Embed Size (px)
Citation preview

Peripheral Arterial Disease (PAD):
Diagnosis and Management
Peter J Mackrell, MD
Chief: Division Vascular Surgery
Co-Director: Vascular Lab
Sinai Hospital

WHY?
• Affects approximately 8-12 million Americans
• If positive risk factors prevalence of 29%
• Patients with PAD and no known CAD have 30%
risk of MI, stroke, vascular death over 5 years
Why?
• Often asymptomatic
• Early identification can save lives and limbs
• Poorly taught in all specialties
• Crosses many specialties
Who
• Elderly
• CAD
• Smokers
• Diabetics
• ESRD
• High Cholesterol
• Family history
• HTN
• Male

Anatomy

Leg Pain Differential
• Vascular
-Arterial
-Venous
• Musculoskeletal
-arthritis
• Neurogenic
-spinal stenosis
-DJD

Symptoms
None Claudication
-pain calf,buttock
-ambulation
-consistent
Limb Threatening Ischemia
-rest pain
-ulcer
-gangrene

Claudication
Pain
-with walking-hills versus flat
-calves/thighs/buttocks
-consistent
-reproducible
-resolved with standing vs sitting
-no pain when recumbent

Rest Pain
Pain
-Often at night/lying flat
-More distal pain/feet
-Relieved by gravity/walking

Evaluation
• Inspection-hair
-capillary refill
-cyanosis/rubor
-edema
-nails
-foot architecture/callouses
-cellulitis
-ulcers
-gangrene

Palpation
Sitting
Supine
PE Findings Suggestive of PVD
• Decreased Pulses
-Femoral
-Popliteal
-Dorsalis Pedis
-Posterior Tibial
• Muscle atrophy/hair loss/nail changes
• Dependent Rubor
• Ulcers/Gangrene

Indirect Physiologic Tests consists of:
• Pressure assessment– ABI and/or segmental pressures
• ( or) Doppler waveform analysis

Segmental pressure principle
• In a normal individual in a supine position, ankle systolic pressure is ≥ brachial pressure.

The Ankle/Brachial Index
(ABI)
• bilateral ankle pressures divided by the higher brachial pressure

• Dorsalis Pedis– easily compressed
– harder to locate
Doppler Pressure Sites for ABI
• Posterior Tibial• harder to compressharder to compress
• easier to locate
• Posterior Tibial• harder to compressharder to compress
• easier to locate
Essential not to drift off vessel !

Brachial pressure
ABI
Resting ABI values
• > 1.0 = normal (usually)
• < 0.92 = abnormal, – exercise patient if borderline
• < 0.8 = probable claudication
• < 0.5 = multi-level disease or long segment occlusion
• < 0.3 = ischemic rest pain

The bane of pressure measuremements:
• Calcific medial sclerosis
– diabetics – chronic steroid therapy – renal dialysis patients – elderly patients
• Segmental pressures unobtainable or excessively high
• In these patients use toe pressures– >40 mmHg for tissue healing in diabetics– >20 mmHg for tissue healing in non-diabetics

Doppler waveform analysis:Normal lower arterial waveforms
are “triphasic”
Analog, low-cost zero-crossing detector

Doppler Waveform analysis: Interpretation
• Abnormal: • loss of triphasic waveform• dampening of amplitude• slow upstroke
CFA
SFA

ABI Interpretation
ABI
0.92 normal
0.50-0.91 claudication
0.3-0.5 rest pain
<0.3 ulcer/gangrene
Non-compressible
Toe Pressure
>20 mmHg non-diabetic
>40 mmHg diabetic
PE Findings Suggestive of PVD
• Decreased Pulses
-Femoral
-Popliteal
-Dorsalis Pedis
-Posterior Tibial
• Muscle atrophy/hair loss/nail changes
• Dependent Rubor
• Ulcers/Gangrene
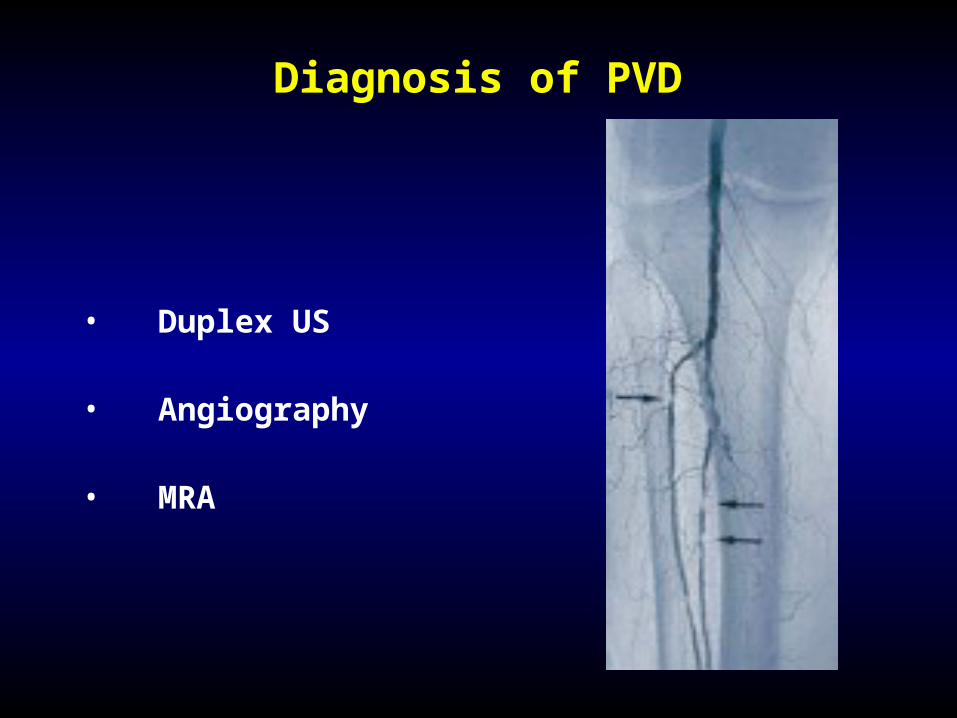
Diagnosis of PVD
• Duplex US
• Angiography
• MRA

Treatment of PVD
• Medical Therapy
•Antiplatelet Tx\
• Statins
• Risk factor Mgt
• Foot Care
-moisturizers
-footware
• STOP SMOKING!!!!
• Walking Program
• Pharmacologic Tx-Pletal

Treatment of PVD
• Medical Therapy
• Open Surgery
• Endovascular Repair

Surgical RevascularizationAorto-iliac ASO
Excellent patency
Operative mortality 3.3%
Peri-op morbidity 8.3%
Meta-analysis - Meta-analysis - DeVriesDeVriesJVS 1997;26:558-69JVS 1997;26:558-69

PTA of Iliac Arteries
AUTHOR TECHNICAL SUCCESS
Colapinto (1986) 78%
Gupta (1993) 78%
Johnston (1987) 82%
Vorwerk (1995) 81% *
Blum (1993) 98% * — 71% in 1st 50 patients
— 93% in 2nd 50 patients

Stenting of Iliac Arteries
• Palmaz 1992 92% (1 yr)
• Sullivan 1997 84% (2 yrs)
AuthorAuthor Date Date Patency Patency

PTA Versus Stents
Limited data
4 yr patency stents = 94%
4 yr patency PTA = 69%
Richter et al Radiology Richter et al Radiology 19911991181 Supplement181 Supplement





AORTO-ILIAC ASOSUMMARY
Focal disease – endovascular therapy
More complex disease
Good risk – surgical revascularization
Poor risk – endovascular

OUTCOME OF THERAPY FOR FEM-POP ASO - CLAUDICATION
Method/indication 5-yr patency
PTA-stenosis 68%
PTA-occlusion 35%
Fem-pop bypass – vein 80%
Fem-pop bypass – AK PTFE 75%
Fem-pop bypass – BK PTFE 65%




Fem-pop and tibialSUMMARY
Focal disease – endovascular therapy
More complex disease
Good risk – surgical revascularization
Poor risk – endovascular
Claudication - open surgery
Tissue Loss - endovascular therapy