Embed Size (px)
Citation preview

(CANCER RESEARCH 37, 2395-2406, July 1977]
Summary
The nutritional consequences of major cancer chemotherapeutic and immunotherapeutic agents are reviewed. Inaddition, nutritional approaches to cancer treatment arediscussed. Effects on host nutrition are related to two pnimany drug functions, i.e., biochemical interaction with thetarget tissues and pharmacological action on the host.Treatments with these agents result in profound effects onthe gastrointestinal, central nervous, cardiopulmonary,renal, musculoskeletal, hematopoietic, and constitutionalsystems of cancer patients who have already been nutritionally compromised.
Prevention and treatment of the nutritional consequencesof chemotherapy and immunotherapy include specifictreatment against particular agents and nonspecific symptomatic or supportive therapy. A modern concept of panenteral nutrition combined with chemotherapy and immunotherapy is one example of a nonspecific approach with ahigh promise for general use.
More importantly, increasing success in the long-termcontrol of leukemia, Hodgkin's disease, and certain otherneoplasms has interrupted the vicious cycle promulgatedon the host nutrition by neoplasia and toxic agents. Newconcepts of chemotherapy, e.g. , short intensive treatmentinstead of prolonged treatment, and surgical adjuvant treatment instead of therapy of patients with advanced cancer,have minimized the nutritional consequences of chemotherapeutic and immunotherapeutic agents.
Introduction
Cachexia and malnutrition are among the major causesof morbidity in patients with advanced cancer. Anorexia,inanition, and progressive weight loss are commonplace.
Therapeutic approaches with chemotherapy, immunotherapy, radiotherapy, surgery, and anesthesia unavoidablyaffect host cells, often producing a variety of side effects,e.g. , nausea, vomiting, oral pain, diarrhea, fever and chills,and further decrease in appetite, physical activity, and bodyweight. These effects, together with biochemical and histological injuries to major organ systems, may leave the patient with a profound nutritional insufficiency. Treatment istherefore justified only when the patient can recover from
I Presented at the Conference on Nutrition and Cancer Therapy, No
vember 29 to December 1, 1976, Key Biscayne, Fla. Supported in part byUSPHS Grant 5 P01 CA15936-03 from the National Cancer Institute, Department of Health, Education and Welfare.
2 Presenter.
its consequences. Otherwise the vicious cycle of cachexiaproduced by tumor and toxic agents will not end, even if thetumor is apparently regressing. It is important to weigh therisks of treatment versus the possible benefits. Adversenutritional consequences produced by treatment are 1 component of the equation. Many of the nutritional consequences of chemotherapy are explained as the result ofinterference in necessary metabolic reactions (“biochemical nutrition―) and pharmacological effects on the hosttarget tissue(s) (“pharmacological nutrition―).For example,the megaloblastic anemia produced by cytosine arabinoside can be readily explained by its biochemical effectsselectively on DNA synthesis of erythrocyte precursors. Onthe other hand, the profound host effects of methotrexate inpatients with even mild renal impairment result from thedrug's excretion from the host nearly exclusively by therenal route.
In this paper the nutritional impact of commonly usedchemotherapeutic and immunothenapeutic agents is reviewed. In addition, the effects of several less commonlyused compounds of particular interest are discussed (Tables 1 and 2). Finally, the consequences of nutritional approaches to the treatment of human cancer are summanized. No attempts have been made to detail the nutritionalconsequences of combination chemotherapy on combinedmodalities of therapy, dietary manipulation, or hormonaltreatment.
ImpairedNutritiondue to DecreasedIntake p.o. and Toxicity in the Alimentary Canal
Nausea and vomitingfollowingchemotherapyonimmunotherapy with antineoplastic agents are mediated by thechemoreceptor trigger zone located in the area postrema ofthe 4th ventricle (10, 22). Nausea and vomiting are themost common immediate manifestations Of administrationof many chemotherapeutic or immunotherapeutic agents. Indeed, this complication occurs with almost every majorclass of compounds including a majority of alkylatingagents (e.g. , mechlorethamine and cyclophosphamide), thenitrosouneas, folate analogs, punine analogs, pynimidine analogs, derivatives of tniazene and hydrazene, anthracyclineantibiotics (daunorubicin and adniamycin), and other antibiotics (e.g. , mitomycin C, bleomycin, actinomycin D, andmithramycin), enzymes (e.g., aspanaginase), the simplemolecule hydroxyurea and certain immunotherapeuticcompounds [e. g., poly(IC),3 Corynebacterium parvum, and
3 The abbreviations used are: poly(lC), polyriboinosinic, polyribocytidylic
acid; CNS, central nervous system; BCG, Bacillus Calmette-Gudrin.
JULY 1977 2395
Nutritional Consequences of Cancer Chemotherapy andImmunotherapy1
Takao Ohnuma2 and James F. Holland
Department of Neoplastic Diseases, Mount Sinai School of Medicine, New York, New York 10029
on May 20, 2020. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Table 1
ChemotherapeuticagentsRecommended as 1st-line drugs for a variety of human neoplasms (137). Some other
drugs have also been used as 1st-line drugs alone or in combination. Others are listed fortheir nutritional implications.
Mechlorethamine (nitrogen mustard,HN2)
CyclophosphamideL-Phenylalaninemustard (melphalan,Alkeran)
Chlorambucil (Leukeran)Triethylene melamineDibromomannitol
Alkyl sulfonate Busulfan (Myleran)
Nitrosoureas BCNUaCCNUMethyI@CCNUbStreptozotocin
Punine analogs Azaserinec6-Mercaptopunine6-Thioguanine
Pyrimidine analogs 5-FluorouracilCytosinearabinoside5-azacytidine@
Derivatives of tn- Dimethyltriazenoimidazole carboxamazene and hydra- ide (DTIC, DIC)zine Procarbazine
Natural products Antibiotics MitomycinbBleomycin bDaunorubicinAdriamycinActinomycin DMithramycin'@
Vincaalkaloids VincnistineVinblastineb
Miscellaneous HydroxyureacMethylglyoxalbisguanylhydrazone1,1-Dichloro-2-(o-chlorophenyl)-2-(p-
chlorophenyl)ethanea The abbreviations used are: BCNU, 1 ,3-bis(2-chloroethyl)-1-nitrosourea; CCNU, 1-(2-
chloroethyl)-3-cyclohexyl-1-nitrosourea;methyl-CCNU, 1-(2-chloroethyl)-3-methylcyclohexyl-1 -nitrosourea.
‘IThe drug has been used as 1st-line drug alone or in combination.
C Listed for its nutritional implications.
levamisole]. Violent and prolonged nausea and vomiting cation 1 on more days before the emetogenic drug is helpmay occur after administration of procarbazine (16, 46, 109, ful.118, 120), streptozotocin (13, 112), cis-diamminedichloroplatinum (for review see Ref. 49), and 5-azacytidine (60, forreview see Ref. 127), and may be dose limiting. Presentlyavailable antiemetics are not wholly effective in the controlof drug-induced vomiting. Initiation of phenothiazine med i
T. Ohnuma and J. F. Holland
Alkylating agents
Antimetabolites Folate analogs MethotrexateDichloromethotrexate
Enzyme Asparaginaseb
Heavy metal Organic platinum cis-Diamminedichloroplatinum 1'
Hormone Corticosteroid
Nausea, vomiting, and accompanying anorexia not onlyresult in decreased oral intake, but also produce fluid andelectrolyte imbalance, general weakness, and weight loss.cis-Diamminedichloroplatinum-induced anorexia may becumulative, and some patients develop less and less appe
2396 CANCER RESEARCH VOL. 37
on May 20, 2020. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Table 2
Immunotherapeutic agents used inman
BCGMethanol extraction residueof BCGC, parvumLevamisoletRNAImmune RNAThymosin ne
Antiviral agent used in man with neoplastic disease
Poly(lC)
tite while they are responding to the treatment (52, 53).There are only a few cancer chemotherapeutic agents
which are not associated with nausea and vomiting. Theseare certain alkylating agents (e.g. , L-phenylalanine mustard,chlorambucil, busulfan, dibromomannitol), vincnistine, andsteroids.
Stomatitis, in the form of oral ulceration, cheilosis, glossitis and pharyngitis, and other mucosal toxicities of thealimentary canal are common with many of the chemotherapeutic agents. The alimentary canal is one of the mostvulnerable targets of chemotherapeutic agents. This isprobably due to a rapid turnover of the epithelial cells of themucosa. Rapid cell division at the depths of mucosal cryptsproduces cells that are pushed in migration up the cryptwall. The squamous mucosa of the oral, pharyngeal, andesophageal surfaces also displays more rapid turnover thanskin. Tumors of the alimentary canal usually do not grow asrapidly as do the adjacent normal mucosa (see Ref. 78).
Certain phases of the cell cycle are more sensitive tocytotoxic effects of cancer chemotherapeutic compounds,and even “cyclenonspecific―drugs have greater effects oncells which periodically expose to injury their most vulnerable cell phase. Dose-limiting oral mucosal toxicities occurafter actinomycin D (61, 116, 123), methotrexate (see below), and methylglyoxal bisguanylhydrazone (105). Oralmucosal toxicity is unpredictable in patients receiving highdose methotrexate and leucovonin rescue (33). Severeesophagitis may occur after methylglyoxal bisguanylhydrazone. Severe oral toxicity has also been observed afterazasenine, daunorubicin, adniamycin, and 5-fluorouracil.During infusion treatment with 5-fluorouracil, hematological toxicity is less and oral toxicity may become the doselimiting complication (114). Mucosal ulcerations are rarewith alkylating agents but may be seen with phenylalaninemustard and cyclophosphamide (91).
These toxicities are accompanied by inability to continueadequate intake p.o. and result in dehydration and furtherdeterioration of the nutritional status of the patient.
Constipationand AdynamicIleus. Theseare the majortoxicities of vincnistine. In 1 broad study troublesome constipation was reported in one-third of the patients with agreaten frequency, severity, and earlier onset at a higherdose (57).
MalabsorptionSyndrome. It is likelythat the profoundeffects of the chemotherapeutic agents on the intestinalmucosa and/on major secreting organs result in the development of malabsorption syndrome. These effects have
Cancer Chemotherapy and Immunotherapy
not, however, been systematically studied during chemotherapy. Positive Shilling tests with and without intrinsicfactor compatible with malabsorption syndrome were notedduring the nadir of serum albumin and body weight in apatient with acute myelocytic leukemia who was treatedwith asparaginase (95).
Diarrhea. This is part of the general mucosaltoxicityproduced by a number of chemotherapeutic agents. Diarrhea is particularly severe after actinomycin D, 5-fluorouracii, and methylglyoxal bisguanylhydnazone. Abdominal painmay accompany it. Diarrhea is also commonly seen aftermethotrexate, hydroxyunea, nitrosouneas, and 5-azacytidineand less frequently after 6-mencaptopunine, cyclophosphamide, procanbazine, and levamisole. In severe cases, proctitis, mucosal ulceration, bleeding, and perforation accompany diarrhea. Diarrhea alternates with constipation aftervincnistine treatment. Prolonged uncontrolled diarrhea resuits in dehydration, electrolyte imbalance, inanition, andaccelerated malnutrition. Hospitalization may be indicated,and adequate supportive cane is essential.
Additional effects of chemothenapeutic compounds onthe alimentary canal include jaw pain seen after vincnistine(57) and peptic ulcer in patients receiving corticosteroidhormones (Table 3).
Nutritional Consequences due to Dysfunction of SpecificMajor Organ Systems Produced by Chemotherapeuticand ImmunotherapeuticAgents
The HematopoieticSystem.This is anotherof the mostvulnerable targets of cancer chemothenapeutic agents. Hematological toxicities, especially leukopenia and thrombocytopenia, are dose limiting in a majority of cancer chemotherapeutic compounds. This is true for all agents exceptadrenocortical steroids and most imm unothenapeuticagents. Certain drugs active against hematological neoplasms exploit this principle. Although vincnistine, bleomycm, and asparaginase are relatively free from hematologicaltoxicity, they induce hematopoietic depression in a few
Table 3Nutritional consequences of long-term administration of adrenal
steroidModified from Ref. 67.
MusculoskeletalMuscleatrophy and myopathyOsteoporosis and vertebral
compression fractures
CirculatoryHypertension
Cushingoid appearance
Endocrine abnormalitiesPolyphagiaHyperglycemiaand glycosuniaObesity
Fluid and electrolyte disturbancesEdemaHypokalemic alkalosis
GastrointestinalPeptic ulcerationAcute pancreatitis
ImmunologicalInfectious complicationsBacterial, fungal, and tu
berculous infection
PsychologicalEuphoriaInsomniaPsychosis
DermalAtrophy(striae)AcneHirsutism
JULY 1977 2397
on May 20, 2020. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

T. Ohnuma and J. F. Holland
patients (57, 93, 97). Profound leukopenia is often accompanied by infection. Fever, chills, anorexia, and increasedenergy consumption accelerate the deterioration of the nutnitional status of the patient.
Anemia, a nutritionally important consequence, is frequently seen after administration of chemothenapeuticagents. Megaloblastic anemia is a predictable toxic effect ofchemothenapeutic agents that interfere with DNA synthesis.This complication has been reported with folate analogs(128), 6-mercaptopunine, 5-fluonounacil (12), cytosine anabinoside (122), cyclophosphamide (6), and hydnoxyunea (18).
Anemia induced by other agents has been less clearlydefined. Anthracycline antibiotics produce anemia (7) andprobably normochromic and normocytic anemia (126). Actinomycin D, another agent that binds with DNA, also produces anemia as part of general marrow depression (seeRef. 79). The same appears to be true for high dose cisdiamminedichloroplatinum administration (60 mg/sq mtwice weekly) (D. J. Higby, personal communication). Someinsignificant anemia was also seen after nitnosouneas (87)and dimethyltniazenoimidazole carboxamide (82). The genenal mechanism of drug-induced megaloblastic anemia ispnesumed to be the same as the one that results in megaloblástosis in vitamin B,2 and folate deficiencies, i.e. , DNAsynthesis is retarded in growing cells, whereas the synthesis of cytoplasmic constituents is affected to a lessendegreeor not at all (136). However, the “biochemicalanemia―produced by drugs may be different from the anemia thatresults from pure nutritional deficiency. The clinical charactenistics of anemia produced by biochemical interference atdifferent stages of maturity from stem cell to enythrocytehave not been well defined. This is in part related to theclinical material; i.e. , most patients with advanced cancerand leukemia already have preexisiting anemias of variouskinds (see Ref. 72), and many have received frequent tnansfusions of blood components.
The dose-limiting toxicity of mithnamycin is a hemonrhagic diathesis produced by alterations of the vascularbed, platelets, coagulation factors, and fibninolytic activity(88).
CNS. Thisis influencedbya varietyof chemothenapeuticagents (133). Especially noteworthy are intnathecal methotnexate, which can cause meningeal irritation, panapanesis,and encephalopathy (68, 85, 115); procanbazine, which caninduce somnolence, confusion, cerebral ataxia, psychosis,and coma (16, 109, 118, 120); vincnistine, which at higherdoses can produce weakness, insomnia, confusion, psychosis, disorientation, and hallucination (57, 110); asparaginase, which can produce unpredictable lethargy, depression, disorientation, confusion, and hallucination (20, 50,93-95, 135); 1,1-dichloro-2-(o-chlorophenyl)-2-(p-chlorophenyl)ethane, which can produce somnolence and lethargy (62, 81); cycloleucine, which can produce dizziness,lethargy, hallucination, ataxia, and convulsion (see below);and corticosteroids, which can produce psychosis (Table3). Administration of high doses of cis-diamminedichlonoplatinum (60 mg/sq m twice weekly) can result in confusion,coma, increase in cenebrospinal fluid pressure, and death(D. J. Higby, personal communication). CNS dysfunctionsoften result in impaired oral intake. Other neurological
complications include lassitude, apathy, and confusion following azasenine (37), cenebellan dysfunction from 5-fluonouracil (58, 86, 104), and headache after iv. levamisole andC. parvum (see Ref. 92). Levamisole also produces insomnia, nervousness, irritability, euphonic sensory stimulation,and mone severe psychiatric reactions (92). These complications may also have important nutritional consequences.
Narcotics given to patients with cancer most frequentlyaffect the CNS and compromise nutrition. Somnolencefrom drug effects leads to missed nourishment. Constipation from intestinal side effects of narcotics may also dim inish appetite.
The AlimentarySystem.The liver,whichplaysa criticalrole in overall nutrition, is often influenced by chemothenapeutic on immunotherapeutic agents, leading to seriousnutritional problems. Anorexia is particularly common afterhepatic injury. Diffuse hepatocellulan damage leads to hypoalbuminemia, a classic form of malnutrition. Liven damage is commonly seen after administration of aspanaginase(see below). Glutamine antagonists such as azasenine andduazomycin also cause hepatic impairment (see below).Jaundice occurred in about one-third of the patients whotook 6-mencaptopunine in reported series (34, 37). Histologically, bile stasis and hepatic necrosis have been reported.Hepatic dysfunction is also common after methotrexate (seebelow), nitnosouneacompounds(13, 112), mithnamycin (14),and 5-azacytidine (4, 127). Several cases of hepatic fibrosisand cirrhosis have been reported in leukemic children andin patients with psoniasis after long-term administration ofmethotrexate (107). In contrast, intensive courses given towomen with trophoblastic neoplasia and in whom remissionlasted more than 10 years were not followed by late complications (67). Thus, the exact role of the compounds in thedevelopment of this condition has not been completelydefined. Dose, schedule, and chronicity may all be critical.Abnormalities in hepatic function tests occur in a smallnumber of patients treated with cytosine arabinoside; how
even, evidence of definite hepatic toxicity related to thiscompound is not well established (Ref. 35; for review seeRef. 71). Cyclophosphamide, chlonambucil, and dimethyltniazenoimidazole canboxamide rarely cause hepatic dysfunction.
BCG-induced hepatic dysfunction ranges from mild elevation of alkaline phosphatase and aspartate aminotransferase to clinical jaundice and hepatomegaly (3). Granulomatous hepatitis was documented by liver biopsy in all 3jaundiced patients treated by intratumoral injection of BCGin Sparks' series (117). BCG administered via the aerosolroute appears to avoid hepatic toxicity (45).
Pancreatic dysfunction is produced by aspanaginase (seebelow). Streptozotocin affects islet cells, resulting in hyperglycemia and abnormal glucose tolerance tests. Insulin wasrequired in none (108). Severe hypoglycemia and comawere produced by methylglyoxal bisguanylhydnazone (105).Exocnine pancreatic function has not been systematicallystudied during cancer chemotherapy.
TheCardiovascularSystem.Cardiacdamageisa seriouscomplication of anthracycline antibiotics which includeboth daunonubicin and Adniamycin (see Refs. 7 and 32).Clinically, cardiac toxicity manifests as a fnank picture of
2398 CANCERRESEARCHVOL. 37
on May 20, 2020. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Cancer Chemotherapy and Immunotherapy
congestive heart failure with water retention and electrolyteimbalance. No specific antidote on preventive measures areavailable at present except limitation of the cumulativedose.
Certain chemothenapeutic agents are local tissue irritantsand produce tissue necrosis when extravasated (e.g. , ymcaalkaloids, most alkylating agents, actinomycin D, and anthracycline compounds). Other compounds are thnombogenic at the local venipunctune site (e.g., bleomycmn) (seeRef. 8). Repeated venipunctune results in inability to findsuitable peripheral veins for panenteral fluid, electrolyte,and nutritional support, thus exacerbating problems of nutnition in the advanced stages of disease in patients whohave had extensive chemotherapy.,
The UrinarySystem.Renalcomplicationsleadto varyingdegrees of the unemic syndrome, with its attendant nutnitional disorder. They are particularly apparent after administration of cis-diamminedichlonoplatinum , methotnexate(see below), and stneptozotocin . cis-Diamminedichlonoplatinum (see Ref. 49) produced dose-limiting renal complications. cis-Diamminedichlonoplatinum-induced nephnotoxicity manifests clinically as a rise in blood urea nitrogen andcreatinine and as decreased cneatinine clearance. Histologically, cis-diamminedichlonoplatinum appears to causerenal tubular necrosis. Renal toxicity is similar to that seenwith other heavy metal poisoning and appears to be doserelated, cumulative, and only partly reversible. Renal toxicity of stneptozotocin manifests as pnoteinunia occurring 2 to3 weeks into the course of therapy. Decrease in creatinineclearance and increase in cneatinine on blood urea nitrogenwere observed (13, 112). Renal tubular acidosis and Fanconi's syndrome (aminoacidunia, renal glycosunia, andrenal hyperphosphatunia) have also developd in 15 to 20%of patients (13). Fatal renal toxicity was recorded in 5 of 46patients with islet cell carcinoma. Aminoacidunia also occurs after cycloleucine (see below) (5).
A slight rise in blood urea nitrogen commonly observedafter aspanaginase treatment represents pnenenalazotemia,but in a few cases frank renal failure with marked oliguniahas been described. This usually accompanies other severetoxic manifestations (50). Renal complications also occurafter other nitnosoureas (30), mithnamycin (14), high-dosecyclophosphamide (more than 50 mg/kg body weight) (28),and after immunotherapy with C. parvum (92).
The MusculoskeletalSystem. Musculoskeletalconsequences of chemothenapeutic agents are exemplified bymuscle atrophy, osteoporosis, and pathological fracturesproduced by corticostenoids (Table 3). Vincnistine can alsocause muscle atrophy as a consequence of its neurotoxicity. Methotrexate given over long periods of time can lead toosteoporosis and pathological fractures.
Nutritional Consequences due to Systemic Effects ofChemotherapyand Immunotherapy
Fever and Chills. These are common and immediate sideeffects of treatment with bleomycin (see Ref. 8), asparaginase (19, 50, 93, 94), BCG (117), i.v. poly(IC)(29), and i.v. C.parvum (92).
BCG induces fever which begins 4 to 8 hr after injection
and persists for as long as 24 hr. Prunitus or a rash at the siteof injection develops in most patients (3, 117). The methanol extraction residue of BCG (131, 132) produces fever,malaise, and severe local pain at the site of intradermalimmunizations that ulcerate (see Ref. 132). poly(IC) (38, 74)is a double-stranded, helical synthetic RNA with a molecularweight of the order of 1,000,000. There is evidence that thesize distribution may be biologically important in terms ofboth toxicity and activity (74). poly(lC) produces fever whichappears by 6 to 8 hr and peaks at 24 to 36 hr. Indeed, feverappears to be a prerequisite for the production of interferon(29, 38). C. parvum has been reported to exercise its immunostimulatony effects through the neticuloendothelial system and B-cells, thus differing from BCG (48, 59, 99, 113). Itis of note that these chemotherapeutic and immunotherapeutic agents are all macromolecular, and, in certain instances, with the exception of poly(IC), contamination withextraneous pyrogens is possible. Fever has also been associated with the administration of cyclophosphamide, 6-mercaptopunine, and cytosine anabinoside. A “flu-like―syndrome has been reported after dimethyltriazenoimidazolecarboxamide (66, 79) and BCG (117) with nausea, myalgia,and, occasionally, arthralgia lasting 8 to 9 weeks.
Electrolyte Imbalance. This condition, induced by cyclophosphamide, includes hyponatremia, which has been reganded as due to inappropriate antidiuretic hormone production . Mithramycin , diazo-oxo-nonleucine (89), methotrexate (90), and actinomycin D (21) are known to producehypocalcemia. Mithramycin is used to treat hypercalcemia(102). Renal impairment produced by other chemothenapeutic agents can also be associated with varying degreesof electrolyteimbalance.
Weight Loss. This is a compositephenomenonin patients who have decreased oral intake, poor intestinal absonption, diarrhea, fever, CNS dysfunction, myopathy, and othercauses of negative nitrogen balance. Fluid overload in patients with hypoalbuminemia and hyponatnemia oftenmasks important weight loss related to the treatment. Distinct weight loss after treatment with asparaginase mayreflect decreased protein biosynthesis (see below).
The malnutrition effect of the antivitamins is implicit intheir mechanism of action and is very different from themalnutrition caused by corticosteroids onymca alkaloids.
A syndromeassociatedwithlate toxicityof busulfanhasbeen described. It consists of hypenpigmentation, asthenia,hypotension, nausea and vomiting, amenorrhea, andweight loss, sometimes associated with pulmonary fibrosis(72, 91, 98). Although the clinical picture suggests adrenalinsufficiency, this has not been documented. The pathogenesis of the syndrome is not well understood, but it maybe due to the prosthetic group of the bus@uIfanmoleculerather than to its aikylating properties (67). Pulmonary fibrosis produced by busulfan may be nodular on diffuse histologically (69) and can lead to fatal outcome (98).
One of the most serious systemic nutritional complications of chemotherapy and immunotherapy is graft-versushost disease in patientswith acute leukemiatreatedwithbone marrow transplantation. In a recent review by Thomaset a!. (124), cyclophosphamide treatment plus total-bodyradiation plus syngeneic transplantation using monozygotictwin marrow, and subsequent immunotherapy with normal
JULY 1977 2399
on May 20, 2020. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

T. Ohnuma and J. F. Holland
twin buffy-coat lymphocytes and s.c. injections of irradiatedautologous leukemic cells produced remissions of from 3 tomore than 49 months in 10 of 13 leukemic patients. Intensive combination chemotherapy is being added to the regimen to reduce the total-body burden of leukemic cells before the bone marrow tranplantation. In the overall marrowgraft experience, despite use of sibling donors matched atthe major histocompatibility leukocyte antigen and despitepostgraft immunosuppression , graft-versus-host diseasehas occurred in approximately 70% of successfully graftedpatients. Evidently, incompatibility for histocompatibility regions other than the major complex is an important determinant of graft-versus-host disease . Clinically, the principaltarget organs of graft-versus-host disease are the skin, gastrointestinal tract, and liven. The initial organ involved in
almost all cases is the skin, and the disease manifests as amaculopapulan rash; in severe cases it manifests as generalized erythnodermia with bullae and desquamation. Hepatic and intestinal involvement usually appear several daysafter the rash. Intestinal involvement is usually manifestedas diarrhea but may progress to abdominal pain and ileus.Liver disease is characterized by rises in bilirubin (mainlyconjugated), aspartate aminotransferase, and alkalinephosphatase. Fever, wasting, and debility status are alsoregularly seen. Chronic graft-versus-host disease is chanactenized by a more indolent clinical course involving thesame tissues. A fatal outcome may ensue with profoundnutritional impairment.
AdrenalCorticosteroid-inducedMalnutrition.The widespread metabolic consequences of corticostenoids are often seen in cancer patients given large doses for prolongedperiods. These consequences are summarized in Table 3.
The nutritional impact of newer immunothenapeuticagents such as thymosine, a calf thymus fraction (25, 111),transfer factor (80), and immune RNA (103) has yet to bedetermined.
Nutritional Consequences of a Specific Nutritional Approach to Chemotherapy
Although few qualitative differences have been observedin the essential nutrient requirements of tumor and normalcells, there are some quantitative differences that are probably dependent on growth rate, and this observation has ledto the design of new therapies using inhibitors of glucose,lipids, amino acids, and vitamins.
CarbohydrateAntagonist.2-Deoxy-D-glucose,a glucoseantagonist, competes with glucose for phosphorylation byhexokinase and thus diminishes the utilization of glucoseby tissues. Inhibition of glycolysis by treatment with 2-deoxyglucose produced inhibition of the growth of mouse andrat tumors. This is in keeping with the high glucose consumption of rapidly growing tumor tissue, independently ofwhether the glucose is subsequently metabolized by nespiration or glycolysis to lactate. 2-Deoxyglucose was given byinfusion to 8 patients with various neoplastic diseases (75).The patients developed diaphonesis, drowsiness, headache,generalized flush, and tachycandia, but tumor growth wasnot affected. The major limitation of this approach is theexquisite sensitivity of the CNS to glucose deprivation.
Lipid Antagonists.Tniparanolis a hypocholestenolemicagent that inhibits the conversion of desmostenol to cholestenol. The drug likewise exerts modifying effects on theformation of adrenocortical steroid hormones in man. In 3patients with metastatic prostate carcinoma, treatment withtnipananol produced disappearance of pain, X-ray evidenceof healing of bony metastases, and a decrease in acidphosphatase in each case for a year on more (27). There wasno clinical evidence that tnipananol exerted an estrogeniceffect. Eight patients with metastatic breast carcinoma werealso treated with tnipananol (70). All had prior surgical castration on were at least 10 years postmenopausal. Temponary subjective and objective antitumon response was observed in only 1 patient. Two of 4 patients, including the 1who responded, had a decrease in urinary estrogen excretion, and it was postulated that an inhibition of adrenalestrogen production might have caused the antitumon effects. Alternatively, hypocholestenolemia per se or the accumulation of intermediary steroids or steroid precursorsmight be causally related to the antitumor effect. Complications of this compound include cataract, alopecia, and denmatosis.
Boxidine, 1- [2-[[4' -tnifluonomethyl)-4- diphenyloxy]ethylpyrrolidine, is a nonsteroidal hypocholesterolemic agent.The compound blocks the conversion of 7-dehydroxycholestenol to cholesterol, thus producing hypocholestenolemiawith an accumulation of 7-dehydroxycholestenol in bloodand tissues. Of 13 patients with advanced cancer of varioussites, objective regression of pulmonary metastatic lesionswas observed in 1 patient with nonfunctional adrenal cancinoma (43). Side effects include anorexia, nausea, and vomiting. Decrease in serum cholesterol and appearance of 7-dehydnoxycholestenol were also shown.
Amino Acid Antagonists.Cycloleucine,1-amino-cyclopentane carboxylic acid, is a synthetic amino acid withantitumon effects in experimental neoplasms. Cycloleucineantagonizes the incorporation of valine into protein, probably by preventing the attachment of valine to tRNA (17). Incancer patients treatment with cycloleucine results in areversible, marked amino acidunia primarily involving cystine, ornithine, lysine, and arginine (15). Cycloleucine hasbeen reported to be effective against Ieiomyosancoma (1, 2).It also produced a partial response in a small number ofpatientswith head and neck cancer, colorectalcancer,ovarian carcinoma (125), melanoma (1, 125), and chondrosarcoma (65). Beneficial effects have also been seen in asmall number of patients with multiple myeloma (84). Toxiceffects of cycloleucine in man include nausea, vomiting,anorexia, diarrhea, weight loss, thnombocytopenia, a fall inconcentration of all the serum proteins, and neurologicaltoxicities (1, 5).
Selenocystmnehas been reported to be an effective agentin the treatment of animal tumors. Inorganic selenium perse could not reproduce the antitumon effect. The compoundwas thought to act by competing with L-cysteine for incorporation into protein. Two patients with acute leukemia and2 with chronic myelocytic leukemia were treated with selenocystine daily for 10 to 57 days (130). In each of thesepatients there was a marked reduction in the circulatingleukocytes, and splenomegaly became less pronounced.
2400 CANCERRESEARCHVOL. 37
on May 20, 2020. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Cancer Chemotherapy and Immunotherapy
However, treatment with this drug produced severe nauseaand vomiting, and it was not possible to continue its administration to determine whether remission could be induced.
Ethionine, a structural analog of methionine, has beenknown to impair the growth of experimental tumors. In 6patients with advanced cancer of various sites, treatmentfor short periods of time with ethionine and a diet relativelylow in methionine led to various toxic manifestations including skin rash, diarrhea, liver damage, renal injury, andpsychotic disturbances (134). No significant antitumor effects were observed.
Azasenine, O-diazoacetyl-L-senine, is a glutamine antagofist isolated from cultures of a strain of Streptomyces. Itexerts antitumon activity by inhibition of punine and pynimidine synthesis through the inhibition of amidation reactionsutilizing glutamine. Azasenine was tested in 56 patients withvarious types of cancer (36). Toxicities appeared in 5 to 20days. The alimentary tract was most prominently involved,with redness of the tongue and buccal mucosa, progressingto ulceration. Nausea and vomiting were commonly observed. One-fourth of these patients developed anorexia,apathy, electrolyte imbalance, and jaundice. These tendedto occur in old and debilitated patients. Marrow depressionand leukopenia were also observed. Brief partial remissionwas seen in 3 of 14 children with acute lymphocytic leukemia. Azasenine was tested p.o. in the treatment of multiplemyeloma without therapeutic effect (56).
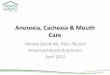
Escherichia coli aspanaginase exerts its antineoplasticactivity by depleting host L-aspanagine which is critical forthe survival of certain neoplastic cells. Aspanaginase is active in inducing remission in about 35 to 60% of patientswith acute lymphocytic leukemia (see Ref. 19). This therapeutic effect appears to be related to specific nutritionalrequirements for L-asparagine by malignant and presumably by normal T-lymphocytes. “Normal'‘and “malignant―B-lymphocytes do not require L-aspanagine in culture (Chart1) and, in comparison to T-lymphocyte lines, are affectedonly at 800 to 2000 times higher concentrations of the enzyme (96). The majority of patients with acute lymphocytic leukemia have “null―cells, some of which appear tohave been on the path to T-cell differentiation where prolifenation of the malignant clone led to the clinical neoplasm.Because there would be a deficiency of T-ceII leukemias toaccount for the asparaginase responses, some of thesecells must share the nutritional requirement for L-aspanagine. In general, differential nutritional requirements of individual host and neoplastic cells have not yet been clearlyelucidated. L-Aspanagine depletion by the enzyme treatmentresults in profound effects on host organ systems leading toa variety of nutritionally important toxicities (19, 20, 50, 93,94). The toxic effects on liven and pancreas are largely theresult of inhibition of protein synthesis in these organs.Patients may complain of nausea and vomiting, chills, andfever within hours of the 1st dose of aspanaginase. Biochemical hepatic dysfunction is observed in a majority ofpatients. Elevation of blood ammonia, a product of theenzyme reaction, has not produced majorconcomitant neurological problems. Hepatic functional impairment is accompanied by profound hypoalbuminemia, hypocholestenolemia, and diminished clotting proteins (Factors V, VII, X,
DAYS
E
0
U)-j-jwC.,
w-j
w
z,
Chart 1. Cell growth of 2 T-Iymphocyte lines (MOLT 3 and RPMI 8402) and4 B-lymphocyte lines in culture in the presence (•)and in the absence ( 0) of i.asparagine in Roswell Park Memorial Institute Medium 1640 with 10% dialyzed fetal calf serum. Call growth was shown by the number of viable cellsas measured by the dye exclusion test (from T. Ohnuma at al (96).
VIII, and IX, prothrombin, and fibninogen). Microscopic observation has shown severe fatty metamorphosis of theliven. The endocrine and exocnine functions of the pancreasare also commonly affected by aspanaginase, and approximately 5% of adults have overt pancreatitis. Hyperglycemiaand hypoinsulinemia without clinical evidence of pancreatitis have frequently been recognized (44). Toxic effects onthe CNS appear to be due to depression of necessary aminoacids. CNS dysfunction ranging from mild depression anddrowsiness to impaired sensonium, psychosis, and frankcoma has been noted in adults. Electroencephalogramsobtained from patients exhibiting CNS dysfunction havebeen diffusely abnormal. The CNS dysfunction from asparaginase might be due to a decreased amount of available Lasparagine on L-glutamine onto the increased concentrationof L-aspartate and L-glutamate. L-Asparagine administrationin such patients coincided with clinical improvement ofmental status (54, 94, 95). Loss of up to 20% of pretreatmentbody weight was seen after aspanaginase treatment (Chart2) (95). Aspanaginase has minimal effects on the bone manrow and is not cytotoxic to oral and intestinal mucosa on tohair follicles.
Vitamin Antagonists. Galactoflavin, 6,7-dimethyl-9-(2'-acetoxyethyl)isoalloxazine, is a potent riboflavin antagonistin rats. Six patients with advanced neoplasms were treatedwith galactoflavin in combination with a synthetic diet (76).All developed riboflavin deficiency, i.e., weight loss, cheilosis, glossitis, seborrheic dermatitis, and normochnomicnonmocytic anemia. Two suggestive instances of transientclinical improvement were seen.
4-Deoxypynidoxine is a vitamin B6 antagonist. Three patients with histiocytic lymphoma and 3 with acute lymphocytic leukemia on a vitamin B6-poor diet were fed the antagonist (47). Two of the patients were treated with 4-deoxypynidoxine, and both developed grand mal seizures. The remaining patients were treated with a smaller dose of 4-deoxypynidoxmne.A slight reduction in lymph node size for a
JULY 1977 2401
on May 20, 2020. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

T. Ohnuma and J. F. Holland
may be related to the subclinical folate deficiency commonly observed in patients with neoplastic diseases, particularly with cancer of the head and neck. Low pretreatmentlevels of serum folate appear to predispose patients to thetoxic effects of methotnexate, but correlation with the degree of tumor response has not been good. Oral mucosaltoxicity occurs as redness, pain, and ulceration. Diarrhea isseen occasionally. Skin rash occurs in approximately 10 to20% of patients treated with therapeutic doses. Nausea,anorexia, and, less commonly, vomiting are noted during onafter methotnexate administration, especially with largedoses. Subclinical injury is particularly noteworthy, andrepeated doses could prove catastrophic since methotnexate is excreted almost exclusively by the kidney. Liven damage is rarely noted after moderate doses because of ratherrapid clearance, but hepatic fibrosis and cirrhosis havebeen reported after long-term administration of methotnexate (see above).
Clinical toxicity of methotrexate is almost a direct function of the duration of administration of the drug and, to alessen extent, a function of the dose of the drug (121). Thisis shown distinctly in high-dose treatment with methotnexate followed by leucovonin rescue which extends the usefulness of this compound in other types of solid tumors with,in general, remarkably little hematological toxicity (33). This
has been particularly therapeutic in osteogenic sarcoma(41, 64). At high doses methotnexate appears to exert itstherapeutic effects by entering into the tumor cells by filtnation, diffusion, on by other passive mechanisms rather than
by carrier transport alone (41). The clinical toxicity has beencorrelated with the drug concentration in the circulatingblood. New data indicate that administration of high-dosemethotnexate (more than 50 mg/kg) is accompanied byexcretion of significant amounts ofthe metabolite 7-hydroxymethotrexate (63). The lower aqueous solubility of the 7-hydnoxy metabolite may have significant toxicological importance.
Trace MetalsandElectrolytes.Manyof the metalsfoundin trace quantity in normal and neoplastic tissues are knownto be essential for certain biological reactions. The biological role of some metals that are often present in tissues isnot known. In some cases their presence may simply nepresent contamination from the environment. Funst (42) hasindicated that most antitumor drugs can act as chelatingagents and has speculated that this property may be importantly involved in chemothenapeutic action. 3-Ethoxy-2-oxo-butylaldehyde bis-thiosemicanbazone (kethoxal thiosemicanbazone) is a copper chelating agent. Thirty-fourpatients treated with this compound developed dose-limiting neunotoxicity, e.g. , panesthesias, myalgia, motor weakness, and hallucinations. Nausea, vomiting, and bone marrow depression were also observed (106).
Regression of malignant tumors was observed in magnesium and potassium depletion induced by diet and hemodialysis (101). This observation will undoubtedly stimulatecontinuing investigation into the effects of minerals and
electrolytes on tumor growth.
Perspectives
Years ago when chemotherapy was considered the last
I
>-
0
2402 CANCER RESEARCH VOL. 37
Asporag nose
l000!U/kQ
@3:O@@
@ 0@
0 @:1@t@@ T“i―t―[―T―f―I―i'[―i―i―iI I@ I
0 2 4 6 8 10 2 14 6 8 20WEEKS
Chart 2. Changes in serum albumin and body weight after treatmentwith 1000 IU of E. coil asparaginase per kg in a patient (D. W.) with acutemyalocytic leukemia.
brief duration was noted in 2 patients with histiocytic lymphoma.
Four patients with acute lymphocytic leukemia who wereon a normal diet were treated with 4-deoxypynidoxine for 33to 80 days (129). Two of the patients developed sebonrheicdermatitis, which is taken as evidence of vitamin B. deficiency. However, there was no clinical evidence of bonemarrow remission.
6-Aminonicotinamide is an antagonist of nicotinamide. Ithas been shown to be active against a number of expenimental tumors. 6-Aminonicotinamide produced 1 negression in 25 patients with renal cell carcinoma. Toxicity appears to take 2 clinical forms. One is a “deficiency'‘stateand occurs as a form of stomatitis which includes buccalulceration, cheilosis, and glossitis, as well as blephanitiswith photophobia and dryness. The other manifestation isneurological, i.e. , 8th nerve damage manifested by a grosson audiometnically detectable hearing defect and tinnitus.
Nausea and vomiting are also commonly seen (26, 51).Methotnexate (amethoptenin) is the folate antagonist. De
nivatives of tetrahydrofolate function as cofactors for manyof the enzymes that are required for the de novo synthesis ofnucleotides, punines, and thymidylate. Modifying the structune of folic acid by substituting an amino group for the 4-hydnoxy group in the ptenidine nucleus produced aminoptenin, a very potent and specific inhibitor of dihydnofolateneductase. Both aminoptenin and its N'°-methyl derivative,methotnexate, proved to be effective chemothenapeuticagents in the treatment of acute lymphocytic leukemia inchildren. Antifols are also of curative value in choniocancinoma and related tnophoblastic tumors of women. Methotnexate has broad spectrum activity in a modest percentageof cases against squamous cell carcinomas of the head andneck and in adenocancinoma of the breast (see Ref. 79).
The bone marrow and alimentary tract epithelium are the2 tissues most affected by folic acid analogs. Bone marrowtoxicity manifests as neticulocytopenia, anemia, leukopenia, and thrombocytopenia. After a single iv. dose ofmethotnexate the bone marrow begins to recover in 10 to 14days. The toxicity may be more severe and pronounced ifpatients are in poor condition or have infection on com promised livenor bone marrow function. This increased toxicity
on May 20, 2020. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Cancer Chemotherapy and Immunotherapy
resort for the hopelessly ill patient with advanced cancer,antitumon drugs were frequently given too late to be effective. Even active drugs were often indicted for shorteningthe lives of cancer patients. This is understandable whenone recognizes that the list of complications of chemothenapeutic and immunothenapeutic agents is long and the nutnitional impact is formidable. The risks, however, must beviewed in proper perspective. Most of the complicationslisted are reversible and resolve in a matter of weeks. Therisks of cancer chemotherapy and immunotherapy are smallcompared to the natural consequences of untreated canceron the host. The most drastic reactions described rarelyoccur in day-to-day management. Many nutritionally impontant untoward effects can be prevented on treated nonspecifically with antiemetics, analgesics, antidiannheal agents,antibiotics, and transfusions of blood components duringthe initial critical phase of chemotherapy and immunothenapy to maintain an appropriate nutritional status.
Cancer patients who were placed on an elemental dietrich in calories, amino acids, and vitamins before and duning treatment with 5-fluonounacil and, in some cases, radiotherapy showed no drug-related rectal lesions and maintamed their pretreatment body weight (11). Chemotherapyin combination with panentenal nutrition is well tolerated(23, 24) in cancer patients who are nutritionally depletedand who would otherwise have been deprived of adequateantitumon chemotherapy for fear of complications frommalnutrition and inanition. Suggestive evidence has beenpresented that nutritionally less deprived patients are morelikely to respond to chemotherapy (77). Specific antidoteshave been used to counteract toxic effects of the chemotherapeutic agents. Leucovonin against methotnexate, deoxycytidine against cytosine arabinoside (100), thymidineagainst 5-iodo-2'-deoxyunidine (83), and L-asparagineagainst aspanaginase (54, 94, 95) are some examples.
Additionally, increasing success in the long-term controlof acute leukemia (55), Hodgkin's disease (31) and otherlymphomas, and certain carcinomas and sarcomas has 5evened the vicious cycle promulgated on the host by neoplasiaand toxic agents. Indeed, with the use of appropriate induction regimens, certain diseases can be brought under satisfactony clinical control within a few weeks. With maintenance therapy, such patients may enjoy good health andnormal daily activity for a period of years. The time is athand when physicians must consider chemotherapy as pnimany therapy with the objective of cure or with the intent ofeffecting increase in life-span for patients with certainhighly sensitive tumors. In such cases it makes no sense towait until the patient is far along in his disease and suffersfrom advanced nutritional consequences of metastatic cancer.
It has been shown that tumor growth is slowed by starvation and that i.v. nutrition makes tumors grow fasten (119).In experimental animal systems and in man, accumulatingevidence indicates that intermittent intensive treatment issuperior to continuous treatment (see Ref. 40). These findings should lead to short-term intensive combined modalities to attempt tumor debulking, remission induction, oncure, rather than long continuous treatment with nutritionalmaintenance.
More importantly, the concept of chemotherapy haschanged from last resort in the treatment of advanced disease to surgical adjuvant in the treatment of breast cancer(9, 39) and other neoplasms. Chemotherapy is now given topatients who show no evidence of disease, who are ambulatory and maintain normal activity, and who thus have normal appetite and nutrition. Chemotherapy is given to thesepatients with minimal nutritional consequences.
As cancers become more definitely characterized andunderstood, the nutritional treatment of tumor and normaltissues may be more effectively approached.
References
1. Aust,J.B.,Andrews, N. C.,Schroeder,J.M.,and Lawton, R. C. ClinicalNote: Phase II Study of 1-Aminocyclopentane Carboxylic Acid (NSC1026) in Patients with Cancer. Cancer Chemotherapy Rept., 54: 237-241, 1970.
2. Aust, J. B., and Roux, K. Phase I Study of 1-Aminocyclopentane Carboxylic Acid (NSC-1026) in Cancer Patients. Cancer ChemotherapyRept., 49: 63-64, 1965.
3. Bast, A. C., zbar, B., Borsos, T. and Rapp, H. J. BCG and Cancer. NewEngI. J. Med., 290: 1413-1429, 1458-1469, 1974.
4. Bellet, R. E., Mastrangelo, M. J., Engstrom, P. F., Strawitz, J. G.,Weiss, A. J., and Tarbro, J. W. Clinical Trial with SubcutaneouslyAdministered 5-Azacytidine (NSC-102816). Cancer ChemotherapyRept., 58: 217-222, 1974.
5. Bergsagal, D. E., Ross, S. W., and Baken, D. T. Evaluation of NewChemotherapeutic Agents in the Treatment of Multiple Myeloma. V. 1-Aminocyclopentane Carboxylic Acid (NSC-1026). Cancer Chemotherapy Rept., 21: 101-106, 1962
6. Berndt, J., and Hiller, I. Formininoglutaminsaure Auscheidung unterder Therapie mit Cyclophosphamid, KIm. Wochschr., 43: 333-334,1965.
7. BIum, A. H., and Carter, S. K. Adriamycin, a New Anticancer Drug withSignificant Clinical Activity. Ann. Internal Med., 80: 249—259,1974.
8. Blum, R. H., Carter, S. K., and Agre, K. Clinical Review of Bleomycin —aNew Antineoplastic Agent. Cancer, 31: 903-914, 1973.
9. Bonadonna, G., Brusamolino, E., Valagussa, P., Rossi, A. , Brugnatelli,L. , Brambilla, C., DeLena, M. , Tancini, G., Bajetta, E., Musumeci, R.,and Veronessi, U. Combination Chemotherapy as an Adjuvant Treatment in Operable Breast Cancer. New EngI. J. Med., 24: 405—410,1976.
10. Borison, J. L. Arena Postrema: Chemoreceptor Trigger Zone for Vomiting. Life Sci., 14: 1807—1817,1974.
11. Bounous, G., Gentile, J. M., and Hugon, J. Elemental Diet in theManagement of the Intestinal Lesion Produced by 5-Fluorouracil inMan. Can.J.Surg.,14:312-324,1971.
12. Brennan, M. J., Vaitkevicius, V. K., and Rebuck, J. W. MegaloblasticAnemia Associated with Inhibition of Thymidine Synthesis. Blood, 16:1535-1545, 1960.
13. Broder, L. E., and Carter, S. K. Pancreatic Islet Cell Carcinoma. II.Results of Therapy with Streptozotocin in 52 Patients. Ann. InternalMed.,79:108-118,1973.
14. Brown, J. H., and Kennedy, B. J. Mithramycin in the Treatment ofDisseminated Testicular Neoplasms. New Engl. J. Med., 272: 111-118,1965.
15. Brown, R. R. Amino Aciduria Resulting from Cycloleucine administration in Man. Science, 157: 432—434,1967.
16. Brunner, K. W., and Young, C. W. A Methylhydrazine Derivative inHodgkin's Disease and Other Malignant Neoplasms: Therapeutic andToxic Effects Studied in 51 Patients. Ann. Internal Med., 63: 69—86,1965
17. Burdinguet, L., Begin, N., and Sarkar, N. K. Mechanism of AntitumorAction of 1-Aminocyclopentane Carboxylic Acid. Nature, 194: 1082-1083, 1962.
18. Calabresi, P., and Parks, R. E., Jr. Alkylating Agents, Antimetabolites,Hormones, and other Antiproliferative Agents. In: L. 5. Goodman andA. Gilman (eds.), The Pharmacological Basis of Therapeutics, Ed. 4,pp. 1348-1395. New York: The MacMillan Co., 1970.
19. Capizzi, R. L., Bertino, J. R., and Handschumacher, A. E. L-Asparaginase. Ann. Rev. Med., 21: 433-444, 1970.
20.Capizzi,A.L.,Bertino,J.R.,Skeel,R.T.,Creasey,W. A.,Zanes,A.,Olayon, C., Peterson, A. G., and Handschumacher, A. E. L-Asparaginase: Clinical, Biochemical, Pharmacological and Immunological Studies. Ann. Internal Med., 74: 893—901,1971.
21. Chauvergne, J., LaPorte, G., Hoerni, B., and Legendre, P. Hypocal
JULY 1977 2403
on May 20, 2020. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

T. Ohnuma and J. F. Holland
cdmie par Actinomycine D. Presse Med., 78: 847, 1970.22. Cockel, P. Antiemetics. Practitioner, 206: 56—63,1971.23. Copeland, E. M., MacFadyen, B. V., Lanzotti, V. J., and Dudrick, 5. J.
Intravenous Hyperalimentation as an Adjuvant to Cancer Chemotherapy. Am. J. Surg., 129: 167-173, 1975.
24. Copeland, E. M., MacFadyen, B. V., MacComb, W. S., Guillamondegni,0. , Jesse, A. H., and Dudrick, S. J. Intravenous Hyperalimentation inPatients with Head and Neck Cancer. Cancer, 35: 606-61 1, 1975.
25. Costanzi, J., Gagliano, A., Loukas, D., Sakai, J., Thurman, G., Harris,N., and Goldstein, A. The Use of Thymosin (thy.) in Patients withDisseminated Neoplasia: Toxicity and immunological Correlation.Proc. Am. Assoc. Cancer Res., 16: 135, 1975.
26. Cowan, D. H., and Alison, A. E. Evaluation of 6-Aminonicotinamide inthe Treatment of Metastatic Hypernephroma. Cancer ChemotherapyAept., 54: 175-179, 1970.
27. Davis, P. L. Decrease in X-ray Evidence of Bone Metastasis in ProstaticCancer during Use of Triparanol. Clin. Med., 8: 2360-2362, 1961.
28. DeFronze, A. A. , Colvin, 0. M. , Braine, H., Robertson, G. L. , and Davis,P. J. Cyclophosphamide and the Kidney. Cancer, 33: 483-491 , 1974.
29. DeVita, V. T., Canellos, G., Carbone, P. P., Baron, S., Levy, H., andGralnick, H. Clinical Trials with the Interferon (lnF) Inducer Polyinosinic-cytidylic Acid. Proc. Am. Assoc. Cancer Res., 11: 21, 1970.
30. DeVita, V. T., Carbone, P. P., Owens, A. H., Jr., Gold, G. L., Krant, M.J., and Edmonson, J. Clinical Trials with 1,3-Bis(2-chloroethyl)-1-nitrosourea, NSC-409962. Cancer Res., 25: 1876-1881, 1965.
31. DeVita, V. T. , Serpick, A. A. , and Carbone, P. P. Combination Chamotherapy in the Treatment of Advanced Hodgkin's Disease. Ann. InternalMed.,73:881-895,1970.
32. DiMarco, A. , and Lenaz, L. Daunomycin and Adriamycin. In: J. F.Holland and E. Frei, Ill (eds.), Cancer Medicine, pp. 826-835. Philadelphia: Lea & Febiger, 1973.
33. Djerassi, I., Rominger,J., Kim, J. S., Turchi, J., Suransri, U., andHuges, D. Phase I Study of High Doses of Methotrexate with CitrovorumFactor in Patients with Lung Cancer. Cancer, 30: 22-30, 1972.
34. Einhorn, M., and Davidsohn, I. Hepatotoxicity of Mercaptopurine. J.Am. Med. Assoc., 188: 802-806, 1964.
35. Ellison, A., Holland, J. F., Weil, M., Jacquillat, C., Boiron, M., Bernard,J., Sawitsky, A., Rosner, F., Gussoff, B., Silver, A. T., Karanas, A.,Cuttner, J., Spurr, C. L., Hays, D. M., Blom, J., Leone, L. A., Haurani,F., Kyle, A., Hutchison, J. L. , Forcier, R. J. , and Moon, J. M. ArabinosylCytosine: A Useful Agent in the Treatment of Acute Leukemia in Adults.Blood, 32: 507-523, 1968.
36. Ellison, A. A., Karnofsky, 0. A., Sternberg, S. S., Murphy, M. L., andBurchenal, J. H. Clinical Trials of O-Diazoacetyl-L-serina (Azaserine) inNeoplastic Diseases. Cancer, 7: 801-814, 1954.
37. Ellison, A. A. , Silver, R. T., and Engle, R. L. ,Jr. Comparative Study of 6-Chloropurine and 6-Mercaptopurine in Acute Leukemia in Adults. Ann.InternalMed., 51: 322-338, 1959.
38. Field,A. K.,Young,C. W., Krakoff, I. H.,Tytell,A.A., Lampson,G. P.,Nemas, M. M., and Hilleman, M. A. Induction of Interferon in HumanSubjects by Poly I:C. Proc. Soc. Exptl. Biol. Med., 136: 1180-1186,1971.
39. Fisher, B., Carbone, P., and Economou, S. G. L-Phenylalanine Mustard(L-PAM) in the Management of Primary Breast Cancer: a Report of EarlyFindings.New EngI.J. Med., 292: 117-122,1975.
40. Frei,E., III.Effectof DoseandScheduleon Response.In: J. F.Hollandand E. Frei, Ill (eds.), Cancer Medicine, pp. 717-730. Philadelphia: Lea& Febiger, 1973.
41. Frei, E., Ill, Jafte, N., Tattersall, M. H. N., Pitman, S., and Parker, L. NewApproaches to Cancer Chemotherapy with Methotrexate. New EngI. J.Med.,292:846-851,1975.
42. Furst, A. Chemistry of Chelation in Cancer, pp. 20-23. Springfield, Ill.:Charles C Thomas, 1963.
43. Gailani, S. D., Holland,J. F., and Glick, A. Effects of Boxidine onHuman Serum Sterols and Neoplasms. CIIn. Pharmacol. Therap., 13:91-96, 1972.
44. Gailani,S.D.,Nussbaum,A., Ohnuma,T., andFreeman,A. DiabetesinPatients with Asparaginase. Clin. Pharmacol. Therap., 12: 487-490,1971.
45. Garner, F. B., Meyer, C. A. , White, D. S. , and Lipton, A. Aerosol BCGTreatment of Carcinoma Metastasis to the Lung: a Phase I Study.Cancer, 35: 1088-1094, 1975.
46. GeIler,W.,andLacher,M.J. Hodgkin'sDisease.Med.Clin. NorthAm.,50: 819-832, 1966.
47. Gellhorn, A. , and Jones, L. 0. Pyridoxine Deficient Diet and Desoxypyridoxine in the Therapy of Lymphosarcoma and Acute Leukemia in Man.Blood, 4: 60-65, 1949.
48. Ghaftar,A., Cullen, A. T., Dunbar,N., and Woodruff,M. F. A. Antitumour Effect in Vitro of Lymphocytes and Macrophages from MiceTreated with Corynebacterium parvum. Brit. J. Cancer, 29: 199-205,1974.
49. Gottlieb, J. A., and Drewinko, B. Review of the Current Clinical Statusof Platinum Coordination Complex in Cancer Chemotherapy. Cancer
Chemotherapy Rept., 59: 621-628, 1975.50. Haskell, C. M., Canellos, G. P., Leventhal, B. G., Carbone, P. P., Block,
J. B. , Serpick, A. A. , and Selawry, 0. S. L-Asparaginase, Therapeuticand Toxic Effects in Patients with Neoplastic Disease. New Engl. J.Med.,281:1028-1034,1969.
51. Hailer, F. P., Weismann, S. G., Thompson, H. G., Jr., Hyman, G., andMartin, D. S. Clinical Experience with 6-Aminonicotinamide. CancerRca., 21: 31-37, 1961.
52. Higby, D. J., Wallace, J. J., Jr., Albert, D., and Holland J. F. D@mminodichloroplatinum in the Chemotherapy of Testicular Tumors. J. Urol.,112: 100-104, 1974.
53. Higby, D. J. , Wallace, J. J., Jr., and Holland, J. F. Diamminodichloroplatinum (NSC-119875): a Phase I Study. Cancer Chemotherapy Rept.,57: 459-463, 1973.
54. Holland, J. C. B., Fasanelio, S., and Ohnuma, T. Psychiatric SymptomsAssociated with L-Asparaginase Administration. J. Psychiat. Ras., 10:105-113, 1974.
55. Holland, J. F. The Acute Leukemias. In: P. B. Beeson and W. McDermott (eds.), Textbook of Medicine, Ed. 14, pp. 1485-1492. Philadelphia:W. B. Saunders Co., 1975.
56. Holland, J. F., Gehan, E. A. , Brindley, C. 0. , Dederick, M. M. , Owens, A.H., Jr., Shnider, B. I., Taylor, A., Frei, E., Ill, Selawry, 0. S., Aegelson,W., and Hall, T. C. A Comparative Study of Optimal Medical Care withand without Azaserine in Multiple Myeloma. Clin. Pharmacol. Therap.,2: 22-28, 1961.
57. Holland, J. F., Scharlau, C., Gailani, S., Krant, M. J., Olson, K. B.,Horton, J., Shnider, B. ‘.,Lynch, J. J., Owens, A., Carbone, P. P.,Colsky, J. , Grob, D., Miller, S. P., and Hall, T. C. Vincristine Treatmentof Advanced Cancer: A Cooperative Study of 392 Cases. Cancer Res.,33: 1258-1264, 1973.
58. Horton, J. , Olson, K. B. , Sullivan, J., Reilly, C. , Shnider, B., and theEastern Cooperative Oncology Group. 5-Fluorouracil in Cancer: anImproved Regimen. Ann. Internal Med., 73: 897-900, 1970.
59. Howard, J. G., Scott, M. T., and Christie, G. H. Cellular MechanismsUnderlying the Adjuvant Activity of Corynebacterium parvum ; lnteractions of Activated Macrophages with T and B Lymphocytes. In: Immunopotentiation, pp. 101-120. New York: American Elsevier PublishingCo., 1973.
60.Hrodak,0.,and Vesely,J.5-AzacytidineinChildhoodLeukemia.Neoplasma, 18: 493-503, 1971.
61. Humphrey, E., Hymes, A., Ausman, A., and Ferguson, D. J. An Evaluation of Actinomycin D and Mitomycin C in Patients with AdvancedCancer. Surgery,50: 881-885,1961.
62. Hutter, A. M., and Kayhoe, D. E. Adrenal Cortical Carcinoma: Results ofTreatment with op-ODD in 138 Patients. Am. J. Med., 41: 581-592,1966.
63. Jacobs, 5. A. , Stoller, R. G. , Chabner, B. A. and Johns, D. G. 7-Hydroxymethotrexate as a Urinary Metabolite in Human Subjects andRhesus Monkeys Receiving High Dose Methotrexata. J. CIin. Invest.,57: 534-538, 1976.
64. Jaffe,N., Frei,E., Ill, Traggio,D.,andBishop,T.AdjuvantMethotrexateand Citrovorum Factor Treatment of Osteogenic Sarcoma. New EngI. J.Med., 291: 994-997, 1974.
65. Johnson, A. 0. Preliminary Phase II Trials with 1-Aminopentane Carboxylic Acid (NSC-1026), Cancer Chemotherapy Rept., 32: 67-71 , 1963.
66. Johnson, A. 0., Matter, G., Wilson, W., Hice, G., and Kramentz,E.Phase I Evaluation of DTIC (NSC-45388) and Other Studies in MalignantMelanoma in the Central Oncology Group. Cancer Treat. Rept., 60:183-187, 1976.
67. Karnofsky, 0. A. Late Effects of Immunosuppressive Anticancer Drugs.Federation Proc., 26: 925—932,1967.
68. Kay, H. E. M., Knapton, P.J., O'Sullivan,J. P., Wills, D. G., Harris, R. F.,Innes, E. M., Stuart, J., Schwartz, F. C. M., and Thompson, E. N.Encephalopathy in Acute Leukemia Associated with Methotrexate Therapy. Arch. Disease Childhood, 47: 344—354,1972.
69. Koss, L. G., Melamed, M. A., and Mayer, K. The Effect of Busulfan onHuman Epithelia. Am. J. Clin. Pathol., 44: 385-397, 1967.
70. Kraft, R. 0. Triparanol in the Treatment of Disseminated MammaryCarcinoma. Cancer Chemotherapy Rept., 25: 113-115. 1962.
71. Kramer, W. B. Cytarabine. Ann. Internal Med., 82: 684-688, 1975.72. Kremer, W. B., and Laszlo, J. Hematologic Effects of Cancer. In: J. F.
Holland, and E. Frei, III, (ads.), Cancer Medicine, pp. 1085—1099.Philadelphia: Lea & Febiger, 1973.
73, Kyle, A. A., Schwartz, A. S., Oliner, H. L., and Dameshak, W. A Syndrome Resembling Adrenal Cortical Insufficiency Associated withLong-term Busulfan (Myleran) Therapy. Blood, 18: 497-510, 1961.
74. Lampson, G. P., Field, A. K., Tytell, A. A., Names, M. M., and Hilleman,M. R. Relationship of Molecular Size of rln:rCN (poly I:C) to Induction ofInterferon and Host Resistance. Proc. Soc. Exptl. Biol. Med., 135: 911-916,1970.
75. Landau, B. A., Laszlo, J., Stengle, J., and Burk, D. Certain Metabolicand Pharmacologic Effects in Cancer Patients Given Infusions of 2-Daoxy-D-Glucose. J. NatI. Cancer Inst., 21: 485—494,1958.
2404 CANCER RESEARCH VOL. 37
on May 20, 2020. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Cancer Chemotherapy and Immunotherapy
103. Pilch, V. H., Fritze, D., and Kern, D. H. Immune ANA in the Immunotherapy of Cancer. Med. Clin. North Am., 60: 567-583, 1976.
104. Piro, A. J., Wilson, R. E., Hall, T. C., Aliapoulios, M. A., Nevinny, H. B.,and Moore, F. D. Toxicity Studies of Fluorouracil Used with Adrenalectomy in Breast Cancer. Arch. Surg., 105: 95-99, 1972.
105. Regelson, W., and Holland, J. F. Clinical Experience with Methylglyoxal-bis-guanyl-hydrazone Dihydrochloride. A New Agent with Clinical Activity in Acute Myalocytic Leukemia and the Lymphomas. CancerChemotherapy Rept., 27: 15-26, 1973.
106. Aegelson, W., Holland, J. F., and Talley, R. W. Clinical PharmacologicStudy of Kethoxal bis(thiosemicarbazone) (NSC-82116) in AdvancedCancer. Cancer Chemotherapy Rept., 51: 171-177, 1967.
107. Aoenigk, H. H. Hepatotoxicity of Methotrexate in the Treatment ofPsoriasis. Arch. Dermatol., 103: 250-261 , 1971.
108. Sadoff, L. Patterns of Intravenous Glucose Tolerance and Insulin Response before and after Treatment with Streptozotocin (NSC-85998).Cancer Chemotherapy Rept., 56: 61-69, 1972.
109. Samuels, M. L., Leary, W. V., Alexanian, A., Howe, C. D., and Frei, E.,Ill. Clinical Trials with n-lsopropyl-a-(2-methylhydrazino)-p-toluamideHydrochloride in Malignant Lymphoma and Other Disseminated Neoplasia. Cancer, 20: 1187-1194, 1967.
110. SandIer, S. G., Tobin, W., and Henderson, E. S. Vincristine InducedNeuropathy in a Clinical Study of Fifty Leukemic Patients. Neurology,19: 367-374, 1969.
111. Schafer, L. A., Washington, M. L., and Goldstein, A. L. ThymosinImmunotherapy—A Phase I Study. Proc. Am. Assoc. Cancer Res.,16: 233, 1975.
112. Schein, P. S., O'Connell, M. J., Blom, J., Hubbard, S., Magrath, I.Bergevin, P., Wiernik, P. H., Ziegler, J. L., and DeVita, V. T. ClinicalAntitumor Activity and Toxicity of Streptozotocin (NSC-85998). Cancer,34: 993-1000, 1974.
113. Scott, M. T. Biochemical Effects of the Adjuvant Corynebacteriumparvum. Cellular Immunol., 5: 459-479, 1972.
114. Seifert, P., Baker, L. M., Reed, M. L., and Vaitkevicius, V. K. Comparison of Continuously Infused 5-Fluorouracil with Bolus Injection inTreatment of Patients with Colorectal Adenocarcinoma. Cancer, 36:123—129,1975.
115. Shapiro, W. A., Chrenik, N. L., and Posner, J. B. Necrotizing Encephalopathy Following lntraventricular Instillation of Methotrexate. Arch.Neurol., 28: 96-102, 1973.
116. Shaw, A. K., Moore, E. W., Mueller, P. S., Frei, E., III, and Watkin, D. M.The Effect of Actinomycin D on Childhood Neoplasms. Am. J. DiseaseChildhood, 99: 628—635,1960.
117. Sparks, F. C., Silverstein, M. J., Hunt, J. S., Haskell, C. M., Pilch, Y. H.,and Morton, D. L. Complications of BCG Immunotherapy in Patientswith Cancer. New Engl. J. Med., 289, 827-830, 1973.
118. Spies, 5. K., and Snyman, H. W. Procarbazine (Natulan) in the Treatment of Hodgkin's Disease and Other Lymphomas. South African Med.J., 40: 1061-1064, 1966.
119. Steiger, E., Oram-Smith, J., Miller, E., Kuo, L., and Vars, H. Effects ofNutrition on Tumor Growth and Tolerance to Chemotherapy. J. Surg.Aes., 18: 455-461, 1975.
120. Stolinsky, D., Solomon, J., and Pugh, R. P. Clinical Experience withProcarbazine in Hodgkin's Disease, Reticulum Cell Sarcoma and Lymphosarcoma. Cancer, 26: 984—990,1970.
121. Sullivan, A. D., Miller, E., and Sikes, M. P. Antimetabolite-metaboliteCombination Cancer Chemotherapy. Cancer, 12: 1248-1262, 1959.
122. Talley, A. W., and Vaitkevicius, V. K. Megaloblastosis Produced by aCytosine Antagonist, 1-@-D-Arabinofuranosylcytosine. Blood , 21: 352-362, 1963.
123. Tan, C. T. C., Cargeon, H. W., and Burchenal, J. H. The Effect ofActinomycin D on Cancer in Childhood. Pediatrics, 24: 544-561 , 1959.
124. Thomas, E. D., Storb, A., Clift, A. A., Fefer, A., Johnson, L., Neiman, P.E. , Lerner, K. G. , Glucksberg, H., and Buchner, C. D. Bone MarrowTransplantation. New EngI. J. Med., 292: 832-843, 895-902, 1975.
125. Veterans Administration Cancer Chemotherapy Study Group. Preliminary Clinical Note 1-Aminocyclopentane-1-carboxylic Acid (NSC-1026).Cancer Chemotherapy Rapt., 6: 59-60, 1960.
126. Vogl, S., Ohnuma, T., Perloff, M., and Holland, J. F. CombinationChemotherapy with Adriamycin and cis-Diamminedichloroplatinum inPatients with Neoplastic Diseases. Cancer, 38: 21-26, 1976.
127. Von Hoff, D. D., and 5lavik, M. 5-Azacytidina—a New Anticancer Drugwith Significant Activity in Acute Myelocytic Leukemia. Advan. Pharmacol. Chemotherapy, 85: 237-245, 1976.
128. Waxman, S., Corcino, J. J., and Herbert, V. Drugs, Toxins and DietaryAmino Acids Affecting Vitamin B,2 or Folic Acid Absorption or Utilization. Am. J. Med., 48: 599—608,1970.
129. Weir, D. A., and Morningstar, W. A. The Effect of Pyridoxine DeficiencyInduced by Desoxypyridoxine on Acute Lymphatic Leukemia of Adults.Blood, 9: 173-182, 1954.
130. Weisberger, A. S., and Suhrland, L. G. Studies of Analogues of LCysteine and L-Cystine Ill. The Effect of Selenium Cystine on Leuke
76. Lane, M., Alfrey, C. P., Mengel, C. E., Doherty, M. A., and Doherty, J.The Rapid Induction of Human Riboflavin Deficiency with Galactoflavin. J. Clin. Invest., 43: 357—373,1964.
77. Lanzotti, V. L., Copeland, E. M., Ill, George, S. L., Dudrick, S. L., andSamuels, M. L. Cancer Chemotherapeutic Response and IntravenousHyperalimentation. Cancer Chemotherapy Rapt., 59: 437-439, 1975.
78. Lipkin, M. Cell Replication in the Gastrointestinal Tract in Man. Gastroenterology, 48: 616—624,1965.
79. Livingston, A. B., and Carter, S. K. single Agents in Cancer Chemotherapy. New York: lFl/Plenum, 1970.
80. LoBuglio, A. F., and Neidhart, J. A. A Review of Transfer Factor Immunotherapy in Cancer. Cancer, 34: 1563-1570, 1974.
81. Lubitz, J. A., Freeman, L., and Okun, A. Mitotane Use in InoperableAdrenal Cortical Carcinoma. J. Am. Med. Assoc., 233: 1109-1112, 1973.
82. Luce, J. K., Thurman, W. G., Isaac, B. C., and Talley, A. W. ClinicalTrials with the AntitumorAgent 5-(3,3-Dimethyl-1-triazeno) imidazole-4-carboxamide (NSC-45388). Cancer Chemotherapy Rapt., 119—124,1970.
83. Mark, J. B. D., and Calabresi, P. Regional Protection in Cancer Chemotherapy. II. Preliminary Studies with Hypogastric Artery Infusion ofThymidine during Treatment with 5-lodo-2'-deoxyuridine. CancerChemotherapy Rept., 16: 545-551 , 1962.
84. Mass, A. E. Clinical Evaluation of 1-Amino Cyclopentane CarboxylicAcid (NSC-1026) in Plasmacytic Myeloma. CancerChemotherapy Rept.,28: 17-19, 1963.
85. McIntosh, S., and Aspnes, G. T. Encephalopathy Following CNS Prophylaxis in Childhood Lymphoblastic Leukemia. Pediatrics, 32: 612-618, 1973.
86. Moertel, C. G., Reitemeier, A. J., Bolton, C. F., and Shorter, A. G.Cerebellar Ataxia Associated with Fluorinated Pyrimidine Therapy.Cancer Chemotherapy Rapt., 41: 15-18, 1964.
87. Moertel, C. G., Reitemeier, R. J., and Hahn, A. G. Therapy of AdvancedGastrointestinal Cancer with 1-3-bis(2-Chlorethyl)-1 -nitrosourea(BCNU). Clin. Pharmacol. Therap., 9: 652-656, 1968.
88. Munto,A.W.,Talley,R.W.,Caldwell,M.J.,Levin,w.C.,andGuest,M.M. Observations on the Mechanism of Hemorrhagic Toxicity in Mithramycin (NSC-24559) Therapy. Cancer Res., 29: 697-704, 1969.
89. Myers, W. P. L., and Magill, G. B. Alterations in Calcium Metabolism inCancer Patients Treated with 6-Diazo-5-oxo-L-norleucine. Proc. Soc.Exptl. BioI. Med., 93: 314-318, 1956.
90. Nevinny, H. B., and Hall, T. C. Effects of Methotrexate on Hormoneinduced Hypercalcemia in Breast Cancer. Second InternationalSymposium on Chemotherapy, Naples, 1961. In: A. T. Kuennerle at al.(eds.), Antineoplastic Chemotherapy, pp. 211-218. Basel: S. Karger,1963.
91. Ochoa, M., Jr. Alkylating Agents in Clinical Cancer Chemotherapy.Ann. N. Y. Acad. Sci., 163: 921-930, 1969.
92. Oettgen, J. F., Pinsky, C. M., and Delmonte, L. Treatment of Cancerwith Immunomodulators Corynebacterium parvum and Levamisole.Med. Clin.NorthAm.,60:511-537,1976.
93, Oettgen,J. F., Stephenson, P. A., Schwartz, M. K., Leaper, A. D., Tallal,L., Tan, C. C., Clarkson, B. D., Golbay, A. B., Krakoff, I. H., Karnofsky,D. A., Murphy, M. L., and Burchenal, J. H. Toxicity of E. coli LAsparaginase in Man. Cancer, 25: 251-278, 1970.
94. Ohnuma, T., Holland, J. F., Freeman, A., and Sinks, L. F. Biochemicaland Pharmacological Studies with Asparaginase in Man. Cancer Res.,30: 2297-1305, 1970.
95. Ohnuma,T.,Holland,J. F.,Nagel,G.,andSt.Arneault,G.Effectsof LAsparaginasa in Acute Myelocytic Leukemia. J. Am. Med. Assoc., 210:1919-1921,1969.
96. Ohnuma, T., Holland, J. F., Arkin, H., and Minowada, J. L-Asparagina Requirements of Human T- and B-Lymphocytes in Culture. J.NatI. Cancer Inst. , in press.
97. Ohnuma, T., Selawry, 0. 5., Holland, J. F., DeVita, V. T., Shedd, D. P.,Hansen, H. H., and Muggia, F. M. Clinical Study with Bleomycin:Tolerance to Twice Weekly Dosage. Cancer, 30: 914-922, 1972.
98. Oliner, H., Schwartz, A. , Aubio, F., Jr. , and Damershek, W. InterstitialPulmonary Fibrosis Following Busulfan Therapy. Am. J. Med., 31: 134-139,1961.
99. O'Neill, G. J., Henderson, D. C., and White, A. G. The Role of AnaerobicCoryneforms on Specific and Non-specific Immunological Reactions.Immunology, 24: 977-995, 1973.
100. Papac, A., Creasay, W. A., Calabresi, P., and Welch, A. D. Clinical andPharmacological Studies with 1-@-ArabinofuranosyIcytosine (CytosineArabinoside). Proc. Am. Assoc. Cancer Res., 6: 50, 1965.
101. Parsons, F. M., Edwards, G. F., Anderson, C. K., Ahmad, S., Clark, P.B. , Hetharington, C., and Young, G. A. Regression of Malignant Tumours in Magnesium and Potassium Depletion Induced by Diet andHemodialysis. Lancet, 1: 243-244, 1974.
102. Perlia, C. P., Bubisch, N. J., Wolter, J., Edelberg, 0., Dederick, M. M.,and Taylor, S. G., Ill. Mithramycin Treatment of Hypercalcemia. Cancer,25: 389—394,1970.
2405JULY 1977
on May 20, 2020. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

T. Ohnuma and J. F. Holland
mias. Blood, 11: 19-30,1956.131. Weiss, D. W. Nonspecific Stimulation and Modulation of the Immune
Response and of States of Resistance by the Methanol ExtractionResidue Fraction of Tubercle Bacilli. NatI. Cancer Inst., Monograph,35: 157-171, 1972.
132. Weiss, D. W. MER and Other Mycobacterial Fractions in the lmmunotherapy of Cancer. Med. CIin. North Am., 60: 473—497,1976.
133. Weiss, H. D., Walker, M. D., and Wiernik, P. H. Neurotoxicity of Commonly Used Antineoplastic Agents. New EngI. J. Mad., 291: 75-81 , 127-133, 1974.
134. White, L. P., and Shimkin, M. B. Effects of DL-Ethionine in Six Patientswith Neoplastic Diseases. Cancer, 7: 867-872, 1954.
135. Whitacar, J. P., Jr., Bodey, G. P., Harris, J. E., and Freireich, E. J. LAsparaginase. New EngI. J. Med., 282: 732-734, 1970.
136. Wintrobe, M. M. Clinical Hematology, Ed. 7, Chap. 55, pp. 1703-1737..Philadelphia: Lea & Febiger, 1974.
137. Zubrod, C. G. Agents of Choice in Neoplastic Disease. In: A. C. Sartorelli and D. G. Johnes (ads.), Antineoplastic and ImmunosuppressiveAgents; Handbook of Experimental Pharmacology, Vol. 38, Part 1, pp.1-11 . New York: Springer-Verlag, 1974.
2406 CANCERRESEARCHVOL. 37
on May 20, 2020. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1977;37:2395-2406. Cancer Res Takao Ohnuma and James F. Holland ImmunotherapyNutritional Consequences of Cancer Chemotherapy and
Updated version
http://cancerres.aacrjournals.org/content/37/7_Part_2/2395
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/37/7_Part_2/2395To request permission to re-use all or part of this article, use this link
on May 20, 2020. © 1977 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from