Embed Size (px)
Citation preview

Jeffrey W. Olin, D.O., F.A.C.C., F.A.H.A.
Professor of Medicine (Cardiology)
Director of Vascular Medicine &
the Vascular Diagnostic Laboratory
Icahn School of Medicine at Mount Sinai
Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options

Peripheral Artery Disease (PAD)
• The presence of a stenosis or occlusion in the aorta or arteries of the limbs
• Usually caused by atherosclerosis
• Associated with an increased risk of death, myocardial infarction, and stroke
• May impair walking or cause critical limb ischemia
• The global burden of PAD is estimated to be 202 million persons

10%
40%50%
Classic Claudication Atypical Leg Pain Asymptomatic
Some Not So Well Known Facts
• Only 8%–10% of patients with
peripheral arterial disease (PAD)
have “classic” claudication
• ~40% of patients with PAD have
“atypical” leg symptoms
• ~50% of patients with PAD are
asymptomatic with regard to the
leg

ABI and Mortality
Ankle Brachial Index Collaboration. JAMA 2008.
Association of ABI with all-cause mortality in a meta-analysis of 16 cohort studies including 48,294 subjects and 480,325 person-years of follow-up.

Diehm, C. et al. Circulation 2009;120:2053-2061
The German Epidemiological Trial on ABI Study: Event-free Survival by PAD status
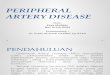
Reinecke et al. Eur Heart J 2015;36:932-938
Death (n= 10,880) Amputation (n= 7,825)
Contemporary PAD Outcomes in Germany
n = 41,882 PAD patients hospitalized during 2009 – 2011
Followed until 2013, (mean 1144 days)

Cardiovascular Risk Increases
With Decreases in ABI
>1.1 1.1–1.01 1.0–0.91 0.9–0.71 <0.7
ABI
CH
D E
ven
t O
utc
om
es*
per Y
ear (
%)
0
1
2
3
4
5-year risk:
10%
5-year risk:
19%
Framingham “High Risk” = 20% at 10 years Every patient with PAD is at “very high risk”
PAD *Fatal or nonfatal MI
2%
3.8%
1.4%
Leng GC et al. Brit Med J. 1996;313:1440-1444.
0
1
2
0
1
3
0
1
0
2
1
0
3
2
1
0
4
3
2
1
0
3.8%
2%
3.8%

The Peripheral Artery Disease Prescription
Olin JW et al. J Am Coll Cardiol 2016, In Press.

• 7458 eligible participants aged >40 years
• Prevalence of PAD is 5.9%, or 7.1 million US adults
with PAD – Statin use 30.5%
– ACE/ARB use 24.9%
– Aspirin use 35.8%
• Among patients with PAD (and no other clinical
cardiovascular disease), use of multiple preventive
therapy was associated with a 65% lower all-cause
mortality (HR 0.35, P=0.02)
Pande RL et al. Circulation. 2011;124:17-23.
National Health and Nutrition Examination
Study, 1999–2004
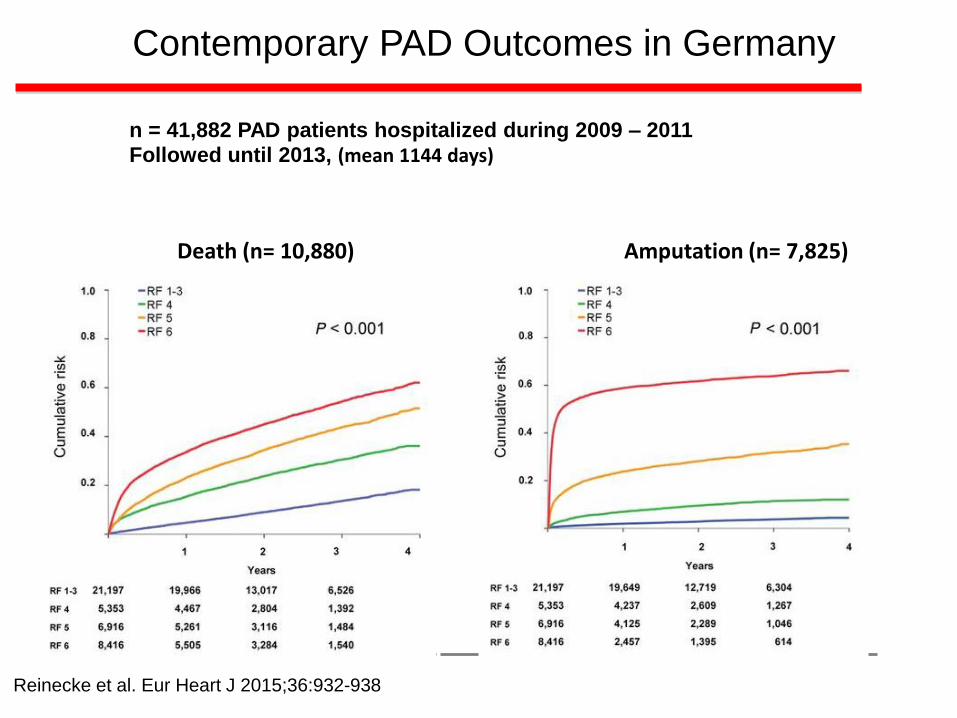
Armstrong E et al. J Am Heart Assoc 2014;3:e000697.
Adherence to Guideline-Recommended Medical Therapies
and Outcomes in Peripheral Artery Disease.
Major Adverse CV Events Major Adverse Limb Events
A total of 237 (32%) patients met all four guideline-recommended therapies
(antiplatelet, statin, ACE, smoking cessation)

The Efficacy of Statin Therapy The Heart Protection Study
Heart Protection Study Collaborative Group. Lancet. 2002;360:7-22.
Previous MI 23.5 29.4
Other CHD 18.9 24.2
No prior CHD or CBV disease 18.7 23.6
Diabetes 13.8 18.6
All patients 19.8 25.2
1.2 1.4 0.6 0.4
24% Reduction
(P<.0001)
Existing disease
Statin Control
Incidence of events
(n=10,269) (n=10,267) Statin favored Placebo
Risk vs Control
PAD 24.7 30.5
0.8 1.0

ACE Inhibitors in PAD
The HOPE Trial
HOPE Study Investigators. N Engl J Med. 2000;342:145-153.
History of CAD 7477
No history of CAD 1820
Prior MI 4892
No prior MI 4405
CBV disease 1013
No CBV disease 8284
Peripheral vascular disease 4051
No peripheral vascular disease 5246
Microalbuminuria 1956
No microalbuminuria 7341
No. of Patients
Reduced Increased
Relative risk in ramipril group
0.6 0.8 1.0 1.2

Collagen
Thrombin
TXA2
ADP
TXA2
ADP Phosphodiesterase
ADP
(fibrinogen
receptor)
GP IIb/IIIa Activation
COX
Clopidogrel bisulfate
Ticlopidine HCl
ASA
Dipyridamole
cAMP
Mechanisms of Action of Oral Antiplatelet Therapies
Schafer AI. Am J Med. 1996;101:199
Ticagrelor- reversible P2Y12 inhibitor
Vorapaxar

-40 -30 -20 -10 0 10 20 30 40
Aspirin better Clopidogrel better
CAPRIE
Stroke
MI
PAD
All patients
• 3867 (20.2%) had diabetes
• ~ 1/3 PAD patients had diabetes
CAPRIE Steering Committee. Lancet. 1996;348:1329-1339.
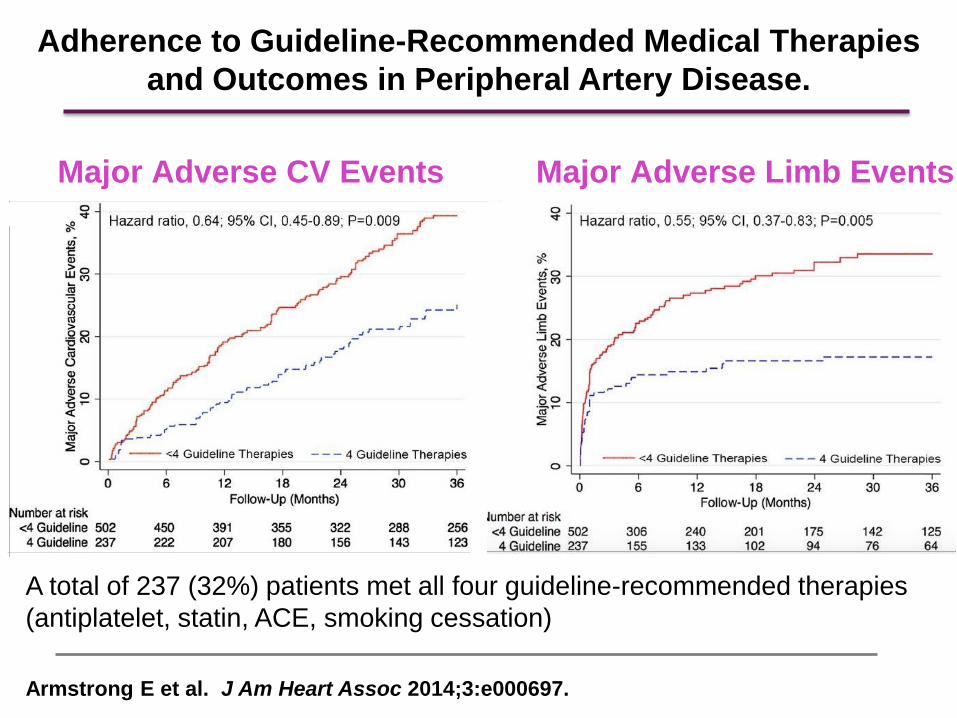
Population RRR (95% CI) P
Qualifying CAD, CVD, or PAD 0.88 (0.77, 0.998) .046
(n=12,153)
Multiple risk factors 1.20 (0.91, 1.59) .20
(n=3,284)
Overall population* 0.93 (0.83, 1.05) .22
(N=15,603)
CHARISMA: Clopidogrel plus Aspirin vs. Aspirin Alone on MI, Stroke, or CV Death
0.6 0.8 1.4 1.2
Clopidogrel better Placebo better
1.6 0.4
Bhatt DL, Fox KA, Hacke W, et al. New England Journal of Medicine, 2006

CHARISMA: Outcomes in the PAD Cohort
P Cacoub et al., Euopean Heart Jounal, 2009

EUCLID Study Design
Primary Endpoint: cardiovascular death, myocardial infarction, or ischemic stroke
Inclusion Criteria: Symptomatic PAD AND
one of the following:
A.ABI ≤0.80 at Visit 1
≤0.85 at Visit 2
OR
B.Prior lower extremity
revascularization > 30
days
Key Exclusion Criteria: Poor
metabolizer for CYP2C19
Patients requiring dual anti-platelet therapy
Patients with Symptomatic PAD
Ticagrelor 90 mg bid
Clopidogrel 75 mg od
N=11,500
Follow-Up Visits 2, 6, 12 Months; Every 6 months after 1st year
Telephone visits @ a 3 month interval between regular visits
Duration: approximately 18 month recruitment and 18 month follow up
1:1
Double-blind
Double-dummy

Vorapaxar- TRA2P Timi 50
Morrow D et al. N Engl J Med 2012.

0%
2%
4%
6%
8%
10%
12%
14%
0 180 360 540 720 900 1080
Effect of Vorapaxar on Cardiovascular
Events in PAD Cohort
CV Death, MI, or Stroke
11.3%
11.9%
Hazard Ratio 0.94;
95% CI (0.78 - 1.14)
p = 0.53
Placebo
Vorapaxar
N = 3767
Days from randomization
P-interaction:
PAD vs. MI/CVA = 0.35
PAD vs. MI cohort = 0.16
12
10
8
6
4
2
14
Even
t R
ate
(%
)

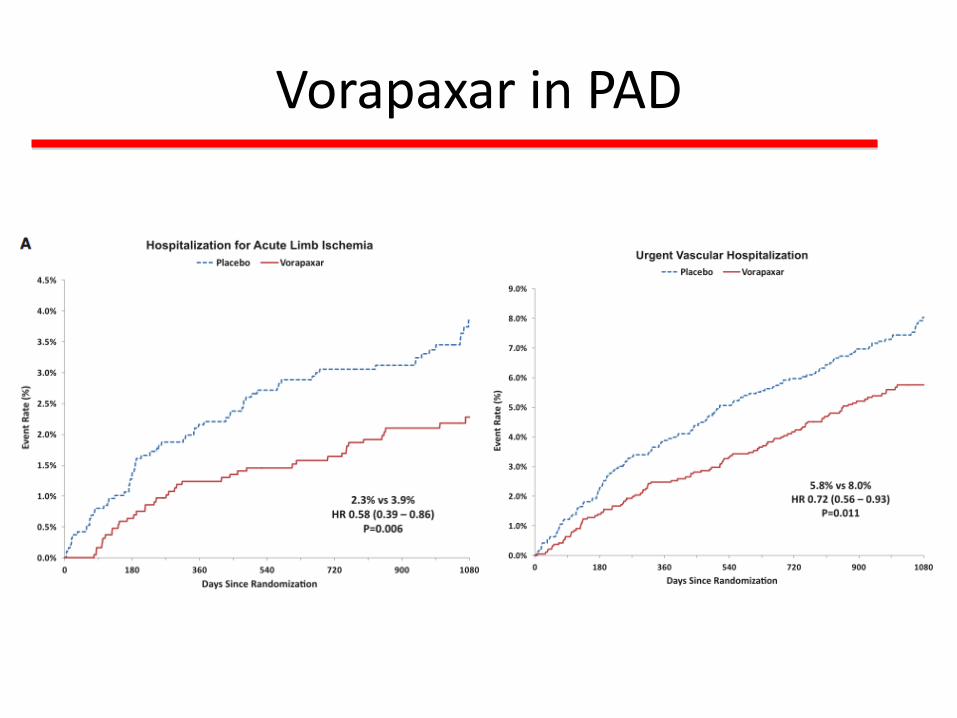
Vorapaxar in PAD


Circulation. 2012;125:130-139

Murphy T P et al. Circulation 2012;125:130-139
CLEVER Primary Endpoint:
Peak Walking Time Secondary Endpoints:
QOL,
Supervised Exercise
Better than Stenting,
P<0.001)
Stenting Better than
Supervised Exercise

The ERASE Trial Endovascular Revascularization and Supervised Exercise
vs. Supervised Exercise for Intermittent Claudication
Fahkry et al., JAMA. 2015;314(18):1936-1944

The ERASE Trial Endovascular Revascularization and Supervised Exercise
vs. Supervised Exercise for Intermittent Claudication
Fahkry et al., JAMA. 2015;314(18):1936-1944


Claudication Treatment—Exercise
• Supervised exercise training should be the
initial treatment
–30–45 minute sessions
–3 or more times per week
–At least 12 weeks
• Value of unsupervised exercise programs
is not well established
Rooke T et al. J Am Coll Cardiol. 2013;61:1555-70

Pande R et al. Vascular Medicine 2010;15:181-188.
Double-Blind, Randomized Controlled Trials of
Cilostazol In Patients with Intermittent Claudication

Medical Therapy (all patients)
• Detailed written and verbal (28 page booklet):
– Risk factors
– Management
– Structured training advice
• Perform submaximal walk exercise sessions for at least 30 min/day
at least 3 times/week. Nordic pole use was encouraged.
– This program was evaluated and reinforced at 3 and 6 months.
• Aspirin or clopidogrel, statin therapy and cilostazol 100mg twice daily
in all patients
• Additional risk factors (hypertension, diabetes, smoking) managed
according to national guidelines by primary doctor.
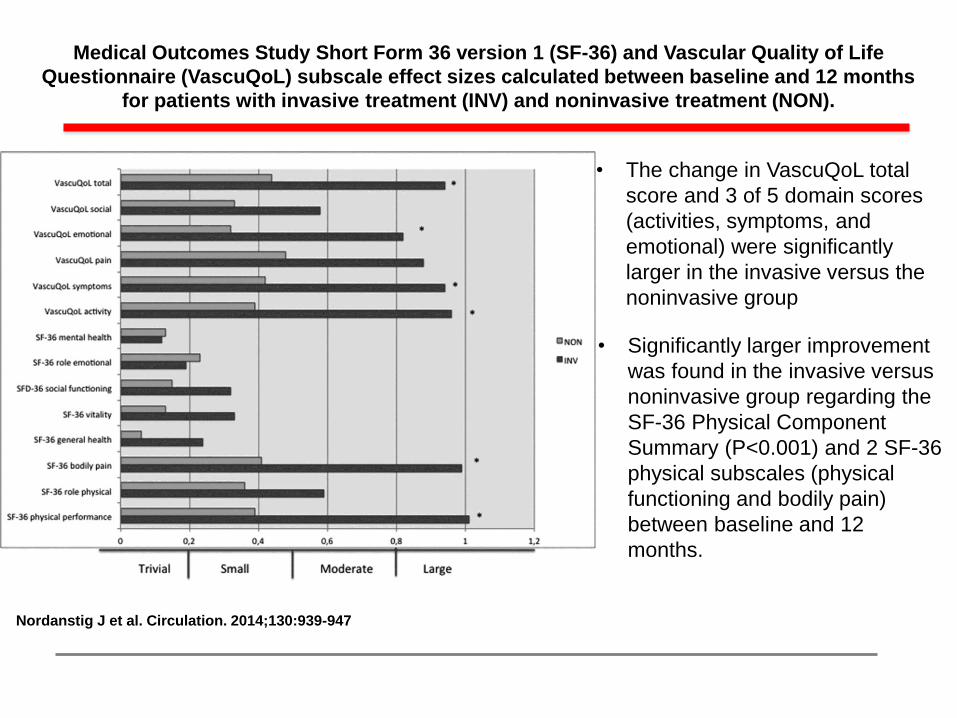
Medical Outcomes Study Short Form 36 version 1 (SF-36) and Vascular Quality of Life
Questionnaire (VascuQoL) subscale effect sizes calculated between baseline and 12 months
for patients with invasive treatment (INV) and noninvasive treatment (NON).
Nordanstig J et al. Circulation. 2014;130:939-947
• Significantly larger improvement
was found in the invasive versus
noninvasive group regarding the
SF-36 Physical Component
Summary (P<0.001) and 2 SF-36
physical subscales (physical
functioning and bodily pain)
between baseline and 12
months.
• The change in VascuQoL total
score and 3 of 5 domain scores
(activities, symptoms, and
emotional) were significantly
larger in the invasive versus the
noninvasive group
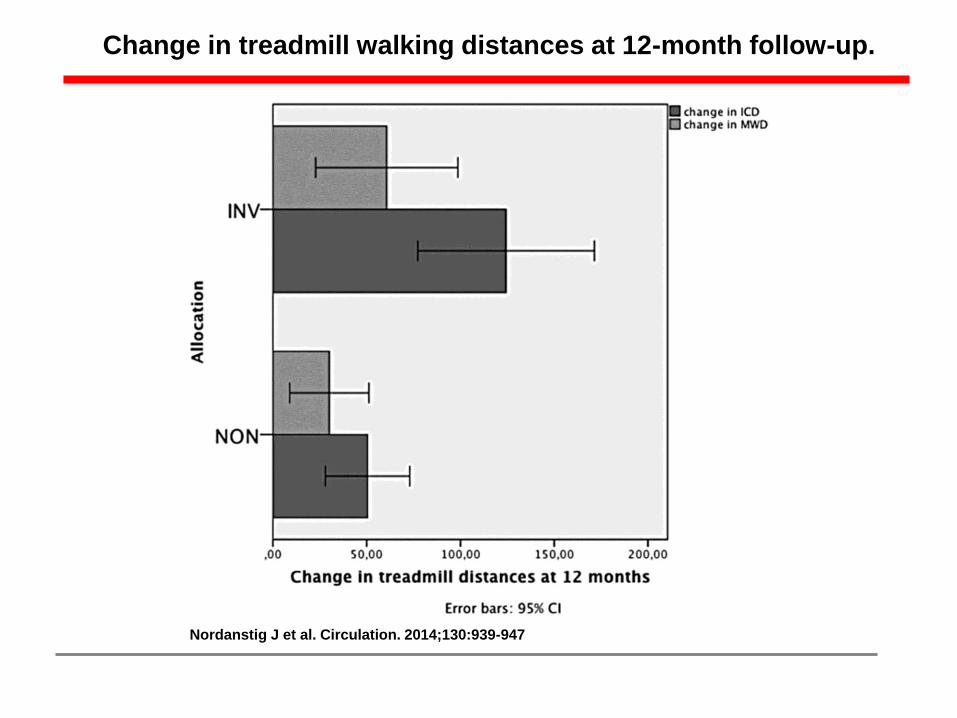
Change in treadmill walking distances at 12-month follow-up.
Nordanstig J et al. Circulation. 2014;130:939-947
Guiding Principles for Revascularization
in Patients With PAD
Patients with PAD should have their feet inspected during every office
visit. This is the single most important thing you can do to prevent
amputations.
Olin JW, Sealove B. Mayo Clin Proc. 2010;85(7):678-692

Indications for Revascularization
• Iliac disease
– Hip, thigh, or buttock claudication
– Reduced or absent femoral pulses
– Imaging to identify iliac disease and stenting
• Infrainguinal disease
– Trial of medical therapy for 4–6 months:
–Structured exercise program
–Cilostazol
– If failure, additional imaging to define anatomy and, if
feasible, stent placement
– If short segment SFA disease is identified, can proceed
directly with stenting

Indications for Intervention in Patients With PAD
• Life-style disabling claudication
• Rest pain
• Ischemic ulcers
interfering



Case—A 62-Year-Old Diabetic Man
• ½ block calf claudication, Lt > Rt
• Heavy smoker
• ABI 0.41 on the right and 0.43 on the left
• Femoral pulse 1+ bilaterally
• Popliteal, DP, and PT=0





RESILIENT TRIAL
Nitinol Stent Implantation vs. Balloon
Angioplasty for Superficial Femoral Artery Disease
Schillinger M et al. N Engl J Med 2006;354:1879-88. d
6 month 10 Endpoint (Angio) 12 month 20 Endpoint (Duplex)
Treatment of superficial-femoral-artery disease by primary implantation of a self-
expanding nitinol stent yielded results that were superior to those with the currently
recommended approach of balloon angioplasty with optional secondary stenting.

Rosenfield K et al. N Engl J Med 2015;373:145-153
LEVANT 2 Trial Efficacy of Paclitaxel-Coated Balloon for Femoropopliteal Artery Disease
476 patients with
symptomatic femoral-
popliteal disease were
randomized in a 2:1
manner to angioplasty
with a paclitaxel-coated
balloon or to standard
angioplasty.
The primary efficacy end
point was primary
patency of the target
lesion at 12 months
(defined as freedom from
binary restenosis or from
the need for target-lesion
revascularization).

JAMA Surgery Oct 2014

• NHLBI-sponsored prospective, randomized, multicenter,
open label superiority trial
• 2,100 patients at 120 clinical sites in United States and Canada
• 4-year trial extending from 2014-2017, with each patient having
minimum of 2 year follow-up

The Peripheral Artery Disease Prescription
Olin JW et al. J Am Coll Cardiol 2016, In Press.