Embed Size (px)
Citation preview
J Neurosurg Spine Volume 24 • May 2016806
caSe reportJ Neurosurg Spine 24:806–809, 2016
Spinal dural arteriovenous fistula (dAVF) is the most common vascular malformation of the spinal cord. The initial symptoms are vague and might resemble
those of degenerative spine disease, explaining the consid-erable time delay between symptom onset and diagnosis. At diagnosis the vast majority of patients have symptoms of myelopathy, related to a venous congestion of the spinal cord by arterialization of the veins that normally drain the spinal cord parenchyma. Left untreated, the disease is pro-gressive and leads to disability within 5 years. Treatment options are embolization and microsurgery. Microsurgery is favored by many because the occlusion rates are higher and the complications, if they occur, are less severe. For both treatment options, spinal digital subtraction angiog-raphy (DSA) is required to localize the fistula exactly and to exclude other vascular malformations that might have a similar appearance on MRI. Computerized tomography angiography (CTA) has the potential to replace spinal DSA in the future, but until now has been considered to be a useful diagnostic adjunct only if surgery is planned. We report a unique case of transient neurological deficits occurring after both spinal DSA and CTA, and we discuss the possible pathomechanisms.
case reportHistory and Examination
A 76-year-old man, a general practitioner, reported in-creasing gait disturbances due to intermittent weakness of his legs for the 3 months prior to presentation. Lumbar or radicular pain was denied. His walking distance was reduced to 100 m. Clinical examination revealed a mild proximal paraparesis of his legs, with a muscle strength of Grade 4 according to the Medical Research Council (MRC) scale. No distal paresis, sensory deficits, signs of myelopathy, or vegetative deficits were found.
Neuroimaging FindingsAn MRI study of the lumbar spine raised suspicion of a
spinal dural arteriovenous fistula (dAVF). The patient un-derwent an uneventful spinal DSA with a total dose of 100 ml of the nonionic contrast medium iomeprol (Imeron 300 [30 g iodine/100 ml, trometamol, hydrochloric acid, and water for injection], Bracco Imaging Germany). The DSA confirmed a spinal dAVF arising from the left L-1 radicu-lomeningeal artery (Fig. 1). Within 1 hour after the DSA, the patient developed a paraplegia of his legs. An MRI
abbreviatioNS BBB = blood-brain barrier; CM = contrast media; CTA = CT angiography; dAVF = dural arteriovenous fistula; DSA = digital subtraction angiography; MRC = Medical Research Council. Submitted January 28, 2015. accepted May 20, 2015.iNclude wheN citiNg Published online November 6, 2015; DOI: 10.3171/2015.5.SPINE15114.
Paraplegia after contrast media application: a transient or devastating rare complication? Case report dorothee mielke, md,1 Kai Kallenberg, md,2 marius hartmann, md,3 and veit rohde, md1
Departments of 1Neurosurgery and 2Neuroradiology, Georg-August-University, Göttingen; and 3Department of Neuroradiology, HELIOS Hospital Berlin-Buch, Berlin, Germany
The authors report the case of a 76-year-old man with a spinal dural arteriovenous fistula. The patient suffered from sud-den repeated reversible paraplegia after spinal digital subtraction angiography as well as CT angiography. Neurotoxicity of contrast media (CM) is the most probable cause for this repeated short-lasting paraplegia.Intolerance to toxicity of CM to the vulnerable spinal cord is rare, and probably depends on the individual patient. This phenomenon is transient and can occur after both intraarterial and intravenous CM application.http://thejns.org/doi/abs/10.3171/2015.5.SPINE15114Key wordS contrast media application; paraplegia; complication; digital subtraction angiography; CT angiography
©AANS, 2016
Unauthenticated | Downloaded 10/31/21 11:10 PM UTC

paraplegia after contrast media application
J Neurosurg Spine Volume 24 • May 2016 807
study of the spine was performed immediately, and ex-cluded intramedullary bleeding, ischemia, and progressive dAVF-related venous congestion (Fig. 2). The paraplegia resolved completely within 24 hours under dexametha-sone medication. Surgery for the dAVF was scheduled to
be performed 3 weeks after DSA. To shorten the waiting time, the patient presented at our institution 17 days after the first DSA.
By the time of presentation at our clinic the patient was experiencing a mild proximal paraparesis of his legs, with a muscle strength of Grade 4 according to the MRC scale. Furthermore, he had a sensory deficit including both prox-imal thighs. To better delineate the relation of the dAVF to the bony structures of the spine, CTA, with intrave-nous injection of 80 ml of the nonionic contrast medium iomeprol (Imeron 400 [40 g iodine/100 ml, trometamol, hydrochloric acid, and water for injection], Bracco Imag-ing Germany), was performed. Again the patient devel-oped a complete paraplegia of his legs. Furthermore, he had a complete hypesthesia below the L-1 level as well as an atonic sphincter muscle. We obtained MRI stud-ies, which ruled out intramedullary bleeding and ische-mia, but showed contrast enhancement in the region of the intramedullary venous congestion (Figs. 3 and 4). There were no documented adverse events of blood pressure dropping throughout the whole admission period in both clinics. Paraplegia resolved completely within 72 hours
Fig. 1. A DSA study (SOMATOM Definition AS+, Siemens) demon-strates the dAVF at the level of L-1 by applying a Simmons 2 catheter via a transfemoral approach.
Fig. 2. MRI studies of the lumbar spine (1.5-T Titan, Toshiba), obtained immediately after paraplegia developed, demonstrate significant edema of the conus medullaris (white arrow) as well as tortuous and elongated vessels as an indicator of a dAVF (black arrows). a: Sagittal T2-weight-ed image (fast spin echo, slice thickness 3.5 mm, TR 3000 msec, TE 106 msec, averages 1, flip angle 90°). b: Coronal maximum intensity projection of an MR myelography study (3D field echo steady state, slice thickness 2 mm, TR 15 msec, TE 7.2 msec, averages 2, flip angle 55°).
Unauthenticated | Downloaded 10/31/21 11:10 PM UTC
d. mielke et al.
J Neurosurg Spine Volume 24 • May 2016808
after the application of dexamethasone, which had already been started prior to the examination. Furthermore, the patient received intravenous injections of 4 mg clemastine and 250 mg prednisolone (once each).
Operation and Postoperative Course Three days later, the fistula was ligated microsurgically
via a hemilaminectomy at the L-1 level on the left side. Surgery was uneventful. The patient demonstrated no new neurological deficit postoperatively. The preoperative gait disturbance as well as sensory deficits were already in de-cline by the time of discharge. So far, the follow-up period is 9 months. The patient still reports unspecified sensory deficits of the left leg. Furthermore, the gait disturbance is still present, but has clearly improved during the last months. Prior to the operation the patient was able to walk only a couple of steps without assistance. At the moment he does not need any assistance for walking, but still re-ports episodes of stumbling.
discussionpossible pathomechanisms of Neurological Symptoms after cerebral angiography
Short-term transient neurological symptoms as well as fully reversible but long-lasting seizures, cortical blind-ness, and encephalopathy have been reported after cere-bral DSA with intraarterial injection of contrast media (CM).2–4,6,7 Four major pathomechanisms have been pro-posed to explain these neurological deficits, as follows. 1) Direct displacement of blood by the CM lasts only seconds, but might produce enough tissue hypoxia to al-ter brain function transiently in some cases. 2) High con-centrations of CM cause aggregation and clumping of red blood cells, leading to local stasis and occlusion of small arterial branches.2 3) Conventional iodinated CM have high affinities for plasma water, low affinities for plasma proteins, and extremely low partition coefficients. Nor-mally, CM do not penetrate an intact blood-brain barrier (BBB). However, it has been shown in animal models that the hyperosmolarity of intraarterially injected ionic CM can cause BBB breakdown,7 allowing CM to leak into brain tissue and exert their chemotoxic property. Possibly,
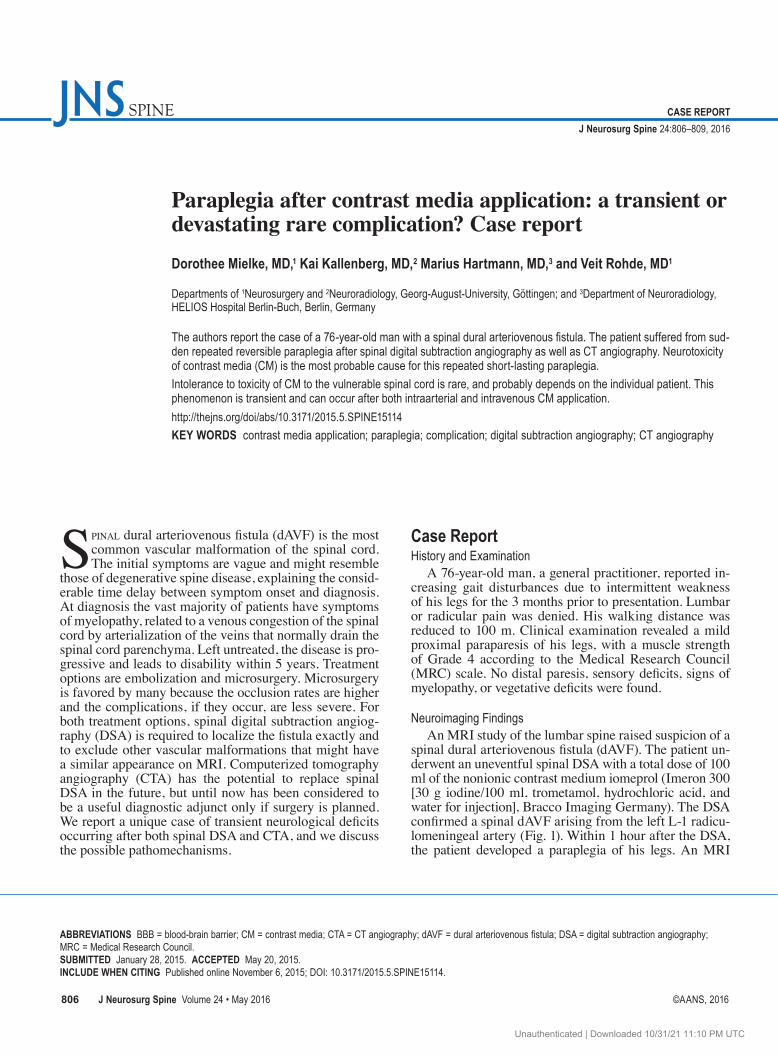
Fig. 3. MRI study of the cervical and thoracic spine (1.5-T Intera, Philips Medical Systems). Sagittal T1-weighted image (spectral presaturation inversion recovery [SPIR], slice thickness 3 mm, TR 812.8 msec, TE 9.5 msec, averages 3, flip angle 90°), obtained after the intravenous appli-cation of a Gd-containing contrast agent, shows contrast enhancement of the lower thoracic spinal cord (white arrowheads).
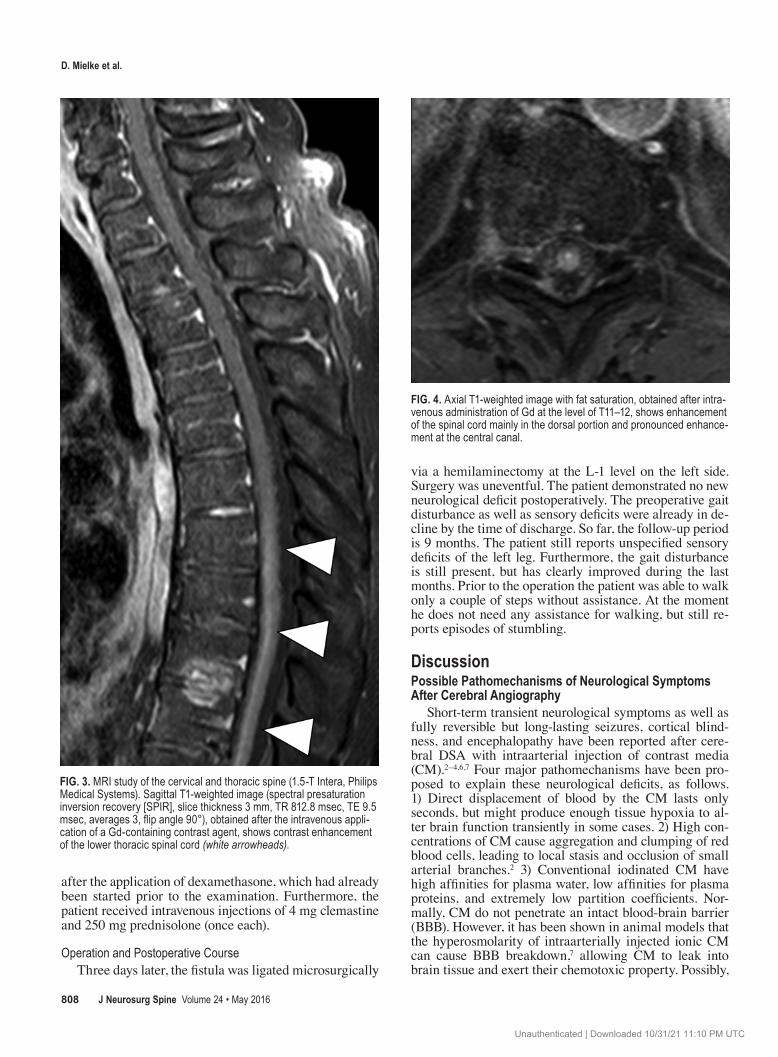
Fig. 4. Axial T1-weighted image with fat saturation, obtained after intra-venous administration of Gd at the level of T11–12, shows enhancement of the spinal cord mainly in the dorsal portion and pronounced enhance-ment at the central canal.
Unauthenticated | Downloaded 10/31/21 11:10 PM UTC

paraplegia after contrast media application
J Neurosurg Spine Volume 24 • May 2016 809
the chemotoxic effects are enhanced by red blood cell ag-gregation, by induction of ischemia (contributing to BBB breakdown), and by prolongation of the CM transit time.6 4) It has been shown that the effect of local ischemia, in-duced either by mere CM injection or by red blood cell aggregation, might be intensified if underlying vascular disease of the brain has already caused a situation of hy-poperfusion or ischemia.3
possible pathomechanisms of Neurological Symptoms after cerebral cta
In CTA, intravenous instead of intraarterial CM are being applied. Complete recovery of neurological deficits within hours to days after CTA of the cerebral vessels is much more rare than after DSA, but has been reported. Junck and Marshall3 report that the peak osmolality of blood plus CM perfusing the CNS is not nearly as high as with arteriography, but that the osmolality remains el-evated for a longer time, which might lead to an opening of the BBB and leakage of the chemotoxic CM into the brain parenchyma. They further suggest that the barrier defect is being repaired while the concentration of CM remains high; thus the CM may be unable to diffuse freely back into the blood and their clearance from the CNS may be prolonged, with a subsequent risk for prolonged che-motoxic effects.3
Neurological Deficits After Spinal DSA and CTA?A permanent neurological deficit after diagnostic spi-
nal DSA with CM injection into the radiculomeningeal artery has been described only once: Oumerzouk et al. re-ported on the case of a 73-year-old man with sudden wors-ening of a preexisting paraparesis after spinal DSA.5 This patient harbored a dAVF as well. The patient underwent surgery, but unfortunately the paraplegia remained, with only slight improvement. The authors suggested a sudden increase of venous pressure as the cause for this devastat-ing complication.5
Transient neurological complications after spinal DSA have not been described yet; in a retrospective study re-viewing 302 spinal angiographies, no neurological compli-cations were encountered and no case reports were retriev-able. The same holds true with spinal CTA; a neurological deficit after spinal CTA has never been mentioned in the international literature. Thus, our case report appears to be unique. Because this complication is fully reversible and also occurs after intravenous CM application, not after the sudden increase of the spinal venous pressure, the causative pathomechanisms are probably similar to those assumed in cerebral DSA with transient neurologi-cal symptoms. Because of this assertion, the occurrence of this complication after spinal DSA and CTA should not be regarded as being completely unexpected. The dAVF led to focal intramedullary edema as seen on MRI (Fig. 2), which can be taken as a sign for an already disturbed BBB. Thus, CM could have easily entered the spinal cord, with a subsequent local chemotoxic effect that did not re-solve until the CM were being washed out. Contrast media can cause a combination of excitatory effects associated
with their chemical nature and inhibitory effects associ-ated with their hyperosmolality.1 In our case, the patient demonstrated only inhibitory effects.
conclusionsTransient paraplegia after intraarterial as well as in-
travenous application of CM for spinal DSA and CTA has never been reported before. Because CM neurotoxic-ity together with a disturbed BBB is the most probable cause, the already reported complications after cerebral DSA and CTA suggest that the uniqueness of the present case is related to the considerably less-frequent need for spinal DSA and spinal CTA. Thus, despite being unique up to now, we strongly believe that this complication will repeatedly occur with the increasing use of spinal DSA and CTA in the future. Therefore, indications for CM ap-plication in spinal diseases should be carefully selected, especially if a neurological deficit related to intravascular CM application has already occurred.
references 1. Bryan RN, Dauth GW, Gilman S, Hilal SK: Effects of ra-
diographic contrast agents on spinal cord physiology. Invest Radiol 16:234–239, 1981
2. Johnson JH, Knisely MH: Intravascular agglutination of the flowing blood following the injection of radiopaque contrast media. Neurology 12:560–570, 1962
3. Junck L, Marshall WH: Neurotoxicity of radiological con-trast agents. Ann Neurol 13:469–484, 1983
4. Mentzel H-J, Blume J, Malich A, Fitzek C, Reichenbach JR, Kaiser WA: Cortical blindness after contrast-enhanced CT: complication in a patient with diabetes insipidus. AJNR Am J Neuroradiol 24:1114–1116, 2003
5. Oumerzouk J, Jouehari A, Hssaini Y, Raggabi A, Bourazza A: Sudden worsening of paraparesis complicating dorsal du-ral arteriovenous fistula after spinal angiography: case report and review of literature. Rev Neurol (Paris) 169:356–358, 2013
6. Rand PW, Lacombe E: Effects of angiocardiographic injec-tions on blood viscosity. Radiology 85:1022–1032, 1965
7. Sage MR, Wilson AJ: The blood-brain barrier: an impor-tant concept in neuroimaging. AJNR Am J Neuroradiol 15:601–622, 1994
disclosureThe authors report no conflict of interest concerning the materi-als or methods used in this study or the findings specified in this paper.
author contributionsConception and design: Mielke. Acquisition of data: Mielke. Analysis and interpretation of data: Mielke, Kallenberg, Rohde. Drafting the article: Mielke. Critically revising the article: Mielke, Hartmann, Rohde. Reviewed submitted version of manu-script: all authors. Approved the final version of the manuscript on behalf of all authors: Mielke. Administrative/technical/mate-rial support: Kallenberg, Hartmann.
correspondenceDorothee Mielke, Department of Neurosurgery, Georg-August-University Göttingen, Robert-Koch-Strasse 40, 37075 Göttingen, Germany. email: [email protected].
Unauthenticated | Downloaded 10/31/21 11:10 PM UTC