Embed Size (px)
Citation preview


Case reports /review articlesan Unusual Breast Malignancy .....................................................................................................................................................................07S. Naqash, A.H. Sarmast, H.I. Showkat, M. Wani, S. Besina, M. Banday, M. Shah
nuchal fibroma: a rare entity of neck masses ............................................................................................................................................10N. Alsaleh, H. Amanguno
epinephrine-secreting large incidental pheochromocytoma in a normotensive male with stormy intraoperative hemodynamics .......13O. Nazir, T. Sharma, M. Maqsood, A. Khatuja, R. Misra
everolimus induced Pneumonitis.................................................................................................................................................................. 18Q. Badar, N. Masood, A. N. Abbasi
Primary Mantle Cell lymphoma of appendix ...............................................................................................................................................25VL Gaopande, SD Deshmukh, VC Shinde
a rare variant of Multiple Myeloma: non-Secretory Myeloma with diffuse osteolytic lesions ...............................................................28
S. Sultan, S.M. Irfan
Pain and Cancer: a systematic review .........................................................................................................................................................32F. Elomrani, N.Berrada, I .Ouziane , S.Lkhoyaali , H. Mrabti , H. Errihani.
original articlestumor thickness: a predictor of nodal disease in early squamous cell carcinomas of buccal mucosa ..................................................38G. Deshpande, S. Das
Hypofractionated Simultaneous integrated Boost (SiB) versus Conventional fractionation in localized Prostate Cancer: a randomized Pilot Study ..............................................................................................................................................................44K. Al- Ghamrawi, M. El-Haddad, S. Hanna, A. Ali, M. Kamal
Quantitative evaluation of the dosimetric effects of balloon deformation and source position in high-dose rate mammosite breast brachytherapy ................................................................................................................................................................54I. Ali, S. Negusse, S. Ahmad, O. Algan
Spectrum of ovarian tumors: Histopathological study of 218 cases ..........................................................................................................64N.A. Mansoor, H.S. Jezan
rare Chromosome Structural aberration Characterizing oncology Malignancy ........................................................................................71A. Movafagh, A. Sayad, M. Hashemi, H. Darvish, D. Zare-Abdollahi, B. Emamalizadeh, F. Shahvaisizadeh, N. Mansouri, S. A. Mortazavi-Tabatabaei
infectious complications after allogeneic bone marrow transplantation: Sheikha Badryia Center, Kuwait .............................................79S. AlShemmari, S. Refaat, A. A. Abdullah, M.A. Abul
Cancer news and Scientific events in the arab region• NewsNotes ............................................................................................................................................................................................. 87
• Advertisements ....................................................................................................................................................................................... 90
• ScientificeventsintheGCCandtheArabWorldfor2015 .................................................................................................................... 91
table of Contents

5454
Original Study
Quantitative evaluation of the dosimetric effects of balloon deformation and source position in high-dose
rate mammosite breast brachytherapyI. Ali1, S. Negusse2, S. Ahmad1, O. Algan1
1Department of Radiation Oncology, University of Oklahoma Health Sciences Center, Oklahoma City, USA. 2Muskogee Regional Cancer Center, 300 Rockefeller Dr, Muskogee, OK, USA
Corresponding author: Dr. Gururaj Deshpande, Consultant Surgical Oncologist. City Cancer Center, D.No.33-25-33, Ch. Venkata Krishnaiah Street, Suryaraopet, Vijayawada- 520002. Andhra Pradesh, India. Email: [email protected]
Phone: +91866-2436661
abstract
Purpose
To investigate quantitatively the deformation of the mammosite balloon, eccentricity of the source position and their effects on the dose delivered to the tumor lumpectomy site and critical structures.
Materials and Methods
The distances of the brachytherapy source to the surface of the mammosite balloon were measured in using radiographic images for fractions 1 to 10 for twelve patients. The dose at the balloon surface (nearly 680cGy) and prescription dose of 340cGy at 1cm from the balloon surface were calculated for the different fractions and their dependence on the balloon volume and source position were investigated.
results
The position of the source can be offset from the center of the mammosite balloon by up to 6mm. Deformation of the balloon led to variations in its
dimensions by up to 8mm. The dose at 1cm from the balloon surface that covers the lumpectomy site varied by up to 19% from 340cGy along the elongated diameter of the balloon and by up to 40% along the short diameter. Maximal doses to the skin, ribs and lung were 420cGy, 630cGy and 500cGy per fraction, respectively, which depended mostly on their distance from the balloon surface.
Conclusion
The geometric variations in the shape of the balloon and position of the source can cause lack of dose coverage to the lumpectomy site or create hot dose spots in the surrounding normal tissue that might compromise intended clinical goals. Users as well as vendors should consider correction measures for the deformation of the balloons and the eccentricity of the position of the high dose source.
Keywords
breast cancer, lumpectomy site, mammosite, high-dose-rate brachytherpay, balloon deformation, source centricity
Corresponding author: imad ali, Ph.D., DABR, Associate Professor, Medical Physics,
Department of Radiation Oncology, University of Oklahoma Health Sciences Center, 800 NE 10th Street,
Suite #L100, Oklahoma City, OK 73104, Tel: 405-271-8290, Fax: 405-271-9240
Email: [email protected]
introduction Breast conserving therapy (BCT), defined as
breast conserving surgery (BCS) followed by radiation therapy, has been shown to be equivalent to mastectomy in terms of overall survival in numerous randomized phase III trials (1-6). In all of these trials, the radiation therapy consisted of whole breast irradiation (WBI), with treatment of the regional lymph nodes as indicated. However, the majority of recurrences after breast conserving surgery occur in
the vicinity of the lumpectomy cavity (1,7-11). Because of this, there has been growing interest in utilizing

55
G. J. O. Issue 18, 2015
partial breast irradiation (PBI) after BCS. Even though there is no randomized data to demonstrate the equivalency of PBI to whole breast radiation therapy, there are numerous institutional experience suggesting local recurrence rates after accelerated partial breast irradiation similar to patients receiving whole breast irradiation (12,13).
The treatment of the surgical bed with a single catheter mammosite balloon (Cytyc Corporation, Palo Alto, CA) with high-dose-rate brachytherapy 192Ir-source (Nucletron Holding USA Inc., Columbia, MD) provides a simple, practical and efficient radiotherapy treatment option (14-16). The mammosite brachytherapy is superior to the three-dimensional conformal external beam partial breast therapy in terms of requirements of patient setup and breast immobilization, tumor localization and sparing critical structures receiving entrance and exit doses from external beam. It is also simpler and less invasive than interstitial brachytherapy where multiple catheters are used with several dwell positions (17). The goals of this study were to measure the position of the brachytherapy source within the balloon and quantify its deviations from the balloon center, evaluate the extent of deformations of the balloon from the spherical shape. The effects of the source eccentricity and balloon deformation on the dose coverage of the surgical bed and critical structures such as skin, ribs in the chest wall and lung were investigated in slected breast cancer patients from our institution retrospective to treatment.
Materials and Methods
Mammosite Brachytherapy and Patients
Partial breast treatment with mammosite brachytherapy was approved by the U.S. Food and Drug Administration in May 2002. This technique employs a balloon that is placed in the lumpectomy site either at the time of lumpectomy or percutaneously after the procedure (14,16,18). The mammosite device consists of a silicon balloon and a dual-lumen catheter. The catheter is located centrally within the balloon where the outer lumen is used to inflate the balloon with saline and the inner lumen to insert the brachytherapy source in the treatment position. The balloon is available commercially in different sizes that fit small to large lumpectomy cavities. In our
patients, the mammosite balloon was inserted 1-2 weeks after BCS when a final pathology report was available. The balloon was placed by the breast surgeons under ultrasound image guidance. Patients generally had their balloon inflated with a mixture of saline solution and contrast (10%) to improve the balloon visibility in CT and radiographic images. Prior to start of treatment, all patients underwent an initial treatment planning CT scan. This scan was utilized to evaluate the balloon shape, lumpectomy cavity size, the extent of air or fluid around the mammosite balloon, and proximity of the balloon edge to the chestwall and the skin surface. The dose delivery was performed with a single dwell position using an 192Ir high-dose-rate brachytherapy source. The PTV was defined as the volume of breast tissue 1 cm around the balloon surface. The PTV was treated with 340 cGy twice daily for 5 days for a total prescription dose of 3400 cGy. A minimum of 4 hours was required in between the two daily treatments, and in general the two treatment seessions were separated by about 6 hours.
CT simulation was performed with a dummy source inserted in the balloon to locate the dwell position at the distal end of the catheter. The symmetry of the balloon was evaluated initially before treatment planning using axial, coronal and sagittal views from CT imaging. The treatment planning was performed using CT images acquired with the balloon in site using the geometric and dosimetric recommendation of the NSABP B-39 trial (ClinicalTrials.Gov identifier NCT00103181). Several parameters were used to determine the quality of the initial treatment plan including: symmetry and fitness of the balloon to the lumpectomy site, air cavities, appropriate distance from the surface of the balloon to the critical structures such as the skin (> 7 mm), ribs and lung (> 10 mm). To ensure dose coverage, the dose was calculated at four points that are located 1 cm from the surface of the balloon (anterior, posterior, superior, and inferior points) and the dose has to be within 15% from the prescribed dose. In treatment planning, the dose calculation algorithm considered the balloon with its contents and the surrounding tissue as homogenous water equivalent and no inhomogeneity corrections were considered for air cavities or contrast material. The sparing of critical structures such as skin, lung and ribs was considered by ensuring that the distance

56
Quantitative evaluation and high-dose rate mammosite breast brachytherapy, I. Ali, et. al.
between any of them and the balloon surface was larger than nearly 7 mm.
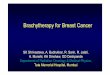
Twelve patients with stage I and II breast cancer treated with high-dose-rate brachytherapy using a mammosite balloon were selected for this study. Each patient was treated with ten fractions delivered in a bid fashion for a total dose of 3400 cGy using an 192Ir source with a single dwell position at the center of the balloon. Before each treatment session, two orthogonal radiographs (anterior-posterior (AP) and lateral) with a dummy source in the catheter were acquired as shown in Fig. 1a-b. The radiographic images were used to verify the integrity of the balloon and reproducibility of the initial treatment plan by measuring the position of the source within the balloon. The diameter of the balloon was measured and position of the source was determined and compared with the center of the balloon.
Physical parameters of the balloon
The mammosite balloon was assumed to be an ellipsoid with a, b and c as the equatorial radii in the superior-inferior, lateral-medial and anterior-posterior directions, respectively. The equatorial radii were measured directly from the anterior-posterior (AP) and lateral (RL) radiographs that are obtained prior to each treatment session as shown in Fig.1a-c. From the AP view, radius a was calculated from an average distance between the source position and to the superior and inferior ends of the balloon (Z-axis). b was calculated from the average distance between the source and right and left ends of the balloon (X-axis). c was obtained from average distance between the source and the anterior and posterior ends of the balloon on RL view (Y-axis). The longest or shortest dimension of the balloon could be along
any direction. Figure 1c shows a schematic of the balloon with the reference coordinate system.
The volume of the mammosite balloon was calculated from the following formula:
(1)
Eccentricity of the high-dose-rate source was obtained for position offsets in the different directions as given by the following equation:
(2)
where 1a , 2a are the distances between the source and superior and inferior ends of the balloon,
1b , 2b are distances between the source and right
and left ends, and 1c , 2c are the distances between the anterior and posterior ends, respectively.
Dose calculation
The 192Ir high-dose-rate source was assumed to be a point source and the dose was calculated using the formalism of AAPM task group 43 (17,19) using the following equation:
(3)
where is the dose rate at r, KS is the air-kerma strength of the source, A is dose rate constant
figure 1 : (a-b) radiographic anterior and right lateral views of a patient with a mammosite balloon implanted. (c) Schematic with balloon dimensions and coordinate system.

57
G. J. O. Issue 18, 2015
in water, ( )Pg r is the radial dose function, øan(r) is the anisotropy correction constant. These parameters were obtained from TG-229 for the the 192Ir source (20). The dose was calculated at two positions: (a) at the hypothetical surface of the balloon at an average equatorial radius, a , of (a,b,c) which represented
surface dose of the balloon, and (b) at 1a cm+ which was the dose that covers 1cm of tissue beyond the surface. The 192Ir source at the center of the balloon was assumed to deliver a dose of 340
cGy per fraction at the 1a cm+ to cover the PTV using a single dwell position. In order to investigate quatatively the actual clinical doses delivered to the patient considered in this study, the doses at the surface of the balloon at distances a, b and c were calculated and compared with 200% isodose line (680 cGy).
results Figure 2a shows histograms of the variations in
the dimensions (a,b,c) of the balloons from the total of 12 patients who were treated with 10 fractions twice a day for five days. The balloon dimensions varied widely along the different dimensions from nearly 18 mm to 36 mm. The balloons were oriented in different ways where the balloon elongation were along any direction (X,Y,Z) with means of 23.7 , 23.6, and 26.6 mm and standard deviations of 2.1, 4.8, and 4.2 mm, respectively, as listed in Table 1. Deformation of the balloon resulted variations in its dimensions by up to 8 mm considering all fractions and patients selected for this study. Figure 2b shows histograms of the variations in the position of the source from the
center of the balloon along the different directions (X,Y,Z) for the same 12 patients. The mean position of the source was -0.2, 0.1, and -0.7 mm off-set from the center of the balloon in (X,Y,Z) directions, respectively. The standard deviation of the position of the source from the center of the balloon was 1.3, 1.5 and 2.0 mm in the (X,Y,Z) directions, respectively, as listed in Table 1. The position of the source was offset from the center of the mammosite balloon by up to 6 mm. Figure 2c shows that the variations in the dimensions of the balloon is diffent during the treatment course where the mean and standard variations are listed in Table 1. In two patients, the variation in the dimensions of the balloon was up to 8 mm in some of their fractions.
The dose at the surface of the balloon varied by up to 28% from 680 cGy along the large diameter of the ellipsoid and by up to 60% along the shorter diameter of the balloon as shown in Fig. 3a. The mean of the dose at the balloon surface was -4.1%, -14.2% and 6.1% higher or lower than 680 cGy and standard deviation was 14.8%, 33.4% and 30.3% along (X,Y,Z), respectively, as listed in Table 2. The dose at 1 cm from the balloon surface that coverd the lumpectomy site, which was defined as the planning target volume (PTV), varied by up to 19% from 340 cGy along the elongated diameter of the balloon and by up to 40% along the short diameter as shown in Fig. 3b. The mean dose at 1 cm from the balloon along the (X,Y,Z) direction was -1.7%, -5.7%, and 9.5% from the 340 cGy and percentage standard deviations were 10.3%, 22.7%, 21.7% , respectively.
figure 2 : (a) Histograms of the dimensions (a,b,c) of the balloon along (X,Y,Z). (b) Histograms of the source position relative to the center of the balloon in three directions (X,Y,Z). (c) variations of the dimensions (a,b,c) of the balloon over the treatment course for ten patients treated bid with two fractions a day.

58
Quantitative evaluation and high-dose rate mammosite breast brachytherapy, I. Ali, et. al.
Dose to critical structures
Figure 4a shows a scatter plot of the skin maximal dose as function of the distance between the skin and the balloon surface for the different patients obtained from CT images used in treatment planning. The distance of the balloon surface from skin varied for different patients starting from 5 mm to about 45 mm. The maximal skin dose decreased with the increase
of the distance from the surface of the balloon to the skin and ranged from nearly 90-420 cGy per hypo-fractionation of 340 cGy. Similarly, Fig. 4b shows that the lung maximal dose increased with decrease of the distance between the balloon surface and the lung in closest proximity. The maximal lung dose ranged
figure 3 : (a) Histograms of the percentage dose difference (relative to 680 cgy) at the surface of the balloon (a,b,c). (b) Histogram of the percentage dose difference at 1 cm from the surface of the balloon (a,b,c) relative to 340 cgy.
table 1 : Mean and standard deviation in the balloon dimensions (a,b,c), difference between the balloon dimensions and position of the source from the balloon center along (X,Y,Z) directions.
table 2 : Mean and standard deviation of the dose at surface of the balloon and dose at 1 cm from balloon surface along (a,b,c).

59
G. J. O. Issue 18, 2015
figure 4 : Scatter plots of the maximum dose of the critical structures per fraction: (a) skin (b) lung and (c) ribs as a function of distance from the surface of the mammosite balloon in patients treated with Hdr brachytherapy.
figure 5 : (a) variation of maximal dose of the lung, skin and ribs with volume of the mammosite balloon for breast brachytherapy. (b,c,d) variations of the maximal dose of the lung, skin and ribs with the different dimensions of the mammosite balloon, respectively.

60
Quantitative evaluation and high-dose rate mammosite breast brachytherapy, I. Ali, et. al.
from 100 cGy for lungs 38 mm from the surface of the balloon to 500 cGy for lung at 7 mm distance from the surface of the balloon per treatment fraction of 340 cGy. Figure 4c shows the correlation between ribs maximal dose and distance between the rib in close proximity to the surface of the balloon. Similar to skin and lung maximal doses, the maximal dose of the ribs increased with decrease of the distance between the rib and surface of the balloon. The maximal rib dose ranged from 110 cGy at 34 mm to nearly 630 cGy to 3 mm per treatment fraction of 340 cGy. The mean and standard deviations of the maximal dose and distance from the surface of balloon to the three critical structures: skin, lung and ribs are listed in Table 3.
Figure 5a shows a scatter plot of maximal dose variation of the lung, skin and ribs with the volume of the mammosite balloon used in treatment. There was no correlation between the maximal dose and the volume of the balloon. Similarly, the maximal dose for these critical structures did not correlate with the dimensions (a,b,c) of the mammosite balloon as shown in Figs 5 b-d, respectively.
discussion The dimensions of the different balloons varied
from one patient into another in the range 17.5-35.5 mm as shown in Fig. 2a. In addition, balloon alignment varied from one patient into another depending on the lumpectomy tumor bed with the major axis being oriented in any direction relative to patient coordinate system. The mammosite balloons average dimensions were a = 23.7 mm, b = 23.6 mm, and c = 26.6 mm as listed in Table 1. In addition the position of the source was off-set from the center of the balloon as shown in Fig 2b.
The eccentricity of the source position and balloon deformation affected significantly the dosimetric coverage of the PTV as represented in Figs 3a-b. The balloon deformations may have resulted from various causes including: (a) variation in edema buildup around the balloon, (b) variation in skin pressure due to position of the patient, breast tissue or the ipsilateral arm and (c) leakage of fluid from the balloon. The balloon shape and dimensions should be tested before each treatment sessions. Corrective actions should be considered in cases where the variation in the dimensions or size of the balloon are larger than departmental tolerance. These corrective actions should include: (a) removal of fluid from around the balloon within the lumpectomy cavity, (b) recentering of the balloon within the surgical cavity, (c) consistent positioning of the patient and the breast tissue in the same position as the treatment planning simulation, and (d) evaluating fluid leakage from the balloon. Alhough, leakage from the balloon is a possibility, our findings from patients who had measurements of the amount of fluid into the balloon prior to the beginning of treatment, and the amount of fluid removed at the end of treatment suggested that this was not a common occurance. Thus, in our patient population, the variation in balloon volume were not correlated with variations in the volume of saline where no leakages were detected.
The most deterministic parameter in the dose of critical structures is its location relative to the surface of the balloon. The maximal dose for the skin, rib and lung increased with decrease of the distance from the surface of the balloon. For example, the mean maximal dose for the skin was 240.7 cGy and the mean distance of of the skin from the balloon surface was 18.5 mm as listed in Table 3. In our patients,
table 3 : Mean and standard deviation of the maximal dose per fraction and distance of critical structures including skin, lung and ribs from the mammosite balloon.

61
G. J. O. Issue 18, 2015
however, there was only mild skin complications that cleared few weeks after brachytherapy. None of the patient population investigated in this study have suffered from rib or lung complications even some balloons were in close proximity to these critical structures as shown in Figs. 4b-c. Fat necrosis is another reported side effect of APBI. It most commonly occurs in the fatty breast tissue immediately adjacent to the balloon, where the radiation doses can exceed 200% depending on balloon deformation and non-isocentricity of the source position as shown in Fig. 2c. The rates of fat necrosis reported in the literature ranges from 2.5% to 27% (12,21). No patient in the current series developed symptomatic fat necrosis, and further evaluation of this toxicity was not possible.
This investigation showed the dosimetric limitations of single catheter, single dwell position APBI treatment using the mammosite catheter. These limitations included compromises in the dose coverage of the PTV and sparing of critical structures due to shape deformation of the balloon and eccentricity of the source position. Furthermore, the position of critical structure relative the balloon depended on the location of the disease within the breast, for example skin in close proximity was located in the range 5-45 mm and the closest ribs were located 3-34 mm relative to the surface of the balloon as presented in this work. It seems that the usage of a mammosite balloon with one catheter with multiple dwell position or other available commercial products with mammosite balloons with multiple catheters and multiple dwell position (22) might provide the tools to conform dose coverage of the PTV for deformed balloons and adapt with patient anatomy to spare critical structures such as skin, ribs and lung that are in close proximity to the balloon surface. Comparison with other techniques as mentioned above with balloon and multiple catheter and source dwel positions might the subject of a future study.
One limitation of the doses presented here for the critical structures such skin, lung and ribs is the use of the AAPM TG-43 empirical formalism (17,19) which does not consider heterogeneity (23-25) and scattered radiation correctly (26,27). The AAPM TG-186 (28) reported that large dose discrepancies as large as 15% or more can exist between model-based
dose calculation algorithms and TG-43 formula considering contrast in the balloon, lung and bone heterogeneity. The dose from lack of backscatter contribution (27) might be as large as 10% depending on the size of the balloon and thickness of tissue interface between the ballon and skin which causes underdose of the PTV that is not considered in the dose calculation using TG-43.
Conclusions Two main geometric parameters has been
investigated in this study that affected the dose to the PTV and critical structures in mammosite balloon brachytherapy. Large variations in the dimensions of the mammosite balloon from one fraction to another during the course of treatment of one patient were measured. The position of the source was found to be shifted in some treatments significantly from the center of the balloon. These geometric variations might lead to lack of the dose coverage of the lumpectomy site or create hot spots in the surrounding normal tissue compromising the intended clinical goals. The data illustrated in this work suggests that user as well as vendors should consider correction measures for the eccentricity of the position of the high dose source and deformation of inflated balloons in order to achieve intended clinical dose coverage of the lumpectomy site. Other mammosite balloons with multiple dwell position in one catheter or multiple catheters with multiple dwell positions provide dosimetric tools to conform dose distributions in order to account for balloon deformations, ecentricity of the source position, and location of critical structures.

62
Quantitative evaluation and high-dose rate mammosite breast brachytherapy, I. Ali, et. al.
references 1. Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch
M, Fisher ER, Jeong JH, Wolmark N. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. New England Journal of Medicine 2002;347:1233-1241.
2. Veronesi U, Cascinelli N, Mariani L, Greco M, Saccozzi R, Luini A, Aguilar M, Marubini E. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. New England Journal of Medicine 2002;347:1227-1232.
3. Litiere S, Werutsky G, Fentiman I, Rutgers E, Christiaens MR, Van Limbergen E, Baaijens MH, Bogaerts J, Bartelink H. Breast conserving therapy versus mastectomy for stage i-ii breast cancer: 20 year follow-up of the eortc 10801 phase 3 randomised trial. Lancet 2012;13:412-419.
4. Arriagada R, Le MG, Guinebretiere JM, Dunant A, Rochard F, Tursz T. Late local recurrences in a randomised trial comparing conservative treatment with total mastectomy in early breast cancer patients. Ann Oncol 2003;14:1617-1622.
5. Blichert TM, Nielsen M, During M, et al. Long-term results of breast conserving surgery vs. Mastectomy for early stage invasive breast cancer: 20-year follow-up of the danish randomized dbcg-82tm protocol. Acta Oncology 2008;47:672-681.
6. Poggi MM, Danforth DN, Sciuto LC, et al. Eighteen-year results in the treatment of early breast carcinoma with mastectomy verser breast conserving therapy: The national cancer institute randomized trial. Cancer 2003;98:697-702.
7. Veronisi U, Marubini E, et al. Radiotherapy after breast-conserving surgery in small breast carcinoma: Long-term results of a randomized trial. Annals of Oncology 2001;12:997-1003.
8. Clark RM, Whelan T, Levine M, Roberts R, Willan A, McCulloch P, Lipa M, Wilkinson RH, Mahoney LJ. Randomized clinical trial of breast irradiation following lumpectomy and axillary dissection for node-negative breast cancer: An update. Ontario clinical oncology group. J Natl Cancer Inst 1996;88:1659-1664.
9. Holli K, Saaristo R, Isola J, Joensuu H, Hakama M. Lumpectomy with or without postoperative radiotherapy for breast cancer with favourable prognostic features: Results of a randomized study. British Journal of Cancer 2001;84:164-169.
10. Liljegren G, Holmberg L, Bergh J, Lindgren A, Tabar L, Nordgren H, Adami HO, Grp U-OBCS. 10-year results after sector resection with or without postoperative radiotherapy for stage i breast cancer: A randomized trial. Journal of Clinical Oncology 1999;17:2326-2333.
11. Fisher ER, Dignam J, Tan-Chiu E, al. e. Pathologic findings from the national surgical adjuvant breast and bower project (nsabp) eight-year update of protocol b-17: Intraductal carcinoma. Cancer 1999;86:429-438.
12. Shah C, Badiyan S, Ben Wilkinson J, Vicini F, Beitsch P, Keisch M, Arthur D, Lyden M. Treatment efficacy with accelerated partial breast irradiation (apbi): Final analysis of the american society of breast surgeons mammosite breast brachytherapy registry trial. Annals of Surgical Oncology 2013;20:3279-3285.
13. Vargo JA, Verma V, Kim H, Kalash R, Heron DE, Johnson R, Beriwal S. Extended (5 year) outcomes of accelerated partial breast irradiation using mammosite balloon brachytherapy: Patterns or failure, patient selection, and dosimetric correlates for late toxicity. Internation Journal of Radiation Oncology Biology Physicis 2014;88:285-291.
14. Keisch M, Vicini F, Kuske RR, Hebert M, White J, Quiet C, Arthur D, Scroggins T, Streeter O. Initial clinical experience with the mammosite breast brachytherapy applicator in women with early-stage breast cancer treated with breast-conserving therapy. Int J Radiat Oncol Biol Phys 2003;55:289-293.
15. Dickler A, Kirk MC, Chu J, Nguyen C. The mammosite breast brachytherapy applicator: A review of the technique and outcomes. Brachytherapy 2005;4:130-136.
16. Vu KN, Dragun AE, Cole DJ, Jenrette JM. Accelerated partial breast irradiation using mammosite brachytherapy: A multidisciplinary approach to breast-conservation therapy. Commun Oncol 2005;2:477-482.
17. Nath R, Anderson LL, Luxton G, Weaver KA, Williamson JF, Meigooni AS. Dosimetry of interstitial brachytherapy sources: Recommendations of the aapm radiation therapy committee task group no. 43, american association of physicists in medicine. Med Phys 1995;22:209-226.
18. Edmundson GK, Vicini FA, Chen PY, Mitchell C, Martinez AA. Dosimetric characteristics of the mammosite rts, a new breast brachytherapy applicator. Int J Radiat Oncol Biol Phys 2002;52:1132-1139.
19. Rivard MJ, Coursey BM, DeWerd LA, Hanson WF, Huq MS, Ibbott GS, Mitch MG, Nath R, Williamson JF. Update of aapm task group no. 43 report: A revised aapm protocol for brachytherapy dose calculations. Med Phys 2004;31:633-674.
20. Calatayud JP, Ballester F, Das RK, DeWerd LA, Ibbott GS, Meigooni AS, Ouhib Z, Rivard MJ, Sloboda RS, Williamson JF, Dose calculation for photon-emitting brachytherapy sources with average energy higher than 50 kev. AAPM and ESTRO, 2012.
21. Rosenkranz KM, Edmund T, McCabe EB, J. Gui J, Underhill K, Barth RJ. Increased rates of long-term complications after mammosite brachytherapy compared with whole breast radiation therapy. J Am Coll Surg 213;217:497-502.

63
G. J. O. Issue 18, 2015
22. Gurdalli S, Kuske RR, Quiet C, Ozer M. Dosimetric performance of strut-adjusted volume implant: A new single-entry multicatheter breast brachytherapy applicator. Brachytherapy 2011;10:128-135.
23. Kassas B, Mourtada F, Horton JL, Lane RG. Contrast effects on dosimetry of a partial breast irradiation system. Med Phys 2004;31:1976-1979.
24. Kirk MC, Hsi WC, Chu JCH, Niu H, Hu Z, Bernard D, Dickler A, Nguyen C. Dose perturbation induced by radiographic contrast inside brachytherapy balloon applicators. Med Phys 2004;31:1219-1224.
25. Cheng CW, Mitra R, Li XA, Das IJ. Dose perturbations due to contrast medium and air in mammosite treatment: An experimental and monte carlo study. Med26. Pantelis E, Papagiannis P, Karaiskos P, Angelopoulos A, Anagnostopoulos G, Baltas D, Zamboglou N, Sakelliou L. The effect of finite patient dimensions and tissue inhomogeneities on dosimetry planning of 192ir hdr breast brachytherapy: A monte carlo dose verification study. Int J Radiat Oncol Biol Phys 2005;61:1596-1602.
27. Kassas B, Mourtada F, Horton JL, Lane RG, Buchholz TA, Strom EA. Dose modification factors for 192ir high-dose-rate irradiation using monte carlo simulation. J Appl Clin Med Phys 2006;7:28-34.
28. Beaulieu L, Carlsson Tedgren A, Carrier J, Davis S, Mourtada F, Rivard M, Thomson R, Verhaegen F, Wareing T, Williamson J. Report of the task group 186 on model-based dose calculation methods in brachytherapy beyond the tg-43 formalism: Current status and recommendations for clinical implementation. Med Phys 2012;39:6208-6236.Phys 2005;32:2279-2287.