Embed Size (px)
DESCRIPTION
Citation preview

Elbow Dislocation and PhysiotherapyD. N. Bid
The elbow joint displays an elegant balance between stability and mobility. While allowing a wide range of motion, the joint has an inherent stability that requires a considerable force to dislocate. As a result, a significant percentage—approximately one third of elbow dislocations—are associated with fractures of bony components of the elbow.
Dislocations without associated fracture are termed simple, while dislocations with accompanying fracture are termed complex.
Classification
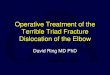
Simpson classification
Simpson classification of elbow dislocation
Both Radius and Ulna
PosteriorLateral
Medial
Medial
Lateral
DivergentAnteroposterior
Mediolateral
Ulna aloneAnterior
Posterior
Radius
Anterior
Posterior
Lateral
Most commonly, the elbow dislocates posteriorly. Immediate reduction is essential to reduce the risk of neurovascular or cartilaginous complications. Hence, this will be discussed here in detail.
Definition of Posterior Elbow Dislocation
Image 1: Elbow dislocation
1

Posterior elbow dislocation (PED) occurs when the radius and ulna are forcefully
driven posterior to the humerus. Specifically, the olecranon process of the ulna moves into
the olecranon fossa of the humerus and the trochlea of the humerus is displaced over the
coronoid process of the ulna. PED is classified as simple or complex and staged according to
severity.
Epidemiology /Etiology
In children under 10 years, PEDs are the most common type of joint dislocation. In adults,
they are the second most commonly dislocated joint proceeded by shoulder
dislocations. Elbow dislocations annually affect between 6 and 7 people per
100,000. Approximately 90% of all elbow dislocations are directionally classified as posterior
or posterolateral and are more commonly seen in the non-dominant upper extremity (UE).
Typically, this injury is caused by a traumatic fall onto an outstretched arm resulting in an
hyper-extension injury. However, more recent research has suggested that axial
compression, elbow flexion, valgus stress, and forearm supination lead to a rotational
displacement of the ulna on the distal humerus. Most commonly, the dislocation is
associated with a damaged or torn anterior capsule.
PED can be classified as simple (74%) or complex (26%). A simple dislocation is absent of
fractures while a complex dislocation has related fractures. Fractures may exist on the radial
head, coronoid process, olecranon, humeral condyles, or capitellum. These fractures may
lead to disruption of the medial collateral ligament (MCL), lateral collateral ligament (LCL), or
interosseous membrane.
'Terrible triad' is a term used to describe a severe complex dislocation with intra-articular
fractures of the radial head and coronoid process. Elbow dislocations are staged depending
on the disruption of the following stabilizers: the ulnohumeral articulation, MCL, and LCL.
(see Table 1 below)
2

Table 1 Adapted from O’Driscoll SW, Jupiter JB, King GJW, Hotchkiss RN, Morrey BF. The unstable elbow. J Bone Joint Surg. 2000;82-A(5):724-738.
Characteristics/Clinical Presentation
After a PED, a person may feel immediate instability. Depending on the severity of the
damage, they may report a 'popping' sensation or noise upon dislocation.
With palpation and observation, the olecranon is prominent creating a divot over the distal
triceps.
After reduction, radial-sided elbow pain may persist in addition to 'snapping' with
supination.
Swelling, joint line tenderness, and decreased range of motion (ROM) should be expected.
Various degrees of injury are also seen in muscles surrounding the elbow that originate at
the medial or lateral epicondyles.
When ligaments are not compromised, recurrent dislocations are not common.
Differential Diagnosis
To diagnose PED, radiographs in the anterior, posterior, and lateral views with valgus stress
are obtained.
Table 2: below depicts other injuries that should be considered when suspecting PED.
Diagnosis Cause Examination Findings
Posterolateral
Rotary
Instability
Insufficiency of the ulnar LCL
Varus instability, positive lateral
pivot-shift test, recurrent
dislocations
Associated
Fracture
Traumatic forces through radial
head,humeralcondyles, coronoid
process,olecranon, or capitellum
Radiographic diagnostics in
addition to tenderness over
fracture sight. Positive Elbow
Extension Sign
Compartment
Syndrome
Fractures, swelling, casting,
trauma
Pain out of proportion to the injury,
pulselessness, pallor, paresthesia,
paralysis, poikilothermia
Complex Regional Unknown Persistent pain after injury,
3

Pain Syndrome
(CRPS)
swelling, increased sensitivity,
change in skin color/texture,
decreased ROM, weakness
Examination
Physical therapy examination should include a vascular and neuromuscular screen,
observation, palpation, muscle testing, ROM, and special ligamentous tests. The following
information outlines ways to test for potential impairments after PED.
A vascular assessment should include palpation of the brachial, radial, and ulnar arteries.
During the neuromuscular screen, dermatomes, myotomes, and reflexes should be
evaluated with emphasis on the ulnar, median, and radial nerves.
Observe the elbow for any ecchymosis, rubor, or deformities.
During palpation, a disrupted triangle sign may indicate joint dislocation.
The triangle sign is obtained by palpating the tip of the olecranon, medial, and lateral
epicondyles while in elbow flexion, resulting in a triangle configuration.
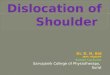
Image 3: Physiotherapist applies supination with a
valgus stress and axial compression while taking the
patient from extension into flexion. The elbow will
sublux at 40 degrees of flexion if instability exists.
Further flexion will reduce the joint with an audible and
palpable clunk.
It is essential to palpate for associated fractures in the elbow complex.
The elbow extension sign can be used to rule out a fracture.
Specific muscles that attach to the elbow should be evaluated including the elbow and wrist flexors/extensors and supinators/pronators.
Documentation of elbow ROM is necessary when following the progression of rehabilitation.
Other outcome measures include the Mayo Elbow Performance Index (MEPI) and the Disabilities of the Arm, Shoulder, and Hand (DASH).
Patients with PED may also have concomitant collateral ligament ruptures at the elbow. If this occurs, the patient will be at greater risk of developing recurrent instability.
4

To assess for this, the following special tests should be performed:
-varus and valgus stress test, - the lateral pivot-shift test (Posterolateral Rotational Instability Test) (see Image 3), and -apprehension testing.
Physical therapists should be alert for the following potential complications associated with PED:
-neurological deficits including hypoaesthesia of the hand in the ulnar nerve distribution,
-concomitant fractures,
-myositis ossificans, and
-degenerative changes in the joint.
Radiographs are indicated when there is no response to care after four weeks of conservative treatment, significant activity restriction for more than four weeks, or non-mechanical pain is present.
As with all patients, clinicians should be aware of red flags listed in Table 3 below.
Table 3 Adapted from Bussieres AE, Peterson C, Taylor JA. Diagnostic imaging guideline for musculoskeletal
complaints in adults - an evidence-based approach. Part 2: upper extremity disorders. J Manipulative Physiol Ther
2008 Jan;31(1):2-32.
Medical Management
Before surgery is considered, research indicates reduction under local or general anesthesia as the primary treatment for PED. Patient presentation including elbow stiffness and pain are key factors when considering the need for surgery along with irreducible dislocation, gross
5

instability, neurovascular injuries, and associated fractures. The most common surgical options include an open procedure, with or without Speed's procedure, and excision or closed arthroplasty. An open procedure, more commonly seen in neglected PED < three months, involves ulnar nerve release, humeroulnar and humeroradial reduction, possible triceps lengthening using Speed's procedure, and wires and/or screws placed in the olecranon for stabilizing the joint.
In the Elzohairy study, within two weeks the wires were removed and active motion was initiated, while the screws were removed six months after surgery. Excision arthroplasty is also used when patients present with neglected PED, but studies suggest high reoccurrences of pain and instability.
In other studies, surgery was indicated only when concomitant fractures occurred with PED.
Ligaments injured with fractures or dislocations are repaired via sutures attaching them back to the bone.
Once surgery is complete, the patient is immobilized with time frames varying based on the individual and the surgeon's protocol.
Hinged braces, fixators, plaster casts, and slings are utilized to keep the elbow in a position of approximately 70-80o of flexion and slight pronation.
Active movement is usually initiated between three to fourteen days, with slow, gradual supination.
When treating a post-surgical PED patient, physical therapists should be cautious of pin site infection.
A patient is able to return to functional activities around twelve weeks and sports around six months.
While much of the research highlights general dislocation of the elbow with some positive outcomes following surgery, there is not enough evidence to support surgical interventions for PED.
Physical Therapy Management
While nonsurgical treatment approaches to PED can vary depending on the level of tissue involvement, there are key elements to consider throughout the clinical decision-making process. PED can occur on a continuum of severity; therefore, the treatment must be diverse as well.
Treatment can vary from aggressive immediate AROM to traditional plaster immobilization for several days.
If a fracture occurs secondary to dislocation, intra-articular bone fragments and fracture position may dictate treatment.
Closed or nonsurgical reduction by a physical therapist is only performed if there are no associated fractures.
6

Uhl et al. described one technique for reduction: the patient hangs their affected arm over the back of a chair as the clinician tractions the ulna in a downward direction.
After reduction of the joint, instability is evaluated. A splint should be applied and the patient should be referred for radiographs if the joint subluxes or dislocates while assessing instability.
If left untreated (unreduced) patients may develop soft tissue contractures and localized osteoporosis.
The following clinical decision-making algorithm for immobilization and surgical options can be used following acute dislocations.
Decision-Making Algorithm: Adapted from O’Driscoll SW, Jupiter JB, King GJW, Hotchkiss RN, Morrey BF. The
unstable elbow. J Bone Joint Surg. 2000;82-A(5):724-738.
7

Surgical Treatment Algorithm: Adapted from O’Driscoll SW, Jupiter JB, King GJW, Hotchkiss RN, Morrey BF. The
unstable elbow. J Bone Joint Surg. 2000;82-A(5):724-738.
Generally following reduction the patient is placed in a posterior splint at 45-90o of elbow
flexion for three days to three weeks.
Evidence reveals detrimental effects of prolonged immobilization including flexion
contractures, enhanced perception of pain, and increased duration of disability, all of which
prolong the rehabilitation process.
Throughout the immobilization phase, wrist and shoulder function should be maintained
through ROM and strengthening exercises.
Inflammation is a common sequela following PED and can be addressed using compression,
ice, and effleurage.
When the patient no longer requires immobilization, functional treatment begins with gentle
AROM and PROM exercises in a pain-free range targeting the entire UE.
8

Research by Haan et al. shows better outcomes when early rehabilitation is functionally-
based and pain-free.
Multi-angle isometric activities and Proprioceptive Neuromuscular Facilitation patterns for
the elbow help decrease pain, increase ROM, and begin to target strengthening components
in the preliminary stages of recovery.
When pain is no longer a barrier to treatment, functional progressive resistance exercises
should be implemented to improve total UE muscle strength and endurance.
Although full extension should be a goal of rehabilitation, care must be taken to protect the
vulnerable elbow and avoid hyperextension. It is important to be cautious during passive
mobilization and ROM.
Multiple articles have warned that aggressive PROM (especially into extension) and forceful
manipulation may cause myositis ossificans and should be avoided.
Also, Uhl et al. suggested that any valgus stress applied to the elbow should be avoided
throughout treatment so not to stress the already compromised tissues.
Therapeutic goals in the later phase of rehabilitation include attaining full ROM and strength
capabilities of the entire affected arm, suppression of pain, and restoration of functional
abilities to pre-injury level.
Clinical Bottom Line
Since the elbow joint is one of the most commonly dislocated joints, it is imperative that
physical therapists are aware of its complications and the best evidence for treatment.
It is important to explore the level of severity and degree of complication associated with
each PED since this dictates the patients' prognoses. Patients who have had simple PED with
early reduction usually have good outcomes.
In most cases, there is potential for developing instability and degenerative joint disease.
Overall the best treatment for PED is initial short term restricted motion (usually two weeks
or less) followed by early mobilization including PROM and progressing to AROM and
functional strengthening.
Long duration plaster of Paris immobilization has been show to have poorer functional
outcomes.
9

Hinged Brace.
===================================
POSTOPERATIVE REHABILITATION OF ELBOW DISLOCATION
Note: There is currently no rehabilitation program developed specifically for elbow dislocations.The following rehabilitation protocol was developed from numerous sources of literature.
Individual cases will vary dependent upon age, pain tolerance, and complications with thereductions. In most articles prognosis is excellent if the patient has full ROM within 3 weeks.
Phase I: Weeks 1-4
Goals: Control edema and painEarly full ROMProtect injured tissuesMinimize deconditioning
Intervention:• Continue to assess for neurovascular compromise• Elevation and ice• Gentle PROM - working to get full extension• Splinting as needed• General cardiovascular and muscular conditioning program• Strengthen through ROM• Soft tissue mobilization if indicated – especially assess the brachialis myofascia
Phase II: Weeks 5-8
Goals: Control any residual symptoms of edema and painFull ROMMinimize deconditioning
Intervention:
10

• Active range of motion (AROM) exercises, isometric exercises, progressing to resistedexercises using tubing or manual resistance or weights• Incorporate sport specific exercises if indicated• Joint mobilization, soft tissue mobilization, or passive stretching if indicated• Continue to assess for neurovascular compromise• Nerve mobility exercises if indicated• Modify/progress cardiovascular and muscular conditioning program
Phase III: Weeks 9-16
Goals: Full range of motion and normal strengthReturn to preinjury functional activities
Intervention:
• Interventions as above• Modify/progress cardiovascular and muscular conditioning• Progress sport specific or job specific training
11