Upload
esther-tirado
View
171
Download
1
Tags:
Embed Size (px)
Citation preview
C H A P T E Rz z z z z z z z z z z z z z z z z z z z z z z z z z z54
Patella Fractures andExtensor Mechanism InjuriesPatella Fractures andExtensor Mechanism Injuries
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Michael T. Archdeacon, M.D.Roy W. Sanders, M.D.
HISTORICAL BACKGROUNDz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Before the beginning of the 20th century, treatment ofpatella fractures was extremely controversial. Nonoperativemethods, usually extension splinting and rest, were mostcommonly used. Results were poor, bony union was rare,and permanent disability was expected.31 As improve-ments in surgical asepsis occurred, two operative solutionsto the problem emerged: arthrotomy with open wiring andpatellectomy. Heineck reviewed 1100 patella fractures andadvised operative treatment over extension splinting forthe following reasons: improved fracture reduction, main-tenance of reduction until union, reestablishment of softtissue continuity, and restoration of the functional integrityof the knee joint.48 Open reduction and wire fixationsubsequently became the treatment of choice for patellafractures.
Although reduction of simple transverse fractures wasmade possible by an open procedure, stable fixationremained difficult. Various materials were tried, includ-ing silver, aluminum, and copper wire; chromic suture;kangaroo tendon; cancellous bone pegs; Achilles tendon;and fascial strips.50 In 1936, Blodgett and Fairchildreported 35 patella fractures treated with open reduc-tion and wire suture; less than 50% had good re-sults.10 They then reported on the use of partial or, incertain cases, total excision of the patella for fracturesand described excellent clinical results.10 A year earlier,Thompson also recommended partial excision of thepatella.100 In the same year as Blodgett and Fairchildsstudy, Brooke published a revolutionary paper on thetreatment of patella fractures by total excision.16 Quot-ing embryologic data to support the vestigial nature ofthe patella, his functional studies showed that postpatellec-tomy limbs were stronger than their normal counterparts.Based on these studies, patellectomy gained significantpopularity.31, 40, 44, 45, 50
This initial enthusiasm was tempered by many ex-perimental and long-term clinical studies that disprovedthe benefits of patellectomy as routine treatment of frac-tures of this bone.* Cohn27 and Bruce and Walmsley18
studied patellectomized rabbits and found degenerativechanges on the femoral condyles. They suggested thatthis complication could occur in humans as well. Haxtonand others presented biomechanical evidence that thepatella served a necessary purpose in the extensor mecha-nism.30, 47, 58, 67, 105, 109 In long-term clinical studies eval-uating patients after total patellectomy, variable resultswere also found.30, 35, 56, 70, 76, 99, 110, 112 These studiesrevealed poor patient satisfaction, decreased quadricepspower, prolonged recovery time, and significant changes inactivities of daily living.35, 89, 99, 112
Treatment of patella fractures with the anterior tensionband principle was first reported in the 1950s.79 Thistechnique was subsequently advocated by the Arbeitsge-meinschaft fur Osteosynthesefragen/Association for theStudy of Internal Fixation (AO/ASIF) group as the treat-ment of choice for transverse patellar fractures.79 Weberand colleagues compared the tension band principle withcerclage and interosseous wire suture in cadavers andfound that modified anterior tension band wiring withretinacular repair gave the most stable fixation of a trans-versely fractured patella.108 Additionally, this construct wasthe only one that allowed early active range of motion ofthe knee.108 Other authors subsequently confirmed thisfact clinically.11, 12, 54, 64
At present, three forms of operative treatment survive:various types of fixation, usually with tension band wiring;partial patellectomy; and total patellectomy. Definitiveindications for each procedure are related to the type of
*See references 18, 27, 30, 35, 47, 56, 58, 67, 70, 76, 89, 99, 105,109, 110, 112.
2013
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 1/32 P 2013 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 1/32 P 2013 BLACK T
fracture encountered, and good results can be expectedwith proper treatment.
ANATOMYz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Skeletal Anatomy
The patella lies deep to the fascia lata and the tendinousfibers of the rectus femoris (Fig. 541A). It is flat androughly ovoid and comes to a rounded point, known asthe apex, on its anteroinferior margin. Its proximal part iscalled the basis (see Fig. 541B).
Wiberg classified patellas into three types based on thesize of the medial and lateral facets.111 In type I, the medialand lateral facets are approximately equal, whereas in typesII and III, the medial facets are progressively smaller thanthe lateral. Baumgartl described a fourth type, the Jagerhutpatella, in which the medial facet is lacking altogether.5
These facets have importance with respect to the functionalanatomy of the patellofemoral joint (see the section Exten-sor Apparatus Biomechanics).
Soft Tissue Anatomy
QUADRICEPS MECHANISM
The quadriceps muscle complex is composed of fourseparate muscles: the rectus femoris, vastus medialis,vastus lateralis, and vastus intermedius (Fig. 542). Classi-cally, the quadriceps tendon is described as trilaminar instructure; it inserts onto the patella with the rectus femorissuperficial, the vastus medialis and lateralis in the middle,and the vastus intermedius deep.67 The actual arrangementis more complex because of blending of the tendons as theyinsert on the patella.86
The rectus femoris is a long fusiform muscle thatassumes the central and superficial position in the quadri-ceps structure.86 The fibers angle 7 to 10 medially in thefrontal plane relative to the shaft of the femur.67 The vastus medialis divides into two parts. The more
proximal fibers are known as the vastus medialis longusand enter the patella at an angle of 15 to 18. The moredistal fibers, the vastus medialis obliquus, enter the patellaat an angle of 50 to 55.67 The fibers of each group aredivided by fascia into separate fascicles. Innervation of thevastus medialis obliquus is by a separate branch of thefemoral nerve.67, 86
The fibers of the vastus lateralis approach the patella atan angle of approximately 30 and terminate more proxi-mally than do the fibers of the vastus medialis. The mostmedial fibers insert into the supralateral edge of the patella,with the more lateral fibers traveling laterally past thepatella. These fibers contribute to the lateral retinaculumand, at their lateral extreme, fuse with the iliotibial tract.
The vastus intermedius lies in a plane deep to the otherthree elements of the quadriceps. Most of the fibers insertdirectly into the superior aspect of the patella. Deep to themajor components of the quadriceps lies the articularisgenus. This muscle is highly variable in occurrence andarises from the anterior aspect of the supracondylar por-
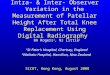
BAFIGURE 541. A, Superficial aspect of the patella, with extensive softtissue attachments indicated by roughened surface. B, Articular surface ofthe patella (see text). Note the extra-articular distal pole occupying asignificant portion of the bones length. The articular surface is dividedinto seven facets by several ridges (see Fig. 541A). A major vertical ridgeseparates the medial from the lateral facets, and a second vertical ridgenear the medial border isolates a narrow strip known as the odd facet. Inaddition, two transverse ridges create superior, intermediate, and inferiorfacets (Bostrom, 1972; Reider et al., 1981).
FIGURE 542. Soft tissue attachments of the patella. Major components ofthe extensor mechanism include the quadriceps tendon proximally andthe patellar ligament (tendon) distally. The medial and lateral retinaculahelp position the patella and can provide active knee extension if theyremain intact after a patella fracture without significant displacement.
2014 SECTION V Lower Extremity
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 2/32 P 2014 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 2/32 P 2014 BLACK T
tion of the femur. It inserts on the joint capsule at thesuprapatellar pouch.
PATELLAR RETINACULUM
The deep investing fascial layer of the thigh is known as thefascia lata. As it spreads over the anterior surface of theknee, its medial and lateral extensions combine withaponeurotic fibers from both the vastus medialis and thevastus lateralis to form the patellar retinaculum, whichinserts directly into the proximal part of the tibia (see Fig.522). The patellofemoral ligamentsdeep transverse fi-bers that are palpable thickenings of the joint capsuleconnecting the patella with the femoral epicondylescomplete the retinaculum.13, 86 In addition, the lateralaspect of the vastus lateralis and the iliotibial tract bothcontribute to the thicker lateral patellar retinaculum.Together, the patellar retinaculum and the iliotibial bandserve as the auxiliary extensors of the knee.13
PATELLAR TENDON
Derived primarily from fibers of the rectus femoris, thepatellar tendon is flat and strong and inserts onto the tibialtubercle. Its average length is slightly less than 5 cm. Thefascial expansions of the iliotibial tract and the patellarretinaculum blend into the patellar tendon as it inserts ontothe anterior surface of the tibia.
ARTERIAL BLOOD SUPPLY
The anterior surface of the patella is covered with anextraosseous arterial ring derived mainly from branches ofthe geniculate arteries28 (Fig. 543). The intraosseousblood supply of the patella is supplied by two systems ofvessels, both derived from this extraosseous vascular ring:the midpatellar vessels, which penetrate the middle third ofthe anterior surface of the patella, and the polar vessels,which enter the patella at its apex.3, 87
The patellar tendon receives its blood supply from twosources. The infrapatellar fat pad supplies the deep surfaceof the patellar tendon with contributions from the inferiormedial and inferior lateral geniculate arteries. The anterioror superficial surface of the tendon is supplied by theretinaculum, which receives its supply from the inferiormedial geniculate artery and the recurrent tibial artery.3
EXTENSOR APPARATUSBIOMECHANICSz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
The principal function of the extensor mechanism of theknee in humans is to maintain the erect position. Ambu-lation, rising from a chair, and ascending or descendingstairs are examples of this ability to overcome gravity.The biomechanical principles necessary for these actionsshould be understood to treat extensor mechanism injuriesrationally.
A moment is a force that produces rotation about anaxis. It is equal to the product of a force and theperpendicular distance from the line of action of that forceto the axis of rotation. This perpendicular distance is themoment arm.91 The force necessary for knee extension(torque) is directly dependent on the perpendicular dis-tance between the patellar tendon and the knee flexion axis(moment arm)58 (Fig. 544A).
Twice as much torque is needed to extend the knee thefinal 15 as to bring it from a fully flexed position to 15.67
To do so, the knee requires a moment arm that increasesduring extension so that it can maintain a constant level oftorque. The patella provides this mechanical advantage bytwo separate mechanisms: linking and displacement.58
As the knee begins extension from the fully flexedposition, the patella functions primarily as a link betweenthe quadriceps and the patellar tendon. This linkingfunction allows for generation of torque from the quadri-ceps muscle to the tibia.58 Maximal forces across thequadriceps tendon have been recorded at 3200 N, whereasthose across the patellar tendon are 2800 N.52 These valuesare between four and five times the standard body weightof 700 N. For young, physically trained men, these forcescan reach up to 6000 N.52
Typically, the linking function occurs in the more flexedpositions. At 135 of flexion, the patella slips into theintercondylar notch. The patellar facets of the femur havean extensive contact area with both the patella and thebroad posterior surface of the quadriceps tendon. Loadbearing shifts to a combination of the patellofemoral andthe tendofemoral areas, with the latter being the greater ofthe two after 90 of flexion.41 Without patellofemoral
FIGURE 543. Blood supply of the patella. Note the extraosseous arterialanastomotic ring, which receives inflow from branches of each of thegenicular arteries. (From Scapinelli, R. J Bone Joint Surg Br 49:563570,1967.)
2015CHAPTER 54 Patella Fractures and Extensor Mechanism Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 3/32 P 2015 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 3/32 P 2015 BLACK T
contact, the moment arm is small41 (see Fig. 544B). From135 to 45 of flexion, the odd facet engages the femur. It isthe only part of the patella that fails to meet the truepatellar facets of the femur and the only part to articulatewith the true tibial surface of the medial femoral condyle ofthe femur.41
From 45 of flexion to full extension, the patella is theonly component of the extensor mechanism that contactsthe femur. It acts to displace the quadriceps tendonpatel-lar tendon linkage away from the axis of knee rotation. Thisaction increases the effective moment arm of the quadri-ceps mechanism and contributes the additional 60% oftorque that is needed to gain the last 15 of knee exten-sion.67 This second action therefore creates a mechanicaladvantage analogous to that of a pulley.58, 109
By displacing the tendon away from the axis of rota-tion, greater excursion of the quadriceps is needed fora given range of motion.109 Theoretically, when perform-ing a patellectomy, a quadriceps-shortening or tubercle-elevating procedure may be performed to take this require-ment into account.
DIAGNOSISz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
History and Physical Examination
Fractures of the patella are diagnosed by obtaining ahistory of the injury, performing a thorough physicalexamination, and acquiring the appropriate radiographicstudies. Completion of these investigations should resultin a final diagnosis that includes the fracture type, thepresence or absence of retinacular disruption, a description
of the wound, if any, and the presence of any associatedinjuries.
The history usually describes a fall from a height, a nearfall, a direct blow to the patella, or a combination of thesemechanisms. Correlation with the mechanism of injuryallows the physician to anticipate the fracture pattern. Ifthe patient has an open wound, the history should includequestions regarding the location of the accident (e.g., athome, in the water, on a farm).
The physical examination should include an evalua-tion of the skin to look for contusions, abrasions, blisters(if treatment has been delayed), and the presence of anopen fracture or an open-joint injury. In patients witha displaced patella fracture, physical examination willreveal a visible or palpable defect between the frag-ments. Significant hemarthrosis usually develops second-ary to the fracture. If a palpable bony defect is presentwith little or no effusion, a large retinacular tear should beexpected.
Knee extension is then evaluated. A tense hemarthro-sis will make this part of the examination extremelypainful for the patient. Arthrocentesis with injection oflidocaine or bupivacaine into the joint is often helpful. Thepatients ability to extend the knee does not rule out apatella fracture and may simply mean that the patellarretinaculum is intact. An inability to extend the knee,however, suggests a discontinuity in the extensor mecha-nism. With a patellar fracture, such inability implies a tearof both the medial and the lateral quadriceps expan-sion.13, 73, 92
Occasionally, a laceration may be noted in proximity toa patella fracture. It may represent an open fracture oran open-joint injury. Because both are surgical emer-gencies, it is imperative to diagnose these injuries early.A simple means of evaluation is the saline load test.A large-bore needle (18 gauge or higher) and a 50-mLsyringe are used to perform joint aspiration. A signifi-cant amount of bloody fluid may be removed, usuallyresulting in relief of pain. The needle is left in place whilethe syringe is removed and filled with saline solution,which is then injected into the knee joint. Any communi-cation between the fracture or joint and the outsideenvironment will become obvious if the saline solutionexits the wound.
After the history and physical examination, radio-graphic evaluation is performed. Once a diagnosis is made,the knee is splinted in a position of comfort (usually slightflexion), iced, and elevated. If the patient requires immedi-ate transfer to the operating room or intensive care unit,portable radiographs will suffice.
Radiographic Evaluation
Radiographic evaluation of the patella includes stan-dard and specialized radiographic techniques, tomography,computed tomography (CT), bone scanning, and magneticresonance imaging (MRI). When time permits, standardradiographic evaluation of the uninvolved knee should beobtained. Such imaging affords the physician a comparison
A
BFIGURE 544. Mechanical role of the patella. A, The patella increases themoment arm of the extensor mechanism (i.e., the distance between thevector of applied force and the knees instant center of rotation). B, Afterpatellectomy, this moment is decreased, and thus extensor force iseffectively diminished. (A, B, Redrawn from Kaufer, H. J Bone Joint SurgAm 53:15511560, 1971.)
2016 SECTION V Lower Extremity
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 4/32 P 2016 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 4/32 P 2016 BLACK T
view for evaluation and assists in any preoperative plan-ning that might be necessary.
STANDARD VIEWS
AnteroposteriorThe normal anteroposterior (AP) radiograph is taken withthe patient standing, but this position is impossible for apatient with an acute fracture. Instead, the film must betaken with the cassette underneath the knee of a supinepatient. The extremity should be aligned so that the patellapoints straight up. Such alignment is especially importantin a patient with an ipsilateral femoral shaft fracture. If thepatient has a large hemarthrosis creating moderate kneeflexion, the x-ray beam must be angled accordingly. Be-cause of the possibility of concomitant occult ipsilateral leg
injuries, the largest cassette possible (14 17 inches)should be used.
Evaluation of the AP radiograph requires analysis ofseveral factors. Patella position should be assessed; thepatella should lie in the midline of the femoral sulcus. Inaddition, patellar height should be examined; the inferiorpole of the patella is normally located just above a linedrawn across the distal profile of the femoral condyles (Fig.545A).
At times mistaken for a patellar fracture, a bipartite ortripartite patella is a developmental residuum from avariation in which the patella arises from two or moreossification centers that fail to fuse (Fig. 546). It is usuallya bilateral finding. The most common type is a bipartitepatella, in which a bony mass is located in the upper outerquadrant of the patella. It is separated from the mainpatellar mass by opposing smooth bony surfaces. The
A
D
C
B
FIGURE 545. Radiographic indicators of an abnormal patel-lotibial relationship. An excessive distance between the distalpole of the patella and the tibial tubercle may representdisruption of the patellar ligament or chronic patella alta.A, On the anteroposterior view, the distal pole of the patellalies no more than 20 mm above the plane of the femoralcondyles. B, When the knee is flexed 90, a lateral radiographshould show that the proximal pole of the patella lies posteriorto the anterior surface of the femoral shaft. C, On a lateralradiograph, the length of the patellar ligament (from the distalpole of the patella to the tibial tubercle) approximates that ofthe patella. If the patella-to-patellar ligament ratio is less than0.8, the patella is excessively high. D, Blumensaats line, theplane of the residual distal femoral physeal scar, normallyprojects near the distal pole of the patella (see Fig. 547).(AD, Redrawn from Resnick, D.; Niwayama, G. Diagnosisof Bone and Joint Disorders, 2nd ed. Philadelphia, W.B.Saunders, 1988.)
2017CHAPTER 54 Patella Fractures and Extensor Mechanism Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 5/32 P 2017 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 5/32 P 2017 BLACK T
condition is generally asymptomatic and requires no treat-ment, but it can cause confusion when treating patientswith a history of injury to the knee area.73 In such cases, aradiograph of the opposite patella should be obtained.Invariably, a similar pattern will be found, thus making thediagnosis. A true unilateral bipartite patella is very rare andmay represent an old marginal patella fracture.32
LateralAlthough a lateral radiograph is easy to obtain, attention todetail is necessary because rotation of the limb will negatethe benefits of this view. The proximal end of the tibia mustbe seen so that rupture or avulsion of the patellar ligamentcan be excluded (Fig. 547). This view of the knee willportray a transverse or comminuted patellar fracture ratherdramatically. Unfortunately, however, it may prevent dis-covery of more subtle findings.
With the knee flexed 90, the proximal patellar polenormally lies posterior to the anterior surface of the femur;with a ruptured patellar tendon, the proximal part of thepatella rests anterior to the anterior surface of the femoralshaft (see Fig. 545B). The most reliable means of assessingpatellar height is the method of Insall and co-workers,21, 55
which involves determination of the ratio of the greatestdiagonal patella length to patellar tendon length. In anormal subject, this ratio is 1.0. A ratio less than 1.0suggests a high-riding patella (patella alta) or rupture of thepatellar tendon. Up to 20% variance is normal (see Fig.545C). Blumensaats line, the plane of the residual distalfemoral physeal scar, normally projects near the distal poleof the patella (see Fig. 545D).
TangentialTangential or axial (sunrise, sunset, or skyline) views of thepatella are primarily used in the analysis of patellofemoraldisorders (Fig. 548). In fractures of the patella, thesestudies aid the surgeon in diagnosis of longitudinal (i.e.,marginal or vertical) fractures and osteochondral defects.
The three most common views are those of Hughston,Laurin, and Merchant.21, 74 Although all give approxi-mately the same information with respect to patellofemoralcongruence, the views of Hughston and Laurin are imprac-tical in a trauma setting. The former requires that thepatient be prone, whereas the latter requires patient partic-ipation.
Merchant and associates in 1974 described a method ofobtaining an axial view of the patella74 (see Fig. 548A).The patient is placed supine on the x-ray table with theknees flexed 45 over the end. The knees are elevatedslightly to keep the femurs horizontal and parallel with thetable surface. An x-ray beam is angled 30 from thehorizontal. The cassette is then placed about 1 ft belowthe knees and perpendicular to the x-ray beam. Thismethod is simple, easily reproducible by x-ray technicians,and able to obtain accurate radiographs in a patient with apainful, partially flexed knee secondary to hemarthrosis(see Fig. 548B).
TOMOGRAPHY
The principal use of tomography in the evaluation of bonyinjuries about the knee is in the detection of occultfractures. Apple and associates recommended tomographyover bone scanning in these cases, especially for stressfractures and in elderly patients with osteopenia andhemarthrosis.2 In their series, routine radiographs werenegative in all cases; 71% of the fractures were identified
FIGURE 547. Lateral radiograph of a normal patella. (From Resnick, D.;Niwayama, G. Diagnosis of Bone and Joint Disorders, 2nd ed.Philadelphia, W.B. Saunders, 1988.)
FIGURE 546. Radiograph of a bipartite patella demonstrating thecharacteristic proximal lateral ossification center with a curved, well-demarcated lucent zone of separation.
2018 SECTION V Lower Extremity
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 6/32 P 2018 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 6/32 P 2018 BLACK T
with tomography versus only 30% with bone scans.2
Tomography may also be of benefit in the evaluation ofpatellar nonunion or malunion.107
Although theoretically of benefit to the diagnostician,CT scanning is rarely used for evaluation of an isolatedpatella fracture. It is generally performed as an incidentalstudy during the evaluation of distal femoral or proximaltibial fractures. The information presented rarely adds tothat obtained with more conventional techniques. CT mayaid the surgeon in evaluation of articular incongruity incases of nonunion, malunion, and patellofemoral align-ment disorders (Fig. 549).
BONE SCANNING
Scintigraphic examinations with technetium-labeled phos-phate compounds are helpful in the diagnosis of stressfractures, although our preference would be to obtain plaintomograms. A bone scan may also be useful with indium-labeled leukocytes or gallium scanning for the assessmentof patellar osteomyelitis.
MAGNETIC RESONANCE IMAGING
MRI has become increasingly useful in the early diagnosisof extensor mechanism injuries. A normal quadricepstendon has a laminated appearance on MRI studies,whereas the patellar tendon has a homogeneous low signalintensity. The normal patella has the signal intensity ofcancellous and cortical bone.115
Injuries of all types can produce hemorrhage andedema, which cause increased signal intensity on T2-weighted images. Patella fractures and avulsions of thetibial tubercle do not generally require MRI evaluation butwill result in changes in marrow signal intensity.115
Complete rupture of the quadriceps tendon is welldemonstrated by MRI, and transection of all layers of thetendon is diagnostic of a complete rupture. In the moreunusual patellar tendon ruptures, MRI evaluation showsabsence of distinct margins and increased signal intensitywithin the patellar tendon.115
Dislocation of the patella produces a characteristicpattern of change on MRI that allows diagnosis of this
FIGURE 549. Computed tomographic scan of a fractured patella. Notethe extent of comminution, as well as the secondary sagittal fracture andthe resulting articular incongruity.
Camera
Nose
X-ray plate
A
FIGURE 548. A, A Merchant tangential view of the patellais made with the knee flexed 45 and the radiographexposed as shown (see text). B, A skyline radiographexposed in this fashion demonstrates the patellofemoralrelationship, which may be made incongruent by quadri-ceps contraction. The image on the left is normal; that onthe right shows lateral subluxation. (B, From Resnick, D.;Niwayama, G. Diagnosis of Bone and Joint Disorders, 2nded. Philadelphia, W.B. Saunders, 1988.)
2019CHAPTER 54 Patella Fractures and Extensor Mechanism Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 7/32 P 2019 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 7/32 P 2019 BLACK T
injury even if the patient is initially seen after relocation ofthe patella.104 These findings include contusion of thelateral femoral condyle (manifested as low signal intensityon T1-weighted images), tear of the medial retinaculum,and joint effusion.
FRACTURE CLASSIFICATIONz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
The three major categories of patella fractures are trans-verse, stellate, and vertical. Transverse fractures that areproximal (basal) or distal (apical) are termed polar. Because
these usually extra-articular disruptions of the quadricepspose different therapeutic challenges, they are classifiedseparately13, 68 (Fig. 5410). Wide variations within eachfracture pattern have prevented the creation of a usefulclassification scheme.11, 13, 92 Because of this difficulty,most authors have reviewed long-term results according totreatment rather than fracture type.11, 13, 14, 25, 68, 82, 92, 100
For the purposes of this chapter, existing classifi-cation schemes were combined for better understand-ing11, 13, 68, 100 (Table 541). Although the terms stellateand comminuted are interchangeable in much of thepublished literature, we recommend distinguishing com-minuted transverse fractures, which often have retinaculardisruption, from stellate patellar fractures, which are asso-ciated with an intact retinaculum.
Nondisplaced Fractures
STELLATE
Stellate fractures of the patella are the result of a directcompressive blow that forces the bone against the femoralcondyles. Damage to the articular cartilage of the femoralcondyles and the creation of osteochondral fragments mayoccur and must be ruled out.19 Typically, well over half(65%) of these fractures are nondisplaced. In these frac-tures, the blow is insufficient to tear the patellar retinacu-lum, and active extension of the knee is therefore possible.Displacement between fragments is, by definition, less than3 mm, and displacement between the articular surfaces,less than 2 mm. Unless an osteochondral fragment ispresent and requires arthrotomy or arthroscopy, nonopera-tive therapy is indicated (Fig. 5411).
TRANSVERSE
Transverse fractures of the patella are the result of a tensilestress applied to the extensor mechanism. Typically, 35%or more of all transverse patellar fractures are nondis-placed.1, 13 Damage to both the femoral and the patellararticular surface is minimal,89 and the force is usually
B
A
C
DFIGURE 5410. Examples of patellar fractures. A, Undisplaced fracturesmay have any degree of comminution, but fragments are displaced nomore than 3 mm. The articular surface as seen on the lateral view shouldhave a step-off of no more than 2 mm. B, Displaced transverse fracturewith comminution of the apical pole. C, Displaced transverse fracturewith comminution of both the apical and basilar poles. D, Highlycomminuted, highly displaced fracture.
TABLE 541z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Fracture Classication
A. Nondisplaced fractures1. Stellate2. Transverse3. Vertical
B. Displaced fractures1. Noncomminuted
a. Transverse (central)b. Polar
1. Apical2. Basal
2. Comminuteda. Stellateb. Transversec. Polard. Highly comminuted, highly displaced
C. Fractures associated with bonepatellar tendonbone autograft1. Longitudinal2. Transverse
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
2020 SECTION V Lower Extremity
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 8/32 P 2020 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 8/32 P 2020 BLACK T
insufficient to tear the medial and lateral patellar retinacu-lum.13, 42, 73, 89, 92 As a result, the patient retains the abilityto extend the knee. In addition, the intact soft tissueenvelope maintains patellar alignment; typically, less than3 mm of fragment diastasis and 2 mm of articular incon-gruity exist. If these conditions are met, nonoperativetreatment is suggested (see Fig. 5410).
VERTICAL
Vertical fractures (marginal or longitudinal fractures), con-trary to earlier reports, are a common type of patellarfracture, with a combined incidence of 22% (384/1707) inseveral large series.9, 14, 32 The fracture may be caused bydifferent mechanisms. Dowd stated that direct compres-sion of the patella in a slightly hyperflexed knee creates thisfracture.32 In Bostroms series, lateral avulsions accountedfor more than 75% of all vertical fractures.14 Bony separa-tion is most commonly found at the junction of the middleand lateral thirds of the patella; less commonly, a medialpole avulsion may occur.
Clinically, the patient has a somewhat painful knee anda mild effusion. Full extension of the joint is possiblebecause the patellar retinaculum is intact.9, 14, 32 A diastasisof greater than 3 mm is most unusual.13, 14 The fracturemay be missed on standard radiographs, and thereforeaxial views are usually necessary to make the diagnosis.9, 14
If the defect is seen on the AP radiograph, it may easily bemistaken for a bipartite patella, so radiographs of theopposite limb should be obtained. Because the fracturefragments are minimally displaced and the patellar retinac-ulum remains intact, these fractures are best treated nonop-eratively.
Displaced Fractures
NONCOMMINUTED
Transverse/MidpatellarDisplaced fractures account for slightly more than half(52%) of all noncomminuted transverse fractures of the
patella. The diagnosis is made in a patient with loss ofactive extension of the knee (after aspiration), more than3-mm separation between fracture fragments, or an articu-lar step greater than 2 mm.810, 73, 92 These findingssuggest retinacular disruption and joint incongruity. Eitherfinding warrants operative repair (Fig. 5412).
Some patients may have a gap of 4 to 5 mm betweenfracture fragments but can extend their leg actively. McMas-ter warned of nonunion in these patients when treatedconservatively.73 Bostrom, in reviewing the results of hisand other large published series, however, concluded thatactive extension implied retinacular continuity and thatthese patients could heal satisfactorily without surgery.13
We concur with his advice.
PolarPolar fractures of the patella are transverse fractures occur-ring either proximal or distal to the patella equator andtaking varying amounts of bone. Proximal, or basal pole,fractures imply avulsion of the quadriceps mechanismfrom the patella. The amount of accompanying retinacularrupture determines the patients ability to extend the leg.Displacement is extremely rare and was seen in less than4% of patients in several large series.13, 92
Distal, or apical, fractures are bony avulsions of theproximal patellar tendon (Fig. 5413). These fractures,which occur toward the distal margin of the retinacu-lum, are almost invariably associated with loss of kneeextension. As a result, displacement in apical fracturesis almost three times as common (11.5%) as in basalinjuries.
COMMINUTED
StellateA result of direct compression, comminuted stellate frac-tures usually exhibit displacement with varying degrees ofcomminution.19 Although the patellar retinaculum is in-tact, operative intervention is indicated because of existingarticular incongruity (Fig. 5414).
FIGURE 5411. Nondisplaced stellate fracture of the patella. Radiographic projections are anteroposterior (A), oblique (B), and lateral (C).
2021CHAPTER 54 Patella Fractures and Extensor Mechanism Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 9/32 P 2021 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 9/32 P 2021 BLACK T
FIGURE 5413. Displaced distal polar frac-ture of the patella. A, Anteroposteriorradiograph. B, Lateral radiograph.
FIGURE 5414. Displaced stellate fracture of the patella. A, Anteroposterior view. The fracture is difficult to see. B, Lateral view. The fracture is apparent,but displacement appears to be only moderate. C, A skyline radiograph clearly indicates displacement and incongruity of the articular surfaces.
FIGURE 5412. Displaced transversefracture of the patella. A, Anteroposteriorradiograph. B, Lateral radiograph.
2022 SECTION V Lower Extremity
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 10/32 P 2022 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 10/32 P 2022 BLACK T
Transverse/PolarThese comminuted fractures exhibit varying degrees ofcomminution of one major patellar fragment. Upper frag-ment comminution is usually accompanied by one or twoadditional fracture lines that are minimally displaced.Lower fragment comminution is generally more severe andmay be accompanied by upper pole comminution.11, 13
Comminution is much more prevalent in the lower polethan the upper pole.
Highly Comminuted, Highly DisplacedHighly comminuted and displaced fractures consist ofeither transverse fractures with massive comminution sec-ondary to compression or stellate fractures with massivediastasis secondary to a violent quadriceps contraction(Fig. 5415). All major fragments are separated by morethan 6 mm, and sagittal splits are often present as well.These fractures frequently occur as open injuries and canbe accompanied by supracondylar femur fractures.
Fractures Associated with BonePatellarTendonBone Autograft
A subset of patella fractures has been reported in patientswho have had a bonepatellar tendonbone autograft forreconstruction of the anterior cruciate ligament.6, 17, 75, 103
An incidence of approximately 0.2% has been reportedin one study involving 1320 anterior cruciate reconstruc-tions.103 The etiology of these fractures is most oftenrelated to a traumatic fall or injury, but it has beenhypothesized that an accelerated rehabilitation protocolmay put patients at higher risk than the traditional rehabil-itation protocol.17 These fractures occur in two patterns. Atransverse fracture is the most common and is generallytreated with traditional tension band wiring or screwfixation techniques.6 Vertical, or fissure, fractures havebeen noted as well. These injuries are thought to occurfrom a stress riser created by a rectangular bone plug in thepatella or as a nondisplaced fracture created by the
osteotome at the time of graft harvest.7, 75 These fracturesare treated by neutralization with screws directed in thecoronal plane. The screws are not placed in a lag fashionbecause of the potential to create a distracting force at thearticular surface secondary to the defect from harvesting ofa graft.6 The rehabilitation protocol need not be modified ifthe fractures are rigidly fixed, and rehabilitation should beaggressively pursued.
TREATMENTz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Management of patella fractures is based on the morphol-ogy of the injury. Options include nonoperative treatment,tension band wiring, lag screw fixation, partial patellec-tomy, partial patellectomy combined with tension bandwiring, and total patellectomy. These techniques are per-formed with careful reconstruction of the extensor mecha-nism and the patellar joint surface whenever possible.Figure 5416 outlines this chapters proposed algorithm forthe management of patella fractures. Specific details offixation may need to be modified to accommodate a givenfracture pattern.
Biomechanics of PatellarFracture Fixation
Carpenter and colleagues compared three internal fixationconstructs for transverse patella fractures in a cadavermodel.20 The three constructs included a modified tensionband (AO technique), two parallel 4.5-mm interfragmen-tary lag screws, and a 4.0-mm cannulated lag screwtechnique with a tension band through the cannulatedscrews20 (Fig. 5417). A significant difference in displace-ment was noted between the modified tension bandconstruct and the lag screw techniques. The highest load tofailure occurred with the cannulated lag screw and tensionband construct. They concluded that the cannulated lag
FIGURE 5415. Comminuted transversefracture of the patella. A, Anteroposte-rior view. The details of the fracturesconfiguration are hard to see. The maindisplaced transverse component andsecondary vertical fracture lines areevident. B, Lateral view. Displacement ismore obvious, but comminution is lessapparent.
2023CHAPTER 54 Patella Fractures and Extensor Mechanism Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 11/32 P 2023 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 11/32 P 2023 BLACK T
screw and tension band technique provided improvedstability in the fixation of transverse fractures of the patella.
Scilaris and associates compared tension band tech-niques with a monofilament wire versus a braided cable ina transverse patella fracture cadaver model.88 The braidedcable construct allowed significantly less fracture displace-ment in cyclic loading than did the monofilament con-struct. They concluded that the braided cable plus tension
band construct was superior to the monofilament tech-nique and was more predictable in cyclic loading.
Open Fractures
Open patellar fractures are surgical emergencies, andsurgeons must be aware of the possibility of osteomyelitis
NONDISPLACED
TransverseStellateVertical
LAB/CWiring
Modifiedanteriortensionband wire
Modifiedanteriortensionband plusscrews
Highly comminutedHighly displaced
Partialexcision
Totalexcision
Cylinder cast/cast brace
Polar
Noncomminuted Comminuted
Stellate
Polar
Transverse
Transverse
DISPLACED
FIGURE 5416. Displacement and the fracture pattern both guide the choice of treatment with which to obtain the twoprimary goals of quadriceps mechanism continuity and stable anatomic reduction of the patellar articular surface.Nondisplaced fractures are managed nonoperatively. Displaced articular fractures are repaired, if possible, by using tensionband wiring techniques with or without screws or interosseous wiring. Polar avulsion fractures may be excised, but securereattachment of the quadriceps or patellar tendon is required. If comminution prevents satisfactory repair, total patellectomymay be the only option to restore the quadriceps. Abbreviation: LAB/C, longitudinal anterior band plus cerclage.
2024 SECTION V Lower Extremity
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 12/32 P 2024 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 12/32 P 2024 BLACK T
and septic arthritis. Irrigation, debridement, and stablefixation remain the principles of treatment. Devitalizedfragments should not be saved, and heroic efforts at salvageare not indicated. Fixation should be performed with aminimum of soft tissue stripping and must be stable.Subsequent repeat debridement will be necessary, andclosure may require skin grafts, muscle flaps, or free tissuetransfer.
Catalano and co-workers retrospectively reported on aseries of 79 open patella fractures with an average of 21months of follow-up.22 Open fractures were classified asgrade I (15%), grade II (53%), and grade III (32%) injuries.Additionally, most open patella fractures were displaced,with 22% being transverse fractures and 39% being com-minuted fractures. Approximately 80% of the patientssustained multiple injuries. Treatment consisted of opera-tive debridement and irrigation with appropriate antibiot-ics, followed by open reduction and internal fixation in57% and partial patellectomy in 32%. Eleven percent weretreated with debridement only, and no patients had aprimary total patellectomy. They reported no deep infec-tions, and only one patient required repeat open reductionand internal fixation. Seventy-six percent of the patientswere available for follow-up, and they had an average of112 of knee motion.22
Nonoperative Treatment
Indications for nonoperative management include trans-verse, stellate, and vertical nondisplaced closed patellar
fractures. Treatment consists of extension splinting for 4 to6 weeks.13, 42, 73, 89, 92 If plaster is used, care should betaken to extend the cast from a few centimeters above themalleoli to the groin (not the middle of the thigh). If thepatient is elderly or has varicose veins, an Unna boot isapplied to the foot and ankle before casting to minimizeswelling.92
Immediate weight bearing as tolerated is permitted.Isometric quadriceps exercises and straight leg raises areencouraged within several days.13, 42, 73 After radiographicevidence of consolidation, usually at 4 weeks, the plastermay be removed, and progressive active (not passive)flexion and strengthening exercises are begun.
In reliable patients, we prefer the use of an off-the-shelfhinged knee brace. These braces are lightweight and easilyadjustable and permit controlled motion of the knee joint.The knee hinge is locked in extension during ambulationbut may be opened to permit controlled motion during theconvalescent period. This type of brace may be advanta-geous for elderly patients. A simple knee immobilizer ofadequate length is a similar alternative.
Operative Treatment
PREOPERATIVE PLANNING
Before embarking on surgical repair of the patella, anoperative plan should be firmly established. Formulation ofthe plan requires radiographic evaluation of the normalopposite patella. On tracing paper or clear x-ray film, thenormal patella is outlined. The fracture fragments are then
A
B
CFIGURE 5417. Comparison of constructs for internal fixation of patella fractures. A, AO modified tension band construct. B, AO compression screws, 4.5mm. C, Cannulated 4.0-mm screws combined with a tension band. (From Carpenter, J.E.; et al. J Orthop Trauma 11:351356, 1997.)
2025CHAPTER 54 Patella Fractures and Extensor Mechanism Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 13/32 P 2025 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 13/32 P 2025 BLACK T
superimposed onto this outline in both the AP and thelateral planes. In effect, such superimposition reduces thefracture. Attention is then turned to fixation, be it wires,screws, partial excision, or a combination of methods.These elements should be drawn onto the plan andnumbered in sequence. Finally, contingency plans, as wellas the necessary equipment, should be listed. The surgeonshould be aware that superimposition of the patella on thefemur makes this exercise difficult at times. It thereforerequires optimal radiographic technique and an awarenessthat unanticipated comminution may be encountered.
Preoperative planning allows the surgeon to thinkthrough the operative procedure and become acquaintedwith the personality of the fracture. In addition, equipmentrequirements will be known beforehand, thus promoting asmoother operation without unnecessary delays. Whenthis plan is followed, the postoperative film will appearremarkably similar to the preoperative plan.
EQUIPMENT
A wire set incorporating Kirschner wires (K-wires),1.2-mm (18-gauge) and 1-mm (19-gauge) wire on spools,wire holders, wire tighteners, wire pliers, and a wire passeris necessary, along with a power drill and a wire driver(Fig. 5418). A small-fragment instrument and implantset and Weber (large, pointed) bone reduction forcepsare also useful. A special patella clamp is an invaluabledevice because the Weber clamps may rotate. Angiocath-eters (14 or 16 gauge) are helpful for passing wire. A
large-fragment set should always be available. Large os-teochondral fragments will require minifragment screwsor Herbert screws, and for small fragments, absorbablepolyglactin 910 (Vicryl) pins (Ethipins) should be on hand.
SETUP
The patient is placed in the supine position, and atourniquet is applied high on the thigh, if desired. Trappingof the quadriceps may cause difficulty in repositioning thepatella when the tourniquet is inflated. This complicationmay be prevented by flexing the knee carefully beyond 90to bring the quadriceps and proximal patella fragmentdown before inflating the tourniquet. In patients withcomplete retinacular disruption and a high-riding proximalpatellar fragment, a sterile tourniquet can be inflated, ifnecessary, after the patella has been brought down with anEsmarch bandage wrapped in a proximal-to-distal direc-tion.23
INCISIONS
Although any anterior knee incision can be used, atransverse, midline longitudinal, or lateral parapatellarincision is preferred (Fig. 5419). In patients with severeretinacular disruption, a transverse incision should parallelthis disruption to minimize the development of flaps.68, 79
In more comminuted fractures, a midline longitudinal orlateral parapatellar incision is necessary, especially if con-comitant injuries suggest the possibility of joint replace-
FIGURE 5418. Instruments and im-plants helpful for fixation of patellafractures include pointed reductionforceps for large bones (A), patellaforceps (B), wire tightener (C), wire-bending pliers (D), wire cutter (E) forKirschner wires, wire bender/impac-tor (F), Kirschner wire (G), and mal-leable wire at least 1 mm in diame-ter (H).
2026 SECTION V Lower Extremity
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 14/32 P 2026 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 14/32 P 2026 BLACK T
ment in the future. These latter incisions also avoid damageto the saphenous branch of the femoral nerve medially. Apercutaneous fixation technique for patella fractures hasbeen described. This method might be considered withseverely compromised skin.69 Berg has described an exten-sile exposure for comminuted fractures of the patella thatinvolves osteotomy of a tibial tubercle for retropatellarexposure and fracture fixation.7 This technique facilitatesexposure and reconstruction of the patella and mainte-nance of bone stock without any morbidity associated withthe tibial tubercle osteotomy. Additionally, ablative salvageprocedures can be avoided and thus further improve jointreconstruction options in the future.
OPERATIVE TECHNIQUES
All displaced fractures of the patella require operativeintervention. As previously mentioned, the techniquesused are based on the fracture pattern and concomitantinjuries (Table 542).
Tension Band WiringModified Anterior Tension Band Wiring. For
displaced noncomminuted two-part transverse patellarfractures, open reduction and internal fixation using themodified anterior tension band technique is the treatmentof choice (Fig. 5420).
A midline longitudinal incision is made through theskin and overlying bursa. The fracture edges are exposedand completely cleaned of debris and clot, with care takento not devitalize the fragments. The knee joint is thenirrigated to remove any loose fragments.
A preliminary reduction is performed to evaluate theproper position of the fragments. The reduction is thentaken down, and the proximal fragment is flexed 90. Ahole is drilled through the proximal fragment in a retro-grade manner with a 2-mm drill bit. This hole should startwithin the fracture line, approximately 5 mm from theanterior surface of the patella and at the junction of a lineseparating the patella into thirds. The drill bit is thenexchanged for a 1.6-mm K-wire that is pushed proximallyuntil it is flush with the fracture edge. A second hole(parallel to the first and at the junction of a line separatingthe patella into thirds) is drilled. The drill bit is exchangedwith a K-wire in a similar manner. The fracture is thenreduced and held with Weber or patellar reduction forceps.The wires are sequentially removed and the holes drilleddistally with a 2.0-mm drill bit up to, but not through, thedistal cortex. A prebent 1.6-mm K-wire is inserted into thedrill hole and hammered through the far cortex. Next, a1.2-mm (18-gauge) wire is placed underneath the upperhooks and the lower protruding pin tips. The wire isloosely tightened with a wire tightener. The reduction is
TABLE 542z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Treatment of Patella Fractures
Patella Fracture Type Treatment
A. Nondisplacedfractures
Cylinder cast
1. Transverse2. Stellate3. Vertical
B. Displaced fractures1. Noncomminuted
a. Transverse Modied anterior tension band wiringb. Polar Partial patellectomy
1. Apical Modied anterior tension band wiring2. Basal
2. Comminuteda. Stellate Modied anterior tension band wiring
Longitudinal anterior tension band pluscerclage
b. Transverse Independent lag screws plus modiedanterior tension band wiring
Longitudinal anterior tension bandwiring
Partial patellectomyc. Polar Partial patellectomyd. Highly
comminuted,highlydisplaced
Modied anterior tension band wiringLongitudinal anterior tension bandwiring
Partial patellectomyTotal patellectomy
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
FIGURE 5419. Incisions for exposure and treatment of patellar fractures.Either a longitudinal or a transverse approach may be used. Sufficientexposure to see and effectively repair medial and lateral retinacular tearsis important. Superficial dissection should be avoided to preservethickness and viability of the skin flaps.
2027CHAPTER 54 Patella Fractures and Extensor Mechanism Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 15/32 P 2027 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 15/32 P 2027 BLACK T
checked by extending the knee and palpating the under-surface of the patella with a finger. If a finger cannot beeasily inserted through the retinacular tear (or if noneexists), the retinaculum should be longitudinally incised topermit insertion. If articular congruity is satisfactory, thewire should be twisted tightly with a wire tightener andburied. The K-wires are twisted so that the bend is facingbackward and then buried in the patella. The excess distalends of the K-wires are cut off distally.
Although certain authors recommend crossing the ten-sion band wire, in our experience, crossing reduces the
area of patella that can be compressed and often leads to anunstable osteosynthesis. A prefabricated cerclage loop (AOtype) is also not recommended for use as a tension bandwire because it can come undone with early motion.Finally, the retinaculum is sutured closed with figure-of-eight 0 Vicryl interrupted sutures, and the wound is closedin layers over a drain.
Modified Anterior Tension Band Wiring throughCannulated Compression Screws. When failure of thestandard tension band technique is a concern in an elderlypatient with osteopenic bone, an alternative is a modified
BA
CD
FIGURE 5420. Modified AO tension band technique for patella fracture fixation (see text). A, Retrograde drilling of the proximal fragment. Kirschnerwires mark the proximal ends of the holes during reduction. B, Reduction, clamping, and antegrade partial drilling of the distal fragment. K-wireswith prebent proximal ends are then hammered through the remaining bone of the distal pole. C, With a large-bore needle, the 1.2-mm tension bandwire is placed deep to the proximal and distal ends of the K-wires immediately adjacent to the patella through the stout soft tissue attachments ofthe quadriceps tendon and patellar ligament. Medially and laterally, the tension band wire lies anterior to the patella and is not usually crossed. Itis tightened and twisted securely, and the pigtail end is bent flush with the bone surface. A twist or a square knot is reliable. The AO bent-wirefastening technique is not secure enough for definitive fixation. D, The prebent proximal ends of the K-wires are driven into the proximalpole, and the distal ends are trimmed if necessary. E, F, Anteroposterior (AP) and lateral radiographs show a displaced comminuted patellar fracture.G, AP radiograph after fixation. Note the modifications in technique for fixation of comminuted fragments: supplementary K-wires,distal-to-proximal K-wire insertion, and a distally crossed tension band wire, which was tightened with medial and lateral twists to equalize tension.H, I, Lateral and skyline views show anatomic reduction and anterior placement of the tension band wire.
2028 SECTION V Lower Extremity
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 16/32 P 2028 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 16/32 P 2028 BLACK T
anterior tension band through cannulated compressionscrews.8 Berg described this technique in which twoparallel cannulated cancellous screws are placed longi-tudinally over guide wires with lagged interfragmentarycompression. An 18-gauge AO wire is then passed in afigure-of-eight fashion through the cannulated screws andtightened with a Kirschner traction bow. The remainder ofthe fixation technique remains the same as for the standardanterior tension band construct (Fig. 5421).
Longitudinal Anterior Band plus Cerclage Wiring.Minimally displaced stellate fractures requiring operativeintervention may not have a single fragment large enoughto permit a modified anterior tension band technique. Inthese cases, either the K-wire should be angled appropri-ately or the longitudinal anterior band plus cerclage(LAB/C) wiring technique of Lotke and Ecker may beused68 (Fig. 5422).
The patella is approached, and the fragments arecleaned as described in the section Modified Anterior
Tension Band Wiring. Two parallel Beath-Steinmann pins(with holes in the distal tip) are drilled 1 cm from thepatellar edges through the aligned patella fragments in anantegrade manner. A 22-gauge wire is then inserted intoboth drill holes, and both pins are removed proximally. Thedistal loop is brought anteriorly, and one free proximal endis passed through this anterior loop. It is then tied to theother proximal end and tightened. This technique resultsin a strong and secure combination of anterior band andinterosseous wiring techniques. Heavier-gauge wire may besafer for fixationfor example, 18-gauge wire passed withthe aid of a large angiocatheter placed over the K-wire andheld in place when it is withdrawn.
If marked comminution is present, a cerclage wireshould first be placed around the circumference of thepatella, which can easily be done with a wire passer or a16- or 14-gauge angiocatheter inserted immediately nextto the patella. The LAB/C wiring is then performed. Theretinaculum is sutured closed with figure-of-eight 0 Vicryl
A B CFIGURE 5422. Longitudinal anterior band plus cerclage technique for interfragmentary wire loop fixation of patella fractures. A, For transverse fractures,the two ends of a wire loop are passed through longitudinal drill holes in the patella. One of these wire ends is then passed through the loop made bythe middle of the wire distally. Next, the ends are pulled tight and twisted to provide a taut anterior tension band. B, Lateral view. C, In fractures withsignificant comminution, fixation is aided by first placing a cerclage wire around the patella to trap the comminuted fragments and then drilling andapplying the longitudinal anterior band wire as in A. (AC, Redrawn from Lotke, P.A.; Ecker, M.L. Clin Orthop 158:180184, 1981.)
FIGURE 5421. Tension band technique through cannulated compression screws. A, Transverse patella fracture. B, Anteroposterior view of 4.5-mmcannulated compression screw fixation with a tension band wire. C, Lateral view demonstrating the tension band construct through cannulatedcompression screws.
2029CHAPTER 54 Patella Fractures and Extensor Mechanism Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 17/32 P 2029 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 17/32 P 2029 BLACK T
interrupted sutures, and the wound is closed in layers overa drain.
Independent Lag Screws plus Modified AnteriorTension Band Wiring. Transverse fractures may have oneor two additional fracture lines in the main fragments thatseparate the main fragments into halves or thirds. Thesesecondary fracture lines are not usually displaced, but theymay become so after operative intervention is attempted.The general principles of internal fixation of fracturesshould be followed (i.e., to make many fragments into twomain fragments and then unite these two into one). Suchfixation can usually be accomplished with independent lagscrews placed in a horizontal direction, followed by amodified anterior tension band wiring technique. The sizeof the screw should fit the size of the bone (e.g., 3.5-mmcortical screws will usually suffice, except in large adultmen, in whom 4.5-mm screws should be used) (Fig.5423). If the fragment is comminuted at the point ofscrew entry, a washer is used. Frequently, a fragment has oracquires a sagittal split during insertion of the lag screw;the split separates the anterior cortex from the mainchondral surface of that fragment. If this fragment cannot
be salvaged by repositioning the screw, LAB/C wiring orexcision of the fragment should be considered.
Partial PatellectomyNot infrequently, patellar fractures exhibit significant com-minution of one pole, and the fragments may involve asmaller or larger portion of the patella. At times, indirectreduction with a modified anterior tension band or LAB/Cwiring technique will be effective. If these techniques arenot possible, the time-honored method of partial patellec-tomy should be performed1, 25, 79, 101 (Fig. 5424).
The patella is approached and the fracture exposed aspreviously described. All large, stable, distal fragmentsshould be retained, and all small, comminuted fragmentsshould be excised. All loose strands of the torn quadricepsexpansion are removed. If one large distal fragment ispresent, it may be lagged into position with screws afterreduction has been secured. Care must be taken to notangle this fragment or patellofemoral arthritis will develop(see Fig. 5424C). This procedure can be simplified byplacing a bolster underneath the ankle to extend the knee.
A B
FIGURE 5423. AO lag screw plus tension band technique. A, Small-fragment screws can be used alone to fix vertical components or comminuted portionsof the patella. B, These screws should be supplemented with a tension band wire for fixation of displaced transverse fractures because screws alone maynot withstand the significant forces developed by the quadriceps mechanism. Anteroposterior (AP) (C), lateral (D), and skyline (E) radiographs show adisplaced oblique (functionally transverse) patellar fracture. Postoperative AP (F) and lateral (G) radiographs show the use of 4.0-mm cancellous lag screwssupplemented by an anterior tension band wire. The wire is crossed in this case to maintain its position anterior to the fracture.
2030 SECTION V Lower Extremity
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 18/32 P 2030 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 18/32 P 2030 BLACK T
Because of the powerful tension developed in thequadriceps mechanism, significant stress is placed on itsrepairs, which must be protected. This goal can be ac-complished by using a crossed tension band througheither the quadriceps insertion or the proximal part ofthe patella and through the proximal end of the tibiaby a variety of means (Fig. 5425). We prefer wirepassed directly through the bone because it is less bulkyand easier to remove. Mersilene tape or fascia may alsobe used.
If only small fragments remain distally, the followingtechnique is used. The anterior periosteum is reflected onthe proximal fragment approximately 5 mm, and with arongeur, a transverse groove is made in the proximalfragment within the fracture line itself. Three holes aredrilled so that they are equally spaced from the fracture lineand exit the superior aspect of the patella. Next, with aheavy, braided, nonabsorbable suture and an atraumaticneedle, the suture is passed distally in a running, lockingstitch along one edge of the tendon and then returned inthe midline of the tendon. A second suture is passed in asimilar manner along the opposite side of the tendon and
back along the midline. The suture ends are passedthrough the appropriate drill holes in the patella, with twosutures through the central hole. A straight, free needle canbe used to pass the sutures. Each suture is tied to itsopposite end. This step should be done while the knee ishyperextended and should bring the tendon end into closeapproximation with the trough in the distal aspect of theproximal part of the patella. A tension band should beadded to neutralize stress on the repair. The retinaculum isthen sutured closed with figure-of-eight 0 Vicryl inter-rupted sutures, and the wound is closed in layers, over adrain if desired.
Total PatellectomyFor highly displaced, highly comminuted fractures, anattempt at reconstruction should be made before totalpatellectomy is performed. Several authors have stressedthe retention of even one fragment to maintain a leverarm.33, 92, 100, 101 A combination of partial patellectomyand modified anterior tension band or LAB/C wiring isusually tried before total excision is performed. Al-though many techniques exist, those presented in the
A
B C
FIGURE 5424. Techniques of partial patellectomy. A, Extensive comminution of the central portion may be excised, with fixation of the proximal-to-distalpoles with screws or K-wires and a tension band. The results of this technique are not well documented. B, A small (usually extra-articular) bony fragmentmay aid in reattachment of the patellar ligament distally. Screws, K-wires, or sutures may be used, but they should always be protected with a tensionband, either limited to the patella if the distal pole fragment is sufficient or from the patella to the tibial tubercle if it is not sufficient. C, When suturingthe patellar ligament into a defect in the distal pole of the patella, it is essential to not attach it too anteriorly because such positioning will result inmalalignment of the patella (left), the distal articular surface being forced too far posteriorly. The example on the right shows proper reattachment of thepatellar ligament. A tension band from the patella to the tibia should protect this repair.
2031CHAPTER 54 Patella Fractures and Extensor Mechanism Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 19/32 P 2031 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 19/32 P 2031 BLACK T
DCBA
FIGURE 5425. A tension band wire techniqueshould be used to protect the patellar ligamentreattachment after distal pole fracture fixation,partial patellectomy, or repair of a rupturedpatellar ligament (A). B, C, The 1.0- or 1.2-mmwire can be attached to a screw through the tibialtubercle. D, It can be placed through thequadriceps tendon just proximal to the patella orthrough a drill hole in the patella and through adrill hole distally. Anteroposterior (E) and lateral(F) radiographs show the tension band wireprotecting the reattached patellar ligament afterdistal partial patellectomy.
2032 SECTION V Lower Extremity
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 20/32 P 2032 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 20/32 P 2032 BLACK T
following paragraphs are the most favorably reviewed inthe literature.
Because total patellectomy is often a salvage procedure,the surgeon may find various skin incisions and retinacularremnants. Once a decision for total extirpation has beenmade, all fragments of bone and shredded tendon areremoved sharply, but as much tendinous expansion aspossible is left. The critical feature of a total patellectomy isthe tendinous repair. Because the quadriceps tendon iseffectively lengthened by the removal of bone, this slackshould be taken up by imbrication (i.e., in a pursestringrepair), or an extensor lag will result.
If insufficient tendon exists for primary repair, severaloptions are available. These options can be separated intotwo categories: quadriceps turndown procedures and fas-cial or tendinous weaving. The former technique is usedwhen prepatellar soft tissue is absent, whereas the latteris reserved for injuries with destroyed quadriceps tendonas well.
The most common quadriceps turndown technique isthe inverted V-plasty of Shorbe and Dobson.93 After thepatella has been excised, the quadriceps tendon is exposedfor approximately 3 inches (Fig. 5426). A full-thicknessincision is made into the quadriceps tendon in the shape ofa V, with the apex located 2.5 inches proximal to theformer proximal patellar edge. The limbs of the incisionsextend distally for 2 inches such that ] to 12 inch oftendon is continuous with the retinaculum. The cornersmay be reinforced with suture if necessary. The apex issubsequently folded down, inserted through the proximalportion of the patellar tendon, and sutured down. Thequadriceps tendon should then be closed and all edgesrepaired. This repair is simple to perform, yet has theadvantage of being strong enough to allow early motion.
Should a large defect involving the quadriceps tendon
be present, a free fascial or tendinous strip is woven intothe tendinous remnants after the method of Gallie andLemesurier.39 First, all excess tendinous shreds are re-moved from the wound. The knee is extended withpadding under the ankle and the defect measured. Thislength should be doubled and 2 inches added to obtain theideal length of a fascial graft. A separate lateral incision ismade or the wound is extended, and a strip of fascia lata oran iliotibial band of the appropriate length and 1 to 1.5 cmin width is obtained. The strip of fascia is rolled into acylinder along its long axis and sutured to itself. It is thenwoven through the remaining quadriceps tendon or mus-cle, sewn to itself, passed through the patellar tendon, andtacked down after the slack is taken out. The graft shouldbe of sufficient length to sew one end down to the other.Finally, all edges are firmly sutured down. If the defectrequires an exceptionally long strip, plantaris tendon canbe used.
POSTOPERATIVE MANAGEMENT
With a stable osteosynthesis, the patient may begin using acontinuous passive motion machine to tolerance immedi-ately postoperatively. In our experience, use of this devicedecreases pain and stiffness. On the first postoperativeday, the patient can be out of bed with the leg elevated,and quadriceps isometric exercises are begun. Drains, ifused, are generally removed after 48 hours. The patient isthen placed in a removable knee brace and permitted toambulate with weight bearing as tolerated and the kneelocked in extension. The hinges may be loosened for activerange-of-motion exercises. These exercises should not beperformed until the wound is well healed, usually at3 weeks. Active extension and straight leg raising exer-
CBA
FIGURE 5426. Inverted V-plasty tech-nique of Shorbe and Dobson for repairof a patellectomy defect. A, The patellais resected, with a transverse defect leftin the quadriceps mechanism. Theretinacular rents are repaired first. B, Ifa defect remains centrally, an inverted,distally based, V-shaped flap of quad-riceps tendon is turned distally asshown. C, The flap is sutured in placeto cover and reinforce the defect.
2033CHAPTER 54 Patella Fractures and Extensor Mechanism Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 21/32 P 2033 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 21/32 P 2033 BLACK T
cises may be initiated as early as 1 week postoperatively.Progressive resistance exercises are performed after radio-graphic evidence of healing, usually at 6 weeks. The patientis then weaned from the brace and, by 3 months postoper-atively, usually has a healed fracture and strong quadriceps.Sports and vigorous work may be resumed after rehabilita-tion is complete, usually in 4 to 6 months.
For an unstable osteosynthesis, the repair must beprotected. Ideally, a knee brace with locking hinges willpermit controlled motion. The hinges are set to allow fullextension. Flexion to the degree possible during intraop-erative assessment of the repair is permitted, primarily forcartilage nutrition. The brace should be worn at all times,and active flexion exercises should not begin until thefracture has healed. Isometric quadriceps extension exer-cises should be initiated at 2 weeks. Weight bearing in fullextension can usually be allowed once comfort permits.Weight bearing on the flexed knee should be avoided untilfracture healing is secure. The patient should be madeaware of possible knee stiffness. When the fracture hashealed radiographically and is clinically stable, attempts atrehabilitation are begun to improve flexion range andstrength of all muscle groups.
Implant removal should be delayed until fracture unionis mature, which usually requires a minimum of 6 months.K-wires may be extracted if they are painful and protrud-ing, but loss of fixation with fracture displacement gener-ally requires revision surgery. Asymptomatic implants maybe retained indefinitely. Wires used to protect tendonrepairs should be left in place for a minimum of 3 to6 months.
Results
No generally accepted outcome assessment system isavailable for patellar fractures. Most authors base outcomeon subjective complaints of pain, limitation in activities ofdaily living, change in job status, and ambulation.14, 35, 92
Bostman and colleagues developed the most completeevaluation of clinical results to date11 (Table 543). How-ever, this table, like most reports in the literature, doesnot evaluate radiographic findings. Radiographic criteriawould include osteoarthritis, fibrous union or nonunion,the presence of osteochondral fragments, and the degree ofarticular step-off on the radiograph.11, 19, 92 The lack of auniform assessment scale allows only broad generalizationsto be made about the results of treatment of these injuries(Table 544).
NONOPERATIVE TREATMENT
Nonoperative treatment of nondisplaced fractures nearlyalways has a uniformly good outcome,13, 73, 89, 96 whichimplies full range of motion and no arthrosis, weakness, orpain (see Table 543). In Bostroms series of 422 patellarfractures, 219 were treated nonoperatively and were avail-able for follow-up.13 All cases initially had less than 4 mmof articular incongruity; 54% (118/219) had excellentresults, and 44% (97/219) had good results. Only twofailures occurred. His results agree with the findings of
other large series in that the failure rate from nonopera-tively treated, nondisplaced patellar fractures was 5%.
OPERATIVE TREATMENT
Results of operative repair are based on the type offracture and the technique used (Table 545). Modifiedanterior tension band wiring has given the best resultsin the literature to date, with 57% excellent and 29%good results11, 12, 54, 64, 108 (Table 546). Unfortunately,many studies are vague in reporting results, and studies
TABLE 544z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Combined Results of Various Forms of OperativeTreatment in the Literature
Treatment
ResultsTotalNo.Excellent Good Fair
ORIF 135 (37%) 129 (36%) 97 (27%) 361Partial excision 32 (23%) 67 (49%) 39 (28%) 138Total excision 62 (28%) 96 (44%) 61 (28%) 219Totals 229 292 197 718
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z zAbbreviation: ORIF, open reduction and internal xation.
TABLE 543z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Clinical Grading Scale
Clinical Grading Scale/Variable Score
Range of motion (ROM)Full extension, ROM >120 6Full extension, ROM 90120 3Loss of full extension, ROM
reporting this technique are few. Analysis of combined datashows tension band wiring to be superior to simplecerclage wiring clinically. In addition, Weber and col-leagues showed the superiority of tension band wiringbiomechanically108 (see Table 526). Modified wiringtechniques can also be effective. In Lotke and Eckers reporton LAB/C wiring, 16 cases were presented; 13 (81%) hadexcellent results.68
Partial PatellectomyPartial patellectomy may give functional results com-parable to those of open reduction and internal fixation,but comparison is difficult because the fracture patternstreated by these techniques are different.12, 13, 64, 68, 101
Sutton and co-workers showed that the only deficit withpartial excision of at least one third of the patella is an18 loss of motion.99 In studies by Bostman and as-sociates, Bostrom, Mishra, Nummi, and Seligo, a nearlynormal outcome occurred when large fragments of pa-tella were retained and articular congruity was main-tained.12, 13, 76, 82, 92 Small fragments without soft tissue,sagittally split fragments, and those missing cartilage wereexcised. These authors found that saving these fragmentsdid not improve function and even compromised it.Retention of one or two large fragments, however, im-proved quadriceps function.12, 13, 41, 58, 64, 101, 109 Hungand colleagues reported the results of a 25-monthfollow-up in a retrospective series of patients in whichradiographic changes consistent with post-traumatic ar-thritis developed in 55% after partial patellectomy andtension band repair.53 However, most of these patientswere asymptomatic within that time frame.
Total PatellectomyTotal patellectomy has yielded varying degrees of success.Before the 1970s, poor reconstructive results justified totalpatellectomy.16, 31, 40, 44, 45, 50 Investigators compared op-erative repair with a single cerclage wire and total excision.Although many stated that good clinical results wereexpected, more recent studies have questioned this conclu-sion11, 13, 64, 89 (see Table 545).
Sutton and co-workers evaluated quadriceps strength,activities of daily living, and functional ability in patientswho had undergone either partial or total patellectomy.99
The opposite normal knee was the control. Both groupshad an average loss of 18 range of motion. A 49%reduction in strength of the extensor mechanism waspresent in the total-excision group. This reduction instrength was the result of loss of the lever arm produced byloss of the patella. Instability was greater in this group, withthe patellectomized knee losing almost 50% of excursion instance-phase flexion. This loss was a result of the patellartendon sinking into the intercondylar notch. Clinically, this
TABLE 546z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Comparison of Anterior Tension Band vs. Cerclage Wiring
Author No. Patients
Results of Anterior Tension Band Results of Cerclage Wiring
Excellent Good Poor Excellent Good Poor
Bostman et al.12 29 9 3 2 6 6 3Bostrom13 75 19 42 14Levack et al.64 30 7 5 2 2 5 9Seligo92 31 10 14 7Ma et al.69 81 59 15 7Nummi82 66 3 18 45Totals 312 16 8 4 99 100 85
(57%) (29%) (14%) (35%) (35%) (30%)
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
TABLE 545z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Results of Operative Repair in Patellar Fractures
Author, YearNo.
Patients
Results
Excellent Good Fair
OPEN REDUCTION, INTERNAL FIXATION
Seligo,92 1971 35 10 18 7Nummi,82 1971 66 3 18 45Bostrom,13 1972 75 19 42 14Bostman et al.,12 1983 48 17 21 10Ma et al.,69 1984 107 77 20 10Levack et al.,64 1985 30 9 10 11Totals 361 135 129 97
(37%) (36%) (27%)
PARTIAL EXCISION
Seligo,92 1971 3 0 1 2Nummi,82 1971 68 14 28 26Bostrom,13 1972 28 8 15 5Mishra,76 1972 4 2 1 1Bostman et al.,12 1983 35 8 22 5Totals 138 32 67 39
(23%) (49%) (28%)
TOTAL EXCISION
Seligo,92 1971 44 14 25 5Nummi,82 1971 13 0 5 8Bostrom,13 1972 5 0 1 4Mishra,76 1972 26 3 15 8Einola et al.,35 1976 28 6 18 4Wilkinson,112 1977 31 7 12 12Bostman et al.,12 1983 10 0 3 7Levack et al.,64 1985 34 20 7 7Jakobsen et al.,56 1985 28 12 10 6Totals 219 62 96 61
(28%) (44%) (28%)
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
2035CHAPTER 54 Patella Fractures and Extensor Mechanism Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 23/32 P 2035 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 23/32 P 2035 BLACK T
instability was manifested as insufficiency and inability tosupport the loaded knee in stair climbing. Biomechanicalstudies on cadaver knees performed by Watkins andassociates, Wendt and Johnson, and others all showed thattotal patellectomy resulted in loss of tibial torque and,therefore, strength.42, 58, 105, 109
Srensen noted that the quadriceps did not improve instrength after patellectomy.96 All patients complained offrequent giving way and difficulty running and walkingdown stairs. He concluded that none of his operativereconstructions would have fared better with total exci-sion of the patella and thus justified attempts at salvage.Wilkinson evaluated 31 patients 4.5 to 13 years after totalexcision.112 In this study, less than a fourth of the pa-tients had an excellent result. He also noted that maxi-mal recovery took up to 3 years. Einola and colleagueswere able to monitor 28 patients for an average of 7.5 yearsafter total excision.35 Good results were seen in only sixpatients. The predominant complaint was weakness andpain on movement and exertion. The most commonfinding was quadriceps atrophy. Quadriceps power waswithin 75% of the normal knee in only seven cases. Heconcluded that saving as much patella as possible wasadvisable. Scott reported that only 6% (4/71) of patientswere happy with their long-term outcome after patellec-tomy.89 Ninety percent had aching in the joint, and 60%complained of weakness. Quadriceps wasting was a con-stant finding.
The present recommendations are to therefore retain asmuch patella as possible.1113, 33, 54, 64, 79, 100, 101 Totalpatellectomy is reserved for fractures that are so commi-nuted that repair is futile. This plan will offer the patientthe best possible knee function for the longest period. Howmuch patella should be saved? No definitive answer exists.It is our opinion that as little as 25% of the patella (i.e., onequadrant) may be retained with a subsequently goodoutcome. We have never found a patella so comminutedthat one fragment could not be salvaged with repair. If noarticular congruity exists, however, excision is the onlyoption.
COMPLICATIONSz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Infection
Superficial wound infections should be treated by standardprotocol based on the degree of soft tissue involvement.Osteomyelitis is aggressively treated with resection of allsequestra and dead tissue. Irrigation and debridement ofthe knee must be repeated every 48 to 72 hours until thejoint is free of necrotic tissue to prevent septic arthritis.Daily bedside aspiration is not indicated. The patientshould receive 6 weeks of culture-specific intravenousantibiotics. Once the deep bone infection is under con-trol, an attempt should be made to salvage any remain-ing patella by individualized and modified wiring tech-niques. If salvage is not possible, total patellectomy may berequired.
Breakage of Wires, Loss of Fixation,and Refracture
After osteosynthesis, especially with early motion, thetension band may break, but it is unusual for such breakageto occur before healing of the patella. If the fracture ishealed, the wire, pins, or screws may be removed if theycause symptoms.
Loss of fixation during the healing phase will re-quire revision if the fragments separate more than 3 to4 mm or if the articular surface has an incongruity greaterthan 3 mm. Before returning to the operating room, aradiograph should be obtained in full extension. Ifreduction has improved, the patient may benefit from6 weeks of extension splinting. Usually, however, isomet-ric exercises will continue to separate the fragments, andunless the patient refuses, revision should be undertaken.
Refracture should be treated as a fresh fracture accord-ing to the principles previously described (i.e., nondis-placed fractures are treated nonoperatively and displacedfractures are treated operatively).
Delayed Union and Malunion
Delayed union, once a routine result, is extremely uncom-mon. If identified, a period of decreased motion is begunbecause the fracture will often spontaneously unite. Weberand Cech could find only three cases of patellar pseudar-throsis in their large series of nonunions.107 All healed afterrevision surgery performed with established fracture fixa-tion methods. If it is an old nonunion with 4 to 5 inches ofseparation, reconstruction should be attempted. Quadri-ceps shortening will make this repair difficult, and formalquadricepsplasty may be required. Care must be taken toobtain the correct length or disability will continue. Ifchondromalacia exists, consideration should be given toperforming a total patellectomy and fascial reconstructionaccording to the method of Gallie and Lemesurier.39
Loss of Knee Motion
The advent of tension band wiring has permitted earlyrange of motion, and functional range of motion can beexpected in most cases. If flexion is still decreased severalmonths postoperatively, intensive physiotherapy is begun.If such physiotherapy does not suffice, manipulation underanesthesia should be contemplated. Care must be exercisedin patients requiring manipulation who have had patellec-tomies because rupture of the repair may occur. A reporthas been published of a boutonnie`re deformity aftermanipulation of a longitudinally repaired extensor retinac-ulum.81 If gentle manipulation is unsuccessful, consider-ation is given to arthroscopic lysis of intra-articular adhe-sions. Quadricepsplasty is performed only in exceptionalcases, usually when no improvement is seen after 9 to 12months. This situation is most often the case after concom-itant injury to the distal end of the femur has resulted inbinding down of the quadriceps mechanism.
2036 SECTION V Lower Extremity
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 24/32 P 2036 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h54 10/15/02 31 P 24/32 P 2036 BLACK T
Occasionally after total patellectomy, the extensormechanism is too long, which may result in loss of fullextension. The patient has a sensation of instability andgiving way.96 In this rare situation, consideration is given toa Maquet procedure to bring the patellar tendon forwardand increase its mechanical advantage. This technique hasbeen described by Kaufer in excellent biomechanical stud-ies.58 Reports of clinical results of the Maquet procedurefor this purpose are nonexistent. We would caution againstusing too large a bone block because of subsequent skinbreakdown and pain. Other authors suggest reefing theextensor mechanism, but this maneuver runs the risk ofrerupture.93
Osteoarthritis and Patellar Enlargement
Although Bruce and Walmsley18 and Cohn27 showedthat osteoarthritis occurred in rabbits after patel-lectomy, this complication has never been borne outin long-term studies of postpatellectomy humanknees.1, 13, 19, 35, 56, 76, 99, 112 In addition, articular incon-gruity causing osteoarthritis has not been reported inlong-term studies.13, 96
Two situations have been demonstrated to increase theincidence of osteoarthritis. Patellar enlargement, a result ofexuberant bone formation during the healing of commi-nuted fractures, has