Embed Size (px)
Citation preview
Molecular Genetics of Paediatric TumoursGino Somers MBBS, BMedSci, PhD, FRCPAPathologist-in-ChiefHospital for Sick Children, Toronto, ON, CANADA

Financial Disclosure
NanoString - conference costs for TriCon Molecular Medicine Conference, San Francisco, 2015
Molecular Genetics of Paediatric Tumours
Introduction and methodologies
Paediatric sarcomas*
Neuroblastoma*
Wilms tumour
Concluding remarks
Molecular Genetics of Paediatric Tumours
Discovery of recurrent genetic abnormalities in paediatric tumours “transformational”
more precise diagnostic accuracy (e.g. EWSR1)
discovery of prognostic markers (e.g. NMYC)
paradigm shift in tumour classification (e.g. DICER1)
better understanding of biology
Methodologies
Traditional
G-banding cytogenetics
FISH
RT-PCR
Newer and Emerging
Array technologies
NanoString assay
Next generation sequencing (NGS)
Methodologies
Traditional
G-banding cytogenetics
FISH
RT-PCR
Newer and Emerging
Array technologies
NanoString assay
Next generation sequencing (NGS)
Paediatric Sarcomas
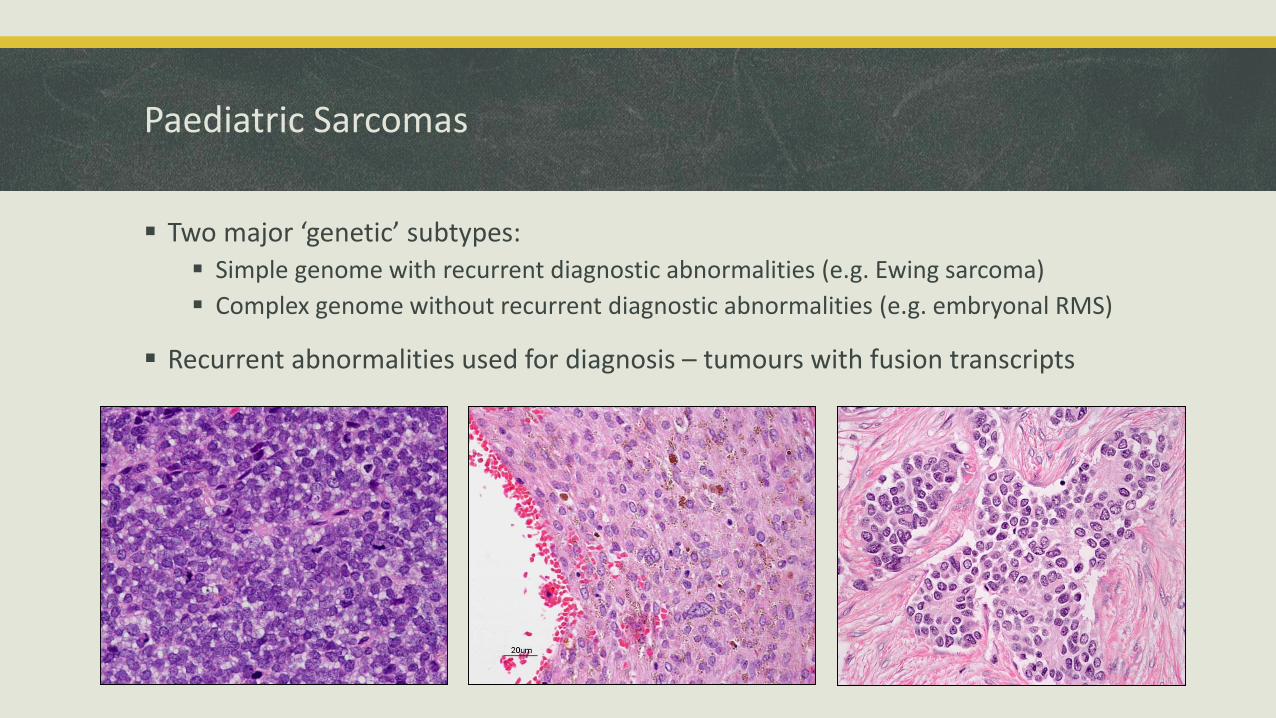
Paediatric Sarcomas
Two major ‘genetic’ subtypes:
Simple genome with recurrent diagnostic abnormalities (e.g. Ewing sarcoma)
Complex genome without recurrent diagnostic abnormalities (e.g. embryonal RMS)
Recurrent abnormalities used for diagnosis – tumours with fusion transcripts
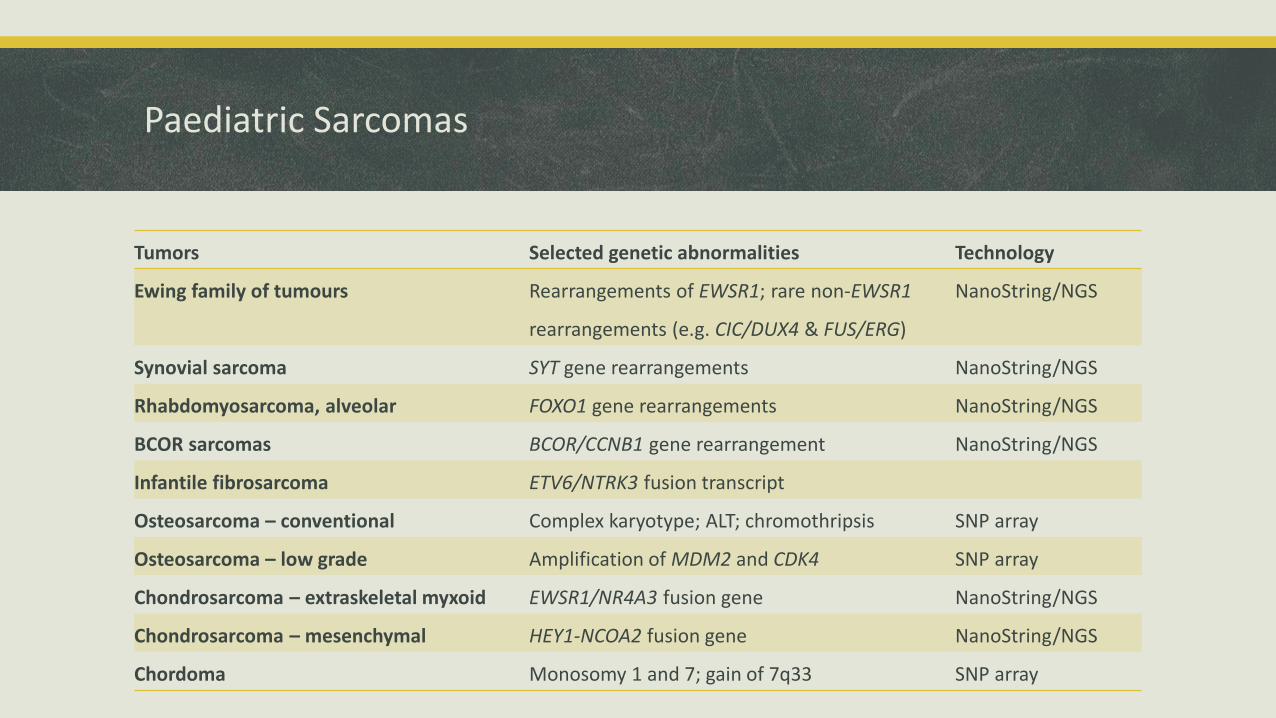
Paediatric Sarcomas
Tumors Selected genetic abnormalities Technology
Ewing family of tumours Rearrangements of EWSR1; rare non-EWSR1
rearrangements (e.g. CIC/DUX4 & FUS/ERG)
NanoString/NGS
Synovial sarcoma SYT gene rearrangements NanoString/NGS
Rhabdomyosarcoma, alveolar FOXO1 gene rearrangements NanoString/NGS
BCOR sarcomas BCOR/CCNB1 gene rearrangement NanoString/NGS
Infantile fibrosarcoma ETV6/NTRK3 fusion transcript
Osteosarcoma – conventional Complex karyotype; ALT; chromothripsis SNP array
Osteosarcoma – low grade Amplification of MDM2 and CDK4 SNP array
Chondrosarcoma – extraskeletal myxoid EWSR1/NR4A3 fusion gene NanoString/NGS
Chondrosarcoma – mesenchymal HEY1-NCOA2 fusion gene NanoString/NGS
Chordoma Monosomy 1 and 7; gain of 7q33 SNP array
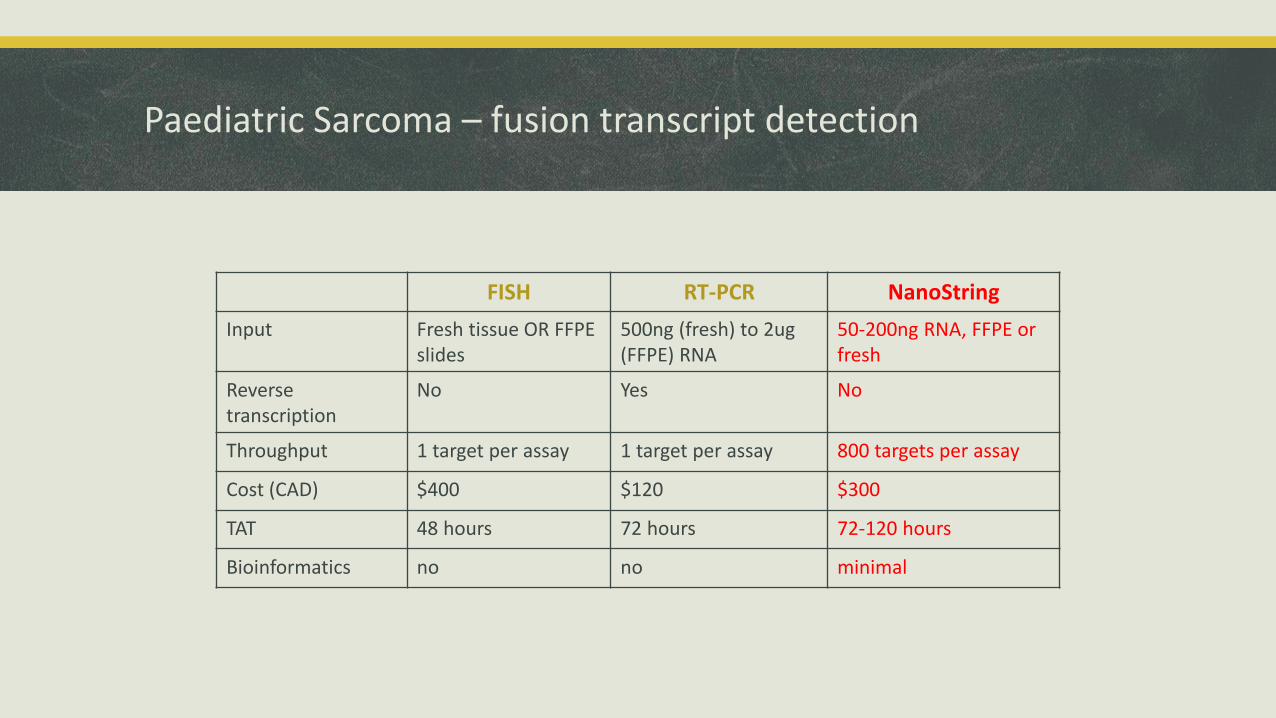
FISH RT-PCR NanoString
Input Fresh tissue OR FFPE slides
500ng (fresh) to 2ug (FFPE) RNA
50-200ng RNA, FFPE or fresh
Reversetranscription
No Yes No
Throughput 1 target per assay 1 target per assay 800 targets per assay
Cost (CAD) $400 $120 $300
TAT 48 hours 72 hours 72-120 hours
Bioinformatics no no minimal
Paediatric Sarcoma – fusion transcript detection
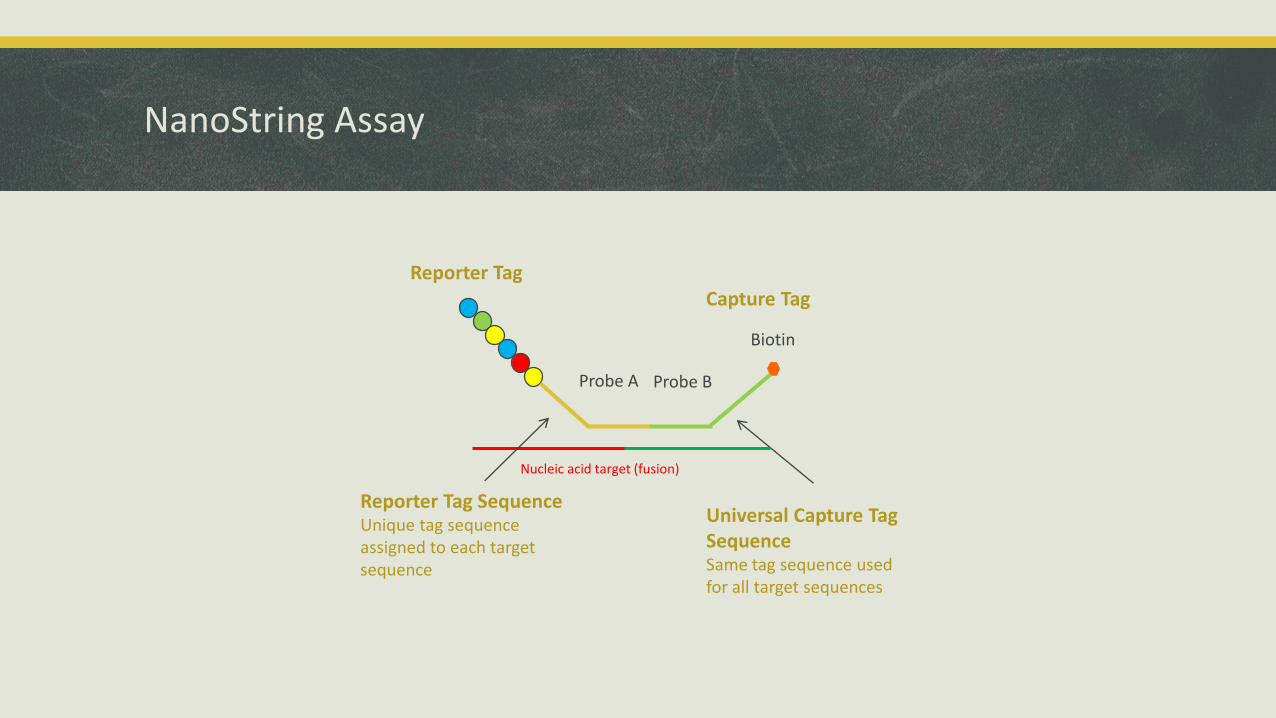
Reporter Tag SequenceUnique tag sequence assigned to each target sequence
Universal Capture TagSequenceSame tag sequence used for all target sequences
Biotin
Nucleic acid target (fusion)
Capture Tag
Probe A Probe B
Reporter Tag
NanoString Assay
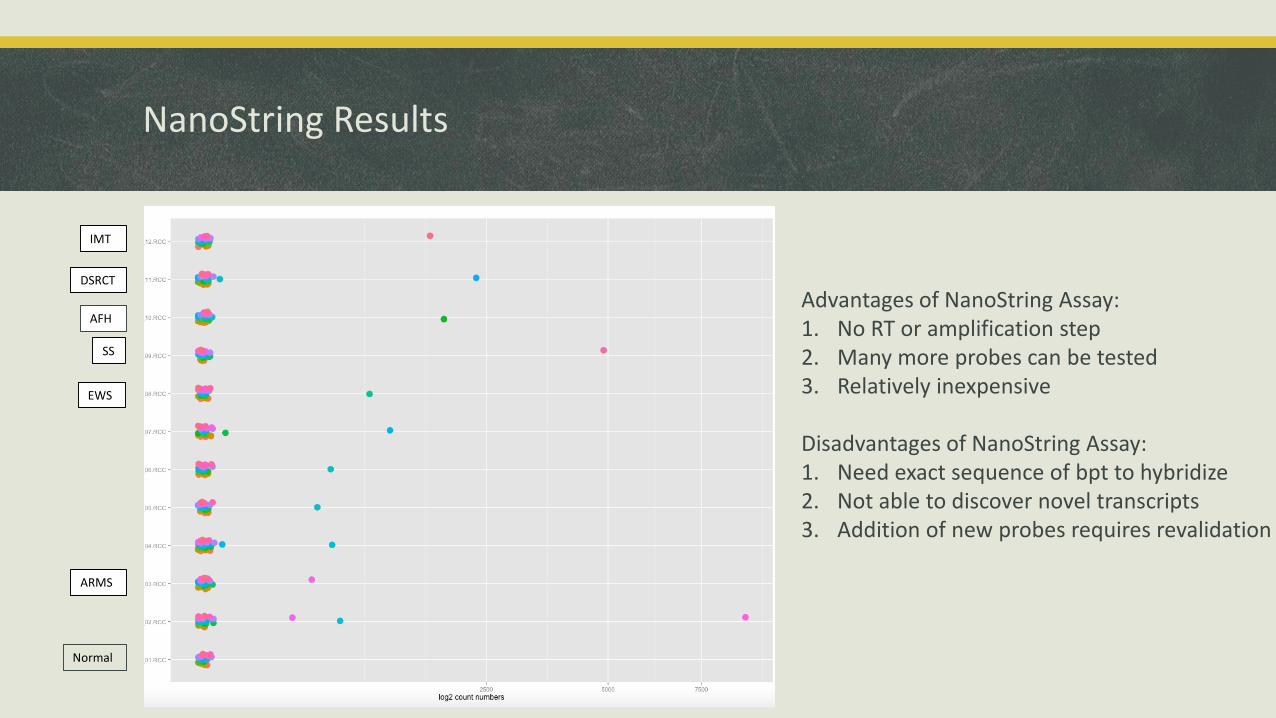
Normal
DSRCT
AFH
IMT
SS
EWS
ARMS
NanoString Results
Advantages of NanoString Assay:1. No RT or amplification step2. Many more probes can be tested3. Relatively inexpensive
Disadvantages of NanoString Assay:1. Need exact sequence of bpt to hybridize2. Not able to discover novel transcripts3. Addition of new probes requires revalidation
Paediatric rhabdomyosarcomas – emerging molecular abnormalities
Rhabdomyosarcoma:
MyoD1 L112R mutations – higher frequency in spindle/sclerosing ERMS; poor outcome
NCOA2 fusions – < 1 year old, spindle cell morphology
FOXO1 gene amplification – associated with PAX7 partner >> PAX3 partner
FGFR4 & pathway gene mutations – potential therapeutic targets
Paediatric sarcomas – emerging molecular abnormalities
Ewing sarcoma
CDKN2A – copy number loss confers a poorer outcome
NR0B1 microsatellites – role in susceptibility to fusion transcript growth promotion
STAG2 – mutations seen at increasing clonal frequency with increased stage of disease
Synovial sarcoma
CCND1 & KRAS – mutations in older patients
Small percentage with CTNNB1 gene mutations and WNT pathway activation
Paediatric Sarcomas - summary
Recurrent abnormalities – fusion transcript detection
Complex genomes – copy number changes +++
Emerging molecular abnormalities
Neuroblastoma
Neuroblastoma
Critical to have additional molecular genetic data to classify risk
NMYC and 1p the classical abnormalities with prognostic significance
Several other changes now associated with prognosis:
Segmental copy number changes (especially 11q loss or 17q gain) = unfavorable
Whole chromosomal copy number changes = favorable
Single gene mutations (ALK, Phox2B, PTPN11, ATRX)
Need molecular data for complete report
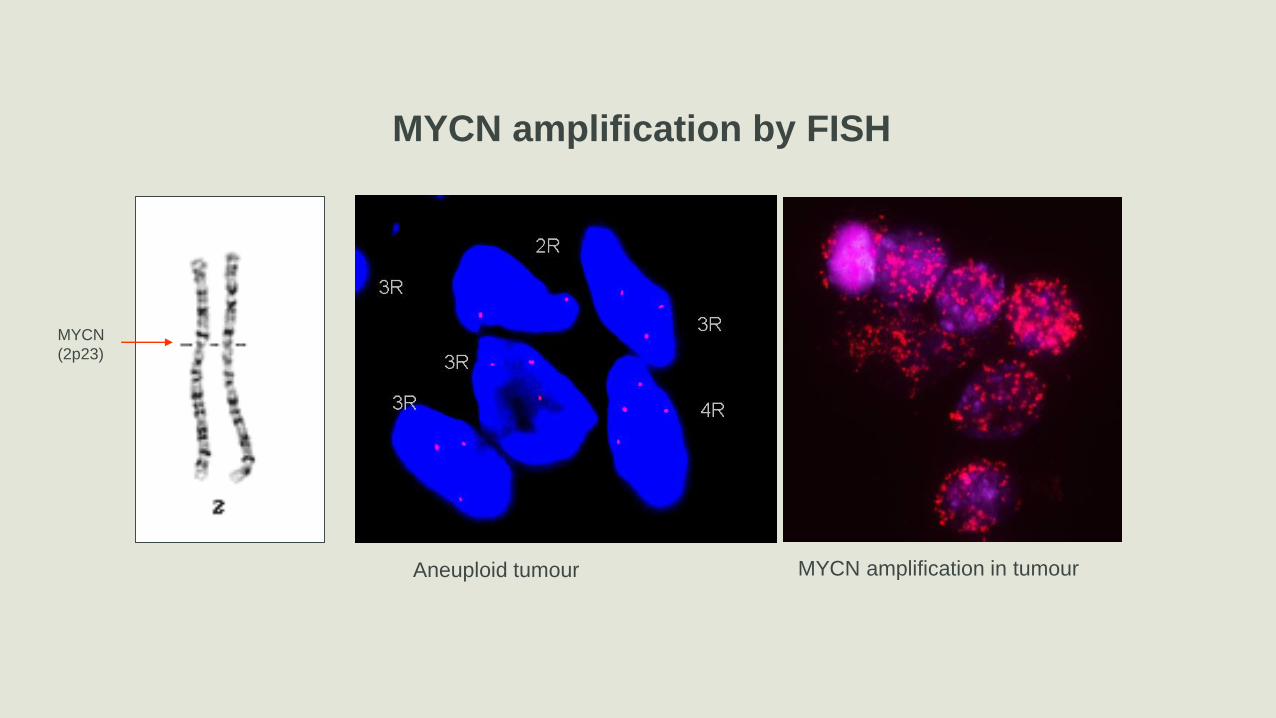
Aneuploid tumour MYCN amplification in tumour
MYCN
(2p23)
MYCN amplification by FISH
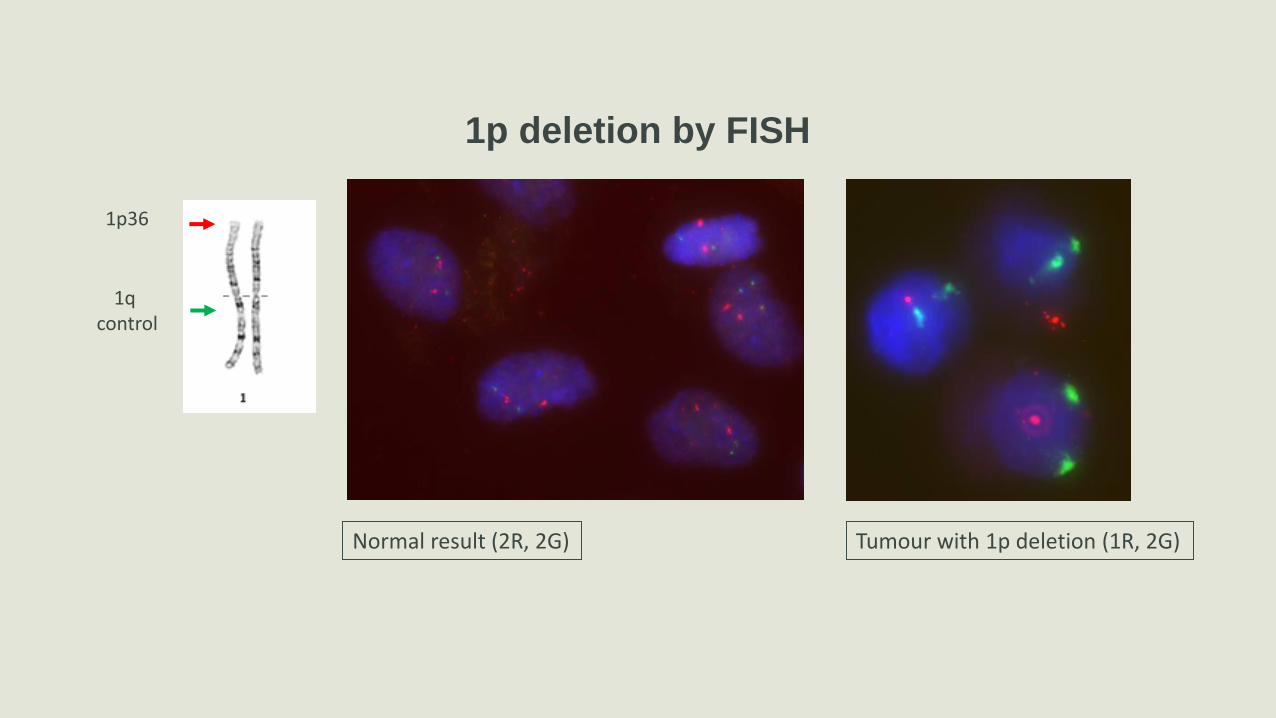
1p deletion by FISH
1R2G
Tumour with 1p deletion (1R, 2G)
1p36
1q control
Normal result (2R, 2G)
Challenge: FISH vs array technology
FISH assay:
rapid TAT
iterative – one probe per assay
becomes expensive with > 2 probes
Array/SNP assay
slower TAT
MUCH more data
expense inversely proportional to number of loci reported
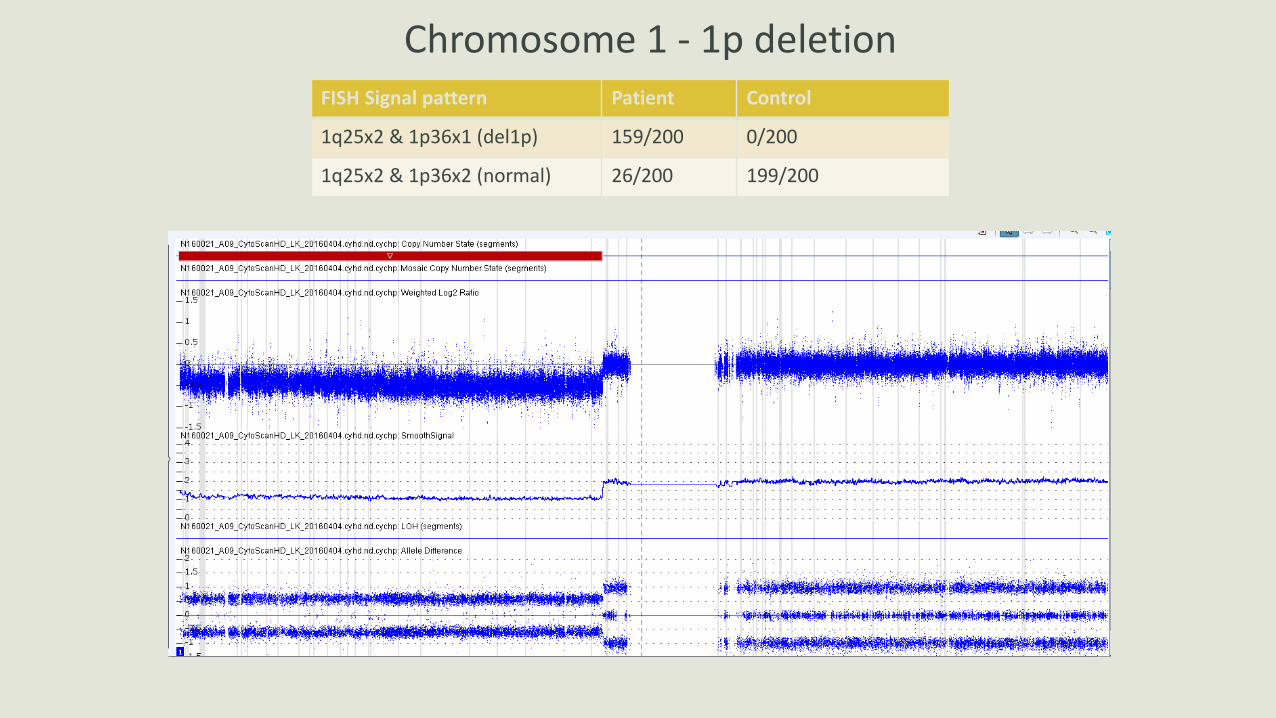
Chromosome 1 - 1p deletionFISH Signal pattern Patient Control
1q25x2 & 1p36x1 (del1p) 159/200 0/200
1q25x2 & 1p36x2 (normal) 26/200 199/200
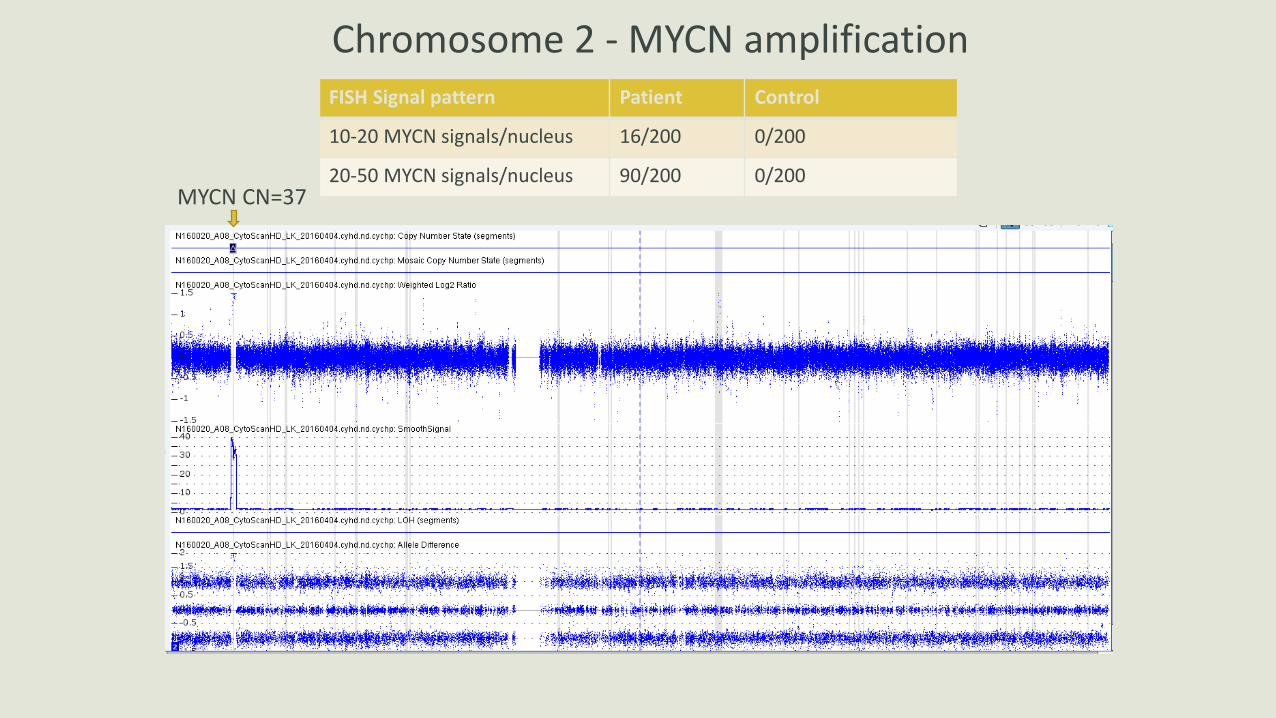
Chromosome 2 - MYCN amplification
MYCN CN=37
FISH Signal pattern Patient Control
10-20 MYCN signals/nucleus 16/200 0/200
20-50 MYCN signals/nucleus 90/200 0/200
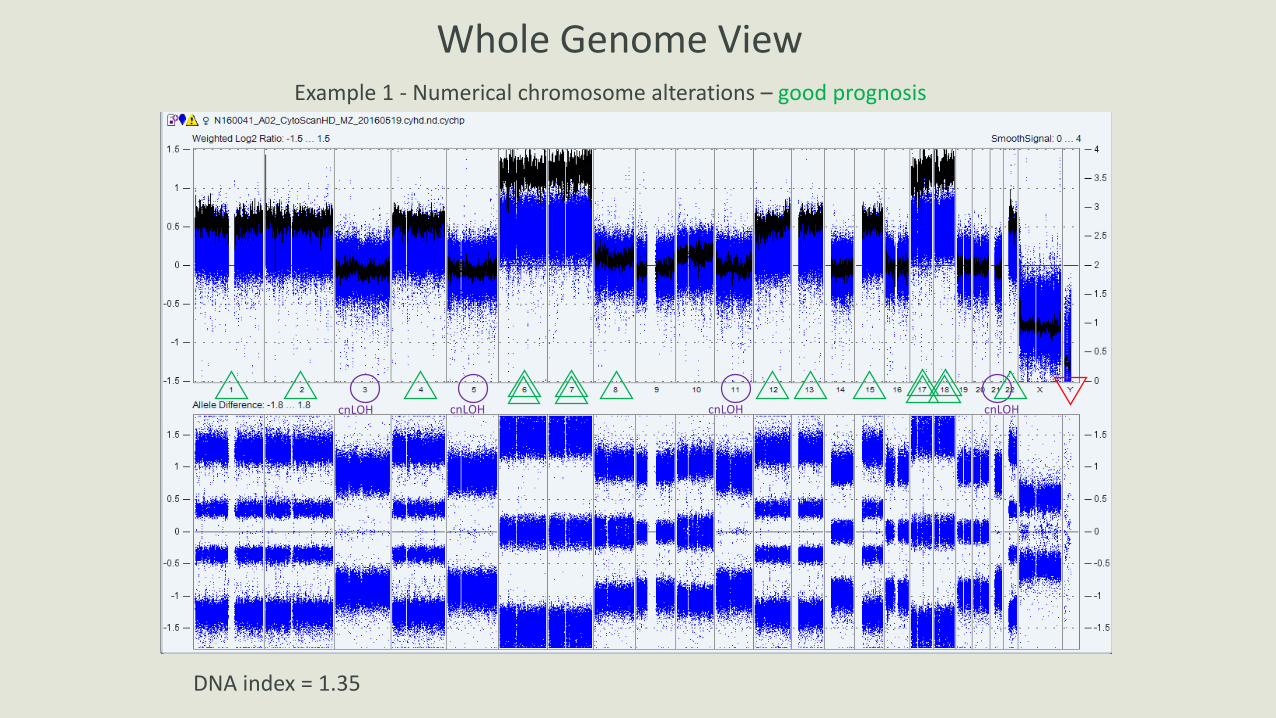
Whole Genome View
DNA index = 1.35
cnLOH cnLOH cnLOH cnLOH
Example 1 - Numerical chromosome alterations – good prognosis
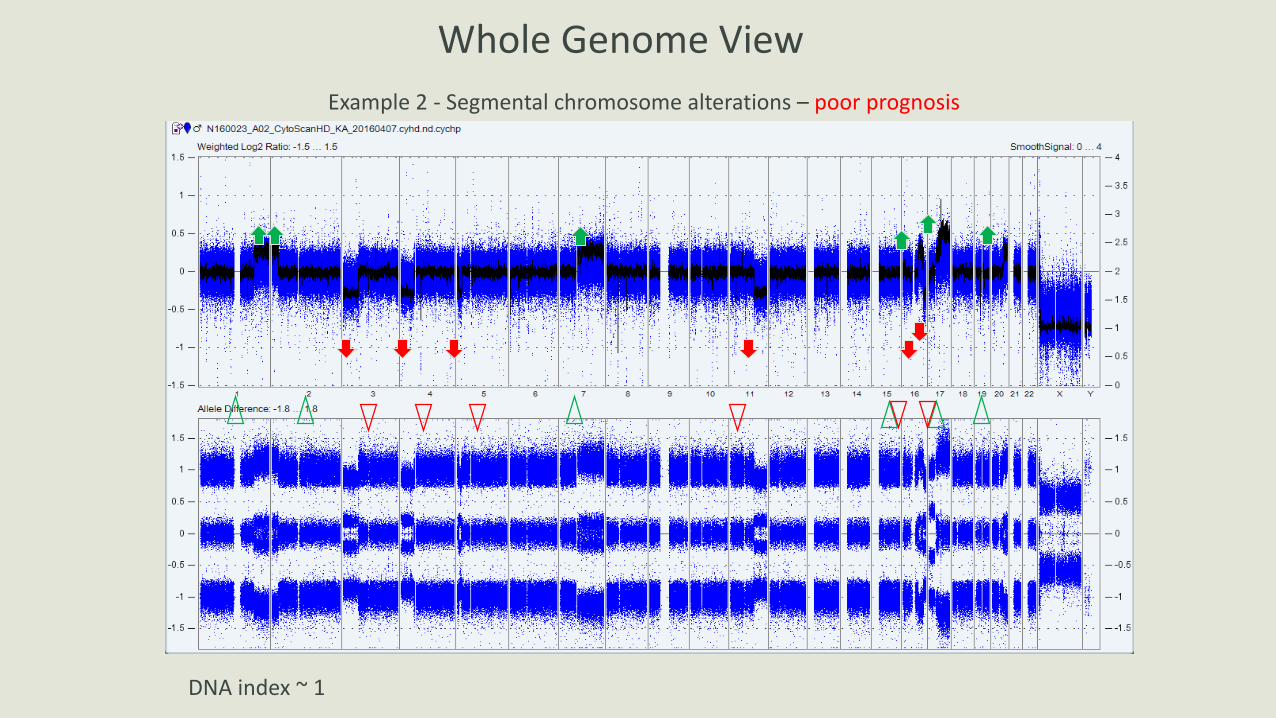
Example 2 - Segmental chromosome alterations – poor prognosis
DNA index ~ 1
Whole Genome View
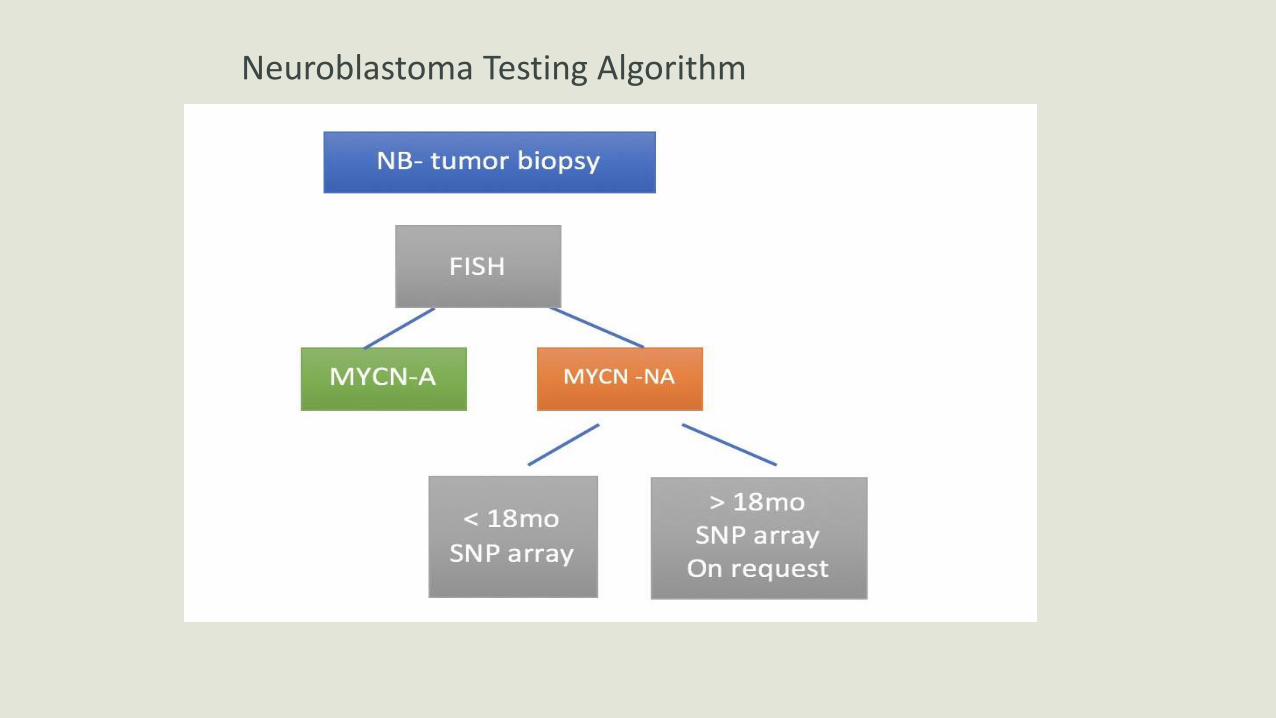
Neuroblastoma Testing Algorithm
Neuroblastoma - Single Gene Mutations
ALK, ARID1/ARID1A, ATRX – poorer outcome
Phox2B – rare; plays a role in familial neuroblastoma
Neuroblastoma Summary
Classical abnormalities – NMYC, 1p deletion
Broader genome-wide abnormalities – whole chromosome vs. segmental change
Single gene abnormalities
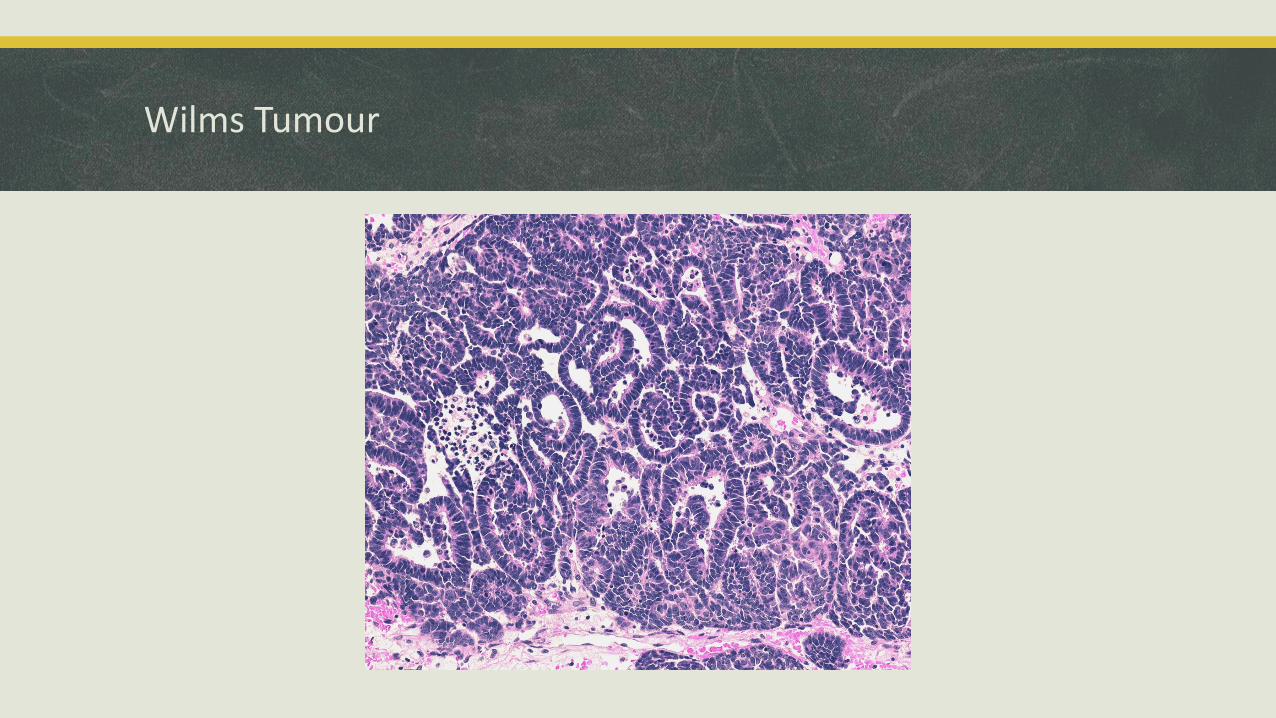
Wilms Tumour
Wilms tumour –genetic abnormalities
LOH 1p and 16q:
portends a worse prognosis
detectable using SNP arrays
Mutations in TP53
associated with anaplasia
associated with more aggressive disease and poorer outcome
Mutations in DROSHA gene
Associated with more aggressive blastemal-predominant tumours
Inherited syndromes – BW syndrome, WT1 mutations
Future Directions
NGS in the clinic
Liquid biopsy
‘3D’ assays
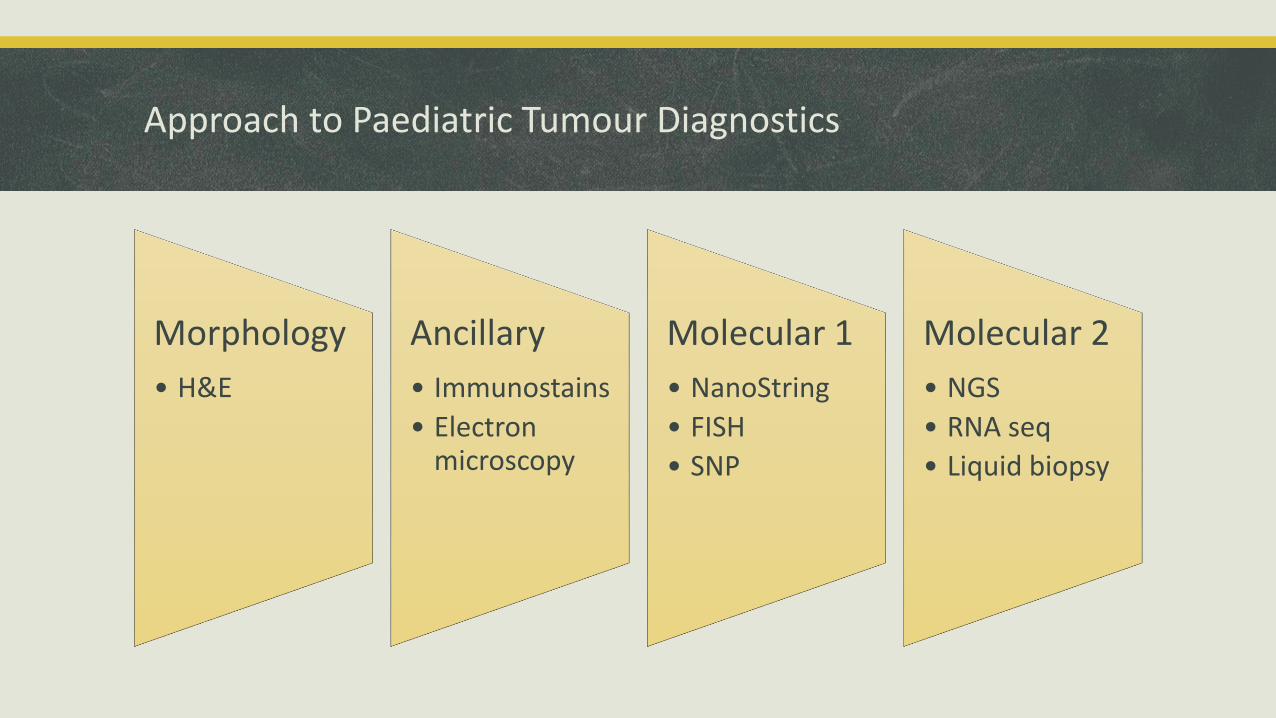
Approach to Paediatric Tumour Diagnostics
Morphology
• H&E
Ancillary
• Immunostains
• Electron microscopy
Molecular 1
• NanoString
• FISH
• SNP
Molecular 2
• NGS
• RNA seq
• Liquid biopsy
Contact details
Email: [email protected]
Address: Division of Pathology
Hospital for Sick Children
555 University Avenue
Toronto, ON M5G 1X8


![INDEX [2014.cimtec-congress.org]2014.cimtec-congress.org/data/image/pdf/Congress_programme.pdf · southampton, southampton, UK; Centre for Disruptive Photonic technologies, nanyang](https://img.dokumen.tips/doc/110x75/5fbea60703ecf8063b57d74a/index-2014cimtec-2014cimtec-southampton-southampton-uk-centre-for-disruptive.jpg)