Embed Size (px)
Citation preview
HISTORY
36-year-old man.
CHIEF COMPLAINT: Increasing shortness of breath for the past month and
recent onset of neck pain.
PRESENT ILLNESS: He first noted eight years ago the onset of pulsations
in the neck while shaving and “felt” his heart beat when recumbent.
Progressive dyspnea on exertion and profuse sweating without fever have
been noted for the past two months. There is a history of a murmur in early
childhood, but no history of acute rheumatic fever.
Question: What diagnosis is suggested by this history?
17-1

Answer: The presence of a murmur in early childhood is compatible with a
congenital etiology, although rheumatic heart disease may occur without a
definite history of rheumatic fever.
Prominent pulsations in the neck may be arterial or venous. The neck pain
suggests that the pulsations are arterial. This pain may be due to a vigorously
pulsating artery that stretches the carotid sheath, causing arteritis. Prominent
arterial pulsations in the neck usually reflect a large stroke volume, as seen in
aortic regurgitation (AR) and patent ductus arteriosus (PDA).
Dyspnea on effort is a common and relatively early symptom of left ventricular
failure. Sweating may be a clue to the diagnosis of severe AR, and is thought
to be secondary to autonomic dysfunction.
Proceed
17-2

17-3
PHYSICAL SIGNS:
a. GENERAL APPEARANCE- 36-year-old mildly dyspneic man.
b. VENOUS PULSE - The CVP is estimated to be 7 cm H2O.
Question: How do you interpret the venous pulse?
ECG
JUGULAR
VENOUS
PULSE

Answer: The estimated CVP is at the upper limits of normal and the
venous wave form is normal.
c. ARTERIAL PULSE - (BP = 160/35 mm Hg)
Question: How do you interpret the arterial pulse?
CAROTID
PULSE
ECG
17-4

Answer: The pulse pressure is wide and the diastolic pressure is low. This
suggests a lesion with increased stroke volume and rapid diastolic runoff, such
as AR or PDA.
The carotid pulse is bifid or bisferiens (twice beating) in systole. Its presence is
most consistent with the diagnosis of AR, with or without a mild degree of
aortic stenosis. While hypertrophic obstructive cardiomyopathy may be
associated with a bifid arterial pulse, the wide pulse pressure is inconsistent
with this lesion.
Question: How do you explain the bisferiens pulse?
17-5

Answer: The first (percussion) wave relates to the forceful initial contraction
of the pre-(volume) loaded left ventricle (Starling’s Law of the Heart).
In addition, the velocity of left ventricular contraction is increased due to
the reduced after-(pressure) load associated with compensatory
peripheral vasodilation.
The second (tidal) wave is likely caused by reflected waves from the periphery
that are accentuated because of the large stroke volume in association with a
decreased peripheral resistance.
Following the second peak of the pulse wave, there is a rapid fall in the
pressure during late systole, the so-called “systolic collapse.” This likely relates
to the rapid loss of blood volume into the dilated peripheral vessels and across
the incompetent aortic valve.
Proceed
17-6
17-7
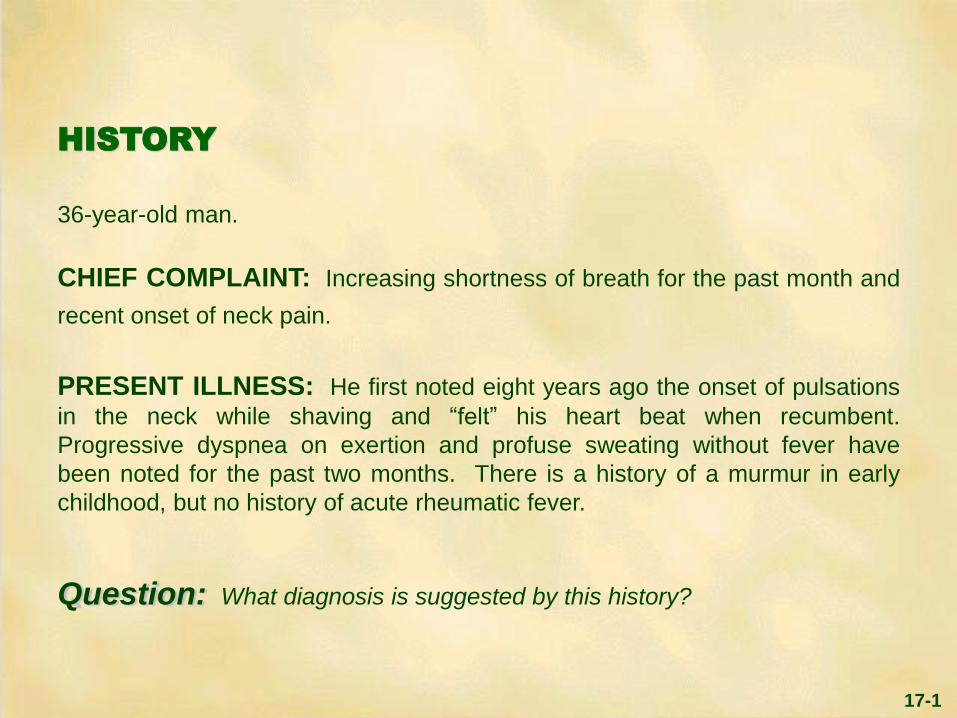
d. PRECORDIAL MOVEMENT and e. CARDIAC AUSCULTATION
Questions: 1. How do you interpret the precordial movement?
2. How do you interpret the acoustic events at the upper right sternal edge?
PHONO
UPPER RIGHT
STERNAL EDGE
ECG
APEXCARDIOGRAM
5TH & 6TH ICS
ANTERIOR
AXILLARY LINE
S1
S2

Answers: 1. The apical impulse is displaced laterally, enlarged, hyperdynamic and non-
sustained. The displacement and enlargement are consistent with a
chronically preloaded left ventricle, as seen in mitral or aortic regurgitation
or PDA. The hyperdynamic non-sustained character of the impulse is due
to an increased stroke volume associated with the increased preload and an
increased velocity of contraction due to the reduced afterload.
2. There is an ejection sound (arrow), a short early systolic crescendo-
decrescendo murmur and a high frequency diastolic decrescendo murmur
at the upper right sternal edge.
Proceed
17-8

Answer (continued): An ejection sound may arise from either a pliable
congenitally abnormal semilunar valve or in association with a dilated great
vessel. The fact that it is heard at the upper right sternal edge makes it
most likely aortic in origin. Aortic ejection sounds, in contrast to pulmonary
ejection sounds, have no respiratory variation, and in some cases may be
heard at the apex.
The short systolic murmur is most likely due to increased flow across a
non-stenotic aortic valve, as it occurs only during maximum ejection, and may
be related to turbulence alone.
A diastolic murmur of high frequency and decrescendo character in this location
is consistent with AR. Auscultation at the mid left sternal edge may help to
further define this murmur.
Proceed
17-9
17-10
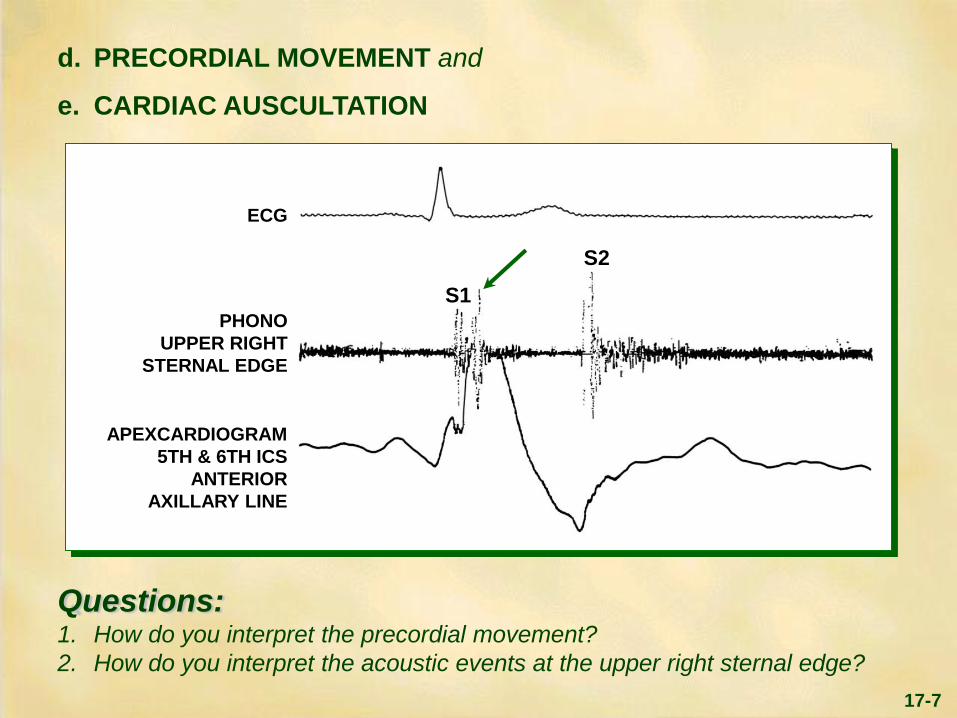
e. CARDIAC AUSCULTATION (continued)
Question: How do you interpret the murmur at the mid left sternal edge?
PHONO
MID LEFT
STERNAL
EDGE
ECG
S1
S2

17-11
The murmur begins with
the aortic sound (A2),
because the aortic root
diastolic pressure exceeds
left ventricular pressure
(LV) diastolic pressure
immediately after the onset
of diastole. The murmur
then diminishes as the
aortic root pressure falls
and left ventricular
pressure rises in diastole.
Answer: There is a high frequency (blowing), early diastolic, decrescendo
murmur consistent with AR. The murmur is typically loudest at the mid left
sternal edge, but may be audible in other areas.
Proceed
AORTA
LV
PHONO
PR
ES
SU
RE
(m
m H
g)
S1 A2
S1

17-12
e. CARDIAC AUSCULATION (continued)
Question: How do you interpret these acoustic events?
PHONO APEX
(Low Frequency)
PHONO
UPPER RIGHT
STERNAL EDGE
(High Frequency)
ECG
S1 S2

Answer: At the apex, the first heart sound is diminished, and there is a low
frequency apical diastolic murmur (arrow) which is either an Austin Flint rumble
secondary to AR, or due to associated mitral stenosis. These findings are also
well heard posterolateral to the mitral area over the enlarged left ventricle.
The Austin Flint murmur is related to the premature closure of the mitral valve.
With severe AR, the left ventricular diastolic pressure rises early and
approaches that of the left atrium causing the mitral valve leaflets to begin to
close prematurely. The velocity and turbulence of diastolic flow through the
reduced mitral valve orifice causes this low frequency murmur of “relative”
mitral stenosis. The reduced intensity of the first heart sound is also explained
by premature mitral valve closure.
The simultaneously recorded phonocardiogram at the upper right sternal edge
helps to correlate the diastolic murmur of aortic regurgitation with the
Austin Flint rumble. The broken arrow denotes the ejection sound
previously described.
f. PULMONARY AUSCULTATION
Question: How do you interpret the acoustic events in the pulmonary lung
fields?
Proceed 17-13

17-14
Answer: In all lung fields, there are normal vesicular breath sounds.
ELECTROCARDIOGRAM
Question: How do you interpret the ECG?
I II III aVR aVL aVF
V1 V2 V3 V4 V5 V6
ALL LEADS 1/2 STANDARD
17-15
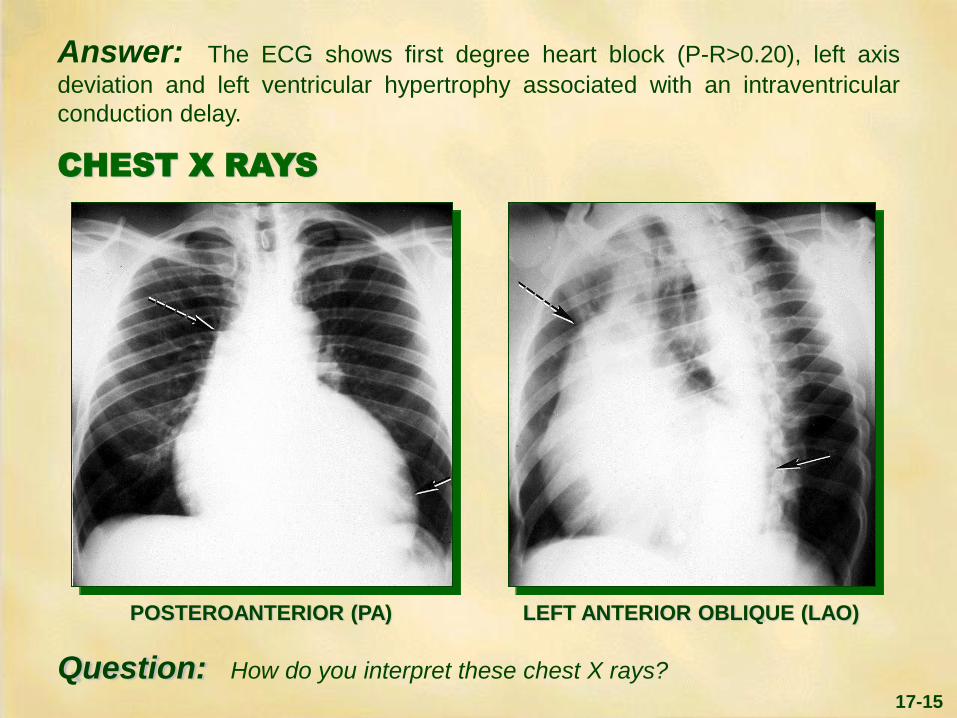
Answer: The ECG shows first degree heart block (P-R>0.20), left axis
deviation and left ventricular hypertrophy associated with an intraventricular
conduction delay.
CHEST X RAYS
Question: How do you interpret these chest X rays?
POSTEROANTERIOR (PA) LEFT ANTERIOR OBLIQUE (LAO)

Answer: In the PA view, the cardiac silhouette is convex or “boot shaped”
(arrow) and extends below the diaphragm. This is typical of a markedly dilated,
inferolaterally displaced left ventricle due to chronic volume overload. Moderate
dilatation of the aortic root (broken arrow) is also consistent with chronic
volume overload.
The findings are confirmed in the LAO view which shows the dilated ventricle
extending beyond the spine (arrow) and the dilated aortic root (broken arrow).
Question: Based on the history, physical examination, ECG and chest
X rays, what is your initial diagnostic impression and plan to further evaluate
this patient?
17-16

Answer: The history, physical examination, ECG and chest X rays are all
consistent with a preloaded left ventricle due to isolated, severe aortic
regurgitation with left ventricular dysfunction. With rheumatic heart disease, the
mitral valve is essentially always involved. Although the exact etiology of the
aortic regurgitation is not definite, the history of a murmur in childhood, the
absence of rheumatic fever and the absence of other valvular involvement
detectable at the bedside, suggest a congenital etiology.
An echocardiogram is likely to further define the cause of the apical murmur
and may define the etiology of the aortic regurgitation. The patient’s
study follows.
Proceed
17-17

17-18
LABORATORY - ECHOCARDIOGRAM
TWO-DIMENSIONAL PARASTERNAL LONG AXIS (Systole)
Question: How do you interpret this echocardiogram?
RV = Right Ventricle
LV = Left Ventricle
Ao = Aorta
LA = Left Atrium

Answer: The two-dimensional echocardiogram shows systolic doming
(arrow), a characteristic of a congenitally malformed aortic valve. The left
ventricle is moderately dilated.
In the real-time study the left ventricle is hyperkinetic, the aortic valve bicuspid,
and the mitral valve structurally normal.
Proceed
17-19

17-20
LABORATORY (continued) A color Doppler flow study clearly demonstrates the jet of aortic regurgitation
(arrow) as shown below.
The configuration of the jet suggests that the regurgitation is
moderately severe.
Proceed
RV = Right Ventricle
LV = Left Ventricle
Ao = Aorta
LA = Left Atrium
MV = Mitral Valve
PARASTERNAL LONG AXIS (DIASTOLE)

The echocardiographic studies support the clinical diagnosis of isolated severe
AR due to a congenitally bicuspid aortic valve.
In the presence of isolated AR, a dilated hyperkinetic left ventricle is virtually
diagnostic of chronic AR.
Question: How would you treat this patient?
17-21

Answer: The patient was treated with salt restriction, digitalis, diuretics and
a vasodilator to reduce afterload. He improved significantly, but still had mild
dyspnea and cardiomegaly. Because of this and his bedside findings of severe
AR, he is a candidate for valve replacement.
While catheterization is not mandatory, it will confirm the diagnosis, assess left
ventricular function and define the anatomy of the coronary arteries.
Proceed
17-22

17-23
LABORATORY (continued) - CARDIAC CATHETERIZATION
Question: How do you interpret the above data?
ADDITIONAL DATA:
No gradient across the
mitral valve.
Cardiac Index =
2.2 L/Min/M2
LV = Left Ventricle
AO = Aorta
ECG
INTRA AORTIC PHONO
INTRA VENTRICULAR PHONO
AO
LV
mm
Hg
0
100
200

Answer: There is a wide pulse pressure (110 mm Hg), typical of severe AR.
There is no significant systolic gradient across the aortic valve, confirming the
clinical impression that the systolic murmur was due to increased flow alone.
The left ventricular end-diastolic pressure is increased (30 mm Hg) and the
cardiac index is reduced (normal = 2.5-4.0 L/Min/M2), reflecting a decrease in
left ventricular function.
The intraaortic phonocardiogram shows systolic and diastolic murmurs, while
the intraventricular phonocardiogram shows only a diastolic murmur and
correlates exactly with the bedside examination.
Proceed
17-24

17-25
LABORATORY (continued)
AORTIC ROOT ANGIOGRAM
ADDITIONAL DATA:
The coronary
arteriograms were
normal. Left ventricular
injection showed no
mitral regurgitation.
Ao = Aorta
LV = Left Ventricle
Question: How do you interpret the angiograms?
PA LATERAL

Answer: In both the PA and lateral views, injection of dye into the aortic
root results in marked opacification of the left ventricle, reflecting severe aortic
regurgitation. The ventricle and ascending aorta are dilated.
Based on the clinical and laboratory evaluation, the patient underwent
prosthetic aortic valve replacement. His postoperative course was uneventful
and he improved markedly.
Proceed for Summary
17-26

SUMMARY
Aortic regurgitation can be secondary to intrinsic aortic valve disease
(e.g., rheumatic, infectious, congenital, traumatic) or aortic root disease (e.g.,
syphilis, cystic medial necrosis, aortic dissection, ankylosing spondylitis).
When the etiology is rheumatic, the mitral valve is nearly always involved.
A congenital bicuspid aortic valve may leak because the two cusps are unequal
in size, with the larger cusp prolapsing into the left ventricle during diastole.
Fibrosis and calcification often occur over a period of years, resulting in a rigid
structure associated with both stenosis and regurgitation.
Left ventricular volume overload is the basic hemodynamic abnormality. The
compensatory response of the left ventricle is hypertrophy and dilation. The left
ventricle is able to tolerate significant volume overload for years prior to
decompensation.
Proceed
17-27

SUMMARY(continued)
The peripheral manifestations of AR related to the wide pulse pressure have
been described with a variety of eponyms:
Corrigan’s pulse = abruptly rising and falling pulsations (or Waterhammer) de Musset’s sign = rhythmical nodding of the head synchronous with each
heart beat Quincke’s sign = alternate reddening and blanching of the nail bed when the
tip of the nail bed is slightly compressed Duroziez’s murmur = biphasic to and fro bruit detected by mild pressure of
the stethoscope over the femoral artery Hill’s sign = disproportionate femoral systolic hypertension detected by leg
blood pressure Pistol shots = sharp, high frequency systolic sounds, analogous to Korotkoff
sounds, heard over the peripheral arteries
Proceed
17-28

SUMMARY(continued)
Endocarditis prophylaxis is mandatory in AR, since infection of the deformed
valve is the most important factor in producing sudden deterioration. Proper
timing of surgery is essential.
Patients with mild AR may have a long and uncomplicated course with normal
life expectancy. Those with a wide pulse pressure, those with moderate to
severe left ventricular enlargement by echocardiography and those with
decrements in left ventricular function should be considered for surgery. The
onset of angina pectoris or symptoms of left ventricular failure are indications
for further evaluation.
The goal of management is to operate before irreversible deterioration in
ventricular function occurs.
Proceed
17-29

17-30
PATHOLOGY
Specimen of a bicuspid aortic valve associated in life with aortic regurgitation.
Proceed for Case Review
RAPHE
OSITA Right Coronary Artery and Accessory Vessel
COMMISSURE ( )
OSTIUM
LEFT
CORONARY
ARTERY
LEFT
VENTRICLE
AORTIC
CUSPS
(Pliable,
non-
calcified)

17-31
To Review This Case of
Isolated Congenital Aortic Regurgitation:
The HISTORY is typical, including a murmur in childhood and the later
onset of prominent arterial pulsations and left ventricular failure. Additional
features include neck pain and diaphoresis.
PHYSICAL SIGNS
a. The GENERAL APPEARANCE reveals a mildly dyspneic man in his
mid 30’s.
b. The JUGULAR VENOUS PULSE mean pressure and wave form
are normal.
c. The CAROTID PULSE is bisferiens and the pulse pressure is wide,
reflecting increased stroke volume and rapid diastolic runoff.
Proceed

17-32
d. PRECORDIAL MOVEMENT is hyperdynamic and inferolaterally
displaced, consistent with a preloaded left ventricle.
e. CARDIAC AUSCULTATION reveals the characteristic features of chronic
AR:
1) The diastolic decrescendo murmur of AR;
2) The basilar systolic crescendo-decrescendo murmur secondary to
increased flow across the aortic valve;
3) The apical diastolic Austin Flint rumble and diminished first sound due
to premature closure of the mitral valve that are also well heard
posterolateral to the mitral area over the enlarged left ventricle.
4) An ejection click characteristic of a bicuspid aortic valve.
A fourth murmur, not present in this case, and due to mitral regurgitation
associated with dysfunction of the mitral apparatus from left ventricular
dilation, may occasionally be heard.
f. PULMONARY AUSCULTATION reveals normal vesicular breath sounds
in all lung fields.
Proceed

The ELECTROCARDIOGRAM shows first degree heart block, left
axis deviation, an intraventricular conduction delay and left ventricular
hypertrophy, reflecting the chronically volume loaded left ventricle.
The CHEST X RAY also reflects chronic volume overload, with marked
left ventricular enlargement and mild aortic root enlargement.
LABORATORY STUDIES include echo Doppler showing a
congenitally abnormal aortic valve associated with severe AR. Catheterization
and angiography show isolated AR of severe degree, normal coronary arteries
and evidence of left ventricular failure.
TREATMENT is aortic valve replacement.
17-33