Embed Size (px)
Citation preview


Objectives of this presentation…Objectives of this presentation…• Historical background of intraosseous (I.O.) infusion.
• The anatomical and physiological principle of I.O. infusion.
• Familiarization with the B.I.G™.
• Indications for I.O. infusion.
• Technique of insertion.
• Medications and fluids.
• Questions.
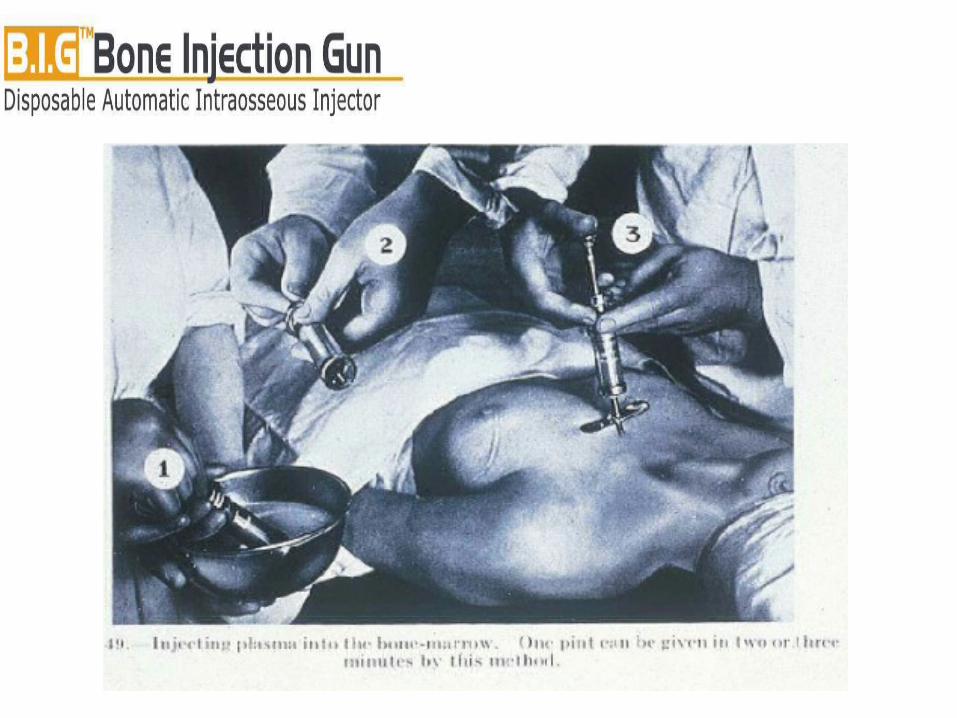
Historical background of I.O. Historical background of I.O. infusions…infusions…• First described by Drinker et al., in 1922.
• In 1941, the method was introduced for clinical use by Tocantis et al., mainly in children.
• Bailey et al. described cannulation of the sternum in 1946.
• Intraosseal regional anesthesia is described by Thorn-Alquist in 1971.
• 2000, recommended for use in the emergency setting by ILCOR.

The anatomical and physiological The anatomical and physiological principle of I.O. infusion…principle of I.O. infusion…
Utilizes the the emissary veins that lead from the intramedullary cavity to the general circulation.

Anatomy of long bones, Anatomy of long bones, another look…another look…
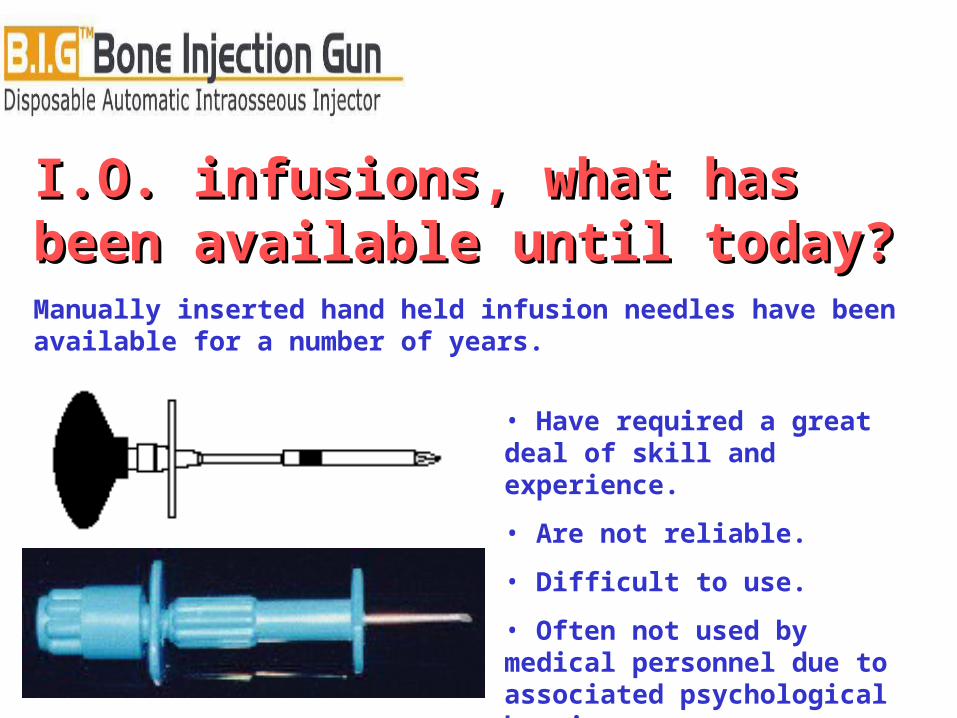
I.O. infusions, what has been I.O. infusions, what has been available until today?available until today?Manually inserted hand held infusion needles have been available for a number of years.
• Have required a great deal of skill and experience.
• Are not reliable.
• Difficult to use.
• Often not used by medical personnel due to associated psychological barriers.

Introducing the Introducing the B.I.GB.I.G™™……
Adult B.I.G - 15GCE & FDA Approved
Pediatric B.I.G - 18GCE Approved

Design of theDesign of the B.I.G™B.I.G™…… • Developed to be easily used by a single rescuer.
• Allows immediate vascular access.
• Permits the rapid infusion of medications and fluids.
• Minimizes exposure to the patient’s bodily fluids.
• Can be successfully used by physicians and paramedics.
Design of theDesign of the B.I.G™ B.I.G™……
Instrument in locked position (before triggering).
Design of theDesign of the B.I.G™ B.I.G™……
After triggering.

Indications for I.O. infusions…Indications for I.O. infusions…1. TRAUMA
2. NON-TRAUMA
• Fluid replacement in shock.
• Rapid vascular access during mass casualty incidents.
• All cardiac arrests.
• Acute respiratory syndromes (COPD, Asthma, APE).
• When ever rapid vascular access is required.
FROM THE ECC GUIDELINES 2000
Rescuers should increase attention to early vascular access, including immediate Intraosseous access for victims of cardiac arrest, and extend the use of Intraosseous techniques to victims >6 years
ECC Guidelines 2000: Pediatric Advanced Life Support

When You Might Need I.O.When You Might Need I.O.

How It WorksHow It Works
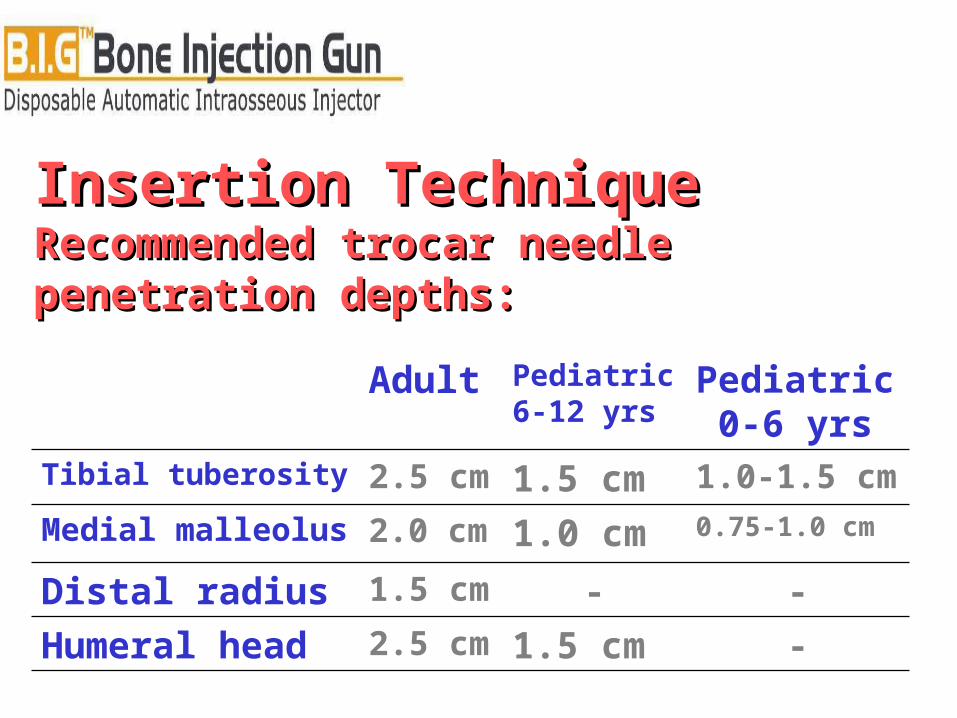
Insertion TechniqueInsertion TechniqueRecommended trocar needle penetration Recommended trocar needle penetration depths:depths:
Pediatric 0-6 yrs
Pediatric6-12 yrs
Adult
2.5 cm
1.5 cm
2.0 cm
2.5 cm
1.5 cm
-
1.0 cm
1.5 cm
-Humeral head
-Distal radius
0.75-1.0 cmMedial malleolus
1.0-1.5 cmTibial tuberosity
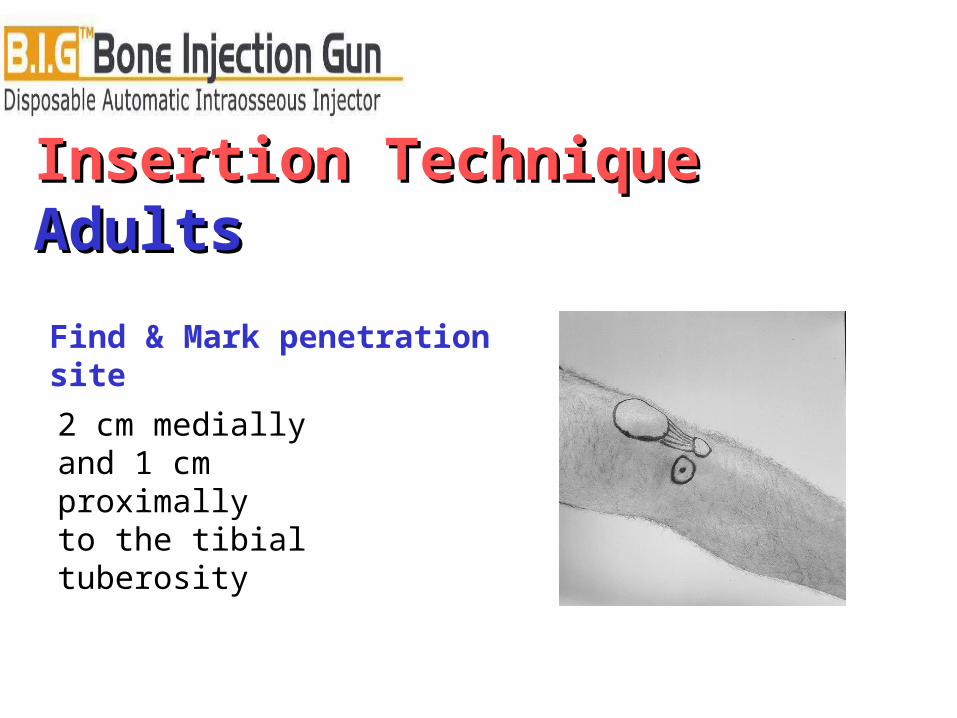
Insertion TechniqueInsertion TechniqueAdultsAdults
Find & Mark penetration site
2 cm medially and 1 cm proximally to the tibial tuberosity

Insertion TechniqueInsertion TechniquePediatricsPediatricsFind & Mark penetration site
Age 0-6:1 cm medially and 1 cm proximally To the tibial tuberosity
Age 6-12:1-2 cm medially and 1-2 cm proximally To the tibial tuberosity
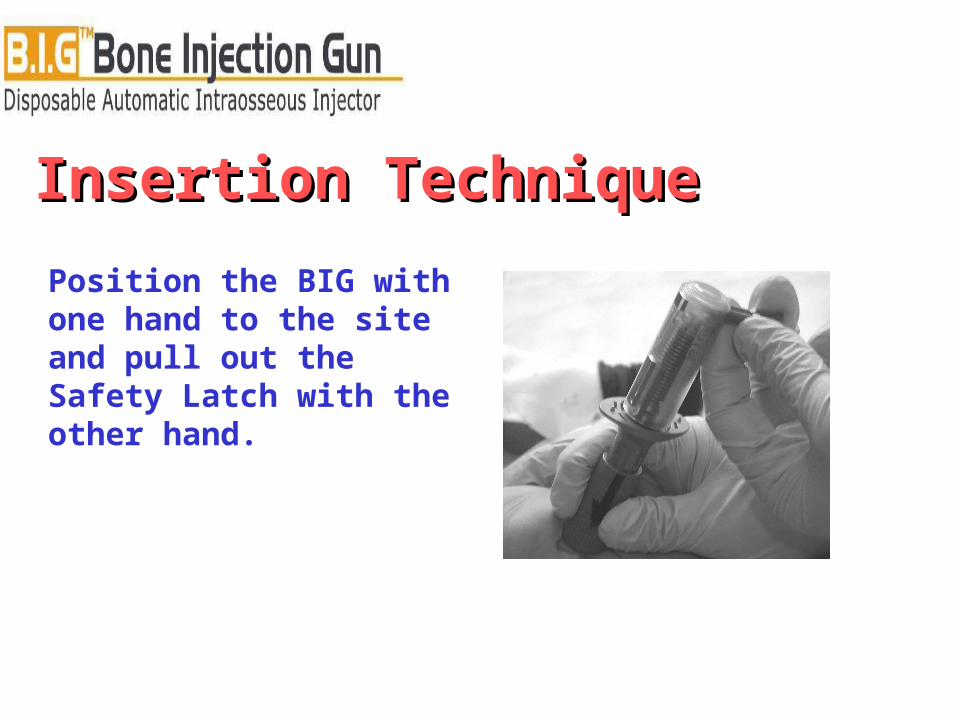
Insertion Technique Insertion Technique
Position the BIG with one hand to the site and pull out the Safety Latch with the other hand.
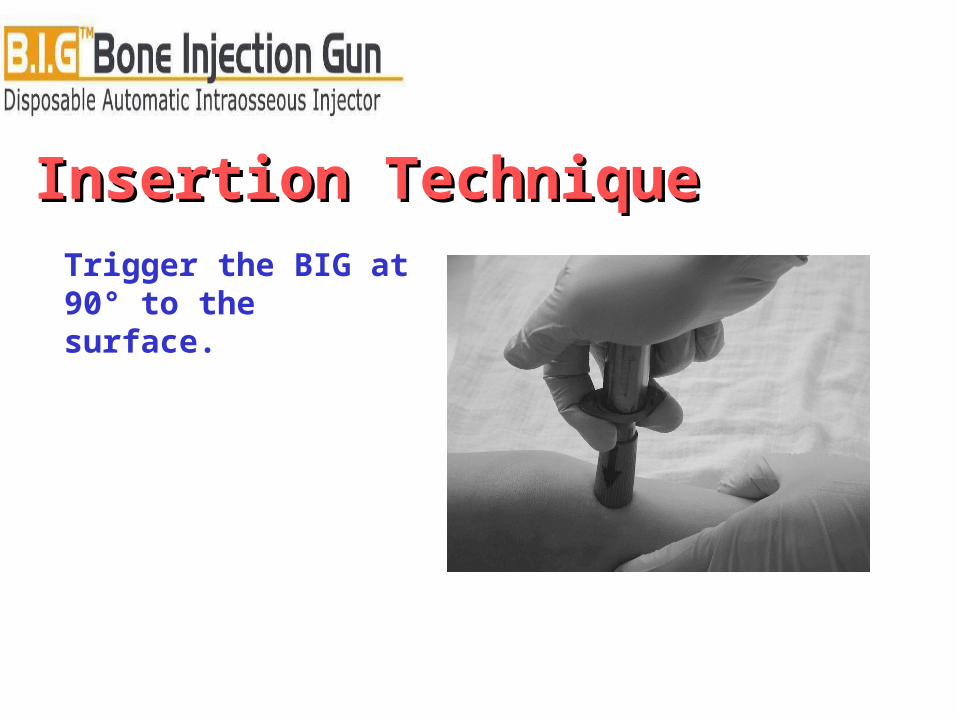
Insertion Technique Insertion Technique Trigger the BIG at 90° to the surface.

Insertion Technique Insertion Technique
Remove the BIG. Pull out the stylet trocar.

Insertion Technique Insertion Technique
Fix the cannula with the Safety Latch.
Connect IV Set with a stopcock Adults: flush with 1mg/ kg for I.O. local anesthetics.

Insertion TechniqueInsertion Technique
Now 2 – 5 cc of bone marrow can be aspirated into a heparin-coated syringe for laboratory sampling, or proceed to inject medications or infuse fluids.
To maintain optimal flow, high pressure, up to 300 mmHg to the infusion bag may be necessary.

Anatomical insertion point of the tibial tuberosity.
Insertion TechniqueInsertion TechniqueRecommended insertion sites:Recommended insertion sites:

Medications and fluids…Medications and fluids…
• All medications and fluids can be safely injected into the B.I.G™.
• I.O. medication and fluid boluses remain the same as those for I.V. injection.
• It is not recommended that large boluses of hypertonic solutions be infused through the I.O. cannula.
• In case of user inaccuracy, or technical malfunction, it is strongly recommended to always have a second B.I.G. On hand.

Questions?Questions?

Thank you.Thank you.