Embed Size (px)
Citation preview
ORIGINAL ARTICLE
Our Experience in Lower Limb Reconstruction WithPerforator Flaps
Jaume Masia, MD, PhD, Fabrizio Moscatiello, MD, Gemma Pons, MD, Manuel Fernandez, }"fD,Susana Lopez, MD, and Pere Serret, MD
Abstraet: The application of Taylor's concept about body angio-somes, referred to tissue transfers, has meant that the developmentof the perforator flaps and musc1es is no longer needed as a carrierof skin flap vascularity. In this papel', \Ve revise 59 lower limbreconstructions with local and free perforator flaps perfonned in thelast 5 years, and a basic reconstructive algorithm is also suggested lohelp with the management of the lower limb soft tissue reconstruc-tion with perforator flaps.
The advantages of the perforator flaps are (1) muscles and theirfunction are preserved; (2) the main vascular lrunks are spared; (3)it is possible to make a more specific rcconstruclion, replacing "likcwith like" (even perfonning compound or chimeric flaps); (4) thedonar site can often be c10sed primarily; (5) the general morbidity isreduced; (6) a bener cosmetic result can be achieved.
Key Words: perforator flap, propeller, lower limb reconstruction
(Ann Plus! Surg 2007;58: 507-512)
The lower limb has always been known for poor woundhealing ami, since the first steps of the plastic surgery, as
a scarce sourcc 01'flaps. Before the introduction of microsur-gcry, surgeons had few reconstructive options such as localflaps (random skin flaps, muscular or musculocutancousflaps) and performed cross-legs, immobilizing the limbs forweeks, to transfer a large amount of skin. 1
With the introduction 01'microsurgery, tissue transfershave become one 01' the main reconstructive options for thelower limb, above al! in those arcas where there is a scarceavailability of local flaps. In the distal third 01'the leg or inorthopedic problcms, a muscular local flap could worsen asignificant muscular function.
With the deveIopment 01'perforator flaps,2.3newer andmore reliable flaps have become avai]able for lower limb recon-
Received July 4, 2006 and accepted for publication July 20, 2006.From the Department of Plastic Surgery, Hospital dc la Santa Creu i Sant Pau
(Universitat Autonoma de Barcelona), Barcelona, Spain.No sources of support that require acknowledgment.Reprints: Jaume Masia, MD, PhD. Chief ofDepartmentiAssociate Profcssor,
Department of Plastic Surgery, Hospital de la Santa Creu i Sant Pau(Universitat Autonoma de Barcelona), Sant Antoni M. Claret 167,08025Barcelona, Spain. E-mail: [email protected].
Copyright rg 2007 by Lippincott Williams & WilkinsISSN: 0148-7043/07/5805-0507
DOI: 10.1097/0 l.s"p.0000239841.47088.a5
Annals of Plastic Surgery . Volume 58, Number 5, May 2007
struction. Referring to Taylor and Palmer's4 and Taylor's5 con-cept 01' angiosomes, almost al! the tissues 01'an angiosomecan be harvested on I adequate perforator vessel. The per-forator pedic1es 01' these flaps originate from one 01' themain vessels 01' the lower extremity, course through I ormore musc1es or one 01' the intermuscular septa IIp to thefascia, and ramify at a sllprafascial level in the subcuta-neous fat.
Perforator flaps can be used as local or free flaps.Whenever the defect size and the vascular condition 01' theneighboring tissues alJow a reconstruction with local perfo-rator flaps, the surgicaJ intervention and the morbidity oughtto be limited to a single body region. The early designs of thelocal flaps along the vertical axis of the leg or the thigh witha proximal pedicle have been modified by the use 01'perfo-rator flaps. To transfer a larger amount of tisslle rather thanrandom local flaps, a surgeon can carefully isolate the wholecourse of a perforator vessel and effectively rotate through180°, like a "propeller," almost all the tissues 01'an angio-some or more (descending genicular,6 posterior tibial,7,8 per-oneaI9). Tissue transfer through a rotation like a propelJer wasfirstly dcscribed by Hyakusoku et allOin 1991 to release scarcontractllres ofthe lIpper limb by subcutaneOLlSpedicled flapsrotated through 90°. The propeller method applied to perfo-rator flaps becomes a microsurgical technique where thedissection of the pedicJe is carried out with binocular mag-nifying glasses but a microvasclllar anastomosis is notneeded.
When it is not possible to choose a local perforator flap,limiting the morbidity to a single region 01' the body, freeperforator tissue transfers from other regions can be per-formed. GeneralJy, we use anterolateral thigh (ALT)! t orthoracodorsal artery perforator (TAP) 12perforator free flaps.In composite-tissue loss, it is possible to harvest a compoundflap, for example, by inclusion 01'the fascia lata in the ALTto reconstruct a tendon of one of the main joints, or a"chimeric" flap,13 where each component 01'the flap can beseparately placed because each is supplied by a distinctbranch 01'the common source vessel.
This review, derived from ollr experience in reconstruc-tion of oncologic and orthopaedic lower limb defects, couldsuggest the use of local or free perforator tissue transfers in10wer limb soft tissue reconstruction and further propose aneasy algorithm regarding which would be the most effectivefor patient rehabilitation.
507
Copyriqt,t~:;jLippincottWílliams& Wilkins.Unauthorizedreproductionof this artide is prohiblted.
Masia el al Annals of PlasticSurgery . Volume 58, Number 5, May 2007
MATERIALS AND METHODS
From December 2000 to June 2005, 59 perforator flapswere performed in 35 male and 24 female patients. The meanage was 43 years. Five patients usually smoked more than 20cig/d. Three patients had type II diabetes. Follow-up timeranged from 5 months to 4 years.
Our series was as follows (Table 1): 35 local perforatorflaps, transferred with the propeller method, were performedfor soft tissue reconstructions after oncologic resections,traumas, and unstable scars; 19 patients underwent an ALTFfor chronic osteomyelitis and oncologic resections; 5 TAPFwere used to reconstruct oncologic resections and chronicosteomyelitis.
Among the 59 perforator flaps performed, 2 chimericflaps and 1 compound flap were carried out. One patient hada bimalleolar fracture of the left inferior limb, with Achillestendon and bone exposed. A chimeric ALTF with vastuslateralis was performed. Another patient underwent a "chi-meric" TAP with latissimus dorsi, used as a razor flap,14 forchronic osteomyelitis after oncologic and orthopedic surgery.A compound flap was carried out in a patient with an infectedrupturc of the rotulean tendon after a prosthetic implant andan ALTF flap with vascularized fascia lata were performed.
Patients with chronic osteomyelitis, prior to flap cov-erage, were additionally treated with preoperative and post-operative culture-specific antibiotics, and an intraoperativeradical debridcment was performed until only healthy tissueremained in the wound bed. Infected and devitalized bonewas removed until active bone bleeding was observed.
'Planning a perforator flap, the location ofthe perforatorvessel was dcfincd with the assistance of Doppler ultrasound,
TABLE1. Fifty-NineLocaland FreePerforatorFlapsWerePerformed for 50ft Tissue Lower Limb Reconstruction in thePeriod Between December 2000 and June 2005
No. FlapsMeanAgeSex
Local perforator flaps(propeller method)
Oncologic surgeryTraumas
Unstable scars
9
14
12
ALTF
Chronic osteomyelitis
Oncologic sllrgeryTAPF
7
10
Chronic o,teomyelilis
Oncologic surgery
Chimeric and compoundlIaps
Traumas
3
1 ALTF with vasluslateralis
Chronic osteomyelilis
After onhopedicsurgery
After oncologic andonhopedic surgery
Total
1 ALTF with fascialata
1 T APF with LD
(razor lIap)59
508
but its use is only orientative because of some false posi-tives.ls It is not possible to study the size and the course ofthe perforator vessel with Doppler. The right technique tofind a suitable perforator is intraoperative assessment carriedout with an exploratory incision on one of the flap bordcrs.
In posttraumatic situations, in elderly patients withvascular disease, in uncertain vascular viability, or in freetissue transfers, preoperative arteriography could be useful indetermining the degree of patency of the main vessels.
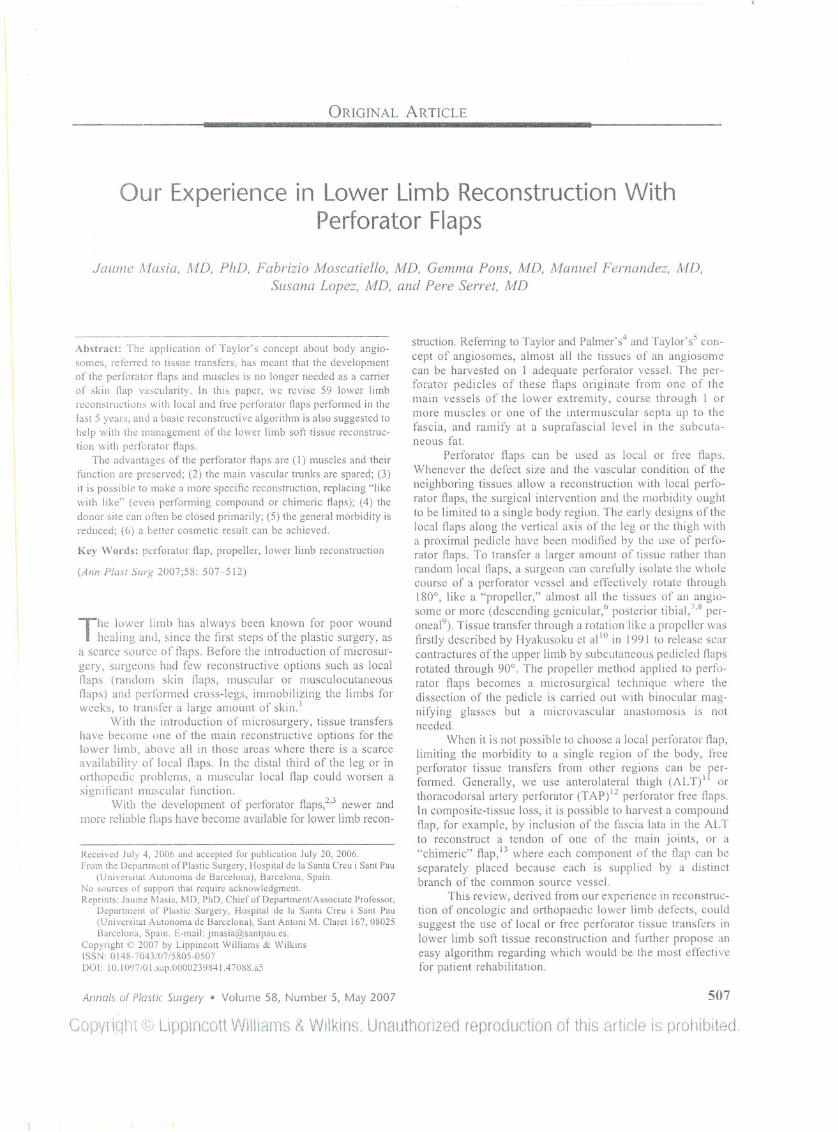
In the last patient, a new tcchnology of perforatormapping was uscd by the aid of mllltidetector row-computedtomography (Fig. 1). This technology proved to be veryeffective and useflll in planning perforator abdominalflaps.16.17Unfortunately, \Vecannot yet show the reslllts of itsclinical application in preoperative mapping of perforatorflaps in lower limb reconstruction because we have not yet alarge series.
Our surgical strategy for harvesting a perforator flap isas follows: we perform an exploratory incision of a border ofthe flap, throllgh the skin, sllbcutaneous tissue, and deepfascia. With a subfascial approach, the flap is paJ1ially raisedto identify the location and the size of the perforators. Whena perforator vessel of adequate size is identified, we separateit back to the source vessel. If the perforator previollslyidentified by Doppler is not adequate, we look for anothersuitablc perforator vessel and adapt the flap design.18 Onlywith the perforator isolated and dissected are the remaining
FIGURE 1. An example of a preoperative perforators map-ping with the aid of the multidetector row-computed to-mography.
Copyriqht @Upplncott WiUlams& Wílkjns.Unauthorizedreproductionof thisarticleis prohibited.
~ 2007 Lippincott Wi/lialns & Wilkins
2F,7M 56
6F,8M 47
9F,3M 33
2F,5M 41
4F,6M 52
lF 43
3M 46
1M 42
1M 53
1M 20
24F, 35M 43
Annals of Plastic Surgery . Volume 58, Number 5, May 2007 Perforator Flaps Lower Umb
borders of the flap incised and is the flap quite easily raisedfrom the underlying muscle.
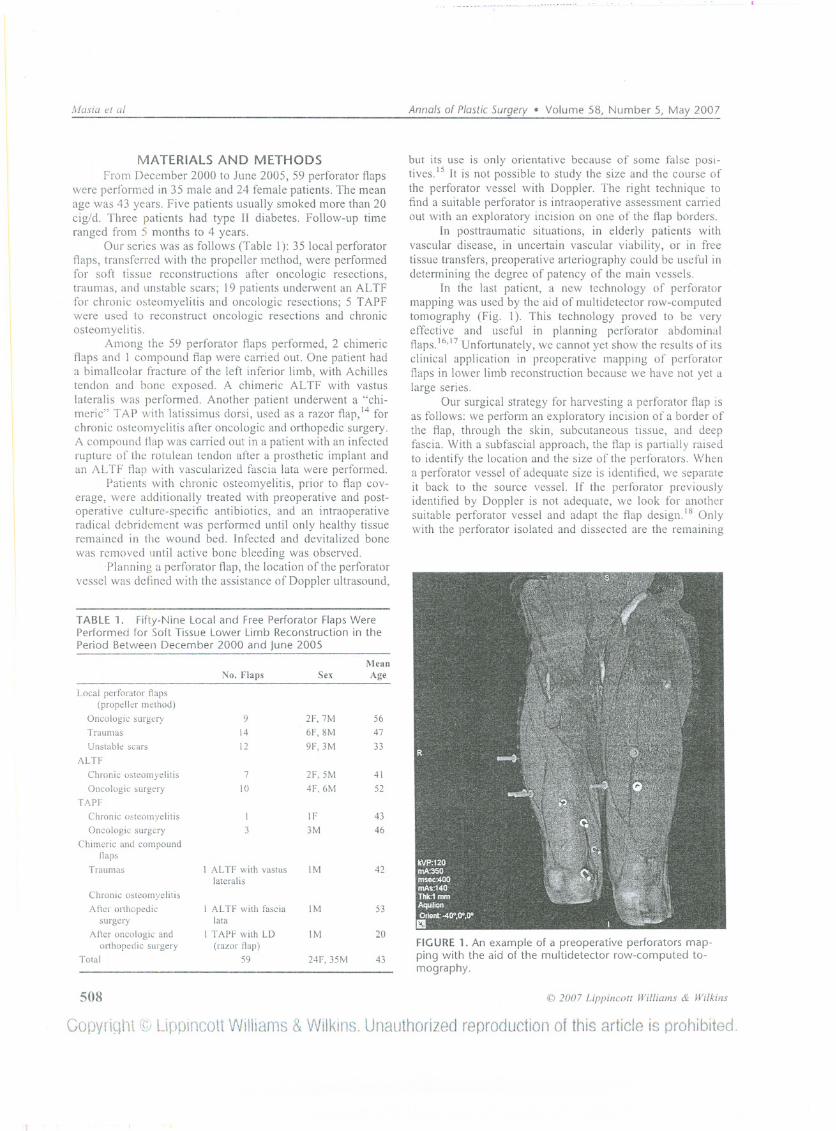
In the design of perforator flap as a "propeller,,,19 weconsider the location of the perforator as a pivot point (Fig.2). The distance between the proximal border of the flap andthe pivot point (A in Fig. 2) has to be a httle longer (1.5-2cm) than the 1ength between the pivot point and the farthestborder of the injury zone (B + e in Fig. 2). So, after therotation of the flap, the suture can be performed without anytension.
In the ALT perforator flap, the patient is placed insupine position. A line is drawn between the anterior superioriliac spine amI superolateral border of the patella. The per-forators are concentrated in a circle of 6 cm at the midpointof the marked line. The flap is designed in an eIJipticalvertical skin island. It is possible to directly close the donorsite with a flap width less than 8 cm?O
In the TAP flap, the patient is placed in supine position,with the homolateral arm elevated and a httle torsion of thethorax. The lateral border of the latissimus dorsi muscle ismarked. The perforators are normally about 6-8 cm belowthe posterior axillary fold and 2-4 cm inside the lateralborder of the latissimus. Additional perforators could beidentified at 1.5- to 4.0-cm intervals below to the first. Thewidth is detennined by the pinch test to determine what canbe closed primarily. Flaps up to 25 cm in length have beenreported2!
RESULTS
Our overall results include resolution of the problempresented in 93.2% of cases (55 of 59); there were 4 flaplosses (6.8%). Two losses occurred for a compression of thepedicle by a hematoma not drained quickly enough; 2 lossesdue to a compression of the flap from incorrect patientpositioning in bed. In all these cases, a second operation witha latissimus dorsi free flap was performed. Partial necrosis<20% occurred in 3 propeller ftaps (5%) in heavy-smokerpatients; partialnecrosis >20% happened in I propeller flap(1%) in a diabetic patient. AlI these cases occurred when theflap extended farther than the angiosome territory corre-sponding to the chosen perforator. The vascular connectionsbetween the angiosomes showed themselves to be inadequateto nourish the distal part of the flap, probably due to themicrovascular damage caused by smoke and diabetes. Sec-ondary healing was suitable in these cases. Some delayedrefinemcnts wcre carricd out to achicvc bcttcr cosmetic rc-sults such as a debulking procedure, liposuction mediated,22in a patient where an ALT perforator flap was used to covera dorsal aspect of a foot.
DISCUSSION
In recent years, perforator flaps have become one ofthemost useful surgical options in soft tissue lower limb recon-struction. In local flaps reconstructions, the harvesting of apcrforator-based flap guarantccs a morc rcliablc vasculariza-
FIGURE2. Schematicposteriortibialartery perforatorflapwith the propellertransfermethod. 1.We calculatethe total lengthof the flap by measuring the distance between the pivot point, identified by Doppler ultrasound, and the farthest border ofthe injury zone (distance A is 1.5-2 cm longer than B + C, so that, after rotation, the flap is sutured without any tension). 11.With the exploratory incision the most suitable perforator is evaluated and the flap design is adapted to the location of thenew pivot point. 111.The propeller movement of the flap. IV. Flap rotated through 1800 to cover the injury zone. V. Two years'postoperative result.
«J 2007 Lippincot{ Williams & Wilkins 509
Copyrintlt CQ)Uppincott Williams &WJlkins.Unauthorízed reproduction of this article is prohibited.

Masia el al Anna/s of P/asticSurgery . Volume 58, Number 5, May 2007
Defect Size
smal~~
Medium Large
FIGURE 3. Algorithm for lower limbsoft tissue reconstruction with perfora-tor flaps.
Perforator ALTFlocal flaps(propeller method)
tion, greater possibility of movement, and a larger amount ofavailable tissue than the classic random flaps. In free-flapreconstructions, perforator flaps have indications (in orthopedicand oncologic surgery, radiodermitis, osteomyelitis, etc) thatoverlap with musculocutaneous flaps but present reduced mor-bidity. Free perforator flaps can provide the same amount oftissue and the same vascular supply as a musculocutaneous flap.
Planning a lower limb reconstruction, we evaluate thedefect size, the structures involved in the defect, whether thevascular condition of the neighboring tissues is adequate ornot, the vascular anatomy of the extremity, the donor-sitequality and the vascular pedic1e length needed. Wheneverpossible, the surgical intervention and the morbidity ought tobe limited to a single body region.
Perforator ALTF TAPF TAPFlocal flaps 1stchoice 2ndchoice
(propeller method)
Chimeric flaps
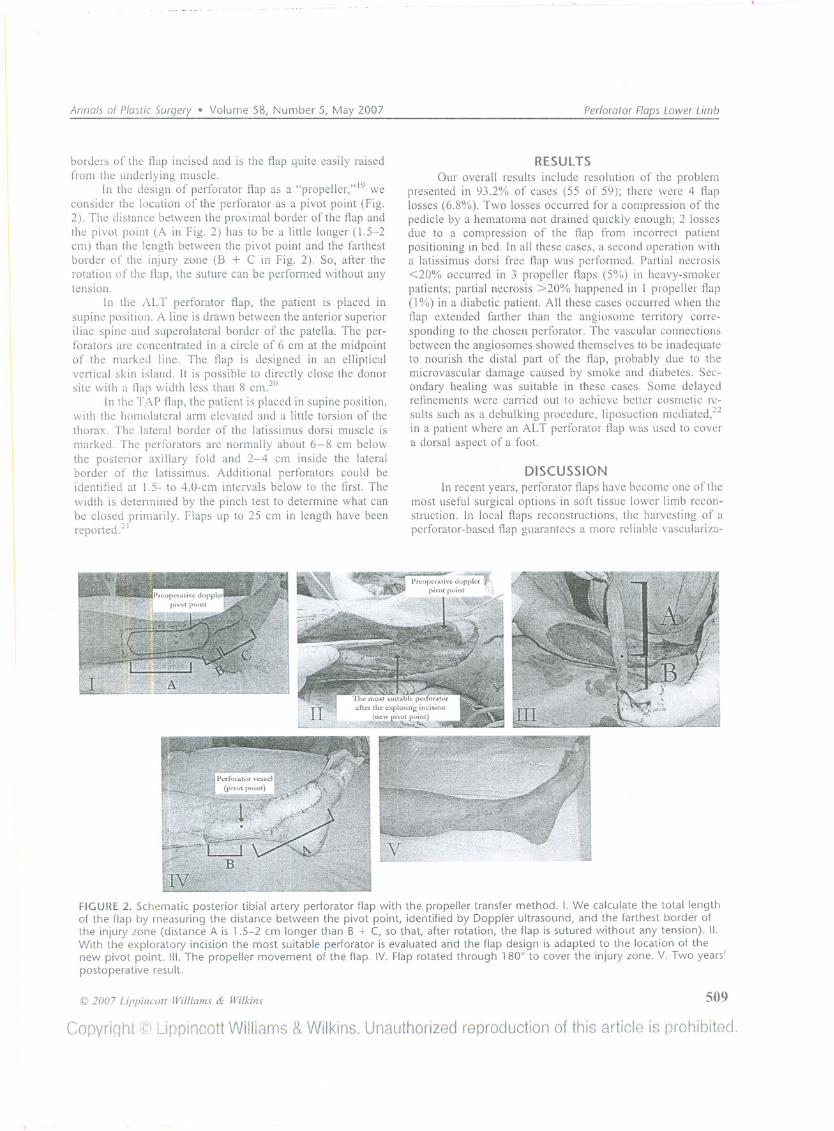
Our reconstructive strategy is as follows (Fig. 3): (l) Indefects of small and medium size, with suitable vascularcondition ofthe neighboring tissues, we select, as first choice,local perforator flaps with a "propeller" transfer method.lO, 19(2) In defects of small and medium size with pOOl'vascularcondition of the nearby tissues, AL TF is used as first choice,so the same anatomic body region is the source of a free flap(Fig. 4). When an AL TF is not indicated due to scars thatcould limit the size of the flap or if the pedic1e lengthrequired exceeds the AL TF one, we look for anotheranatomic region as a source offlaps and we prefer the TAPflap, beeause of its qualities (Fig. 5). (3) In defeets of largesize, with on1y a coverage required, the flrst selected flapis the T APF; in complex cases, we perform compound or
djq.
rA
FIGURE 4. A 38-year-old male patientwith a traumatic soft tissue loss (9 x 6cm) of the anterolateral aspect 01 theleft ankle, with osteosynthesis materialexposed, underwent surgery. After theremoval 01 the osteosynthesis materialsand a surgical debridement, an ALTflap was harvested and transferred tocaver the delect. A, The delect; preop-erative planning 01 the flap (B); 2years' postoperative result (C).
510
Copynql'1t uppincottWilliams& Wilkins.Unauthorizedreproductionof this artide is prohibited.
@ 2007 Lippillco/l Williams & Wilkins
/ \ / \ / \Good Uncertain Good Uncertain Onlv Complex
vascular vascular vascular vascular coveraqe reconstructionsanatomy anatomv anatomv anatomv
/ \
Annals of Plaslic Surgery . Volume 58, Number 5, May 2007 Perforator Flaps Lower Limb
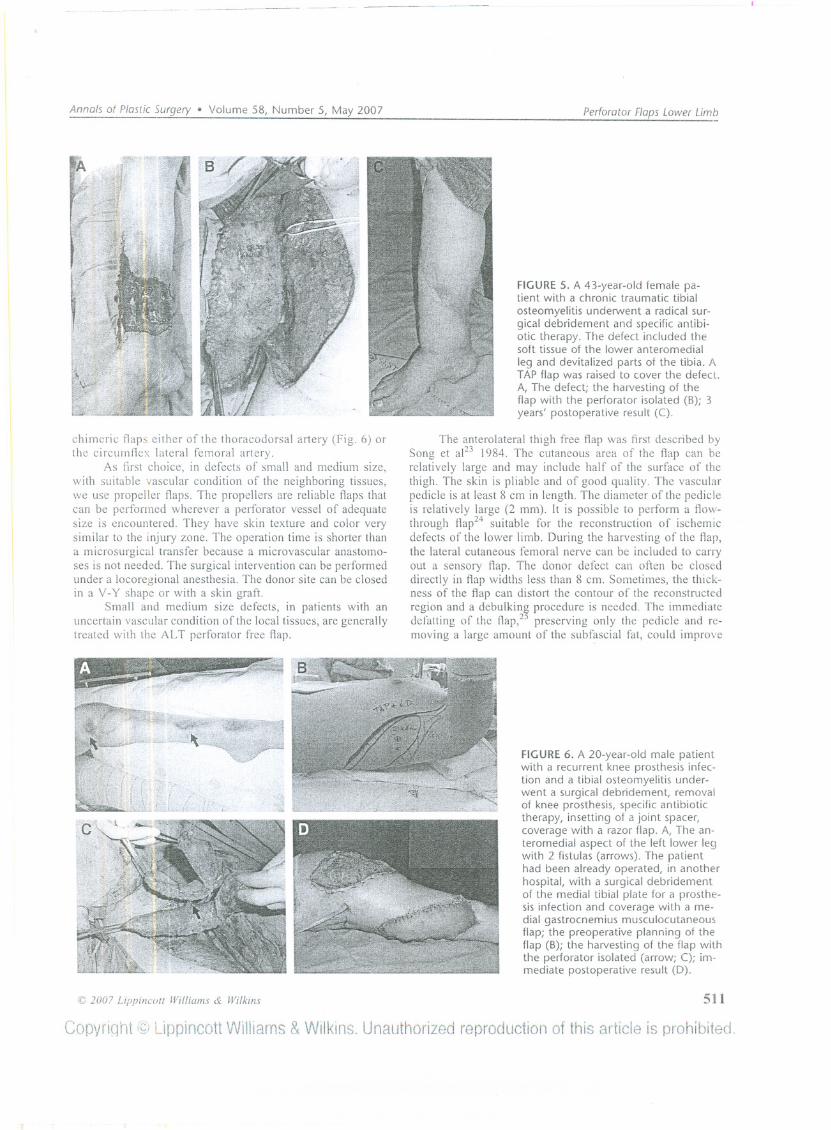
chimeric ftaps either of the thoracodorsal artery (Fig. 6) orthe circumftex lateral femora1 artery.
As first choice, in defects of smal1 and medium size,with suitable vascular condition of the neighboring tissues,we use propeller flaps. The propel1ers are reliable flaps thatcan be performed wherever a perforator vessel of adequatesize is encountered. They have skin texture and color verysimilar to the injury zone. The operation time is shorter thana microsurgical transfer because a microvascular anastomo-ses is not needed. The surgical intervention can be performedunder a locoregional anesthesia. The donor site can be c\osedin a V-y shape or with a skin graft.
Small and medium size defects, in patients with anuncertain vascular condition ofthe local tissues, are generallytreated with the ALT perforator free flap.
FIGURE5. A 43-year-oldfemale pa-tient with a chronic traumatic tibialosteomyelitis underwent a radical sur-gical debridement and specific antibi-otic therapy. The defect included thesoft tissue of the lower anteromedialleg and devitalized parts of the tibia. ATAPflap was raised to cover the defect.A, The defect; the harvesting of theflap with the perforator isolated (B); 3years' postoperative result (C).
The anterolateral thigh free flap was first described bySong et al23 1984. The cutaneous area of the flap can berelatively large and may include half of the surface of thethigh. The skin is pliable and of good quality. The vascularpedicle is at least 8 cm in length. The diameter of the pedicleis relatively large (2 mm). It is possible to perform a flow-through flap24 suitable for the reconstruction of ischemicdefects of the 10wer limbo Ouring the harvesting of the flap,the lateral cutaneous femoral nerve can be included to carryout a sensory flap. The donor defect can often be c\oseddirectly in flap widths less than 8 cm. Sometimes, the thick-ness of the flap can distort the contour of the reconstructedregion and a debulking procedure is needed. The immediatedefatting of the Hap,25 preserving only the pedic\e and re-moving a large amount of the subfascial fat, could improve
@ 200? Lippincutt Williams & Wilkins
Copyriqr'it
FIGURE6. A 20-year-oldmale patientwith a recurrent knee prosthesis infec-tion and a tibial osteomyelitis under-went a surgical debridement, removalof knee prosthesis, specific antibiotictherapy, insetting of a joint spacer,coverage with a razor flap. A, The an-teromedial aspect of the left lower legwith 2 fistulas (arrows). The patienthad been already operated, in anotherhospital, with a surgical debridementof the medial tibial plate for a prosthe-sis infection and coverage with a me-dial gastrocnemius musculocutaneousflap; the preoperative planning of theflap (B); the harvesting of the flap withthe perforator isolated (arrow; C); im-mediate postoperative result (D).
511
Uppincott Williams&Wllkins.Unauthorizedreproduction of this article is prohibited.

Masia el al Annals of PlasticSurgery . Volume 58, Number 5, May 2007
the final shapc of the flap but the risk of dal11agingthe vessels,in less skilled hands, is increased. So, we usually wait andperforl11a delayed defatting of the flap through a liposuctionproceclure,22 íf necessary.
The ALT perforator flap may be, aclditionally, raised asa compouncl flap (including for example the fascia lata) or asa chil11eric flap,13 inclucling rectus femoris muscle, vastuslateralis muscle, etc, for more complex reconstructions (com-plex clefects, tenclon defects, etc).
In patients with medium-size defects where it is notpossible to ¡¡mit the morbíclíty to a single regíon, due to aninsufficient available amount of the ALT perforator flap orthe requirement of a longer vascular pedicle, we perform aTAP free flap. We use the TAP free flap even in reconstruc-tions of large-size clefects.
The thoracodorsal artery perforator flap, initially de-scríbed by Angrigiani et al12 in 1995, can include a thin andpliable skín-soft-tissue padclle up to 14 by 25 cm. The vascularpeclícle length is about 18 cm, useful when the anastomosis hasto be performecl outsicle a large zone of injury. The TAP can beused as a flow-through flap, and it is possible to include sensorybranches of intercostal nerves. The donar site can be closeddirectly ar, rarely, with a split-thickness skin graft. Finally,a chil11ericflap with a combined latissimus dorsi flapl4 canbe raised.
The advantage of a chimeric free flap]] is that complex,extensíve, 3-climensional defects can be reconstructecl usingmultiple tissues that are independently moved and inset.The combination of more tissues expands the total surfaceof the flap and, furthermore, as these kinds of flaps haveseparate vascular pedicles but a common source vessel, onlya single recipient site has to be available.
[n our experience, perforator flaps have provided con-sistent ancl reliable solutions for soft tissue reconstruction ofthe lower limb. They are very versatile flaps, allowing us toselective]y choose and transfer the tissues of an angiosomethat are required for a specific reconstruction, and the mor-bidity of the donar site is often minima!.
We propose a simple reconstructive algorithm far lowerlimb soft tissue reconstruction with perforator flaps that coulclbe helpful in choosing the right flap for a specific defect,always focusing on getting the most "like-to-like" tissues;whenever possible, selecting the same anatomic region of thedefect as source of flaps; reducing the morbidity; improvingthe cosmetic results.
CONCLUSIONPerforator flaps are safe and reliable flaps and represent
an important step forward in reconstructive plastic surgery ofthe lower limbo Whenever possible, surgical intervention anddonor-site morbidity ought to be limited to a single bodyregíon, and the use of propeller perforator flaps can con-cretely widen the reconstructive options far inferior limbdefects. Furthermore, when a free tissue transfer is needecl, aperforator flap would be employed because of its undoubtedaclvantages: (1) important decrease in donor-site morbidity,preserving muscles and their functions and sparing the main
vascular trunks; (2) specificity in "1ike-to-like" soft tissuereplacement; (3) a better cosmetic and reconstructive result.
REFERENCES1. Jayes PH. Cross-Ieg flaps: a review of 60 cases. El' J Plast Surg.
1950;3:1-5.2. Geddes CR, Morris SF, Neligan pe. Perforator flaps: evolution, classi-
ficationand applications.A/1/1 Plast Silrg. 2003;50:90-99.3. Hallock GG. Lower extremity muscle perforalor tlaps for lower extrem-
ity reconstruction. Plasl Recol/Slr Surg. 2004; 114: 1123-1130.4. Taylor GI, Palmer JH. The vascular territaries (angiosomes) ofthe body:
experimentalstudy and clinical applications.El' J Plast Silrg. 1987;40:113-141.
5. Taylor Gl. The angiosomes of the body and their supply to perforatorflaps. Clil/ Plast Surg. 2003;30:331-342.
6. Acland RD, Schusterman M, Godina M, et al. The saphenous neurovas-cular free flap. Plast Reconstr Surg. 1981;67:763-774.
7. Koshima 1, Moriguchi T, Ohta S, et al. The vasculature and clinicalapplication of the posterior tibia! perfÓrator-based flap. Plast ReconslrSlIrg. 1992;90:643-649.
8. Leung-Kim H, Jie L, Pak-Cheong H. Free posterior tibial perforator flap:anatomy and a reporl of 6 cases. Microsurg. 1996;17:503-511.
9. Taylor Gl, Pan WR. Angiosomes of the leg: anatomic study and clinicalimplications. Plasl Reconstr SlIrg. 1998;102:599-616.
lO. HyakusokuH, YamamotoT, Fumiiri M. The propeller flap method. !IrJ Plast Surg. 1991;44:53-54.
11. Wei FC, Jain V, Celik N, d al. Have \Ve JOllnd an ideal sofi-tissue tlap?An cxperiencewith 672 anterolatcral thigh flaps. Plast Recollstr Surg.2002; 109:2219-2230.
12. Angrigiani C, Grilli D, Siebert J. Latissimus dorsi musculocutaneollstlap witholltmuscle. Plast ReconstrSlIrg. 1995;96:1608-1614.
13. Huang WC, Chen HC, Wei FC, et al. Chimeric tlap in clinical use. ClinPlast Surg. 2003;30:457-467.
14. Cavadas PC, Teran-Saavedra PP. Combined latissimus dorsi-thora-codorsal artery perJoratorfn:e flap: the "razor flap." J Reconslr Micro-sllrg.2002;18:29-31.
15. Blondeel PN, Beycns G, Vcrhaeghc R, et al. Doppler flowmctry in theplanning of perforator tlaps. El' J P1aslSlIrg. 1998;51:202-209.
16. Masiá J, Clavero JA, Larrañaga J, et al. Multidetector-row computedtomography in the planning of abdominal perlorator flaps. J PlastReconstrAeslhet SlIrg. 2006;56:594-599.
17. Voet DVAM, Petrovic M, Masia J, et al. Preoperative planning. In:Blondeel PN, Morris SF, Hallock GG, et al, eds. Perforator Flaps:Anatomy. Teclzniqlle and Clillical Applica/iolls. SI. Louis: Quality Med-ical Publishing; 2006.
18. Wei FC, Mardini S. Free-style free flaps. Plasl Reconstr SlIrg- 2004;114:910-916.
19. Moscatiello F, Masiá J, Pons G, et al. Our experience of the propellerdeseending genicular artery perforator tlap. Abstract Book, 9th Intema-tional Course on Perforator Flaps; Barcelona, October 5-8, 2005.
20. Mardini S, Un CH, Wei Fe. Lateral circumflex femaral artery-vastuslateralis pertorator flap. In: Blondeel PN, Morris SF, I-Iallock GG, d al.PerforalOr Flaps: Anatomy, TecJmiqlle am1 Clillical Applications. SI.Louis, MO: Quality Medical Publishing, Inc; 2006:618-633.
2 J. Van Landuyt K, Hamdi M. Thoracodorsal artery perforator flap. In:Blondeel PN, Morris SF, Hallock GG, et al. Perforator Flaps: Anatomy,Teclzniqlle ami Clinical Applicatiolls. SI. LOllis, MO: Quality MedicalPublishing, Inc; 2006:441-460.
22. Hallock GG. Conventional liposuction-assisted deblllking of muscleperlorator tlaps. Ann Plast Surg. 2004;53:39-43.
23. Song TG, Chen GZ, Song YL. The trec thigh tlap: a ncw frec flapconcept based on the septocutaneollsartery. El' J PlclStSlIrg. 1984;37:149-159.
24. Koshima 1, Kawada S, Etoh H, et al. Flow-through anterolateral thighftaps for one-stage reconstruction 01' sofl-tissue defects and revascular-ization of ischemic extremities. Plasl Reconstr SlIrg. 1995;95:252-260.
25. Kimura N, Satoh K, Hsaka Y. Microdissected thin perforator tlaps: 46cases. Plast Reconstr SlIrg. 2003;112:1875-1885.
512 (¡J2007 Lippincotl Wi/liams & Wilkins
Copyriqtlt @ Uppincott WiHiams& Wilkíns,Unauthorizedreproductionof this artícleís prohibited.



















![The keystone-design perforator-based flap for leg defects ... · reconstruction.[2] A modification is proposed, which combines the philosophies of perforator‑based flaps and the](https://img.dokumen.tips/doc/110x75/5f03de807e708231d40b2adb/the-keystone-design-perforator-based-flap-for-leg-defects-reconstruction2.jpg)









