Embed Size (px)
Citation preview
M ultim oda lity Therapy for Med ullo blastorn a
PATRICK R. M. THOMAS, MB, MRCP, FRCR,* PATRICIA K. DUFFNER, MD,t MICHAEL E. COHEN, MD,+ LUClUS F. SINKS, MD,§ CAMERON TEBBI, MD," ARNOLD I . FREEMAN, MD#
Eight patients with recurrent medulloblastoma were treated with a chemotherapy regimen consisting of vincristine, BCNU, dexamethasone and intrathecal and intermediate dose intravenous methotrexate (500 mg/m2). Five also received local low dose radiotherapy (RT). All 8 patients responded to treatment; 6 completely and 2 partially. These latter 2 were in their second and third recurrences. Three remain in remission. The median duration of response was 18.8 months, and median time from start of chemo- therapy to death was 32 months using the Kaplan-Meier technique.
In addition, 9 other patients with newly diagnosed medulloblastoma were treated with craniospinal radiation and the same adjuvant chemotherapy as above. The first 5 patients also received intraventricular methotrexate and/or intravenous BCNU during radiotherapy. The toxicity in the 5 patients was very severe. There were three toxic deaths, one death from cancer; one patient survives disease-free, but he is demented. With the discontinuance of intraventricular methotrexate and the postponement of myelo- suppressive chemotherapy until after the completion of radiotherapy, the regimen has been well tolerated. A11 4 patients treated this way remain alive, well, and disease-free at intervals up to 36 months.
We conclude that recurrent medulloblastomas are sensitive to multiagent chemotherapy and that prolonged remissions may occur. With primary adjuvant chemotherapy, extreme caution with myelo- suppressive drugs must be exercised during the period of craniospinal radiotherapy. We also do not recommend the use of intraventricular methotrexate. When these two criteria were followed, the preliminary results with adjuvant chemotherapy appear encouraging.
Cancer 45:666-669, 1980.
URGERY ALONE cannot cure medullobl?stoma. S Indeed, Bailey and Cushing, who coined the name for this tumor in 1924, recognized this and noted that the optimum management consisted of suboccipital decompression followed by radiotherapy.
Irradiation to the entire central nervous system (CNS) using modern equipment and dosimetry has resulted in a disease free survival rate of approximately
Supported in part by the Association for the Research of Childhood Cancer (AROCC), Buffalo, New York.
* Associate Chief, Department of Radiation Medicine, Roswell Park Memorial Institute, Buffalo, New York.
t Assistant Professor of Neurology and Pediatrics, State University of New York at Buffalo. School of Medicine and Buffalo Children's Hospital, Buffalo, New York.
i Associate Professor of Neurology and Pediatrics, State Univer- sity of New York at Buffalo, School of Medicine and Buffalo Chil- dren's Hospital, Buffidfalo, New York.
5 Chief, Pediatric and Adolescent Oncology, Vince Lombardi Cancer Research. Georgetown University, Washington, D. C.'
I' Associate Chief, Department of Pediatrics, Roswell Park Memorial Institute. Buffalo, New York.
# Chief, Department of Pediatrics, Roswell Park Memorial Insti- tute, Buffalo, New York.
Address for reprints: A. I. Freeman, MD, Department of Pedi- atrics, Roswell Park Memorial Institute, 666 Elm Street, Buffalo, NY 14263.
The authors thank Dr. M. Pagano for statistical advice. Accepted for piiblication March 2, 1979.
40 percent at five year^^.^,^ although the occasional small series has produced better figures." It is there- fore clear that a cure can be obtained by radiotherapy alone.
However, it appeared unlikely that modification in radiation dosage and technique would result in a marked improvement in the rate of cure, and since patients with medulloblastoma were theoretically good candi- dates for a chemotherapeutic approach,1° we began, in 1969, to investigate the role of chemotherapy in this disease.
We have previously reported5 the results of multi- agent chemotherapy in 5 patients with recurrent medul- loblastoma. The current paper updates these results as of December 1978 and broadens the observation to include 8 patients with recurrent disease. In addition, we are reporting the results in nine children who re- ceived primary adjuvant chemotherapy and radiotherapy.
Patients and Methods
Guoi4p I-Recurrent Merlullnblnstornas (Putietlt.5 1-8)
Eight patients with evidence of recurrent medullo- blastorna were treated with multiagent chemotherapy.
0008-543X/80/02 1.510666 $0.70 Q American Cancer Society
666

No. 4 MULTIMODALITY THEKAPY . Thornus et ( i l . 667
T . Z R L ~ 1. Clinical Details-Recurrent Medulloblastomas (Group I)
Initial post. fossa Patient Age at Initial radiotherapy dosei Site of Therapy following
no. Sex diagnosis therapy wks. of treatment recurrence recurrence
14 S + R?' 15 10 s + RI' I5 S + RT 3 S + RT 8 S A RT 3 S + RT
23 S + RT
S + Sh T RT 400019 480017 350019 500018 300014 175013 372013 5835i7
P F PF + SC PF PF PF PF + SC PF + SC Hypothalamus
CT Laminectomy &r C T Shunt & CT Shunt & CT Surgery and RT + CT RT + C T RT + CT RT + CT
S = surgery: Sh = shunt; R.T = radiotherapy; PF ~ posterior fossa; SC = spinal cord; CT = chemotherapy.
Clinical details are outlined in Table 1. All of the patients had their initial radiotherapy elsewhere and were re- ferred to Roswell Park Memorial Institute at time of recurrence. Patient 6 had one recurrence and Patient 7 had two recurrences treaied by further radiation before being referred. The initial posterior fossa radiotherapy doses are also presented in Table 1. All patients (except 5-see below) had craniospinal radiotherapy at diag- nosis. The doses to the remainder of the cranium and spine were correspondingly lower in those patients when the posterior fossa dosage was inadequate (Pa- tients l , 3, 6, and 7).
The diagnosis of recurrent tumor was made on histo- logical grounds in Patients 2, 5 , 6, and 7. In the other patients, i t was based on changing neurologic signs and abnormal neuroradiologic studies; in Patient 8, a CAT scan demonstrated an enlarging mass in the hypothalamus, which regressed after treatment.
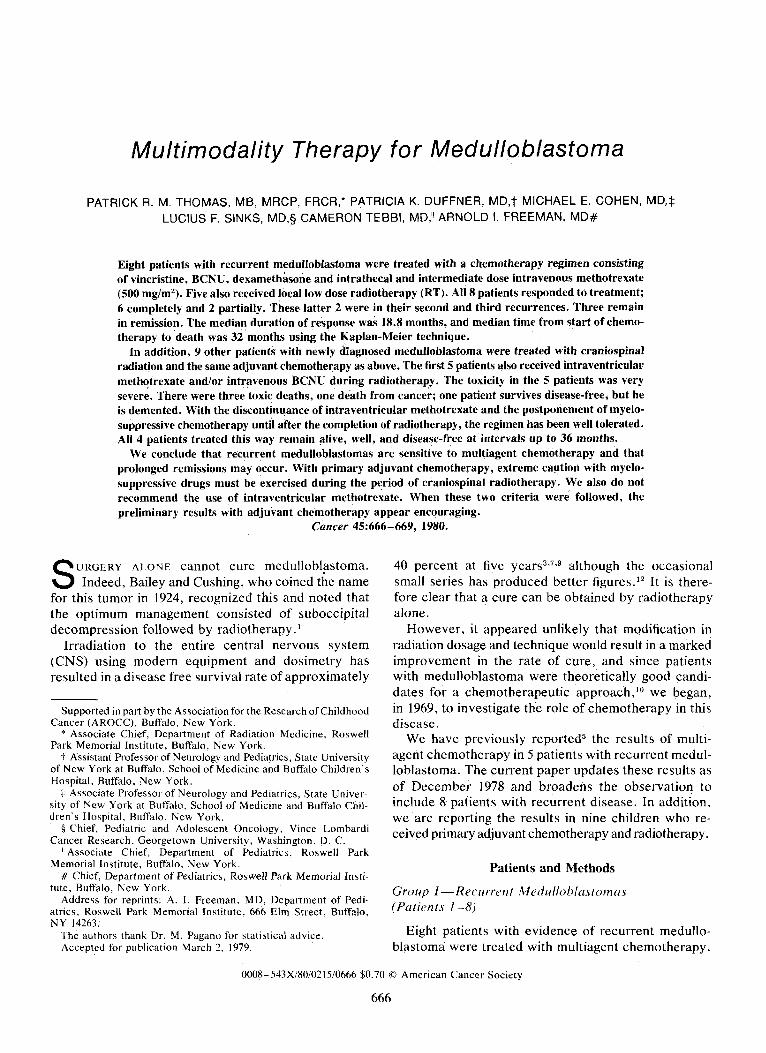
The patients were treated according to the protocol as described previously5 and summarized in Figure 1. Patients 5 through 8 also received additional radiother- apy to the area of recurrence at this time at low doses. The extra posterior fossa dosage ranged between 2000 rad in three weeks and 3000 rad in four weeks.
Group I I - Prirnary Adjuvcin t Cherizoth crapy (Putients 9-17)
Another 9 patients were treated with craniospinal radiotherapy at Roswell Park after the initial diagnosis of medulloblastoma was made. The treatment was de- livered for each patient by a 6 MV Linear Accelerator to a dosage of between 4500 and 5500 rad in five to eight weeks to the posterior fossa, 3500 and 4500 rad in four to seven weeks to the brain, and 2500 and 3500 rad in four to six weeks to the spinal column. The only exception to this was !Patient 9 who died before RT was completed. The brain was treated with two lateral parallel opposed fields-both fields treated daily-and there was an alternating gap at the lower cervical level to the spinal field(s). The spine was treated with one
or two direct posterior fields depending on the length required (with an alternating gap, where necessary). The lower border of S2 was the lower border of the field(s). The posterior fossa was boosted either with parallel opposed photon fields or with a suitable electron field.
Primary adjuvant chemotherapy was given according to the protocol (Figure 1 ) from day one. Patients 9-13 (Group IIA) received BCNU during RT, or they re- ceived intraventricular MTX as part of their chemo- therapy regimen. Patients 9 and 10 received weekly intraventricular methotrexate (6 mg/m2) through an Ommaya reservoir together with 6 mg/m2 of intrathecal methotrexate and BCNU 100 mg/m2 intravenously every four weeks during radiotherapy. Patients 11 and 12 received the intraventricular and intrathecal metho- trexate as above, but no BCNU during the radiotherapy. Patient 13 received BCNU during the radiotherapy but no intraventricular methotrexate. Patients 14- 17 (Group
INDUCTION
o o v v v S I 8 15 22 29 36 43
0 0 0 0 0 - [ rodialjon Therapy hf appLcobis1 1
50
CONSOLIDATION
57 64 71 78 85 92
I] I]
00 no 99
0
n o
MAINTENANCE 106 113 I20 127 I35 147 149 156 163
V V R E P q 28 days for 2 years E or until relapse 5 a
V 500 rng/m2 IV % push and '/, drw ovar 24 hours PLUS I T MTX 12mg/rn2 on.-
3 ~ C N U 1 0 0 m g / m 2 x I IV n halt hour attar start of I V HTX PLUS
VCR 2rngl rn2 x 1 I V
Leucovorin 12rng/m2 48 hwrs a t b r O D E X A M E T H A S O N E 8mgrn2/d.
PO in Ihrw dose1 uo start of I V MTX
I] METHQTREXATE 12mglm2 XIIT
FIG. 1. Chemotherapy schema.
668 CANCER February 15 1980 VOl. 45
TABLE 2 . Recurrent Medulloblastomas (Group I) Time from Start of Chemotherapy to Progression of Disease and Survival
Time Following Start of Chemotherapy in Month3
Patient no.
From start of chemotherapy Survival following start to disease progression of chemotherapy
(months) (months)
18 18 29 38? 60* 12 17* 9*
19 32 44t 60 607 18 17t 9t
* No progression. + Alive.
TTB) received the chemotherapy regimen precisely as outlined by the protocol (Figure 1) i .e . the intraventric- ular route was not employed and BCNU was delayed until after the completion of RT and after the comple- tion of intermediate dose methotrexate.
Results
Group I-Recurrent Medullohlustomus
All 8 patients responded to treatment, and there were six complete and two partial responses, (Patients 6 and 7-both of whom had suffered previous recur- rences treated by local radiation alone). The criterion for complete response was disappearance of all abnormal clinical signs and neuroradiologic studies that had de- veloped prior to recurrence. Partial response was defined as incomplete improvement in these signs and studies. In keeping with our previous report, the toxicity was minima1.j
TABLE 3 . Results of Adjuvant Chemotherapy (Group I1 A)
Age at Patient diag- Survival
no. nosis Sex (months) Comments
9t 6 M 2 Overwhelming sepsis (Neutropenic)
Autopsy no gross tumor
lot 2 M 590 Convulsions/demented
11* 4 F 4 Deccrebrate rigidity
12* 9 M 11 V.P. shunt
no autopsy
Bone marrow metastases
13t 4 M 3 Varicella pneumonia panc ytopenia
Autopsy no tumor
* Intra-Ommaya methotrexate (no BCNU with RT). t BCNU with radiotherapy and Intra-Ommaya methotrexate. I: BCNU with radiotherapy (no intra-ommaya therapy). I Remains alive.
The time from recurrence to progression of disease ( i .e . following retreatment with CT) and the survival time following recurrence are presented in Table 2 . Patients 1,2 , and 6 died with active disease after further relapse in the posterior fossa. Patient 3 also relapsed a second time in the posterior fossa but after additional local radiotherapy (3500 rad in five weeks) and the same regimen of chemotherapy is disease free. Patient 4 developed progressive quadriparesis and died. Lumbar and cisternal myelography both had suggested arach- noiditis, but permission for autopsy was not obtained. It was not possible, then, to determine whether his disease had progressed. Patient 5 was initially misdiag- nosed as a partially excised cerebellar astrocytoma and therefore received only local radiotherapy at the initial diagnosis and only at the time of relapse did he receive craniospinal radiotherapy and chemotherapy. This patient remains alive and continuously disease-free from 60 months since retreatment.
The median duration of remission (assuming disease progression in Patient 4) was 18.8 months, the median survival time from start of multiagent chemotherapy was 32 months using the Kaplan-Meier method.
Group I I - Primary Adju vut? t Chernotherupj
Group I I A : The results are presented in Table 3 . Of these 5 patients, only 1 died with recurrent tumor. The remaining 4 patients experienced serious cornpli- cations: two had severe leukoencephalopathy secondary to intraventricular methotrexate, and one of these died; two died from severe infections while myelosuppressed from HCNU.
Group II B: Thus it was decided to discontinue intraventricular methotrexate completely and withhold BCNU during radiotherapy. The results of treatment for this group of patients are shown on Table 4. All 4 patients remain alive and disease-free. Toxicity has been low. All patients have been able to complete radio- therapy as prescribed.
Discussion
The results of treatment in recurrrrit medulloblastoma (Group I) confirm our previous findings5 that these tumors are sensitive to the multiagent chemotherapy employed with resultant prolonged remissions. The results in the present report compare those results with procarbazine, CCN U and vincristine." In Edwards's study, 2 out of 6 patients showed a response to therapy and 4 out of 6 had stable disease. The median time to progression was 63 weeks;6 in ours it was 81 weeks (18.8 months). The experience of Bloom cf ul.3 and Harisiadis and Chang7 suggest that low-dose. local irradiation to

No. 4 MULTIMODALITY THERAPY . Tliotnas (>t al . 669
recurrent medulloblastoma may also produce good results. The experience of our 6 patients who received local radiotherapy besides multiagent chemotherapy suggests that it may be worthwhile to compare low-dose irradiation (of bulk recurrent disease) and chemotherapy to chemotherapy alone in this situation.
The predilection for recurrence in the posterior fossa is also confirmed.2 In view of this tendency and the staging system used at the Columbia Presbyterian H ~ s p i t a l , ~ which demonstrated in their series that smaller tumors had a better prognosis, we support the concept of removing as much tumor as possible (with- out causing neurologic d.amage) rather than performing a biopsy at the initial diiagnosis.
Our initial experience with (idjrtvnnt chemotherapy (Group I1 A) demonstrates the danger of intraventricular MTX. Shapiro et (11." described 3 patients who had evidence of ventricular obstruction of the CSF flow and who developed encephallopathy following intraventric- ular installation of methotrexate. In retrospect, patients 10 and 11 likely had partial obstruction of the CSF pathways. Unfortunately, these patients were treated before this toxicity was known. Patients 9 and 13 il- lustrate the problem of profound myelosuppression secondary to simultaneous spinal radiotherapy and BCNU. We recommend that potent myelosuppressive chemotherapy be avoided during craniospinal radio- therapy.
Patient 12 had a ventriculo-peritoneal shunt placed for decompression without a millipore filter. It is pos- sible that the bone marrow metastases resulted from spread through the shunt, but this does not fit the pat- tern of spread described by Hoffman ( I t ( r / . 8 who sug- gested that the peritoneal cavity was the first site of recurrence in this situation. Shunting, per se, may allow systemic access of the tumor through the peritoneum or through circulation.
When BCNU was postponed until after spinal radio- therapy was completed, and the use of intraventricular methotrexate was discontinued, this regimen was well tolerated (Group 11 B). The disease-free survival times are too short at present for meaningful comment. None- theless, to date, none of our 4 patients has developed recurrent disease on the revised study. The randomized international trials, now in progress, are testing if
TABLE 4. Results of Adjuvant Chemotherapy (Group I1 6)
Age at Patient diag- Survival
nosis Sex (months) Comments no.
14 10 M 35'+ Disease free-no toxicity
15 2 M 31" Disease free-no toxicity
16 4 F 20" Disease free-moderate Thrombocytopenia during
17 3 M 6* Disease free-no toxicity
later chemotherapy
~ Remains alive
adjuvant chemotherapy can improve the cure rate in primary medulloblastoma with the drugs employed.
At present, radiotherapy has a definite cure rate in this disease. Should primary adjuvant chemotherapy prove to be of value, the next logical step would be to evaluate the reduction of the RT dose to the spine as has been ~ugges t ed .~ However, at the present time, this step appears premature.
REFERENCES
1. Bailey, P. E . , Cushing, H.: Medulloblastoma cerebelli. i lrc,h. Ncirrol. c r i id P s w h . 14: 192-224, 192.5.
2. Bloom, H. J . G.: Medulloblastoma: Prognosis and prospects. I n [ . J . Raditrf. Oncol. Biol. Phys. 2: 103 I - 1033, 1977.
3. Bloom, H. J . G., Wallace. E. N. K . and Henk, J . M.: The treatment and prognosis of medulloblastoma in children. Am. J . Roentgeiiol. I0.5:43 - 62, 1969. 4. Brown, R. C., Gunderson, L. L. and Plenk, H. P.: Medul-
loblastoma. 4 Review of the LDS Hospital Experience. C ~ I I C P Y 40: 56-60, 1977.
5 . Duffner, P. K., Cohen, M. E., Thomas, P . K. M.. Sinks, L. F. and Freeman. A. 1.: Combination chemotherapy in recurrent medul- loblastomas. Clinrrr 43:41-45, 1979.
6. Edwards, M. , Levin, V. A . and Wilson, C. B.: Personal com- munication.
7. Harisiadis, L. and Chang, C. H.: Medulloblastoma in children: A correlation between staging and results of treatment. In?. J . Kadicir. Oncol. Biol. Pliys. 2:833-841, 1977.
8. Hoffman, H. J . , Hendrick, E. B. and Humphreys, K. P.: Metastases via ventriculo-peritoneal shunt in patients with medul- loblastoma. J . Neurosurg. 44:.562-566, 1976.
9. Mealey, J . and Hall, P. V.: Medulloblastoma in children. J . .?ieirrnsur.g. 46:56-74, 1977.
10. Shapiro, W. R.: Chemotherapy of primary malignant brain tumors in children. C o w e r 35:96.5 -972, 1975.
11. Shapiro, W. R . , Chernik. N. L. and Posner, J . B.: Necrotizing encephalopathy following intraventricular instillation of methotrexate. Arch. Neurol. 28:96- 102, 1973.
12. Sheline, G.: Radiation therapy of brain tumors. Cancer. 39: 873-881, 1977.






![Medulloblastoma: [Print] - eMedicine Neurology · accounts for approximately 7-8% of all intracranial tumors and 30% of ... Incidence of medulloblastoma is 1.5-2 cases per ... Medulloblastoma:](https://img.dokumen.tips/doc/110x75/5b7fc2317f8b9ae6088caa0e/medulloblastoma-print-emedicine-accounts-for-approximately-7-8-of-all.jpg)