Embed Size (px)
DESCRIPTION
I made this Booklet as a research paper for the ENT marks in my collage...i hope u enjoyed it and got its benefits...pray for me and for the people of Gaza...
Citation preview

A research presented to:
The Otorhinolaryngology Department,
Tanta School of Medicine
By:
group 438-448
Otosclerosis and Stapedectomy:
The Expected Complications
© 2006, Sherif Magdi Sanad

OTOSCLEROSIS AND STAPEDECTOMY
The Expected Complications
© 2006 Sherif Magdi Sanad

Table of Contents
C H A P T E R 1
Anatomy of the Ear 1
The External Ear 1
The Middle Ear 2
The Inner Eat 3
C H A P T E R 2
Otosclerosis 5
Incidence 5
Etiology 5
Types and Sites 6
Pathology 6
Clinical Picture 7
Differential Diagnosis 7
Investigations 7
Treatment 8
C H A P T E R 3
Stapedectomy 9
Historical View 9
Indications and Patient Selection 10
Contraindications 11
The Technique 11
Anatomical Variation 14
Post-operative care 15
Prognosis 16
C H A P T E R 4
Complications of Stapedectomy 17
Complications of Anesthesia 17
Complications of the procedure 18
recurrence 20
References 21

Chapter
1 O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
Ear Anatomy:
The External, Middle and Inner Ears
he human ear is one of the more remarkable parts of the human body, not only because of the beauty and unlikelihood of its structure, but also because of its remarkable sensitivity to sounds. From an anatomical point of view, the ear is conventionally and conveniently divided into three parts:
the outer, the middle and the inner ears.
The External Ear: The external ear comprises the pinna (auricle), which is made of a convoluted plate of flexible cartilage that extends as a nearly closed tube one-third of the way down the ear canal. This outer third, which is about eight millimetres (one-third of an inch) long, has small hairs that point outwards to form a line of defence against small animals creeping in. The roots of the hairs produce oils and these mix with the secretions from nearby sweat-like glands to form the basis of wax. The deep two-thirds of the ear canal (16 millimeters/two-thirds of an inch long) has a bony wall lined with thin and rather fragile skin which is devoid of glands. At the far end of the ear canal and stretched across it is the eardrum (tympanic membrane), which forms the boundary between the outer and middle ears.
T The ear is a remarkable part of the body sensing sound and balance. It is divided into three parts: the outer, middle and inner ears.
The External Ear: 1- Pinna 2- External
auditory meatus
3- Ear drum
1

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
The Middle Ear: The middle ear itself (the tympanum) lies deep to the eardrum and is an air-filled space that holds three small bones (ossicles), which connect the eardrum to the inner ear.
These bones are called the hammer (malleus), anvil (incus) and stirrup (stapes) because of their resemblance to these objects. The hammer has a handle and a head and the handle lies within the layers of the eardrum. The head of the hammer sits in the upper part of the middle-ear space called the attic (epitympanum) and is connected by a joint – just the same as any other joint in the body – to the rather bulky body of the anvil. From the anvil, a long strut (the long process) descends back into the middle ear proper and is connected to the head of the stirrup. The two arches (crura) of the stirrup join the footplate, which sits in a small (3 mm x 2 mm) hole in the skull called the oval window (fenestra ovalis). This is the opening into the fluid-filled space of the inner ear. Just below the oval window is another small hole into the inner ear called the round window (fenestra rotunda). A thin membrane closes this and, when the footplate of the stirrup moves ‘in and out’, the round window membrane moves ‘out and in’ because the fluid in the inner ear transmits the pressure changes.
The middle ear is an air-filled space that holds three small bones (ossicles), which connect the eardrum to the inner ear.
The hammer and anvil are supported in the middle ear by several membranes and ligaments, which minimise their weight, allow them to move easily and bring them a blood supply. Unfortunately, this leaves only a small space for the passage of air from the middle ear to the attic.
Running through the middle ear is the facial nerve (nerve VII or the seventh nerve). This nerve leaves the brain and has to pass through the skull on its way to supply the muscles of facial expression, that is, muscles for frowning, winking, smiling, scowling, and so on. The nerve lies in a thin bony tube and runs horizontally from the front to the back of the middle ear just above the oval window and stirrup, before it turns downwards to leave the base of the skull. The nerve then turns forwards to reach the face. The facial nerve is therefore relatively vulnerable in diseases of the middle ear and, indeed, in middle-ear surgery itself. A facial palsy results in one side of the face being paralysed, so that the face droops and fails to move. Smiling results in a scowl and drinking in dribbling, and the eye fails to close on blinking.
Running through the eardrum is the nerve that carries taste from the front two-thirds of the tongue (the chorda tympani nerve). This nerve is on its way to join the facial nerve in the middle ear where it ‘hitch-hikes’ a lift back to the brain.
Finally, there are two small muscles in the middle ear. The one at the front (tensor tympani) is attached at the top of the handle of the hammer and tenses up the eardrum when swallowing activates it. The function of this muscle is not clear but it may be to make eating and swallowing a less noisy event.
The muscle at the back of the middle ear (stapedius) arises near the facial nerve, is supplied by it and attaches to the head of the stirrup. It responds to loud sounds by
2

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
contracting and stiffening the chain of small bones, and possibly reduces transmission of prolonged and potentially damaging, loud sounds to the inner ear.
The Inner Ear: The inner ear is probably the most remarkably intricate piece of the body. It makes hearing possible by converting sound into electrical impulses that then travel along the hearing nerve (the acoustic nerve or auditory nerve) to the brain. The inner ear also plays a major role in balance. The balance portions of the inner ear (vestibular labyrinth) can detect acceleration of the head in any direction whether in a straight line (linear) or twisting and turning (angular). The electrical signals that arise in response to head movement pass along the balance nerve (vestibular nerve), which in due course joins with the hearing nerve to form a single bundle (stato-acoustic, vestibulo-acoustic or eighth nerve, nerve VIII) which then enters the brain
The portion of the inner ear that actually hears is the cochlea. This is a hollow coiled tube set in the very dense bone called the bony labyrinth (part of the petrous [rock-like] temporal bone). This tube is filled with fluid, which is much the same as general body fluid (lymph) and that which surrounds the brain (cerebrospinal fluid – CSF). This inner-ear fluid is called perilymph. Inside the perilymph is another coiled triangular-shaped tube called the cochlear duct (scala media), which contains
3

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
the all-important ‘hair cells’ – these convert sound into electricity. These hair cells are arranged in two groups that follow the coils of the cochlear duct and spiral upwards from base to apex. There is a single row of inner hair cells (IHCs), which lie closer to the core of the cochlea (modiolus), and three or four rows of outer hair cells (OHCs), which are further away. In a healthy young human ear there are about 3,500 IHCs and about 12,000 OHCs. Each hair cell has a cluster of small rigid hairs (stereocilia), which project from the thicker upper surface of the cell into the special f luid that fills the cochlear duct. This fluid is called endolymph and is remarkable in that it has a strongly positive electrical charge associated with it – about 80 millivolts – and is rich in potassium, a metallic element.
The hearing nerves travel inwards, along with the balance and facial nerves, through a canal in the inner part of the skull (variously called the internal auditory meatus [IAM], internal auditory canal [IAC] or porus acousticus) to reach the brain stem. About half of the hearing nerves from each ear cross over to the other side of the brain stem and then, on both sides, the nerves pass up the brain stem through the mid-brain, eventually to reach ‘conscious- ness’ in what is called the cortex of the brain. For hearing, this conscious region is located in the temporal lobe portion of the brain, which lies on each side of the head just above the ear.
4

Chapter
2 O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
Otosclerosis:
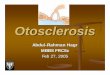
In this undecalcified section, a vascular focus of otosclerosis is seen adjacent to the cochlea.
Measles virus is thought to have a major role inotosclerosis affection.
The Problem and How to Manage?
tosclerosis is a disease of the bony labrynth. It is characterized by formation of a new vascularised spongy bone in localized foci replacing the normal compact bone of the bony labyrinth resulting in conductive hearing loss which is commonly bilateral.
O Incidence: Sex: Females are 2 times affected than males.
Race: Caucasian. The condition is rare in non-Caucasians, except East Indians, in whom the incidence is approximately the same as persons of northern or central European origin.
Bilaterality: Usually bilateral
Otosclerosis causes hearing loss in 0.3% of the general population.
Two-thirds of patients treated for otosclerosis are women.
Etiology: While the etiology of otosclerosis remains unknown, there are two main theories regarding its origin; genetic and viral.
1. Genetic. Otosclerosis seems inherited in approximately 50% of cases. It may be inherited as an autosomal dominant trait with 25-40 percent penetrance and is more common in females. Hearing loss associated with otosclerosis has long been noted to accelerate during pregnancy in some women.
2. Viral. Electron microscopy has demonstrated structures similar to viral nucleocapsids in cells of otospongiotic lesions. Immunohistochemical
5

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
Metabolic activity within the otosclerotic focus varies. In the active phase there are numerous fibrovascular spaces and an increased number of osteoblasts and osteocytes. The overall picture suggests active bone turnover.
Cochlear otosclerosis: The cochlea shows some involvement by theotosclerotic process inapproximately 35% of cases. In this patient the focus has extended through theendosteal layer of bone that affords attachment for the spiral ligament. The most common reaction seen in the spiral ligament is a loss of cellularity and occasionally the deposition of a layer of collagen adjacent to the focus.
studies revealed measles virus nucleocapsid protein in cells associated with otospongiosis. Polymerase chain reaction (PCR) studies have supported these observations and also found anti-measles IgG in the perilymph of patients with otosclerosis.
Types and sites: 1. Stapedial otosclerosis (commonest): causes conductive hearing loss.
2. Cochlear otosclerosis: causes pure sensoryneural hearing loss.
3. Mixed ootosclerosis.
Pathology: otosclerosis is characterized by 2 phases:
1. Otospongiosis: affected bone becomes hypervascular and osteoclasts and osteolytic osteocytes cause enlargement of the vascular spaces of the bone. Osteolytic osteocytes appear at the leading edge of the lesion, and sheets of connective tissue can be observed replacing the bone. Formation of dense sclerotic bone in areas of previous resorption signifies the late phase of otosclerosis. The result is disorganized bone, increased population of osteocytes, and enlarged marrow spaces containing vessels and other connective tissue.
2. Otosclerosis: Spaces are later replaced by dense sclerotic bone with narrow vasculature and few recognizable haversian systems. Pleomorphism is largely due to normal coexistence of both stages of otosclerosis in any single temporal bone.
Initiating lesions often neighbor the fissula ante fenestram and expand via vascular channels. In 80-90% of patients, lesions are limited to the anterior oval window and affect its pathology by calcification of the annular ligament or by involving the stapes. Both processes result in characteristic conductive hearing loss. In 8% of patients, the process involves the cochlea and parts of the labyrinth (labyrinthine otosclerosis), resulting in sensorineural hearing loss. Approximately 2% of patients display both labyrinthine and ossicular chain involvement.
Explanation of the clinical portion of sensorineural loss has been difficult, but investigators theorize that enzymes from the inner ear lesion diffuse via the spiral ligament to suppress neuron and hair cell activity.
6

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
Schwarts sign: The Schwartze sign isa pink flush seen through the tympanic membrane which may be found occasionally on otoscopic examination and is caused by the reflection of light from an active vascular focus of otosclerosis on the promontory. This rare sign is most likely to be seen in young adults with widespread active otosclerosis and generally indicates a poor prognosis.
Clinical Picture: • Otosclerosis is more common in females
• The age of onset is usually 20-40 years
• Juvenile type occurs in a younger age group and may be before puperty.
• Family history is positive in 50% of cases
Symptoms: 1. Hearing loss usually bilateral and progressive. Commonly conductive but
may be sensoryneural hearing loss.
2. Tinnitus: due to irritation of the delicate nerve endings in the inner ear.
3. Paracusis willshii: hearing is better in noisy areas due to the loud voices used against background noise.
Signs: 1. The tympanic membrane is normal in shape and mobility.
2. Bilateral conductive hearing loss usually but may be pure sensoryneural hearing loss or mixed.
3. Schwarts sign: Flamingo red flush seen through the tympanic membrane due to active vascular bone on the promontory. It is usually seen in the juvenile type.
Differential Diagnosis: 1. Chronic non suppurative otitis media.
2. Ossicular disconnection or fixation due to congenital, traumatic or inflammatory causes.
Investigations: Audiological:
1. Pure-tone audiometry: it usually demonstrates low-frequency conductive hearing loss. High-frequency losses begin to manifest with gradual air-bone gap widening. If cochlear involvement is not present, otosclerosis is limited to maximal conductive loss of 50-65 dB across all frequencies. If cochlear involvement is present, a mixed hearing loss appears, with high frequencies more affected. In severe cases, tinnitus may interfere with pure-tone audiometry. Stapes fixation produces an audiometric artifact known as the Carhart notch, which is characterized by elevation of bone conduction thresholds of 5 dB at 500 Hz, 10 dB at 1000 Hz, 15 dB at 2000 Hz, and 5 dB at 4000 Hz. Cochlear otosclerosis is characterized by the presence of
7

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
CT scan in the coronal plane (bone window) reveals extensive bone resorption surrounding the cochlea in a patient with tosclerosis. The zone of esorption highlights the noninvolved bone on either side, creating a "double halo" effect (arrow).
mixed or primary sensorineural hearing loss where air-bone gaps are minimal.
2. Tympanometry: it usually reveals the type As tympanogram with stapedial otosclerosis.
3. Acoustic reflexes: often are abnormal and may provide the earliest evidence of otosclerosis. Observed abnormality depends on stage of disease. Almost half the healthy population may show initial increase in compliance at stimulus onset, but compliance increase observed at offset occurs only in stapedial fixation and is virtually pathognomonic. Advancing fixation affects both ipsilateral and contralateral acoustic reflexes, even in unilateral disease.
Radiological: CT scanning of the temporal bone can often demonstrate foci of demineralization in the otic capsule in cases of cochlear otosclerosis.
Treatment: Medical treatment: Fluoride supplementation has met with variable response and is used sporadically for labyrinthine otosclerosis. It has also been used for postoperative medical management of obliterative otosclerosis. Surgical treatment: Approaches to surgical management of otosclerosis include total stapedectomy, partial stapedectomy, and stapedotomy.
Hearing aids: As with conductive hearing losses of other etiologies, hearing aids usually are helpful. It also useful if surgery is refused or contra indicated.
8

Chapter
3 O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
Stapedectomy:
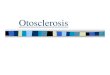
In a stapedectomy, the stapes is removed and a prosthesis is placed to transmit sound vibration from the the incus (anvil), to a fat plug (fascia or vein) in the oval window of the inner ear.
In the 1800s, Kessel attempted to create a fistula in patients with otosclerosis using a hammer and gouge.
The technique, post-operative care and prognosis.
tapedectomy is surgical removal of stapes or its supra structures and replacement by an artificial prosthesis as Teflon piston or fat and wire. This operation is indicated for stapedial and mixed but not cochlear otosclerosis.
Historical view:
S The history of the treatment of otosclerosis is rich in stories of serendipity and of treatments forgotten and rediscovered. In 1704, Valsalva first described stapes fixation as a cause of hearing loss. In the mid-1800s, a young man with otosclerosis was noted to have hearing improvement following a skull fracture. After he died of complications from the head injury, post-mortem examination of his temporal bones revealed a fracture through the horizontal semicircular canal. Kessel, who described the case, attempted to create a similar fistula in patients with otosclerosis using a hammer and gouge. In 1876, Kessel removed the stapes and covered the oval window with scar tissue. These early attempts at treatment failed. Ménière first reported mobilization of the stapes in 1842, but it was not until the late 19th century that stapes surgery became more common in Europe with advances in asepsis, hearing testing (tuning forks) and discovery of the X-ray. However, frequent complications, including meningitis, and transitory hearing improvement due to refixation of the stapes and closure of the fenestration led stapes mobilization and stapedectomy to be condemned as dangerous and useless by the end of the 19th century. Throughout the late 19th and early 20th centuries, dry catarrh was the term used to describe otosclerosis. In 1923, Holmgren first performed horizontal canal fenestration in the modern era, covering the fistula with mucoperiosteum. His associate, Nylen, developed a surgical microscope for the operation. Throughout the ensuing 25 years, variations of the horizontal canal fenestration were performed in Europe and the United States. From its outset, complete closure of the air-bone gap never occurred with fenestration and results frequently
9

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
deteriorated over time due to closure of the fenestrum. Even though the last fenestrations were done in the late 1950s, audiologists and otolaryngologists still encounter patients who had fenestration operations. Only an otolaryngologist or otologist should perform cerumen removal and maintenance of the post-operative mastoid cavity of these patients, due to the risk to the exposed labyrinth. A century after it was first performed, stapes mobilization again came into vogue in the early 1950s after Rosen reported his results. Air-bone gap closure was superior to the results achieved by fenestration, but the limitations of mobilization were soon recognized as refixation and recurrence of conductive hearing loss in a substantial number of patients. While mobilization is still occasionally performed, it has now been replaced by stapedectomy and stapedotomy. In 1956, John Shea reported his early experience with stapedectomy. During his operations, Shea removed the entire stapes and covered the oval window with a vein graft and used a nylon prosthesis from the incus to the graft. Subsequent refinements by Shea and others lead to the use of tragal perichondrium, fascia, and gelfoam to seal the oval window and various alloplastic materials such as wires and bucket-handle prostheses (that have a wire bale that loops over the incus) to reconstruct the ossicular chain. In the early 1970s, surgeons began creating small holes (fenestrum) in the oval window (referred to as a 'stapedotomy') and placing a piston within the hole to reconstruct the hearing mechanism. Since then, stapedotomy has become common although many respected and competent surgeons continue to perform variations of total or partial footplate removal. A variety of tools, including a diamond microdrill or a laser, are now used to create the fenestrum. The advantages of the microdrill include the speedy creation of a perfectly round fenestrum created to the size of the prosthesis, and the ability to work rapidly through thick footplates. The advantages of the laser include the potential for reduced trauma to the vestibule and the ability to create a fenestrum in the face of inadvertent mobilization of the footplate. In reality, both tools are well suited to the task and equally able to achieve excellent results in qualified hands.
Fenestration, Temporal Bone Section:The patent fenestra through the bony wall of the lateral semicircular canal can be seen. The fenestra is closed by the epithelial lining of the mastoid cavity.
Indications of Stapedectomy and patient selection: It is indicated for stapedial and mixed but not cochlear otosclerosis. However, hearing results in patients with air-bone gaps less than 15 - 30dB, most surgeons, recommend non-operative treatment in patients with ‘small’ air-bone gaps. The primary reason for this is that unless complete closure of the air-bone gap is achieved many patients with small air-bone gaps who have surgery will simply not obtain enough subjective benefit to feel the surgery was worthwhile. Nonetheless, patient selection varies from surgeon to surgeon and remains part of the doctor-patient relationship. Also, The age of the patient alone should not be a contraindication to performing surgery. In patients less than 16 years of age, there
10

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
is a greater chance that the conductive impairment is secondary to congenital anomalies rather than otosclerosis. Likewise, very active diffuse obliterative otosclerosis may be found in a young patient, predisposing to a higher incidence of complications. Yet surgery should be considered in the young because hearing acuity is essential during the formative years of development. Patients older than 75 years are still surgical candidates if they are in good health. Hearing acuity becomes more important as other senses decline with age. In order to prepare for surgery and to prevent failures and complications, infections and anatomic variations must also be considered.
Carefully informing patients of potential risks, benefits, and alternatives of treatment is critical in ensuring an outcome satisfactory to all concerned.
Contraindications:
• Coexistent Ménière disease increases the possibility of residual hearing loss in the operated ear.
• Documented dilation of the vestibule or the vestibular aqueduct on CT scanning or MRI also negatively impacts hearing outcome.
The technique: Procedures may be performed under general or local anesthesia with sedation.
The transcanal approach is usually used.
Steps: Raise a tympanomeatal flap and identify and protect the chorda. Next, curette the scutum and identify the pyramidal process, stapedial footplate, and the tympanic segment of the facial nerve. Measure distance from incus to stapes footplate, and then disarticulate the incus-stapes (IS) joint. Divide the posterior crus of the footplate and remove the remainder of the superstructure. Perform either a partial or complete stapedectomy or a stapedotomy. Place a soft tissue autograft, such as fascia, perichondrium, or vein, over the defect. To reestablish the conducting mechanism of the middle ear, interpose a prosthesis between the vestibule and incus. Replace the tympanomeatal flap.
11

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
An incision is made in the ear canal skin adjacent to the eardrum.
The ear canal skin along with a portion of the eardrum is elevated. The shaded area represents the area of bone that must be removed to allow adequate visualization of the stapes bone.
The chorda tympani nerve that transmits information about taste from the tongue frequently has to be moved around. A segment of the facial nerve shown is usually covered with bone.
The incus, stapes, stapedius tendon, chorda tympani nerve and facial nerve
12

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
A laser is used to divide the stapedius tendon.
One of the arches of the stapes bone is divided and the joint between the incus and stapes bones is separated. The outer part of the stapes bone is removed.
A laser is used to make a hole in the footplate of the stapes bone
A prosthesis is inserted and attached to the incus bone.
13

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
Anatomical variation of the Middle Ear:
A persistent stapedial artery is a congenital anomaly reported to occur in 1 of 5,000 – 10,000 ears.
A variety of anatomical issues may challenge the stapes surgeon. A. Persistent stapedial artery: A persistent stapedial artery is a congenital anomaly reported to occur in 1 of 5,000 – 10,000 ears. In this anomaly, the remnant of the dorsal end of the second aortic arch, the stapedial artery, courses through the space between the crura of the stapes (the obdurator foramen) after arising from the carotid artery. In this position, the vessel obscures the stapes footplate. The stapedial artery first appears in the tissue that forms the stapes at about the fifth week of fetal life and normally atrophies during the third month of development. The arch of the adult stapes is partly formed around the stapedial artery in a manner similar to the ‘lost wax’ method of jewelry casting. After ascending the promontory in a bony canal just lateral to the round window and basal turn of the cochlea and passing through the obdurator foramen, it turns anteriorly to join the facial nerve and ends by replacing the middle meningeal artery or by branching into the supra- or infraorbital or mandibular arteries. B. Superiorly located jugular bulb: A superiorly located jugular bulb may come into juxtaposition with a tympanic annulus and in this position is vulnerable to injury during elevation of the tympanic meatal flap. For this reason, the elevation of the tympanic annulus inferiorly should not be performed with both strobes of the elevator. Tears of the jugular bulb, of course, result in profuse bleeding and constitute an alarming, although not serious, complication. Elevating the head of the operating room table and packing the area with Gelfoam may control the bleeding. If the bleeding is readily controlled, the operation may be completed. If the tear is large and the bleeding is difficult to control, the procedure should be terminated.
C. Perilymph ‘gusher’ or ‘ oozer’: Perilymph ‘gushers’ are due to an abnormally patent cochlear aqueduct, or an incomplete partition between the subarachnoid space and the vestibule at the lateral end of the internal auditory canal. Gushers are luckily rare and, once encountered, are not soon forgotten. In about 50% of cases, stapes gusher will result in profound sensorineural hearing loss. Patients have a distinctive enlargement of the internal auditory canal on CT scanning. Surgeons should be particularly watchful in young boys with bilateral mixed hearing losses. Female carriers of the gene may manifest milder hearing losses.
14

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
D. Narrowing of the ear canal: This fairly common problem varies from mild narrowing of the external meatus that limits the exposure of the eardrum to frank stenosis by exostoses or large suture lines. Narrowing of the ear canal can be managed by meatoplasty. While meatoplasty can be performed at the same time stapedotomy is done, for very narrowed canals, I prefer to perform meatoplasty and then perform stapedotomy after the meatoplasty has healed.
Complications: Will be discussed in the next chapter.
Post-operative care: Immediately after the operation, we tell the patient and give him these advices:
1. Immediately after surgery, you will wake up in the recovery room, where you are watched very closely.
2. You will probably have some type of dressing/bandage over your ear. Your ear will feel full because there is packing in your ear.
3. Once your are awake enough and are able to drink fluids and eat food, the nurses will allow you to be discharged from the hospital. With this ear surgery, this is usually 4-5 hours after your procedure.
4. The nurses will check you for the following things prior to allowing you to go home:
a. that you are awake enough to travel comfortably b. that there is little or no bleeding c. that you have minimal or no pain d. that you do not have significant nausea, vertigo or dizziness e. that your overall health (heart rate, blood pressure, breathing) is stable f. that you do not have a fever
5. You will need a ride home after surgery
Diet In the immediate post-operative period, you may experience some vertigo, nausea or vomiting. It is therefore preferable to stick to a liquid diet or a light bland meal. A regular diet may be resumed the day after surgery. It is not unusual to experience some earache on mastication and possibly, some difficulty in fully opening the mouth.
15

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
We tell the patient not to allow any water to enter the operated ear. Protect the ear during showering or washing the hair with a large cotton ball coated with Vaseline.
Wound Care The operated ear is usually packed and full of blood. It will feel clogged and you may hear crackling sounds. You may have a stitch or two on the earlobe or the tragus (the little cartilage knob in front of the ear canal) . You will have a cotton ball in the ear, change it when it gets soaked and replace it with a clean cotton ball. It is not necessary to use a band aid or adhesive tape to hold the cotton ball. Just use a little antibiotic ointment to make the cotton ball stick. In very rare instances, if an incision is made behind the ear, you may have a dressing wrapped around the head or sutured behind the ear, please keep that dressing dry and avoid water at any cost. In general, such a dressing is removed a couple of days after the surgery. 1. Do not allow any water to enter the operated ear. Protect the ear during showering or washing the hair with a large cotton ball coated with Vaseline. When finished washing, remove the coated cotton, wipe the ear with a soft paper tissue and place a clean, dry cotton ball. A little antibiotic ointment may help the cotton ball stick and stay in place. 2. Thick, dark or bloody ear drainage is expected during the first week after surgery. You may clean the crusting from the outer part of the ear with peroxide and Q-tips. Replace the cotton ball in the ear with a clean, dry piece when the current one is soiled. Occasionally, you may see brown or dark red pieces of packing (Gelfoam) extruding from the ear canal. Do not attempt to replace them or to remove the remaining pieces that are still in the ear canal. 3. Do not blow your nose for at least two weeks from the day of surgery. Blowing can build excessive pressure in the operated ear and displace the eardrum. 4. If you have to sneeze, please do it with your mouth wide open to avoid pressure build up in your ear. 5. When sleeping, try to sleep on the unoperated ear. Medications Antibiotics are usually prescribed, please take them as directed until they are all gone. You may take pain medication as needed.
Prognosis: Commonly quoted statistics indicate that 90% of appropriately chosen surgical candidates enjoy a significant hearing improvement. Eight percent experience no significant hearing improvement. Up to 2% (including 0.2% who may experience complete sensorineural hearing loss in the operative ear) experience additional hearing loss. Stapedectomy, in experienced hands, is generally considered a safe procedure.
16

Chapter
4 O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
Stapedectomy:
Anaphylactic shock is a serious complication that may accompany general anesthesia.
The Complications
S any interference with the body functions, Stapedectomy obtains some complications. The complications may be due to anesthesia, the procedure or recurrence of the pathology.
Complications Due to General Anesthesia:
A A. Respiratory and cardiovascular depression.
B. Succinyl choline apnea:
It is due to prolonged paralysis of the respiratory muscles. This reaction may be idiosyncratic due to genetic abnormality in pseudocholinestrase activity, liver disease, malnutrition, plasma loss or organophosphorous poisoning. Artificial respiration is life saving in such condition.
C. Malignant hyperthermia:
It is an idiosyncratic reaction that occurs due to sudden and prolonged release of Ca++ from the Sarcoplasmic R. leading to muscular rigidity, excessive heat production and lactic acidosis. Contoling measures of this problem include I.V. dantrolene, cooling and correction of acidosis.
D. Anaphylactic Shock:
It is a severe, life-threatening, allergic reaction that occurs within minutes of exposure to the anesthetic drug. Symptoms may include sweating, Swelling of the lips, tongue or eyes, Paleness, bluish skin color, rapid pulse and circulatory collapse. Anaphylaxis is treated with the medication epinephrine and with intravenous fluids. The person also may need additional treatment with oxygen, mechanical ventilation, and additional medications such as antihistamines or corticosteroids given intravenously.
E. The risk of liver damage if used repeatedly.
17

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
Infection following Stapedectomy may occur but it is luckily rare.
Injury to the chorda tympani nerve occurs in up to 30% of cases. Symptoms include a dry mouth, sore tongue, and a metallic taste.
Complications Due to The procedure: A. Perilymphatic fistula: By its very nature, stapedotomy or stapedectomy creates a fistula between the perilymph-containing vestibule and the middle ear. What is surprising is how rarely this surgical fistula results in symptoms associated with fistula, namely hearing loss and vertigo. A fistula is the cause of failure in 9 – 10% of cases. The vertigo associated with a perilymphatic fistula is typically triggered or increased by pressure. If symptoms do not resolve with bed rest, surgical re-exploration is warranted. B. Dysgeusia (altered taste sensation): The chorda tympani courses anteriorly from the facial nerve, crossing lateral to the long process of the incus and medial to the malleus to enter the iter chorda anterior – a tiny hole anterior to the malleus. In its normal position, the chorda is at risk of injury during stapes surgery since displacement is usually required to gain the access to the oval window required to safely perform the surgery. Injury to the nerve occurs in up to 30% of cases. Symptoms include a dry mouth, sore tongue, and a metallic taste. Symptoms usually subside in 3 – 4 months. Stretching the chorda is more likely to result in symptoms than simply dividing the nerve. C. Tympanic membrane perforation: This complication arises occasionally. It most commonly occurs when the surgeon, attempting to elevate the tympanic membrane annulus from its groove, accidentally perforates the drum. It can also occur as the result of a post-operative infection. In all but a few cases, these typically small perforations heal uneventfully. Only a few will require surgical closure. D. Infection: Luckily rare, a post-operative infection after stapedotomy can lead to profound hearing loss and, in rare cases, meningitis. The latter occurs when bacteria transgress the vestibule to enter the CSF-containing subarachnoid space. E. Profound hearing loss: The risk of profound hearing loss is 0.6 – 3% in large stapedectomy series. The risk is considerably higher in revision stapes surgery. The chief cause of post-stapedectomy hearing loss is surgical trauma, especially extensive drilling. F. Dislodgement of incus: Two situations that can lead to inadvertent dislodgment of the incus are:
1) during removal of the bony rim of the annulus to expose the ossicles; and,
2) during placement of the prosthesis on the long process.
18

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
Facial nerve affection is an uncommon complication. It is usually due to the use of local anesthesia or dehiscence of the facial nerve.
Post Stapedectomy Granuloma: The oval window in this case is filled with vascular granulation tissue. Extending medially into the vestibule this tissue has become adherent to the saccular membrane.
G. Erosion of incus: While over-aggressive crimping of the crook of the prosthesis can fracture the incus, more commonly the long process of the incus erodes over time, causing the prosthesis to loosen and disarticulate, leading to conductive hearing loss. This erosion may be due to disruption of the blood supply to the distal long process of the incus . It may also be due to erosion by a bucket-style prosthesis or by over-crimping a piston with a wire-crook.
H. Floating footplate: In manipulating the stapes, the footplate may occasionally be dislodged if it is only partially fixed. In stapedectomy, this may create a problem if the footplate becomes depressed into the vestibule and cannot be safely removed. In laser stapedotomy, the floating footplate can be fenestrated and a piston placed as usual. I. Facial weakness: Facial weakness is rare complication of stapes surgery. It is most often temporary and due to the effects of local anesthesia. In these cases, it improves over a few hours. In some cases, it may be delayed and may be the effect of traction on the chorda tympani, heating of the nerve by the laser, or reactivation of herpes simplex virus-1.
J. Postoperative granulomas: postoperative granulomas can also be a cause of dysequilibrium, vertigo or progressive sensorineural hearing loss. Granuloma formation is seen in approximately 1:100 cases of revision stapedectomy. Foreign body reaction is a suspected etiology of postoperative granuloma formation. The condition usually manifests between the 5th and 15th postoperative day and is characterized symptomatically by hearing loss after an initial hearing gain or a sensation of unsteadiness. Associated with the hearing loss are loss of speech discrimination and a sensation of fullness in the ear. Examination reveals an edematous, thickened and hypervascular skin flap as well as dullness and reddening at the posterior part of the tympanic membrane. High-dose steroids may decrease the inflammatory response and its effects on the inner ear. The granuloma, including the portion within the vestibule, must be removed in its entirety along with the prosthesis. They may also be vaporized with laser after the prosthesis has been removed.
K. Cholesteatoma: Cholesteatoma following stapedectomy is a rare complication. Proposed mechanisms for formation include prosthesis extrusion, the presence of a squamous epithelium in the fascial graft, inversion of the tympanomeatal flap and a marginal perforation associated with a disruptive annulus.
19

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
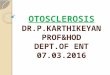
Recurrence and reactivation: In this case, the left side of the otosclerotic focus is highly active, whereas the right side of the focus is inactive.
Profuse middle ear bleeding is a rare complication and is usually associated with persistent stapedial artery.
L. Diplacusis: Diplacusis occurs in approximately one-third of the patients. There may be a variation of distortion of sound, especially music and the human voice, of which patients frequently complain. For the first few weeks after the operation most people complain of pure tones appearing higher in pitch when compared with the unoperated side. It is seldom problematic and usually fades by six weeks postoperatively.
M. Profuse middle ear bleeding: It is a rare complication and is usually associated with persistent stapedial artery. Rupture of the vessel could result in profuse hemorrhage and is to be meticulously avoided.
Recurrence: However, stapedectomy may be considered as a symptomatic treatment and not curative as we hadn't treated the causative pathology. Recurrence is usually due to spread of the pathology towards the cochlea.
20

O T O S C L E R O S I S A N D S T A P E D E C T O M Y : T H E E X P E C T E D C O M P L I C A T I O N S
References:
Saint Louis University, Department of Otolaryngology website.
E-medicine website.
Allrefer.com website.
Aetna InteliHealth website.
www.earsite.com
Gale Encyclopedia of Medicine.
Otorhinolaryngeology Department, Tanta School of medicine book.
Pharmacology Department, Tanta School of Medicine book.
21