Embed Size (px)
Citation preview

Digestive Diseases and Sciences, Vol. 40, No. 2 (Februa~ 1995), pp. 315-319
C A S E R E P O R T
Nonsteroidal Antiinflammatory Drug-Induced Colonic Stricture
An Unusual Cause of Large Bowel Obstruction and Perforation
M I C H A E L H.E . R O B I N S O N , FRCS, T I M O T H Y W H E A T L E Y , FRCS, and IAN H. L E A C H , MB, BS
KEY WORDS: nonsteroidal antiinflammatory drugs; colonic diseases; intestinal perforation; large bowel obstruction.
Over 100 million prescriptions for nonsteroidal anti- inflammatory drugs (NSAIDs) are written annually in the United States (1) and more than 20 million in the U.K. (2). Gastroduodenal mucosal injury is a widely recognized side effect, up to 22% of patients on N S A I D treatment having peptic ulceration (2). More recently, inflammation and ulceration affect- ing both small and large intestine have been recog- nized as adverse effects (3-5). Of particular interest have been the reports of strictures, both broad and "d iaphragml ike , " involving jejunum and ileum as- sociated with the long-term usage of these drugs (6-8). A similar NSAID- induced colonic stricture was first reported in 1989 (9). Subsequent reports of colonic diaphragms have usually been in patients being investigated for iron-deficiency anemia (10- 15). Emergency presentat ion with large bowel ob- struction and perforation secondary to an NSAID- induced colonic stricture is previously unreported. We present such a case and review the literature.
CASE REPORT
A 53-year old white female with a seven-year history of rheumatoid arthritis was admitted as an emergency. She complained of a three-day history of lower abdominal pain, suddenly becoming severe 3 hr before admission with radiation to the right shoulder. She was taking di- clofenac (slow release), aspirin, ranitidine, and coprox-
Manuscript received March 3, 1994; revised manuscript re- ceived July 26, 1994; accepted July 28, 1994.
From the Departments of Surgery and Histopathology, Uni- versity Hospital, Nottingham NG7 2UH, U.K.
Address for reprint requests: Mr. M.H.E. Robinson, Depart- ment of Surgery, University Hospital, Nottingham NG7 2UH, U,K.
amol. Diclofenac had been regularly prescribed for the last five years.
She was distressed, pale, and sweaty. Pulse was 78 beats per minute, blood pressure 78/50, and temperature 36.8°C. Her abdomen was rigid and bowel sounds scanty. Serum amylase was normal and erect chest x-ray re- vealed free gas under the right hemidiaphragm. Following fluid resuscitation, surgical exploration was undertaken.
At laparotomy, she was found to have a l-cm perforation in a grossly distended and thinned cecum. The cause of obstruction was a tight stricture of the ascending colon, but the remaining small and large bowel appeared normal. A right hemicolectomy was performed. Pathologic evaluation of the resected specimen showed two separate similar areas of circumferential mucosal ulceration with stenosis second- ary to extensive submucosal fibrosis and hypertrophy of the muscularis propria; prominent lymphoid follicles were pres- ent through the bowel wall (Figures la,b and 2). One stric- ture was located in the ascending colon and the other at the ileocaecal valve involving the root of the appendix. Be- tween these strictures the cecum was distended and thinned, leading to perforation. The remaining resected small and large bowel was grossly and microscopically normal. There was not evidence of Crohn's disease and the mesenteric blood vessels were unremarkable without evi- dence of occlusion, vasculitis or amyloid.
The patient made an uneventful recovery.
DISCUSSION
The most widely recognized complicat ions of N S A I D therapy are the consequences of gastroduo- denal inflammation and ulcerat ion--pain , bleeding, and perforation. The first report of N S A I D damage in the more distal gastrointestinal tract was in 1966, cecal ulceration occurr ing in association with oxy- phenbutazone and indomethacin therapy (3). In a comprehensive review of the literature, Bjarnason et al (5) summarize a number of adverse effects of
Digestive Diseases and Sciences, VoL 40, No. 2 (February 1995) 0163-2116/95/0200-0315507.5(110 ,© 1995 Plenum Publishing Corporalion
315

ROBINSON ET AL
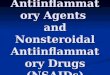
Fig 1.(a) Photograph of the opened resected specimen demonstrating obstructing stenoses proximal and distal to the perforated caecum, and (b) line drawing.
ingested NSAIDs on the small and large intestine, but do not include colonic stricture and obstruction. Small intestinal stricture associated with NSAID ingestion was described in 1973 (6), but obstruction due to "diaphragm disease" (multiple, 2- to 4-mm- thick concentric diaphragrnlike septa that narrow the lumen to a pinhole) was not recognized until
1987 (7). This unusual condition was identified in five separate cases by Lang et al (8) in a retrospec- tive review of 576 small bowel resections for ob- struction over a 16-year period. In this series, they also recognized broad-based stenoses associated with NSAID ingestion. They hypothesized an evo- lution of pathological changes in which tall, thin
316 Digestive Diseases and Sciences, Vol. 40. No. 2 (February 1995)

NSAID-INDUCED COLONIC STRICTURE
terminal ileum mucosa
Stenosis at ileocaecal valve
Grossly distended & thinned caecum with central perforation
Stenosis in ascending colon
Normal distal ascending colon mucosa
Fig 1. Continued.
mucosal diaphragms become broader-based humps or ridges and eventually short, fiat strictures due to the increasing fibrous obliteration of the segment of submucosa (8). It is conceivable that a similar pro- cess also occurs in the large bowel.
The first report of a colonic stricture caused by ingestion of NSAIDs was a letter by Sheers and Williams (9). They described two patients being investigated for " 'microscopic gastrointest inal blood loss" in whom colonoscopy revealed circum- ferential colonic scars with a "thin rim of erosion on the edge of each scar" leading to stricturing (9). Since then, a total of 10 more completely docu- mented cases have been reported (10-15), six from a single center in Switzerland (10, 15). Among these, there are several common themes relating to presentation, site of damage, implicated NSAID and method of delivery, and finally microscopic features. In all, histological examination of the strictures were consistent with NSAID-induced damage, the dominant feature being submucosal
fibrosis. The colonic stricture(s) have all occurred in the proximal transverse or right colon (apart from one of the originally described cases in the sig- moid). Third, eight of the 10 patients had an iron- deficiency anemia (10-15); in all but one of these (13), the strictures were associated with ulceration, restricted to the haustral folds (15). Finally, di- clofenac was an implicated drug in eight cases, all but one of the patients (12) taking a slow-release preparation. One of the two not on diclofenac was taking slow-release indomethacin.
The introduction of slow-release preparations may be moving the site of NSAID-induced gut dam- age more distally and suggests that its effect is local rather than systemic. Further evidence for a local effect is the observation that active NSAIDs in- crease intestinal permeability, while prodrugs, acti- vated after absorption, do not (16). The frequency with which diclofenac is implicated suggests the possibility of an idiosyncratic reaction. However, this is a commonly prescribed slow-release NSAID,
Digestive Diseases and Sciences, VoL 40, No. 2 (February 1995) 317

ROBINSON ET AL
Fig. 2. Mucosal ulcertion and conspicuous submucosal fibrosis (hematoxylin and eosin, x23),
and this drug is manufactured and widely pre- scribed in Switzerland (15), from where the major- ity of the reports have come.
The pathogenesis of the condition is uncertain, but it is possible that "'diaphragm disease" and longer intestinal strictures are a sequel to the preceding ul- ceration. This causality is suggested by two of the reports. In one patient (11), a diaphragm (attributed to
sulindac) in the transverse colon was segmentally resected. Four months later, having restarted sunlin- dac against medical advice, she presented again with anemia. Colonoscopy showed extensive ulceration proximal to the anastomosis. Repeat examination one month later showed four tight weblike strictures at the site of the ulceration, which had healed. In the second patient (10), colonoscopy revealed confluent ulcer-
318 Digestive Diseases and Sciences, VoL 40, No. 2 (February 1995~

N S A I D - I N D U C E D COLONIC STRICTURE
ation of the ascending colon which, at colonoscopy two years later, had healed to multiple diaphragmlike rigid circumferential septa. NSAIDs increase intesti- nal permeability and, in the face of a reduced mucosal barrier, intestinal contents may produce ulceration (5). Going et al (17) described narrow circumferential ulcers in the ileum of a woman on long-standing indo- methacin therapy and suggested that these may be the precursor of diaphragm disease. However, if ulcer- ation does progress to diaphragm disease, it probably happens infrequently. A postmortem study found small bowel ulceration in 21 of 74 subjects who had regularly taken NSAIDs in the six-month period prior to death, while no diaphragms were found (18).
Although the scale and significance of the problem, in terms of morbidity and mortality, is still poorly understood, various therapeutic options have been suggested. Withdrawal of NSAIDs is often not prac- tical since many patients would suffer intolerable symptoms. Prevention of enteropathy in those taking NSAIDs may be possible by the addition of misopros- toi, although the importance of enteropathy in causing strictures is unclear. Substitution of NSAID pro- drugs, like sulindac, has been suggested (5), but this was an implicated drug on two occasions (11, 12).
We are unaware of any other reported cases of NSAID-induced colonic stricture and believe that this report is the first to describe large bowel obstruction with subsequent cecal perforation caused by NSAIDs.
SUMMARY
Nonsteroidal antiinflammatory drugs (NSAIDs) are widely prescribed drugs that can result in gas- troduodenal ulceration. Adverse effects upon the small and large intestine are now more often recog- nized. Small intestinal obstruction secondary to both mucosal diaphragms and broad-based stenoses is reported, but colonic strictures appear to be less common. A case of NSAID-induced colonic stric- ture leading to large bowel obstruction and second- ary cecal perforation (previously unreported) is pre- sented. Twelve additional cases of NSAID-induced colonic stricture are reviewed from the literature and its possible pathogenesis is discussed.
ACKNOWLEDGMENTS
The authors thank Mr. C.A.S. Pegg, FRCS, for per- mission to report his patient and Dr. I. Talbot, FRCPath, for review of the pathology of this case.
REFERENCES
1. Gibson T: Nonsteroidal antiinflammatory drugs--another look. Br J Rheumatol 27:87-90, 1989
2. Hawkey C J: Nonsteroidal antiinflammatory drugs and peptic ulcers. Br Med J 300:278-284, 1990
3. Debenham GP: Ulcer of the caecum during oxyphenbuta- zone (Tanderil) therapy. Can Med Assoc J 94:1182-1184, 1966
4. Hudson N, Wilkinson MJ, Swannell AJ, Steele RJ, Hawkey CJ: Ileo-caecal ulceration associated with the use of di- clofenac slow release. Aliment Pharmacol Ther 7:197-200, 1993
5. Bjarnason I, Hayllar J, MacPherson AJ, Russell AS: Side effects of nonsteroidal anti-inflammatory drugs on the small and large interstine in humans. Gastroenterology 104:1832- 1847, 1993
6. Sturges HF, Krone CL: Ulcers and strictures of the jejunum in a patient on long term indomethacin therapy. Am J Gas- troenterol 59:162-169, 1973
7. Sukumar L: Recurrent small bowel obstruction with piroxi- cam. Br J Surg 74:186, 1987
8. Lang J, Price AB, Levi A J, Burke M, Gumpel JM, Bjarnson I: Diaphargm disease: pathology of disease of the small intestine induced by non-steroidal anti-inflammatory drugs. J Clin Pathol 41:516-526, 1988
9. Sheers R, Williams WR: NSAIDs and gut damage. Lancet 2(8672):1154, 1989
10. Huber T, Ruchti C, Halter F: Nonsteroidal antiinflammatory drug-induced colonic strictures: A case report. Gastroenter- ology 100:1119-1122, 1991
11. Monahan DW, Starnes EC, Parker AL: Colonic strictures in a patient on long-term non-steroidal anti-inflammatory drugs. Gastrointest Ednosc 38:385-388, 1992
12. Haque S, Haswell JE, Dreznick JT, West AB: A cecal diaphragm associated with the use of nonsteroidal anti- inflammatory drugs. J Clin Gastroenterol 15:332-335, 2992
13. Fellows IW, Clarke JMF, Roberts PF: Non-steroidal anti- inflammatory drug-induced jejunal and colonic diaphragm disease: a report of two cases. Gut 33:1424-1426, 1992
14. Pucius RJ, Charles AK, Adair HM, Rowe RCG, Hacking JC: Diaphragm-like strictures of the colon induced by non-steroidal anti-inflammatory drugs. Br J Surg 80:395-396, 1993
15. Halter F, Weber B, Huber T, Eigenmann F, Frey M, Ruchti C: Diaphragm disease of the ascending colon associated with sustained-release diclofenac. J Clin Gastroenterol 16:74-80, 1993
16. Bjarnason I, Fehilly B, Smethurst P, Menzies IS, Levi AJ: The importance of local versus systemic effects of non- steroidal anti-inflammatory drugs to increase intestinal per- meability in man. Gut 32:275-277, 199t
17. Going JJ, Canvin J, Sturrock R: Possible precursor of dia- phragm disease in the small intestine. Lancet 341:638-639, 1993
t8. Allison MC, Howatson AG, Torrance CA, Lee FD, Russell RI: Gastrointestinal damage associated with the use of non- steroidal anti-inflammatory drugs. N Engl J Med 327:749- 754, 1992
Digestive Diseases and Sciences, VoL 40, No. 2 (Februa~ 1995) 319