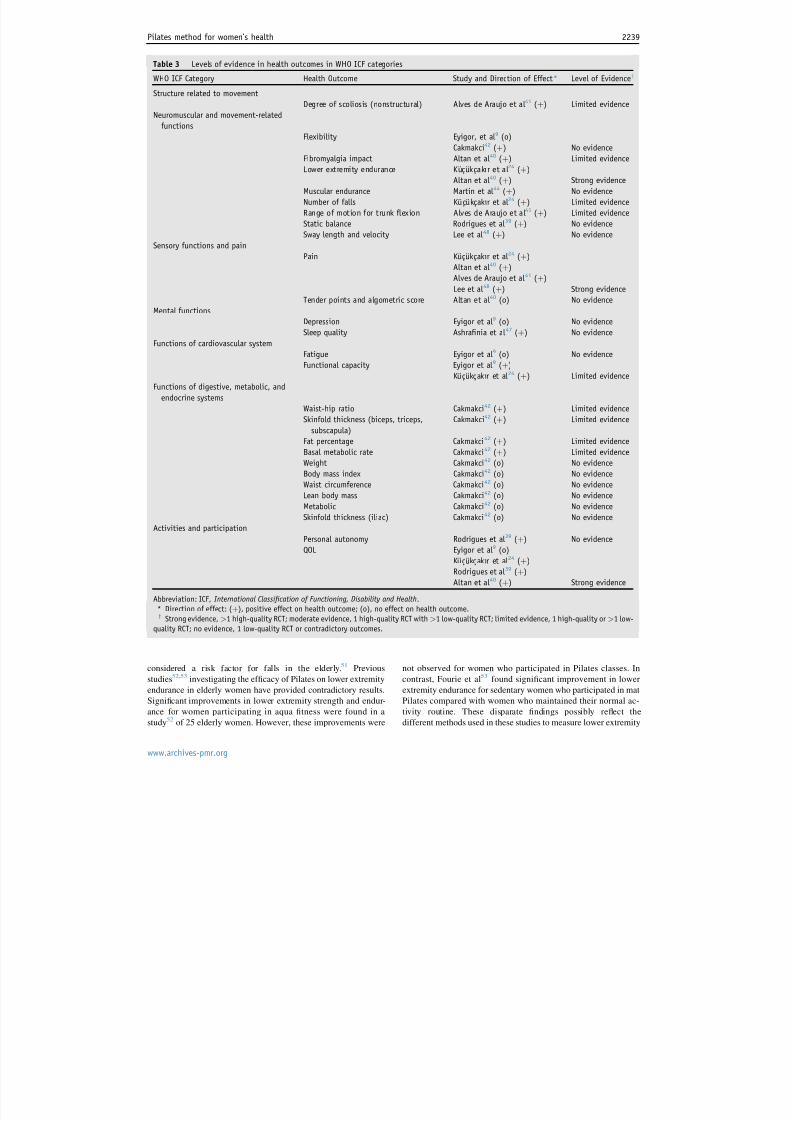
Best-evidence synthesis: strength of evidence
Health outcomes are presented in table 3. With the application of
BES, strong evidence was f ound for Pilates in improving health
outcomes for pain,24,40,41,48 lower extremity endurance,24,40 andQOL.24,39,40 Reduction in pain was demonstrated in 3 high-quality
RCTs investigating fibromyalgia syndrome,40 nonstructural
scoliosis,41 and postmenopausal osteoporosis,24 and 1 low-quality
RCT48 investigating low back pain. Strong evidence for lower
extremity endurance was provided by 2 high-quality RCTs24,40
investigating postmenopausal osteoporosis24 and fibromyalgia
syndrome.40 Strong evidence for improvement in QOL was pro-
vided by 2 high-quality RCTs24,40 investigating postmenopausal
osteoporosis24 and fibromyalgia syndrome,40 and 1 low-quality
RCT39 of elderly women. In a study of female breast cancer pa-
tients by Eyigor et al,9 no improvement was found for QOL.
Limited evidence was found f or improving the degree of
scoliosis,41 impact of fibromyalgia,40 number of falls,24 range of
motion in trunk flexion,41 functional capacity,9,24 waist-hip ratio,42
skinfold thickness (biceps, triceps, subscapular),42 fat percent-
age,42 and basal metabolic rate.42 No evidence was found for
improving muscular endurance,44 static balance,39 sway length
and velocity,48 tender points,40 depression,9 sleep quality,47 fa-
tigue,9 personal autonomy,39 weight,42 body mass index,42 waist
circumference,42 lean body mass,42 metabolic rate,42 and iliac
skinfold thickness.42 Contradictory results were found for flexi-
bility, in which improvement was found in obese women,42 but no
effect was found in female breast cancer patients.9
Discussion
This systematic review of Pilates for women’s health found
emerging evidence for reducing pain and improving QOL and
lower extremity endurance. However, overall, the methodological
quality of eligible RCTs was relatively low (mean score, 4.5).
There was a lack of high-quality trials investigating the benefits of
Pilates for improving women’s health outcomes.
This review found a reduction in pain based on studies
investigating fibromyalgia,40 nonstructural scoliosis,41 post-
menopausal osteoporosis,24 and low back pain.48 For these
studies, the Pilates intervention was compared with control con-
ditions including home exercise relaxation and stretching,40 no
intervention,41 and thoracic extension exercises,24 and in 1 study48
mat-based Pilates was compared with Pilates apparatus exercise.
This demonstrates that there is a paucity of evidence as to whether
other treatment regimens or forms of exercise are more or less
effective in reducing pain.16,19,20,23
Improvement in QOL was found in studies investigating fi-
bromyalgia syndrome40 and postmenopausal osteoporosis,24 and
in a study of elderly women.39 It is unclear from the current re-
view whether participating in a therapeutic ritual provided a pla-
cebo effect,50 and whether the acuity of a health condition
influences QOL in women.
Emerging evidence was found f or lower extremity endurance
in RCTs investigating fibromyalgia40 and postmenopausal osteo-
porosis.24 Weakened low extremity strength and endurance sec-
ondary to physiological changes associated with aging are
Fig 1 Flow diagram to summarize stages of systematic review.
Abbreviation: MA, meta-analysis.
2238 M. Mazzarino et al
www.archives-pmr.org
8/18/2019 Pilates Method for Women’s Health
http://slidepdf.com/reader/full/pilates-method-for-womens-health 9/12
considered a risk factor for falls in the elderly.51 Previous
studies52,53 investigating the efficacy of Pilates on lower extremity
endurance in elderly women have provided contradictory results.
Significant improvements in lower extremity strength and endur-
ance for women participating in aqua fitness were found in a
study52 of 25 elderly women. However, these improvements were
not observed for women who participated in Pilates classes. In
contrast, Fourie et al53 found significant improvement in lower
extremity endurance for sedentary women who participated in mat
Pilates compared with women who maintained their normal ac-
tivity routine. These disparate findings possibly reflect the
different methods used in these studies to measure lower extremity
Table 3 Levels of evidence in health outcomes in WHO ICF categories
WHO ICF Category Health Outcome Study and Direction of Effect* Level of Evidencey
Structure related to movement
Degree of scoliosis (nonstructural) Alves de Araujo et al 41 (þ) Limited evidence
Neuromuscular and movement-related
functions
Flexibility Eyigor, et al 9 (o)
Cakmakci42
(þ) No evidenceFibromyalgia impact Altan et al 40 (þ) Limited evidence
Lower extremity endurance Kucukcakır et al 24 (þ)
Altan et al 40 (þ) Strong evidence
Muscular endurance Martin et al 44 (þ) No evidence
Number of falls Kucukcakır et al 24 (þ) Limited evidence
Range of motion for trunk flexion Alves de Araujo et al 41 (þ) Limited evidence
Static balance Rodrigues et al 39 (þ) No evidence
Sway length and velocity Lee et al 48 (þ) No evidence
Sensory functions and pain
Pain Kucukcakır et al 24 (þ)
Altan et al 40 (þ)
Alves de Araujo et al 41 (þ)
Lee et al 48 (þ) Strong evidence
Tender points and algometric score Altan et al 40 (o) No evidence
Mental functions
Depression Eyigor et al 9 (o) No evidence
Sleep quality Ashrafinia et al 47 (þ) No evidence
Functions of cardiovascular system
Fatigue Eyigor et al 9 (o) No evidence
Functional capacity Eyigor et al 9 (þ)
Kucukcakır et al 24 (þ) Limited evidence
Functions of digestive, metabolic, and
endocrine systems
Waist-hip ratio Cakmakci42 (þ) Limited evidence
Skinfold thickness (biceps, triceps,
subscapula)
Cakmakci42 (þ) Limited evidence
Fat percentage Cakmakci42
(þ) Limited evidenceBasal metabolic rate Cakmakci42 (þ) Limited evidence
Weight Cakmakci42 (o) No evidence
Body mass index Cakmakci42 (o) No evidence
Waist circumference Cakmakci42 (o) No evidence
Lean body mass Cakmakci42 (o) No evidence
Metabolic Cakmakci42 (o) No evidence
Skinfold thickness (iliac) Cakmakci42 (o) No evidence
Activities and participation
Personal autonomy Rodrigues et al 39 (þ) No evidence
QOL Eyigor et al 9 (o)
Kucukcakır et al 24 (þ)
Rodrigues et al 39 (þ)
Altan et al 40 (þ) Strong evidence
Abbreviation: ICF, International Classification of Functioning, Disability and Health.
* Direction of effect: (þ), positive effect on health outcome; (o), no effect on health outcome.y Strong evidence, >1 high-quality RCT; moderate evidence, 1 high-quality RCT with >1 low-quality RCT; limited evidence, 1 high-quality or >1 low-
quality RCT; no evidence, 1 low-quality RCT or contradictory outcomes.
Pilates method for women’s health 2239
www.archives-pmr.org

8/18/2019 Pilates Method for Women’s Health
http://slidepdf.com/reader/full/pilates-method-for-womens-health 10/12
endurance (time to walk up stairs test,52 squat till fatigue test53) as
well as the varied control conditions. Future studies require con-
gruency in the methodological approach to measuring lower ex-
tremity endurance in elderly women, and for specific health
conditions such as fibromyalgia and osteoporosis.
Limited evidence was found for 4 health outcomes related to
body composition: waist-hip ratio,42 sk infold thickness,42 fat
percentage,42 and basal metabolic rate.42 These findings are
consistent with those of Aladro-Gonzalvo,10
who found poorempirical evidence supporting Pilates having a positive effect on
body composition. Change in body composition health outcome
metrics may be mediated by factors such as life stage (pregnancy,
menopause), health conditions (ie, bulimia, obesity), pre-
intervention fitness level (ie, athletic vs sedentary), and energy
intake (ie, diet),10,54 and these variables require further
consideration.
Contradictory results were found for flexibility. Improvement
was found in obese women,42 but no effect was found in female
breast cancer patients.9 These studies, however, had significant
methodological differences. The method of measuring flexibility
was not stated in 1 study,9 and the sit and reach test42 was used in
the other. Both studies implemented the intervention over 8
weeks; however, the frequency and duration of Pilates were 4
sessions per week, 60 minutes per session for obese woman, 42 and
3 sessions per week, 20 to 30 minutes per session for female breast
cancer patients.9 In a review6 of healthy adults, strong evidence
was f ound for improvement in flexibility in sedentary adult fe-
males,55 healthy adults,56 healthy middle-aged adults,57 and
elderly women,26 with flexibility measured in the following body
areas: trunk,55 lower back,26,56 hamstrings,26,56,57 and upper
body.56 For these studies, the duration of the Pilates intervention
was 60 minutes, and the frequency of sessions was 257 or 326,55,56
times per week for a period of 5 weeks,55 8 weeks,56 and 12
weeks.26,57 Factors underpinning exercise prescription, including
body area of focus, type of exercise, number of repetitions, and
frequency of sessions, may influence health outcomes such asflexibility6 and should be considered in future research.
Pilates is advocated for alleviating discomforts of preg-
nancy58,59 and assisting in strength and endurance for labor and
birth60; however, this review found that evidence is absent for
improving perinatal outcomes in these situations. The American
College of Obstetricians and Gynecologists and the Centers for
Disease Control and Prevention61-63 recommended that in the
absence of medical or obstetric complications, women should
moderately exercise for 30 minutes daily. Evidence is needed to
verify the benefits of Pilates as a form of exercise for pregnancy
and birthing outcomes.
Study limitationsLimiting the eligibility criteria to women may have omitted evi-
dence on health outcomes previously found in mixed samples. For
example, a large body of evidence on mixed samples of men and
women shows that Pilates may reduce pain and disability in in-
dividuals with chronic low back pain.23 Those studies do not
discern differences in outcomes for men and women. The BES
focused on 3 high-quality24,40,41 and 2 low-quality9,48 studies,
which limits the generalizability of findings. Another limitation
was that only RCTs were included; observational and qualitative
studies may provide additional findings in improving health out-
comes for women.6 In addition, the search was limited to English-
language journals, and studies using other languages were not
considered. This review focused on findings that were statistically
significant. Overall, the studies were small (n<80), and this may
have affected the strength of findings. Larger, well-designed RCTs
are needed. A lack of homogeneity, range of conditions, and
variation in the Pilates intervention inhibited the synthesis of
findings. Also, the extent to which the placebo effect associated
with the therapeutic intervention influences the reduction in pain
and improves QOL in women requires further investigation.
Future research recommendations
Future RCTs could be strengthened by incorporating concealed
allocation, intention-to treat analysis, and blinding. Congruency in
the methodological approach for smaller studies should be
considered, including the type of Pilates intervention, exact ex-
ercise prescription, duration and frequency of exercise, and mea-
surement tools. The nonspecific effects or contextual benefits
associated with participating in a mindful approach to exercise
such as the participantePilates instructor relationship may
contribute to a placebo effect and needs verification.50 The
effectiveness of Pilates for improving health for specific condi-
tions such as breast cancer, obesity, and chronic low back pain isyet to be determined. Given the popularity of Pilates for pregnant
women,60 evidence is needed to support claims of antenatal and
birthing benefits.
Conclusions
Pilates is a popular form of exercise for women who strive to
improve their physical and psychological health. However, there is
a paucity of evidence that Pilates improves women’s health. We
found emerging evidence to show that Pilates may reduce pain and
may improve QOL and lower extremity endurance. Whether
Pilates improves women’s health during pregnancy or optimizeshealth outcomes for breast cancer, obesity, and chronic low back
pain is yet to be confirmed.
Keywords
Pilates-based exercises; Rehabilitation; Review; Women’s health
Corresponding author
Melissa Mazzarino, MCMid, Victoria University, McKechnie St,
Melbourne, Victoria, Australia 3021. E-mail address: melissa.
References
1. Lange C, Unnithan VB, Larkam E, Latta PM. Maximizing the ben-
efits of Pilates-inspired exercise for learning functional motor skills. J
Bodyw Mov Ther 2000;4:99-108.
2. Pilates J, Miller W. Return to life through contrology. Incline Village:
Presentation Dynamics; 1945.
3. Pilates JH. Your health. Incline Village: Presentation Dynamics;
1934.
4. Latey P. The Pilates method: history and philosophy. J Bodyw Mov
Ther 2001;5:275-82.
2240 M. Mazzarino et al
www.archives-pmr.org

8/18/2019 Pilates Method for Women’s Health
http://slidepdf.com/reader/full/pilates-method-for-womens-health 11/12
5. Lessen D. The P.M.A. Pilates certification exam study guide. Miami:
Pilates Method Alliance; 2014.
6. Cruz-Ferreira A, Fernandes J, Laranjo L, Bernardo LM, Silva A. A
systematic review of the effects of Pilates method of exercise in
healthy people. Arch Phys Med Rehabil 2011;92:2071-81.
7. Anderson B. Fitting Pilates into a rehabilitation practice. Rehab
Manag 2010;23(24):26-7.
8. Kloubec J. Pilates: how does it work and who needs it? Muscles
Ligaments Tendons J 2011;1:61-6.
9. Eyigor S, Karapolat H, Yesil H, Uslu R, Durmaz B. Effects of Pilatesexercises on functional capacity, flexibility, fatigue, depression and
quality of life in female breast cancer patients: a randomized
controlled study. Eur J Phys Rehabil Med 2010;46:481-7.
10. Aladro-Gonzalvo AR, Machado-Dıaz M, Moncada-Jimenez J, Her-
nandez-Elizondo J, Araya-Vargas G. The effect of Pilates exercises
on body composition: a systematic review. J Bodyw Mov Ther 2012;
16:109-14.
11. Stan DL, Collins NM, Olsen MM, Croghan I, Pruthi S. The evolution
of mindfulness-based physical interventions in breast cancer survi-
vors. Evid Based Complementary Altern Med 2012;2012:758641.
12. Granacher U, Gollhofer A, Hortobagyi T, Kressig RW,
Muehlbauer T. The importance of trunk muscle strength for balance,
functional performance, and fall prevention in seniors: a systematic
review. Sports Med 2013;43:627-41.
13. Cancela JM, de Oliveira IM, Rodriguez FG. Effects of Pilates inphysical fitness on older adults. A systematic review. Eur Rev Aging
Phys Act 2014;11:81-94.
14. Barker AL, Bird ML, Talevski J. Effect of Pilates exercise for
improving balance in older adults: a systematic review with meta-
analysis. Arch Phys Med Rehabil 2015;96:715-23.
15. Bo K, Herbert RD. There is not yet strong evidence that exercise
regimens other than pelvic floor muscle training can reduce stress
urinary incontinence in women: a systematic review. J Physiother
2013;59:159-68.
16. Sullivan AB, Scheman J, Venesy D, Davin S. The role of exercise
and types of exercise in the rehabilitation of chronic pain: specific or
nonspecific benefits. Curr Pain Headache Rep 2012;16:153-61.
17. La Touche R, Escalante K, Linares MT. Treating non-specific chronic
low back pain through the Pilates Method. J Bodyw Mov Ther 2008;
12:364-70.
18. Posadzki P, Lizis P, Hagner-Derengowska M. Pilates for low
back pain: a systematic review. Complement Ther Clin Pract 2011;
17:85-9.
19. Lim EC, Poh RL, Low AY, Wong WP. Effects of Pilates-based ex-
ercises on pain and disability in individuals with persistent nonspe-
cific low back pain: a systematic review with meta-analysis. J Orthop
Sports Phys Ther 2011;41:70-80.
20. Pereira LM, Obara K, Dias JM, et al. Comparing the Pilates method
with no exercise or lumbar stabilization for pain and functionality in
patients with chronic low back pain: systematic review and meta-
analysis. Clin Rehabil 2012;26:10-20.
21. Aladro-Gonzalvo AR, Araya-Vargas GA, Machado-Dıaz M, Salazar-
Rojas W. Pilates-based exercise for persistent, non-specific low back
pain and associated functional disability: a meta-analysis with meta-
regression. J Bodyw Mov Ther 2013;17:125-36.
22. Wells C, Kolt GS, Marshall P, Hill B, Bialocerkowski A. Effective-
ness of Pilates exercise in treating people with chronic low back pain:
a systematic review of systematic reviews. BMC Med Res Methodol
2013;13:7.
23. Wells C, Kolt GS, Marshall P, Hill B, Bialocerkowski A. The
effectiveness of Pilates exercise in people with chronic low back
pain: a systematic review. PLoS One 2014;9:e100402.
24. Kucukcak ır N, Altan L, Korkmaz N. Effects of Pilates exercises on
pain, functional status and quality of life in women with post-
menopausal osteoporosis. J Bodyw Mov Ther 2013;17:204-11.
25. Culligan PJ, Scherer J, Dyer K, et al. A randomized clinical trial
comparing pelvic floor muscle training to a Pilates exercise program for
improving pelvic muscle strength. Int Urogynecol J 2010;21:401-8.
26. Irez GB, Ozdemir RA, Evin R, Irez SG, Korkusuz F. Integrating
Pilates exercise into an exercise program for 65þ year-old women to
reduce falls. J Sports Sci Med 2011;10:105-11.
27. Bird ML, Hill KD, Fell JW. A randomized controlled study inves-
tigating static and dynamic balance in older adults after training with
Pilates. Arch Phys Med Rehabil 2012;93:43-9.
28. World Health Organization. International Classification of Func-
tioning, Disability and Health. Geneva: WHO; 2001.
29. World Health Organization. WHO International Statistical Classifi-
cation of Diseases and Related Health Problems, 2010. Available at:http://apps.who.int/classifications/icd10/browse/2010/en. Accessed
January 11, 2015.
30. World Health Organization. Definition of an older or elderly person.
Geneva: WHO; 2010. Available at: http://www.who.int/healthinfo/
survey/ageingdefnolder/en/ . Accessed January 11, 2015.
31. Mayer CG, Sherrington C, Herbert RD, Moseley AM, Elkins M.
Reliability of the PEDro scale for rating quality of randomized
controlled trials. Phys Ther 2003;83:713-21.
32. Verhagen AP, de Vet HC, de Bie RA, et al. The Delphi list: a criteria
list for quality assessment of randomized clinical trials for con-
ducting systematic reviews developed by Delphi consensus. J Clin
Epidemiol 1998;51:1235-41.
33. de Morton NA. The PEDro scale is a valid measure of the method-
ological quality of clinical trials: a demographic study. Aust J
Physiother 2009;55:129-33.34. Olivo SA, Macedo LG, Gadotti IC, Fuentes J, Stanton T, Magee DJ.
Scales to assess the quality of randomized controlled trials: a sys-
tematic review. Phys Ther 2008;88:156-75.
35. Slavin RE. Best-evidence synthesis: an alternative to meta-analytic
and traditional reviews. Educ Res 1986;15:5-11.
36. Slavin RE. Best evidence synthesis: an intelligent alternative to meta-
analysis. J Clin Epidemiol 1995;48:9-18.
37. Treadwell JR, Singh S, Talati R, McPheeters ML, Reston JT. A
framework for best evidence approaches can improve the trans-
parency of systematic reviews. J Clin Epidemiol 2012;65:1159-62.
38. Trinh K. Summaries and recommendations of the global impression
method. J Acupunct Tuina Sci 2009;7:296-302.
39. Rodrigues BG, Cader SA, Torres NV, de Oliveira EM, Dantas EH.
Pilates method in personal autonomy, static balance and quality of
life of elderly females. J Bodyw Mov Ther 2010;14:195-202.
40. Altan L, Korkmaz N, Bingol U, Gunay B. Effect of Pilates training
on people with fibromyalgia syndrome: a pilot study. Arch Phys Med
Rehabil 2009;90:1983-8.
41. Alves de Araujo ME, Bezerra da Silva E, Bragade Mello D,
Cader SA, Shiguemi Inoue Salgado A, Dantas EH. The effectiveness
of the Pilates method: reducing the degree of non-structural scoliosis,
and improving flexibility and pain in female college students. J
Bodyw Mov Ther 2012;16:191-8.
42. Cakmakci O. The effect of 8 week Pilates exercise on body
composition in obese women. Coll Antropol 2011;35:1045-50.
43. Marinda F, Magda G, Ina S, Brandon S, Abel T, Ter Goon D. Effects
of a mat Pilates program on cardiometabolic parameters in elderly
women. Pak J Med Sci 2013;29:500-4.
44. Martin E, Battaglini C, Groff D, Naumann F. Improving muscular
endurance with the MVe Fitness Chair in breast cancer survivors: a
feasibility and efficacy study. J Sci Med Sport 2013;16:372-6.
45. Plachy JK, Kovach MV, Bognar J. Improving flexibility and endur-
ance of elderly women through a six-month training programme.
Hum Mov 2012;13:22-7.
46. Fourie M, Gildenhuys GM, Shaw I, Shaw BS, Toriola AL, Goon DT.
Effects of a mat Pilates programme on body composition in elderly
women. West Indian Med J 2013;62:524-8.
47. Ashrafinia F, Mirmohammadali M, Rajabi H, et al. The effects of
Pilates exercise on sleep quality in postpartum women. J Bodyw Mov
Ther 2014;18:190-9.
48. Lee CH, Hyun J, Kim SG. Influence of Pilates mat and apparatus
exercises on pain and balance of businesswomen with chronic low
back pain. J Phys Ther Sci 2014;26:475-7.
Pilates method for women’s health 2241
www.archives-pmr.org

8/18/2019 Pilates Method for Women’s Health
http://slidepdf.com/reader/full/pilates-method-for-womens-health 12/12
49. Gildenhuys GM, Fourie M, Shaw I, Shaw BS, Toriola AL,
Witthuhn J. Evaluation of Pilates training on agility, functional
mobility and cardiorespiratory fitness in elderly women. Afr J Phys
Health Educ Recreation Dance 2013;19:505-12.
50. Kaptchuk TJ, Kelley JM, Conboy LA, et al. Components of placebo
effect: randomised controlled trial in patients with irritable bowel
syndrome. BMJ 2008;336:999-1003.
51. Horlings CG, van Engelen BG, Allum JH, Bloem BR. A weak bal-
ance: the contribution of muscle weakness to postural instability and
falls. Nat Clin Pract Neurol 2008;4:504-15.52. Boguszewski D, Monika, Adamczyk J, Ochal A. The role of Pilates
and aquafitness exercises in sustaining the health and fitness of
elderly women. Sport Sci Rev 2012;21:127-38.
53. Fourie M, Gildenhuys GM, Shaw I, Shaw BS, Toriola AL, Goon DT.
Effects of mat Pilates programme on muscular strength and endur-
ance in elderly women. Afr J Phys Health Educ Recreation Dance
2012;18:299-307.
54. Jakicic JM, Clark K, Coleman E, et al. American College of Sports
Medicine position stand. Appropriate intervention strategies for
weight loss and prevention of weight regain for adults. Med Sci
Sports Exerc 2001;33:2145-56.
55. Sekendiz B, Altun O, Korkusuz F, Akin S. Effects of Pilates exercise
on trunk strength, endurance and flexibility in sedentary adult fe-
males. J Bodyw Mov Ther 2007;11:318-26.
56. Rogers K, Gibson AL. Eight-week traditional mat Pilates training-
program effects on adult fitness characteristics. Res Q Exerc Sport
2009;80:569-74.
57. Kloubec JA. Pilates for improvement of muscle endurance, flexi-
bility, balance, and posture. J Strength Cond Res 2010;24:661-7 .
58. Balogh A. Pilates and pregnancy. RCM Midwives 2005;8:220-2.
59. Robinson L. Pilates in pregnancy: the body control method. PractMidwife 2007;10:24-6.
60. Pia SD. Pilates and pregnancy: programming ideas and exercise
guidelines. IDEA Fitness J 2007;4:89-92.
61. Artal R, O’Toole M. Guidelines of the American College of Obste-
tricians and Gynecologists for exercise during pregnancy and the
postpartum period. Br J Sports Med 2003;37:6-12.
62. ACOG Committee opinion. Number 267, January 2002: exercise during
pregnancy and the postpartum period. Obstet Gynecol 2002;99:171-3.
63. Pate RR, Pratt M, Blair SN, et al. A recommendation from the
Centers for Disease Control and Prevention and the American Col-
lege of Sports Medicine. JAMA 1995;273:402-7.
2242 M. Mazzarino et al
www.archives-pmr.org

















![[T] The effect of Pilates method on elderly flexibility · Guimarães ACA, de Azevedo SF, ... Pilates method presented a lower flexibility degree, ... exercises for each session,](https://img.dokumen.tips/doc/110x75/5b14e1447f8b9a54488ca053/t-the-effect-of-pilates-method-on-elderly-guimaraes-aca-de-azevedo-sf-.jpg)











![[fisioterapia] Pilates Ejercicios Del Metodo Pilates (Español)](https://img.dokumen.tips/doc/110x75/5571fc664979599169972c58/fisioterapia-pilates-ejercicios-del-metodo-pilates-espanol.jpg)