Embed Size (px)
Citation preview

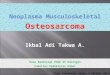
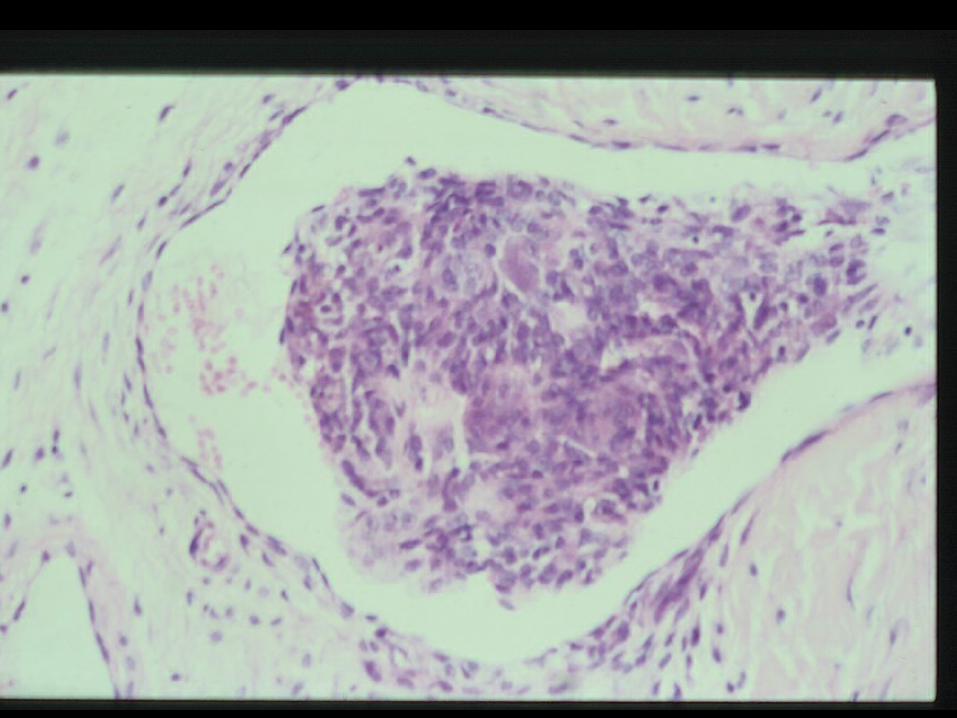
OsteosarcomaClinical and Imaging• 5% of primary malignant spinal
tumours
• 4th decade (older than long bone)
• Associated with Paget’s, DXRT
• Mixed lytic / sclerotic appearance
• Aggressive, soft tissue extension
• Osteoid mineralisation
T1W T2W
T1WCT
Differential diagnosis
• Ewings• Chondrosarcoma • Metastasis• Osteoblastoma• Lymphoma

SBTR 4346, AB22M
7/12 Hx LBP
2/12 Hx right leg / foot pain and weakness
more recently urinary problems

4346, Ant Bishop, 22M

Ewing’s sarcoma
• Bone or soft tissue
• Now accepted to be primitive neurectodermal tumour
• Includes Ewing, PNET, peripheral neuroepithelioma, Askin tumour
• t (11;22)(q24;q12) and other rearrangements


PAS




Chimaeric protein
Control
sequenceControl sequence
Overexpression of target gene
Fusion geneTranslocation

ES Cytogenetics
t(11,22)(q24;q12) (95%) EWS/FLI1
t(21,22)(q22;q12) (5%) EWS/ERG
t(7,22)(p22;q12) EWS/ETV1
t(17,22)(q21;q12) EWS/EIAF
t(2,22)(q33;q12) EWS/FEV
inv(22)(q12;q12) EWS/ZSG
t(16,21)(p11;q22) FUS/ERG

Ewing’s sarcoma
Clinical and Imaging Usually 10 – 30yrs >50% metastases at presentationMetastatic involvement more common than primaryPermeative pattern of bone destruction Large soft tissue mass and infiltrationNo matrix mineralisation but reactive sclerosisMR – inhomogeneous, haemorrhage & necrosis
T1W
T2WGRE
Differential diagnosis
• Osteosarcoma • Osteoblastoma• Lymphoma• Langerhans

30F, LBP

30F, LBP
T1W
T2W











Giant Cell TumourClinical and Imaging• >60% of primary benign sacral tumours
• 3rd – 5th decades, 2F:1M
• Locally aggressive, 12-50% recurrence rate
• Lytic, expansile, absent matrix,
• +/- cortical breakthrough
• CT / MR may show fluid-fluid levels
• MR – low signal on T2W due to collagen, high cellularity and haemosiderin from haemorrhage
• Can undergo sarcomatous degeneration
Differential diagnosis • Expansile metastasis
• Chordoma
• Myeloma
• Aneurysmal bone cyst
• Osteoblastoma
• Brown tumour of hyperparathyoidism

DH, SBTR 4513Mid thoracic pain



Myeloma
Clinical
Proliferation of malignant plasma cellsMost common primary bone malignancyMost common in 6th and 7th decadesPlasmacytoma usually precedes myeloma
Differential diagnosis
• Metastases • Lymphoma • Sarcoma • Chordoma • GCT

Patterns on T1W - Myeloma
Baur-Melnyk. Role of MRI in multiple myeloma. EJR 2005; 55:56
<20% plasma cells
20 – 50% plasma cells
>50%plasma cells
Normal Infiltration Replacement

MC, 1907806113
• 30F
• Left neck pain
• Prominent ECA / pulsatile mass
• ?carotid body tumour






Eosinophilic Granuloma • 5 – 10yrs
• 15% axial skeleton
• Can be asymptomatic
• Vertebral body
• Multifocal in 10%
Differential • Ewing’s
• Metastatic neuroblastoma
• ABC

60F, LBP
Haemangioma
Haemangioma



56F, right L5 sciatica

Pagets – later phase

Paget’s disease of bone• increased bone turnover osteoclastic and osteoblastic activity• age > 40 M>F• 3% of routine autopsies• aetiology unknown ? viral racial predilection• monostotic or polyostotic• raised alkaline phosphatase• complications fracture deformity and sarcoma



Lolge S. Isolated solitary vertebral body tuberculosis. Clin Rad 2003
22F, Indian
Differential diagnosis
Sarcoma Eosinophilic granulomaGCT

Summary: Imaging
• In children / adults, metastases most frequent bone tumour.• Patient age, location and relative frequency important• In sacrum , Paget’s, chordoma and GCT• Scintigraphy mainly for staging metastatic disease • CT - optimal imaging technique for osteoid osteoma• CT - bony detail , mineralisation, cortical shell & sequestra • CT - often complementary to MRI. • MRI - imaging method of choice.



SBTR 4319Wal Millerchondrosarcoma grade 3

GJ, SBTR 4530LBP,Osteoblastoma