Embed Size (px)
Citation preview

British Journal of Anaesthesia 1995; 74: 100-103
EQUIPMENT
Overfill testing of anaesthetic vaporizers
E. PALAYIWA AND C. E. W. HAHN
Summary
We tested six anaesthetic vaporizers with keyedfiller adaptors to see if it was possible to overfillthem. For those vaporizers which could be over-filled, the maximum level of overfill was determinedand the effect of overfilling on the vaporizer outputconcentration was measured. Three of thevaporizers, the TEC 4, PPV Mk 1 and MIEVapamasta 5, could be overfilled. In the case of theTEC 4 and PPV vaporizers, overfilling by more than100 ml caused a large increase in the vaporizeroutput concentration. Overfilling the Vapamasta 5by this amount caused the output concentration todecrease. (Br. J. Anaesth. 1995; 74: 100-103)
Key wordsEquipment, vaporizers.
Keyed fillers were developed as a safety feature onanaesthetic vaporizers to prevent accidental fillingwith the wrong agent. However, all users of keyedfillers are familiar with the problems which thesedevices caused. Air locks may make filling thevaporizer almost impossible and busy staff may betempted to develop their own techniques to over-come this. Unfortunately, these "in-house"techniques, which are contrary to the manu-facturer's instructions on filling, may allow thevaporizer to be overfilled. A recent Safety ActionBulletin [1] pointed out that it is possible to overfillthe Fluotec 4 vaporizer. The aim of this study was toexamine several commonly used vaporizers whichhave keyed fillers to determine: (a) if overfilling ofeach vaporizer is possible; (b) to what extent eachvaporizer can be overfilled; and (c) the effect ofdifferent levels of overfilling on vaporizer output.
Methods
VAPORIZERS
We examined the following vaporizers: (i) Fluotec 3(halothane), (ii) Tec 4 (enflurane), (iii) PenlonAbingdon vaporizer (halothane), (iv) Penlon PPV(isoflurane), (v) Drager Vapor 19 (isoflurane) and(vi) MIE Vapamasta 5 (isoflurane).
It is clear from the above that the same anaestheticagent was not used throughout the studies describedin this paper, as we could only use vaporizers whichwere readily available to us. However, we have
assumed that all vaporizers of a particular design willbehave in a similar fashion when filled with otheragents.
OVERFILLING TECHNIQUE
It is common practice for staff experiencing diffi-culties when filling vaporizers to turn them to the"on" position. We found that it was not possible tooverfill any of the vaporizers by this manoeuvrealone if the filler cap formed a good seal with thebottle. Also, it was not possible to overfill thevaporizer by loosening the seal with the vaporizerturned "off". However, if the connection betweenthe bottle of agent and the filler cap was loosenedwhile the vaporizer was turned "on", overfilling waspossible in some cases. In these instances, the use ofan old filler cap which did not form a proper sealwith the bottle would also allow overfilling if itsvaporizer was turned "on".
The vaporizers which could not be overfilled werethe Abingdon vaporizer, Fluotec 3 and Drager Vapor19. All of these vaporizers had drainage holes whichcaused excess liquid to drain out. Thus we studiedonly the TEC 4, PPV and Vapamasta vaporizers.
MAXIMUM OVERFILL LEVELS
In order to determine the maximum amount bywhich it was possible to overfill each of the remainingvaporizers, the test vaporizers were first filled to the"max " level using the manufacturer's recommendedtechnique. The "max" was denned as the maximumlevel of filling possible using the manufacturer'srecommended technique and was indicated by themarking on the sight glass. The volume of liquidrequired to reach this level was not measured. Theagent bottle and filler cap were then weighed and thevaporizer overfilled maximally after which anotherweighing was carried out. It was found that over-filling progressed easily and rapidly at first until apoint was reached where it became difficult to addmore liquid. At this point it was necessary to tilt thebottle in the filler cap in order to introduce moreliquid and only a few extra millilitres could be addedin this way.
E. PALAYIWA, MA, PHD, C. E. W. HAHN, MA, BSC, MSC, DPHIL,Nuffield Department of Anaesthetics, John Radcliffe Hospital,Headington, Oxford OX3 9DU. Accepted for publication:August 1, 1994.
Dow
nloaded from https://academ
ic.oup.com/bja/article/74/1/100/260405 by guest on 14 February 2022

Overfill testing of anaesthetic vaporizers
MEASUREMENT OF OUTPUT
The output of each test vaporizer was measuredwhen filled to the "max" level and at various levelsof overfilling. A flow rate of oxygen 4 litre mkr1 wasused and the dial settings were 0.6, 1.0 and 2 % v/v.A mass spectrometer (Centronics MGA 200) whichhad been calibrated for the vapour channel using aRiken refractometer was used to measure vapourconcentrations [2]. A plot was made of vaporizeragent concentration output, as measured by the massspectrometer, vs overfill level at each of the dialsettings. The variation in this output concentrationwith time was recorded on chart paper by connectingthe output of the mass spectrometer to a Y-t penrecorder (Linear Corder Mark VII, Watanabe).
The output of each vaporizer was also recordedwhen switched off and at the 0 % dial setting.
Results
The maximum overfill level for each vaporizer was asfollows: TEC 4 =132 ml, PPV = 134 ml andVapamasta =131 ml. Figures 1, 2 and 3 show theoutputs of the TEC 4, PPV and Vapamastavaporizers at the 0.6, 1.0 and 2 % dial settings whenoverfilled to different levels. Readings were obtained1 min after changing the dial setting since, par-ticularly at high overfill levels, the output may varywith time. For all vaporizers die output remainedconstant for overfill levels up to 50 ml. The sectionsof the graphs for overfill volumes greater than 100 mlgive only a qualitative indication of what happens atthese volumes as output may be variable with time atthese volumes.
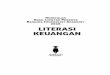
In the case of the TEC 4, enflurane output thenbegan to decrease and reached a minimum atapproximately 90 ml. After this there was a markedincrease in the vaporizer output concentration.Figure 4 shows the output of the TEC 4 at the 0.6 %setting varied with time when the vaporizer wasoverfilled by 127 ml. (This was the initial level ofoverfilling. Obviously, as evaporation takes place theoverall volume will reduce.) The output remainedrelatively constant at approximately 1.6% v/v forapproximately 14 min. The dial setting was thenincreased to 1 % and the output increased to 2.4 %over the next 1 min and then decreased suddenly tozero. After the output had remained at zero for5 min, the flow of gas was increased slightly, byabout 200 ml min"1. This caused an increase inoutput for 1 min and the maximum output obtainedin this period was more than 7 % v/v. The outputthen decreased to 0.2%. When the dial setting wasincreased to 2% the output was very variablebetween 0.4 % and 2 % over the next 5 min and thenstabilized at approximately 0.5 % v/v (fig. 4) whenoverfilled by 132 ml; at the 0 % setting, a bolus of gascontaining more than 3 % vapour was seen for lessthan 10 s. When the dial was set to 0.6 %, output wasinitially less than 0.4% but then increased rapidlyand varied between 3 and 4 %. When the dial settingwas increased to 1 %, output became very variable,between 4.5 and 7%, for approximately 3 min
101
when it decreased rapidly to about 0.4 % v/v withoccasional small increases.
The PPV vaporizer behaved in a similar manner to
C , Iaj 6 •
5-
4-
o
oQ.
-A—A
I D-..
50 100Overfill volume (ml)
150
Figure 1 Output of the TEC 4 enflurane vaporizer at dialsettings 0.6 ( # ) , 1.0 ( • ) and 2.0% (A) when overfilled bydifferent levels.
CDCCD
50 100Overfill volume (ml)
150
Figure 2 Output of the PPV Mk 1 isoflurane vaporizer at dialsettings 0.6 ( • ) , 1.0 ( • ) and 2.0% (A) when overfilled bydifferent levels.
CDC
23
o
ao
oa.
-IV.
-O- ,"D-.
50 100Overfill volume (ml)
150
Figure 3 Output of the Vapamasta isoflurane vaporizer at dialsettings 0.6 ( # ) , 1.0 ( • ) and 2.0% (A) when overfilled bydifferent levels.
Dow
nloaded from https://academ
ic.oup.com/bja/article/74/1/100/260405 by guest on 14 February 2022
102 British Journal of Anaesthesia
— Q Dial 0%afi °~|Off.
Flow rate incrsa:by 200 ml mirr'
Dial 0.6% Dial 1%Dial 2%
Time—» 1 mln
Figure 4 Variation of output of the TEC 4 enflurane vaporizer with time when overfilled by 127 ml with the dialset at 0.6%.
£20,
cucoO o-J
Dial 2%
Time-
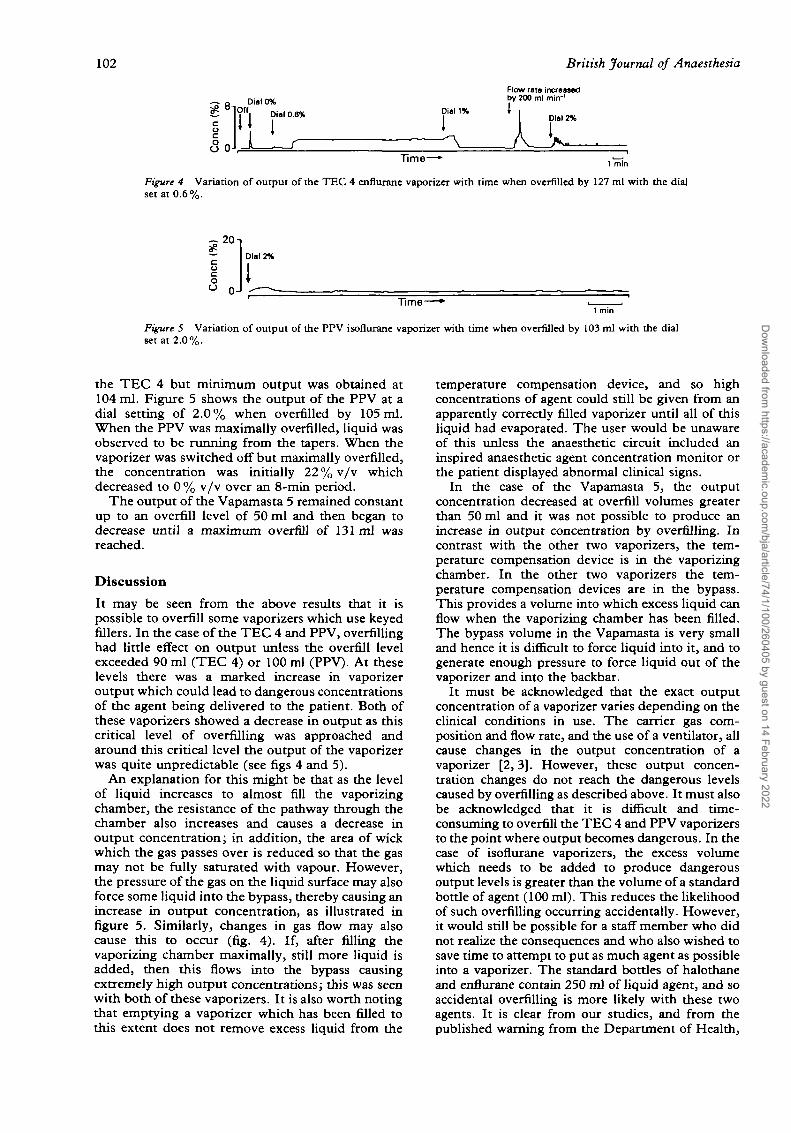
Figure 5 Variation of output of the PPV isoflurane vaporizer with time when overfilled by 103 ml with the dialset at 2.0%.
the TEC 4 but minimum output was obtained at104 ml. Figure 5 shows the output of the PPV at adial setting of 2.0% when overfilled by 105 ml.When the PPV was maximally overfilled, liquid wasobserved to be running from the tapers. When thevaporizer was switched off but maximally overfilled,the concentration was initially 22 % v/v whichdecreased to 0 % v/v over an 8-min period.
The output of the Vapamasta 5 remained constantup to an overfill level of 50 ml and then began todecrease until a maximum overfill of 131 ml wasreached.
Discussion
It may be seen from the above results that it ispossible to overfill some vaporizers which use keyedfillers. In the case of the TEC 4 and PPV, overfillinghad little effect on output unless the overfill levelexceeded 90 ml (TEC 4) or 100 ml (PPV). At theselevels there was a marked increase in vaporizeroutput which could lead to dangerous concentrationsof the agent being delivered to the patient. Both ofthese vaporizers showed a decrease in output as thiscritical level of overfilling was approached andaround this critical level the output of the vaporizerwas quite unpredictable (see figs 4 and 5).
An explanation for this might be that as the levelof liquid increases to almost fill the vaporizingchamber, the resistance of the pathway through thechamber also increases and causes a decrease inoutput concentration; in addition, the area of wickwhich the gas passes over is reduced so that the gasmay not be fully saturated with vapour. However,the pressure of the gas on the liquid surface may alsoforce some liquid into the bypass, thereby causing anincrease in output concentration, as illustrated infigure 5. Similarly, changes in gas flow may alsocause this to occur (fig. 4). If, after filling thevaporizing chamber maximally, still more liquid isadded, then this flows into the bypass causingextremely high output concentrations; this was seenwith both of these vaporizers. It is also worth notingthat emptying a vaporizer which has been filled tothis extent does not remove excess liquid from the
temperature compensation device, and so highconcentrations of agent could still be given from anapparently correctly filled vaporizer until all of thisliquid had evaporated. The user would be unawareof this unless the anaesthetic circuit included aninspired anaesthetic agent concentration monitor orthe patient displayed abnormal clinical signs.
In the case of the Vapamasta 5, the outputconcentration decreased at overfill volumes greaterthan 50 ml and it was not possible to produce anincrease in output concentration by overfilling. Incontrast with the other two vaporizers, the tem-perature compensation device is in the vaporizingchamber. In the other two vaporizers the tem-perature compensation devices are in the bypass.This provides a volume into which excess liquid canflow when the vaporizing chamber has been filled.The bypass volume in the Vapamasta is very smalland hence it is difficult to force liquid into it, and togenerate enough pressure to force liquid out of thevaporizer and into the backbar.
It must be acknowledged that the exact outputconcentration of a vaporizer varies depending on theclinical conditions in use. The carrier gas com-position and flow rate, and the use of a ventilator, allcause changes in the output concentration of avaporizer [2,3]. However, these output concen-tration changes do not reach the dangerous levelscaused by overfilling as described above. It must alsobe acknowledged that it is difficult and time-consuming to overfill the TEC 4 and PPV vaporizersto the point where output becomes dangerous. In thecase of isoflurane vaporizers, the excess volumewhich needs to be added to produce dangerousoutput levels is greater than the volume of a standardbottle of agent (100 ml). This reduces the likelihoodof such overfilling occurring accidentally. However,it would still be possible for a staff member who didnot realize the consequences and who also wished tosave time to attempt to put as much agent as possibleinto a vaporizer. The standard bottles of halothaneand enflurane contain 250 ml of liquid agent, and soaccidental overfilling is more likely with these twoagents. It is clear from our studies, and from thepublished warning from the Department of Health,
Dow
nloaded from https://academ
ic.oup.com/bja/article/74/1/100/260405 by guest on 14 February 2022

Stay Informed
Order your
subscription to
BJA:INTERNATIONAL
JOURNAL OF
ANAESTHESIA
NOW
N.B Canadian subscribers must add"̂ o GST to quoted sterling price-Subscribers in Italy must add 4% IVAlo the quoted sterling price, unlessthey can provide an IVA registrationnumber. Subscribers in the IrishRepublic must add 21% VAT to thequoted sterling price, unless they canprovide a VAT registration number-Subscribers in Belgium must add 6%TVA BTVC' to the quoted sterlingprice, unless they can provide aTVA BTW registration number.
O R D E R F O R MBJA: INTERNATIONAL JOURNALOF ANAESTHESIAPUBLICATION: Monthly ISSN: 0007-09121995 SUBSCRIPTION RATE:WORLDWIDE: £149. (USA Only: $223)•IARS MEMBERS RATE:£73, (USA Only: $115)Please tickQ Please enter my subscription
start dateQ Please send me Instructions to AuthorsQ I enclose a cheque for
(Payable to British Medical Journal)
• I wish to pay by credit card.American Express/Visa/Mastercard(Delete as appropriate)
•Members of the International Anaesthesia Research Society(IARS) may subscribe at the reduced rate.
CARD NUMBER
MasterCard users should add the number appearing above their name
EXPIRY DATE .
SIGNATURE(Your signature is essential, especially when paying by credit card)
NAME
ADDRESS.
DATE.
Send Orders to: BMJ Publishing Group, BMJ Marketing, P.O. Box 299 London WC1H 9TD, UKor BMJ Publishing Group, Box No 408, Franklin, MA 02038, USA.
Stay InformedOrder your
subscription to
BJA:INTERNATIONAL
JOURNAL OF
ANAESTHESIA
NOW
N.B Canadian subscribers musi add7% GST to quoted sterling priceSubscribers in Italy must add 4% IVAto the quoted sterling price, unlevsthey tan provide an IVA registrationnumber. Subscribers in the IrishRepublic must add 21% VAT to (hequoted sterling price, unless they canprovide a VAT registration numberSubscribers in Belgium must add 6%TVA • BTW to the quoted sterlingprice, unlevs they can provide aTVA BTW registration number
O R D E R F O R MCARD NUMBERBJA: INTERNATIONAL JOURNAL
OF ANAESTHESIAPUBLICATION: Monthly ISSN: 0007-09121995 SUBSCRIPTION RATE:WORLDWIDE: £149, (USA Only: $223)•IARS MEMBERS RATE:±73, (USA Only: $115)Please tickQ Please enter my subscription
start date ____Q Please send me Instructions to AuthorsQ I enclose a cheque for
(Payable to British Medical Journal)
Q I wish to pay by credit card.American Express/Visa/Mastercard(Delete as appropriate)
"Members of (he International. Anaesthesia Research Society(IARS) may subscribe at the reduced rate
MaslcrOrd users should add the number appearing above iheir name
EXPIRY DATE.
SIGNATURE(Your signature is essential, especially when paying by credit card)
NAME.
ADDRESS.
DATE.
Send Orders to: BMJ Publishing Group, BMJ Marketing, P.O. Box 299 London WC1H 9TD, UKor BMJ Publishing Group, Box No 408, Franklin, MA 02038, USA.
Stay Informed
Order your
subscription to
BJA:INTERNATIONAL
JOURNAL OF
ANAESTHESIA
NOW
N B Canadian subscribers musi ackl""% GST lo qiKXed sterling price.Subscribers in Italy mus( add 4% IVAlo the quoced sterling price, unlessthey can provide an IVA registrationnumber Subscriber* in the IrishRepublic musi add 21% VAT to thequoted sterling price, unles-s they canprovide a VAT registration number.Subscribers in Belgium must add ft%TVA. BTW to (he quoted sterlingprice, unless they can provide aTVA/BTW registration number
O R D E R F O R MBJA: INTERNATIONAL JOURNALOF ANAESTHESIAPUBLICATION: Monthly ISSN: 0007-09121995 SUBSCRIPTION RATE:WORLDWIDE: £149, (USA Only: $223)•IARS MEMBERS RATE:£73, (USA Only: $115)Please tickQ Please enter my subscription
start dateQ Please send me Instructions to AuthorsQ I enclose a cheque for
(Payable to British Medical Journal)
Q I wish to pay by credit card.American Express/Visa/Mastercard(Delete as appropriate)
•Members of the International Anaesthesia Research Society(IARS) may subscribe at the reduced rate.
CARD NUMBER
MasterCard users should add (tie number appearing above their name
EXPIRY DATE
SIGNATURE(Your signature is essential, especially when paying by credit card)
NAME
ADDRESS.
DATE.
Send Orders to: BMJ Publishing Group, BMJ Marketing, P.O. Box 299 London WC1H 9TD, UKor BMJ Publishing Group, Box No 408, Franklin, MA 02038, USA.
Dow
nloaded from https://academ
ic.oup.com/bja/article/74/1/100/260405 by guest on 14 February 2022
Dow
nloaded from https://academ
ic.oup.com/bja/article/74/1/100/260405 by guest on 14 February 2022
Overfill testing of anaesthetic vaporizers 103
that such levels of overfilling can occur if staffindulge in dangerous practices.
References1. Department of Health. Anaesthetic agent vaporizers fitted
with agent specific fillers: Reports of overfilling. SafetyAction Bulletin 1992; 82: SAB (92) 29.
2. Palayiwa E, Sanderson MH, Hahn CEW. Effects of carriergas composition on the output of six anaesthetic vaporizers.British Journal of Anaesthesia 1983; 55: 1025-1038.
3. Hill DW, Lowe HJ. Comparison of concentrations ofhalothane in closed and semi-closed circuits during controlledventilation. Anesthesiology 1962; 23: 291.
Dow
nloaded from https://academ
ic.oup.com/bja/article/74/1/100/260405 by guest on 14 February 2022