Embed Size (px)
Citation preview
P E N I N S U L A H E A L T H
Q u a l i t y o f C a r e R e p o r t 2 0 0 4
As a member of the
Board’s Community Advisory
Committee, Shannon Anastasio
liaises with people throughout
the community. She gathers
information, opinions, concerns
and suggestions which she
shares with Peninsula Health’s
Board and Staff. Shannon,
mother of four, is an active
fundraiser for children’s
charities.
QUALITY OF CARE REPORT 2004
For a spoken version ring 9784 7821
PENINSULA HEALTH
PO Box 52 Frankston Victoria 3199
ph: (03) 9784 7777
For those outside the MelbourneMetropolitan Area ph: 1800 858 727
web: www.phcn.vic.gov.au
Peninsula Health proudly supports and encourages organ donation.
Australians Donate
Suite 2 Level 3 20-22 Albert Road South Melbourne(03) 9696 0651www.organdonation.org.au
To register, please call:
Australian Red Cross
Blood Service
Victorian Organ Donation Service - LifeGift538 Swanston StreetCarlton VIC 3053Ph: 1300 133 050www.organdonor.com.au
organ donor
Kidney Health Australia
VictoriaPh: 1800 682 531www.kidney.org.au
Right now there are nearly 2,000seriously ill Australians waiting foran organ donation.
So the more people there are whochoose to become organ donors, themore chance these very ill peoplehave to live.
Please consider joining the ranks of Australians on the Organ DonorRegister. If you decide you want yourorgans to save lives, register yourintentions and tell your family aboutyour wishes.
Pledge the gift of life.

Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 21 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
In our fourth annual Quality of CareReport we want to acknowledge thepartnerships that contribute toPeninsula Health’s scope of service.We value these alliances, bothwithin our organisation and withindividuals and agencies throughoutthe community, because we knowthey promote productivity andexcellence.
With this focus, we will again use theQuality of Care Report to give anaccount of our performance over thelast year. We’ll explain – throughtext, tables, patient stories andstatistics – how we solved problems,improved standards, comparedourselves with other healthagencies, progressed with ourstated goals and met the needs of
our community. We will note both ourachievements and our shortcomings,and we will outline strategies wehave developed to improve.
With feedback from our partners, we
are reporting on issues that are most
important to the community, such as
waiting times for services. We have
also focused on outcomes – it is not
enough to simply say we have done
something; we need to make clear
what the effort achieved.
We invite you to become an active
partner in Peninsula Health’s quest
for quality by sharing your view-
points and ideas about our services,
our performance and this report.
Details of ways in which you can
participate are listed on page 39.
Barry NichollsChairman, Board of Directors
We are pleased to present our 2004 PeninsulaHealth Quality of Care Report to theCommunity. We hope you will find the reportinteresting and informative and that it will behelpful if you need to use our services.
Dr Sherene DevanesenChief Executive
T H A N K Y O U F O R Y O U R I N T E R E S T I NP E N I N S U L A H E A LT H A N D O U R M I S S I O N
PartnershipsA R E T H E E S S E N C E O F C O M M U N I T Y.
Five year old Jayde Boothroyd enjoysa game with Paediatric Unit NurseClare Burns
Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 2
Barry NichollsChairman, Board of Directors
We are pleased to present our 2004 PeninsulaHealth Quality of Care Report to theCommunity. We hope you will find the reportinteresting and informative and that it will behelpful if you need to use our services.
Dr Sherene DevanesenChief Executive
Five year old Jayde Boothroyd enjoysa game with Paediatric Unit NurseClare Burns
3 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
S E R V E SOver 300,000 people living in the Frankston/
Mornington Peninsula region, as well as
holiday makers from Victoria, other parts of
Australia and overseas
A D M I N I S T E R S21 public health facilities located on 10 sites
including hospitals, rehabilitation, aged and
palliative care units, nursing homes, hostels,
a community health centre and mental health
facilities
O F F E R SAcute medical, paediatric, surgical and
maternity care, critical care, psychiatric
services, rehabilitation, palliative care,
community health and health education,
outpatient services, aged care and
assessment, investigative and medical support
services, allied health and clinical training
T R E A T S60969 inpatients and 293604 outpatient
occasions of service (69,089 of which were
delivered by Community Health Services)
Emergency patients: 62518
(2003/04 statistics)
E M P L O Y S3400 people made up of full time, part time and
casual positions.
These include administrative, support, allied
health, managerial, medical and nursing staff
and tradespeople.
Peninsula Health and the community also
benefit from the work of 700 volunteers.
E D U C A T E SMedical students, nursing students, allied
health students, hospital medical officers,
graduate nurses and students in health
administration
M A N A G E SA budget of more than $231million (2003/2004)
O U R Q U E S T F O R Q U A L I T Y –P A G E S 5 - 1 0
This section describes the systems we haveestablished to keep a constant check on howwe perform against accepted standards, the community’s expectations and our owntargets.
I N C O R P O R A T I N G Q U A L I T Y –P A G E S 1 1 - 2 8
Here we show how we apply the elements ofquality, as defined by the Victorian QualityCouncil, to our service – using thesestandards as goals. From reducing risks tomanaging resources responsibly, we reviewactivities undertaken this year in pursuit ofexcellence.
P U T T I N G Q U A L I T Y T O W O R K –P A G E S 2 9 - 3 8
Finally, we combine the information from
Sections One and Two to focus on two of our
core services – Rehabilitation, Aged and
Palliative Care Services (RAPCS) and our
Emergency Services – to demonstrate how
our quality control systems and our goals
merge to help build a healthy community.
C O N T A C T S – P A G E S 3 9 - 4 2
We provide a profile and contact details forour partners, and outline how you can haveyour say about our services and ourcommunications.
And please detach our handy list of usefulhealth service numbers and put themagnetised card on your fridge for quickreference.
SPECIAL NOTE: People who use our servicesdo so under a variety of conditions. Some arevery ill and need hospitalisation, and weusually call them patients. Those who use our clinics and other day only services areusually referred to as clients. The ladies and gentlemen living in our assistedaccommodation (nursing homes, hostels andcommunity care facilities) are known asresidents. Everyone using our services is ahealth care consumer. We’ll be using the termthat best describes the consumer in each ofour articles throughout this report.
ContentsPeninsulaHealth
The 2004 Peninsula Health Quality of Care Report is written for our partners– the people who use our services, their families and carers, thegovernment agencies that fund us, the health care and education providerswe work with, our volunteers and the wider community.
We want our partners to know how we monitor and measure what we doso that we can expand on what we do well and make improvements inother areas. We want to show our partners how we emphasise safety andcreate a culture that values and continuously improves quality.
To provide that information, we have organised our report to reflect how wemeasure, manage and maximise the safety and high quality of our services.

P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 4
I T ’ S A H I TOur new Peninsula Health Website,www.phcn.vic.gov.au, offering news,contacts, services and job opportunities, waslaunched in October 2003. The site currentlyrecords an average of 6000 hits (on-line visitsto the web page) every month, with traffic(hits on the site) coming from around theworld. If you have a compliment, comment orconcern about any of our services, you’ll finda direct email link to our Customer RelationsManager on the website.
P U B L I C H E A L T HDuring the last year our Health ForumProgram conducted sessions on Drugs inSport, Road Safety, Type 1 Diabetes,Osteoporosis, Medication Safety andSurviving the Workplace. A Men’s Health &Wellbeing Forum for the general public isscheduled for October 2004.
S A F E C R O S S I N GCrossing the road in front of FrankstonHospital is now a lot safer with the installationof a $171,000 pedestrian crossing on busyHastings Road. The project featurestechnology that gauges the foot speed ofpedestrians and adjusts the timing of thelights accordingly. Our Community AdvisoryCommittee joined with local clinicians andMembers of Parliament to improve safety on aroadway that has seen 20 pedestrian injuriesand 4 deaths over the last five years.
S T I L L R E A D YThe World Health Organisation declared asecond SARS (Severe Acute RespiratorySyndrome) alert in April this year. PeninsulaHealth immediately re-activated the SARSworking party and reviewed preventionstrategies and preparedness. Fortunately thealert was stood down in May, but the exercisereconfirmed our readiness to deal withinfectious disease outbreaks.
I C U I IThe ICU Breakthrough Collaborative wefeatured last year involved our Intensive CareUnit working with ICUs around Victoria andSouth Australia to determine standards andimprove ICU care. The collaborative is nowcomplete and of the four goals set out in theproject we:
• achieved two – providing all elements ofventilation care and a reduction in waitingtime for patients to be transferred to ageneral ward
• made progress in one – reducing pressureulcers (we completely eliminated the twomost serious stages of pressure ulcer)
• but had no change in the fourth goal – toreduce the incidence of MethicillinResistant Staphylococcus aureus (MRSA).However, our rates have consistently beenbelow benchmark ‘alert’ levels.
F O C U S I N G O N V I S I O N C A R EOur new Optometry Service for health cardholders is now open five days a week withtwo optometrists on duty three of thosedays. Marketing activities since the launchhave been very successful with theaverage number of clients seen per monthrising from 56 to 170.
You’ll find updates on other activities andperformance indicators from last year’s reporton the following pages:
Accreditation 6
Complaints Management 7
Pressure Ulcer Prevention 15
Electronic Prescribing 16
Hospital Initiated Postponements 19
Elective Surgery Waiting Lists 19
Overseas Nurses 21
Financial Viability 27
Dental Services 28
Falls Statistics 38
RetrospectiveQuality improvement is for keeps. The strategies we use to achieve high standards may change and this is an ongoing process. In last year’s Quality of Care Report we featured numerous projects we had set up, to addressspecific issues and improve our services. Some are still going strong, while others have beenmodified to work better.
A year later...

5 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
At Peninsula Health, we demonstrate ourcommitment to Quality and Safety through awell-established framework of processes andpartnerships. The Board of Directors, seniormanagers and staff join with communityadvisors, government agencies, accreditingbodies and other health agencies to measure,monitor and manage Quality and Safety. Thisprocess is continuous and thorough, providingthe checks and balances necessary to ensureQuality and Safety in our services.
This framework and the strategies we use to promote excellence is called ClinicalGovernance. An important element of ClinicalGovernance is the accountability of ourorganisation for the quality and safety of the work we do. We have a Board subcommittee for this purpose as discussed onthe next page.
Whether you have broken your leg, developed pneumonia, had troublecontrolling your diabetes or been overwhelmed by depression, healthcare is supposed to make you better. It’s not supposed to make you sicker,injure you, expose you to unnecessary risks or leave you feelinghumiliated, bewildered or neglected.
Your safety and wellbeing in a health care environment are very muchdependent on how your health providers ensure Quality and Safety. Whena health system puts Quality and Safety at the top of its list, you know youare in good hands.
A health system that operates from a
culture of Quality and Safety–
- consistently monitors performancethroughout the organisation
- ensures that the performance data itcollects is accurate, timely and relevant
- identifies and seeks to reduce risks
- responds quickly to problems, mistakes,risks or underachievement
- certifies that its employees are wellqualified for their jobs
- maintains high standards
- continually seeks to improve services
- consults with its community to determineand meet needs and expectations
- reports openly on its performance
- and uses resources responsibly.
Excellence...is not an act but a habit.
A R I S T O T L E
Monitoring, Measuringand Managing Quality
Marilyn Rowe had her first contact withPeninsula Health as a client in the DiabetesEducation Program at Frankston IntegratedHealth Service.
Staff, impressed with her enthusiasm andinterest in health issues, encouraged her tojoin the Frankston Community Health ServiceQuality Committee. She then began workingon the Quality of Care Report Committee andwas asked to expand her participation bybecoming a member of the Board’sCommunity Advisory Committee (CAC). Fromthere a Board Director’s nomination saw herselected as the consumer representative onthe Peninsula Health Quality and ClinicalGovernance Committee, one of the mostimportant committees in the health service.
It goes without saying that Marilyn has a lotof drive. And it’s also no surprise that she isretired from more than one career. She’sbeen a secretary, has worked for the BBC,was employed by Monash University andwas in TV and film production in Australia formany years. Getting up at 4.30 am to film,made her ready for a change and shefinished her career years as a secretary inhealth care. “I want to spend my retirementbeing productive and keeping my brainactive,” she says characteristically.
She notes that as a CAC member, she islistened to and encouraged to put forwardsuggestions. She also values her work onthe Quality Committees because shestrongly believes that “quality is the linchpinin good health care”.
Marilyn is the only community repre-sentative on the Quality and ClinicalGovernance Committee, but joins 20 othermembers of the public on the PeninsulaHealth Community Advisory Committees.The three CACs focus on issues affecting thenorthern and southern sites as well as thehealth service as a whole. Among their manyduties is reviewing documents to check thatthey’re easy to read and that they answerquestions the public wants to know. Theyrecently helped staff develop a betterconsent form for medical treatment.
Community Advisory Committee members,including Marilyn, recently attended thePeninsula Health Strategic Planning Day,assisting the health service to identify itspriorities for the next three years.
With all her committee work, Marilyn spendsseveral hours each month reading reportsand agendas and attending formal andinformal meetings.
But she doesn’t mind. “I’m excited by the lotof it,” she says.
Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 6
Accreditation is to a healthservice what passing a grade is to a student –confirmation that recognised standards have been met.
Peninsula Health is regularly assessed by severalaccrediting agencies:
- The Australian Council on Health Care Standards(ACHS) evaluates our work throughout the healthservice against standards accepted across Australia
- Our residential aged care services are also surveyedby the Aged Care Standards Agency (ACSA)
- Our medical training programs undertake accreditationthrough the Post Graduate Medical Council of Victoria(PMCV).
This Year:• Lotus Lodge Hostel was surveyed by ACSA in July 2004,
successfully achieving all 44 mandatory standards inthe survey. We have now received confirmation of fullthree-year accreditation.
• The PMCV reviewed intern and hospital medical officer (HMO) positions in September 2003 and fullyaccredited Peninsula Health.
• An in-depth audit of psychiatric services for the sixmonths September 2003 to March 2004 notes numerousinitiatives such as a successful health promotion groupfor older women with depression.
• In March 2003 Peninsula Health was surveyed by theACHS under the new Evaluation and QualityImprovement Program (EQuIP3) framework. Like 67% ofhealth services nationwide, Peninsula Health receivedaccreditation for a two year period and after the surveypromptly drew up a Quality Action Plan to addressspecific recommendations made by the ACHSsurveyors. Examples of these recommendations and theactions were:
R: Improvement to internal and external signage forPsychiatric Services at Frankston Hospital to facilitateaccess A: Enlargement and updating of directional street andinternal signage.
R: Replacement of the patient chairs in the dialysis unit toensure patient safety A: Purchase and installation of chairs December 2003
R: Relocation of equipment storage in the Palliative CareUnit away from patient care and access areas A: Building of a storage shed outside the Palliative Carefacility
To date, actions on all recommendations have either beencompleted or are in progress. An updated Quality ActionPlan was submitted to ACHS in June 2004.
R = Recommendation A = Action

7 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
Q U A L I T Y A N D C L I N I C A LG O V E R N A N C E C O M M I T T E E :This committee is chaired by a Board Directorand is attended by three Board Directors(including the Board Chair) plus the ChiefExecutive and the Senior Management Teamas well as community representation. TheCommittee also includes departmentmanagers responsible for various aspects ofquality such as infection control and fallsprevention. It meets every eight weeks toreview reports that provide information onPeninsula Health’s performance. Using thisdata the Committee can identify trends, gaugethe value of strategies, evaluate progress andmake recommendations.
The Quality and Clinical GovernanceCommittee considers:
C O M P L A I N T S , C O M P L I M E N T SA N D C O N C E R N SComplaints assist us in identifying and solvingproblems within our services. Every complaintis thoroughly investigated and all areacknowledged in writing within 24 hoursunless received directly by telephone.Complaints vary in complexity and mayinvolve a number of issues that need to beinvestigated – or it might only be one. All aretaken seriously. Last year the CustomerRelations Manager assisted patients andclients throughout Peninsula Health with 524complaints containing 790 issues. It took anaverage of 30 days to resolve thesecomplaints. Access, communication andtreatment remain the key areas of concern asshown in the following chart:
The Customer Relations Manager is availablefor anyone wishing to express concerns, butwe have learned from consumer surveys thatmany patients and clients are not aware ofthe formal complaint process. So we arefocusing on this issue through writteninformation, admission procedures and our
web page. In addition, a video is currently inproduction clarifying the issue of patients’rights and responsibilities, including theprocess for making complaints. The video willbe shown in the Emergency Departments andat other locations across the health service.
The contact number for our CustomerRelations Manager is 9784 7298.
B E N C H M A R K I N G‘Benchmarking’ is the process of measuringperformance against established standards andoften involves comparisons with similarorganisations. Benchmarking is used in our 28Quality Key Performance Indicators (KPIs). Forexample, we benchmark the cleanliness of ourfacilities against Department of Human Servicesexpected targets. The chart below illustratesthat we continue to perform above the DHStarget for the cleanliness of our facilities.
0 20 40 60 80 100
High Risk areas
Moderate Risk areas
V.High Risk areas
Peninsula Healthoverall score
2003 20022004
(intensive care,operating theatres)
(emergency,sterilising depts)
(general ward areas,laboratories)
DHS Target 80%
Cleaning Audit Results 2002/2004Average compliance scores by area risk
We continue to achieve high levels of cleanliness in clinical areas of our service
Peninsula Health Complaint IssuesFinancial Years 02/03 Compared toFinancial Year 03/04
Clinical GovernanceAT P E N I N S U L A H E A LT H
What is Clinical Governance?
It’s most commonly defined as “a framework through which health care organisations are accountable forcontinually improving the quality of their services and safeguarding high standards of care by creating anenvironment in which excellence in clinical care will flourish”. Peninsula Health takes this very seriously andin this section outlines the way in which we carry out these responsibilities.
G. Scally and L.J. Donaldson ‘Clinical Governance and the drive for quality improvement in the new NHS in England’ BMJ (4 July 1998):61-65

P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 8
Q U A L I T Y K E Y P E R F O R M A N C EI N D I C A T O R S ( K P I s ) KPIs are the targets set by the Department ofHuman Services and Peninsula Health tomonitor areas of risk and to measure ourperformance. Our 28 quality focused KPIsprovide data on a whole range of issues suchas the incidence of pressure ulcers and therate of induced births (see page 24).
C L I N I C A L R I S K M A N A G E M E N T‘Adverse events’ are incidents in whichpeople are unintentionally injured orotherwise harmed. At Peninsula Health wedon’t believe that people come to work to doa bad job or to make an error, but given theright set of circumstances any of us canmake a mistake. That’s why our culture ofpatient safety focuses on prevention, not punishment. Adverse events areopportunities to learn and examine andimprove our work processes.
In order to maximise this opportunity, weencourage all staff to report not only adverseevents, but also ‘near misses’ or ‘close calls’in a cooperative way.
Peninsula Health’s Clinical Risk ManagementUnit works with staff to investigate incidentsand use what is learned to minimise the riskof future adverse events. In this process staffare encouraged to make reports. During thelast year 3057 incidents were reportedthroughout Peninsula Health. Of these 94%did not involve any or only minor injury orharm but did contribute to the learningprocess. Peninsula Health’s emphasis onsafety and risk reduction was evident in theincreased 2003/04 incident reporting rate -this was a third higher in 2003/04 comparedwith 2002/03 (2143 reported incidents with91% involving no or only minor injury or harm).
More serious incidents are known asSentinel Events and are reported to theDepartment of Human Services. Last yearPeninsula Health had four sentinel eventsinvolving falls. As a result, a Peninsula Health
Falls Steering Committee was established tomonitor falls across the health service.
One of the outcomes of this has been theresurfacing of bathroom floors in older wardsto reduce the risk of falls, especially forelderly and frail patients.
Some of the improvements made by PeninsulaHealth as a result of its Clinical RiskManagement Program included:
• new forms developed to ensure that whenpatients are discharged they arescheduled for a follow-up appointment
• development of guidelines for staff, basedon the latest and best evidence, outliningthe treatment of epiglottitis (an infection ofthe epiglottis, the flap of cartilage thatprotects the windpipe when swallowingfood or fluids. The condition can swell theepiglottis so that it blocks the airway,diminishing or even preventing breathing.This is a potentially fatal, emergencycondition.)
Physiotherapist Barry Akers assists Ernest Treagus in hisrehabilitation – from injuries suffered in a bicycle accident!

9 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
C L I N I C A L P A T H W A Y SSort of a combination of a road map and a rulebook, Clinical Pathways set out theprocedures for treating certain conditions.Since these are formulated using the most up-to-date and carefully researched evidence,the pathways represent ‘best practice’. Staffare required to follow pathways exactly andany variance from these is reported. During2003/04 new pathways were established for:Fractured Forearm, Gastroenteritis andBronchiolitis, in children and the existingpathways in Diabetic Ketoacidosis, BreastSurgery, Maternal and Newborn pathwayswere reviewed. At 30th June 2004 PeninsulaHealth had 28 active pathways.
M O R T A L I T Y R E V I E W SThe Mortality Review Committee consideredall unexpected deaths that occurred at any ofour sites to ensure that we had actedappropriately and to learn lessons for thefuture.
C O M M U N I T Y A D V I C E A N DP A T I E N T S A T I S F A C T I O NS U R V E Y SPeninsula Health invites members of thepublic to serve on various bodies, includingthe Quality and Clinical GovernanceCommittee, three Community AdvisoryCommittees, Research and Ethics Committee
special project groups and focus groups. Inaddition, Peninsula Health has consumer andcarer consultants. These communityrepresentatives provide us with directfeedback on how well we are meetingcommunity expectations and makerecommendations to our planning and servicedevelopment. Peninsula Health also continuesto participate in the Victorian PatientSatisfaction Monitor which independentlysurveys samples of people who have used ourinpatient services. The results of thesesurveys are illustrated in the table below andare reported to the Quality and ClinicalGovernance Committee as are the actionstaken to address issues.
Other initiatives supporting ourapproach to Clinical Governance are:
L E G A L C O M P L I A N C ETo help safeguard the public, the delivery ofhealth services is a highly regulated industry.There are regulations, legislation, guidelinesand codes of conduct for most aspects ofhealth care, such as controlling infections,maintaining security, writing in medicalrecords and servicing equipment. Weregularly check to see that we are complyingwith all relevant laws. Through our LegalCompliance Program, managers across thehealth service report every two months
whether their areas are fulfilling all legalrequirements. If they identify any areas thatare not fully compliant, they must detail whataction is being taken. We were instrumentalin liaising with other health services toexplore the idea of a common compliancesystem to aid comparison and ensure bestpractice.
C R E D E N T I A L L I N GA crucial step in ensuring patient safety iscredentialling – the process whereby wemake sure that all senior medical staff whotreat patients at our facilities are qualified to do so. It is such a high priority that the process must go through severaladministrative levels. When a Specialist orGeneral Practitioner applies to be allowed totreat patients at Peninsula Health, theprocess includes:
• the doctor’s credentials (qualifications,registration, specialty training, experienceand referees) are exhaustively checked bythe Executive Director of Medical Servicesand the relevant Clinical Director
• the two recommend a level of ‘privileges’ forthe candidate. These might be the privilegeto work within a certain specialty (such assurgery) or subspecialty (such asorthopaedics) or could be restricted to onlycertain procedures
• next this recommendation is considered bythe Senior Medical Staff AppointmentsCommittee, a subcommittee of the Board ofDirectors chaired by the Chief Executive
• which then sends its recommendation to theBoard of Directors – the only onesauthorised to appoint and allocateprivileges to General Practitioners andSpecialists
An Australian Standard on Credentialling wasissued in July 2004 by the Australian Councilfor Safety and Quality in Health Care. We willnow review our Senior Medical StaffAppointments Policy to make sure itcompletely complies with ‘best practice’.
Clinical GovernanceAT P E N I N S U L A H E A LT H
Victorian Patient Satisfaction MonitorOverall satisfaction with hospital stay as expressed by consumersindependently surveyed. September 2000 - September 2003
Frankston Hospital
A2 hospital category average
Rosebud Hospital
C hospital category average
Sept 00-Mar 01
92%
94%
WAVE 1
98%
98%
Apr 01-Sept 01
87%
94%
WAVE 2
94%
97%
Oct 01-Mar 02
90%
94%
WAVE 3
95%
98%
Apr 02-Sept 02
94%
94%
WAVE 4
92%
98%
Oct 02-March 03
91%
95%
WAVE 5
97%
98%
Apr 03-Sept 03
91%
95%
WAVE 6
98%
98%
‘A2’ and ‘C’ are the DHS groupings for similar hospitals to aid comparison of performance

P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 10
In December 2003 the Victorian Quality Council (VQC)issued a document entitled “Better Quality, BetterHealth Care: A Safety and Quality ImprovementFramework for Victorian Health Services”. Thepublication outlined the elements of quality and offeredguidelines for improving the quality of health careacross Victoria.
The Council emphasises that quality must be as high apriority for health services as the more traditionalfinancial performance. For the 2004/05 year, the StateGovernment has introduced, for the first time, aStatement of Priorities Agreement for each HealthService. This is to be signed by the Board Chair and theMinister for Health and includes quality objectives.
The VQC identifies four key elements in qualityimprovement – good clinical governance,community and consumer involvement,competent health care providers and openreporting of accurate performance data. Withthese elements in place, a health careorganisation can work to ensure that its servicesreflect the six dimensions of quality –
Safety, Access, Effectiveness, Appropriateness,Acceptability, Efficiency
We have chosen to focus on these six dimensionsof quality in our 2004 Quality of Care Report,highlighting activities undertaken this year toachieve these goals.
Dimensions of Quality
Quality care is defined as “the extent to which a healthcare service or product produces a desired outcome”.2
Quality improvement is defined as “the continuousimprovement of all processes and the products and servicesthat are the outcomes of those processes”.13
Safety is defined as “a state in which risk (measured in terms ofconsequences and likelihood) has been reduced to an acceptable level”.2
“The dedication of nursing staff at Frankston Hospital is well known
throughout our local community.” I C U PAT I E N T *
“The focus was completely about us being together as a family.” M AT E R N I T Y PAT I E N T *
* Victorian Patient Satisfaction Monitor. Period ending September 2003 (Wave 6)
2 Australian Council for Safety and Quality in Health Care,2001 National Report on Patient Safety, Canberra.
13 Australian Council On Health Care Standards, 2002, TheEQuiP Guide, 3rd ed., ACHS, Sydney
“During times of blood transfusions two nurses attended, each checking
procedures for the type of blood being transfused.” E L E C T I V E S U R G E R Y PAT I E N T *
“Hospital in the Home service also was excellent and of great convenience.”
E M E R G E N C Y PAT I E N T *
11 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
F I R S T, D O N O H A R M .
This saying is attributed to the great Greek physician, Hippocrates. It captures perhaps the most crucial element of good health care.
When people are in our care, their safety is our responsibility. We mustkeep them safe from: injury, mistakes with medication, transmittedinfections, pressure ulcers, errors with transfusions, contaminated food,smoke-filled air . . . . the list is long and requires constant monitoring.
Ensuring safety is the first of the Victorian Quality Council’s Dimensionsof Quality. In this section we feature some of the initiatives undertakenthis year to improve safety for the people we serve.
Focusing on the valuable partnershipbetween health providers and patients, theinaugural annual Patient Safety Week washeld in May. Displays, poster competitions,quizzes, video showings and a public forumhighlighted how providers and consumerscan work together for safe, quality healthcare. Guest speakers included the Managerof the Victorian Quality Council and PeninsulaHealth’s Deputy CEO as well as a SeniorPharmacist who discussed medication safety.
Although the events were advertised in thelocal press, interest from the public wassparse with very few members of thecommunity attending forums. Organisers arealready planning strategies to encouragemore consumer participation in next year’sPatient Safety Week.
We want to put the word out into thecommunity because the first step in patientsafety is that the patients themselves areaware of risks.
A P R E M I U M R E DEvery Christmas the Red Cross makes aspecial appeal – for blood.
With so many people on holiday or busilypreparing for festivities, blood bank suppliesinvariably shrink at this time of year. A pleagoes out and good citizens answer the call –but not many. In fact, only 3% of the Australianpopulation ever donates blood at all.
Ensuring Safety N O B U T T S A B O U T I TWhen Kathleen Maund was waiting fora taxi to pick her up in front of FrankstonHospital, she was dismayed to find therewas no bench to sit on. She realisedthough, by noting all the cigarette buttsbeing swept up in the area, that anybenches provided would no doubtquickly fill with smokers.
(All indoor spaces throughout PeninsulaHealth are designated ‘Non-Smoking’.)
Kathleen decided she’d donate $100 to Peninsula Health for a benchspecifically for non-smokers – a greatidea but hard to enforce. Luckily heridea and donation fit right into work inprogress on a new smoking policy thatis limiting smoking to designatedsmoking areas.
Smoking Shelters have been installed at Frankston and Rosebud Hospitals anddesignated areas are being establishedat all other Peninsula Health sites.
Those who smoke close to theentrances of our buildings will be askedto move to a nearby designatedSmoking Shelter to ensure the comfortand safety of others.
Non-smokers can now sit comfortablyoutside Frankston Hospital in a smoke-free zone – on Mrs Maund’s brand newbench!
P AT I E N T S A F E T Y- W E A R E A L L R E S P O N S I B L E
T R A N S F U S I O N R I S KM A N A G E M E N T
Mrs Kathleen Maund

Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 12
With so little supply and a constant demand,it’s very important that precious blooddonations are not wasted – through incorrectstorage, mis-ordering, punctured bags, mis-labelling and so on.
At Peninsula Health, a Transfusion Committeepromotes the careful use of blood products.Along with the Transfusion Nurse Consultant,the committee also has the crucial job ofoverseeing safe transfusion procedures.
The Committee was formed as part ofPeninsula Health’s participation in the state-wide ‘Blood Matters’ Collaborative, which wasfeatured in last year’s Quality of Care Report.
Other goals achieved through thecollaborative were transfusion educationcourses for staff, the development of selflearning packages which enable the HealthService to identify issues to target in training,more efficient record keeping procedures,transfusion protocol badges for each staffmember and a transfusion site on the healthservice intranet.
Planning is currently underway to make itpossible for staff to ask questions on line.
Perc
enta
ge o
f err
ors
per m
onth
June 2003
Aug2003
Sep2003
Oct2003
Nov2003
Dec2003
Jan2004
Mis-Labelling Errors
Pre Zero-Tolerance
0
2
4
6
8
10
12
Blood Tube Mis-Labelling ErrorsBefore and after the zero-toleranceeducation campaign
With the introduction of ‘Zero Tolerance’,any sample with an error on the labellinghas to be retaken.

understand. We appreciate this feedback.There are now six consumer informationpamphlets available in all inpatient careareas and available for downloading from theInfection Control site on Peninsula Health’swebsite (www.phcn.vic.gov.au).
E X T R A S P E C I A L C A R EIn March 2004 the Neo-natal Intensive CareUnits at several major Melbourne hospitalsexperienced an outbreak of the bacteriaSerratia. When some babies from thesehospitals were transferred to Special CareNurseries in their own communities, extraprecautions were needed. At FrankstonHospital, all babies coming from affectedhospitals were tested for the bacteria onarrival and kept segregated from other infantsuntil the test results were available. A fewinfants tested positive for the bacteria, butwere not actually infected. These babies weretreated in a separate area at one end of theSpecial Care Nursery. Staff wore gowns andgloves and used dedicated equipment. Thestrategies worked well as there was no crossinfection of Serratia in Frankston’s SpecialCare Nursery at any time during the outbreak.
P A R T N E R S H I P S P R O M O T EP E R F O R M A N C EWe continue to work closely with theDepartment of Human Services, otherhospitals and professional groups to monitorthe effectiveness of our infection preventionand control program at Peninsula Health. Wehave been part of the Victorian HospitalAcquired Infection Surveillance Program(known as VICNISS) since May 2003 andcontinue to perform well within theestablished benchmarks. We monitorsurgical site infections and this year we arecollecting additional data on infection controlat Rosebud Hospital. We have also joined agroup established by the Victorian InfectionControl Professionals Association to shareideas for monitoring infection controlpractice in long term care facilities such asnursing homes. “The VICNISS CoordinatingCentre provides reports on state aggregatedata. Hospital-level risk adjusted data will notbe publicity released until at least 2005. Thistimeline will allow for refinement of thesystem, definitions and methods, and ensurethat data released to the public are accurateand reliable.”1
T H I N K P I N KThe mineral potassium helps regulate ourheartbeat and blood pressure, builds musclecells, and controls the water balance in ourtissues. It is in lots of food and most of us getwhat we need in our diet.
If we are a little low, our skin gets dry and we become tired, depressed and slow tomove. If we are very low our blood pressurecan go up and we can develop congestiveheart failure.
13 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
Mean/1000 bed days
Linear (MRSA Rate per 1000 Bed Days)
MRSA Rate per 1000 Bed Days
Jul 02
Aug 02
Sep 02
Oct 02
Nov02
Dec02
Jan 03
Feb 03
Mar 03
Apr 03
May 03
Jun 03
Jul 03
Aug 03
Sep 03
Oct 03
Nov 03
Dec 03
Jan 04
Feb 04
Mar 04
Apr 04
May04
Jun 04
0
11.5
2
2.5
3.54
Rate
per
100
0 Be
d Da
ys
3
0.5
Health Care Associated MRSA (Methicillin Resistant Staphylococcus aureus,also known as ‘Golden Staph’) Surgical Ward July 2002 to June 2004
D O I N G B A T T L E W I T H T H O S E B U G SWe have developed a short course onInfection Control to help our staff to monitorinfection control risks throughout PeninsulaHealth. The Infection Control Liaison programstarted in 2000 with 13 enrolments. Thatnumber rose by 38 in 2003 and as of July 2004we have 84 Infection Control LiaisonPersonnel, including registered nurses, alliedhealth workers, patient services assistantsand support staff. These staff are helpingkeep Peninsula Health safe.
S A Y, W H A T ! ? ! ?Vancomycin Resistant Enterococci andClostridium difficile are not exactly householdnames – and hearing that you actually haveone of these infections can be a bitbewildering. So our Infection Prevention andControl Unit has prepared pamphletsexplaining what the germs are and whatspecial infection control measures we use toprevent them from spreading. Our CommunityAdvisory Committees, patients and theirfamilies have helped us to refine theinformation so that it is easy to read and
Ensuring Safety
This graph is a control chart showing the rate of health care associated MRSA in a surgicalward. This rate has been monitored for the past 3 years and as a result of infection controlpractices, shows an ongoing downward trend.
M E D I C A T I O NS A F E T Y
I N F E C T I O N P R E V E N T I O N A N D C O N T R O L
1 VICNISS Hospital Acquired Infection Project Year 2 Report - March 2004.

Some conditions such as diabetes and kidneydisease can lead to potassium deficiency, ascan taking diuretics and laxatives.
When patients need extra potassium, it isabsolutely critical that it is administered withcare. While it is almost impossible to take too much potassium orally, injections ofconcentrated potassium can be fatal.
To avoid the accidental administration ofconcentrated potassium, Peninsula Healthhas initiated special protocols and conducteda service-wide staff awareness campaign.
First, concentrated potassium was removedfrom most patient care areas and replacedwith safer, pre-mixed infusions. New clinicalguidelines were drawn up that minimised theuse of potassium injection, and all potassiumproducts were packaged or labelled in brightpink to make them more visible. Thesestrategies were then communicated to allstaff through a publicity campaign with theslogan ‘Save Lives, Think Pink’.
The changes were made in December 2003and by February 2004 figures showed nearly a 300% increase in the administration ofpotassium by tablet rather than through less safe but sometimes necessary routes,such as rapid injection, that bypass thedigestive tract. This is illustrated below.
B E E A L E R TWhat do eggs, peanuts, penicillin andcockroach droppings have in common?
They can all cause allergic reactions in somepeople – reactions that vary from mild to fatal.There is a long list of allergens, and many ofthe substances are medicines.
To reduce the risk of patients receivingmedications they are allergic to, PeninsulaHealth is running a ‘Bee Alert’ campaign.Posters (with a little bee), education sessionsand publicity in staff newsletters arereminding acute health and aged care staff ofthe importance of documenting all allergies inpatients’ medical records and of avoiding theadministration of any drugs that havepreviously produced an allergic reaction.
Other posters target patients, encouragingthem to become active partners in ensuringthat all their allergies are noted and recorded.Patient alertness to what medications theyare being given and the willingness to askquestions whenever they are concerned is avital part of reducing allergic risks.
Since the campaign began, medicationincidents due to allergic reactions have beenreduced by 30%.
P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 14
February 04February 030
2000
4000
6000
8000
10000
Think Pink ProjectPotassium Usage by Product Form (Tablet)
S I M P L E R S C R I P T SWhen patients go home from hospital andhave several medications they need to takewithout help from a nurse. It can get prettyconfusing. And the prescription names canadd to the confusion.
But a recent initiative may help solve thatproblem. Peninsula Health is currentlyworking alongside health services rightacross Australia to improve medicationsafety. Called the National Medication SafetyBreakthrough Collaborative, this project aimsto reduce the harm that can result frommedication errors.
One initiative of the collaborative (whichincludes a Consumer Advisory Committeemember), was to introduce the addition ofsimple words onto medication labels in Maywhich describe the reason for themedication. The label might say ‘PAIN’ sothat once home, patients can rememberwhich medication is for pain. By July 2004,51% of the medications issued by ourpharmacy had the new labelling.
The consumer representative helped ensurethe patient perspective was considered andis helping us to evaluate the success of theinitiative.

15 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
A S O R E S U B J E C TYou would expect it to be relaxing, but lyingaround in bed can actually give you ulcers –specifically, pressure ulcers.
Bedridden patients are vulnerable to thedevelopment of what used to be called bedsores. That is because when a patient’sbones press down on skin tissue for extendedperiods, it restricts blood flow. If thatpressure is not relieved, the tissue can beginto die and a wound develops. This isparticularly true for elderly people andpeople who are unable or too unwell to movethemselves in bed.
Not everyone is at risk of getting pressureulcers, but nursing staff regularly assessmost patients’ risk of developing ulcers(exceptions are maternity, paediatrics andyoung adult psychiatric patients). This isdone using a Pressure Ulcer RiskAssessment Tool (PRAT) that was introducedat Peninsula Health early in 2003. Nursingstaff complete the PRAT for all patients whenthey are admitted and then weekly while theyare in our care. Overall across PeninsulaHealth, the completion rate of the PRATincreased from 81.2% to 88.7% during the lastyear as illustrated below.
Patients are sometimes admitted toPeninsula Health with existing pressureulcers (as shown in the chart above), andstaff are educated by the Skin Integrity Nurseon the best methods to manage thesewounds. This occurs on the wards as well asat dedicated study days when dieticians,physiotherapists, surgeons and specialistnurses contribute to the education.
Peninsula Health has been collectinginformation on pressure ulcers through itsincident reporting system since January 2002.This enables us to better target our efforts forthe future management and prevention ofpressure ulcers.
PeninsulaHealth
Health Services
0%
5%10%15%20%
Statewide Mean 26.5%
21%
30%35%
Prev
alen
ce
40%45%50%
25%
Victorian Quality Council Pressure Ulcer Prevalence Survey 2003Pressure ulcer prevalence by health service
Jul 03 - Dec 04
Peninsula Health Target
Completion Rate
Aver
age
%
Jan 04 - Jun 04
76.0078.0080.0082.0084.0086.0088.0090.00
Peninsula Health Average PressureUlcer Risk Assessment ToolCompletion Rate 2003 - 2004
Pressure ulcers are of great concern in thehealth industry. In 2003 the Victorian QualityCouncil invited all public health care servicesacross Victoria to join in a survey of pressureulcers (PUPPS). Forty-eight services tookpart, and results showed that PeninsulaHealth’s prevalence of pressure ulcers is5.5% lower than the state average.
The prevalence of pressure ulcers isregularly reported to and monitored by theQuality and Clinical Governance Committee.
Ensuring Safety
Hospital acquired Present on admission
Frankston Hospital Rosebud Hospital Mt Eliza Rehabilitation& Palliative Care
Peninsula HealthProp
ortio
n of
pat
ient
s w
ith u
lcer
s
0%
20%
40%
60%
80%
100%
Victorian Quality Council Pressure Ulcer Prevalence Survey October 2003Hospital acquired pressure ulcers by campus as at October 2, 2003
M A N A G E M E N T A N D P R E V E N T I O N O F P R E S S U R E U L C E R S
P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 16
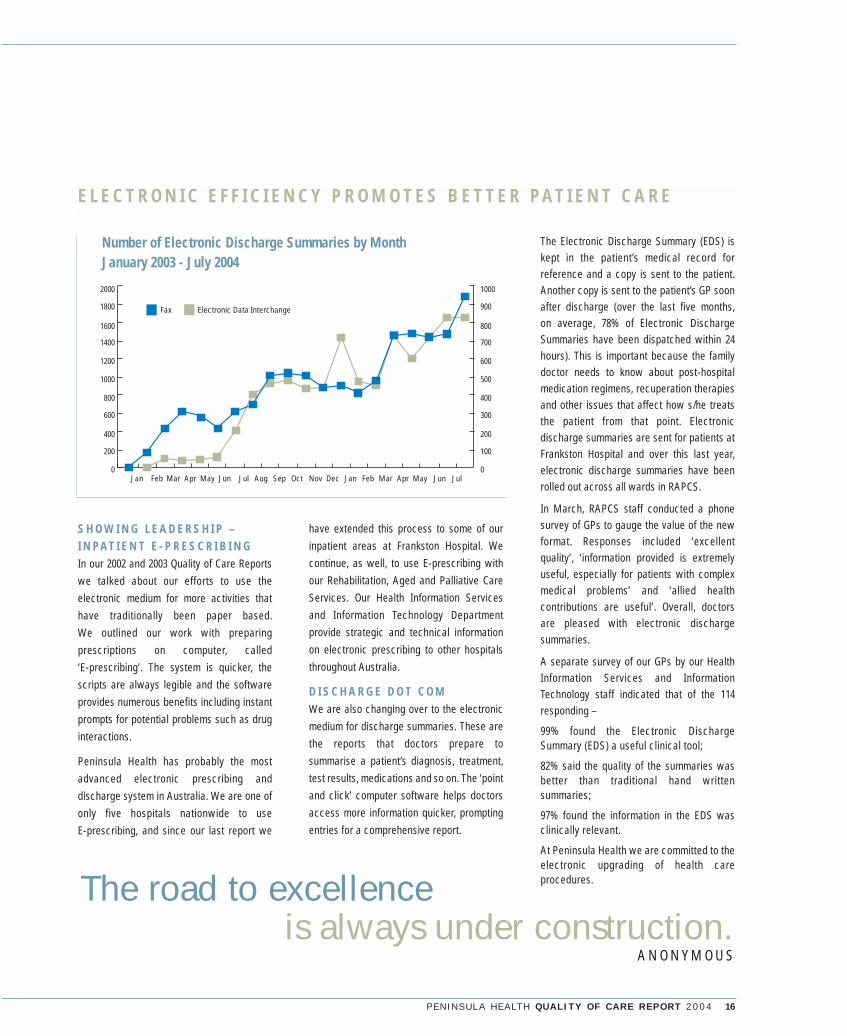
have extended this process to some of ourinpatient areas at Frankston Hospital. Wecontinue, as well, to use E-prescribing withour Rehabilitation, Aged and Palliative CareServices. Our Health Information Servicesand Information Technology Departmentprovide strategic and technical informationon electronic prescribing to other hospitalsthroughout Australia.
D I S C H A R G E D O T C O MWe are also changing over to the electronicmedium for discharge summaries. These arethe reports that doctors prepare tosummarise a patient’s diagnosis, treatment,test results, medications and so on. The ‘pointand click’ computer software helps doctorsaccess more information quicker, promptingentries for a comprehensive report.
Electronic Data InterchangeFax
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul0
200
400
600
800
1000
1200
1600
1800
2000
1400
0
100
200
300
400
500
600
800
900
1000
700
Number of Electronic Discharge Summaries by MonthJanuary 2003 - July 2004
The road to excellence is always under construction.
A N O N Y M O U S
S H O W I N G L E A D E R S H I P –I N P A T I E N T E - P R E S C R I B I N GIn our 2002 and 2003 Quality of Care Reportswe talked about our efforts to use theelectronic medium for more activities thathave traditionally been paper based.We outlined our work with preparingprescriptions on computer, called ‘E-prescribing’. The system is quicker, thescripts are always legible and the softwareprovides numerous benefits including instantprompts for potential problems such as druginteractions.
Peninsula Health has probably the mostadvanced electronic prescribing anddischarge system in Australia. We are one ofonly five hospitals nationwide to use E-prescribing, and since our last report we
E L E C T R O N I C E F F I C I E N C Y P R O M O T E S B E T T E R P A T I E N T C A R E
The Electronic Discharge Summary (EDS) iskept in the patient’s medical record forreference and a copy is sent to the patient.Another copy is sent to the patient’s GP soonafter discharge (over the last five months, on average, 78% of Electronic DischargeSummaries have been dispatched within 24hours). This is important because the familydoctor needs to know about post-hospitalmedication regimens, recuperation therapiesand other issues that affect how s/he treatsthe patient from that point. Electronicdischarge summaries are sent for patients atFrankston Hospital and over this last year,electronic discharge summaries have beenrolled out across all wards in RAPCS.
In March, RAPCS staff conducted a phonesurvey of GPs to gauge the value of the newformat. Responses included ‘excellentquality’, ‘information provided is extremelyuseful, especially for patients with complexmedical problems’ and ‘allied healthcontributions are useful’. Overall, doctors are pleased with electronic dischargesummaries.
A separate survey of our GPs by our HealthInformation Services and InformationTechnology staff indicated that of the 114responding –
99% found the Electronic DischargeSummary (EDS) a useful clinical tool;
82% said the quality of the summaries wasbetter than traditional hand writtensummaries;
97% found the information in the EDS wasclinically relevant.
At Peninsula Health we are committed to theelectronic upgrading of health careprocedures.
17 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
B E A C H B O N U SEvery summer the Rosebud foreshore fills tocapacity with happy holidaymakers. They aresome of the more than 100,000 annual visitorsto the Mornington Peninsula.
For people with serious kidney disorders, abayside beach holiday would be impossiblewithout Rosebud Hospital’s renal dialysisservice. Each year between Christmas andmid-February, holidaymakers who needdialysis can book in for their thrice-weeklysessions at Rosebud Hospital.
Last summer the service took on 24 extrapatients in addition to their regular 12. Toaccommodate the 64% increase in treatmentsprovided, the hospital added an extra dailynursing shift in the clinic.
C U R R E N T C A R ETrying to say ‘electroencephalogram’ makesit clear why the test is almost always calledan EEG.
With this test, electrodes are placed painlesslyon the patient’s scalp to record the brain’selectrical activity. Along with x-rays, the EEGhelps doctors to diagnose and manageneurological diseases such as epilepsy andassess the cause of unconsciousness forpatients receiving intensive care.
Peninsula Health started an EEG service atFrankston Hospital in December 2003, testing129 patients in the first six months. As theservice becomes better known, the referralsare increasing with 31 tests performed in June.
M A K I N G A N E N T R A N C EAlthough we have two entrances adapted forpeople who are disabled at our RosebudHospital Bayview House, a complaint from aclient of the Lung Function Service alerted usto the fact that clients are often unawarethese entrances are available. So we have putup permanent notices directing clients tothese special entrances.
A C O M F O R T A B L E F I TPeople who are very large face barriers inmany places – airplane and theatre seating,clothing stores, recreational facilities. Butthey should NOT have to endure thediscomfort and embarrassment of ill-sizedfacilities in hospital. Peninsula Health has thisyear purchased purpose-built beds and otherequipment to help care for these patients andis developing strategies to adapt care to theirspecial needs. ‘Bariatric care’, as it’s called,seeks to minimise the special problems facedby large people.
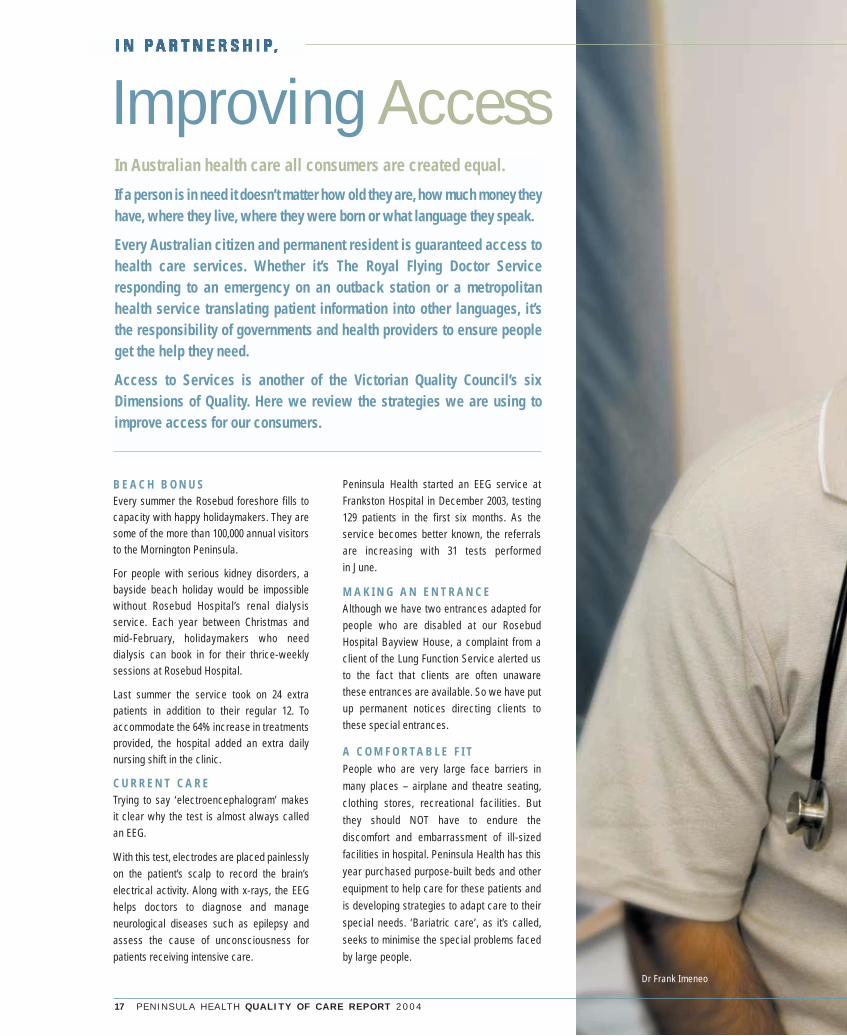
In Australian health care all consumers are created equal.
If a person is in need it doesn’t matter how old they are, how much money theyhave, where they live, where they were born or what language they speak.
Every Australian citizen and permanent resident is guaranteed access tohealth care services. Whether it’s The Royal Flying Doctor Serviceresponding to an emergency on an outback station or a metropolitanhealth service translating patient information into other languages, it’sthe responsibility of governments and health providers to ensure peopleget the help they need.
Access to Services is another of the Victorian Quality Council’s sixDimensions of Quality. Here we review the strategies we are using toimprove access for our consumers.
Improving Access
Dr Frank Imeneo

P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 18
A GENERAL PRACTITIONERSINCE 1988,
Dr Frank Imeneo currently operates Peninsula Health’s verybusy methadone clinic at the Frankston Integrated HealthCentre. Here he works with between 60 and 80 clients every week.
Dr Imeneo entered the field of drug and alcohol treatmenttentatively when he applied for his licence to prescribemethadone in order to help one of his patients who’ddeveloped an opiate dependence. He then began to seeopportunities to offer such patients “more than bandaidtreatment”.
It still took several years before he felt comfortable in the field,and he recalls his initial misconceptions. “I held the commonbelief that a drug user was ‘living it up’ with drug use,” hesays, “not being aware at that time how damaged and scarredthe individual sitting in front of me was.”
He learned from his patients and other providers in the fieldthat society has already taught drug users about their ‘lack ofworth, incapacity to make proper decisions and inability tocope with normal life’. Dr Imeneo fervently believes thathaving another person interested in their welfare encouragesdrug users to develop their sense of self worth and makechanges in their treatment of others and themselves.
This emphasis on showing respect for the inherent worth ofothers extends to entire health systems, according to DrImeneo. He notes that a breakdown of communicationbetween GPs, other health providers and hospitals can notonly risk patients’ health. “It also,” he says, “expresses a levelof disinterest in their welfare, communicating to them thattheir worth is unimportant.”
Dr Imeneo, who settled his family locally after training atFrankston Hospital, would like to see drug and alcoholservices increased throughout the Peninsula region. Hebelieves that Peninsula Health’s methadone clinic and a verysuccessful new program that admits patients to hospital foralcohol withdrawal are helping fill the service gaps. He alsohopes that other clinicians take the opportunity to visit theclinic, possibly dispelling misconceptions about this patientgroup, their worth and their prognosis.
“My philosophy for treating people with substance abuseproblems,” says Dr Imeneo, “can be summed up by the motto‘Dare to Care’.”

Category One involves conditions that could easily deteriorate quickly tothe point of emergency. Recommended admission time – 30 days
19 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
In 2003 Peninsula Health began to participatein the Elective Surgery Access Service (ESAS)initiative through which patients were giventhe option of having their surgery performed ata major regional eye centre in Cranbournewhich offered shorter waiting times. Mostpatients were happy to take up this option.
Early 2004 data showed that most of ourcataract surgery was being done at theCranbourne Regional Eye Centre and thatmany local GPs were referring their patientsdirectly to the Centre, which is administeredby Southern Health. So in partnership withSouthern Health, we transferred all ourcataract surgery to Cranbourne. Now patientscan access their surgery in about two monthsinstead of 18.
G R O W I N G P A I N SAs the population on the Peninsula increasesso does the demand for planned (elective) surgery.
Except for the most critical operations, whichwe always do within 30 days (see graphsbelow), we continue to be challenged by ourplanned surgery waiting lists.
Besides population growth, there are severalreasons why this is so. The number ofemergency patients, many of whom needadmission, increases every year. Ourcommunity’s higher than average populationof people over 65 requires more surgicalservices in areas like Urology andOrthopaedics. The schedules of surgeonspracticing in our region are almost always atcapacity. New surgical procedures are beingdeveloped all the time to treat an everexpanding range of conditions. Surgery isnow safer than ever, making it a moreacceptable option to more people.
All these factors impact on how long ourconsumers wait for planned surgery. For ourconsumers and for us – it’s sometimes longerthan we would wish.
So we continue to attack the problem on all fronts –
• using hospital beds and operating theatresmore efficiently
I T ’ S A D A T ELast year we talked about a new initiative toreduce our HIPS – those frustrating HospitalInitiated Postponements. Having to tell peoplescheduled for elective (planned) surgery thatwe must cancel their operation and re-book,is a trial for us and a burden for our patients.
The initiative was to ensure that no patientwas rescheduled more than 3 times. Thisalong with other strategies helped PeninsulaHealth to achieve a better result than thatwhich was required by the Department ofHuman Services (DHS) as illustrated above.
S E E I N G T H E L I G H TCataracts can make it seem as if you arelooking through milky plastic, a condition thatis both irritating and restrictive. So it’s a realdisappointment to discover you might have towait a year and a half for a permanent cure.
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun0
500
1000
1500
2000
2500
3000
3500
4000
0
Previous Year DHS ThresholdActual
Total Patients on Waiting List 2003 - 2004
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun0
5
10
15
20
25
30
35
Previous Year DHS ThresholdActual
Category 1 Average Waiting Time 2003 - 2004
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun0%
5%
10%
15%
20%
25%
30%
Previous Year DHS ThresholdActual
Hospital Initiated Postponements (HIPS) 2003-2004
Improving Access

P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 20
• offering surgical options at partner hospitalsthrough the Elective Surgery AccessService (ESAS) we featured last year
• ensuring patients are fit and ready forsurgery through pre-admission clinics, thusreducing last minute cancellations
• making pre-surgery reminder calls
• adding extra interim care beds to helpreduce the use of scheduled electivesurgery ward beds for emergency patients
• and many other strategies including theexpansion of our Admission/DischargeLounge.
We are currently working closely with theDepartment of Human Services (DHS) toassist those patients who are waiting aparticularly long time for joint replacements.DHS is funding the appointment of our ownElective Surgery Access Coordinator. Thisclinically trained person will:
• help us develop and implement strategiesto reduce waiting times for elective surgeryand endoscopy
• assist with identifying and referring eligiblepatients to our ESAS program
• liaise with patients and
• explore options for pre-surgical support.
This will introduce an element of ‘casemanagement’ into the scheduling process,providing patients with extra support as theywait for their surgery.
K O O R I C A R EFamily is one of the most important elementsof Koori culture. Changing communities oreven moving interstate to connect with familyis common. Although common place, thistransience can sometimes make it harder forKoori people to access regular health careservices and manage conditions such asdiabetes. Employment, housing, education andother social issues also impact on healthservices for Kooris.
As the Peninsula region has a significant Kooripopulation, Peninsula Health continues todevelop its links with the Koori community.Through the Indigenous Access Program, weare working to connect members of thecommunity with primary health care services.Our two Koori Access Workers provideinformation about health issues and helparrange appointments, transport and other supports. As well, they offer stafftraining, helping increase awareness andunderstanding of Koori issues.
Peninsula Health Psychiatric Services arealso active in Koori outreach, sitting on boththe Koori Mental Health Reference Group andthe Regional Indigenous Action Group. Staffhave recently made a submission to BeyondBlue for the funding of two indigenous mentalhealth liaison workers.
*Koori is a term that refers to people ofAboriginal descent. The word is used mainly inVictoria. Aboriginal populations in other statesuse different terms.
S I G N I N G U PIn 1941, Frankston Hospital had 34 beds andonly two cots for children. There were threehonorary medical officers. As well as nursing,the matron’s duties included boiler repair andcooking the patients’ Sunday roast dinner.
Sixty-three years later Frankston Hospital is afive-story, 380-bed metropolitan teachinghospital with over 2,000 employees. It offersliterally hundreds of services, some of which –like angiography (studying blockages incoronary arteries) and lithotripsy (non-surgical method of removing kidney stones) –didn’t even exist in 1941.
Nobody had trouble finding their way aroundthe place in the 40s, but in today’s huge facilityfinding a service or a ward can be a realchallenge. So this year Peninsula Healthallocated funds to upgrade internal signage atFrankston Hospital. Staff have been updatingdirectional signage from the main entry, at liftlobbies and then to wards and units. At thesame time, redundant signage is beingremoved. More funds are being targeted atupgrading external hospital signage next year.
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun0
50
100
150
200
250
300
350
400
450
Previous Year DHS ThresholdActual
Category 3 Average Waiting Time 2003 - 2004
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun185190195200205210215220225230235240
Previous Year DHS ThresholdActual
Category 2 Average Waiting Time 2003 - 2004
Category Two patients have conditions that cause some pain, dysfunction or disability,but are not likely to deteriorate quickly. Recommended admission time – 90 days
Category Three conditions are very unlikely to deteriorate quicklyand do not involve significant pain or dysfunction.
21 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
Delivering Effectiveness
C L I N I C A L A U D I T - A N E F F E C T I V EE VA L U AT I O NAll relevant birthing statistics are reviewedand presented at the Significant Clinical Eventmeeting, a clinical forum designed to presentpertinent cases for review and discussion byall medical and nursing staff.
This meeting provides important data forcomparison and review enabling staff torecognise the areas of achievement and toidentify areas needing improvement.
Some of the particular areas which have beenfocused on in the 2003/2004 year are
• 3rd and 4th degree tears. Cases werereviewed and the management protocolwas reviewed and updated, providing
- improved process for referral postdischarge from the hospital, promotingbetter long term management
- streamlined documentation and moreaccurate classification of tears, allowingfor consistency of data entry
- increased information provided for clientsand GPs both during the pregnancy andpost delivery.
• Post partum Haemorrhage
- Management of the third stage of labourhas been altered to reflect best practiceguidelines.
- The management protocol for the thirdstage of labour has been reviewed andeducation updates have been held. Whilstit is too early to detect a trend for this area,some early results are positive, and thisarea will remain a focus for the months tocome.
• Term babies admitted to Special CareNursery
- All cases of term infants admitted toSpecial Care Nursery have been reviewed,to detect trends, improve processes and tomonitor protocols. Reviewing six monthsworth of data has revealed appropriateadmission processes, therefore the reviewprocess has been narrowed to threeparticular issues for future months.
C L I N I C A L A U D I T – I M P R O V I N GD E T E C T I O N O F T H Y R O I D C A N C E RSmall rounded lumps are commonly felt in thethyroid gland. In order to determine the causeof the lump, 253 patients underwent aprocedure whereby a fine needle was put intothe lump to retrieve material that wasexamined under a microscope.
This process proved to be invaluable indiagnosing cancer of the thyroid and hasresulted in the refinement of this technique.
P E R S O N N E L P R O M O T EP E R F O R M A N C EAchieving the desired outcome from atreatment or service can only by achieved ifwe have adequate numbers of appropriatelyskilled personnel.
During 2003/04 we put in place a number ofinitiatives to promote effective servicedelivery. These include:
G E T T I N G B A C K I N T H E G A M ETo help ensure we have adequate numbers ofnurses, our Nurse Educators have developeda Supervised Practice Program. Experiencedpreceptors and nurse educators work withnurses who have spent several years out ofthe profession and with overseas nursesseeking registration in Victoria. Using theAustralian Nursing Council NationalCompetencies, instructors help these nursesregain knowledge, competence andconfidence prior to re-registration. The firstthree participants have completed theinaugural program.
I N T E R N AT I O N A L N U R S I N GIn 2001 we travelled overseas to recruit qualifiednurses to Peninsula Health. We were successfulin attracting 57 nurses, particularly from the UKand South Africa. The first recruits arrived inApril 2002 and the last in September 2003.
The recruitment program has been verysuccessful, with 36 of the 57 still working atPeninsula Health. Seventeen completed theircontracts before resigning, staying an averageof 17.5 months. Only four stayed less than 12months.
M A X I M I S I N G T H E M E N TA LH E A LT H W O R K F O R C ENurses in Peninsula Health’s PsychiatricService (PHPS) have been applying someinnovative strategies to attract personnel tomental health nursing.
A comprehensive Recruitment and RetentionCampaign, under the direction of Chief NursingOfficer Barbara Keeble-Devlin, has significantlyincreased interest in Peninsula Health and itsmental health services.
Among the activities Barbara and her teamemploy to spread the word about PHPS andhighlight the professional attractions of coreprograms are:
• Lectures delivered by PHPS staff to first yearnursing students at universities, explainingthe PHPS service profile and theopportunities in mental health nursing
• A program of rotations through psychiatricservices for first year nursing graduates,incorporating a Graduate Diploma inPsychiatric Nursing
• Shared training initiatives with LatrobeRegional Hospital
• A newsletter on psychiatric services madeavailable to Monash University and localschools
The third Dimension of Quality is Effectiveness – ensuring that treatments will produce measurablebenefits and achieve the outcomes we want.
The following activities demonstrate our emphasis on effectiveness.
P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 22
• Manning stalls at public venues duringMental Health Week
• Representation at career exhibitions topromote mental health nursing to thegeneral public and high school students.
The group has also developed an Introductionto Mental Health course for staff who havebeen out of nursing for some time, come fromoverseas or have little mental health nursingexperience.
When the campaign first started, PHPS stafffound it hard to fill even two places in theGraduate Nurse Program. This year therewere 15 applicants for the program. Thecampaign has been so successful thatBarbara was awarded a $10,000 scholarshipto expand her workplace recruitment andretention program.
P H A R M A C I S T S B E L O N G I NH O S P I TA LWell-qualified pharmacists are essential to ahospital’s work, yet throughout the worldhospitals have difficulty recruiting pharmacystaff. For several reasons, especially thehigher pay in the private sector, vacancy ratesfor pharmacists in Australia, America and theUK average 15%.
Working from a 2002 State-sponsored study,Peninsula Health is designing strategies tomake hospital pharmacy positions more
attractive and to expand avenues ofrecruitment.
H E L P F R O M H A R PDiabetes and heart failure are chronicconditions – that is, once you have them theycan be with you for life. Both can be veryserious, requiring repeated admissions tohospital. But by managing their diseasecarefully, people with diabetes or heart failurecan stay well, lead basically normal lives andonly come to hospital to visit sick friends.
Helping people with a range of chronicconditions to better manage their illness is theaim of the Department of Human ServicesHospitals Admission Risk Program (HARP).HARP projects are designed to invest healthresources in monitoring, managing andmaintaining health rather than having to usefar more expensive hospital treatment for acondition that has deteriorated.
The latest HARP project at Peninsula Health isthe Complex Care Program designed toimprove the ongoing care of people with heartfailure, diabetes and drug and alcoholproblems – all of whom have complex needs.
For example, instead of having to locate andmake appointments for the numerousdifferent services they require to stay well,many clients simply attend special clinics or
classes. There, they get a convenient packageof care from physiotherapists, nutritionists,doctors, counsellors, social workers and otherhealth professionals. By utilising these ‘onestop shop’ resources, the consumers aregreatly reducing their risk of hospitalisation.(According to our recent community survey onconsumer expectations, being able to accessseveral services as part of a single program isemerging as an important expectation ofservice users.)
To date HARP initiatives for patients withcomplex conditions have –
• Reduced Length Of Stay (LOS) in hospital by 37%
• Reduced hospitalisation for heart failurefrom the 16th highest cause of admission tothe 24th highest
• Reduced admissions to hospital for peoplewith diabetes by 28%
• Decreased the LOS in the EmergencyDepartment for patients with psychiatricproblems by 38%.
E M E R G E N C Y E F F E C T I V E N E S SWe have focused on the effectiveness of ourEmergency Department in our feature story‘Responding to Emergencies’ commencing onpage 29.
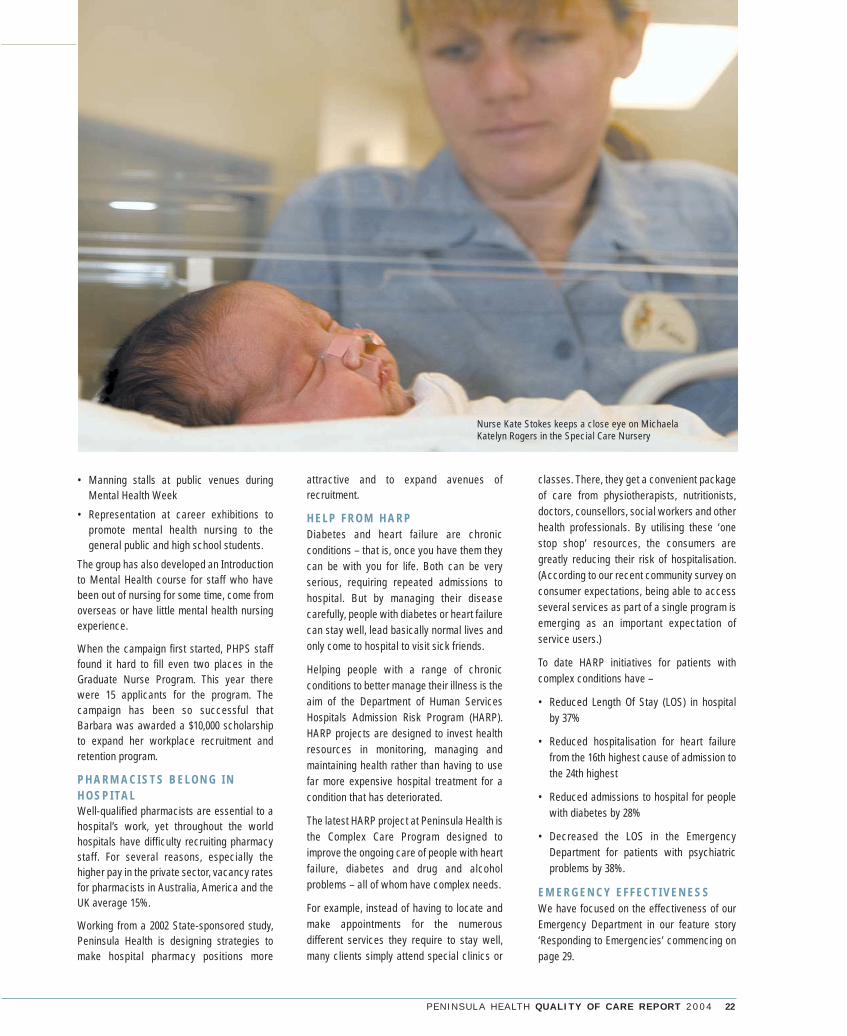
Nurse Kate Stokes keeps a close eye on MichaelaKatelyn Rogers in the Special Care Nursery

23 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
DeterminingAppropriatenessHealth care will never be a ‘one size fits all’ process.
Literally dozens of variables must be considered in caring for everypatient and the treatment and care individualised to each person’sspecific needs.
The third Dimension of Quality is ensuring that care is appropriate toeach individual – the right treatment at the right time for the right patient.
Our efforts to provide appropriate care this year included:
A L L I N T H E F A M I LY
Families who want to play a more active rolein the birth of a baby can now opt for FamilyBirthing Care at Frankston Hospital.
Launched in June 2004 the program istailored for:
- families who want lots of involvement inpregnancy, birth and post natal care withplenty of education from midwives
- women and their families who wantmidwife care and minimal intervention
- women who want to leave hospital within24 hours of birth with ongoing midwiferysupport at home
- women whose health and pregnancy fitstrict low risk profiles.
In two months since the program began, fourfamilies have chosen Family Birthing Care.
The hospital’s Maternity Service encourageswomen to be active partners in their care.With this approach, birthing options and new,spacious facilities, the number of womenchoosing to give birth at Frankston Hospitalhas risen by 18% over the last year.
W E ’ R E D O I N G B E T T E RLast year we talked about the efforts ofpsychiatric services staff to include patientsand carers in planning for discharge fromhospital. In 2002 a consumer survey indicatedonly 40% of the consumers polled, felt positiveabout the discharge process. After dischargeplanning groups were formed last year, thatfigure rose to 66%.
A S H E D F O R M E NMateship is an integral part of Australianculture. Peninsula Health, with its partners,has built on this concept to improve themental health and wellbeing of men in thelocal community.
We are building a Men’s Shed on FrankstonHospital grounds that will provide a safe, drugand alcohol free environment for men in the community. Programs, under a paidcoordinator, will include support groups,mentoring and physical activity.
P R O F E S S O R I A L I N P U TLast year Peninsula Health recruited its firstProfessor Director. This position was in theWomen’s, Children’s and Adolescent HealthService: Professor Burrows and his teamthen set about reviewing all systems andprocesses to provide appropriate care forindividual patient needs. Some of theoutcomes of the reviews were: theintroduction of Information Resource
Manuals beside each maternity bed, morecustomer focussed antenatal clinics, updatedclinical practice guidelines, a new medicalstaff orientation handbook, an increasednumber of midwifery clinic appointment timesincluding after-hours and weekendappointments.
C T A N D M R I S C A N G U I D E L I N E S Growth in Computer Tomography (CT) scanordering has been phenomenal at PeninsulaHealth. Between 1998/99 and 2002/03, ordersfor CT have grown 90% (from 3,735 to 7,109p.a.). The greatest growth has been in after-hours orders, with a 142% growth in ordersbetween 5pm and midnight and 222% growthin orders between midnight and 7.30am.
New guidelines were developed for after-hours CT scan ordering and wereimplemented in January 2004. The guidelineswere trialled over a period of 6 months and,following feedback, they were revised inAugust 04. Patients requiring non-urgent CTwho present overnight have their procedureexpedited first thing in the morning withrostering of additional staff at that time.
The impact has been that the growth in CTorders has slowed from 15% pa to only 2.7%pa. and that recall of staff has decreased.
Guidelines are now in place for the orderingof Magnetic Resonance Imaging (MRI) scans.These include a list of relevant indications

Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 24
Megan Robertson, who is planning to use the new Family Birthing Service for the birthof her first child, looks over amenities in the delivery room. She plans to have herpartner, her parents and her sister involved. Megan is a nurse in Peninsula Health’sMaternity Unit, as was the first mother to give birth in the new Family Birthing Service.
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun0%
5%
10%
15%
20%
25%
30%
Indicator ThresholdActual
Induction Rate Frankston 2003/2004
and the requirement that orders arecountersigned by Clinical Directors.
Pathology test ordering initiatives arediscussed on page 31.
These processes demonstrate that we aim touse investigations appropriately.
S A F E B I R T H I N GThe rate of obstetric inductions is risingworldwide. Natural labour which has notbeen artificially induced, is far morepreferable and minimises the risk ofcomplications. Peninsula Health aims toachieve a balance between safety for motherand baby and letting nature take its course.
Maternity staff at Peninsula Health haveinitiated several policies in an attempt toclosely monitor and reduce the number ofinductions. These include:
• Bookings for inductions can now only bemade in the obstetric clinic or from aconsultant obstetrician
• Induction bookings will only be acceptedfrom the midwife in charge of the ward
• If an induction does not meet the acceptedguidelines, the patient is sent to theobstetric clinic for consultation with theProfessor Director of Women’s, Children’sand Adolescent Health Services
• Each case is reviewed on the day of theprocedure at a team meeting and iscancelled or delayed if required
• Inductions done each month are allreviewed against criteria established bythe Australian Council for Health CareStandards.
Induction rates at Frankston Hospital arecurrently 7% lower than the State targetthreshold (see graph below) and at RosebudHospital are 18% lower.
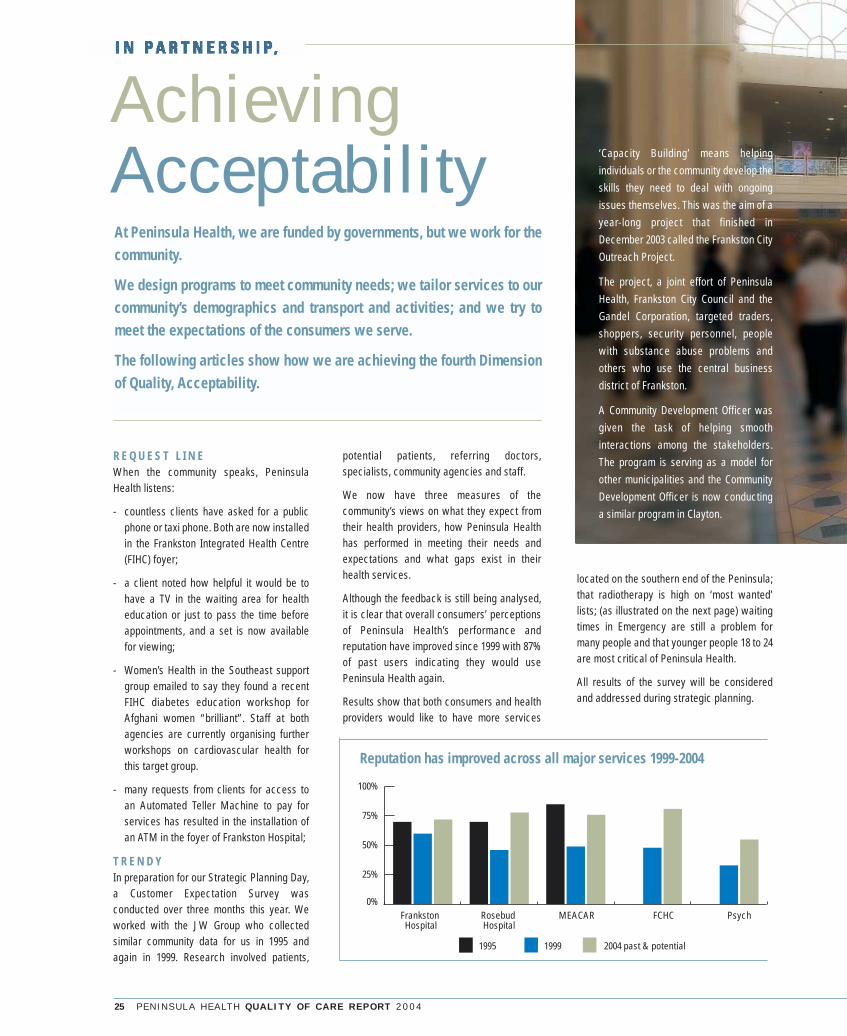
25 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
AchievingAcceptability
R E Q U E S T L I N EWhen the community speaks, PeninsulaHealth listens:
- countless clients have asked for a publicphone or taxi phone. Both are now installedin the Frankston Integrated Health Centre(FIHC) foyer;
- a client noted how helpful it would be tohave a TV in the waiting area for healtheducation or just to pass the time beforeappointments, and a set is now availablefor viewing;
- Women’s Health in the Southeast supportgroup emailed to say they found a recentFIHC diabetes education workshop forAfghani women “brilliant”. Staff at bothagencies are currently organising furtherworkshops on cardiovascular health forthis target group.
- many requests from clients for access toan Automated Teller Machine to pay forservices has resulted in the installation ofan ATM in the foyer of Frankston Hospital;
T R E N D YIn preparation for our Strategic Planning Day,a Customer Expectation Survey wasconducted over three months this year. Weworked with the JW Group who collectedsimilar community data for us in 1995 andagain in 1999. Research involved patients,
potential patients, referring doctors,specialists, community agencies and staff.
We now have three measures of thecommunity’s views on what they expect fromtheir health providers, how Peninsula Healthhas performed in meeting their needs andexpectations and what gaps exist in theirhealth services.
Although the feedback is still being analysed,it is clear that overall consumers’ perceptionsof Peninsula Health’s performance andreputation have improved since 1999 with 87%of past users indicating they would usePeninsula Health again.
Results show that both consumers and healthproviders would like to have more services
located on the southern end of the Peninsula;that radiotherapy is high on ‘most wanted’lists; (as illustrated on the next page) waitingtimes in Emergency are still a problem formany people and that younger people 18 to 24are most critical of Peninsula Health.
All results of the survey will be consideredand addressed during strategic planning.
At Peninsula Health, we are funded by governments, but we work for thecommunity.
We design programs to meet community needs; we tailor services to ourcommunity’s demographics and transport and activities; and we try tomeet the expectations of the consumers we serve.
The following articles show how we are achieving the fourth Dimensionof Quality, Acceptability.
Frankston Hospital
Rosebud Hospital
MEACAR FCHC Psych0%
25%
50%
75%
100%
1999 2004 past & potential1995
Reputation has improved across all major services 1999-2004
‘Capacity Building’ means helpingindividuals or the community develop theskills they need to deal with ongoingissues themselves. This was the aim of ayear-long project that finished inDecember 2003 called the Frankston CityOutreach Project.
The project, a joint effort of PeninsulaHealth, Frankston City Council and theGandel Corporation, targeted traders,shoppers, security personnel, peoplewith substance abuse problems andothers who use the central businessdistrict of Frankston.
A Community Development Officer wasgiven the task of helping smoothinteractions among the stakeholders.The program is serving as a model forother municipalities and the CommunityDevelopment Officer is now conductinga similar program in Clayton.

P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 26
C A R I N G A B O U T C U L T U R EWearing a turban, or ‘Dastar’, is arequirement for a man of the Sikh religion. It isalso an article of his faith that he not removeany hair from his body. These are not familiarcustoms in westernised Australian culture,but are essential to the well-being of Kahlsa(faithful) Sikhs.
Respect for patients’ traditions and beliefsmust be part of their health care. As long as safe medical care is not compromised,staff sometimes need to modify proceduresand practices to accommodate culturaldifferences.
But they can’t do that if they don’t know aboutor understand the customs and how importantthey are to the patient. So Peninsula Healthdeveloped a Language Services StrategyProject 18 months ago to improve services forpeople from diverse cultures and those whospeak little or no English.
Training was provided for staff throughoutPeninsula Health to increase awareness ofand sensitivity to patients’ cultural needs. Thesessions also taught staff how to contactinterpreter services around the clock andhow to work with an interpreter effectively.Since the project began, staff have recordeda 300% increase in interpreter bookings from16 bookings a month before the project to 50 a month.
Over the last year interpreters were requestedmost often for Italian, Greek, Croatian,Cantonese and Mandarin languages. Staffhave noted growth in the local Afghanipopulation through increased requests forDari interpreters.
Last year all cultural and linguistic informationfrom the training sessions was entered on thePeninsula Health Intranet site for referenceby staff.
V E R Y S P E C I A L N E E D SFor most of us the term ‘disability’ conjures upimages of wheelchairs and guide dogs.Mobility and vision problems present manychallenges in daily life and there arenumerous supports in the community forpeople suffering from these disabilities. Thereare just as many challenges facing peoplewith intellectual disabilities but, because ofthe public’s general lack of knowledge aboutthese conditions, society is not usually assupportive of these people.
We discovered during the year that this lackof knowledge even extended to some of our own health services. A complaint was received from the family of anintellectually disabled patient, and asubsequent investigation confirmed that weneeded to improve our care of such patients.We have since developed in-serviceeducation sessions for junior medical staffand nursing staff on managing patients withan intellectual disability. In addition, aninformation package on the needs of patientswith an intellectual disability is beingcompiled as a resource for all staff.
Cancer/chemotherapy/ radiotherapy
Public/comm funded dental service
Number of respondents
Health care for elderly
Improved Audio/optical services
More home based care
More GPs
More paediatricians
Mental health/psychiatric services
Coronary services
Facilities renal/ kidney problems
More public hospitals
0 5 10 15 20 25
Key Service Gaps for past andpotential service usersCustomer Expectation Survey 2004
Mr Steve Luby, Manager of Bayside Shopping Centre,was an active partner in the Frankston CommunityOutreach Program. The Gandel Corporation, whichoperates the centre, donated funds to help supportthe project.

27 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
EnhancingEfficiency
S U C C E S S I N S U R P L U SPeninsula Health ended last year with anoperating surplus of $1.685M which was anexcellent result. During last year, PeninsulaHealth undertook a number of initiativeswhich contributed to this result.
Managers across the health serviceexercised close control over their budgetsand the Health Service implemented somespecific strategies to maximise use of everydollar it received. Some of these aredescribed below:
F I N D I N G S A V I N G S I N F O O DS E R V I C E SOur food services department evaluated howeach dollar in its budget was being spent.Some of the changes they then implementedwere: more effective tendering andpurchasing processes, changes to levels ofstock held (down from one month’s worth totwo weeks), reduction in the number of spare
meals being sent to the wards, therebyreducing wastage, reduction in wastage fromthe staff dining room and reduction in thenumber of disposable containers used acrossPeninsula Health. Overall their strategiesenabled the food services budget to bereduced by $400,000 in 2003-04.
S A V I N G S T H R O U G H S T A F FS A F E T YIn 2003/04 Peninsula Health addressedWorkcover issues by firstly, recovering$400,000 due to be paid to the health servicefor past Workcover claims and secondly,managing its approach to Workcover andReturn to Work practices far better. PeninsulaHealth did this by:
• Ensuring that cases were reported promptlyto Workcover.
• Promptly and actively managing Workcovercases thereby reducing stress on theworker. This also helped reduce costswhere the worker returned to theworkplace in a shorter time.
• Implementing injury prevention strategiessuch as ‘no lift’ training because we wereable to identify back and shoulder injuriesas key risks.
• Implementing Occupational Health andSafety reviews of potential risks such asinappropriate storage areas, workstationsor desks.
Peninsula Health’s significant improvement inWorkcover administration has resulted in thepremium for the year 2004 - 2005 being$587,000 below that of 2003-2004
The chart on this page illustrates that we havereduced the number of New Workcover claimsfrom 85 in 2002 - 2003 to 56 in 2003 - 2004.
In addition last year our average cost perclaim had reduced to $22,720 (from $42,475 in2002-2003). This compared favourably to theunweighted average cost of claims in the 13Metropolitan Health Services which was$34,899 last year.
T R I M M I N G T R A N S P O R T C O S T S Last year we reviewed the efficiency andeffectiveness of our patient transport andwere able to save over $100,000. This wasachieved through better coordination oftransport ordering between sites andbetween departments, as well as the use of a private contractor, for our non urgenttransport rather than the MetropolitanAmbulance Service.
Nobody likes paying tax, but it’s less of a burden when we get a goodreturn on our money through first rate public services. Using resourcesresponsibly and getting as much benefit as possible from each fundingdollar is the Victorian Quality Council’s fifth Dimension of Quality.
2002-2003
85
56
Completion Rate
Num
ber o
f New
Wor
kcov
er C
laim
s
2003-2004
0
20
40
60
80
100
New Workcover Claims 2003-2004Compared to Previous Year

P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 28
E C O N O M I C A L A D V E R T I S I N GLast year Peninsula Health continued itsreview of the way in which it advertises fornew staff, to find a more cost effectiveapproach. Advertising costs in 2001-2002totalled over $500K. The outcomes of ourdeliberations were:-
• to continue to restrict external advertisingto only one publication and to tighten upapproval and the length of advertisements.
• to take advantage of e-recruitment optionson the internet,
• to change the advertising format and styleto reflect our Employer of Choice strategy -Peninsula Health’s employment brand is‘Great place to work - great place to live!’
Our success in this area has reducedexpenditure by 50% and contributed toachievement of our goals to have the right number of appropriately skilledprofessionals at Peninsula Health.
P A C I N G O U R S E L V E SLast year Peninsula Health reviewed the typeof pacemakers used with a view to using astandard type where clinically appropriatewith the potential for saving $100,000 perannum.
S T I L L D R I L L I N G A W A Y A TT H O S E L I S T SLast year we called them ‘staggering’ – thelists of people waiting for publicly fundeddental services. The huge numbers stretchedwaiting times for health card holdersanywhere up to three years.
We’ve good news to report on part of the list– with a $60,000 grant from Dental HealthVictoria we have reduced the number ofpeople waiting for dentures.
Also, in partnership with Dental HealthVictoria, we added a service that treatselderly residents in their nursing homes or hostels. (see ‘Brushing Up on DentalHealth’ pg 37)
We continue to respond quickly to people inpain and have one of the highest emergencytreatment rates in the state.
However, the number of people waiting forbasic examinations or routine procedures hasincreased from 5,697 to 6,950 with waitingtimes up to more than three years.
Although waiting lists and times for publicly-funded dental care are high everywhere,demand for Peninsula Health’s dentalservices is higher than the Victorian average.
Keeping up with this demand is definitely achallenge, but we’ll keep working asefficiently as possible to make dents in thosedental lists.
Jul
Indi
vidu
als
Wai
ting
Wai
ting
Tim
e (m
ths)
Aug Sep Oct Nov Dec Jan Feb Mar Apr0 0
50.5
10
15
20
25 3.5
3
2
1.5
1
2.5
Waiting Time(months) Individual Waiting
Waiting Time For Prosthetics(Dentures) - Most Urgent

29 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
Staff who work in Emergency Departments need to be ready for almostanything. From snakebites to sunstroke and shootings to shatteredbones, there are countless ways people can be hurt.
Peninsula Health is ready at its two 24-hour Emergency Departments(EDs). One of these is located at Rosebud Hospital and two years agowas expanded and redesigned. This year saw the completion of newtriage and waiting room facilities. Many patients from the SouthernPeninsula are treated here, and some are stabilised prior to being senton to the larger facility at Frankston Hospital.
The Frankston Hospital ED was also upgraded two years ago. Thefacility has three resuscitation bays, 30 other beds, a paediatricsection, consultation rooms and a dedicated x-ray room. Adjacent tothe ED is an Observation Ward that can serve as interim care betweenthe Emergency Department and the wards.
Our EDs at Frankston and Rosebud Hospitals saw 62,518 patients lastyear, 2325 more than the previous year.
The EDs are often the hub of hospital operations, with demand foremergency services impacting on all other services.
The following articles and storyboard highlight activity in this core service.
Responding toEmergencies
L O T S T O L E A R N You have to know a lot to be prepared
for anything.
Take emergency nursing, for example.
One minute you are checking a child’s
temperature, the next you are helping
stabilise an elderly woman’s heart rhythm. In
a single day you could deal with a dislocated
shoulder, two asthma attacks, several cases
of gastro, a serious road accident, a rash, a
diabetic coma and a burn. If yours is a night
shift, that list could easily include a knife
wound, injuries from a brawl and two or three
psychiatric emergencies.
Emergency Department nurses need to havea broad scope of clinical knowledge to handleall the different types of illness and injury they see.
To ensure they have got that knowledge and have mastered the necessary skills,Peninsula Health has developed acomprehensive program of ongoingeducation and accreditation for emergencynursing.

Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 30
Treating injuries from chemical, biological or radiation (CBR) hazardstakes special preparation, especially since these incidents often occurto many people at once, as in gas leaks or industrial accidents.
Staff responding to multi-casualty Chemical, Biological and Radiation(CBR) or Hazardous Materials (HAZMAT) incidents like these have beengiven special training by the Department of Human Services. At Frankston Hospital 16 senior nursing and medical staff havecompleted CBR training and Emergency Department staff regularlyundergo in-service education in CBR preparedness.
CBR/HAZMAT emergencies also require a number of specific protocols,involving protective gear, outdoor areas equipped for initial triage andaccess to outside decontamination facilities such as showers. As partof the CBR preparations at Frankston Hospital’s EmergencyDepartment, two Geiger Counters (radiation detection devices) andfifteen complete sets of Personal Protective Equipment are nowpermanently stored in the unit. Additional external lighting has beeninstalled in the ambulance parking bay for night time response.
CBR incidents over the last year included exposure to organicphosphates, a toxic spill and 20 paint factory workers overcome by fumes.
The other vital element in CBR response is a close partnership withfirefighters, ambulance staff, police and other members of an incidentresponse team.
This includes:
- weekly education sessions with one-on-
one clinical supervision
- 2-day rotations in the Emergency
Department for ward staff to familiarise
them with emergency procedures
- ongoing accreditation for Advanced
Cardiac Life Support, Paediatric Life
Support and IV cannulation (insertion of
intravenous lines, commonly known as
‘drips’, used for giving medications,
fluids, etc)
- a wide range of in-service courses such
as Electrocardiogram (ECG) interpretation
(an ECG is a test that measures heart
rhythm)
- provision of learning packages in the
management of burns, difficult intubation
(insertion of breathing assistance
apparatus), spinal trauma management
and other emergency medicine issues
- ongoing education in the use of equipment
such as defibrillators (equipment used to
shock the heart into normal rhythm)
- education and accreditation to enable
nurses to manage pain while patients are
waiting to be seen by a doctor.

31 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
S T A Y I N G W E L L . . . A W A Y F R O M A C R I S I S For some people with chronic diseases, theEmergency Department becomes a homeaway from home. Breathing problems, chestpain, blood sugar disturbances and manyother symptoms of chronic illness can bringpeople into EDs – repeatedly.
It’s far better to help people successfullymanage these chronic conditions so theydon’t become emergencies.
This goal is the basis for a new partnershipbetween Rosebud Hospital and PeninsulaCommunity Health Service (PCHS). The two
agencies began collaborating in February2004 with the hospital referring many ED‘regulars’ to ‘Live Well’, which is part of theMornington Peninsula Chronic IllnessManagement and Support Program at PCHS.‘Live Well’ aims to enhance client self-management skills and build partnershipsacross the community. An integral part of thisis the Better Health Self-Management Courseand ongoing support for clients to improvelifestyle habits, manage illness and stay well.
T H E F A S T L A N EFrom Friday night to Monday evening is thebusiest time at the Frankston EmergencyDepartment up until now. People triaged as
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun0%
10%20%30%40%50%60%70%80%90%
100%110%
Previous Year DHS ThresholdActual
Category 1-% of Patients Seen Immediately
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun0%
20%
40%
60%
80%
100%
120%
Previous Year DHS ThresholdActual
Category 2 -% of Patients Seen in 10 Minutes
Emergency Department Triage (Initial review of patient to determine theseriousness of the condition and the urgency of treatment).
Category
1
2
3
4
5
Description
Life Threatening
Emergency
Urgent
Semi-Urgent
Non-Urgent
Examples
Cardiac Arrest, Respiratory Arrest, Ongoing seizure
Chest Pain, Acid Splash to eye, Major fracture
Persistent vomiting, Moderate shortness of breathModerate limb injury
Mild bleeding, Swollen hot joint, Sprained ankle
Small abrasions, Change wound dressings,Immunisation
Time to be Seen
Immediately
Within 10 minutes
Within 30 minutes
Within one hour
Within two hours
Responding to Emergencies
These graphs illustrate Peninsula Health’s performance against Department of Human Services targets for the year 2003 - 2004 and show that we metour Emergency Department targets for last year with the exception of the month of August 2003 in Category 4.
Category Four or Five (see chart) could expectto spend a very long time in the waiting room.The Streamline Service identifies patients whohave a single simple, easily identifiablecondition – such as a minor laceration – andguides them through a speedier processstaffed by doctors including generalpractitioners. Strategies such as nursesprescribing pain relief and nurse initiated x-rayis helping staff treat 30% of Category Four andFive within 80 minutes. This, in turn, reduceswaiting times for Emergency patients overall.
S T R A T E G Y G E T S T H E G R E E NL I G H T‘Traffic Lights’ is a new system that has beenused in the Emergency Department sinceJanuary. It requires junior medical officers toconsult with senior medical staff beforeordering certain pathology tests and x-rays.This is achieving two positive outcomes:
1) By discussing which test are mostappropriate junior medical officers haveincreased opportunities to learn fromsenior doctors
2) patients have to undergo only tests thattarget their specific symptoms

Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun0%
20%
40%
60%
80%
100%
Previous Year DHS ThresholdActual
Patients admitted to wards < 12hours
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Previous Year DHS ThresholdActual
Category 4 -% of Patients Seen in 60 Minutes
P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 32
I N T H E P I P E L I N EPeninsula Health is preparing to install apneumatic tube system that will connect theFrankston Hospital Emergency Departmentwith the Pharmacy and the PathologyLaboratory. Staff will be able to transportspecimens and medications in less time, withgreater security, using fewer staff.
H A V E W E G O T Y O U R N U M B E R ?Emergency ambulance response is a fast-paced, high-tech process that can beundermined by something very simple –
if your house number can’t be seen it can bedifficult to find you. So our Peninsula HealthSouthern Community Advisory Committee,working with ambulance, emergency andpublic relations staff, handed out fliers onOpen Day and put notices in shop windowsadvising people to make their house numbersclear. The group even walked the streets,dropping leaflets in mail boxes of houses notvisibly numbered. A sample of these houseswill be monitored to see if homeownersrespond to the alerts.
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Previous Year DHS ThresholdActual
Category 5 -% of Patients Seen in120 Minutes
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun0%
20%
40%
60%
80%
100%
Previous Year DHS ThresholdActual
Category 3 -% of Patients Seen in 30 Minutes

On Monday March 22nd Mrs Winters trips over a rug at homeand is unable to walk or bear weight because of intense painin her hip and leg.
She presses the button on the pendant she wears around herneck, and the monitor at the Mount Eliza Personal Alarm CallService contacts the ambulance service for her. MetropolitanAmbulance Service responds and while attending to her, theofficers ring Frankston Hospital’s Response AssessmentDischarge (RAD) team. As the ambulance takes Mrs Wintersto the hospital’s Emergency Department, a RAD team memberarrives at the home to assist Mr Winters.
During her stay in the Orthopaedic Ward, Mrs Winters is assessed bythe Aged Care Liaison Nurse and the Rehabilitation Consultant to seewhat services she might need when she’s discharged. It’s during thistime on the ward that she is diagnosed with Parkinson’s Disease. Shereceives a referral to the Movement Disorders Clinic at RosebudRehabilitation Unit to help her manage the symptoms of her illness.
Meanwhile, Mr Winters is referred by ACAS to Domiciliary Care who will see what aids he needs to function at home. He settles intoLotus Lodge Hostel, where he receives care and support from the staff.
The RAD team refers Mr Winters tothe ACCESS service in Aged Care,who arrange for the Aged CareAssessment Service (ACAS) to visitMr Winters at home. They judge he’llneed Low Level Care. EmergencyRespite Care is arranged for himthrough the Carer Respite Centre andhe’s taken to Lotus Lodge Hostel tostay until Mrs Winters returns home.
Partnerships within Peninsula Health
are very flexible, forming and reforming
to meet the unique needs of each
patient.
Every day hundreds of professionalpartnerships within Peninsula Healthhelp deliver quality care to everyoneusing our services.
When these alliances progress sosmoothly that the consumer haswhatever care s/he needs when s/heneeds it without a maze of red tape andclosed doors, we call it seamless care.
To illustrate this seamless continuity ofcare and to highlight the partnershipsthat support it, we are creating a typicalcase study. Showing the affiliationsbetween our two feature services –Emergency and Rehabilitation, Aged &Palliative Care – we present ‘Jim andAnna Winters’. This storyboard is posed(our special thanks to auxiliary membersSyd Wayling and Thelma Thomas), but itrepresents what would probably takeplace if an elderly woman broke her hip.In this scenario the woman’s husbandhas physical disability and memory lossfollowing a stroke. The couple resides athome in Dromana where Mrs Winters,with extensive community supports, isthe primary carer for her husband.
33 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
Five days after her surgery MrsWinters is transferred to theRosebud Rehabilitation Unit (RRU)where she receives intensiverehabilitation to prevent furtherfalls. She recovers at the RRU forthree weeks. Post Acute Care stafforganise some home help who willassist Mrs Winters with showeringthree times a week at home.
PartnershipsP R O M O T E C O N T I N U I T Y O F C A R E
1
6 7
2
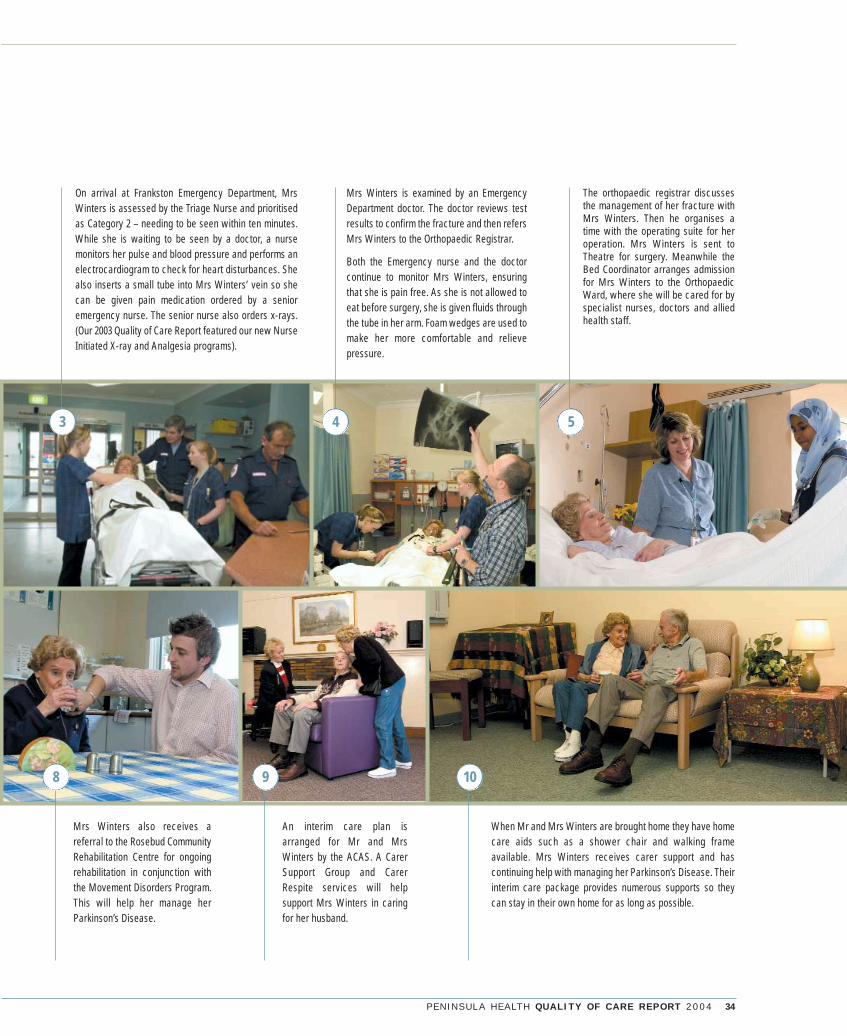
P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 34
Mrs Winters also receives areferral to the Rosebud CommunityRehabilitation Centre for ongoingrehabilitation in conjunction withthe Movement Disorders Program.This will help her manage herParkinson’s Disease.
When Mr and Mrs Winters are brought home they have homecare aids such as a shower chair and walking frameavailable. Mrs Winters receives carer support and hascontinuing help with managing her Parkinson’s Disease. Theirinterim care package provides numerous supports so theycan stay in their own home for as long as possible.
On arrival at Frankston Emergency Department, MrsWinters is assessed by the Triage Nurse and prioritisedas Category 2 – needing to be seen within ten minutes.While she is waiting to be seen by a doctor, a nursemonitors her pulse and blood pressure and performs anelectrocardiogram to check for heart disturbances. Shealso inserts a small tube into Mrs Winters’ vein so shecan be given pain medication ordered by a senioremergency nurse. The senior nurse also orders x-rays.(Our 2003 Quality of Care Report featured our new NurseInitiated X-ray and Analgesia programs).
Mrs Winters is examined by an EmergencyDepartment doctor. The doctor reviews testresults to confirm the fracture and then refersMrs Winters to the Orthopaedic Registrar.
Both the Emergency nurse and the doctorcontinue to monitor Mrs Winters, ensuringthat she is pain free. As she is not allowed toeat before surgery, she is given fluids throughthe tube in her arm. Foam wedges are used tomake her more comfortable and relievepressure.
The orthopaedic registrar discussesthe management of her fracture withMrs Winters. Then he organises atime with the operating suite for heroperation. Mrs Winters is sent toTheatre for surgery. Meanwhile theBed Coordinator arranges admissionfor Mrs Winters to the OrthopaedicWard, where she will be cared for byspecialist nurses, doctors and alliedhealth staff.
An interim care plan isarranged for Mr and MrsWinters by the ACAS. A CarerSupport Group and CarerRespite services will helpsupport Mrs Winters in caringfor her husband.
8 9 10
3 4 5
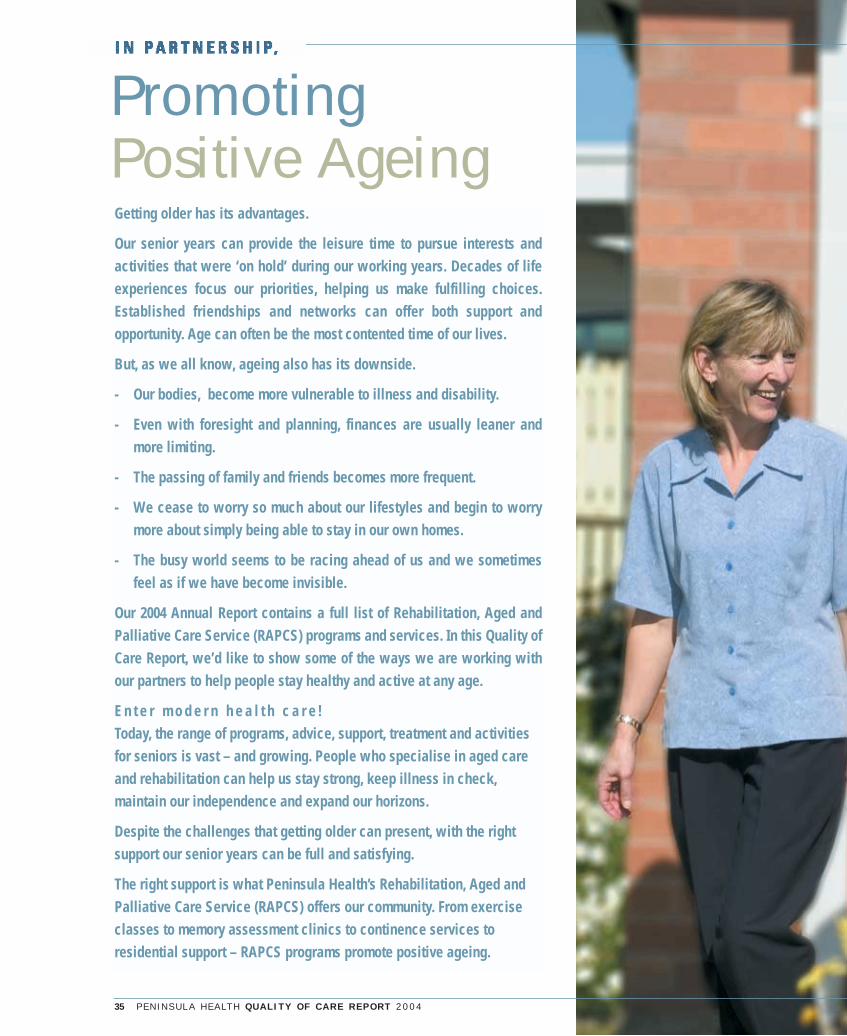
35 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
PromotingPositive AgeingGetting older has its advantages.
Our senior years can provide the leisure time to pursue interests andactivities that were ‘on hold’ during our working years. Decades of lifeexperiences focus our priorities, helping us make fulfilling choices.Established friendships and networks can offer both support andopportunity. Age can often be the most contented time of our lives.
But, as we all know, ageing also has its downside.
- Our bodies, become more vulnerable to illness and disability.
- Even with foresight and planning, finances are usually leaner andmore limiting.
- The passing of family and friends becomes more frequent.
- We cease to worry so much about our lifestyles and begin to worrymore about simply being able to stay in our own homes.
- The busy world seems to be racing ahead of us and we sometimesfeel as if we have become invisible.
Our 2004 Annual Report contains a full list of Rehabilitation, Aged andPalliative Care Service (RAPCS) programs and services. In this Quality ofCare Report, we’d like to show some of the ways we are working withour partners to help people stay healthy and active at any age.
E n t e r m o d e r n h e a l t h c a r e !Today, the range of programs, advice, support, treatment and activitiesfor seniors is vast – and growing. People who specialise in aged careand rehabilitation can help us stay strong, keep illness in check,maintain our independence and expand our horizons.
Despite the challenges that getting older can present, with the rightsupport our senior years can be full and satisfying.
The right support is what Peninsula Health’s Rehabilitation, Aged andPalliative Care Service (RAPCS) offers our community. From exerciseclasses to memory assessment clinics to continence services toresidential support – RAPCS programs promote positive ageing.

Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 36
O N T H E M O V EThere are plenty of hurdles for people livingwith Parkinson’s Disease. Muscles are oftenrigid, weak and slow to respond. Walking,talking and swallowing can be difficult, andsufferers can be embarrassed by tremors,drooling or the inability to show facialexpressions.
The condition is more prevalent as we ageand, with a higher than average proportion ofolder people on the Peninsula, a localprogram for people with movement disorderswas needed. For years these consumers havehad to travel to Cheltenham or Brighton to finda program that specialised in the full range ofservices their conditions require, so inNovember 2003 Peninsula Health establisheda Movement Disorders Program.
Currently the program offers four inpatientbeds and an assessment-only outpatientclinic. Treatment and ongoing support isfocused on medication management,rehabilitation and education for clients andcarers. A doctor specialising in geriatrics(aged care medicine) and rehabilitationmedicine, along with a speech pathologist,occupational therapist, physiotherapist, nurseand social worker provide therapy andsupport. Staff from the Rehabilitation in theHome, Community Rehabilitation, Domiciliaryand Residential Outreach Support servicesalso assist clients. Soon the partnership isexpected to include the ‘Staying Well’program at Peninsula Community HealthService.
In the first six months the clinic treated 43patients and currently about 70 patients arereceiving care.
Michael Court Hostel resident Mr John German takes a strollamong the Spring flowers in the hostel gardens as he chatswith Nurses Karen Harrin (L) and Shirley Temple (R).
37 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
R O S S T O T H E R E S C U EFor some older people, a residential carefacility (RCF) is home. Most of these in ourregion are bright, active, comfortable placeswhere residents feel secure in the careprovided and grateful for the companionshipof people their age. So it’s distressing forresidents to have to leave ‘home’ to go into hospital.
A new program at Peninsula Health, theResidential Outreach Support Service (ROSS),has been set up to help manage residentshealth in the residential environment. Inpartnership with RCFs, residents’ families andGPs, the ROSS team responds to situationsthat can be resolved without admission of theresident to hospital.
Figures show the program definitely works. Of the referrals to ROSS in the first six months of 2004:
• 48% were managed where they live anddid not require a hospital visit
• 14% were identified as at risk of futurehospital admissions and with ROSS helphave not re-presented to the EmergencyDepartment
• 4% were assessed by ROSS as needingadmission to hospital.
One recent case involved a 91 year oldwoman with mild dementia who was living ina hostel. The lady had a change in behaviourand became resistant to care, so her GPordered blood tests to rule out an acuteillness. In her aggressive state, the RCF stafffelt they might have to transfer her to theEmergency Department for the tests. Instead,two ROSS team members visited the lady andtook the blood samples for analysis, so theclient didn’t have to endure a distressing tripto hospital.
Whenever it’s possible to provide community-based services, the ROSS team helps elderly residents in care facilities avoidhospitalisation, at the same time reducing thedemand on public emergency services.
R E S I D E N T I A L S A T I S F A C T I O NA 2004 survey of residents in our aged carefacilities and their families registered a 98.3%positive response to “Overall, I am pleasedwith the treatment and care I/my relativereceives”. Asked if they understood theirrights and responsibilities, 91% said they did.
A satisfaction survey in 2003 showed 65% ofrespondents felt that staff had included themin residential care planning. A continuedemphasis on partnership with our consumerspushed that figure up to 79% in the 2004survey.
A T ‘ H O M E ’ W I T H E . R . I . CThere are lots of devices to make daily lifeeasier for people with physical disabilities.From shower chairs to tap turners, equipmenthas been designed to meet nearly everyspecial need.
Now a large range of these supports areavailable to view, try and buy at PeninsulaHealth’s new Equipment Resource andInformation Centre (ERIC). Opened in May atour Mount Eliza site, the centre is set up as ahome environment so clients can trialequipment in a realistic setting. ERIC isstaffed by experienced OccupationalTherapists who will help clients find whatsuits them best – with no commercialpressure.
In ERIC’s first six weeks, 78 people visited andthe numbers continue to rise. So far ERIC hasreceived requests for tours from communitycare organisations, local governmenthomecare workers, the Department ofVeterans’ Affairs, nursing homes and hostels,the Royal District Nursing Service, General Practitioners and TAFE colleges,demonstrating its innovative approach.
S E N I O R S S T A Y I N G B U S Y Residents in our aged care facilities have
trouble finding a free space in their social
calendars these days. To help our resident
seniors stay fit and active, we have introduced
a number of new services during the year.
Along with therapies targeting exercise, fitness,
mobility and strength training, our RAPCS hostels
and nursing homes have put special emphasis on
leisure activities this year. The schedule now
includes theatre nights, bowls, a hair and beauty
salon, aromatherapy, pet therapy, horticultural
therapy and a computer ‘pen pals’ program.
B R U S H I N G U P O N D E N T A LH E A L T HPeninsula Health and Dental Health Victoria(DHV) have formed a partnership to improve oralhealth for our aged residential clients. A dentalhygienist, employed by DHV, visits residents atour Michael Court and Lotus Lodge Hostels,Carinya Residential Aged Care Unit and JeanTurner Community Nursing Home. In addition adentist from Peninsula Health’s domiciliaryservice assesses each resident. The goal of the12 month trial is to ensure each resident has adental care plan developed in consultation withstaff, carers and the residents themselves.Peninsula Health is the only health service inVictoria providing this service to its residents.
P R E S C R I P T I O N P R E P A R A T I O N SRehabilitation is designed to get hospitalisedpeople ready to function well at home. Naturallythis includes walking and personal care routines,home safety arrangements, home help and othersupports.
Now a new element is being added torehabilitation services. In May RAPCS began atrial of ‘self medication’ at the Golf Links Roadrehabilitation unit. The program helps selectedpatients gradually take on responsibility formanaging their medications.
Patients assessed as appropriate for the programstart out with nursing supervision of eachmedication. As they demonstrate they are able tomanage, supervision is decreased to the pointpatients are confidently handling their ownmedications – just as they’ll have to do when theygo home.
So far, all three participating patients havesuccessfully achieved ‘self medication’.
Promoting Positive Ageing

P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 38
One of the greatest threats to the health ofolder people is falls.
Unfortunately, falls and ageing havetraditionally gone together. Frailty,osteoporosis, dizziness, slower reflexes andfailing eyesight have all contributed toincreased risk of falling and sustaining aserious injury. If the fall itself is not fatal, thesubsequent surgery, hospitalisation andweeks of recuperation can often precipitate adecline from which many don’t recover.
Obviously, falls prevention is one of thehighest priorities at Peninsula Health,especially in Aged Care. In fact, our staff areleaders in the field, having developed a rangeof falls prevention tools, manuals andprograms now in use around Australia. Thematerial is included in the Victorian QualityCouncil guidelines issued in August 2004.
Peninsula Health recently established a FallsSteering Committee to monitor falls and fallsprevention initiatives across the whole healthservice.
During this last year a number of PeninsulaHealth initiatives targeted improved agedcare through falls prevention. Among thesewas the development of an Inpatient FallsProgram across all aged care services andstrategies to improve the reporting of falls.
Others include:
R A V E R E V I E W SStatistics clearly show that screeningpatients for falls risk on admission reducesfalls in hospital. In 2004 our Falls PreventionService (FPS) has worked with staff in theunits to increase the number of patients andresidents screened for falls on admission. Theeffort has been extremely successful in ashort time as illustrated above.
In addition, by June 2004 only therecommended Falls Risk Assessment Tool(FRAT) was being used, standardising the fallsassessments across the aged care service.
T R A I N I N G F A L L S T R A I N E R STo ensure that falls prevention expertise wasreadily available in all RAPCS units, The FallsClinical Nurse Consultant conducted atraining course for selected staff. Thespecialised training has qualified thesestudents to train other staff. Now every unit inRAPCS has a dedicated Falls Prevention‘Portfolio Holder’ and a comprehensive fallsquality plan. A Falls Newsletter and displaysin all areas maintain a high profile for thisimportant health care issue.
R E A D A L L A B O U T I TFalls can happen anywhere. To disseminatefalls prevention information as widely aspossible throughout the community, the FallsPrevention Service developed a bookletcalled ‘A Guide to Preventing Falls’. Thebooklet includes a quick falls risk selfassessment, a listing of local services and apull out medical referral for easy access tothe comprehensive Falls Prevention Program.
To date:• 23 local health service providers are using
the booklet with their clients• 1900 older people received the booklets
last year through local health services• 27 health services outside our region are
utilising the booklet.Other community activities promoting fallsprevention include:• a regular Falls Prevention hour on local
community radio – 3RPP• a directory of physical activity
opportunities throughout the community• talks to community groups on how to
prevent falls• Falls Prevention talks to local health
professionals.
C L I N I C S F O R T H E C O M M U N I T YThe Falls Prevention Service offers a FallsSpecialist Clinical Service to assess andassist people at risk of falls in the community.The service was evaluated by the NationalAgeing Research Institute and showed asignificant reduction in clients falling andsuffering injuries. After six months, the reviewshowed that there was a 62% reduction infalls rates among clients participating in theclinics and a 79% reduction in falls thatcaused injury. The study reviewed falls clinicsaround Victoria and showed what PeninsulaHealth has always believed – falls clinicsprevent falls.
RAPCS patients/residents screened for falls on admission
RAPCS patients/residents were reviewed for falls risk at the scheduled review
April 04 June 04
Perc
enta
ge o
f RA
PCS
Resi
dent
s
0
20
40
60
80
100
RAPCS Residents Screened andReviewed for Falls Risk on Admission
Falls Injuries
62% Reduction
79% Reduction
Before FallsClinic Attendance
After FallsClinic Attendance
Num
ber o
f Fal
ls R
epor
ted
05
101520253035
Falls Clinic Impact on Client Falls
P E N I N S U L A H E A L T H V S F A L L S
National Ageing Research InstituteEvaluation of a Minimum Data Set for Victorian Falls ClinicsClinic Report : Peninsula Health, September 2004

39 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
The fact that you are reading this reportindicates that you are interested in healthcare services for the Frankston/MorningtonPeninsula community. If you would like topursue those interests, we would bedelighted for you to contribute in one of thefollowing ways:
• receive our publications, including ourPulse and Peninsula Perspectivesnewsletters, our Annual Report, Qualityof Care Report, Patients’ Rights andResponsibilities brochure and more
• share your opinions, suggestions orconcerns with us
• join one of our auxiliary or volunteergroups
• apply to serve on one of our CommunityAdvisory Committees. Applications areconsidered as vacancies arise
• tell us about your concerns. You can make a complaint, register a complimentor raise a concern by contacting ourCustomer Relations Manager on 9784 7298
• register your interest in participating inone of many focus groups we establisheach year.
Please contact our Quality and CustomerServices Department on 9784 7051 or ourPublic Relations Department on 9784 7821.
Please help us improve our QualityReporting
We try to produce a Quality of Care Report
that is ‘user friendly’ because we write it
primarily for the community. We try to keep
technical medical terminology to a minimum
and to address issues that interest those we
serve. We want all our readers to find the
report interesting and informative, whether
they know what a sphygmomanometer is,
or not.*
A 15 member Quality of Care Report Working
Group helped us select issues, generate
stories and review the drafts of our 2004
Report. The group, which included three
members of our Peninsula Health Community
Advisory Committees as well as staff from
numerous departments, began meeting in
May. Their input produced this report.
Has the 2004 report addressed issues youcare about? Has it answered your questionsin a straightforward manner? Do you feel as ifwe have been as open as possible about ourperformance – the positive and the negative?Were clinical issues presented in a way thatwas easy to understand?
You can help us evaluate how successful wewere in achieving these goals by joining afocus group on the Quality of Care Report.You can be assured you will be listened to.For example, feedback from last year told usour report was easy to read but was too busywith too much material. So this year we haveattempted to tone the presentation down anotch so it’s more inviting and to focus eventighter on measurable outcomes.
Your feedback this year can help produce abetter report next year. If you’d like to help uswith this, please contact our Quality andCustomer Service Unit on 9784 7051.
* It’s the device doctors and nurses use totake your blood pressure.
You are Invited. . .TO BECOME A PARTNER WITH PENINSULA HEALTH IN BUILDING A HEALTHY COMMUNITY
But wait,there’s more.
Staff and Consumers from the Qualityof Care Report Working Group 2004reviewing the final draft.

P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4 40
“(our daughter) was initially terrified at the prospect of staying in hospital, but with the wonderful care of the staff she has had no hesitation whenwe have had to return”. M O T H E R O F PA E D I AT R I C W A R D PAT I E N T *
“Give the nurses more time to spend one on one time witheach patient.Time seems to be a big problem. They all seemso rushed off their feet”. E M E R G E N C Y PAT I E N T *
“I had to have a few tests – scan, ultrasound, x-rays, and each test tooka wait for a whole day. I felt that if these tests had been done quicker Icould have been discharged earlier”. E M E R G E N C Y PAT I E N T *
“Admitted for a day procedure.Very long boring wait withfasting”. E L E C T I V E S U R G E R Y PAT I E N T *
“Took about five hours tocheck out – I thought this wasa little too long”. E L E C T I V E S U R G E R Y
PAT I E N T *
“I was quite impressed with theimprovement since I was herelast”. E L E C T I V E S U R G E R Y PAT I E N T *
“Take televisions out of the wards”. E M E R G E N C Y PAT I E N T *
* Victorian Patient Satisfaction Monitor. Period ending September 2003 (Wave 6)
“The food was great, please thank the cooks”. PAT I E N T *
“Those warm smiles each morning
make one’s day”. R E H A B I L I TAT I O N PAT I E N T *

41 P E N I N S U L A H E A L T H Q U A L I T Y O F C A R E R E P O R T 2 0 0 4
The odds are you and your family will need touse health services at some time, possiblyeven in an emergency.
When you do you will find it much easier if youhave an idea how to get the help you need.
Understanding more about health serviceswill make it easier for you to workproductively with your health team and bebetter able to ask the right questionsregarding your care.
Knowing your rights and responsibilities willhelp you make decisions about your care.
Having more knowledge about health issueshelps you make the best choices for your owngood health.
Confidence in your health providers canreduce stress, promoting well being andcontributing to better recovery.
All in all, there are plenty of good reasons tolearn more about your community’s healthresources. That’s why Peninsula Health has
put together this Quality of Care Report and ismaking it –
- free upon request
- available at the Annual General Meeting in October
- part of its Web Page atwww.phcn.vic.gov.au
- the basis of a four page insert in local press
- a feature on local community radio 3RPP
- part of packages sent to GPs surgeries
- available at local libraries, shoppingcentres, retirement villages, RSLs andcrèches
- handy for members of local ethnic groupsthrough clubs and events.
- available as a spoken version bytelephoning 9784 7821.
So please keep these important health carenumbers close at hand and put our ContactsCard on your fridge .
We are hereF O R Y O U R G O O D H E A LT H

P E N I N S U L A H E A L T H
Q u a l i t y o f C a r e R e p o r t 2 0 0 4
As a member of the
Board’s Community Advisory
Committee, Shannon Anastasio
liaises with people throughout
the community. She gathers
information, opinions, concerns
and suggestions which she
shares with Peninsula Health’s
Board and Staff. Shannon,
mother of four, is an active
fundraiser for children’s
charities.
QUALITY OF CARE REPORT 2004
For a spoken version ring 9784 7821
PENINSULA HEALTH
PO Box 52 Frankston Victoria 3199
ph: (03) 9784 7777
For those outside the MelbourneMetropolitan Area ph: 1800 858 727
web: www.phcn.vic.gov.au
Peninsula Health proudly supports and encourages organ donation.
Australians Donate
Suite 2 Level 3 20-22 Albert Road South Melbourne(03) 9696 0651www.organdonation.org.au
To register, please call:
Australian Red Cross
Blood Service
Victorian Organ Donation Service - LifeGift538 Swanston StreetCarlton VIC 3053Ph: 1300 133 050www.organdonor.com.au
organ donor
Kidney Health Australia
VictoriaPh: 1800 682 531www.kidney.org.au
Right now there are nearly 2,000seriously ill Australians waiting foran organ donation.
So the more people there are whochoose to become organ donors, themore chance these very ill peoplehave to live.
Please consider joining the ranks of Australians on the Organ DonorRegister. If you decide you want yourorgans to save lives, register yourintentions and tell your family aboutyour wishes.
Pledge the gift of life.





























