Embed Size (px)
Citation preview

TN
615.309.6053
www.healthtechs3.com
New Discharge Planning Requirements
What You Need to Know
5110 Maryland Way, Suite 200, Brentwood,2745 North Dallas Pkwy, Suite 100, Dallas,TX
800.228.0647
www.gaffeythealthcare.com
1

Preferred vendor to:
Currently provides hospital
management, consulting
services and technology to:
• Serving community, district, non-profitand critical access hospitals
MT. Ranked as a Top 100 Critical Access
Hospital for 8 years in a row
• Example technology and AR servicesclient includes two-hospital NFP system
in southeast GA with numerous
associated physician practices
• Example managed hospital client includes•
Barrett Hospital and Healthcare in Dillon,
• California Critical Access Hospital
Network
• Western Healthcare AlliancePartner with Illinois Critical Access
Hospital Network
• Vizient Group Purchasing Organization
Nationwide Client Base
2

• Executive management & leadership development
• Community health needs assessment
• Lean culture
• Executive and interim recruitment
• CEOs, CFOs, CNOs
• VP and Department Directors
• Performance optimization & margin improvement
• Revenue cycle & business office improvement
• AR outsourcing
• Continuous survey readiness
• Care coordination
• Swing bed consulting
Governance & Strategy
Recruitment Clinical Care & Operations
Finance
Areas of ExpertiseStrategy – Solutions - Support
3

What’s New In The 2020: Physician Fee Schedule That May Impact Your Care Coordination Program?Date: January 23, 2020 Time: 12pm CSTPresenter : Faith M Jones, MSN, RN, NEA-BC – Director of Care Coordination and Lean Consulting, HealthTechS3https://bit.ly/3ayuXER
Swing Bed Regulatory Requirements Revised – Again!Date: January 24, 2020 Time: 12pm CSTPresenter : Carolyn St.Charles, RN, BSN, MBA, Regional Chief Clinical Officerhttps://bit.ly/2Gcw27l
New Discharge Planning Requirements – What You Need To KnowDate: February 7, 2020 Time: 12:00 pm CSTPresenter : Carolyn St.Charles, RN, BSN, MBA, Regional Chief Clinical Officerhttps://bit.ly/30LDC2z
Health Promotion Is The Goal Of An Effective Care Coordination Program – Are You Reaching Your Goal?Date: February 20, 2020 Time: 12pm CSTPresenter : Faith M Jones, MSN, RN, NEA-BC – Director of Care Coordination and Lean Consulting, HealthTechS3 https://bit.ly/2RF4RHU
Implementing An Effective Quality Assurance/Performance Improvement Program –A Cheerleader’s GuideDate: March 6, 2020 Time: 12pm CSTPresenter : Carolyn St.Charles, RN, BSN, MBA, Regional Chief Clinical Officerhttps://bit.ly/2RkkGol
The Art And Science Of Interim Placement: Speed DatingDate: March 11, 2020 Time: 12pm CSTPresenter: Mike Lieb, Vice President – Interim Services, HealthTechS3https://bit.ly/3avl6Qt
Recruiting A Difference Maker For Your Rural HospitalDate: March 19, , 2020 Time: 12pm CSTPresenter: Peter Goodspeed – VP of Executive Search, HTS3 Executive Recruitinghttps://bit.ly/37jyyVw
Managing Behavioral Health Patients In Your Primary Care Practice With Collaborative Care ManagementDate: March 26, 2020 Time: 12pm CSTPresenters: Faith M Jones, MSN, RN, NEA-BC, Director of Care Coordination and Lean Consulting, HealthTechS3https://bit.ly/36mmL7j
ALL WEBINARS ARE RECORDED

Instructions for Today’s Webinar
✓ You may type a question in the text box if you have a question during the presentation
✓ We will try to cover all of your questions – but if we don’t get to them during the webinar we will follow-up with you by e-mail
✓ You may also send questions after the webinar to our team (contact information is included at the end of thepresentation)
✓ The webinar will be recorded and the recording will be available on the HealthTechS3 web site at
www.healthtechs3.com
HealthTechS3 hopes that the information contained herein will be informative and helpful on industry topics. However, please note that this information is not intended to be definitive. HealthTechS3 and its affiliates expressly disclaim any and all liability, whatsoever, for any such information and for any use made thereof. HealthTechS3 does not and shall not have any authority to develop substantive billing or coding policies for any hospital, clinic or their respective personnel, and any such final responsibility remains exclusively with the hospital, clinic or their respective personnel. HealthTechS3 recommends that hospitals, clinics, their respective personnel, and all other third party recipients of this information consult original source materials and qualified healthcare regulatory counsel for specific guidance in healthcare reimbursement and regulatory matters.
5

Carolyn St.Charles began her healthcare career as a staff nurse in Intensive Care. She has worked
in a variety of staff, administrative and consulting roles and has been a consultant with
HealthTechS3 for the last fifteenyears.
St.Charles conducts mock surveys for a variety of organizations including: Critical Access Hospitals,
Acute Care Hospitals, Long Term Care, Rural Health Clinics, Home Health and Hospice. Carolyn
also provides assistance in developing strategies for continuous survey readiness and developing
plans of correction.
Carolyn has extensive experience in working with rural hospitals to both develop and strengthen
SwingBed programs.
Carolyn has a B.S.N. from the University of Arizona, and a Masters of Business Administration
from the Foster School of Business at the University of Washington.
Email: [email protected]
Phone: 360-584-9868
6
Presenter

Clarifications – Before We Start!1. The CAH Annual Evaluation, C-0331 – C-0343 are still effective until March 30, 2021 – at which point the evaluation will be required
biennially. Coincides with implementation of QAPI date.
2. The requirements to provide dental care is still in the CAH and Hospital CoPs. (A-1573 and C-1624)
7

Regulatory Resources
• State Operations Manual Appendix W – Critical Access Hospitals Rev. 183, 10-12-18)
• State Operations Manual Appendix A – Hospitals (Rev. 183, 10-12-18)
• State Operations Manual Appendix PP – Long Term Care (Rev. 173, 11-22-17)(CAH Swing Bed still references Appendix PP)
• Omnibus Burden Reduction Final Rule CMS (Effective 11-29-19 except QAPI and Antibiotic Stewardship)o https://www.cms.gov/newsroom/fact-sheets/omnibus-burden-reduction-conditions-participation-final-rule-cms-3346-fo file:///C:/Users/carol/OneDrive/Documents/Resources/2019-20736%20Federal%20Register.pdf
• Omnibus Burden Reduction Final Rule CMS Discharge Planning (Effective 11-29-2019)o https://www.cms.gov/newsroom/fact-sheets/cms-discharge-planning-rule-supports-interoperability-and-patient-preferenceso file:///C:/Users/carol/OneDrive/Documents/Resources/2019-20732%20discharge%20planning%20rules.pdf
• APPENDIX A AND APPENDIX W – BUT NO INTERPRETATIVE GUIDELINES YETo https://www.cms.gov/files/document/burden-reduction-discharge-planning-som-package.pdf
8

Word(s) of Caution
State law may be more restrictive
Deeming authorities may have other requirements (TJC, DNV, HFAP)None (that I know of) have incorporated the new CMS regs. in their standards
Interpretative Guidelines have not been published
I’ve tried to capture the new regulations accurately – but PLEASE REVIEW
9

10

REVISED – Nursing Care Plan
A-0396 §482.23(b)(4) - The hospital must ensure that the nursing staff develops and keeps current a nursing care plan for each patient that reflects the patient’s goals and the nursing care to be provided to meet the patient’s needs. The nursing care plan may be part of an interdisciplinary care plan.
Interpretive Guidelines §482.23(b)(4) Nursing care planning starts upon admission. It includes planning the patient’s nursing care to meet the patient’s needs and interventions toward meeting patient treatment goals while in the hospital as well as planning for discharge to meet post-hospital needs. A nursing care plan is based on assessing the patient’s nursing care needs (not solely those needs related to the admitting diagnosis). The assessment considers the patient’s treatment goals and, as appropriate, physiological and psychosocial factors and patient discharge planning. The plan develops appropriate nursing interventions in response to the identified nursing care needs. The nursing care plan is kept current by ongoing assessments of the patient’s needs and of the patient’s response to interventions, assessment of patient treatment goals, and updating or revising the patient’s nursing care plan in response to assessments. The nursing care plan is part of the patient’s medical record and must comply with the medical records requirements at §482.24.
Hospitals have the flexibility of developing the nursing care plan as part of a larger, coordinated interdisciplinary plan of care. This method may serve to promote communication among disciplines and reinforce an integrated, multi-faceted approach to a patient’s care, resulting in better patient outcomes. The interdisciplinary plan of care does not minimize or eliminate the need for a nursing care plan. It does, however, serve to promote the collaboration between members of the patient’s health care team.
The required documentation for the nursing component of an interdisciplinary care plan remains the same. For other components, the hospital should follow the current documentation policies that it uses to document services provided by other disciplines, such as services provided by physical therapists, occupational therapists, speech-language pathologists, and others. Documentation should follow the standards of practice for those disciplines in addition to any specific requirements that the hospital might want to establish. The documentation must also comply with the requirements of the medical records requirement at §482.24. (77 FR 29049, May 16, 2012)
C-1050 (Rev. ) §485.635(d)(4) A nursing care plan must be developed and kept current for each inpatient.
Interpretive Guidelines §485.635(d)(4) There must be a nursing care plan for every CAH inpatient. Nursing care planning starts upon admission. It includes planning the patient’s care while in the CAH as well as planning for transfer to a hospital, to a post-acute care facility or for discharge. A nursing care plan is based on assessing the patient’s nursing care needs (not solely those needs related to the admitting diagnosis). The assessment considers the patient’s treatment goals and, as appropriate, physiological and psychosocial factors and patient discharge planning. The plan develops appropriate nursing interventions in response to the identified nursing care needs. One resource for information about nursing care plans is The American Nurses Association https://www.nursingworld.org/practice-policy/ workforce/what-is-nursing/the-nursing-process/.
The nursing care plan is kept current by ongoing assessments of the patient’s needs and of the patient’s response to interventions, and updating or revising the patient’s nursing care plan in response to assessments. The nursing care plan is part of the patient’s clinical record and must comply with the clinical records requirements at §485.638.
CAHs have the flexibility of developing the nursing care plan as part of a larger, coordinated interdisciplinary plan of care. This method may serve to promote communication among disciplines and reinforce an integrated, multi-faceted approach to a patient’s care, resulting in better patient outcomes. The interdisciplinary plan of care does not minimize or eliminate the need for a nursing care plan. It does, however, serve to promote the collaboration between members of the patient’s health care team.
11

Patient’s Discharge Planning Goal
A-0799 (Rev. ) §482.43 The hospital must have in effect a discharge planning process that focuses on the patient goals and treatment preferences and includes the patient and his or her caregivers support person(s) in the discharge planning for post-discharge care. The discharge planning process and the discharge plan must be consistent with the patient’s goals for care and his or her treatment preferences, ensure an effective transition of the patient from hospital to post-discharge care, and reduce the factors leading to a preventable hospital readmissions. .
.
C-1400 (Rev. ) §485.642 A Critical Access Hospital (CAH) must have an effective discharge planning process that focuses on the patient’s goals and treatment preferences and includes the patient and his or her caregivers/support person(s) as active partners in the discharge planning for post-discharge care. The discharge planning process and the discharge plan must be consistent with the patient’s goals for care and his or her treatment preferences, ensure an effective transition of the patient from the CAH to post discharge care, and reduce the factors leading to preventable CAH and hospital readmissions.
12
For Your ConsiderationMake sure you are documenting what the patient wants ---- NOT JUST WHAT THE CARE TEAM WANTS.

Discharge Planning For Everyone?
A-0800 (Rev. ) §482.43(a) (a) The hospital’s discharge planning process must identify at an early stage of hospitalization those patients who are likely to suffer adverse health consequences upon discharge in the absence of adequate discharge planning and must provide a discharge planning evaluation for those patients so identified as well as for other patients upon the request of the patient, patient’s representative, or patient’s physician.
A-0801 (Rev. ) §482.43(a)(4) (4) Upon the request of a patient’s physician, the hospital must arrange for the development and initial implementation of a discharge plan for the patient.
.
C-1404 (Rev. ) a)The CAH’s discharge planning process must identify, at an early stage of hospitalization, those patients who are likely to suffer adverse health consequences upon discharge in the absence of adequate discharge planning and must provide a discharge planning evaluation for those patients so identified as well as for other patients upon the request of the patient, patient’s representative, or patient’s physician.
C-1412 (Rev. ) (4) Upon the request of a patient’s physician, the CAH must arrange for the development and initial implementation of a discharge plan for the patient.
13
For Your ConsiderationHow will you identify patients, “who are likely to suffer adverse health consequences upon discharge”? This should be in policy.
Will you complete a discharge evaluation for ALL patients?

Services Needed – And Availability of Services
A-0805 (Rev. ) §482.43(a)(1) (1) Any discharge planning evaluation must be made in a timely basis to ensure the appropriate arrangements for post-hospital care will be made before discharge and to avoid unnecessary delays in discharge.
A-0807 (Rev. ) §482.43(a)(2) (2) A discharge planning evaluation must include an evaluation of a patient’s likely need for appropriate post-hospital services, including, but not limited to hospice care services, post-hospital extended care services, home health services, and non-health care services and community based care providers, and must also include a determination of the availability of the appropriate services as well as of the patient’s access to those services.
C-1406 (Rev. ) (1)Any discharge planning evaluation must be made on a timely basis to ensure that appropriate arrangements for post-CAH care will be made before discharge and to avoid unnecessary delays in discharge.
C-1408 (Rev. ) (2) A discharge planning evaluation must include an evaluation of a patient’s likely need for appropriate post-CAH services, including, but not limited to, hospice care services, post- CAH extended care services, home health services, and non-health care services and community based care providers, and must also include a determination of the availability of the appropriate services as well as of the patient’s access to those services.
14
For Your ConsiderationHow will you define timely?How will you provide patient’s information about available community resources – and provide them with a choice?

Can a RN Develop the Discharge Plan?
A-0809 (Rev. ) §482.43(a)(5)Any discharge planning evaluation or discharge plan under this paragraph must be developed by or under the supervision of a registered nurse, social worker, or other appropriately qualified personnel.
C-1417 (Rev. ) (5) Any discharge planning evaluation or discharge plan required under this paragraph must be developed by, or under the supervision of, a registered nurse, social worker, or other appropriately qualified personnel.
15
For Your ConsiderationMost organizations utilize a Discharge Planner and/or Social Worker with specific job responsibilities related to the discharge planning function.
However, this may not always be feasible due to:• Coverage on evenings / weekends• Short LOS when Discharge Planner is not available
There is no reason the RN caring for the patient cannot fulfill this function – at least for less complex patients. However – you will need to:• Include responsibilities in job description• Provide orientation• Develop and implement competencies
And ---- the RN is probably already performing some of the function as part of the initial nursing assessment.

Discharge Plan Re-Evaluation
A-0802 (Rev. ) §482.43(a)(6)(6) The hospital’s discharge planning process must require regular re-evaluation of the patient’s condition to identify changes that require modification of the discharge plan. The discharge plan must be updated, as needed, to reflect these changes.
A-0808 (Rev. ) §482.43(a)(3) (3) The discharge planning evaluation must be included in the patient’s medical record for use in establishing an appropriate discharge plan and the results of the evaluation must be discussed with the patient (or the patient’s representative).
C-1420 (Rev. ) (6) The CAH’s discharge planning process must require regular reevaluation of the patient’s condition to identify changes that require modification of the discharge plan. The discharge plan must be updated, as needed, to reflect these changes.
C-1410 (Rev. ) (3) The discharge planning evaluation must be included in the patient’s medical record for use in establishing an appropriate discharge plan and the results of the evaluation must be discussed with the patient (or the patient’s representative).
16
For Your ConsiderationMost hospital’s have multi-disciplinary rounds (sometimes daily). MAKE sure you document that the discharge needs have been both developed – and re-evaluated – and that you document discussions with the patient or patient’s representative.

Discharge and Provision of Necessary Medical Information
A-0813 (Rev. ) §482.43(b) The hospital must discharge the patient , and also transfer or refer the patient where applicable, along with all necessary medical information pertaining to the patient’s current course of illness and treatment, post-discharge goals of care, and treatment preferences, at the time of discharge, to the appropriate post-acute care service providers and suppliers, facilities, agencies, and other outpatient service providers and practitioners responsible for the patient’s follow-up or ancillary care.
C-1430 (Rev. ) The CAH must discharge the patient, and also transfer or refer the patient where applicable, along with all necessary medical information pertaining to the patient’s current course of illness and treatment, post discharge goals of care, and treatment preferences, at the time of discharge, to the appropriate post acute care service providers and suppliers, facilities, agencies, and other outpatient service providers and practitioners responsible for the patient’s follow-up or ancillary care.
17
For Your ConsiderationEnsure you have a reliable process for disseminating information, including to the physician responsible for follow-up care.
IF the physician office has access to your EMR – make sure they know the patient was in the hospital.

Discharge / Readmit to Swing18
Source: Federal Register
Comment: One commenter requested that CMS create an exception for real time discharge summaries for transfers from acute care to SNF facilities. The commenter noted that while it is essential to know a patient’s medical and treatment history, the discharge summary requirement does not make sense if information is being sent when the transfer is from the ‘‘doctor to him or herself’’ and from the ‘‘nurse to the same nurse.’’ The commenter further pointed out that this may be an issue in rural communities, where the practitioners are the same on either side of the transfer.
Response: We understand the commenter’s concerns about a repetitive or time consuming process for rural or small hospitals or CAHs, particularly when the services being provided to the patient changes from acute inpatient to swing bed. We note that the discharge planning process does apply to patients whose status changes from acute inpatient to swing bed services.
For Your ConsiderationDon’t forget that the discharge regulations apply to Swing Bed too! Even when you admit to Swing Bed from your own facility.

Selection of PAC Provider
A-0804 (Rev. ) §482.43(a)(8)(8) The hospital must assist patients, their families, or the patient’s representative in selecting a post-acute care provider by using and sharing data that includes, but not limited to, HHA, SNF, IRF, or LTCH data on quality measures and data on resource use on measures. The hospital must ensure that the post-acute care data on quality measures and data on resource measures is relevant and applicable to the patient’s goals and treatment preferences.
C-1425 (Rev. ) (8) The CAH must assist patients, their families, or the patient’s representative in selecting a post-acute care provider by using and sharing data that includes, but is not limited to, HHA, SNF, IRF, or LTCH data on quality measures and data on resource use measures. The CAH must ensure that the post-acute care data on quality measures and data on resource use measures is relevant and applicable to the patient’s goals of care and treatment preferences.
19

Patient Choice of Post Acute Care ProvidersA-0815 (Rev. ) §482.43(c)(1)The hospital must include the discharge planning a list of HHA’s, SNF’s, IRF’s, or LTCH’s that are available to the patient, that are participating in the Medicare program, and that serve the geographic area (as defined by the HHA) in which the patient resides, or in the case of a SNF, IRF, or LTCH, in the geographic area requested by the patient. HHAs must request to be listed by the hospital as available.
(i) The list must only be presented to patients for whom home health care post hospital extended care services, SNF, IRF, or LTCH services are indicated and appropriate as determined by the discharge planning evaluation. (ii) For patients enrolled in managed care organizations, the hospital must make the patient aware of the need to verify with their managed care organization which practitioners, providers or certified suppliers are in the network of the patient’s managed careorganization, it must share this with the patient or the patient’s representative. (iii) [The hospital must] document in the patient’s medical record that the list was presented to the patient or to the patient’s representative
A-0816 (Rev. ) §482.43(c)(2) The hospital , as part of the discharge planning process, must inform the patient or the patient’s representative of their freedom to choose among participating Medicare providers and suppliers of the post-discharge services and must, when possible, respect the patient’s or the patient’s representative goals of care and treatment preferences, as well as other preferences they express. The hospital must not specify or otherwise limit the qualified providers or suppliers that are available to the patients. .
A-0817 (Rev. ) §482.43(c)(3) The discharge plan must identify any HHA or SNF to which the patient is referred in which the hospital has a disclosable financial interest, as specified by the Secretary, and any HHA or SNF that has a disclosable financial interest in a hospital under Medicare. Financial interests that are disclosable under Medicare are determined in accordance with the provisions of part 420, subpart C, of this chapter.
A-0815, A-0816 and A-0817 do not have comparable tags to Appendix W.
However my recommendation is to implement the Appendix A requirements..
20

Post Acute Care Quality Measures21
Source: Federal Register
New discharge planning requirements, as mandated by the IMPACT act for hospitals, HHAs, and CAHs, that requires facilities to assist patients, their families, or the patient’s representative in selecting a post-acute care (PAC) services provider or supplier by using and sharing PAC data on quality measures and resource use measures.
This data must be relevant and applicable to the patient’s goals of care and treatment preferences.
We would also expect the hospital – CAH – HHA - to document in the medical record that the PAC data on quality measures and resource use measures were shared with the patient and used to assist the patient during the discharge planning process.
We believe that providers have the ability and knowledge to interpret and discuss the publicly available data on quality and resource use measures at the most basic levels. We note that we do not expect providers to give overly detailed and complex analyses of the quality and resource use data, which may only service to confuse patients and/or their caregivers, nor do we expect providers to attempt to provide patients and their caregivers with data that do not exist regarding PAC facilities. We expect providers to put forth their best effort to answer patient questions regarding the data.

Post Acute Care Quality Measures22
Federal Register
Comment: One commenter stated that the requirement to utilize data on quality measures and data on resource use measures could be utilized to discourage the use of CAH swing beds in rural communities. Since the CAH swing bed program does not have to report data on its performance, referring facilities will list CAH Swing Bed on their referral list delivered to patients, but would have no data to include on the list. The commenter suggested that we require referring facilities to note on their discharge provider list that CAH swing beds are not required to report data similar to freestanding SNFs.
Response: The CAH’s responsibility is to advise and assist patients with their choices based on quality data and the patient’s goals of care and treatment preferences. As such, we do not believe that any provider will be disadvantaged with this requirement.

Post-Acute Quality Initiatives Home Page23
Welcome to the Post-Acute Quality Initiatives Home Page – August 13, 2018We have updated the webpages for the IMPACT Act with up-to-date information pertaining to quality measures and activities associated with data standardization as required under the IMPACT Act of 2014. For upcoming stakeholder engagement opportunities and general announcements, refer to the IMPACT Act of 2014 Spotlight Announcements & Opportunities for
General Information:This webpage is intended to provide information pertaining to the Centers for Medicare & Medicaid Services (CMS)-related quality improvement initiatives. This site will serve as a general information platform for information for all stakeholders, including the public.
About CMS' Quality Initiatives:Quality health care for people with Medicare is a high priority for the President, the Department of Health and Human Services (HHS), and the Centers for Medicare & Medicaid Services (CMS). HHS and CMS began launching quality initiatives in 2001 to assure quality health care for all Americans through accountability and public reporting. Various quality initiatives touch every aspect of the healthcare system. Some initiatives focus on publicly reporting quality measures for settings such as nursing homes, home health agencies and dialysis facilities. Consumers can use the quality measures information that is available on www.medicare.gov for these healthcare settings to assist them in making healthcare choices or decisions.As CMS moves forward with its strategies to facilitate quality measurement and quality improvement across multiple settings, this site will serve as a guide for post-acute care measurement development-related information.
About Reports and Links:We intend to provide reports on this site that we hope will serve as an opportunity to educate and inform the public about work related to various quality initiatives. The bottom section of the page will provide these reports as downloads. In addition, we will provide links to other websites for additional information related to quality initiatives. Please know that although this site may not be able to serve as an exhaustive resource, we are looking forward to providing information related to quality initiatives that may span several settings so that you are able to find materials in one location. As materials are added related to our various, quality initiatives, CMS expects that sub-pages will be added to this webpage.We encourage readers to browse the page, including downloads and links, frequently for materials and information, as well as web page enhancements and updates.

Sources of Post Acute Care Quality Measures24
Nursing Home Comparehttps://www.medicare.gov/nursinghomecompare/search.html
Hospital Comparehttps://www.medicare.gov/hospitalcompare/search.html
Inpatient Rehabhttps://www.medicare.gov/inpatientrehabilitationfacilitycompare
Home Health Compare (SNF)https://www.medicare.gov/homehealthcompare/search.html
Long Term Care Hospitalhttps://www.medicare.gov/longtermcarehospitalcompare

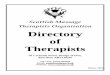
Example PAC Quality Measures25
Nursing Home Results44 nursing homes within 50 miles from the center of 98502
Name Overall Rating Health Inspections Staffing Quality Measures Distance
Puget Sound Healthcare Center
Regency Olympia Rehabilitation and Nursing Center
Providence Mother Joseph Care
vvc

For Your Consideration26
❑ Develop a list of “referral” PACs (including your hospital swing bed)
❑ HHAs must request to be listed by the hospital ---- ask if they want to be included
❑ Access Quality Data from CMS web site(s)
❑ Develop template information for patients with both choice of facilities and corresponding PAC datao Decide how you are going to provide PAC data on your swing bed program
❑ Develop documentation templates to include verification that information was provided to the patient --- and their choice of PAC
❑ Identify who is responsible in your organization for compiling and providing data to patients
❑ Educate staff and providers on new process
❑ Audit for compliance
❑ Identify frequency that data is updated for each PAC on CMS web site – and ensure the data you are providing patients is the most “current”

Assessment of Discharge Planning Processes
A-0803 (Rev. ) §482.43(a)(7)(7) The hospital must assess its discharge planning process on a regular basis. The assessment must include ongoing, periodic review of a representative sample of discharge plans, including those patients who were admitted within 30 days of a previous admission, to ensure that the plans are responsive to the patient post-discharge needs.
C-1422 (Rev. ) (7) The CAH must assess its discharge planning process on a regular basis. The assessment must include ongoing, periodic review of a representative sample of discharge plans, including those patients who were readmitted within 30 days of a previous admission, to ensure that the plans are responsive to patient post-discharge needs.
27
For Your Consideration❑ Include a representative sample of ALL discharge plans – not just patients who are readmitted (which you are probably already reviewing)❑ Develop criteria for auditing, frequency of auditing and sample size (Representative sample should include a minimum of 30 records)❑ Identify WHO will complete the audits and analyze the data❑ Determine where data will be reported

Readmission Audit
1. Date of Acute Care Admission
2. Reason for Acute Care Admission
3. Length of Stay in Acute Care
4. Reason for Swing Bed admission, if applicable
5. Length of Stay in Swing Bes, if applicable
6. Complications that occurred during the hospitalization to
extend Length of Stay
7. Discharge disposition (place)
8. Discharge plan in place (Yes/No)
9. Post-hospital support services / systems in place
10.Reason for readmission
11.Readmission Length of Stay
12.Post-readmission discharge disposition
13.Was the post-readmission discharge disposition the same
as the initial discharge disposition
14.What could have been done differently to prevent the
readmission? (Think ROOT Cause / Failure Mode
analysis)
2828
DO NOT USE RATE BASE ADMISSION DATACOUNT AND REPORT EVERY READMISSION

Discharge Planning Sample Audit Tool29
Audit Criteria NA YES NO UNSUREMAYBE
COMMENTS
1 C-1400: Are patient’s discharge goals documented?
2 C-1400: Is the discharge plan documented by the provider consistent with the patient’s goals?
3 C-1400: Is the discharge plan documented by the care team consistent with the patient’s goals?
4 C-1404: Is there evidence that the patient has the potential to suffer adverse health consequences upon discharge?
5 C-1404: Was a discharge plan developed for the patient with the potential to suffer adverse health consequences upon discharge?
6 C-1404: If there was a request for a discharge plan by the patient, patient’s representative, or physician, was a discharge plan developed and implemented?
7 C-1406: Was the discharge planning evaluation timely? (within 24 hours of admission)
8 C-1406: Did the discharge planning evaluation include an evaluation of a patient’s likely need for post-hospital services, including, but not limited to, hospice, extended care, home health, and other community based providers like Meals on Wheels, Housekeeping Services, etc.?

Discharge Planning Sample Audit Tool30
Audit Criteria NA YES NO UNSUREMAYBE
COMMENTS
9 C-1406: If services are needed post-discharge was the availability of the services determined?
10 C-1410: Is the discharge assessment documented in the medical record?
11 C-1410: Does the medical record include documentation that the discharge assessment, plan and any reassessment was discussed with the patient?
12 C-1420: Was the patient regularly re-evaluated to identify changes that require modification in the discharge plan.
13 C-1420: If modifications were needed to the discharge plan, was it documented and discussed with the patient, patient’s representative, or physician?
14 C-1430: When the patient was transferred was all applicable medical information provided to the appropriate post-acute provider?
15 C-1425: Was the patient given a choice of post acute care providers including information about quality and resource use measures?
16 C-1425: Was the patient’s choice of post acute providers documented?
17 C-1422: Was the patient readmitted within 30 days of discharge from acute care or swing bed?

Discharge Planning Swing Bed – NOT NEW LANGUAGE
Hospitals with a Swing Bed Program utilize the RAI.
C-1620 (Rev. ) §485.645(d)(5) Comprehensive assessment, comprehensive care plan, and discharge planning§483.20(b) Comprehensive assessments—(1) Resident assessment instrument. A facility must make a comprehensive assessment of a resident's needs, strengths, goals, life history and preferences, using the resident assessment instrument (RAI) specified by CMS. (RAI not required for CAHs.) The assessment must include at least the following: (xvi) Discharge planning.
§483.21(b) Comprehensive care plans. (1) The facility must develop and implement a comprehensive person-centered care plan for each resident, consistent with the resident rights set forth at §483.10(c)(2) and §483.10(c)(3), that includes measurable objectives and timeframes to meet a resident's medical, nursing, and mental and psychosocial needs that are identified in the comprehensive assessment. The comprehensive care plan must describe the following: (7) In consultation with the resident and the resident's representative(s)—(A) The resident's goals for admission and desired outcomes. (B) The resident's preference and potential for future discharge. Facilities must document whether the resident's desire to return to the community was assessed and any referrals to local contact agencies and/or other appropriate entities, for this purpose. (C) Discharge plans in the comprehensive care plan, as appropriate, in accordance with the requirements set forth in paragraph (c) of this section.
31

Discharge Planning Swing Bed – NOT NEW LANGUAGE
A-1569 (Rev.) §482.58(b)(5) Discharge summary (§483.20(l)) “When the facility anticipates discharge a resident must have a discharge summary that includes, but is not limited to: (i) A recapitulation of the resident’s stay that includes, but is not
limited to, diagnoses, course of illness/treatment or therapy, and pertinent lab, radiology, and consultation results.
(ii) A final summary of the resident’s status to include items in paragraph (b)(2) of §483.20, at the time of the discharge that is available for release to authorized persons and agencies, with the consent of the resident or legal representative.
(iii) Reconciliation of all pre-discharge medications with the resident's post-discharge medications (both prescribed and over-the-counter).
(iv) A post-discharge plan of care that is developed with the participation of the resident and, with the resident’s consent, the resident representative(s), which will assist the resident to adjust to his or her new living environment. The post-discharge plan of care must indicate where the individual plans to reside, any arrangements that have been made for the resident's follow up care and any post-discharge medical and non-medical services.”]
§483.21(c)(2) Discharge summary. When the facility anticipates discharge a resident must have a discharge summary that includes, but is not limited to, the following: (i) A recapitulation of the resident's stay that includes, but is not limited to, diagnoses, course of illness/treatment or therapy, and pertinent lab, radiology, and consultation results. (ii) A final summary of the resident's status to include items in paragraph (b)(1) of §483.20, at the time of the discharge that is available for release to authorized persons and agencies, with the consent of the resident or resident's representative. (iii) Reconciliation of all pre-discharge medications with the resident's post-discharge medications (both prescribed and over-the-counter). (iv) A post-discharge plan of care that is developed with the participation of the resident and, with the resident's consent, the resident representative(s), which will assist the resident to adjust to his or her new living environment. The post-discharge plan of care must indicate where the individual plans to reside, any arrangements that have been made for the resident's follow up care and any post-discharge medical and non-medical services.
32

Next Steps1. Review the regulations
2. Complete a gap analysis – you may have many things in place already
3. Develop an action plan with timelines and accountabilities – and implement your plan
4. Audit your processes
33

34

If you are interested in a Hospital mock survey or a Swing Bed mock
survey, please contact me.
Carolyn St.Charles [email protected]
Office: 360-584-9868Cell: 206-605-3748