Embed Size (px)
Citation preview

Nelly Ziade-Zoghbi, MD, MPH
Rheumatology department, Hotel-Dieu de France
IV therapy for radicular pain
A literature review and retrospective analysis of a case series at HDF

1- Literature review of IV treatments in radiculopathies
2- Case series at HDF: IV pentoxifylline in radiculopathies
Agenda2

1- Literature review of IV treatments in radiculopathies
2- Case series at HDF: IV pentoxifylline in radiculopathies
Agenda3

4
www.pubmed.com

NSAIDs
Ketoprofene 100 mg / 8hrs for 3 days transcient effect
5
Etienne JC. Gaz Med 1986

Corticosteroids
RCT, sciatica < 6 weeks 65 patients
High-dose pulse methylprednisolone (500mg)
Transcient effect / small magnitude No effect on functional disability
6
Finckh et al, Spine 2006

Anti-TNF alpha
Role of anti-TNF alpha in the pathogenesis of the disco-radicular conflict
[Rannou F, Revel M. L’actualite rhumatologique 2005] [Mulleman et al. Joint Bone Spine 2006]
One RCT: 40 pts suffering from LS (2-12 wks) one infliximab infusion 1-year follow-up Improvement 67% versus 63% (p 0.72) Benefit+with Modic changes at symptomatic level 20% surgery
[Korhonen, Spine 2005]
7

What about Pentoxifyllin?
PTX is a PDE4 inhibitor increasing intracellular cAMP and stimulating PKA activity.
Primary actions: PTX increases red blood cell deformability, reduces blood viscosity and decreases the potential for platelet aggregation and thrombus formation
It is also a known inhibitor of TNF-alpha
8
Marques et al. Am J Respir Critic Care Med 1999

Evidence from PTX
Effects in experimental nerve injury Intraperitoneal PTX in rats with crushed
sciatic nerve Electrophysiologic studies 3 weeks later:
better amplitudes of compound muscle action potentials
Suggests positive effect on axon regeneration
9
Baykal el al. Turk J Med Sci 2002.

Evidence from PTX
Effects on nerve conduction velocity and blood flow in diabetic rats 2 weeks PTX Diabetic deficits in sciatic motor and
saphenous sensory nerve conduction velocity were 56.5% and 69.8% corrected, respectively
Sciatic endoneurial blood flow was 50.4% corrected
10
Flint et al. Int J Experimental Diab Res 2000

1- Literature review of IV treatments in radiculopathies
2- Case series at HDF: IV pentoxifylline in radiculopathies
Agenda11
12

Baseline demographic characteristics
Age in years (SD) 57.64 (13.68 )
Male sex 8 [28.6%]
Smoking 4 [14.3%]
Diabetes 3 [10.7%]
13
Baseline clinical characteristics
Duration of symptoms in weeks [range]
45.68 [2-160]
SLR (Lasegue) sign < 30 degrees 6 [21%]
Controlateral SLR (Lasegue) sign < 30 degrees 2 [7%]
Sensory deficit 3 [11%]
Motor deficit (but => 3/5) 12 [43%]
Urine incontinence 2 [7%]
At least one reflex absent 10 [36%]
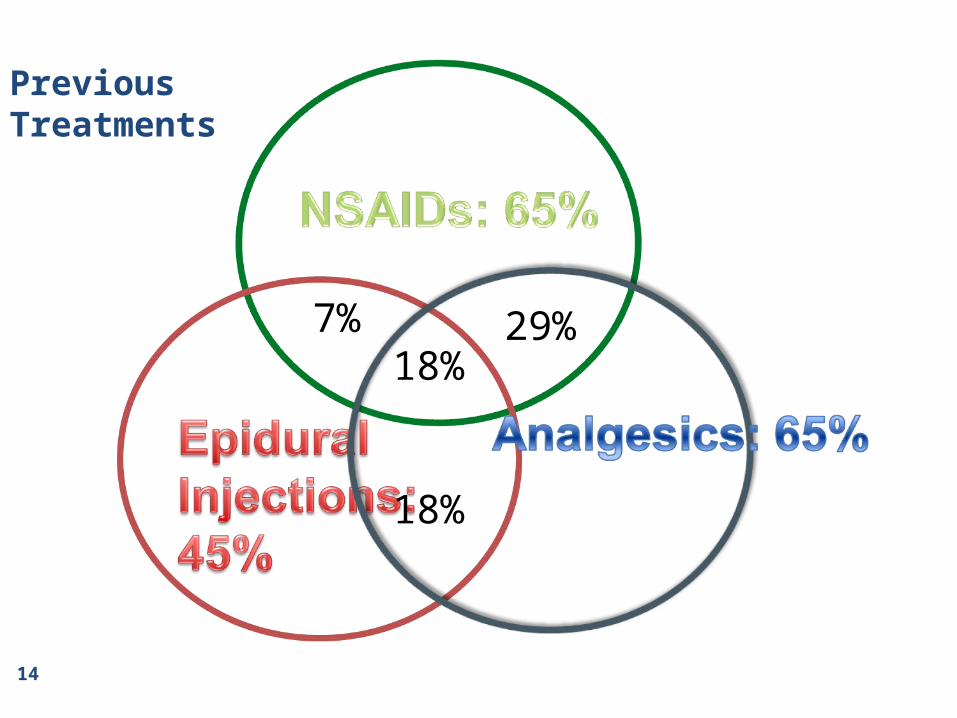
29%
18%
7%18%
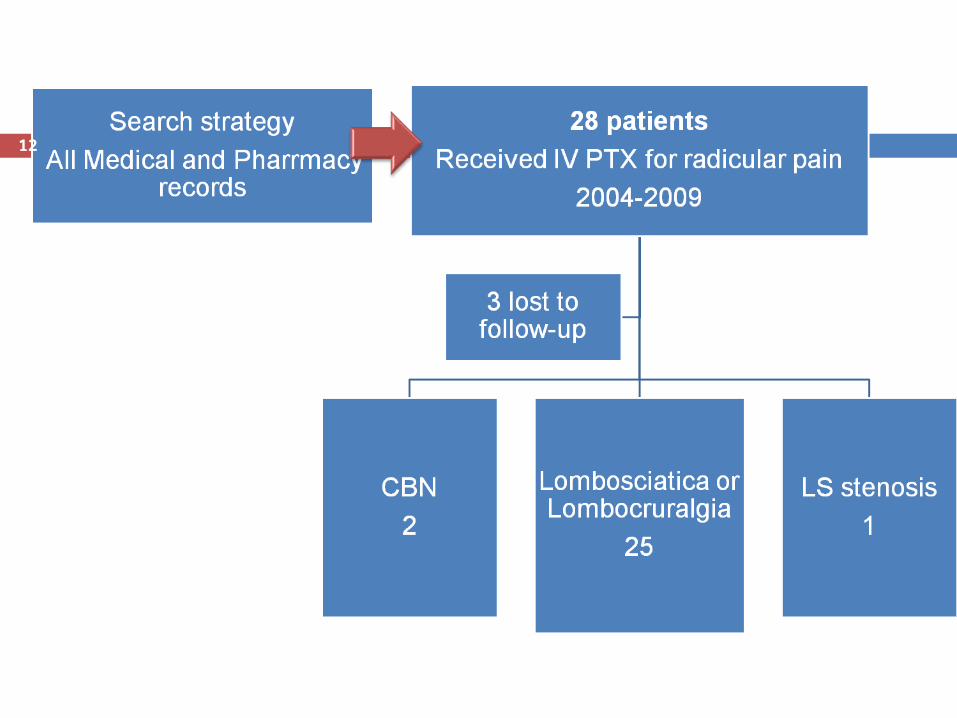
14
PreviousTreatments

Protocols
Protocol N (%)
PTX 900 mg/day IV for 3 days followed by 1200 mg po /day
13 (46.4%)
PTX 900 mg/day IV for 4 days followed by 1200 mg po /day
3 (10.7%)
PTX 900 mg/day IV for 5 days followed by 1200 mg po /day
8 (29%)
PTX 900 mg/day IV for 3 or 4 days 4 (14.3%)Associated treatment N (%)
NSAIDs 14 (50%)
Analgesics 19 (67.8%)
Muscle relaxants 6 (21.4%)
Local injections (epidural / foraminal) 10 (35.7%)
Corticosteroids (oral / IV) 7 (25%)
15

Δ VAS (%)
-60
-50
-40
-30
-20
-10
0
Δ VAS radicular pain Δ VAS back pain
Immediately
At one month
Last Follow-up
16
38 months[3-84]

VAS response categories over time
0%
20%
40%
60%
80%
100%
Immediately At one month Last Follow-up
80-100%
60-79%
40-59%
20-39%
0-19%
17

Outcomes
Mean time to improvement
N (SD)
2.2 weeks (3.1)(36% in the following
week)
Mean time to returning to normal activities
3.56 weeks (4.1)
Willingness to repeat treatment if needed
48%
Surgery during follow-up 4 patients (14%)
18

Adverse events
AE N (%) N leading to discontinuation
Nausea / Vomiting
6 (21%) 1
Hypotension 3 (11%) 1
Tremor 1 (4%) 0
Skin rash (1) 4% 1
Fatigue (2) 7% 0
At least one AE
9 (32%) 3 (11%)
19
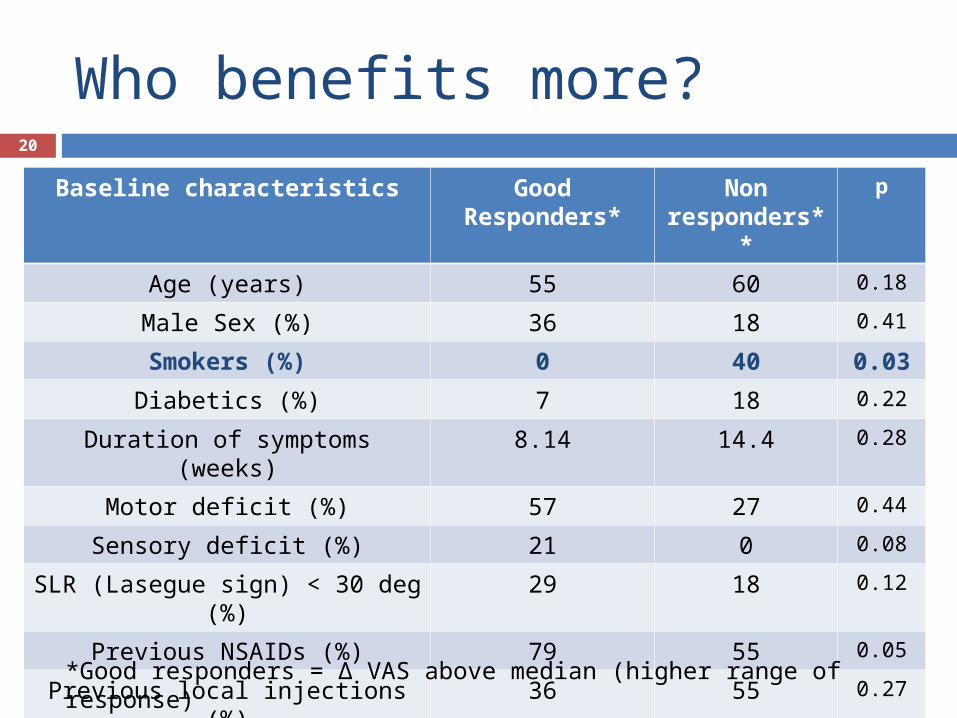
Who benefits more?
Baseline characteristics Good Responders*
Non responders
**
p
Age (years) 55 60 0.18
Male Sex (%) 36 18 0.41
Smokers (%) 0 40 0.03
Diabetics (%) 7 18 0.22
Duration of symptoms (weeks) 8.14 14.4 0.28
Motor deficit (%) 57 27 0.44
Sensory deficit (%) 21 0 0.08
SLR (Lasegue sign) < 30 deg (%)
29 18 0.12
Previous NSAIDs (%) 79 55 0.05
Previous local injections (%) 36 55 0.27
20
*Good responders = Δ VAS above median (higher range of response)**Non-responders = Δ VAS below median
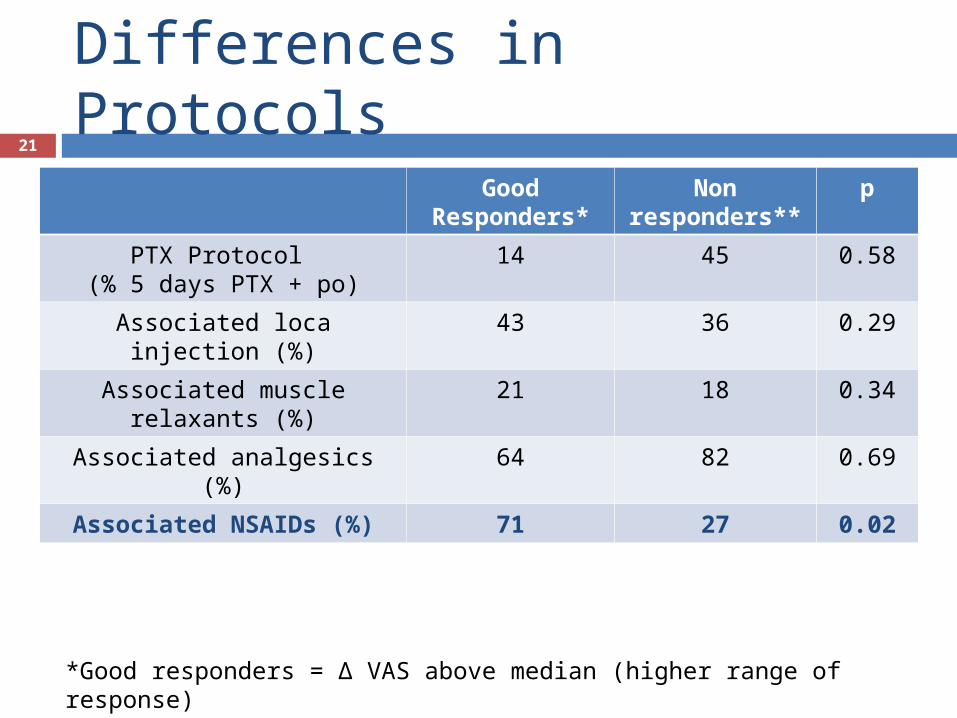
Differences in Protocols
Good Responders*
Non responders**
p
PTX Protocol (% 5 days PTX + po)
14 45 0.58
Associated loca injection (%) 43 36 0.29
Associated muscle relaxants (%)
21 18 0.34
Associated analgesics (%) 64 82 0.69
Associated NSAIDs (%) 71 27 0.02
21
*Good responders = Δ VAS above median (higher range of response)**Non-responders = Δ VAS below median

Role of associated NSAIDsBaseline characteristics NSAIDs + (14
pts)NSAIDs – (14
pts)P
Age (years) 53.43 61.86 0.10
Male Sex (%) 43 14 0.21
Smokers (%) 21 7 0.60
Diabetics (%) 7 14 0.33
Duration of symptoms (weeks) 7.29 15.57 0.16
Motor deficit (%) 29 57 0.25
Sensory deficit (%) 14 7 0.38
Lasegue sign < 30 deg (%) 36 7 0.17
Previous NSAIDs (%) 86 43 0.04
Previous epidural inj (mean nb) 36 50 0.70
22
Outcomes NSAIDs + NSAIDs - p
Δ VAS radicular pain (immediate) -53.85% -40.83% 0.77
Δ VAS radicular pain (at one month) -66.15% -45.42% 0.45
Δ VAS radicular pain (last follow-up) -72.69% -32.50% 0.02

Summary of main results
Δ VAS radicular pain around 50% (immediate and late response)
Good responders tend to be younger, male and non-smokers
Response at least partially explained by associated / previous NSAIDs
23

Study limitations
Retrospective analysis (recall bias) Small number of patients Different treatment protocols Different treatments associations (open study) No placebo arm / No blinded treatment
24

Study strenghts
Very few lost to follow-up (10.7%)
Evaluation of initial hospital chart + telephone contact with patients
Careful identification of all associated treatments
Careful identification of tolerability profile
25

Conclusion
Need in practice for a safe and efficacious treatment in resistant radiculopathies
Pentoxifylline / Anti-TNF family needs further dedicated well-designed studies, that takes into account associated treatments, especially NSAIDs
26

Thank you for your attention

28
Back-up29

Immediate response
Baseline characteristics Good Responders*
Non responders
**
p
Age (years) 57 57.8
Male Sex (%) 20 40
Smokers (%) 0 40
Diabetics (%) 13 10
Duration of symptoms (weeks) 10.8 11.1
Motor deficit (%) 73 0
Sensory deficit (%) 20 0
Lasegue sign < 30 deg (%) 7 50
Previous NSAIDs (%) 60 80
Previous epidural inj 47 40
30
*Good responders = Δ VAS above median (higher range of response)**Non-responders = Δ VAS below median

Immediate response
Good Responders*
Non responders**
p
PTX Protocol (5 days PTX + po)
20 36
Associated Epidural injection
33 50
Associated NSAIDs 47 60
Associated muscle relaxants
13 30
Associated analgesics 60 90
31
*Good responders = Δ VAS above median (higher range of response)**Non-responders = Δ VAS below median

One month response
Baseline characteristics Good Responders*
Non responders
**
p
Age (years) 53.60 61.33
Male Sex (%) 31 25
Smokers (%) 0 33
Diabetics (%) 8 17
Duration of symptoms (weeks) 11.23 10.58
Motor deficit (%) 69 17
Sensory deficit (%) 23 0
Lasegue sign < 30 deg (%) 15 33
Previous NSAIDs (%) 77 58
Previous epidural inj (mean nb) 38 50
32
*Good responders = Δ VAS above median (higher range of response)**Non-responders = Δ VAS below median
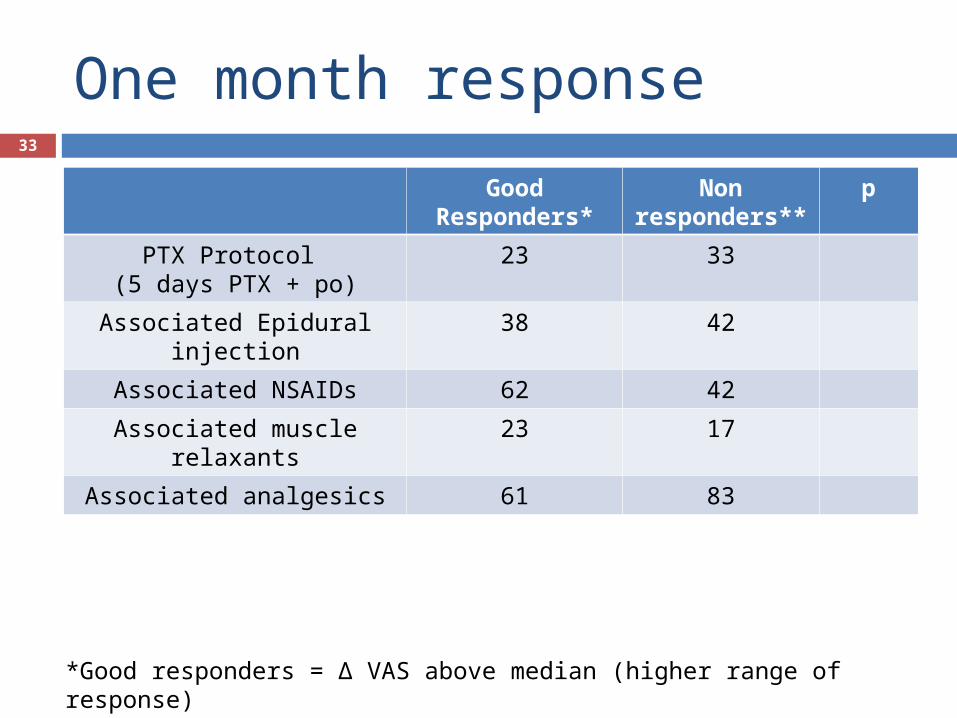
One month response
Good Responders*
Non responders**
p
PTX Protocol (5 days PTX + po)
23 33
Associated Epidural injection
38 42
Associated NSAIDs 62 42
Associated muscle relaxants
23 17
Associated analgesics 61 83
33
*Good responders = Δ VAS above median (higher range of response)**Non-responders = Δ VAS below median

Who benefits more?
Baseline characteristics Good Responders*
Non responders
**
p
Age (years) 55.3 57.9 0.64
Male Sex (%) 36 20 0.4
Smokers (%) 0 40 0.0095
Diabetics (%) 7 10 0.8
Duration of symptoms (weeks) 8.14 11.9 0.55
Motor deficit (%) 57 20 0.068
Sensory deficit (%) 21 0 0.11
Lasegue sign < 30 deg (%) 20 29 0.77
Previous NSAIDs (%) 79 60 0.32
Previous epidural inj (mean nb) 0.79 1.7 0.51*Good responders = Δ VAS above median (higher range of response)**Non-responders = Δ VAS below median
34

Differences in protocols
Good Responders*
Non responders**
p
PTX Protocol (5 days PTX + po)
14% 50% 0.17
Associated Epidural injection
43% 30% 0.52
Associated NSAIDs 71% 30% 0.044
Associated muscle relaxants
21% 20% 0.93
Associated analgesics 64% 90% 0.15
35

Mean Δ VAS radicular pain: No increase in response with PTX dose
36

Median ΔVAS response over time
37
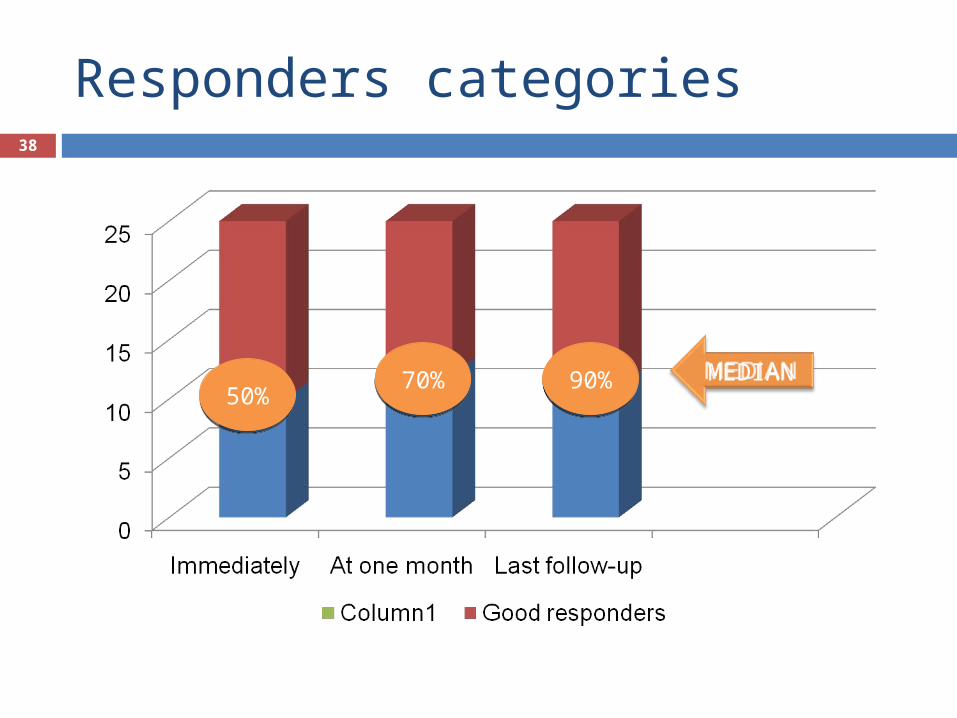
Responders categories38
MEDIAN50%50%
90%90%
70%70%









![Quiste Radicular[1]](https://img.dokumen.tips/doc/110x75/557211e7497959fc0b8fad33/quiste-radicular1.jpg)