Embed Size (px)
Citation preview
POST-OPERATIVE POST-OPERATIVE PAIN PAIN
MANAGEMENTMANAGEMENT
Dr Suleman MumtazDr Suleman Mumtaz
PG Ward 2 PG Ward 2

OBJECTIVEOBJECTIVE• The purpose of this presentation is to The purpose of this presentation is to
review Common methods of relieving acute review Common methods of relieving acute post-operative pain post-operative pain
• In this we will discuss how to use Common In this we will discuss how to use Common peripherally-acting analgesics (like non-peripherally-acting analgesics (like non-steroidal anti-inflammatory drugs(NSAIDS), steroidal anti-inflammatory drugs(NSAIDS), centrally-acting agents (such as opioids) centrally-acting agents (such as opioids) and also local anaesthetics .and also local anaesthetics .
• This review is not comprehensive but is This review is not comprehensive but is intended to summarise current thought intended to summarise current thought about the practical management of about the practical management of postoperative pain in most hospital of our postoperative pain in most hospital of our Country like JPMCCountry like JPMC
• Finally WHO recomendation Finally WHO recomendation

Adverse pathophysiological Adverse pathophysiological consequences of poor pain consequences of poor pain management(What if not management(What if not
considered)considered)• CardiovascularCardiovascular – Hypertension, tachycardia – Hypertension, tachycardia
• RespiratoryRespiratory - if patient is unable to cough and - if patient is unable to cough and expand lung expand lung bases it increases bases it increases risk of chest infection/pneumonia.risk of chest infection/pneumonia.
• Urinary Urinary – Urinary retention – Urinary retention • Psychological Psychological – Pain can lead to anxiety, sleep – Pain can lead to anxiety, sleep
deprivation,patient:s unsatisfaction deprivation,patient:s unsatisfaction towards treatmenttowards treatment
• Generally, if patient’s pain is well controlled they will Generally, if patient’s pain is well controlled they will recover quicker and be discharged sooner.recover quicker and be discharged sooner.

Misconceptions about post-Misconceptions about post-operative pain operative pain
• Doctor believe that they, rather than the Doctor believe that they, rather than the patient, are the authority on the patient’s pain patient, are the authority on the patient’s pain
• Post-operative pain can not be prevented Post-operative pain can not be prevented • Patients will become addicted Patients will become addicted • Side effects of analgesics can not be Side effects of analgesics can not be
controlled controlled • Opioids must not be given as primary Opioids must not be given as primary
treatment treatment • The same operation produces comparable The same operation produces comparable
severity of pain in different people severity of pain in different people
Pain Assessment Pain Assessment Pain must be assessed regularly by asking the Pain must be assessed regularly by asking the
patient. Pain can not be assessed accurately by patient. Pain can not be assessed accurately by observers observers
• Believe the patient! (pain is the patients own Believe the patient! (pain is the patients own experience) experience)
• Ask them to rate their pain as ‘none’, ‘mild’, Ask them to rate their pain as ‘none’, ‘mild’, ‘moderate’ or ‘severe’ –‘moderate’ or ‘severe’ –PAIN SCOREPAIN SCORE
• Ask the patient to assess their pain on movement (eg. Ask the patient to assess their pain on movement (eg. deep breathing) deep breathing)
• Pain should be assessed for at least 4 days to 1½ week Pain should be assessed for at least 4 days to 1½ week post-operatively. Level of sedation and respiratory post-operatively. Level of sedation and respiratory rate must also be observed (in case of OPIODS)rate must also be observed (in case of OPIODS)
• Surgeon should assess by using Surgeon should assess by using PAIN SCOREPAIN SCORE

Pain Assessment Cont:Pain Assessment Cont:Pain ScorePain Score

Principles of good pain Principles of good pain management management
• Involve the patient in the management of their pain Involve the patient in the management of their pain • Aim to predict and prevent pain if possible Aim to predict and prevent pain if possible • Analgesics should be used regularly for continuous pain Analgesics should be used regularly for continuous pain • Always use the IM/IV route Always use the IM/IV route • If patient is requiring regular Opiod injections consider If patient is requiring regular Opiod injections consider
PCA PCA • Dose and frequency must be individualised. Opioids Dose and frequency must be individualised. Opioids
(IM) can be given safely 6 hourly if patient is stable (IM) can be given safely 6 hourly if patient is stable • Next dose of analgesia should be given before previous Next dose of analgesia should be given before previous
dose has completely worn off dose has completely worn off • Use Use multi-modal approachmulti-modal approach. Combine use of . Combine use of
compound analgesics with NSAID. The addition of an compound analgesics with NSAID. The addition of an NSAID or paracetamol will reduce need for opioids by NSAID or paracetamol will reduce need for opioids by 30%.Also known as 30%.Also known as COMPOUND ANALGESIACOMPOUND ANALGESIA

Recommended Analgesics Recommended Analgesics • ParacetamolParacetamol (use for mild pain) Dose: 1g (use for mild pain) Dose: 1g DONOT USE in hepatic disordersDONOT USE in hepatic disorders
• Compound analgesiaCompound analgesia (use for mild-moderate pain) Action: Contain mild (use for mild-moderate pain) Action: Contain mild opioid which binds to opioid receptors in dorsal horn opioid which binds to opioid receptors in dorsal horn
Preparation of choicePreparation of choice : TRAMAL 100mg and DICLOFENAC Na 75mg : TRAMAL 100mg and DICLOFENAC Na 75mg Stronger alternativeStronger alternative : KINZ and DICLOFENAC Na 75mg : KINZ and DICLOFENAC Na 75mg Soluble preparationSoluble preparation : KINZ and PARACETAMOL 1g : KINZ and PARACETAMOL 1g
Side effectsSide effects : Constipation, nausea and vomiting and drowsiness (treat with ant-emetics : Constipation, nausea and vomiting and drowsiness (treat with ant-emetics and laxatives DO NOT WITHDRAW ANALGESIA)and laxatives DO NOT WITHDRAW ANALGESIA)
• BuprenorphineBuprenorphine can be used as an alternative for moderate to severe pain. It has less incidence of can be used as an alternative for moderate to severe pain. It has less incidence of respiratory depression and constipation. But can cause more nausea and vomiting. respiratory depression and constipation. But can cause more nausea and vomiting.
Dose: 0.3mg IM or Slow IV Push every 6hrlyDose: 0.3mg IM or Slow IV Push every 6hrly Rarely usedRarely used

Recommended Analgesics Recommended Analgesics Cont: Cont:
• NSAIDs (use with compound analgesia) Action : Inhibits inflammation (prostaglandin synthesis) that causes pain after surgery
Drug of Choice:DiclofenacNa 75mg IM Ketorolac(Toradol) 30mg
IV/IM 6h Contraindications : NSAIDs should not be
given to patients with poor renal function, dyspepsia or peptic ulcer.
• Opioids (use for moderate – severe pain with NSAID/paracetamol) Action: Binds to opioid receptors in dorsal horn
Drug of choice: Morphine/Nalbuphine(Kinz 10mg)

Recommended Analgesics Recommended Analgesics Cont: Cont:
• TRAMALTRAMAL..
Is Is TRAMADOLTRAMADOL –Non –Non 0piod agent0piod agent
100mg IV/IM 4-6hrly100mg IV/IM 4-6hrly
Max dose 400mg/dayMax dose 400mg/day
Singal Regime/Compound Singal Regime/Compound Analgesia Analgesia

Management of pain Management of pain
• Pain score Pain score mild/no painmild/no pain - consider - consider change to oral analgesia change to oral analgesia
• Pain score Pain score moderate-severemoderate-severe - Repeat - Repeat morphine/Nalbuphine/Tramal for up to morphine/Nalbuphine/Tramal for up to 2 doses and consider 2 doses and consider NSAID/paracetamol NSAID/paracetamol
• Pain score still remains Pain score still remains moderate-moderate-severesevere - - Clinical review (look for Clinical review (look for Hematoma/Wound Infection)Hematoma/Wound Infection)If not then consider 3 doses rather If not then consider 3 doses rather then 2then 2

Guidelines for Guidelines for administration of all administration of all opioids via any route opioids via any route
• All patients must have an anti-emetic All patients must have an anti-emetic
administered administered • Patients over 60 years old should have Patients over 60 years old should have
oxygen oxygen • Do not give other sedatives with opioids Do not give other sedatives with opioids • If sedation is there , respiratory rate<10 or If sedation is there , respiratory rate<10 or
BP<90mmHg STOP ALL OPIOIDS AND BP<90mmHg STOP ALL OPIOIDS AND REVIEW IN 15 MINS REVIEW IN 15 MINS
• If sedation is Unarousable, respiratory rate If sedation is Unarousable, respiratory rate <8 or BP<90mmHg STOP ALL OPIOIDS, <8 or BP<90mmHg STOP ALL OPIOIDS, TRY TO WAKE PATIENT, ADMINISTER TRY TO WAKE PATIENT, ADMINISTER OXYGEN, NEED TO CONSIDER NALOXONEOXYGEN, NEED TO CONSIDER NALOXONE
Contraindications and side Contraindications and side effects: effects:
• Liver disease and renal impairment (action of Liver disease and renal impairment (action of opioids is prolonged) opioids is prolonged)
• Causes respiratory depression which may further Causes respiratory depression which may further elevate intracranial pressure for patients with elevate intracranial pressure for patients with head injury –Opiods givenhead injury –Opiods given
• Nausea and vomiting (treat with anti-emetics) Nausea and vomiting (treat with anti-emetics) Always DO ThatAlways DO That
• Sedation Sedation • Dependence is not likely to occur when used Dependence is not likely to occur when used
appropriately for the treatment of acute pain appropriately for the treatment of acute pain • Slowing of gastric emptying and GI motility Slowing of gastric emptying and GI motility
(treat with metoclopramide)(treat with metoclopramide)

Guidelines for post-Guidelines for post-operative IV/IM analgesia operative IV/IM analgesia
• AgeAge WeightWeight Morphine/KinzDoseMorphine/KinzDose<70yrs >65Kg 10mg <70yrs >65Kg 10mg
<70yrs <65Kg 7.5mg <70yrs <65Kg 7.5mg
>70yrs >65Kg 7.5mg >70yrs >65Kg 7.5mg
>70yrs <65Kg 5mg>70yrs <65Kg 5mg

Guidelines for post-Guidelines for post-operative intramuscular operative intramuscular
analgesia Cont:analgesia Cont:• Frequency : every 5-6 hours Frequency : every 5-6 hours
providing that:providing that:
• Pain is mild to moderate Pain is mild to moderate Sedation is there Sedation is there Systolic BP >100mmHg Systolic BP >100mmHg Resp rate >10/minResp rate >10/min

Other methods of treating Other methods of treating Postop pain Postop pain
• Patient Controlled Analgesia (PCA)Patient Controlled Analgesia (PCA) PCAs are usually set up in theatre for patients PCAs are usually set up in theatre for patients
undergoing major surgery. PCAs can also be set up undergoing major surgery. PCAs can also be set up for patients that are having regular injections of an for patients that are having regular injections of an opioid . This system allows the patient to self-opioid . This system allows the patient to self-administer a small IV bolus of an opioid analgesic. administer a small IV bolus of an opioid analgesic. An IV loading dose needs to be given to establish An IV loading dose needs to be given to establish analgesia before PCA is started. The system has a analgesia before PCA is started. The system has a lockout period built into it to allow the patient to re-lockout period built into it to allow the patient to re-assess their pain before administering a further assess their pain before administering a further dose. The safety mechanism of the pump is that the dose. The safety mechanism of the pump is that the patient MUST be the only person to press the patient MUST be the only person to press the button so if they become sedated they will not be button so if they become sedated they will not be able to press the button and avoid overdose.able to press the button and avoid overdose.

Patient Controlled Analgesia Patient Controlled Analgesia (PCA) Cont:(PCA) Cont:
• Advantages: Patients experience less Advantages: Patients experience less anxiety and discomfort. The delay anxiety and discomfort. The delay associated with nurse administered IM associated with nurse administered IM analgesia does not occur analgesia does not occur
• Disadvantages: Potential for Disadvantages: Potential for malfunction and user error. malfunction and user error. Continuous training is essential. Continuous training is essential. Needs patient co-operation.Needs patient co-operation.

Patient Controlled Analgesia Patient Controlled Analgesia (PCA) Cont:(PCA) Cont:
A photo of the PCA pump that a patient may use for their own pain management.
Local Anaesthesia Local Anaesthesia
• ActionAction: Blocks transmission of nerve : Blocks transmission of nerve impulses impulses
• AdvantagesAdvantages: Profound analgesia : Profound analgesia without opioid-like side effects without opioid-like side effects
• DisadvantagesDisadvantages: Local anaesthetics : Local anaesthetics are toxic in large quantities and short are toxic in large quantities and short duration of action.techniques require duration of action.techniques require specialist skills. specialist skills.

Local Anaesthesia Cont:Local Anaesthesia Cont:• Local Infiltration of wound site at the end of Local Infiltration of wound site at the end of
operation provides short term analgesia. local operation provides short term analgesia. local anaesthetic to be injected around peripheral anaesthetic to be injected around peripheral nerves , gives excellent pain relief .Definately nerves , gives excellent pain relief .Definately applicableapplicable
• Commonly used drugs Commonly used drugs LIDOCAIN,BUPIVACAINLIDOCAIN,BUPIVACAIN..
• Either can be usedEither can be used• These can also used for These can also used for SPINAL ANASTHESIASPINAL ANASTHESIA• Spinal anaesthesiaSpinal anaesthesia blocks the nerves as they blocks the nerves as they
leave the spinal canal and before they separate leave the spinal canal and before they separate into branches, resulting in analgesia in deep into branches, resulting in analgesia in deep tissues as well as around the wound. tissues as well as around the wound. Hypotension may occur .Hypotension may occur .

IV opioid infusions IV opioid infusions
• A continuous infusion of opioid can be A continuous infusion of opioid can be effectively used post-operatively, effectively used post-operatively, especially if patient is unable to use especially if patient is unable to use PCA. Doses can be altered but it is PCA. Doses can be altered but it is not as safe as PCA and serious not as safe as PCA and serious respiratory depression, regular respiratory depression, regular monitoring required and may not be monitoring required and may not be appropriate for general wardappropriate for general ward
• NOT applicable in our systemNOT applicable in our system
Inhalation analgesia Inhalation analgesia
• Entonox (50% nitrous oxide and 50% Entonox (50% nitrous oxide and 50%
oxygen) may be useful during short oxygen) may be useful during short periods of post-operative pain periods of post-operative pain (e.g.removal of drains/dressings). It (e.g.removal of drains/dressings). It cannot be used continuously because cannot be used continuously because nitrous oxide causes bone marrow nitrous oxide causes bone marrow depression.depression.
• Should apply this.Should apply this.

WHO RecomendationWHO Recomendation
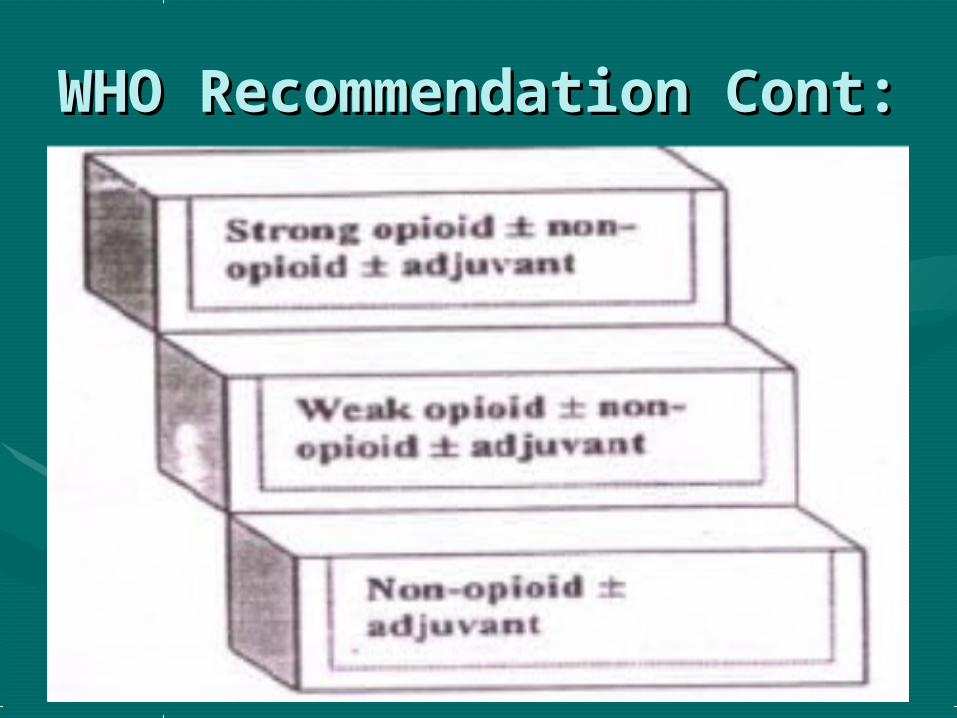
WHO Recommendation WHO Recommendation Cont:Cont:

Epidural analgesia Epidural analgesia
• A catheter can be left in place in the epidural A catheter can be left in place in the epidural
space post-operatively. A combination of space post-operatively. A combination of continuous local anaesthetic and opioid is used. continuous local anaesthetic and opioid is used.
• Advantages:Advantages: Excellent analgesia allowing early Excellent analgesia allowing early mobilisation. Reduction in stress response and mobilisation. Reduction in stress response and post-operative complications. A reduction of post-operative complications. A reduction of opioid-like side effects has been shown. opioid-like side effects has been shown.
• Disadvantages:Disadvantages: Hypotension . Risk of epidural Hypotension . Risk of epidural abcess, haematoma or nerve damage (very rare).abcess, haematoma or nerve damage (very rare).
• RARELY USEDRARELY USED

Epidural analgesia Cont:Epidural analgesia Cont:

Complementary Therapies Complementary Therapies (to be used with analgesics) (to be used with analgesics) • Reassurance. Reassurance. • Education / Information. Education / Information. • Relaxation.(muscle relaxents) Relaxation.(muscle relaxents) • Hypnosis. (Alprazolam)Hypnosis. (Alprazolam)

SUMMARY: SUMMARY: What is commonly What is commonly
accepted accepted • Proper postop pain control is key feature Proper postop pain control is key feature
in postop management.in postop management.• Patient realize that he is been treated by Patient realize that he is been treated by
good doctorgood doctor• Pain Score should be used as a ScalePain Score should be used as a Scale• Recommended Postop RegimesRecommended Postop Regimes• Choices in case of ComorbiditiesChoices in case of Comorbidities• Usage of Local Anesthesia and PCAUsage of Local Anesthesia and PCA• Other Modalities like EpiduralOther Modalities like Epidural• Clinical importance of Pain management Clinical importance of Pain management

MCQs 1MCQs 1
• The local infiltration anesthetic drugThe local infiltration anesthetic drug
1.is ineffective if introduced into an area of 1.is ineffective if introduced into an area of infection.infection.
2.is contraindicated in any clotting 2.is contraindicated in any clotting disorder.disorder.
3.is free from toxic effects.3.is free from toxic effects.
4.with adrenaline is contraindicated if the 4.with adrenaline is contraindicated if the patient is taking tricyclic antidepresant.patient is taking tricyclic antidepresant.
5.usually used with adrenaline.5.usually used with adrenaline.

MCQs Cont: 2MCQs Cont: 2
• Morphine is given for injured Morphine is given for injured primarily because it isprimarily because it is
1.a sedative1.a sedative
2.an analgesic2.an analgesic
3.a diaphoretic 3.a diaphoretic
4.an emetic4.an emetic
5.a mood stimulant5.a mood stimulant
MCQs Cont: 3MCQs Cont: 3• Pt underwent Pyelolithotomy,postop Pt underwent Pyelolithotomy,postop
analgesiaanalgesia
1.Morphine1.Morphine
2.Morphine +Diclofenac Na2.Morphine +Diclofenac Na
3.Tramal+DiclofenacNa3.Tramal+DiclofenacNa
4.Ketorolac4.Ketorolac
5.Nalbuphine+Paracetamol5.Nalbuphine+Paracetamol

MCQs Cont: 4MCQs Cont: 4• Pt underwent Tube Pt underwent Tube
Thoracostomy,analgesia should beThoracostomy,analgesia should be
1.Oral DiclofenacNa1.Oral DiclofenacNa
2.Oral preparation of Tramadol2.Oral preparation of Tramadol
3.IM DiclofenacNa3.IM DiclofenacNa
4.IV Paracetamol(PROVAS)4.IV Paracetamol(PROVAS)
5.Local Anesthetic agent 5.Local Anesthetic agent

MCQs Cont: 5MCQs Cont: 5• Pt is operated for Esophageal varices Pt is operated for Esophageal varices
with Sclerotherapy,postop analgesiawith Sclerotherapy,postop analgesia
1.IM Paracetamol(Detamol)1.IM Paracetamol(Detamol)
2.IV Paracetamol(Provas) 1g2.IV Paracetamol(Provas) 1g
3.Tramal+Provas3.Tramal+Provas
4.IM Morphine4.IM Morphine
5.Tramal+DiclofenacNA5.Tramal+DiclofenacNA

MCQs Cont: 6MCQs Cont: 6• Pt is a case of Warfare injuries,one leg Pt is a case of Warfare injuries,one leg
and one arm amputated,and one deep and one arm amputated,and one deep wound on another leg,postop analgesiawound on another leg,postop analgesia
1.IV Morphine 10mg TDS1.IV Morphine 10mg TDS
2.Nalbuphine 10mg IV TDS2.Nalbuphine 10mg IV TDS
3.Nalbuphine 10mg IV 3.Nalbuphine 10mg IV BD+DiclofenacNa 75mg IM BD+DiclofenacNa 75mg IM TDSTDS
4.Nalbuphine 10mg IV BD+Provas IV 4.Nalbuphine 10mg IV BD+Provas IV 1g TDS1g TDS
5.PCA with nalbuphine5.PCA with nalbuphine

Thank YouThank You