Embed Size (px)
Citation preview

bidities, and reduction in the cost oflong-term medical management andtreatment of these issues. Numeroushealthcare professionals make refer-rals to vascular specialists; but due toits symptomatology, referrals aremore often made by primary carephysicians, endocrinologists, cardiol-ogists, and podiatrists.
Peripheral artery disease is a dis-ease of the upper and lower extrem-ities that affects over eight millionpeople in the United States.19 PADis primarily mediated by atheroscle-rotic disease, and may manifest ascramping muscle pain, pain at rest,
Continued on page 178
Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin-uing Medical Education by the Council on Podiatric Medical Education.
You may enroll: 1) on a per issue basis (at $20.00 per topic) or 2) per year, for the special introductory rate of $139 (yousave $61). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the nearfuture, you may be able to submit via the Internet.
If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned credits. You willalso receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test at no additional cost. A listof states currently honoring CPME approved credits is listed on pg. 186. Other than those entities currently accepting CPME-approvedcredit, Podiatry Management cannot guarantee that these CME credits will be acceptable by any state licensing agency, hospital, man-aged care organization or other entity. PMwill, however, use its best efforts to ensure the widest acceptance of this program possible.
This instructional CME program is designed to supplement, NOT replace, existing CME seminars. Thegoal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscripts bynoted authors and researchers. If you have any questions or comments about this program, you can write or call us at: PodiatryManagement, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at [email protected].
Following this article, an answer sheet and full set of instructions are provided (p. 186).—Editor
MARCH 2010 • PODIATRY MANAGEMENTwww.podiatrym.com 177
tected early, appropriate treatmentof PAD can have profound effects ona patient’s care—including preven-
tion of PAD-related complicationsand cardiovascular-related co-mor-
By Vicken Pamoukian, MD andDamien De Collibus, R-PAC
In many situations, the podiatristis in the best position to screenfor and diagnose asymptomatic
disease. Many disease processes maynot be easily elicited on physicalexam, however, and it is often neces-sary to perform less common diag-nostic testing, or refer to a specialist.Peripheral artery disease (PAD) is onesuch disease that may not be readilydiagnosed on physical exam, andmay require further testing either inthe primary care setting, or with avascular specialist. However, if de-
Goals/ObjectivesUpon completion of this ar-
ticle, the reader should:
1) Have a strong under-standing of the pathophysiol-ogy of and risk factors for pe-ripheral artery disease (PAD).
2) Be able to recognize itssigns and symptoms in theclinical setting.
3) Be aware of the non-in-vasive and invasive screeningmodalities available to practi-tioners to verify the diagnosisof PAD.
4) Understand the basic ra-tionale behind surgical andinterventional indications andoptions.
Continuing
Medical Education
Diagnosis of PAD
may also lead
to suspicion
and early diagnosis
of other diseases.
Here’s what to do when thepipes get clogged.
VascularPlumbing 101:Managementof PeripheralArtery Disease
C L I N I C A L I S S U E SC L I N I C A L I S S U E S

made in pharmacology, enhancedtreatments for hyperlipidemia, dia-betes, and anti-platelet therapy toreduce cardiovascular risk have sub-sequently reducedthe risk of PAD-related morbidity.As with any dis-ease process,treatment of PADmust be personal-ized for each pa-tient, and treat-ment options aremuch more var-ied than theyonce were. Manyhospital centersoffer newer treat-ments for PAD,including en-dovascular andhybrid endovas-cular/open surgical treatments, inaddition to conventional open sur-gical revascularizations.
PathogenesisArteries are constructed of three
discrete layers, differentiated by boththeir composition and function. Thetunica intima is the innermost vessel
layer lined entirelyby endothelialcells that serve tofacilitate circula-tion, prevent un-wanted transportof certain materialsoutside of the ves-sel lumen, and reg-ulate function ofsmooth musclecells. The tunicamedia containssmooth musclenecessary for di-rected contractionand relaxation ofthe muscle layer,and subsequentvasoconstrictionand vasodilation,respectively; thislayer providesstructural integrity
and strength to the vessel. The tuni-ca adventitia is the thin, outermostlayer of loose connective tissue thatgives rise to the blood supply for thevessel itself—the vasa vasorum.10
Atherosclerotic disease involvesthe potential space between the tuni-
ca intima and the surrounding tuni-ca media. Therefore, prevention ofatherosclerotic-related disease re-quires prevention of migration out-
side of the tunicaintima, and treat-ment involves re-pair of the plaqueformed at the siteof this migration.
Atherosclero-sis describes a pro-cess in which ec-centric lesions de-velop and progressto become flow-limiting, or maynarrow the vessellumen enoughthat it becomesthrombosed and,at times, fully oc-cluded. The pro-
cess itself may be characterized infive phases. Phase 1 involves deposi-tion of macrophage-derived foamcells, or smooth muscle cells con-taining lipid droplets or extracellulardeposits, resulting in a small, usuallyeccentric lesion. Phase 2 involvesdestabilization of the initial plaque,now consisting primarily of extracel-lular lipids and fibrous tissue. Phase3 and 4 plaques progress from phase2 to include a partially or fully occlu-sive mural thrombus in the lumen.Finally, fibrosis of the lesion isdemonstrated in phase 5.10 In addi-tion to smooth muscle cells, the fi-brotic cap formed in phase 5 also en-traps inflammatory cells and a lipid-rich core of necrotic debris withinthe plaque, which can lead to chron-ic vessel inflammation and vasocon-striction. (Zhou)
Atherosclerotic disease normallyaffects larger vessels at their bifurca-tions, and other areas where turbu-lent blood flow and low sheer stressare common. Most commonly, arteri-al plaque formation develops in threespecific sites in the lower extremityvasculature, although lesions couldpotentially develop anywhere vascu-lar injury and vessel wall inflamma-tion occur. The three sites, first char-acterized by De Bakey, are the 1. aor-tic bifurcation, 2. tibial trifurcation,and 3. superficial femoral artery atthe adductor hiatus; the disease oftenspares the internal iliac, profundafemoral, and peroneal arteries.
Continued on page 179
178 www.podiatrym.comPODIATRY MANAGEMENT • MARCH 2010
Plumbing...
tissue loss and gangrene, ormay exist entirely symptom-
free. Medical costs in the inpatientand outpatient setting are higherfor patients with PAD, and evenhigher in the setting of arterial anddiabetic ulcers.
In a meta-analysis performed atthe Diabetes Center in Beijing,China, the average medical cost ofhospitalized patients with diabetesand PAD-related foot problems wasmarkedly higher than with patientshaving diabetes alone. Subsets of pa-tients diagnosed with diabetes morethan 20 years prior, or subsets in-cluding laborers and retired workers,demonstrated obviously highermedical costs than average. As ex-pected, patients with infection, is-chemic changes in the feet, or gan-grene of the feet had a longer hospi-tal stay with subsequently highermedical costs.23
Diagnosis of PAD may also leadto suspicion and early diagnosis ofother diseases. Patients with a histo-ry of PAD with claudication have a2.5 times higher risk of experiencinga cardiac event than age-matchedsubjects withoutclaudication. Sim-ilarly, approxi-mately 30% of pa-tients undergoingmajor peripheralbypass surgeriesdemonstrate se-vere triple-vesselcoronary diseaseon pre-operativecardiac catheteri-zation.2 A near30% correlationbetween carotidstenosis and pe-ripheral arterydisease has alsobeen documentedby numerousmeta-analyses.
Surveillance isquickly becomingmore readilyavailable to all practitioners, someopting to maintain on-site resourcesfor performing non-invasive vascu-lar screening, such as ankle-brachialindex measurements, pulse-volumerecording, or peripheral arterial du-plex studies. With the advances
Contin
uing
Medica
l Edu
catio
n
Type 3 lesions
constitute the
remaining 60-70%
of lesions, and
demonstrate multi-
level disease of
aortoiliac,
femoral, popliteal,
and tibial vessels.
The tunica intima
is the innermost vessel
layer lined entirely
by endothelial cells
that serve to facilitate
circulation, prevent
unwanted transport
of certain materials
outside of the vessel
lumen, and regulate
function of smooth
muscle cells.

MARCH 2010 • PODIATRY MANAGEMENTwww.podiatrym.com 179
completely resolved with rest. In onestudy, a rapid decline in lower ex-tremity strength and functional per-formance was seen over a six-yearperiod in women with PAD, al-though the same decline was notseen in men with PAD over the sameperiod. (Herman)
Symptoms are directly related tothe distribution of diseased vessels inan individual—for instance, in thecase of iliac artery stenosis, patientsmay complain of bilateral hip andbuttock claudication and erectiledysfunction. These symptoms associ-ated with absent femoral pulses de-scribes Leriche syndrome, and maybe an alarm that disease is presentelsewhere in the body.2 Symptomsthat do not appear to correlate withactual sites of disease may be at-tributed to other causes. Therefore, itis important to differentiate symp-
toms of claudication from neuro-pathic or radicular pain that origi-nates from the lumbosacral nerveroots, or is isolated to the feet.
Ischemic rest pain occurs in theabsence of exercise or exertion, andis normally isolated to the dorsumof the foot overlying the metatarsalheads. This pain can be elicited withelevation of the extremity or evenlying supine, but can be relieved bymoving the legs to a dependent po-sition, massaging the affected area,or initiating activity to promotepedal circulation. Potential conse-quences of chronic lower extremityischemia include gangrene and softtissue loss, and infection. These con-ditions are imminent when rest painis present. Soft tissue loss can in-clude arterial and diabetic ulcers,
Lesion TypesDe Bakey went on to classify le-
sions as Types 1, 2, and 3 lesions.Seen in 10-15% of atheroscleroticlesions, type 1 lesions are found inaortoiliac distribution, most com-monly in patients with smokinghistories and hyperlipidemia. Type2 lesions account for approximately25%, and involve aortoiliac and ex-ternal iliac vessels. Type 3 lesionsconstitute the remaining 60-70% oflesions, and demonstrate multi-leveldisease of aortoiliac, femoral,popliteal, and tibial vessels. Types 2and 3 are seen more often withmore than two PAD risk factors.2
Commonly, the risk factors associat-ed with atherosclerotic disease is in-creasing age, hypercholesterolemia,diabetes mellitus, smoking, positivefamily history, hypertension, seden-tary lifestyle, and obesity. Elevatedserum marker levels of lipoproteinA, homocysteine, C-reactive protein(CRP), vascular endothelial growthfactor (VEGF), and homocystein-uria.21,26
In the peripheral arteries, nar-rowed vessels can lead to symptomsdue not only to the degree of nar-rowing within the vessel, but also tothe functional limitations they poseto blood flow and velocity. Whenblood velocity through the vessel isimpeded, blood volume reachingmuscle tissue is reduced, and canimpair normal aerobic metabolismof the muscle, more evident duringtimes of high oxygen demand, suchas during exercise and strenuousphysical activity. Oxygen-deprivedmuscle will revert to anaerobic res-piration and metabolism duringtimes of exertion, and can lead tosymptoms of cramping pain in theshort-term.
SymptomatologyPatients with PAD can present
with a multitude of symptoms,sometimes seeming unrelated. Theymay disclose a history of impotence,lower extremity claudication withexertion, rest pain, gangrene or tis-sue loss. When patients describeclaudication, they should be describ-ing reproducible pain, numbness, orweakness predominantly in thecalves, thighs, or buttocks, elicitedwith exertion of the extremities,
Plumbing... and may progress to in-volve underlying bone andjoints, leading to osteomyelitisor septic arthritis if the pe-riostium or joint space is compro-mised, respectively.
UlcersUlcers of the skin and soft tissue
can be characterized by their under-lying pathology. Venous stasis ulcersdevelop in areas where chronicedema results in chronic inflamma-tion, deposition of avascular materialunder the skin, skin atrophy, andsubsequent skin break-through. Arte-rial and diabetic ulcers result frompoor circulation and oxygen deliveryto soft tissue, but present differentlyfrom each other, in location andquality. Arterial ulcers are normallypainful, well-circumscribed lesionslocated over the extensor surface ofjoints, commonly over the interpha-langeal joints, or at pressure points—at the plantar surface of themetatarsal heads, or the heels, for in-stance. Arterial ulcers may be treatedwith conservative therapy andwound care for 6-12 weeks beforerevascularization should be attempt-ed. If ulcers worsen despite appropri-ate conservative therapy, percuta-neous or surgical revascularizationshould not be delayed. Diabetic ul-cers may develop in the presence orabsence of PAD, and most will re-solve with improvement in skin hy-giene, glycemic control, and dailydebridement regimens. Patients withdiabetic ulcers and underlying PADor peripheral artery occlusive disease(PAOD) should be assessed for revas-cularization procedures to expeditehealing, if no improvement is seenwith conservative treatment.22
Screening for PADScreening for PAD can and
should be performed well before apatient encounters a vascular sur-geon, based on populations demon-strating multiple risk factors for thedisease. It can involve a routinephysical exam, questionnaires target-ing PAD and PAD-related diseases, orcan include more selective and spe-cific testing, including ankle-brachialindex and arterial Doppler studies, ormore invasive imaging includingcomputed tomographic (CT) or mag-netic resonance imaging (MRI) stud-
Continued on page 180
Continuing
Medical Education
Patients should be
instructed to refrain
from smoking
immediately prior to
arterial studies, as
nicotine can cause
vasoconstriction in the
upper and lower
extremity vessels.

and non-palpable pulses, if a hand-held Doppler is available.
Non-invasive ScreeningMethods
Non-invasive testing can oftenvalidate concerns of PAD after a clin-ical history and physical is per-
formed. The ankle-brachial index(ABI) measure-ment is a compari-son of occlusivepressures of theupper and lowerextremities used tocalculate a ratio.In the absence ofs i g n i f i c a n tatherosclerotic dis-ease, the externalapplied pressurerequired to ob-struct flow in theankle and brachialarteries should benearly equal,thereby generatinga ratio of approxi-mately 1.0 (accept-
ed range for normal is 0.9-1.1); anABI 0.7—>0.9 is associated with mildarterial insufficiency, can still presentwith palpable pulses, but may beasymptomatic; an ABI 0.4—>0.7 isassociated with moderate arterial in-sufficiency and commonly presentswith claudication; an ABI <0.4 oftenpresents withnon-palpable puls-es, rest pain, andulcers, and is asso-ciated with severearterial insuffi-ciency.
Toe brachialindices (TBI) maybe useful in deter-mining the extentof disease whentibial vessels arecalcified and non-compliant, and anABI is unattain-able, or inaccurate (usually falsely el-evated due to calcification and non-compressibility of the vessel). Suchan elevation in ABI may be sec-ondary to chronic diabetes mellitusor renal failure. In populations ofnew hemodialysis patients, ultra-sonography results of the lower ex-tremities were correlated to ABI re-
sults to assess for PAD, regardless ofsigns or symptoms of ischemia. Thepresence of PAD was noted when sig-nificant stenosis or obstruction oflower limb arteries was seen on ultra-sound. Of this population, 59.3%showed PAD on ultrasound, but only22.2% of the population had anABI<0.9.15
While ABI measurements can besensitive and diagnostic, PAD maybe missed in some patients, and ad-ditional screening methods may benecessary to make the diagnosis ofPAD. Follow-up testing with ABImay be done at scheduled intervalsto monitor the progress of disease.Often, ABI testing is performed incorrelation with pulse volumerecordings, which qualitatively de-scribe vessel compliance at multiplelevels of the lower extremities.
Like most non-invasive testing,ABI and TBI testing can be done inmost practitioner settings, and doesnot always need to be performed bya vascular specialist. In many cases,ABI testing can be performed in fiveminutes, on average, with some ad-ditional time to effectively prepareand educate the patient for the test.19
Arterial duplex testing screensfor PAD, using sound waves that re-flect off a column of moving blood,in order to measure absolute veloci-ty and velocity gradients. Often, ar-terial duplex is performed withDoppler testing, to identify areas of
narrowed lumenwithin the vessel.Such testing is ef-fective in screen-ing patients to de-termine the pres-ence of anystenotic or flow-limiting lesions inthe aorta or lowerextremity vessels,based on abruptchanges in bloodflow velocity; ve-locity gradientscan translate to
estimate degree of stenosis and per-cent of luminal occlusion.
No special preparation is neces-sary for testing, but patients shouldbe instructed to refrain from smok-ing immediately prior to the study,as nicotine can cause vasoconstric-tion in the upper and lower extremi-
Continued on page 181
180 www.podiatrym.comPODIATRY MANAGEMENT • MARCH 2010
Plumbing...
ies, as will be discussed later.On interview, all practitioners
should be able to elicit a history ofPAD or risk factors for the disease, in-cluding: symptoms of calf claudica-tion or pain in the foot, history of ul-cers, recurrent in-fection, or gan-grene of the feetor legs, documen-tation of andtreatment for re-lated diseases, andprevious surgeriesor procedures in-volving the lowerextremities.
On physicalexam, thereshould be a thor-ough evaluationof the lower ex-tremities and feet,assessing skincolor for rubor,pallor, or mot-tling, noting thepresence of any ir-regular lesions, muscle atrophy, andhair distribution over the legs. Size,location, and appearance of ulcersand areas of gangrene should be doc-umented, to help ascertain locationof arterial disease, and to monitorprogress made in wound healingthroughout the treatment course.Extremities should be felt for temper-ature, as arterial insufficiency couldmanifest as a cool extremity, referredto in the acute setting as a “coldfoot.”
A thorough lower extremity pe-ripheral pulse exam can suggest boththe location and severity of occlusivearterial lesions. For instance, iliac oc-clusive disease may be suggested bythe absence of an ipsilateral femoralpulse; superficial femoral artery (SFA)occlusion may be suggested when apopliteal pulse is weak or absent, orif an abnormally bounding femoralpulse is noted, creating a “waterhammer” effect in the vessel; absentdorsalis (DP) or posterior tibial (PT)pulses may allude to anterior or pos-terior tibial artery occlusion, respec-tively. The practitioner should assessthe quality and location of all palpa-ble pulses making bilateral compar-isons, noting absent pulses, and dis-tinguishing between Dopplerable
Contin
uing
Medica
l Edu
catio
n
Pletal (cilostazol)—
increases calcium-
mediated vasodilation
and inhibits platelet
aggregation via
phosphodiesterase III
(PDE-III) inhibition.
Proper use of lipid-
lowering medication
with a correlated drop
in total cholesterol
and lipid levels
resulted in a 40%
risk reduction for new
onset claudication
or progressively
worsening
claudication.

MARCH 2010 • PODIATRY MANAGEMENTwww.podiatrym.com 181
surgical intervention. Initially, con-servative treatment of PAD requiresstrict control of associated risk fac-tors, and may employ behavior mod-ification and medical management.Smoking cessation, lowering serumlipid levels, and adherence to a regi-mented daily exercise program canhave significant improvement in pa-tients with PAD.
In fact, proper use of lipid-lower-ing medication with a correlateddrop in total cholesterol and lipidlevels resulted in a 40% risk reduc-tion for new onset claudication orprogressively worsening claudica-tion.16 Exercise programs, if carriedout over a minimal six monthcourse, can increase pain-free walk-ing by 1.5 times, by increasing thetolerance of anaerobic respiration in
lower extremity muscles. It is also be-lieved that via angiogenic factors,continuous oxygen demand can leadto the formation of collateral circula-tion at areas of high-grade stenosisand occlusion.
Medical ManagementMedical management specifically
for treatment of PAD symptoms andprogression of the disease include,but are not limited to, Vitamin E (al-though its role is not fully under-stood), Trental (pentoxyfylline), Ple-tal (cilostazol), Aspirin (Acetylsali-cylic acid), Plavix (clopidogrel), Ag-grenox (aspirin/dipyridamole), andCoumadin (warfarin). Research withgene transfer therapy of vascular en-dothelial growth factor (VEGF), en-dothelial nitric oxide synthetase(eNOS), angiopoietin-1 is also being
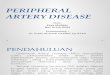
ty vessels.11 Duplex testing is alsouseful as a mode of surveillance ofbypass and stent patency after inter-vention (Figure 3). When performedevery six months, duplex ultrasoundmay identify threats to bypass ofstent life expectancy due to resteno-sis of the vessel, thrombosis, or inti-mal hyperplasia. If diagnosed earlyenough, threatened areas may be re-paired before the progress to com-plete occlusion.
Diagnostic X-rays may be used torule out osteomyelitis as a cause for,or a result of, a non-healing arterialor diabetic ulcer. With severe disease,highly calcified vessels may be seenon X-ray, although the studies areusually non-specific.
Invasive testing such as CTA,MRA, and angiogram can be per-formed when non-invasive testing isnot feasible or inaccurate. These in-vasive tests are especially useful forpre-operative evaluation of vesselsfor bypass targets, and are highlysensitive in determining the degreeof calcification and patency of mostperipheral vessels. Due to the risk ofnephrotoxicity of contrast agents,and complications with implantedmetal devices, CTA and MRA maynot always be appropriate.
In addition, in order to under-go these imaging studies, patientsare required to lie supine in a con-fined space for some time, makingsome patients too anxious to un-dergo them. Patients may also re-sist CTA studies due to exposure toexternal radiation. Post-operative-ly, CTA/MRA studies may not becost-effective for surveillance, butthey can be useful in assessing im-planted grafts for extravasation atanastomotic sites, or for infection.
Conservative Treatment andMedical Management
As with many diseases, patientswith PAD should be evaluated forseverity, and management; andtreatment should be decided basedon all aspects of the patient’s healthand lifestyle. Treatment can be con-servative and may include behav-ioral and/or lifestyle changes, andpharmacological therapy. Often,these treatment regimens are highlyeffective in managing the disease,and can avoid or delay the need for
Plumbing... considered for treat-ment.14 The drug informa-tion below is a summarizationof compiled data from multipledrug references, primarily the NCIDrug Dictionary:
1) Trental (pentoxyfylline)—previously thought to be effective inreducing the symptoms caused byPAD. Trental is a phosphodiesteraseinhibitor that increases levels ofcyclic adenosine monophosphate(cAMP) in erythrocytes, endotheli-um, and surrounding tissues; therebypotentiates vasodilation, improveserythrocyte flexibility, and enhancesblood flow by inhibiting cAMP me-diated platelet aggregation. In con-trolled randomized trials, Trental hasfailed to show any significant im-provement in symptoms or quantifi-able improvement in ABI or flowrates. Trental is typically dosed at400mg TID.
2) Pletal (cilostazol)—increas-es calcium-mediated vasodilation andinhibits platelet aggregation via phos-phodiesterase III (PDE-III) inhibition.It is contraindicated in patients withheart failure, but has been shown toimprove pain-free ambulation inmost patients, especially those whoare not candidates for revasculariza-tion. Dosing for most patients is100mg BID, but may be reduced to50mg BID if new-onset tachycardia isobserved as a result of the medica-tion. In one London study, Cilostazolused in patients with critical limb is-chemia (CLI) improved signs andsymptoms of ischemia in 23% of thepopulation, with 58% of the popula-tion stabilizing.20
3) Aspirin (acetylsalicylicacid)—a non-selective, reversible cy-clooxygenase (COX) inhibitor thatdecreases synthesis of prostaglandin,reduces inflammation, and inhibitsplatelet aggregation. Aspirin dosedminimally at 81mg QD is recom-mended for all patients with PAD ex-cept for those with a sensitivity or al-lergy to the drug, or are at increasedbleeding risk. To date, aspirin is theonly drug to demonstrate reductionof intimal hyperplasia after surgicalor endovascular procedures.
4) Plavix (clopidogrel)—an ir-reversible modifier of the platelet re-ceptor for adenosine diphosphate(ADP), preventing formation of theADP-receptor complex, and inhibit-
Continued on page 182
Continuing
Medical Education
Coumadin
dosage must be
individualized
for each patient to
maintain an
International
Normalized Ratio
(INR) of 2-3 times the
normal prothrombin
(PT) level.

K reductase. Vitamin K serves as a co-factor for clotting factors II, VII, IX,and X, and anticoagulant proteins Cand S. This decrease in clotting factorlevels and activities results in delayedclotting time, and is meant to limitstable thrombus formation and pro-gression in the vessels. Dosage mustbe individualized for each patient tomaintain an International Normal-ized Ratio (INR) of 2-3 times the nor-mal prothrombin (PT) level. Thismedication may be prescribed forpost-arterial bypass patients withhigh risk of thrombosis, includingthose with a hypercoagulable state,thrombogenic conduit use for bypass(e.g., polytetrafluoroethylene (PTFE)or Dacron graft), or poor outflowinto distal run-off vessels.
Endovascular and OpenSurgical Repair for PAD
Revascularization procedures aretypically reserved for patients suffer-ing from claudication that signifi-
cantly impairs activities of daily liv-ing and daily functioning. Theselimitations may be subjectively de-termined on a patient-by-patientbasis, as previous activity levels andexpectations of post-procedure func-tioning may be vastly differentamong patients. Generally, theseprocedures are considered when am-bulation on flat ground is stopped ata half block to a full block due toclaudication, for rest pain, or for tis-sue loss, ulceration, or gangrene as-sociated with arterial insufficiency,and unresponsive to conservativetreatment.
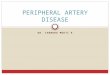
The operative mortality rate foraortic disease is 2-5%, and 1-3% forinfrainguinal disease, requiring by-pass surgery. Due to these anesthe-sia- and surgical-risks associated withformal bypass, endovascular proce-dures are often favored for revascu-larization. These procedures involvelocalization of flow-limiting lesionsusing real-time angiography, fol-lowed by dilation of lesions with aballoon catheter (Figures 1 & 2), andoften deploying a self-expanding orballoon-expandable stent at the areaof repair.
Endovascular RepairEndovascular repair has greater
success for specific types of lesions inkey areas of the lower extremities,specifically with stenotic lesions inthe common iliac arteries, and withshort-segment stenoses and occlu-sion of most infrainguinal lesions.Angioplasty alone has been associat-ed with higher recurrence rates thanangioplasty with stenting, withthree-year patency rates improvingto nearly 80% with either stenttype.17
Drug-eluting stents (DES) bond-ed with drugs such as tacrolimusand sirolimus have demonstratedtheir effectiveness in reducing post-angioplasty intimal hyperplasia toincrease patency rates. Poorer pa-tency rates of up to 60% have beenseen with external iliac artery (EIA)stenting, and success with stentingof the tibial arteries is poorer still.In some cases, endovascular proce-dures can eliminate the need forsurgical bypass; in other cases, hy-brid procedures can combine opensurgical and endovascular tech-niques at one time to maximize pa-
Continued on page 183
182 www.podiatrym.comPODIATRY MANAGEMENT • MARCH 2010
Plumbing...
ing ADP-mediated activationof the glycoprotein complex
GPIIb/IIIa. Inhibition of this path-way ultimately impedes fibrinogenbinding to platelets, and platelet ad-hesion and aggregation. Plavix dosedat 75mg QD is often started in pa-tients in status post-angioplasty andstent deployment to reduce thethrombotic risk of closure.
5) Aggrenox (aspirin/dipyri-damole)—a combination medica-tion that reduces platelet aggrega-tion via COX inhibition and inhibi-tion of adenosine uptake byplatelets and endothelial cells,thereby increasing cAMP levels. Ag-grenox is commonly dosed at 25mgASA/200mg dipyridamole), andgiven to patients who cannot toler-ate Plavix.
6) Coumadin (warfarin)—in-hibits replenishment of Vitamin K1by inhibiting the activity of Vitamin
Contin
uing
Medica
l Edu
catio
n
Figure 2a: Occlusion of the distal rightpopliteal artery proximal to the tibialtrifurcation, resulting in reducedblood flow distally; note the poor vi-sualization of the peroneal artery.
Figure 2b: Balloon angioplasty andstent deployment in the distalpopliteal artery increases distal run-off, demonstrating three-vessel runoffinto the ankle.
Figure 1b: Balloon angioplasty of theSFA results in full patency of the vessel.Angioplasty can be reinforced withballoon- or self-expanding stents.
Figure 1a: Wire access obtained in theright superficial femoral artery (SFA)where a focal high-grade stenosis isnoted.

MARCH 2010 • PODIATRY MANAGEMENTwww.podiatrym.com 183
tologous or cryogenic vein.13 Forhigh-risk surgical patients, or if localinfection at anticipated target anas-tomotic sites is a concern, extra-anatomical grafts such as axillary-femoral artery or femoral-femoralartery bypasses with graft may beemployed, though their 10-year pa-tency rates are lower.
Due to limited ac-cessibility to the hy-pogastric artery, dis-ease in this vessel islimited in terms of re-pair. Options forrevascularization ofthe hypogastric arteryinclude endarterecto-my and bypass, oftenas a SFA-profundafemoral artery (PFA)bypass, or ilio-PFAbypass. In a study ofpatients with proxi-mal lower limb is-chemia, described bythe researchers as “adecrease in exercise-transcutaneous oxy-gen pressure (TcPO2)lower than -15mmHgat the buttock level”-direct versus indirectrevascularization of the hypogastricartery was evaluated for preventionof claudication. Direct revasculariza-tion was characterized as angioplastyor iliac artery bypass, where inflowwas augmented for effect, while indi-rect revascularization was character-ized as aortobifemoral bypass, result-ing in retrograde and collateral per-fusion into the area of the hypogas-tric artery.
Using maximum walking dis-tance (MWD) and ABI as a compara-tive diagnostic marker to the inci-dence of claudication post-therapy,it was found that direct revascular-ization did show improvement overindirect repair for relief of buttockclaudication, though no significantimprovement was seen in MWD orABI in those patients.18 Such studiesmay provide empiric data to clini-cians in determining the indicatedsurgery for a specific patient.
Surgical RevascularizationsSurgical revascularizations carry
risk of occlusion due to conduit ma-terial, but also due to three mainfactors: 1. poor arterial inflow due
tency and minimize surgical risksand length of operating room stay.
Open Surgical RepairOpen surgical repair can be an
alternative to endovascular therapyfor revascularization, or may beused for those patients with pro-gressive disease that are no longerendovascular candidates. The openrepairs are also employed for thosepatients who failed percutaneoustherapy due to thrombosis orrestenosis. The preferred conduit formost peripheral bypasses is the au-tologous greater saphenous vein, asthe average five-year patency ratescan reach higher than 75-80% forall infrainguinal bypasses; in somecases, where the resources are un-available, cryogenically frozen har-vested vein is used.
Biologic ConduitsBiological conduits have a re-
duced risk of thrombosis and occlu-sion than do synthetic conduits,like PTFE and Dacron.8 However,
due to the caliber of the target ves-sels and high flow rates, certain oc-clusions benefit from the use of syn-thetic graft, as is the case of aortoili-ac occlusions necessitating aortoili-ac or aortobifemoral bypasses, orfemoral artery occlusions requiringfemoral-femoral artery bypasses.Data measuring patency rates of re-cent generation modified PTFE graftdemonstrated 1-, 2-, and 3-year pa-tency rates approaching that of au-
Plumbing... to upstream lesions andepisodes of hypotensioncan encourage thrombosiswithin a bypass; 2. poor distaloutflow and downstream obstruc-tion which can increase resistancewithin the bypass leading to com-plete occlusion; and 3. length of
artery segment bypassed and thenecessary length of conduit used. Asthe length of conduit increases, theluminal resistance based on diame-ter also increases, exponentially.Disease involving the foot is usuallya manifestation of extensive tibialdisease. If such a patient is a candi-date for surgical revascularization,these factors should be consideredsince a conduit length of 8-10 cmmay be necessary, thereby hinder-ing flow rate and outflow both an-tegrade and retrograde. Therefore,these patients should be thoroughlyevaluated with CTA or MRA foranastomotic target sites and predic-tors for bypass failure.8
An alternative to bypass for thelesions in the larger arteries of thelower extremity is endarterectomyand thromboendarterectomy. In atrue endarterectomy, the two inner-most layers of the artery, the tunicaintima and tunica media are dissect-ed and resected along with luminalthrombus and intimal plaque. Thismethod can be highly effective forshort segment lesions of the EIA,
Continued on page 184
Continuing
Medical Education
Figure 3a: Near occlusionof right SFA with forma-tion of collateral circula-tion. Continuation of theangiogram distally re-vealed reconstitution ofthe above knee poplitealartery
Figure 3b: After rightfemoral-popliteal arterybypass with PTFE graft,improved blood flow intothe tibial arteries is seen,as is improved flow intothe popliteal artery viaretrograde filling.
In a true
endarterectomy,
the two innermost
layers of the artery,
the tunica intima and
tunica media are
dissected and resected
along with luminal
thrombus and
intimal plaque.

8 Florenes T, Sandbaek G, Stranden E,Jorgensen JJ: Surgical treatment of atheroscle-rosis in the lower limbs. Tidsskr Nor Laege-foren 129(21): 2252-5, 2009.
9 Germani A, Di Campli C, Pompilio G,BiglioliP, Capogrossi MC: Regenerative thera-py in peripheral artery disease. CardiovascTher 27(4): 289-304, 2009.
10 Goldman L, Bennett JC, Atherosclerot-ic Disease, Cecil Textbook of Medicine, 21sted. Philadelphia: WB Saunders Company,2000, PP. 292-3.
11 Grainger RC, Allison D, Adam, DixonAK: Diagnostic Radiology: A Textbook ofMedical Imaging. 4th ed. Orlando: ChurchillLivingstone; 2001.
12 Herman SD, Liu K, Tian L, GuralnikJM, Ferrucci L, Criqui MH, Liao Y, McDer-mottMM. Baseline Lower Extremity Strengthand Subsequent Decline in Functional Perfor-mance at 6-Year Follow-Up in Persons withLower Extremity Peripheral Arterial Disease: JAm Geriatr Soc, published online, 26 Oct2009.
13 Hugl B, Nevelsteen A, Daenens K, etal., PEPE II Study Group: PEPE II-a multicen-ter study with an end-point heparin-bondedexpanded polytetrafluoroethylene vasculargraft for above and below knee bypasssurgery: determinants of patency. J Cardio-vasc Surg 50(2): 195-203, 2009.
14 KimMS, Lee CS, Hur J, ChoHJ, Jun SI,Kim TY, Lee SW, Suh JW, Park KW, Lee HY,Kang HJ, Lee DS, KohGY, Nakagami H,Mor-ishita R, Park YB, Kim HS: Priming With An-giopoietin-1 Augments the Vasculogenic Po-tential of the Peripheral Blood StemCellsMo-bilized With Granulocyte Colony-Stimulat-ing Factor Through Novel Tie2/Ets-1 Path-way. Circulation, published online, 16 Nov2009.
15 Kitaura K, Kida M, Harima K: Assess-ment of peripheral arterial disease of lowerlimbs with ultrasonography and anklebrachial index at the initiation of hemodialy-sis. Ren Fail 31(9): 785-90, 2009.
16 Mukherjee D, Cho L: Peripheral arteri-al disease: considerations in risks, diagnosis,and treatment. J Natl Med Assoc 101(10):999-1008, 2009.
17 Muradin GSR, et al.: Balloon dilationand stent inplantation for treatment offemoropopliteal arterial disease: meta-analy-sis. Radiology 1;38:1843, 2001.
18 Paumier A, AbrahamP,MaheG,Mau-gin E, Enon B, Leftheriotis G, Picquet J: Func-tional Outcome of Hypogastric Revascularisa-tion for Prevention of Buttock Claudicationin Patients with Peripheral Artery OcclusiveDisease. Eur J Vasc Endovasc Surg, pulishedonline, 10Nov2009.
19 Pearson T, Kukulka G, Ur Rahman Z:Ankle Brachial indexmeasurement iin prima-ry care setting: how long does it take? SouthMed J 102(11): 1106-10, 2009.
20 Shalhoub J, Davies AH, Franklin IJ:Cilostazol may improve outcome in criticallimb ischemia. Int Angiol 28(5): 363-6, 2009.
21 Stehr A, Topel I, Muller S, Unverdor-
ben K, Geissler EK, Kasprzak PM, Schlitt HJ,Steinbauer M: VEGF: A Surrogate Marker forPeripheral Vascular Disease. Eur J Vasc En-dovasc Surg, pulishedonline, 2Nov2009.
22 Terashi H: Therapy for diabetic foot ul-cers or gangrene with/without PAD. NihonHansenbyo Gakkai Zasshi 77(3): 237-41,2008.
23 Wang AH, Zhao S, Li Q, Wang PH,Yan L, Du YM, Bian RW, Wang ZJ, Mao JP,Xiao ZH,MaXY, Lin SD, ChenGC, Zhou YS,Xu ZR: The medical cost of diabetic patientswith foot problems due to peripheral arterydisease. ZhonghuaNei Ke Za Ahi 46(6):471-4,2007.
24 Zeng C: Clopidogrel application: be-yond coronary artery disease. Clin Sci (Lond),publishedonline, 4Nov2009.
25 ZhouMS, Schulman IH, Raij L: Vascu-lar inflammation, insulin resistance, and en-dothelial dysfunction in salt-sensitive hyper-tension: role of nuclear factor kappa B activa-tion. J Hypertens, published online, 5 Nov2009.
26 Zusman RM, Chesebro JH, ComerotaA, Hartmann JR,Massin EK, Raps E,Wolf PA:Anti-platelet therapy in the prevention of is-chemic vascular events: literature review andevidence-based guidelines for drug selection.ClinCardiol 22(9): 559-73, 1999.
184 www.podiatrym.comPODIATRY MANAGEMENT • MARCH 2010
Plumbing...
common femoral artery (CFA),PFA, and SFA.
ConclusionPeripheral artery disease affects
eight million people in the UnitedStates and often goes undetectedwhen patients present withoutsymptoms. Early screening and de-tection of PAD can also aid in diag-nosing cardiovascular-related dis-eases, like coronary and carotidartery disease, leading to early treat-ment and improved prognoses.Treatment of PAD should be individ-ualized on a per-patient basis, but isnot limited to surgery alone. Ad-vances in pharmacological therapyand endovascular treatment have al-lowed vascular specialists to reservesurgical procedures for a select groupof patients. �
Bibliography1 Bergin SM, Brand CA, Colman PG,
Campbell DA: A questionnaire for determin-ing prevalence of diabetes related foot disease(Q-DFD): construction and validation. J FootAnkle Res 2(1): 34, 2009.
2 Conte MS, et al.: Impact of Increasingcomorbidity on inrainguinal reconstruction:a 20-year perspective. Ann Surg 233:445,2000.
3 CreagerMA, Libby P: Peripheral arterialdiseases. Braunwald’s Heart Disease, 7th ed.,1437-1461. Philadelphia: Elsevier Saunders:2004.
4 Diehm C, Allenberg JR, Pittrow D,Mahn M, Tepohl G, Haberl RL, Darius H,Burghaus I, Trampisch HJ: Mortality and vas-cular morbidity in older adults with asymp-tomatic versus symptomatic peripheral arterydisease. Circulation 120(21): 2053-61, 2009.
5 Elduayen Gragera J, Munoz Santos L,Nogales Asensio JM, Gimenez Saez F, LopezMinguez JR, Merchan Herrera A: Ankle-brachial index in patients with chest painand suspected acute coronary syndrome.Med Lin (Barc), published online, 29 Oct2009.
6 Eraso LH, Ginwala N, Qasim AN,Mehta NN, Dlugash R, Kapoor S, Schwartz S,SchuttaM, IqbalN,Mohler ER 3rd, ReillyMP:Association of Lower Plasma Fetuin-A Levelswith Peripheral Arterial Disease in Type-2 Di-abetes. Diabetes Care, published online, 12Nov2009.
7 Fenchel M, Scheule AM, Kramer U,Bretschneider C, KlumppB, Seeger A, Rittig K,Claussen CD, Miller S: Determination of Un-known High-Grade Atherosclerotic Lesionsby Whole-Body Cardiovascular Imaging: As-sessment of Patients with SymptomaticAtherosclerotic disease of Peripheral Arteries.AcadRadiol, publishedonline, 10Nov2009.
Contin
uing
Medica
l Edu
catio
n
Dr. Pamoukian is Director of Vascularand Endovascular Surgery at Lenox HillHospital in New York City. Dr.Pamoukian’s clinical expertise is in thearea of minimally invasive vascularsurgery using balloon angioplasty andstenting and atherectomy devices foropening up theblood vessels. Dr.Pamoukian is ex-perienced in allareas of complexendovascularsurgery, includ-ing thoracic anda b d o m i n a laneurysms, aswell as carotid,peripheral, andrenal stenting.
Damien DeCollibus earnedan M.S. in Molec-ular and CellularBiology from St.John’s Universityand a post-gradu-ate degree inPhysician Assis-tant studies fromStony BrookUniversity. He hasworked as aPhysician Assistant in General, Vascular,and Thoracic Surgery, and in EmergencyMedicine. Damien is currently employed atLenox Hill Hospital in the Department ofSurgery, and is a clinical lecturer for theStony Brook University Physician Assistantprogram.

MARCH 2010 • PODIATRY MANAGEMENTwww.podiatrym.com 185
6) Described by De Bakey, whatare the three most commonsites of arterial plaque forma-tion in the lower extremity?
A) Superficial femoral arteryat the adductor hiatusB) Aortic bifurcationC) Tibial trifurcationD) All of the above
7) Type 3 lesions are the mostcommon type in the lower ex-tremity, and account for whatpercentage of lesions?
A) 10-15%B) 25%C) 60-70%D) 95-100%
8) “Leriche syndrome” de-scribes the presentation of iliacartery occlusion with com-plaints of hip and buttock clau-dication, erectile dysfunction,and what finding on physicalexam?
A) Aortic bruitB) Pes plantarisC) Absent femoral pulsesD) Gangrene
9) Pain that develops in the ab-sence of exertion, localized tothe dorsum of the foot overly-ing the metatarsal heads isknown as:
A) Intermittent claudicationB) ColicC) Rest painD) Restless legs syndrome
10) What ABI value is typicallyassociated with severe arterialinsufficiency/PAD?
A) <0.9B) 0.7—>0.9C) 0.4—>0.7D) <0.4
1) Peripheral artery disease de-velops as atheroscleroticchanges in the peripheral vesselsprogress, and may present with:
A) Intermittent claudicationB) Pain at restC) Gangrene and tissue lossD) All of the above
2) Patients with a history of PADwith claudication have a ____times higher risk of experiencinga cardiac event than those pa-tients without claudication.
A) 1B) 2.5C) 5D) 10
3) Which of these studies is notconsidered a non-invasivescreening test for PAD?
A) Ankle-brachial indexB) AngiogramC) Pulse volume recordingD) Arterial duplex
4) From innermost to outer-most, which sequence best de-scribes the layers of the arterialwall:
A) tunica adventitia—>tunicamedia—>tunica intimaB) tunica intima—>tunica ad-ventitia—>tunica mediaC) tunica media—>tunica ad-ventitia—>tunica intimaD) tunica intima—>tunicamedia—> tunica adventitia
5) Which atherosclerotic phaseinvolves destabilization of inti-mal plaque containing extracel-lular lipids and fibrous tissue?
A) Phase 1B) Phase 2C) Phase 3D) Phase 4
11) If ABI measurements arefelt to be inaccurate due tochanges of diabetes and renalfailure, what non-invasive testmay be employed to assess forPAD?
A) Computed tomographicangiographyB) Magnetic resonanceangiographyC) Toe-brachial indexD) Angiogram
12) What substance has beenshown to cause vasoconstric-tion in the peripheral arteries,and should be avoided priorto arterial duplex studies, ifpossible:
A) CilostazolB) AspirinC) NicotineD) Clopidogrel
13) Controlling which PADrisk-factor has been associatedin a 40% risk reduction fornew onset claudication orprogressively worseningclaudication?
A) HypertensionB) ObesityC) HyperlipidemiaD) Increasing age
14) Pletal (cilostazol) may im-prove pain-free ambulation formany patients via inhibition ofwhat cellular messenger?
A) ProstaglandinB) Phosphodiesterase-III(PDE-III)C) Cyclic Adenosinemonophosphate(cAMP)D) Vitamin K
Continuing
Medical Education
E X A M I N A T I O N
See answer sheet on page 187.
Continued on page 186

186 PODIATRY MANAGEMENT
15) Effective coumadin dosing is achieved whena patient’s INR reaches what range?
A) 0.5–1.5B) 2.0–3.0C) 3.5–4.5D) 8.0–9.0
16) Indications for endovascular and surgicalrepair of PAD lesions include:
A) Intermittent claudication limitingactivities of daily living and functionB) Rest painC) Gangrene or tissue lossD) All of the above
17) The bypass conduit of choice for most lowerextremity bypass surgeries is:
A) Autologous greater saphenous vein.B) PTFE graftC) Dacron graftD) Biomodified graft
18) Open surgical revascularizations of thelower extremities include which of thefollowing:
A) Endarterectomy/thromboendarterectomyB) Bypass with autologous greatersaphenous veinC) Bypass with synthetic graftD) All of the above
19) Which factor is NOT believed to increasethe risk of thrombosis of a peripheral bypass?
A) Increased length of bypass materialB) Poor distal outflowC) Hypotension and poor arterial inflowD) Use of vein over synthetic graft
20) Endarterectomy involves surgical resectionof plaque along with which two layers of thearterial wall?
A) Tunica media and tunica adventitiaB) Tunica intima and tunica mediaC) Tunica intima and tunica adventitiaD) Tunica intima and submucosa
E X A M I N A T I O N
(cont’d)
See answer sheet on page 187.
Contin
uing
Medica
l Edu
catio
n
PM’sCPME Program
Welcome to the innovative Continuing EducationProgram brought to you by Podiatry ManagementMagazine. Our journal has been approved as asponsor of Continuing Medical Education by theCouncil on Podiatric Medical Education.
Now it’s even easier and more convenientto enroll in PM’s CE program!
You can now enroll at any time during the yearand submit eligible exams at any time during yourenrollment period.
PM enrollees are entitled to submit ten examspublished during their consecutive, twelve–monthenrollment period. Your enrollment period beginswith the month payment is received. For example,if your payment is received on September 1, 2006,your enrollment is valid through August 31, 2007.
If you’re not enrolled, you may also submit anyexam(s) published in PM magazine within the pasttwelve months. CME articles and examinationquestions from past issues of Podiatry Man-agement can be found on the Internet athttp://www.podiatrym.com/cme. Each lessonis approved for 1.5 hours continuing education con-tact hours. Please read the testing, grading and pay-ment instructions to decide which method of partici-pation is best for you.
Please call (631) 563-1604 if you have any ques-tions. A personal operator will be happy to assist you.
Each of the 10 lessons will count as 1.5 credits;thus a maximum of 15 CME credits may beearned during any 12-month period. You may se-lect any 10 in a 24-month period.
The Podiatry Management Magazine CMEprogram is approved by the Council on PodiatricEducation in all states where credits in instruction-al media are accepted. This article is approved for1.5 Continuing Education Contact Hours (or 0.15CEU’s) for each examination successfully completed.
www.podiatrym.com
Home Study CME credits nowaccepted in Pennsylvania

Over, please
Please print clearly...Certificate will be issued from information below.
Name _______________________________________________________________________Soc. Sec. #______________________________Please Print: FIRST MI LAST
Address_____________________________________________________________________________________________________________
City__________________________________________________State_______________________Zip________________________________
Charge to: _____Visa _____ MasterCard _____ American Express
Card #________________________________________________Exp. Date____________________
Note: Credit card is the only method of payment. Checks are no longer accepted.
Signature__________________________________Soc. Sec.#______________________Daytime Phone_____________________________
State License(s)___________________________Is this a new address? Yes________ No________
Check one: ______ I am currently enrolled. (If faxing or phoning in your answer form please note that $2.50 will be chargedto your credit card.)
______ I am not enrolled. Enclosed is my credit card information. Please charge my credit card $20.00 for each examsubmitted. (plus $2.50 for each exam if submitting by fax or phone).
______ I am not enrolled and I wish to enroll for 10 courses at $139.00 (thus saving me $61 over the cost of 10 individualexam fees). I understand there will be an additional fee of $2.50 for any exam I wish to submit via fax or phone.
Note: If you are mailing your answer sheet, you must completeall info. on the front and back of this page and mail with yourcredit card information to: Podiatry Management, P.O. Box490, East Islip, NY 11730.
TESTING, GRADING AND PAYMENT INSTRUCTIONS(1) Each participant achieving a passing grade of 70% or
higher on any examination will receive an official computer formstating the number of CE credits earned. This form should be safe-guarded andmay be used as documentation of credits earned.
(2) Participants receiving a failing grade on any exam will benotified and permitted to take one re-examination at no extra cost.
(3) All answers should be recorded on the answer formbelow. For each question, decide which choice is the best an-swer, and circle the letter representing your choice.
(4) Complete all other information on the front and back ofthis page.
(5) Choose one out of the 3 options for testgrading: mail-in,fax, or phone. To select the type of service that best suits yourneeds, please read the following section, “Test Grading Options”.
TEST GRADING OPTIONSMail-In GradingTo receive your CME certificate, complete all information
and mail with your credit card information to:Podiatry Management
P.O. Box 490, East Islip, NY 11730There is no charge for the mail-in service if you have already
enrolled in the annual exam CPME program, and we receive this
ENROL LMENT FORM & ANSWER SH E E T
�
187
Continuing
Medical Education
exam during your current enrollment period. If you are not en-rolled, please send $20.00 per exam, or $139 to cover all 10 exams(thus saving $61* over the cost of 10 individual exam fees).
Facsimile GradingTo receive your CPME certificate, complete all information and
fax 24 hours a day to 1-631-563-1907. Your CPME certificate willbe dated and mailed within 48 hours. This service is available for$2.50 per exam if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment period),and can be charged to your Visa, MasterCard, or American Express.
If you are not enrolled in the annual 10-exam CPME pro-gram, the fee is $20 per exam.
Phone-In GradingYou may also complete your exam by using the toll-free ser-
vice. Call 1-800-232-4422 from 10 a.m. to 5 p.m. EST, Mondaythrough Friday. Your CPME certificate will be dated the same dayyou call and mailed within 48 hours. There is a $2.50 charge forthis service if you are currently enrolled in the annual 10-examCPME program (and this exam falls within your enrollment peri-od), and this fee can be charged to your Visa, Mastercard, Ameri-can Express, or Discover. If you are not currently enrolled, the feeis $20 per exam. When you call, please have ready:
1. Program number (Month and Year)2. The answers to the test3. Your social security number4. Credit card information
In the event you require additional CPME information,please contact PMS, Inc., at 1-631-563-1604.
Enrollment/Testing Informationand Answer Sheet

�
188 www.podiatrym.comPODIATRY MANAGEMENT • MARCH 2010
ENROL LMENT FORM & ANSWER SH E E T (cont’d)Con
tinuin
g
Medica
l Edu
catio
n
LESSON EVALUATION
Please indicate the date you completed this exam
_____________________________
How much time did it take you to complete the lesson?
______ hours ______minutes
How well did this lesson achieve its educationalobjectives?
_______Very well _________Well
________Somewhat __________Not at all
What overall grade would you assign this lesson?
A B C D
Degree____________________________
Additional comments and suggestions for future exams:
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
Circle:
EXAM #3/10Vascular Plumbing 101: Management of
Peripheral Artery Disease(Vicken Pamoukian, MD andDamien De Collibus, R-PAC)