Embed Size (px)
DESCRIPTION
physiotherapy
Citation preview

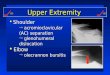
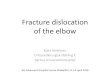
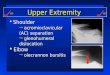
ELBOW DISLOCATION

ANATOMY OF ELBOW JOINT• Three bones come together to make up the elbow
joint.
• The humerus is the bone in the upper arm.
• Two bones from the forearm (the radius and the ulna) form the lower part of the elbow.
• Each of these bones has a very distinct shape.
• Ligaments connected to the bones keep all of these bones in proper alignment.


• The elbow is both a hinge joint and a ball and socket joint.
• As muscles contract and relax, two unique motions occur at the elbow.
• Bending occurs through a hinge joint that allows the elbow to bend and straighten. This is called flexion and extension, respectively.
• Rotation occurs though a ball and socket joint that allows the hand to be rotated palm up and palm down. This is called pronation and supination, respectively.

CAUSES OF INJURY• Elbow dislocations typically occur when a person
falls onto an outstretched hand. When the hand hits the ground, the force is sent to the elbow. Usually, there is a turning motion in this force. This can drive and rotate the elbow out of its socket.
• Elbow dislocations can also happen in car accidents when the passengers reach forward to cushion the impact. The force that is sent through the arm can dislocate the elbow, just as in a fall.


TYPES OF DISLOCATION
There are two common types of dislocation. a. Posterior dislocation: In this type, the
proximal end of ulna radius are displaced posteriorly.
B. Postero-lateral dislocation: In this type which is commonest, in addition to the
posterior displacement, the radius and ulna are displaced laterally. This is often associated with rupture of the medial epicondyle of the humerus and stretching and paralysis of the ulnar nerve.

CLINICAL FEATURES• Severe pain in the elbow• swelling• inability to bend the arm are all signs of an elbow
dislocation. • In some cases, people may lose feeling in their hand
or lose a pulse (can't feel a heartbeat in the wrist). • Arteries and nerves run by the elbow, so it is possible
a person might have injured them during the dislocation. Consequently, a nerve injury may result in abnormal sensations or inability of normal distal arm or hand functions below the elbow dislocation.

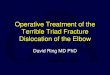
Treatment: Reduction is done under general anaesthesia. After reduction a padded posterior plaster slab is
applied with the elbow in a safe degree of flexion.
Complications: Immediate complication could be injury to brachial
artery or median and ulnar nerves. There could also be fractures of medial epicondyle or coronoid also process. Later complication could be myositis osificans and joint stiffness.

FRACTURES OF THE PROXIMAL END OF THE RADIUS:
The following fractures occur at the proximal
end of the radius. a. Fracture of the head of
radius. b. Fracture of the neck of radius.
c. Epiphyseal separation in children.

FRACTURE HEAD OF RADIUS Mechanism of injury: These fractures are produced by forcible valgus
strain which forces the head of the radius against the capitulum and causes a fracture of one or both.
Clinical features: • Pain in the outer aspect of the elbow. • Tenderness over the head of the radius and
swelling due to haemarthrosis.• Supination and pronation are painful and
restricted.

Treatment : Simple cracks in the head or neck without
displacement or tilt are best treated with posterior plaster slab and cuff and collar. If the swelling is marked, aspiration may be done.
Complications: Myositis ossificans is a common
complication.


FRACTURES OF THE PROXIMAL END OF ULNA:
FRACTURE OLECRANON: This fracture occurs due to a fall on the
flexed elbow. The olecranon is fractured usually near the base. The fragment gets pulled up by the insertion on the triceps tendon.

THE FOREARM:
1) Fracture of the Radius and Ulna. 2) Fracture of Radius alone. 3) Fracture of Ulna alone. 4) Fracture of the proximal third of ulna
with dislocation of the head of radius (Monteggia fracture dislocation).
5) Fracture of the distal third of radius with dislocation of the inferior radio-ulnar joint (galeazzi fracture dislocation).

Radius and ulna fracture:

FRACTURE BOTH BONES FOREARM:
• The radius and ulna are fractured either by a fall on the outstretched hand or by direct injury.
• In children, the greenstick type of fracture is very common.

Clinical features: This is common in young adults due to a
fall on the hand. The diagnosis is obvious by the deformity, swelling and abnormal mobility.
Treatment:
Closed reduction and plaster immobilisation: Displaced fractures of the radius and ulna need manipulative reduction. The fragments are hitched in stable position and an above elbow plaster slab is applied with good padding in front of the elbow. Check radiographs are taken to confirm the alignment.

Finger and shoulder exercises are started immediately. After the subsidence of the swelling, the plaster cast is completed.
These fractures show a great tendency to displace even inside the plaster when it gets loose and the ulna angulates due to gravity. Radiographs are repeated after 2 weeks. If it shows a tendency to angulate, the plaster is removed and reapplied in a close fitting manner. Immobilisation is continued for 8-10 weeks with check radiographs every 2 weeks.

• Open reduction and internal fixation: Closed reduction may fail due to the interposition of soft tissues or instability of the reduction. In such cases, the fractures are treated by surgical reduction and fixation by a compression plate and screws.

Complications: Volkmann's ischaemic contracture. Non-Union. Malunion. Cross Union.

FRACTURES OF THE RADIUS: Fractures of radius alone without
displacement are rare and are immobilised in an above elbow posterior slab for 3 to 6 weeks till the union is sound.
FRACTURES OF THE ULNA: This fracture in the lower 1/3 is common in
adults due to direct injury. When a person tries to ward off blow on is head with his forearm. Hence, it is known stick fracture. Fractures of the ulna alone, without displacement are immobilised in an above elbow posterior slab.

Fracture lower end of radius:

Fracture shaft of ulna: