Embed Size (px)
Citation preview

Pre-conference Workshop Substance Abuse and Brain injury:
It’s complicated
Timothy Schilling, MSW, LSW, LICDC Ohio State University
Annette Pearson MS, LADC, CBIS Vinland National Center
Carolyn Lemsky, Ph.D., ABPP-cn. Community Head Injury Resource Services of
Toronto
Models for Treating Co-Occurring TBI and Substance Abuse

Integrated Treatment of TBI and Substance Abuse
Timothy Schilling MSW, LSW, LICDC
Vocational Specialist, Case
Manager, Substance Use Disorder Counselor
TBI Network

TBI Network
• Background – Established 1991 – Community-based
• Overview – Intensive case management,
SUD grp/ind counseling,TBI education, voc serv., TIF setting
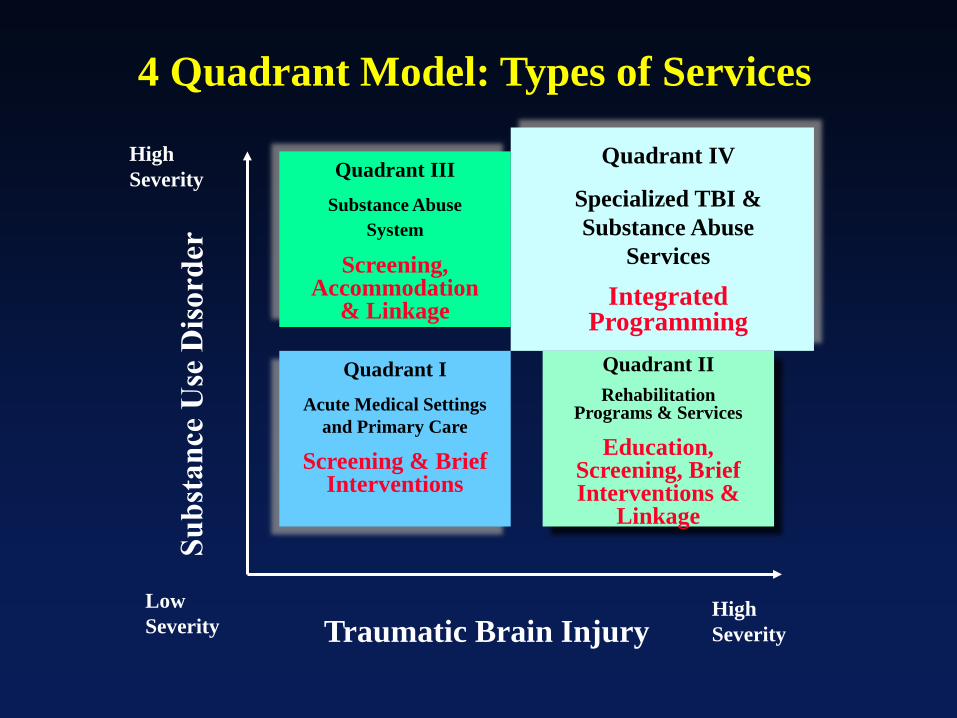
Traumatic Brain Injury Low Severity
High Severity
High Severity
Quadrant I Acute Medical Settings
and Primary Care
Screening & Brief Interventions
Quadrant II Rehabilitation
Programs & Services
Education, Screening, Brief Interventions &
Linkage
Quadrant III Substance Abuse
System
Screening, Accommodation
& Linkage
Quadrant IV
Specialized TBI & Substance Abuse
Services
Integrated Programming
4 Quadrant Model: Types of Services

1. Substance abuse treatment and brain injury rehabilitation are interwoven–not sequential and not just parallel.
2. Is holistic–addressing all aspects of lifestyle, not just TBI and substance use.
3. Key staff are skilled in working with both TBI and substance use disorders.
4. Consumers and clinicians collaborate to develop an individualized treatment plan.
7 Principles of Integrated Treatment for TBI and Substance Abuse

5. During treatment different services will be helpful at different points in recovery.
6. Clinicians use specific listening and counseling skills to help consumers develop awareness, hopefulness, and motivation for recovery.
7. Smaller staff caseloads, more experienced staff, and longer-term treatment usually required.
7 Principles of Integrated Treatment for TBI and Substance Abuse (cont’d)

The OSU TBI Network
• Intensive case management model that is person-centered and holistic.
• Resembles IDDT for co-occurring disorders, except treatment teams are “ad hoc.”
• OSU PM&R Residents provide a free clinic for medical needs including pharmacologic treatment of affective disorders.
• Has a supported employment program embedded using the Individualized Placement and Support model.
Vocational Program
• Individual Placement and Support Model – Principles of IPS Supported Employment – State Vocational Rehab partner
• Education of VR staff of TBI and co-occurring

Interventions Used in the TBI Network:
• “Whatever It Takes”
• Stages of Change theoretical model, including groups based on stages
• Motivational Interviewing
• Strategic Use of Financial Incentives
• Provided in a Trauma-Informed setting

Trauma-Informed Culture
• Realize – Pervasive, individually experienced, behaviors as
coping/defense strategies, holisitc approach, hope (recovery is possible)
• Recognize – Reactions may take different forms, impacts staging, case
management implications, team members needed at the table
Trauma-Informed Culture
• Respond – Safety, access to different services, universal screening
(ACE) secondary trauma
• Resist retraumatizing – Power differentials (collaboration with client on services;
what when and how to be provided
Further Resources
www.OhioValley.org www.BrainLine.org
www.subi.ca

Adapting Residential treatment
For Individuals with Brain Injuries Vinland National Center
Annette Pearson MS, LADC, CBIS

Vinland’s goal MIND-BODY-SPIRIT
Treatment comparison Structure of integrated brain injury treatment
and care Modified Group and individual sessions Mindfulness training Wellness and Fitness Modified 12 steps Goals and relapse prevention

Moving from traditional to integrated, individualized treatment for people with brain injuries: Starts with the philosophy and attitude of
management. Address funding needs – how to licensure and
structure depends on each state. Build the program from the policy on up to meet
the needs of individuals with brain injury. Evidence based practices for Brain Injury and
Substance Use.
Structure Schedules are color coded and have clients in
the same rooms at the same times each day. Groups are 50 minutes in length with breaks. Clinical and more cognitively focused groups
are in the a.m. with less mentally challenging groups in the evening and later evening
Mental health, medical, nutrition, fitness, wellness and recreational groups are part of the program
Many places for individuals to get away and have private time to think
Individual Sessions Assess group skills at intake and in first session. Shorter individual sessions with more frequency to
aid in repetition and retention. Same time, days of the week and location. Work with the same team of individuals from intake
to discharge Have one or two main topics in a session and
break written and reading work to smaller pieces Have a quiet distraction free work environment – limit
the amount of “stuff” in your office Remind them to write main points, assignments,
appointments and structure in their planner and help them do it in your office.
Use a calendar for high risk for use times, places for added supports and structure.

Group Sessions Shorter group sessions with repetition to address
attention, fatigue and concentration 2 to 3 main points per group – main points first Write key points on the board for memory and ask
the person to write it down. Limit written assignments and work together on
them in the group setting. Be quiet while the group or individual is writing, it
is hard to listen, comprehend and write at the same time.
Practice relapse skills in group with role plays, group shaping, drama and plays
Make a signal for an individual who tangents and needs help refocusing

Groups Teach STOP-THINK techniques in group, reinforce with memory aides with motivators for
sobriety, cards with instructions for saying no, homework and individual sessions
Use multimodal group materials including tapes, videos, art, music, handouts, charts
Art medium is a good way to make abstract things such as feelings concrete.

What is Mindfulness? To practice mindfulness means to:
Adopt a nonjudgmental stance to our experience Practice patience and learning to “Let Go” Loosen our grip on what we “know” about our experience Trust our thoughts feelings and experience Recognize the urge to get and hold pleasant experience
and push away unpleasant experience Experience the qualities of acceptance
Can be used as part of any group – at the beginning for 5 minutes or so and can be applied to any stressful situation
Client’s with Brain Injuries often cannot remember specific details of a session but can remember how they felt about it.

How is it Helpful? • Increased activation of areas of the brain
associated with • Executive Decision-Making • Self directed Attention • Emotional processing and regulation • Reinforces experiential learning
• Offers concrete intervention to minimize impact of mental health symptoms including, low frustration tolerance, anxiety, depression and impulsivity Higher rates of self efficacy
• Higher rates of perceived quality of life • Greater recognition of positive experiences • Reduced reactivity and increased impulse control
Source: JFK Johnson Rehabilitation Institute

Strength – improves function in all areas, increase self esteem, motivation
Flexibility – decreases pain and risk of injury Endurance – reduces risk of many diseases
and improves lung and heart function Balance and Coordination – improves safety
with ADL’s and reduces risk for falls Posture and Body Mechanics – helps with pain
management Nutrition – improves function, improves sleep,
increase natural dopamine

TBI and exercise N=230 BIA of MN study, exercise is defined as 30 minutes of activity that increase heart rate.
Non-exercisers Reported higher levels
of forgetfulness and disorganization
Reported poor sleep at least half the days in the past month
Reported at least 10 days in the past month feeling depressed
Exercisers Better overall physical
function, Restful sleep >20 days Better cognitive function
in attention, memory concentration and organization
Reported less irritability Reduced days of feeling
depression < 5 days

Challenges with some 12 step meetings
Abstract nature Traditions/unwritten rules Isolation Feeling misunderstood Confusion over expectations Lack of structure in some
meeting types
12 Steps
Step 1 We admitted that we were powerless over our addiction, that our lives had become unmanageable Admit that if you drink and/or use drugs your life
will continue to be out of control. Admit that alcohol and drugs are not making your problems better.
12 Steps - STEP 2 We came to believe that a power
greater than ourselves could restore us to sanity.
You start to believe that someone
can help you put your life in order. This someone could be God, an AA group, counselor, sponsor, etc.
Many individuals will be angry with
their higher power after an injury and may be resistant to “AA” things due to that association

What works TEACH the three basic points of 12 step groups:
1. What I am doing is hurting me and I need to stop.
2. In order to stop, I need help. 3. In order to get help, I need to get along
better with others and take better care of myself.
USE the 12 steps for concrete thinkers RESEARCH the meeting beforehand about
medications and labels DEFINE terms commonly used at meetings such
as open and closed- have this in writing ROLE PLAY and REHEARSE over what to
expect at a meeting DISCUSS what the meetings and terms mean
before going to a meeting PAIR the person up with a peer mentor who can
help them get comfortable and understand

Evaluate Goals and Roles Many individuals primary role prior to the injury was
‘the party guy’ or the ‘guy with the stuff’. The glamour and money from using needs discussion.
Encourage reevaluation of what roles and goals are most important now.
Review roles and goals they currently have and ones they wish.
Discuss goals, both short term and long term. Discuss did my chemical use help or hinder my long
term goals? Use a life calendar to aid in this decision making,
pairing highs and lows across the lifespan with alcohol and drug use, increases, changes and consequences
Goal Setting (Neimeier and Karol 2011)
Set goals that are realistic and flexible. Set a goal with a scale for goal setting to include: Getting my job back as a banker Best Outcome I am a full time bank teller or bank
employee or with people Next Best Outcome I am a part time bank teller or bank
employee or with people Middle Outcome I work full time as a receptionist or job
where I work with people Next Worse Outcome I work part time as a receptionist or
job where I work with people Worse Outcome I am not able to get any job

Relapse Prevention Planning Relapse planning requires a PLAN, in writing, that is
structured in a way the person is not overwhelmed or bored
Make sure they have a copy of the plan. They need a copy or copies to put in places
where they will use it. Perhaps in places where they used to use.
Use a weekly or monthly calendar and write/put it appointments, meetings, reminders etc. on it.
Remember to think about transportation and funding
The plan needs to address the persons level of cognitive functioning

Relapse Prevention Planning Write out abbreviations List addresses, telephone
numbers, title and what the person is going to the appointment for on the plan
Include maps, bus routes, cab information if needed
List memory aides on the plan and have the person practice WHILE in treatment
List support meetings and people on the plan
with telephone numbers Plan for co-worker
encouragement to use Remind clients that they
have the right NOT to use and list that statement on their memory aides
Have them list the reasons why they want to stay sober on the plan and memory aides

Carolyn Lemsky, Ph.D.,C.Psych

SUBI Bridging Project
To increase access to care for Ontarians living with the effects of acquired brain injury who are also experiencing harm as the result of substance use.

Population: 13 million
1 /3 of Canadians 85% in Urban Centers

Reducing Barriers to Integrated Care
Knowledge Transfer
SUBI Materials
Mixed Provider
Workshops
Shared Care
ABI Outreach
Distance Consultation
Program/Policy Screening Data Outcome Evaluation

Traumatic Brain Injury Low Severity High
Severity
High Severity
Quadrant I Acute Medical Settings
and Primary Care
Screening & Brief Interventions
Quadrant II Rehabilitation
Programs & Services
Education, Screening, Brief Interventions &
Linkage
Quadrant III Substance Abuse
System
Screening, Accommodation
& Linkage
Quadrant IV Specialized TBI & Substance Abuse
Services
Integrated Programming
4 Quadrant Model: Types of Services

Continuum of Alcohol Treatment Services
Prev
entio
n
Levels of Treatment Intensity Minimally Intensive
Highly Intensive
Mild to Moderate
Substantial To Severe
Facilitate Recovery without
Treatment
Brief Community
Interventions (e.g.., self-help manuals, physician’s advice)
Short-term Outpatient
Self-Change Oriented
Interventions Short-term Outpatient Therapist- Directed
Interventions
Residential Hospital-Based
Day Treatment
Residential Social Model
Extended Outpatient
Interventions
Long-term Residential
Severity of Alcohol Problems

Matching Clients to Treatment
Lo Lo Hi
Lo-Hi Lo-Hi Mod-Hi
Mod-Hi Mod-Hi Mod
Mod-Hi Lo Mod-Hi
Brief Outpatient
Problem Multiplicity
Social Support & Stability
Outpatient
Day Treatment
Residential
Severity of Use
Provider Manual
• Designed to promote treatment partnerships • Basic information for ABI providers • Basic information for Addictions providers • Information about community teams
• Expansion of Ohio Valley Materials

• Designed to illustrate adaptations of common practice in addictions for ABI
• A place to ‘get started’
for ABI-trained professionals
Downloadable @ www.subi.ca

Recommended for clients who are ready to begin making a change Can be used to structure inpatient intervention or outpatient intervention Provides ‘homework’ that can be reviewed between sessions by workers/family/ client

Clearly stated goal
Support discussion with
client

Written record that is to be completed with the client

Empirically Supported Interventions (General Population)
• Motivational Interviewing • Behavioural Models (Community Reinforcement
and Family Training CRA/CRAFT) • Harm reduction • Case Management • 12 Step (AA/NA) • Pharmacotherapy • Brief Treatment/FRAMES • Cognitive Behavioural Strategies (Relapse
Prevention)

From the literature… ABI-Specific Treatment Models
• Fewer than 25 Studies • Five types of intervention • Strategies for tx retention (Treatment
Incentives/Barrier Reduction) • Intensive case management • Skills training • Motivational Interviewing • Peer Support • Long-term residential programming

C.R.A.F.T. Community Reinforcement and Family Training

Community Reinforcement and Family Training (CRAFT)
1. Motivational strategies 2. Functional analysis of the substance use behavior 3. Domestic violence precautions 4. Communication training 5. Discouragement of using behavior 7. Significant other self-reinforcement training 8. How to suggest direct treatment to the Identified Patient

General Adaptations Challenge Adaptations
Cognitive Impairment Simplified Content Routines that support cognitive compensation (e.g. journaling with supports) Behavioural rehearsal
Impairments of Awareness Focus on environmental supports Allowing for a lengthy period of engagement
Impaired reward system Focus on accepting environmental supports rather than relying on self-management Incentives Drug Testing (with consent)
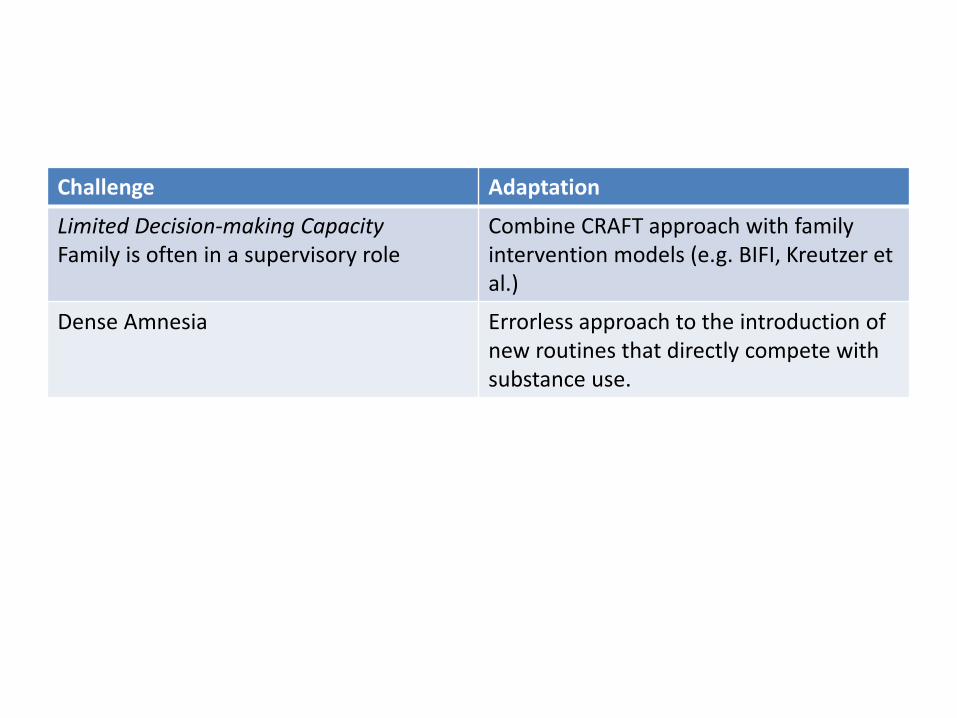
Challenge Adaptation
Limited Decision-making Capacity Family is often in a supervisory role
Combine CRAFT approach with family intervention models (e.g. BIFI, Kreutzer et al.)
Dense Amnesia Errorless approach to the introduction of new routines that directly compete with substance use.

Community Head Injury Resource Services of Toronto
•Outreach
•Residential
• Limited Vocational Services
•Day Programs
1.2 Neuropsychologists
1 Social Worker
1 OT
1 Post-doctoral Fellow
5 Behaviour Therapists
1 Addictions Counselor

Neuro-behavioural Intervention Team
• Ministry Funded • Case load of 25 • 4-8hrs direct community-based support • Unlimited day programming • Neuropsychiatry access • Addictions medicine consultation • Imbedded Addictions Counselor

Services Provided • Neuropsychological Consultation to Partners • Case Resolution/joint triage • Case management • Direct Support • Individual couseling/Psychotherapy • Group
– SUBI – ABI psychoeducation – Support – Psychoeducational groups (anger management, positive
psychology, mindfulness)
ABI-tested interventions
• Treatment incentives • Intensive case management Skills training • Motivational Interviewing • Brief treatment • Long term residential treatment .

SUBI Intervention Structure
• 4-session assessment with treatment incentive • Individualized, based on client goals. • Groups
» MI Based group » (pre-contemplative - contemplative) » 16-week Psycho-educational Group
(Preparation/Action) » After Care/ CHIRS AA
• Intensive Case Management • Integrated Clinical Care
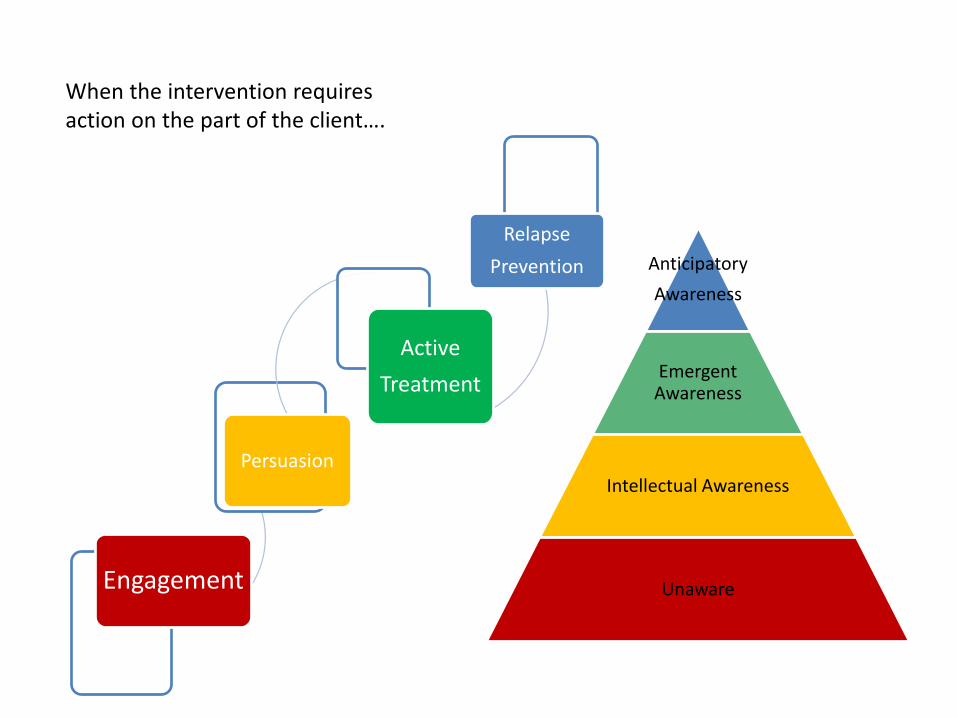
Anticipatory Awareness
Emergent Awareness
Intellectual Awareness
Unaware Engagement
Persuasion
Active Treatment
Relapse Prevention
When the intervention requires action on the part of the client….

Concurrent treatment
Phase of treatment Stage of Change Level of Awareness
Engagement Build rapport
Pre-contemplation No Awareness
Persuasion Build motivation
Contemplation Intellectual Awareness
Active treatment Build intervention
Action Emergent Awareness
Relapse prevention Build safety net
Maintenance Anticipatory Awareness

• Supervision/structured activity • Trustee/Legal system • Reduce exposure to substance • Support to reduce
harms/attend treatment • Family intervention/education
Environmental Supports
Anticipatory awareness
Unaware
Low High

• Client-centered/collaborative goal setting
• Motivational Interviewing • Supported trials • Client education • Cognitive/behavioural
interventions • Cognitive compensation
Collaborative Interventions
Unaware Low High
Anticipatory awareness
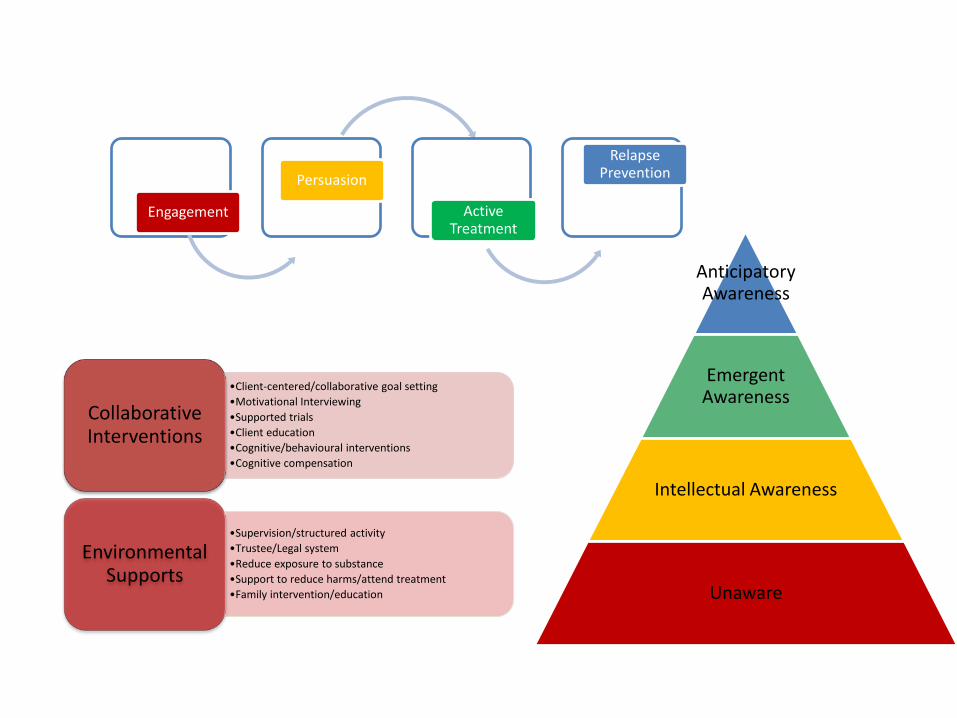
•Client-centered/collaborative goal setting •Motivational Interviewing •Supported trials •Client education •Cognitive/behavioural interventions •Cognitive compensation
Collaborative Interventions
•Supervision/structured activity •Trustee/Legal system •Reduce exposure to substance •Support to reduce harms/attend treatment •Family intervention/education
Environmental Supports
Engagement
Persuasion
Active Treatment
Relapse Prevention
Anticipatory Awareness
Emergent Awareness
Intellectual Awareness
Unaware
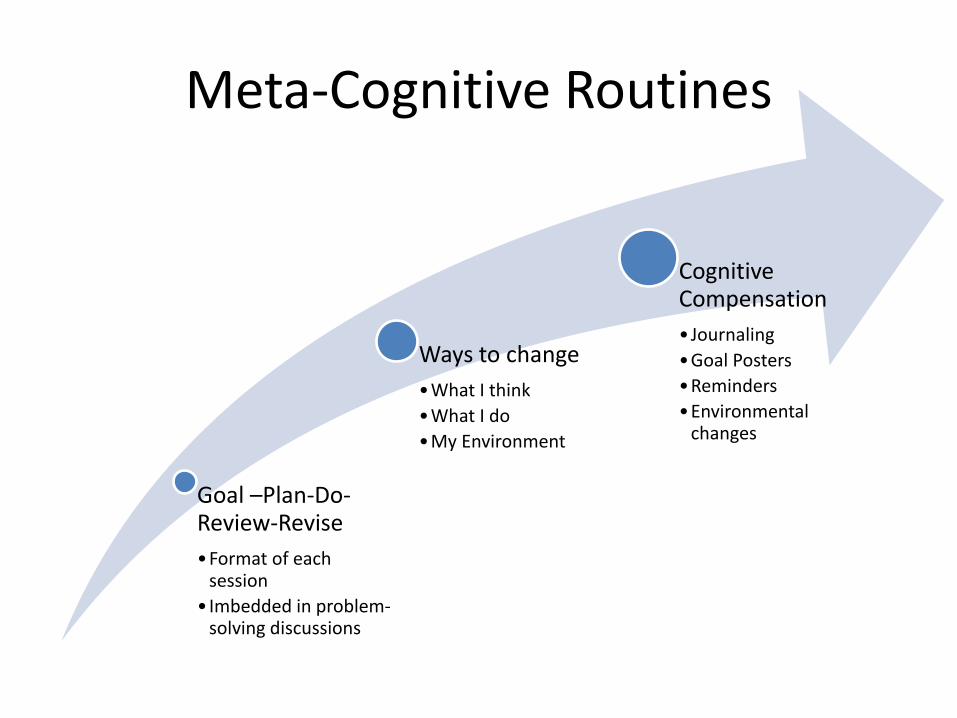
Meta-Cognitive Routines
Goal –Plan-Do-Review-Revise •Format of each
session • Imbedded in problem-
solving discussions
Ways to change •What I think •What I do •My Environment
Cognitive Compensation • Journaling •Goal Posters •Reminders •Environmental
changes

Each phase of the intervention will try to help you to answer different
questions.
Working Together •What is SUBI and how
can it help? What are my rights and responsibilities?
Envisioning the Future •What do I want for my
life? •How does my
substance fit-in with my vision for the future?
•How do I set realistic goals?
Preparing for Change •Formulating goals for
change •Clarifying my reasons
for change
Gathering Resources and Building Skills •How do I fill my time? •Who can support me? •What do I do when I’m
sad, lonely, frustrated or angry?
Taking Action •How do I prevent
problem situations? •What do I do if a
problem occurs? •How do I get around
the problems caused by my brain injury?
Maintaining Gains •What will help me
maintain the gains I have made?
•What is the plan for the long run?

Model of Intervention For the facilitator
Building Alliance
Setting Norms/routines
Creating an emotionally safe
environment
Enhancing Motivation for Change
Clarification of personal goals
Building discrepancy
Fishing for Change Talk
Preparation
Building a schedule of competing
activity
Building a social network/supports
Setting achievable goals
Action
Skill building
Specific changes strategies for substance use
Relapse prevention
Managing Lapses
Building a follow-up plan
A peek at SUBI group

Goals of this session
• Review our challenging situations • Learn to set an intention in a difficult situation • Practice our response in challenging situations

What we heard you say
• C said that you don’t need to be who you were pre-injury. “ you don’t need to (attempt to re-create) the vibrancy of life pre-injury by being intoxicated.
• A identified that it is difficult for her to be the real A. with her friends right now, as they knew A pre-injury, when partying was a way of relating. A also shared that she feels like she is growing up in many ways.

Summary
• We identified that responses to difficult situations will be more successful if we plan ahead.
• We talked about the “rituals” involved in addictive behaviour, and the importance of interrupting the chain of events/ritual
• A, H, and I had the opportunity to problem solve around their triggering events

What we heard you say
• T agreed to try using a prompt this evening in his phone to remind him of his coping strategy.
• I agreed to set up a time to tour the YMCA with Roby- as a potential way to cope with boredom on a Saturday afternoon.
![Clinical Interventions for TBI and Substance abuse [Read-Only] Interventions for TBI... · Clinical Interventions for Individuals with Co-occurring TBI and Substance Abuse Robert](https://img.dokumen.tips/doc/110x75/5e00f2332b224925621e3912/clinical-interventions-for-tbi-and-substance-abuse-read-only-interventions-for.jpg)



























![[Files.indowebster.com] TBI](https://img.dokumen.tips/doc/110x75/577cd9c51a28ab9e78a423d2/filesindowebstercom-tbi.jpg)
