Embed Size (px)
Citation preview

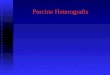
1. Identification of PDX model cohorts with aberrant HER2 genomics and protein expression
While HER2-directed agents are most often used for treating breast cancer, there is increasing evidence that these therapies may be of value in other solid
tumors. Sequencing efforts and immunohistochemistry (IHC) have identified mutations, amplifications, and overexpression of HER2 in ovarian, HNSCC,
NSCLC, melanoma, and GI cancers. PDX models could permit evaluation of HER2 response/resistance mechanisms to optimize therapeutic strategies. In
this pilot study, we evaluated the response of PDX models to HER2-targeted therapies and correlated responses to clinical outcomes.
Patient-derived xenograft (PDX) models expressing HER2 reflect clinical responses to targeted HER2 inhibition1 2 1 1 3Daniel Ciznadija , Amir Sonnenblick , Jennifer Jaskowiak ,Angela Davies , and David Sidransky
1 2 3 Champions Oncology, USA. Sharett Institute of Oncology, Israel. Johns Hopkins University School of Medicine, USA
Incorporation of PDX models into clinical trial strategies could enable real-time analysis of patient treatment outcomes and response biomarkers.
Hypotheses generated from NGS can be tested in clinically-relevant PDX cohorts to improve selection of optimally effective drugs for further development.
Patient-derived xenografts are an important and relevant model for gaining a deeper understanding of drug resistance mechanisms.
A co-clinical trial in metastatic HER2+ breast cancer patients after progression on HER2-directed therapy is planned, incorporating PDX models to further
interrogate mechanisms of resistance in this patient population.
Prospective evaluation of PDX model responses and patient outcomes in response to HER-targeted therapies is ongoing.
Perform extensive integrated genomic analysis and therapeutic screens against anti-HER2 agents to identify potential response biomarkers.
Control
HER2i
We are grateful to the patients who participated in this study and to collaborating oncologists for providing valuable resources and guidance during the course of
this work. For further information, please contact Dr. Angela Davies, Chief Medical Officer ([email protected]).
References: Gao, H et al., Nature Medicine, 21(11): 1318-25. 2015
No alterationLow level gainAmplification Heterozygous deletion
Homozygous deletion
Missense mutation
Truncating mutation
HER2 inhibitors(n=14)
Patient population (n=507)
WES sequencing(gene mutations/CNV)
HER2 IHC staining
HER2i screening(modified RECIST)
A
B
ERBB2
ERBB3
ERBB4
EGFR
ERBB2 amplifications
Future directions
Introduction
Methods
Results
Conclusions
Acknowledgments and References
C
2. Response of PDX models to relevant anti-HER2 therapies stratified by tumor type, HER2 IHC, and HER2 CNV
3. Response of PDX models to HER2-targeted therapy correlates with patient clinical outcomes
B
A
C
Total
Patient response
Positive Negative
PDX response
Total
Positive
Negative
6
0
6 5
2 8
33
11
Number of patients = 9
Clinical accuracy
Positive Predictive Value (PPV)
Analytical accuracy
Sensitivity
Specificity
Negative Predictive Value (NPV)
75% (6/8)
100% (3/3)
100% (6/6)
60% (3/5)
Result
Result
52% - 100%
17% - 93%
36% - 96%
31% - 100%
95% CI
95% CI
5. Uncovering HER2 resistance and identifying new clinical regimens - a PDX case report
4. PDXs allow identification of HER2 resistance pathways when integrated with drug testing
* Includes doublet therapies where
one agent is a HER2-targeted drug.
Intracellular domain Extracellular domain
39 year-old female
HER2+ tumor
Invasive ductal carcinoma
Placed on trastuzumab
No clinical response
Clinical response Clinical response
Metastatic deposits
found in the lungs
Primary and metastatic
sites stable - 5 months
Primary/metastatic
sites regressed
Surgery to de-bulk
Sample from lung metastasis taken
PDX model developed
from lung metastasis
HER2+ confirmed
in PDX model
PDX model fails to
respond to trastuzumab
Correlates with clinical outcome
IHC analysis of PDX model shows it expresses
p95HER2, which lacks the extracellular domain
that trastuzumab needs to bind receptor
Trastuzumab resistance
retained in new clone
PDX model treated simultaneously
with same regimen to develop
lapatinib/capecitabine resistant clone
Patient receives
lapatinib/capecitabine
Patient on
Nab-paclitaxel
Lapatinib inhibits HER2 by
binding intracellular ATP-pocket in
kinase domain, inhibiting auto-phosphorylation
Control
Trastuzumab
Nab-paclitaxel
Day
3T
um
or
volu
me (
mm
)
0 147 210
800
1600
2400
28 35
Control
Lapatinib/Capecitabine
3T
um
or
volu
me (
mm
)
0 73 100
500
250
750
1000
14 2117
Day
Control
Trastuzumab
Day
3T
um
or
volu
me (
mm
)
0 2010 300
1000
500
2000
1500
2500
40 50
A
B
C
Responsive to Nab-paclitaxel
TrastuzumabTrastuzumab emtansine Lapatinib Trastuzumab/PertuzumabPertuzumab Trastuzumab emtansine/PertuzumabAfatinib
0 200 400 600 800 1000 1255
Tyrosine kinase domain C-terminal tailGrowth factor
receptor domainReceptor L
(ligand binding)Receptor L
(ligand binding)Furin-like
cysteine-rich
R74H
R143Q
S310F
P391fs
S463N
P489L
L535F
V666fs R678Q
P699S
L726I
I767M
V842I
E930D
D982fs
Q984fs Q1028K
P1074A
S11
07fs
A1216D
SNV DeletionsERBB2 (n=20/507 models)
n=507 models
Breast
+++
Melanoma Colorectal Breast
++ + -
Esophageal Colorectal Pancreatic NSCLC Gastric ColorectalEsophageal Breast
A
BRC
BRC
BRC
BRC
BRC
BRC
BRC
BRC
BRC
BRC
BRC
BRC
BRC
BRC
BRC
BRC
BRC
BRC
BRC
CRC
CRC
CRC
CRC
CRC
CRC
CRC
CRC
CRC
CRC
CRC
NSC
LCESO
ESO
PANC
PANC
PANC
H&N
H&N
GBM
CHOL
GAST
GAST
GAST
GAST
100
75
50
25
-50
-25
-75
-100
Be
st a
vera
ge
% t
um
or
volu
me
ch
an
ge
0
Bars marked with an asterisk represent the median of response for models tested against the same agent multiple times
CR
PR
SD
PD
Modified RECIST (PDX response)
By tumor type (n=34)
Breast Breast Breast BreastBreast BreastColorectalColorectal H&N H&NCholangio
Patient
PDX model
PR CRSDPD
Trastuzumabemtansine
LapatinibCapecitabine
VinorelbineTrastuzumab
AfatinibMethotrexate
AfatinibLapatinib
Capecitabine Trastuzumab TrastuzumabTrastuzumab
emtansineTrastuzumab
emtansineTrastuzumab
emtansine
Responded
By HER2 CNV status (n=25)
Am
pAm
pAm
pAm
pAm
pAm
pAm
pAm
pAm
pAm
pAm
pAm
pAm
pAm
pAm
pGai
nGai
nDip
Dip
Dip
Dip
Dip
100
75
50
25
-50
-25
-75
-100
Be
st a
vera
ge
% t
um
or
volu
me
ch
an
ge
0
CR
PR
SD
PD
Modified RECIST (PDX response)
Bars marked with an asterisk represent the median of response for models tested against the same agent multiple times
Am
pAm
pDip
Dip
Dip
Het
Loss+++++ ++ ++++ ++ ++++++ ++++ ++ ++++ +++
+++
+++
+++
+++
By HER2 IHC score (n=18)
No alteration
Low level gain
Amplification
Heterozygous deletion
Homozygous deletion
Missense mutation
Truncating mutation
Inframemutation
PTEN
PIK3CA
MET
IGF-1R
MTOR
AKT1
AKT2
surgeryor
biopsy
PDX models
Patient therapy
Clinical response(RECIST criteria)
Radiologicalmeasurements
Tumor volume calculated by:
2width x length x (p/6)
Patient-PDX
correlations
(A) Models were stained with anti-HER2 antibodies (Dako, USA) and scored by a pathologist for intensity of HER2 expression (using the -/+/++/+++
nomenclature). Representative examples of each HER2 staining score are depicted. (B) OncoPrints (cBioPortal) created from whole-exome sequencing
demonstrating mutations and copy number variations amongst HER2 family members. Models with amplifications and focal gains at the ERBB2 locus are
indicated. (C) Lollipop diagram (cBioPortal) highlighting the mutational spectrum of the ERBB2 gene across twenty PDX models harboring SNVs and indels
at that locus (of 507 sequenced). SNVs are indicated by red circles and focal deletions by blue triangles. No focal amplifications were found.
n=11 correlations
Models with HER2 amplifications
Models staining positive for HER2
Poster #1836