Embed Size (px)
Citation preview

397
-An old gentleman in Mount Florida suffered from whatwas presumably malignant disease of the pylorus. He both’vomited and passed dark blood at stool. Palliative measureswere adopted, and his diet was regulated. Fish, which hadnot been particularly forbidden, was partaken of one day,and this was followed by excessive vomiting of blood andby death.A lady in Glasgow is at present suffering from what has
been variously diagnosed as disease of the stomach, pylorus,omentum, and liver. At any rate she is jaundiced, wasted,and subject to severe pains and sickness shortly after takingfood. She feels frequently very sick, vomits frothy fluid anddark bilious matter, and occasionally passes decomposing,loose, bloody, dark matter of a most offensive smell. Onevery occasion on which she has partaken of fish these.symptoms have been aggravated if present, and have beenbrought on if absent.
Cases such as these have been continually cropping up andcausing great anxiety. It seemed to me that, under anycircumstances of debility, fish, instead of being a genialdiet, is a very dangerous one, and I had got into theroutine practice of almost always forbidding it; but I havebeen induced to put these cases on record because I believenow that it is the preparation, the cooking, of the fish thatis at fault, and not the fish itself. Recently I have beenable to see all the recognised benefits of this diet from usingit steamed, and not boiled. And for this hint 1 am indebtedto the intelligence of a patient. I had, as usual, forbiddenfish to be eaten, explaining my reasons. I was told thatfish steamed, as was done in that house, was as tender ascould be, and never disagreed with them. The fish so
prepared was partaken of both with relish and benefit. I
.got a steamer for myself, have recommended this plan of
.cookery to my patients, and have had satisfactory results.Dieting is the half, and sometimes the best half, of medicaltreatment; and, perhaps a little to my chagrin, I find thatthis system of preparing fish has been specially recommendedby various schools of cookery. Perhaps, however, manymedical men, like myself, may be unaware of the fact, simpleas it is, that boiled fish, fried fish, and almost any otherkind of cooked fish, are all inferior in digestibility to steamed.fish. The kettle I have used is a simple and efficientsteamer. The fish is never touched from the moment it isput on the drainer in the kettle till it is cooked, and the,drainer is so constructed that it can be removed fromthe kettle with the fish and placed upon the dish for thetable.
I have ventured to put these few cases on record both onaccount of the dissatisfaction I have had formerly and thesatisfaction I have now in ordering a cheap, nourishing diet.
Glasgow. ______________
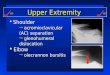
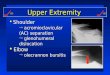
NOTE ON A RARE DISLOCATION OF THEELBOW-JOINT.
BY C. GEORGE BATTISCOMBE, M.B., C.M. Aber.
ON April 9th I was called to see a gentleman who hadmet with an accident while hunting. 1 found him lying ina field, and was told that his horse, after jumping a fencewith a long drop, had fallen over backwards upon his rightarm and leg. He complained of great pain in the elbow-,joint on the slightest movement. It was very much alteredin shape, and evidently severely injured. I secured the armin a sling, and had him removed to the Cottage Hospital(Chislehurst, Sidcup, and Cray Valley), which was close by.On his arrival at the hospital I examined the arm, and
found it in the following condition. The forearm was fixedat rather more than a right angle to the arm; all power ofnatural movement of the elbow-joint was lost; and anyattempt at forcible movement caused great pain. The handwas partially pronated, but on turning it pronation andsupination could be readily performed. The elbow-jointappeared too wide from within outwards and from beforebackwards; it presented two prominences below, an innerand outer, and one above the latter, which projected back-wards and was continuous with the forearm. The innerangle of the joint was too high, so that the arm appeared tobe shortened. There being no amount of swelling, the fol-
Blowing points could be clearly made out. The ulna and Iolecranon were missing from their natural position in rela-
1 Patented by Orme, Evans, and Co., of Wolverhampton.
tion to the humerus, the two condyles of which could be dis-tinctly felt with the notch between them. The ulna andolecranon were resting fully half an inch above the externalcondyle of the humerus, the elbow projecting about an inchbeyond the latter. The radius could be felt above with itshead resting against the outer border of the humerus. It wasnot separated from the ulna, and rotated readily on pronat-ing and supinating the hand.
1 put the patient under chloroform, and carefully examinedfor any fracture. I could find none whatever, and concludedthat it was a case of complete dislocation outwards of bothbones of the forearm. I then proceeded to reduce thedislocation. Grasping the forearm with one hand, and theelbow with the fingers of the other, I pulled it steadilydownwards, endeavouring to get the olecranon over theexternal condyle. It took some minutes to do this, andrequired a good deal of force. Then, holding the olecranonbelow the condyle with the left hand, I seized the forearmlower down and used it as a lever, and while forciblyextending the forearm 1 rotated it outwards. On continuingthe extension, the olecranon suddenly slipped into itsnatural position. The joint immediately answered to allits proper movements, but when left alone tended slightlyto return. I fixed it at a right angle on a posterior angularsplint.When I called in the evening the patient was free from
pain, and complained only of a feeling of numbness in thearm and hand of the injured side. The next morning, whenI arrived at the hospital, he had gone home; but I aseer-’
°
tained that, beyond the numbness and a little swelling, hewas very comfortable. A week afterwards he was doingwell, could move the joint pretty freely, and was free frompain.
Complete lateral dislocation of both the bones of the fore-arm is, I believe, extremely rare. I have seen no descriptionof it, though it is mentioned in several surgical works.
St. Mary Cray, Kent.
HYSTERIA OR TETANUS?
BY JAMES LAFFAN, L.R.C.S.I.
THE following case presents some interesting features :-On Easter Sunday last I was hurriedly called to attend a
young girl, a servant, who had been accidentally shot. I
found her lying on a bed bleeding profusely from a largeragged wound, which seemed to have carried away the
greater part of her right cheek. She had received the con-tents of a gun-a large charge of small (No. 6) shot-dis-charged at a distance of not more than four feet. It beinglate in the evening, I satisfied myself that there was no frac-ture of importance, and merely arrested the haemorrhage.Next day I found that the charge of shot had struck
between the molar teeth of the upper and lower jaws, whichmust have been in apposition at the moment. The teethwere uninjured. The pellets glancing off the teeth had dis-tributed themselves in every ’direction. Some had gonealmost vertically upwards, breaking off the inner end of thezygoma, and finally lodging themselves beneath the eyelidin the inner angle of the orbit. Others had been deflecteddownwards, others back as far as the parotid gland, othersagain forward to the angle of the mouth. A few hadpenetrated deeply through the canine fossa, and lodged them-selves beneath the zygoma. All the muscles of this side ofthe face were more or less bruised and lacerated, and therewas much sloughing.
After three days’ incessent poulticing and syringing all thesloughs and foreign bodies came away, leaving a clean,healthy wound. I extracted in all 311 shot. On the fifthday the patient complained of a good deal of pain aboutthe jaw, also of stiffness in that region (the latter wasattributed to the bandages), and of a burning pain in thestomach. On the sixth day she was seized with violenttetanoid convulsions. I was sent for, and on my arrivalfound her in a state of perfect rigidity, moaning with pain.Opisthotonos was well marked. I gave chloroform, andafter a little while the spasms ceased. I then ordered herfull doses of bromide of potash and chloral hydrate. Shewas quiet until the next day, when she was again seizedwith similar symptoms. They again yielded to chloroform.She was attacked again twice during the night of that day,but much less violently. Her condition was one of stupornow, from the effect of the hypnotics. The following day