Embed Size (px)
Citation preview

JOURNAL OF CLINICAL MICROBIOLOGY,0095-1137/00/$04.0010
July 2000, p. 2655–2660 Vol. 38, No. 7
Copyright © 2000, American Society for Microbiology. All Rights Reserved.
No Evidence of Measles Virus in Stapes Samples from Patientswith Otosclerosis
ALEXIS BOZORG GRAYELI,1* PIERRE PALMER,2 PATRICE TRAN BA HUY,3 JACQUES SOUDANT,4
OLIVIER STERKERS,5 PIERRE LEBON,2 AND EVELYNE FERRARY1
INSERM U.426, Faculte Xavier Bichat, Universite Paris 71; Virology Department, Hopital Saint-Vincent-de-Paul, AP-HP,Universite Paris 52; Otolaryngology Department, Hopital Lariboisiere, AP-HP, Paris3; ENT Department, Hopital
Pitie-Salpetriere, AP-HP, Paris4; and ENT Department, Hopital Beaujon, AP-HP, Clichy,5 France
Received 25 October 1999/Returned for modification 28 December 1999/Accepted 1 May 2000
Otosclerosis is a localized bone dystrophy of unknown etiology mainly involving the stapes. The hypothesisof a persistent infection by the measles virus was based on the inconstant detection of the virus by various meth-ods, including reverse transcription-PCR (RT-PCR) of patients’ stapes samples. The aim of this work was toinvestigate the presence of the measles virus in stapedial otosclerosis foci by different sensitive methods. Patho-logic stapes samples were obtained from 35 patients suffering from otosclerosis. Measles virus detection wasperformed by (i) cocultures of Vero cells and primary cell cultures of bone samples (n 5 7), (ii) immunoflu-orescence study of these cocultures (n 5 3), and (iii) RT-PCR on RNA directly obtained from fresh frozensamples (n 5 28) and on RNA extracted from the primary cell cultures (n 5 2). Viral genomic regions codingfor N (nucleoprotein) and M (matrix) proteins were separately amplified. PCR sensitivity was optimized on themeasles virus Edmonston strain. Glyceraldehyde-3-phosphate dehydrogenase mRNA was used as a marker oftotal RNA recovery. PCR products were tested by Southern blot hybridization technique to improve sensitivityand specificity. PCRs amplifying the M and the N protein genes were able to detect the control measles virusRNA at titers as low as 0.1 and 0.01 50% tissue culture infective dose, respectively. With these highly sensitivemethods, we could not evidence the presence of the measles virus in any of our bone samples or primary bonecell cultures. Our results do not confirm the hypothesis of persistent measles virus infection in otosclerosis.
Otosclerosis is a bone dystrophy localized to the otic capsule,an embryonic structure from which develop the inner ear andthe stapes footplate (9). This disease is a frequent cause ofdeafness in adults, affecting over 10% of deaf adult patientsseen in outpatient activity by otolaryngologists in the UnitedStates (9). Its prevalence is estimated at 0.2 to 0.3% of thepopulation in western Europe and North America (9). About10% of Caucasian adult temporal bones present histologicotosclerosis foci (12). In the early forms, otosclerosis foci arefound only in the stapes and disturb sound transmission, whileadvanced lesions can involve the cochlea, producing sensori-neural hearing loss, or the vestibule, causing vertigo (9, 11).The otosclerosis process in the otic capsule is initiated by anincrease in bone resorption with the presence of numerousresorption foci rich in blood vessels, also designated otospon-giotic foci (11, 27). In response to this increase in bone resorp-tion, a reconstruction phase conducted by numerous osteo-blasts present in otosclerotic tissue leads to fibrous bone foci(11, 27). These lesions showing a high bone turnover are sim-ilar to those observed in Paget’s disease (27). Although theclinical signs and the histologic aspects of otosclerosis arewidely described (9, 12, 27), the pathogenesis of this diseaseremains unclear, and many hypotheses, including autoimmuneand viral origins, have been advanced (1, 2, 4, 15–17, 31).
The hypothesis of persistent measles virus infection in oto-sclerosis has been advanced by some authors based on electronmicroscopy observations (15), immunohistologic studies (2, 16,26), and reverse transcription (RT) followed by PCR results (1,4, 17–19). However, these studies demonstrated the presence
of different viruses in some cases (16, 26), and did not providereproducible data in order to confirm the implication of themeasles virus in otosclerosis foci (1, 4, 17–19). Moreover, themajority of RT-PCR studies were realized on a small numberof patients, ranging from 9 to 14 (17–19). Considering the lackof conclusive evidence in favor of this hypothesis, the aim ofour study was to detect the presence of the measles virus infresh otosclerotic samples in a large population (n 5 35) usinghighly sensitive methods.
MATERIALS AND METHODS
Patients. The population was composed of 16 males and 19 females. The meanage was 42 years (range, 27 to 61). All patients presented normal tympanicmembrane on otoscopy and progressive conductive hearing loss associated withabsent stapedial reflex on preoperative audiometry. Preoperative clinical, audio-metric, and imaging data were obtained from medical files. The diagnosis ofotosclerosis was confirmed during surgery by the aspect of the stapes and itsimmobility. The extent of the disease was assessed during surgery and classifiedin five stages (23): I, stapedial ankylosis with normal aspect; II, stapedial foot-plate involvement in its anterior or posterior part; III, stapedial footplate bipolarinvolvement; IV, stapedial footplate entire involvement; and V, total obstructionof the oval window by otosclerosis. During surgery, the involved stapes’ footplateand the superstructure were removed in 24 cases (69%), and only the pathologicsuperstructure was obtained in 11 cases (31%). The approval of the ethicscommittee and the patients’ consent were obtained for these samplings.
Cell cultures. Stapedial bone fragments were placed in 10-cm2 culture platesin a culture medium composed of Dulbecco’s minimal essential medium (MEM)with 4.5% glucose (Gibco-BRL Life Technologies, Cergy-Pontoise, France) con-taining vancomycin (12.5 mg/liter) (Lilly, Saint-Cloud, France) and 30% fetal calfserum in a humidified atmosphere of 95% air and 5% CO2 at 37°C. Vancomycinwas used to prevent the infection of the culture medium by cutaneous saprophytebacteria. In fact, the middle ear was approached through the external auditorycanal for these samplings, and the samples were frequently in contact with theskin. During culture, cells migrated from bone explants, and maximal cellulargrowth from the explants was obtained in about 21 days, at which time cells weretrypsinized, plated homogeneously on the culture surface, and allowed to grow toconfluence for 14 to 21 additional days in contact with the explants. At conflu-ence, cells were trypsinized and counted. Half of the cells were used for cocul-tures with Vero cells (African green monkey renal cells), and the other half were
* Corresponding author. Mailing address: INSERM U.426, Facultede Medecine Xavier Bichat, 16, rue Henri Huchard, 75018 Paris,France. Phone: 33 (0) 1-44-85-62-73. Fax: 33 (0) 1-42-28-15-64. E-mail:[email protected].
2655
on October 26, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

replated in three 10-cm2 culture wells and used for RNA extraction at conflu-ence. This stage was defined as the first passage.
Cells obtained from the primary stapes cultures at confluence were mixed 1:1with a suspension of Vero cells and replated in 2.5-cm2 wells in the presence ofDulbecco’s MEM plus 10% fetal calf serum, 5 mM glutamine, 250 IU of peni-cillin per ml, and 80 mg of gentamicin per ml. The cocultures was observed for3 weeks.
Immunofluorescence assays were performed on cocultures obtained fromthree patients (patients 1 to 3) using anti-measles virus monoclonal antibody(Biosys, Compiegne, France) and a mixture of monoclonal antibodies againstparainfluenzae viruses 1, 2, and 3, adenovirus, and respiratory syncytial virus(Sanofi-Pasteur, Paris, France) on separate slides for each sample. Mouse mono-clonal antibodies were used as the primary antibodies, and polyclonal goatanti-mouse immunoglobulin antibody conjugated with fluorescein isothiocyanatewas used as the conjugated antibody (Sanofi-Pasteur). Cocultures were preparedin duplicate on slides and allowed to grow to confluence for 7 days. At this stage,cells were fixed with 90% acetone for 10 min at 4°C and dried. Slides weresubsequently incubated with primary antibodies diluted 1:10 to 1:20 in phos-phate-buffered saline (PBS) solution for 30 min at 37°C, washed three times withPBS, and incubated with the conjugated antibody for 30 min at 37°C. Finally,slides were washed three times with PBS and observed under a fluorescencemicroscope.
RNA extraction, RT-PCR, and Southern blot assays. To extract total RNAfrom bone fragments obtained from patients 8 to 35, the bone fragments werecrushed in 1 ml of lysis buffer (guanidium thiocyanate, 4 M; sodium citrate, 25mM [pH 7.0]; N-laurylsarcosine, 0.5%; b-mercaptoethanol, 0.1 M) using a Poly-tron. RNA was then extracted using phenol-water and isoamyl alcohol-chloro-form (1:24, vol/vol) and precipitated with isopropranol (7). The pellet was re-suspended in 20 ml of nuclease-free water and used for RT. For RNA extractionfrom the first-passage primary cell cultures (patients 1 and 2), cells were lysed ina similar lysis buffer using a cell lifter, samples were processed as describedabove, and the pellet was suspended in 50 ml of water. RNA solution was heatedat 95°C for 3 min and cooled to 4°C before RT.
Synthesis of cDNA was performed in reverse transcriptase buffer (50 mMTris-HCl, [pH 8.4], 40 mM NaCl, 10 mM dithiothreitol, 6 mM MgCl2) containingeach triphosphate deoxynucleoside (dNTP) at 250 mM, 20 U of RNasin (Pro-mega, Charbonnieres, France), random hexamer at 2.5 mM, 10 U of avianmyeloblastosis virus reverse transcriptase (Promega), and 10 ml of the RNAsolution in a total volume of 20 ml. The reaction mix was incubated for 10 min atroom temperature, followed by 45 min at 42°C, and finally heated at 95°C for 5min.
cDNA amplification of the measles virus genome was performed in two sep-arate regions, one coding for the matrix protein (M protein) and the other codingfor the nucleoprotein (N protein). Optimal PCR conditions, including MgCl2concentration, annealing temperatures, and the effect of different additives (for-mamide and glycerol), were determined in preliminary experiments.
Sequence alignments between several reported strains responsible for acuteand persistent infections permitted verification of the conservation of the targetsequences. The M protein gene was amplified by a single-step PCR, using theoligonucleotide pair designated MVO3/MVO5 already described (28). This PCRyielded a DNA fragment of 414 bp (Table 1). The N protein gene was amplifiedby a nested PCR using two oligonucleotide pairs, designated MVNP1/MVNP2and MVNP3/MVNP4. The pair MVNP1/MVNP2 amplified a 284-bp DNA frag-ment, and the internal pair MVNP3/MVNP4 gave a final product of 125 bp
(Table 1). A 784-bp fragment of glyceraldehyde-3-phosphate dehydrogenase(GAPDH) cDNA was amplified using a pair of oligonucleotides designated 10/11(Table 1).
For PCR, 6 ml of cDNA was added to 44 ml of an amplification mix containing10 mM Tris-HCl (pH 8.4), 50 mM KCl, 1.5 mM MgCl2 (for M protein gene andGAPDH) or 2 mM MgCl2 (for N protein gene), 50 mM each of the four dNTPs,each primer at 0.5 mM (MVO3/MVO5 and 10/11) or 1 mM (MVNP1 to 4) finalconcentrations, and 1.5 U of Taq DNA polymerase (Boehringer-Mannheim,Meylan, France). After an initial denaturation step at 94°C for 3 min, the cDNAwas amplified by 40 cycles of heating at 94°C for 15 s, annealing at 55°C (Mprotein gene), 58°C (N protein gene), or 60°C (GAPDH cDNA) for 15 s, andpolymerization at 72°C for 15 s. The reaction was ended by an elongation step at72°C for 5 min. The specific DNA band was detected by 2% agarose gel elec-trophoresis containing ethidium bromide.
Five microliters of the PCR product obtained with the MVNP1/MVNP2 pairwas subjected to 35 cycles of further amplification with the MVNP3/MVNP4internal pair in the conditions described above.
The specificity of the reaction was confirmed by Southern blot hybridizationusing digoxigenin-labeled oligonucleotide MVO4 for the M protein gene PCRproducts and MVNP3 for the N protein gene first-step PCR products. Afterdenaturation (0.4 N NaOH, 30 min), the gel was blotted by capillarity on apositively charged membrane (Hybond N1; Amersham, Les Ulis, France). Themembrane was hybridized overnight with the labeled probe at 37°C in a hybrid-ization buffer containing 53 SSC (13 SSC is 0.15 M NaCl plus 0.015 M sodiumcitrate), 0.02% sodium dodecyl sulfate (SDS), 0.1% N-laurylsarcosin, 2% block-ing reagent, and 10% formamide. The filters were washed twice with 0.1%(wt/vol) SDS in 23 SSC at 42°C for 15 min, followed by two washes in 0.13 SSCplus 0.1% SDS at 42°C for 15 min. Antidigoxigenin Fab fragments conjugatedwith alkaline phosphatase were incubated with the membrane for 30 min beforewashing and revelation by an enzyme-catalyzed color reaction with nitrobluetetrazolium (NTB)–5-bromo-4-chloro-3-indolylphosphate (BCIP) as the sub-strate. The entire procedure (labeling and detection) was performed according tothe manufacturer’s instructions (Boehringer-Mannheim).
Positive and negative controls were inserted in every PCR run, and theirresults were as expected. The sensitivity of the PCR detection method wasevaluated on dilution series of the Edmonston virus strain. Titration of the viralinfectivity of this strain was performed by culture in Vero cells and was expressedas 50% tissue culture-infective dose (TCID50). In order to decrease the numberof noninfectious particles, the viral stock was prepared from Vero cells with a lowmultiplicity of infection (>0.1 TCID50/Vero cell). In these conditions, the ratioof TCID50 to defective particles is generally estimated to be 0.1 to 0.01 (10).RNA from a human osteoblastic cell line (SaOS-2) was used as positive controlfor the GAPDH RT-PCR assessment. The specificity of the PCR and the South-ern blot assays was evaluated by using other different viral samples, such asparainfluenza viruses, respiratory syncytial virus, cytomegalovirus, and Epstein-Barr virus.
RESULTS
Clinical, audiometric, and imaging data. Clinical and audio-metric data were obtained for all 35 patients. Otosclerosisinvolved both ears in 21 patients (61%) and was unilateral in14 cases (39%). The disease appeared as sporadic in 30 cases(87%), while other family members were reported to be suf-fering from otosclerosis in 5 cases (13%). The mean intervalbetween the onset of symptoms and surgery was 65 months(range, 6 to 204 months). Vestibular signs such as imbalanceand episodic vertigo were reported in three cases (9%). Twentypatients (57%) presented with pure conductive hearing loss,and the remaining 15 patients (43%) suffered from mixedconductive and sensorineural hearing loss. The mean air con-duction hearing loss measured on pure-tone audiometry onfrequencies ranging from 125 to 8,000 Hz was 50 dB (range, 40to 70 dB), and the mean bone conduction hearing loss onfrequencies ranging from 250 to 4,000 Hz was 16 dB (range, 5to 35 dB). Preoperative temporal bone computed tomographyscans were obtained in 11 cases (31%). Among these patients,lytic foci in the anterior part of the oval window (fissula antefenestram) were observed in four cases (36%), bilateral lyticfoci extending to the perilabyrinthine bone were evidenced inthree cases (27%), and a normal bone aspect was noted in fourcases (36%).
The extent of the otosclerotic foci was evaluated duringsurgery as stage II (anterior or posterior footplate involve-ment) in 11 patients (31%), stage III (bipolar footplate in-
TABLE 1. Sequences and positions of the oligonucleotides used formeasles virus and GAPDH cDNA amplification
and Southern blot analysisa
Geneamplified Primer 59 posi-
tion 59339 sequence
Measles virusM protein MVO3 499 GTG TTG TTT ATA TGA GCA TCA C
MVO5 913 AAT CGA TTA AGG TCT TCA TTG ATMVO4 727 CAT TTT GCA ATA ATC GGC AGA GT
N protein MVNP1 719 TCA AGA GAA CAC CCG GAA ACMVNP2 1003 GCT CCA GAG CAG AGG GTA TGMVNP3 740 AAC CCA GGA TTG CTG AAA TGMVNP4 865 TTC ATG CAG TTC AAG AGC AG
GAPDH 10 378 AAG GCT GGG GCT CAT TTG11 1162 GTG TGG TGG GGG ACT GAG
a Reverse primers are shown in bold. The pair MVO3/MVO5 was used toperform the RT-PCR amplification of the matrix protein (M protein) gene. Thepairs MVNP1/MVNP2 and MVNP3/MVNP4 were used for the first and thesecond steps of the nested PCR amplifying the viral nucleoprotein (N protein)gene, respectively. Oligonucleotides MVO4 and MVNP3 were used for thehybridization step. The positions on the M protein cDNA sequence for MVO3-5(8) and on the N protein cDNA sequence for MVNP1-4 (22) are shown.
2656 GRAYELI ET AL. J. CLIN. MICROBIOL.
on October 26, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

volvement) in 13 patients (37%), and stage IV (entire footplateinvolvement) in 11 patients (31%). Stages I and V of otoscle-rosis extension were not observed in this series.
Primary cell cultures. Primary cell cultures and cocultureswith Vero cells were performed for patients 1 to 7. Pathologicstapes samples in these cases comprised both the superstruc-ture and the footplate.
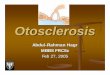
In the primary cell cultures (Fig. 1), cells grew in a centrif-ugal manner from the explants. In bone cell cultures at con-fluence, numerous mineralization foci surrounded by polygo-nal plump cells resembling osteoblasts were observed. Nomorphologic signs of measles virus infection, such as syncytiumformation, fuzzy cytoplasmic inclusions, or stellate and den-dritic cells already described in vitro (5) could be seen in thesefirst-passage primary cell cultures.
Cocultures with Vero cells performed for patients 1 to 7followed by an observation period of 3 weeks did not evidenceany cytopathic effect such as syncytium formation (data notshown). Immunofluorescence assays on cocultures performedon patients 1 to 3 did not reveal the presence of measles virus,parainfluenza viruses 1, 2, and 3, adenovirus, and respiratorysyncytial virus antigens in any of the cocultures tested (data notshown).
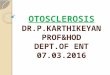
Viral genomic material detection. The single-step PCR am-plifying the M protein cDNA from a measles virus RNA ex-tract containing 1 TCID50 showed a signal of the expected size(414 bp). The nested PCR amplifying the N protein cDNAfrom a measles virus RNA extract containing 0.01 TCID50 alsoshowed a signal of the expected size (125 bp) (Fig. 2A). South-ern blot on M protein PCR and the N protein first-step PCRproducts both yielded a sensitivity of 0.1 TCID50 on titratedcontrol virus samples (Fig. 2B). No signal could be detectedwith respiratory syncytial virus, parainfluenza viruses, Epstein-Barr virus, or cytomegalovirus.
RT-PCR assays were performed on RNA directly extractedfrom the bone samples in 28 cases (patients 8 to 35) and on
RNA extracted from first-passage primary cell cultures in twosamples (patients 1 and 2). The RT-PCR amplifying GAPDHwas performed in all 30 cases (Fig. 3). A GAPDH signal of theexpected size (784 bp) could be evidenced on the agarose gelin 22 of 30 samples (73%) (patients 1, 2, and 8 to 27). None ofthe 30 otosclerotic samples tested in parallel for the M and Nproteins showed a signal of the expected size on the agarose gel(Fig. 3). The Southern blot assays did not detect any specificPCR product in the 30 otosclerotic samples tested (Fig. 3).
DISCUSSION
The hypothesis of persistent measles virus infection in oto-sclerosis is mainly based on RT-PCR studies (1, 4, 16, 19). Ourobservations in stapedial otosclerotic samples using Vero cellcocultures, immunofluorescence, and sensitive RT-PCR meth-ods did not detect the measles virus in the otosclerotic foci.
Clinical, audiometric, and imaging data for our populationwere consistent with ongoing otosclerosis in all cases, and thedisease was extensive (stage IV lesions and associated senso-rineural hearing loss) and highly active (lytic foci on computedtomographic scan) in more than one third of the patients.
Vero cell cocultures did not show any cytopathic effect dur-ing the 3-week observation period in our study. Although thismethod represents a sensitive routine method for the diagnosisof acute measles virus infections (20) and is a preferred meansof isolating defective virus in subacute sclerosing panencepha-litis brain samples (20), the absence of cytopathic effect alonecould not eliminate the possibility of an infection by either adefective virus or a virus present at low titers (20). The immu-nofluorescence was used to enhance the sensitivity and speci-ficity of viral detection in the cocultures. This technique did notreveal any viral antigen in our cocultures, but immunofluores-cence may also yield negative results for a defective virus (20).
Consequently, in addition to these methods, samples wereassessed by RT-PCR. Two different genomic regions coding
FIG. 1. Representative stapes bone cell culture at confluence.
VOL. 38, 2000 NO EVIDENCE OF MEASLES VIRUS IN OTOSCLEROSIS 2657
on October 26, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

for the M and the N proteins, which are highly conservedamong characterized strains responsible for acute and persis-tent measles virus infection, were chosen for the RT-PCRassays (6, 28). The RT-PCR amplifying the M protein gene hadalready demonstrated its high sensitivity in clinical samples(28). However, since N protein mRNA is reported to be moreabundant and less prone to mutations in persistent infection(6), samples were also subjected to RT-PCR to amplify thisregion. This amplification yielded high sensitivity levels interms of TCID50. The recovery of total RNA from the bonesamples or the cell cultures was verified by GAPDH mRNAdetection. Although maximal precaution was employed in thehandling of the samples for RNA conservation, GAPDHmRNA could not be detected in some samples (8 of 30). Thisis probably related to the low cellular content of the samples,since their volumes did not exceed a few tenths of a cubicmillimeter. In a different series, including more than 50 sam-ples of similar size obtained in similar technical conditions, weobtained primary cell cultures in all cases (unpublished data).This observation indicates that all the samples contain viablecellular material. Although maximal precaution was employedin this study to avoid RNA degradation, another possible fac-tor explaining negative GAPDH detection is spontaneousRNA degradation. Finally, insufficient sensitivity of GAPDHdetection may also explain this negative result. By amplifying arelatively long cDNA fragment (784 bp), we aimed to verify thepresence of nonfragmented RNA in our samples, and theGAPDH RT-PCR sensitivity could probably be enhanced bychoosing a smaller cDNA fragment to amplify. Consequently,the negative GAPDH mRNA detection in some samples doesnot completely invalidate the measles virus detection results,and in the majority of our samples the presence of a GAPDHsignal associated with a negative RT-PCR for the measles virus
N and M proteins constitutes a solid argument in favor of theabsence of the virus in otosclerotic foci.
Measles virus genomic material was previously detected inotosclerotic stapes samples by RT-PCR methods, but method-ological limitations prevented definitive conclusions in thesestudies (1, 4, 17–19). Indeed, these positive results have beenexclusively reported by two groups which have amplified the Nprotein gene in otosclerotic stapedial samples using a highnumber of amplification cycles (two steps of 35 and 40 cycles)(4, 17–19). McKenna et al. (17) evaluated 12 otosclerotic and10 normal stapedial postmortem archival samples. They em-ployed a nested PCR with two amplification sets of 35 and 40cycles. The tests were repeated three times for each sample. Atleast one positive test out of three was observed in 30% ofcontrol samples versus 92% of pathologic samples. Addition-ally, the reproducibility of the tests seemed low, since only 25%of pathologic samples had three positive tests. Arnold andNiedermeyer et al. (4, 18, 19) reported a similar proportion ofpositive tests by performing a similar RT-PCR method in freshfrozen samples. They amplified the N protein gene by RT-PCRincluding two amplification steps of 35 cycles each. Primersused for the cDNA synthesis and the PCR amplification of theviral mRNA sequences were the same in their three reports (4,18, 19). These authors observed 44, 93, and 83% of positivetests in series of 9, 14, and 29 otosclerotic patients, respectively.Each series comprised only two control samples for which thetests were negative. The specificity of the final PCR productwas tested by Southern blot assays. In these studies, the smallnumber of control cases does not permit any conclusion con-cerning the relationship between the presence of the measlesvirus and otosclerosis in the studied population.
Data concerning anti-measles virus immune status were notavailable for our population, but considering the high inci-
FIG. 2. RT-PCR and Southern blot sensitivity assessments. (A) RT-PCR amplification of the measles virus nucleoprotein (N protein) and matrix protein (Mprotein) in serial dilution of an Edmonston strain measles virus solution of known titer. PCR products underwent electrophoresis on a 2% agarose gel containingethidium bromide and were visualized under UV light. The expected lengths in base pairs are indicated for each PCR product. The corresponding titers are indicatedin TCID50. (B) Southern blot membranes containing N protein gene first-step PCR and M protein gene PCR products from serial dilution of the control measles virussolution. Corresponding titers are indicated in TCID50 for each lane. Note that for protein M, Southern blot detection was positive at 0.1 TCID50, while the PCR wasnegative at the same titer.
2658 GRAYELI ET AL. J. CLIN. MICROBIOL.
on October 26, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

dence of this infection in France, which is estimated at 300,000to 500,000 annual cases (21), the majority of our patients haveprobably encountered the virus during childhood.
In any case, data on the anti-measles virus immune status ofour patients could not support the hypothesis of a local per-sistent measles virus infection. On one hand, if otosclerosisoccurred in patients who have never encountered the virus, thiswould work against the hypothesis of persistent measles virusinfection in otosclerosis. On the other hand, similar conclu-sions can be reached from the fact that we did not detect thevirus in stapes samples from patients having a history of mea-sles virus infection.
A persistent infection by measles virus has been advanced inmany chronic diseases with an inflammatory component, suchas multiple sclerosis, Paget’s disease, and Crohn’s disease (24).However, in these cases, the detection of the virus has beeninconstant and nonreproducible by different authors (24). Thehigh incidence of acute infections by viruses such as herpessimplex virus and measles virus in the general population andthe persistence of these viruses in different organs, includingthe inner ear (3, 13, 14), in normal individuals hamper theestablishment of a causal relationship between the presence ofthe virus and the chronic disease. Consequently, the responsi-bility of measles virus for these pathologic processes remainscontroversial (24).
To explain the implication of a virus in such pathologies inspite of its inconstant detection, the hypothesis of a “hit andrun” mechanism has been advanced (29). According to thishypothesis, some viruses, such as enterovirus in diabetes mel-litus, have the capacity to trigger pathologic processes which
can develop in a chronic course after elimination of the viruswith the participation of an autoimmune process (29). Thishypothesis may be speculated to occur in otosclerosis, whichdevelops in patients between 30 and 50 years old (10) who haveprobably encountered the virus during childhood, as in thegeneral population (5, 21). In addition, autoimmunity has beensuspected to play a possible role in triggering otosclerosis le-sions (31).
Another common trait of the above-mentioned diseases isthe presence of predisposing genetic factors (22). Otosclerosishas a hereditary character in about 50% of cases (9). Recently,a locus designated Otosclerosis 1 has been identified on chro-mosome 15q25-q26 by linkage dysequilibrium mapping (30).The most important candidate gene reported in this locuscodes for “aggrecan,” an important component of the cartilagematrix, from which develops the stapes footplate during theembryonic phase (30). Although the nature of the triggeringevent in otosclerosis remains unknown, it appears to act on acomplex genetic background.
In conclusion, with highly sensitive methods, measles viruscould not be detected in a large number of otosclerotic sam-ples. This observation does not confirm the hypothesis of per-sistent measles virus infection in the pathogenesis of otoscle-rosis.
ACKNOWLEDGMENTS
Alexis Bozorg Grayeli was the recipient of a research grant fromSynthelabo, Meudon-la-Foret, France, for this work.
This study was supported by INSERM, Faculte Xavier Bichat, Uni-versite Paris 7, and Assistance Publique—Hopitaux de Paris, France.
FIG. 3. Measles virus RT-PCR and Southern blot assessment of 10 stapes samples from patients with otosclerosis. Patient numbers are indicated above each lane(patients 17 to 26). The expected lengths in base pairs are indicated for each PCR product. Electrophoresis on agarose gels containing RT-PCR products of the measlesvirus nucleocapsid protein (N protein) gene after the first-step amplification and matrix protein (M protein) gene after a single-step amplification are shown for 10representative patients. Two positive controls (1) were used at 1 and 0.1 TCID50 titers for the RT-PCR and the Southern blot assays. Their detection was as expectedaccording to the sensitivity assessment. Lanes (—), negative controls. A human osteoblastic cell line (SaOS-2) RNA was used as positive control for GAPDHassessment. Southern blot membranes for N protein gene PCR product after the first-step amplification and M protein gene PCR product are represented under thecorresponding agarose gels. The GAPDH RT-PCR assessment was used as a control for total RNA recovery. Agarose gels containing the GAPDH RT-PCR productsfor the same samples are shown in the lower part of the figure.
VOL. 38, 2000 NO EVIDENCE OF MEASLES VIRUS IN OTOSCLEROSIS 2659
on October 26, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

REFERENCES
1. Arnold, W., and I. Freidmann. 1988. Otosclerosis—an inflammatory diseaseof the otic capsule of viral etiology? J. Laryngol. Otol. 102:865–871.
2. Arnold, W., I. Friedmann, and H. J. Altermatt. Immunohistochemistry ofotosclerosis, p. 21–24. In R. Filipo (ed.), Otosclerosis: proceedings of theinternational workshop on otosclerosis. Kugler and Ghedini Co., Amster-dam, The Netherlands.
3. Arnold, W., and H. P. Niedermeyer. 1997. Herpes simplex antibodies in theperilymph of patients with Meniere’s disease. Arch. Otolaryngol. Head NeckSurg. 123:53–56.
4. Arnold, W., H. P. Nierdermeyer, N. Lehn, W. Neubert, and H. Hofler. 1996.Measles virus in otosclerosis and the specific immune response of the innerear. Acta Otolaryngol. (Stockholm) 116:705–709.
5. Bellini, W. J., J. S. Rota, and P. A. Rota. 1994. Virology of measles virus.J. Infect. Dis. 170:S15–S23.
6. Cattaneo, R., and M. A. Billeter. 1992. Mutations and A/I hypermutations inmeasles virus persistent infections. Curr. Top. Microbiol. Immunol. 172:63–74.
7. Chomczynski, P., and N. Sacchi. 1987. Single step method of RNA isolationby guanidinium-thiocyanate-phenol-chloroform extraction. Anal. Biochem.162:156–159.
8. Curran, M. D., and B. K. Rima. 1988. Nucleotide sequence of the geneencoding the matrix protein of a recent measles virus isolate. J. Gen. Virol.69:2407–2411.
9. Donaldson, J. A., and J. M. Snyder. 1992. Otosclerosis, p. 2997–3016. InC. W. Cummings, J. M. Frederickson, L. A. Harker, C. J. Krause, and D. E.Schuller (ed.), Otolaryngology—head and neck surgery. Mosby YearbookCo., St. Louis, Mo.
10. Girard, M., L. Hirth, G. Lebeurier, and J. Witz. 1989. Virologie moleculaire,p. 93. Doin, Paris, France.
11. Glasscock, M. E., and G. E. Shambough, Jr. 1990. Diagnosis, indications forsurgery and medical therapy of otospongiosis (otosclerosis), p. 370–387. InM. E. Glasscock and G. E. Shambough Jr. (ed.), Surgery of the ear. W. B.Saunders Co., Philadelphia, Pa.
12. Guild, S. R. 1944. Histologic otosclerosis. Ann. Otol. Rhinol. Laryngol. 53:246–266.
13. Katayama, Y., K. Kohso, A. Nishimura, Y. Tatsuno, M. Homma, and H.Hotta. 1998. Detection of measles virus mRNA from autopsied humantissues. J. Clin. Microbiol. 36:299–301.
14. Kumigami, H. 1996. Detection of viral antigen in the endolymphatic sac.Eur. Arch. Otolaryngol. 253:264–267.
15. McKenna, M. J., B. G. Mills, F. R. Galey, and F. H. Linthicum, Jr. 1986.Filamentous structures morphologically similar to viral nucleocapsids in oto-sclerosis lesions in two patients. Am. J. Otol. 7:25–28.
16. McKenna, M. J., and B. G. Mills. 1989. Immunohistochemical evidence of
measles virus antigens in active otosclerosis. Otolaryngol. Head Neck Surg.101:415–421.
17. McKenna, M. J., A. G. Kristiansen, and J. Haines. 1996. Polymerase chainreaction amplification of a measles virus sequence from human temporalbone sections with active otosclerosis. Am. J. Otol. 17:827–830.
18. Niedermeyer, H., W. Arnold, W. J. Neubert, and H. Hofler. 1994. Evidenceof measles virus in otosclerotic tissue. ORL 56:130–132.
19. Niedermeyer, H. P., and W. Arnold. 1995. Otosclerosis: a measles virusassociated inflammatory disease. Acta Otolaryngol. (Stockholm) 115:300–303.
20. Norrby, E., and K. Kristensson. 1997. Measles virus in the brain. Brain Res.Bull. 44:213–220.
21. Ogura, H., M. Ayata, K. Hayashi, T. Seto, O. Matsuoka, H. Hattori, K.Tanaka, K. Takano, and R. Murata. 1997. Efficient isolation of subacutesclerosing panencephalitis virus from patient brains by reference to magneticresonance and computed tomographic images. J. Neurovirol. 3:304–309.
22. Pilly, E. 1990. La rougeole, p. 341–347. In E. Pilly (ed.), Maladies infec-tieuses, Editions C & R, Paris, France.
23. Portmann, M. 1981. Surgical treatment of otospongiosis: different technicsand their evaluation. Acta Otorhinolaryngol. Belg. 35:458–465.
24. Rima, B. K. 1999. Paramyxoviruses and chronic human diseases. Bone 24:23S–26S.
25. Rota, J. S., Z. D. Wang, P. A. Rota, and W. J. Bellini. 1994. Comparison ofsequences of the H, F, and N coding genes of measles virus vaccine strains.Virus Res. 31:317–330.
26. Schrader, M., J. Poppendieck, and B. Weber. 1990. Immunohistologic find-ings in otosclerosis. Ann. Otol. Rhinol. Laryngol. 99:349–352.
27. Schuknecht, H. F. 1974. Disorders of growth, metabolism, and aging, p.351–409. In H. F. Schuknecht (ed.), Pathology of the ear. Harvard UniversityPress Co., Cambridge, Mass.
28. Shimizu, H., C. A. McCarthy, M. F. Smaron, and J. C. Burns. 1993. Poly-merase chain reaction for detection of measles virus in clinical samples.J. Clin. Microbiol. 31:1034–1039.
29. Spoza, T. M., P. A. Titchener, N. D. Portwood, and K. W. Taylor. 1993.Diabetes mellitus due to viruses: some recent developments. Diabetologia36:687–695.
30. Tomek, M. S., M. R. Brown, S. R. Mani, A. Ramesh, C. R. SrikumariSrisailapathy, P. Coucke, R. I. Zbar, A. M. Bell, W. T. McGuirt, K. Fuku-shima, P. J. Willems, G. Van Camp, and R. J. H. Smith. 1998. Localizationof a gene for otosclerosis to chromosome 15q25-q26. Hum. Mol. Genet. 7:285–290.
31. Yoo, T. J., J. M. Stuart, A. H. Kang, A. Townes, K. Tomeda, and S. Dixit.1982. Type II collagen autoimmunity in otosclerosis and Meniere’s disease.Science 217:1153–1155.
2660 GRAYELI ET AL. J. CLIN. MICROBIOL.
on October 26, 2020 by guest
http://jcm.asm
.org/D
ownloaded from