Embed Size (px)
DESCRIPTION
Only You Can Prevent CVD. Matthew Johnson , MD. What can we do to prevent CVD?. What can WE do to save the most lives?. What risk factors are important in the development of heart disease?. Who is at risk and how can we calculate risk?. Background:. - PowerPoint PPT Presentation
Citation preview

Only You Can Prevent CVD
Matthew Johnson , MD

What can we do to prevent CVD?

What can WE do to save the most lives?
What risk factors are important in the development of heart disease?
Who is at risk and how can we calculate risk?

Background:
Clinical guidelines for primary prevention of CAD
recommend a risk management based on the
Framingham score.

Screening for early detection of high risk patients with asymptomatic atherosclerosis and monitoring their response to treatments in order to reduce sudden cardiovascular events remain as major challenges in preventive cardiology.

Background: Cont.
Traditional tools used to assign risk of future cardiovascular
events, at times fail to accurately identify individuals with
severe coronary artery disease.
Despite major advances in the treatment of coronary artery
disease (CAD), a large number of apparently healthy people die
suddenly of a heart attack without prior symptoms and do not
benefit from existing preventive therapies.
Background: Cont.
The Framingham score as applied in these guidelines is a tool to predict the absolute risk of coronary events in populations free of cardiovascular disease.
Reynolds risk score is also a tool to predict the risk of coronary events.
www.reynoldsriskscore.org


Framingham risk score (FRS)
Framingham Risk Score (FRS) is calculated based on NCEP ATP III ( age, gender, total cholesterol, HDL-C, Smoking status, Systolic blood Pressure and Anti-hypertensive medication)

Results: Cont.Receiver operator characteristic curves for 3 models created to assess the ability of Framingham risk score (FRS), coronary artery calcium (CAC) score and the combination in predicting mortality among 730 symptomatic subjects
Variable AUC±SE 95% CI P Comparison P
FRS£ 0.72±0.03 0.68 - 0.75 0.0001 -- CAC¥ 0.82±0.03 0.79 - 0.85 0.0001 0.01 CAC + FRS 0.92±0.02 0.89 – 0.93 0.0001 0.001 £FRS: Framingham Risk Score- FRS<10%, FRS 10-14%, FRS 15-19% and FRS≥20% ¥CAC: Coronary Artery Calcium- CAC 0, CAC 1-99, CAC 100-399 and CAC≥400

Role of Vascular and Neurovascular Function in Cardiovascular Disease
Vascular dysfunction is generally considered a key initial
event in the atherosclerotic process which is a local
manifestation of systemic disorder. Numerous studies have
shown that functional changes in arteries precede the
development of structural changes and also reverse more
quickly in response to therapies
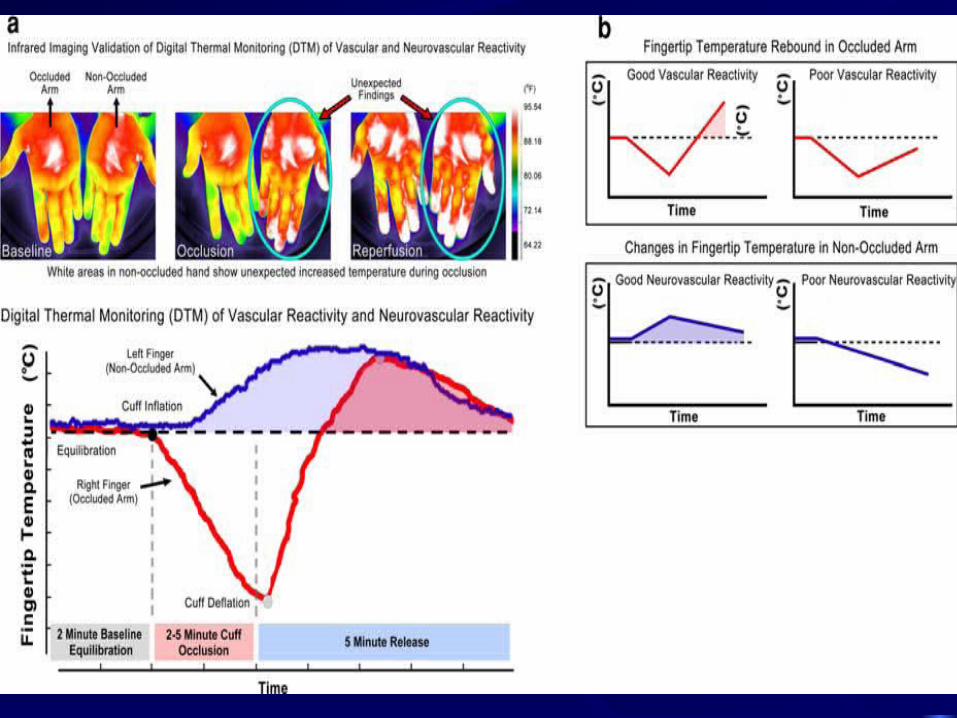

http://www.endothelix.com/vendysmovie.html


What is a calcium score?
A calcium score refers to a screening test that is used to calculate the amount of calcium in the heart. A calcium score looks specifically at calcium in the coronary arteries, where increased calcium leads to narrowing of the artery.

How is a CCS calculated?
The calcium score is calculated from Computed Tomography (CT) scan images. The two main types of CT scanners are "Electron Beam" (EBCT) and "Multi-Detector" (MDCT). Both types of scanners are generally effective in calculating a calcium score.

What is the purpose of a Calcium Score?
The purpose of a calcium score is to determine if a patient is at high risk for coronary artery disease, which may lead to a heart attack. In general, a high calcium score is associated with a higher risk of cardiovascular events, while a calcium score of zero is associated with a very low risk of coronary artery disease or heart attack.





Public Enemy #1
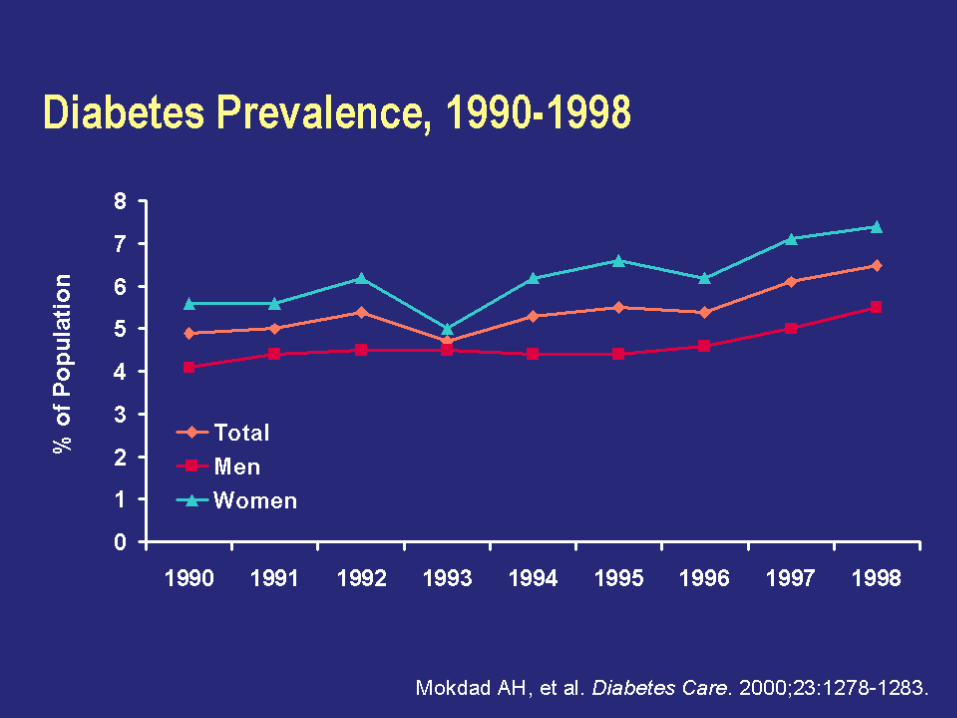
Diabetes Prevalence, 1990-1998


Risk of Cardiovascular Events in Diabetics Framingham Study
Age-adjusted
Biennial Rate Age-adjusted
Per 1000 Risk Ratio
Cardiovascular Event Men Women Men Women
Coronary Disease 39 21 1.5** 2.2***
Stroke 15 6 2.9*** 2.6***
Peripheral Artery Dis. 18 18 3.4*** 6.4***
Cardiac Failure 23 21 4.4*** 7.8***
All CVD Events 76 65 2.2*** 3.7***
Subjects 35-64 36-year Follow-up **P<.001,***P<.0001
_________________________________________________________________
_________________________________________________________________

Insulin Resistance

Natural History of Type 2 Diabetes

Relationship Between Obesity and
Insulin Resistance and Dyslipidemia

Insulin Resistance: Associated Conditions

Cardiovascular Disease and Diabetes

Probability of Death From CHD in Patients With Type 2 Diabetes With
or Without Previous MI

The Metabolic Syndrome
InsulinResistance
Hypertension
Type 2 Diabetes
DisorderedFibrinolysis
ComplexDyslipidemia
TG, LDL
HDL
EndothelialDysfunction
SystemicInflammation
Athero-sclerosis
VisceralObesity
Adapted from the ADA. Diabetes Care. 1998;21:310-314;Pradhan AD et al. JAMA. 2001;286:327-334.

Revised ATP III Metabolic Syndrome Oct 2005
*Diagnosis is established when 3 of these risk factors are present.†Abdominal obesity is more highly correlated with metabolic risk factors than is BMI. ‡Some men develop metabolic risk factors when circumference is only marginally increased.
<40 mg/dL<50 mg/dL or Rx for ↓ HDL
MenWomen
>102 cm (>40 in)>88 cm (>35 in)
MenWomen
100 mg/dL or Rx for ↑ glucoseFasting glucose130/85 mm Hg or on HTN
RxBlood pressure
HDL-C150 mg/dL or Rx for ↑ TGTG
Abdominal obesity† (Waist circumference‡)
Defining LevelRisk Factor

International Diabetes Federation Definition:
Abdominal obesity plus two other components: elevated BP, low HDL, elevated TG, or impaired fasting glucose





Prevalence of the Metabolic Syndrome Among US Adults NHANES 1988-1994Prevalence of the Metabolic Syndrome Among US Adults NHANES 1988-1994
Pre
vale
nc
e (
%)
P
reva
len
ce
(%
)
05
10
15
2025
3035
40
45
20-29 30-39 40-49 50-59 60-69 > 70
MenMenWomenWomen
Age (years)Age (years)Ford E et al. JAMA. 2002(287):356.Ford E et al. JAMA. 2002(287):356.
1999-2002 Prevalence by IDF vs. NCEP Definitions (Ford ES, Diabetes Care 2005; 28: 2745-9) (unadjusted, age 20+)NCEP : 33.7% in men and 35.4% in women IDF: 39.9% in men and 38.1% in women

http://www.nhlbi.nih.gov/guidelines/cholesterol/index.htm






























