Embed Size (px)
Citation preview
MICU GUIDEBOOK 2013
(1st edition © 2011, 2nd © 2013 )

TABLE OF CONTENTS
1
I. Important Phone Numbers 4 II. Introduction a. Daily checklist b. Procedures 5 i. Central line 6 1. Quick Review 2. Anatomy Review 3. Handling Complications ii. Intubation 9 1. Anatomy 9 2. Common drugs 10
III. Pulmonary a. Acute Respiratory Failure (algorithm) 11 b. Mechanical Ventilation 12 i. Modes 1. Assist-‐control Lung-‐protective ventilation
12
2. Pressure-‐Regulated Volume Control 13 3. Pressure Support Ventilation 13 4. SIMV 13 5. APRV/Bi-‐Vent 14 ii. Common Initial Settings 15 iii. Troubleshooting the Vent 15 iv. Stopping the Vent 15 v. Complications of Ventilation 17 c. Non-‐invasive Positive Pressure Ventilation 18 d. ARDS 20 e. COPD and Asthma in the ICU 22 IV. Cardiovascular a. Post-‐Arrest Care 24 b. Hypotension and Shock 26 i. Definitions/Mechanisms/The Table 26 ii. Hypovolemic 27 iii. Traumatic, Neurogenic, & Hypoadrenal 27 iv. Severe Sepsis & Septic Shock (see also: Sepsis) Measures of volume responsiveness
28 29
v. Cardiogenic Shock & Acute Heart Failure 31 vi. Pulmonary Artery Catheter Waveforms 33 c. Acute Coronary Syndrome i. STEMI 34 ii. NSTEMI & UA 34 d. Arrhythmias i. Bradycardia, AV Block, AV Dissociation 36 ii. Narrow-‐Complex Tachycardia 37 iii. Wide-‐Complex Tachycardia 38 e. HTN Urgency/Emergency (see also: vasodilators in Appendix) 39
TABLE OF CONTENTS
2
f. Aortic Dissection 39 V. Renal a. Acute Kidney Injury 40 b. Low Urine Output 41 c. IV Fluids and Electrolyte Disorders i. IVF 42 ii. Sodium and Water 42 iii. Potassium 44 iv. Calcium 45 v. Phosphorous 46 vi. Magnesium 47 d. Acid-‐base disorders i. Suggestions on How To Approach 48 ii. The Vent as Your Friend iii. Formulae and Reference Values 49 iv. Metabolic Disturbances (Table) 50 v. Respiratory Disturbances (Table) 50
VI. GI and Metabolism a. Upper GI bleed 51 b. Lower GI bleed 52 c. Diarrhea, Constipation, Ileus 53 d. Pancreatitis 55 e. Liver i. LFT Interpretation 56 ii. Acute Liver Failure 57 1. Acetaminophen Overdose: Treatment 57 2. Hepatic Encephalopathy 58 iii. SBP (Table) 59 f. Nutrition i. Basics 60 ii. Types of Enteral Feeding (Table) 60 iii. Parenteral 60
VII. Endocrinology a. DKA and HHS 63 b. Thyroid disease 66 c. Adrenal insufficiency/Stress-‐dose steroids 67 VIII. Infectious Disease a. Fever 68 b. Sepsis (see also Septic Shock) i. Definition, Pathogenesis, Treatment Basics 69 ii. Goals (Table) 70 c. Empiric Antibiotics i. Sepsis without Clear Focus (Table) 71 ii. Sepsis with Skin Findings (Table) 71 iii. Sepsis with Soft Tissue Findings (Table) 71 iv. Neurologic Infections (Table) 72
TABLE OF CONTENTS
3
v. Focal Infections (Table) 72 1. Endocarditis 2. CAP 3. VAP/HAP 4. UTI
d. Meningitis: CSF Characteristics 73 e. Hanta 74 IX. Hematology/Oncology a. Anemia 75 b. Thrombocytopenia 77 c. TTP & HUS 79 d. DIC 80 e. Reversing Coagulopathy (Table) 81 f. Neutropenic Fever & Oncologic Emergencies (Table) 82 X. Neurology a. Altered Mental Status Sedation Management
83 84
b. Stroke (including tPA guidelines) 86 c. Seizure (algorithm) 88 d. Withdrawal 90 i. From Alcohol and Benzodiazepines ii. From Opioids iii. From Cocaine and Amphetamines e. Analgesia & Sedation: 92 i. Medication and Drips (Table) ii. Assessment of Adequate Sedation
XI. Prophylaxis in the ICU a. Infectious Isolation 94 b. GI prophylaxis 94 c. VTE prophylaxis 95 d. VAP prophylaxis 95 e. Sinusitis prophylaxis 95 XII. Appendix (Tables) a. Pressors and Inotropes 96 b. Vasodilators 96 c. Other Cardiac Drips 96 d. Sedatives 97 e. Toxins and Antidotes 97 f. Drugs During Intubation 98 g. Scoring Systems and Prognosis i. APACHE II 99 ii. SOFA 101 h. Medico-‐Legal (Decision-‐maker Hierarchy) 102
Phone Numbers
4
Pulmonary/Critical Care Fellows 2010-‐2011 Pager Additional Number Saman Hayatdavoudi 951-‐1021 Shozab Ahmed 951-‐1645 Jarrod Frizzell 951-‐1665 Erik Kraai 951-‐1022 Scott Helberg 951-‐1005 Jonathan Hechanova 951-‐1040 Maan Moualla 951-‐1019
Pulmonary/Critical Care Attendings
Pager Additional Numbers Michel Boivin 951-‐0714 Lee Brown 951-‐0715 Kitty Busby 951-‐0141 Betty Chang 951-‐0716 Richard Crowell 951-‐0717 Michelle Harkins 951-‐0718 Teri Heynekamp 951-‐0467 Gary Iwamoto 951-‐0719 Lana Melendres 951-‐0762 Pope Moseley 951-‐0631 Ali Saeed 951-‐0660 Akshay Sood 951-‐0100 Eleana Zamora 951-‐0478
MICU Front Line: 272-‐2607 MICU Charge RN: 417-‐4441 (*let Charge know when going to admit/evaluate pt) Radiology cell (at night): 2-‐8351 IR: 2-‐2883 Blood Bank: 2-‐2591 Toxicology: 5-‐5555 Gen Surg: 951-‐0708

Introduction
5
DAILY CHECKLIST √ Review daily labs, replace electrolytes (check to see if already done overnight) √ Interpret daily CXR (don’t wait for radiology read!) √ Review meds (esp any changes), don’t forget to check IV drips & current rate/amount of pressor(s) at bedside √ Note any 24h events, talk to post-‐call resident / night nurse to discuss overnight issues √ Review pt’s plan by systems
ICU issues to be addressed in all daily notes: Neurology Δ in neuro status? Why?
Sedation vacation? Why not? Cardiovascular Hemodynamic issues? (BP, HR trends, pressor trends)
Results of cardiac studies? Bedside ultrasound by fellow? Pulmonary Review ABG/O2 sat
Vent settings/changes? O2 setting? Today’s CXR interpretation
Renal/ Fluids/Electrolytes
I/Os? Current IVF Creatinine? Trending up or down?
GI/Nutrition Nutritional status (pre-‐albumin?) Diet? TF type/rate? Last BM?
Endocrinology Glc between 80-‐150? Insulin Δ? Steroids? Why, how long?
Heme/ID ↑Temp or WBC? Abx? # day and planned stop date? Check pending cultures…including outside cultures
Prophylaxis DVT GI (give indication) VAP (± sinusitis) Bariatric bed for obese pt Skin care?
Dispo Ultimate plan? Getting PT/OT? Do they still need to be in the MICU?
AFTER ROUNDS √ TALK TO PATIENT/FAMILIES!!! (every day! This is mandatory!) √ Follow-‐up on tests/images ordered for that day √ Check out to resident on call √ If you have the next day off, make sure your patients have coverage for that day before you leave!
Introduction—Procedures: Central Lines
6
A Note on Procedures: Becoming proficient in procedures is an essential part of education in the MICU. Below are some basic outlines as to approach, but recognize that procedures can really only be taught by experience. Be aggressive about procedures and never shy away because of inexperience. Instead, find someone to teach you. All central line sites should be evaluated by fellow / attending before attempting. Remember, interns, next year it will be you teaching, so make the most of it while you can!!
CENTRAL LINE INSERTION
I. QUICK REVIEW a. General Indications i. Hypotension (need CVC to run pressors) 1. In sepsis, lactate >4 is also an indication (“occult” or “cryptic” shock) 2. In septic shock, EGDT is essential (see “septic shock” and “sepsis”)Measure hemodynamic variables that can’t be measured noninvasively (e.g., CVP)
ii. Volume resuscitation in hypotensive pt (though short, large-‐bore peripheral IVs have higher flow than triple-‐lumen catheter) iii. Delivery of meds/TPN that can’t be given peripherally iv. Unable to obtain peripheral access (last resort) Relative Contraindications (no absolute contraindications exist, must weigh risk/benefit for individual pt) v. Subclavian: coagulopathy, SVC thrombosis, upper thoracic trauma vi. IJ: tracheostomy, excessive pulmonary secretions, CEA vii. Femoral: IVC compromise, local infection, requirements for pt mobility b. Comparison of sites
Pros Internal Jugular Subclavian Femoral ↓r/o PTX ↑pt comfort Technically easy ↓r/o infxn ↓↓r/o infxn Compressible, no risk to airway Able to assess hemodynamics
Able to assess hemodynamics
No need for CXR
Cons R/o carotid puncture Highest risk of PTX Highest r/o infxn(?*)
Avoid in pt w/ prior carotid endartect
Avoid in coagulopathic if possible
R/o DVT
Difficult with restless pts Relative contraind if SVT thrombus
Cannot assess CVP (unless 30cm catheter used) or if ↑intra-‐abd pressure
N Engl J Med 2003; 248:1123-‐33 *Recent systematic review suggests femoral site infection similar to other sites (Crit Care Med. 2012; 40(8):2479-‐2485,)
II. PROCEDURE REVIEW a. Before placing… i. Check coags/Plt before starting ii. Obtain consent iii. Choose a site
Introduction—Procedures: Central Lines
7
1. Ultrasound likely sites prior to insertion a. At least right and left IJs b. Look at IJ from clavicle to mandible for evidence of clot c. Also scan femoral veins for clot prior to insertion 2. Check for pacer wires, previous line or surgical sites, and (esp for IJ lines) look at site under ultrasound to choose best site (i.e., check both IJs before “just going on right”) 3. If pt has chest tube—use same side as site of central line iv. Have all stuff ready 1. Central line kit 2. Sterile gown, gloves 3. Sterile ultrasound sleeve 4. Biopatch, Tegaderm, luer locks/claves for each port, extra gauze, flushes
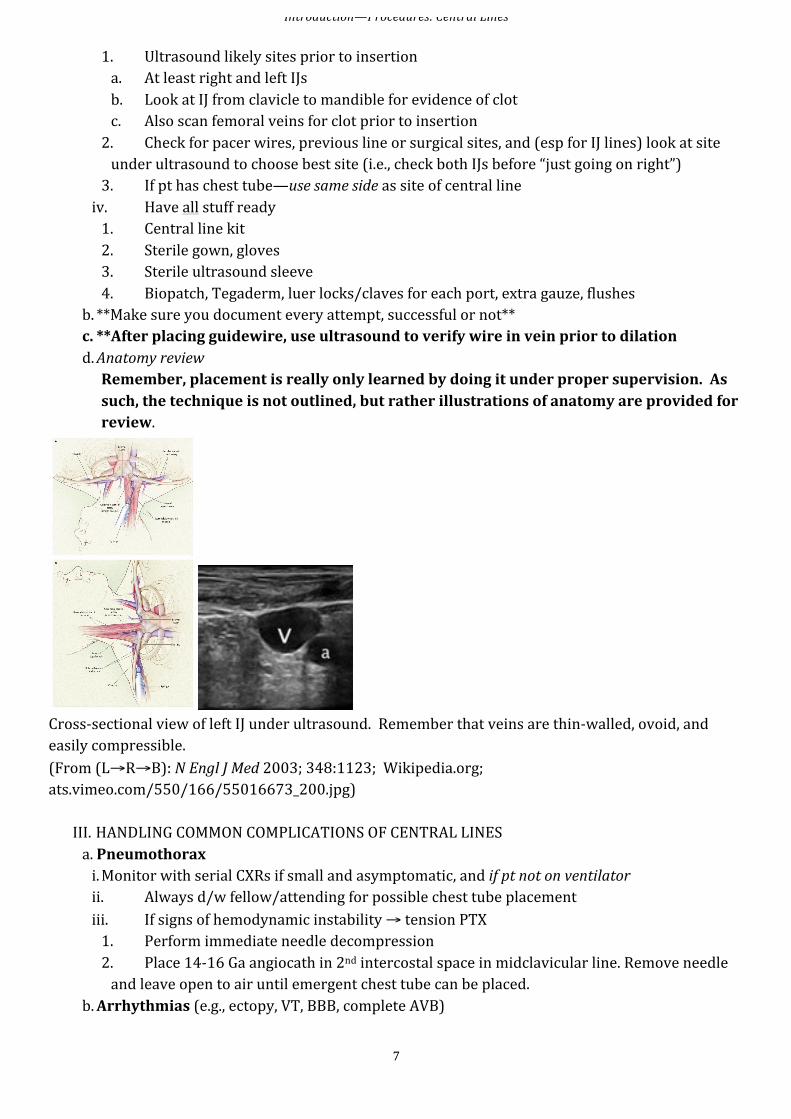
b. **Make sure you document every attempt, successful or not** c. **After placing guidewire, use ultrasound to verify wire in vein prior to dilation d. Anatomy review Remember, placement is really only learned by doing it under proper supervision. As such, the technique is not outlined, but rather illustrations of anatomy are provided for review.
Cross-‐sectional view of left IJ under ultrasound. Remember that veins are thin-‐walled, ovoid, and easily compressible. (From (L→R→B): N Engl J Med 2003; 348:1123; Wikipedia.org; ats.vimeo.com/550/166/55016673_200.jpg)
III. HANDLING COMMON COMPLICATIONS OF CENTRAL LINES a. Pneumothorax i. Monitor with serial CXRs if small and asymptomatic, and if pt not on ventilator ii. Always d/w fellow/attending for possible chest tube placement iii. If signs of hemodynamic instability → tension PTX 1. Perform immediate needle decompression 2. Place 14-‐16 Ga angiocath in 2nd intercostal space in midclavicular line. Remove needle and leave open to air until emergent chest tube can be placed.
b. Arrhythmias (e.g., ectopy, VT, BBB, complete AVB)
Introduction—Procedures: Central Lines
8
i. D/t stimulation of myocardium by catheter or guidewire. Typically resolves after removal of catheter/guidewire ii. If VT → ACLS; if complete AVB, start transcutaneous pacing iii. Prevention; Wire needs only to be advanced to 25cm , follow marks on wiret c. Vascular i. Arterial puncture with needle only: withdraw needle and compress ≥10min ii. Arterial puncture with dilator or catheter: surgical emergency. Leave line/dilator in place and STAT vascular surgery consult. iii. Hematoma: most concerning with IJ line (possible airway/carotid issues) iv. Delayed bleeding can occur, especially with femoral and subclavians sites. If pt becomes hypotensive after line placement follow Hct and consider imaging (CXR or abdo/pelvis CT) to evaluate for occult bleeding as appropriate.
d. Catheter malposition or knotting i. Can withdraw catheter, but cannot advance once placed (change over guidewire) ii. If knotted: don’t pull on catheter, call fellow or IR (risk of venous rupture) e. Air embolism i. Rare; more common during d/c rather than insertion ii. If suspect, position pt in left lateral decub & Trendelenburg to try to trap air in RV iii. Call fellow/attending immediately
Introduction—Procedures: Intubation
9
INTUBATION
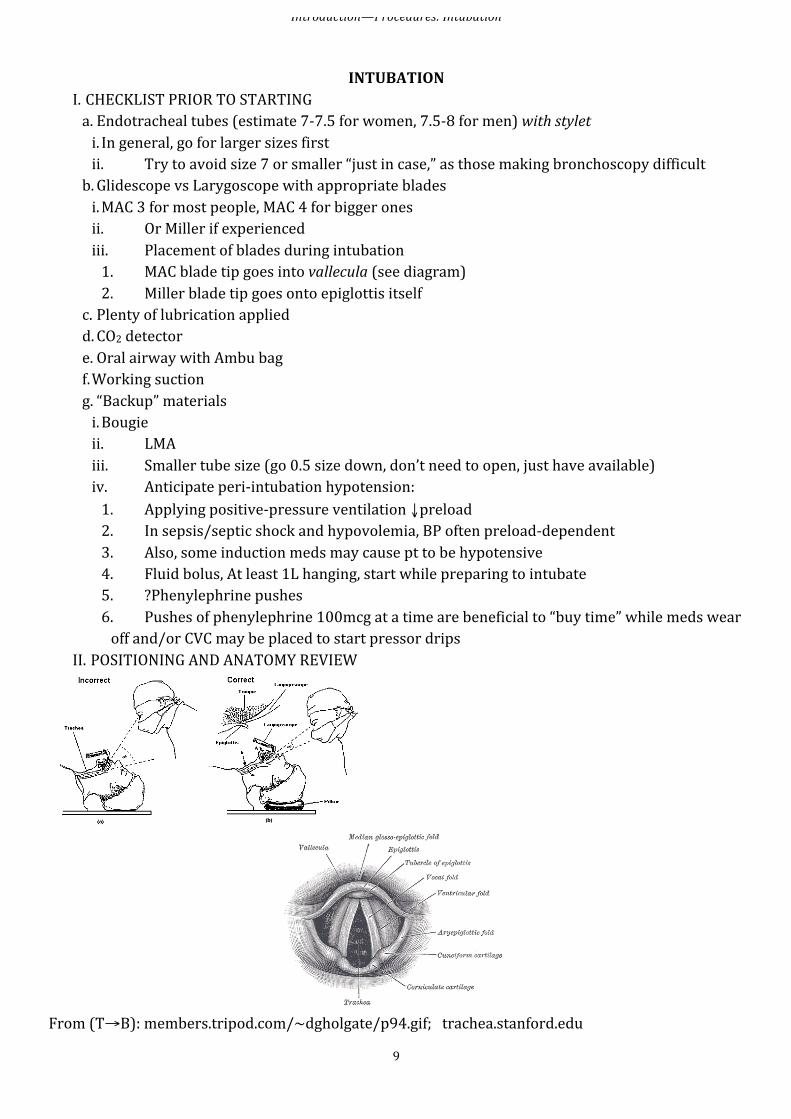
I. CHECKLIST PRIOR TO STARTING a. Endotracheal tubes (estimate 7-‐7.5 for women, 7.5-‐8 for men) with stylet i. In general, go for larger sizes first ii. Try to avoid size 7 or smaller “just in case,” as those making bronchoscopy difficult b. Glidescope vs Larygoscope with appropriate blades i. MAC 3 for most people, MAC 4 for bigger ones ii. Or Miller if experienced iii. Placement of blades during intubation 1. MAC blade tip goes into vallecula (see diagram) 2. Miller blade tip goes onto epiglottis itself
c. Plenty of lubrication applied d. CO2 detector e. Oral airway with Ambu bag f. Working suction g. “Backup” materials i. Bougie ii. LMA iii. Smaller tube size (go 0.5 size down, don’t need to open, just have available) iv. Anticipate peri-‐intubation hypotension: 1. Applying positive-‐pressure ventilation ↓preload 2. In sepsis/septic shock and hypovolemia, BP often preload-‐dependent 3. Also, some induction meds may cause pt to be hypotensive 4. Fluid bolus, At least 1L hanging, start while preparing to intubate 5. ?Phenylephrine pushes 6. Pushes of phenylephrine 100mcg at a time are beneficial to “buy time” while meds wear off and/or CVC may be placed to start pressor drips
II. POSITIONING AND ANATOMY REVIEW
From (T→B): members.tripod.com/~dgholgate/p94.gif; trachea.stanford.edu
Introduction—Procedures: Intubation
10
Assess the Airway: Use the Mnemonic LEMON L – Look externally E-‐ Evaluate the 3-‐3-‐2 rule (3 finger mouth opening, 3 finger hyoid-‐mental distance, 2 finger mandible-‐thyroid M-‐ Mallampatti score O-‐ Obstruction (stridor?) N-‐ Neck mobility
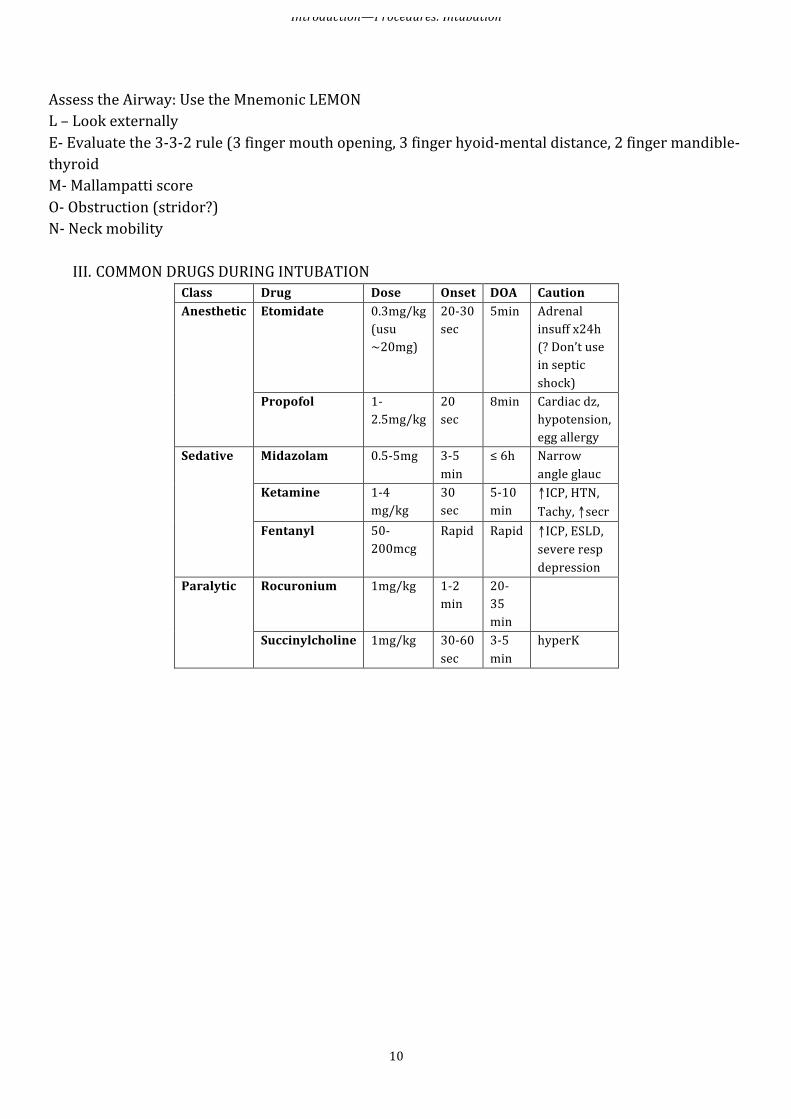
III. COMMON DRUGS DURING INTUBATION Class Drug Dose Onset DOA Caution Anesthetic Etomidate 0.3mg/kg
(usu ~20mg)
20-‐30 sec
5min Adrenal insuff x24h (? Don’t use in septic shock)
Propofol 1-‐2.5mg/kg
20 sec
8min Cardiac dz, hypotension, egg allergy
Sedative Midazolam 0.5-‐5mg 3-‐5 min
≤ 6h Narrow angle glauc
Ketamine 1-‐4 mg/kg
30 sec
5-‐10 min
↑ICP, HTN, Tachy, ↑secr
Fentanyl 50-‐200mcg
Rapid Rapid ↑ICP, ESLD, severe resp depression
Paralytic Rocuronium 1mg/kg 1-‐2 min
20-‐35 min
Succinylcholine 1mg/kg 30-‐60 sec
3-‐5 min
hyperK
PULMONARY—Acute Respiratory Failure
11
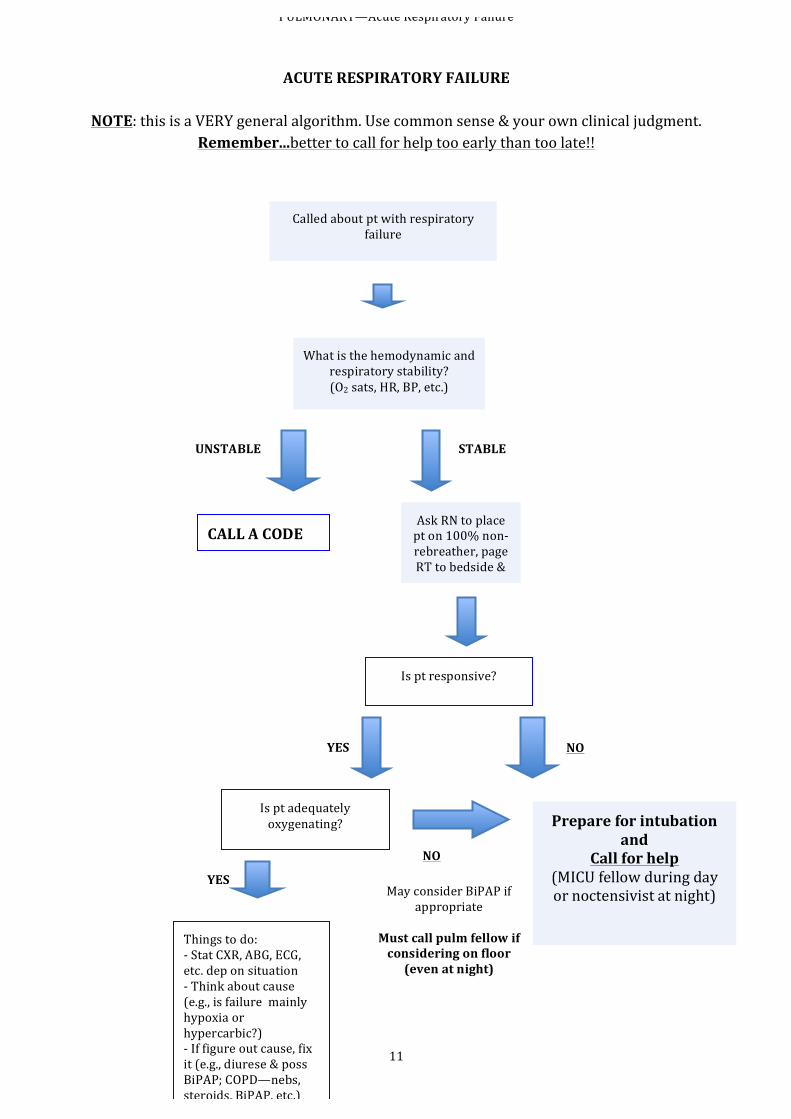
ACUTE RESPIRATORY FAILURE
NOTE: this is a VERY general algorithm. Use common sense & your own clinical judgment.
Remember...better to call for help too early than too late!!
Called about pt with respiratory failure
What is the hemodynamic and respiratory stability? (O2 sats, HR, BP, etc.)
CALL A CODE Ask RN to place pt on 100% non-‐rebreather, page RT to bedside &
SEE PT
Is pt responsive?
Is pt adequately oxygenating? Prepare for intubation
and Call for help
(MICU fellow during day or noctensivist at night)
UNSTABLE STABLE
NO
YES NO
May consider BiPAP if appropriate
Must call pulm fellow if considering on floor (even at night)
Things to do: -‐ Stat CXR, ABG, ECG, etc. dep on situation -‐ Think about cause (e.g., is failure mainly hypoxia or hypercarbic?) -‐ If figure out cause, fix it (e.g., diurese & poss BiPAP; COPD—nebs, steroids, BiPAP, etc.) -‐ If resp failure cannot
YES
PULMONARY—Mechanical Ventilation
12
MECHANICAL VENTILATION
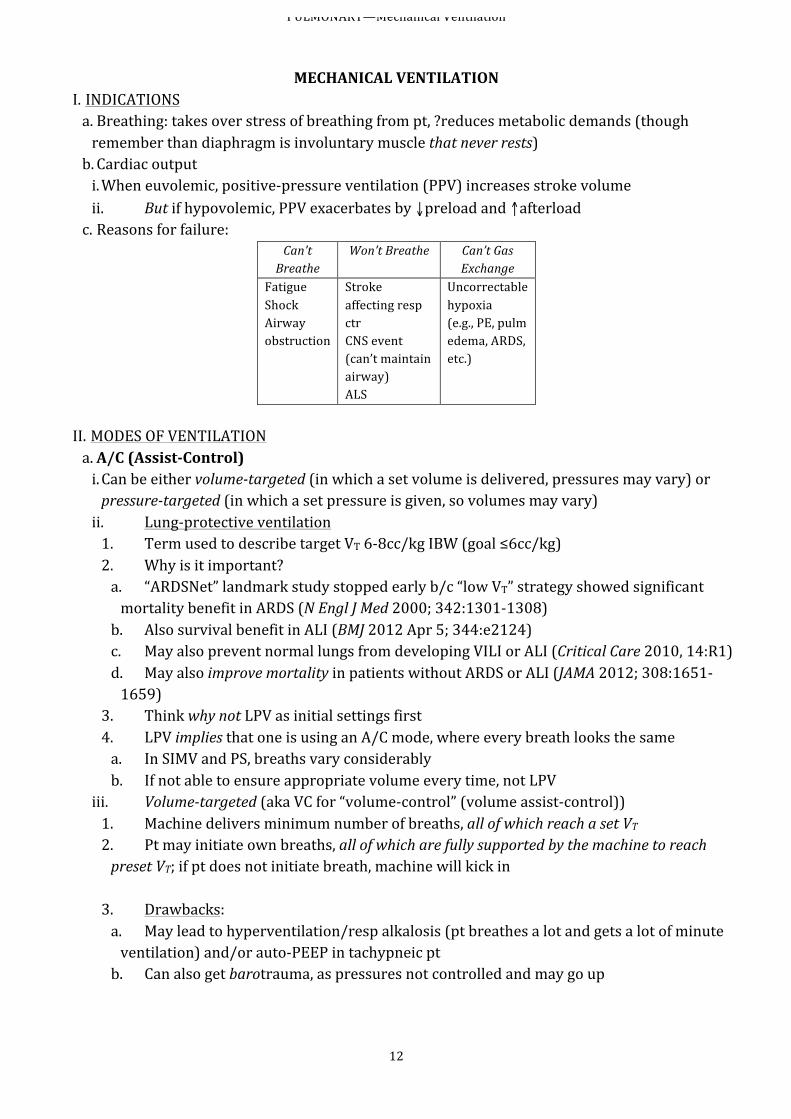
I. INDICATIONS a. Breathing: takes over stress of breathing from pt, ?reduces metabolic demands (though remember than diaphragm is involuntary muscle that never rests) b. Cardiac output i. When euvolemic, positive-‐pressure ventilation (PPV) increases stroke volume ii. But if hypovolemic, PPV exacerbates by ↓preload and ↑afterload c. Reasons for failure:
Can’t Breathe
Won’t Breathe Can’t Gas Exchange
Fatigue Shock Airway obstruction
Stroke affecting resp ctr CNS event (can’t maintain airway) ALS
Uncorrectable hypoxia (e.g., PE, pulm edema, ARDS, etc.)
II. MODES OF VENTILATION a. A/C (Assist-‐Control) i. Can be either volume-‐targeted (in which a set volume is delivered, pressures may vary) or pressure-‐targeted (in which a set pressure is given, so volumes may vary) ii. Lung-‐protective ventilation 1. Term used to describe target VT 6-‐8cc/kg IBW (goal ≤6cc/kg) 2. Why is it important? a. “ARDSNet” landmark study stopped early b/c “low VT” strategy showed significant mortality benefit in ARDS (N Engl J Med 2000; 342:1301-‐1308) b. Also survival benefit in ALI (BMJ 2012 Apr 5; 344:e2124) c. May also prevent normal lungs from developing VILI or ALI (Critical Care 2010, 14:R1) d. May also improve mortality in patients without ARDS or ALI (JAMA 2012; 308:1651-‐1659)
3. Think why not LPV as initial settings first 4. LPV implies that one is using an A/C mode, where every breath looks the same a. In SIMV and PS, breaths vary considerably b. If not able to ensure appropriate volume every time, not LPV
iii. Volume-‐targeted (aka VC for “volume-‐control” (volume assist-‐control)) 1. Machine delivers minimum number of breaths, all of which reach a set VT 2. Pt may initiate own breaths, all of which are fully supported by the machine to reach preset VT; if pt does not initiate breath, machine will kick in 3. Drawbacks: a. May lead to hyperventilation/resp alkalosis (pt breathes a lot and gets a lot of minute ventilation) and/or auto-‐PEEP in tachypneic pt b. Can also get barotrauma, as pressures not controlled and may go up
PULMONARY—Mechanical Ventilation
13
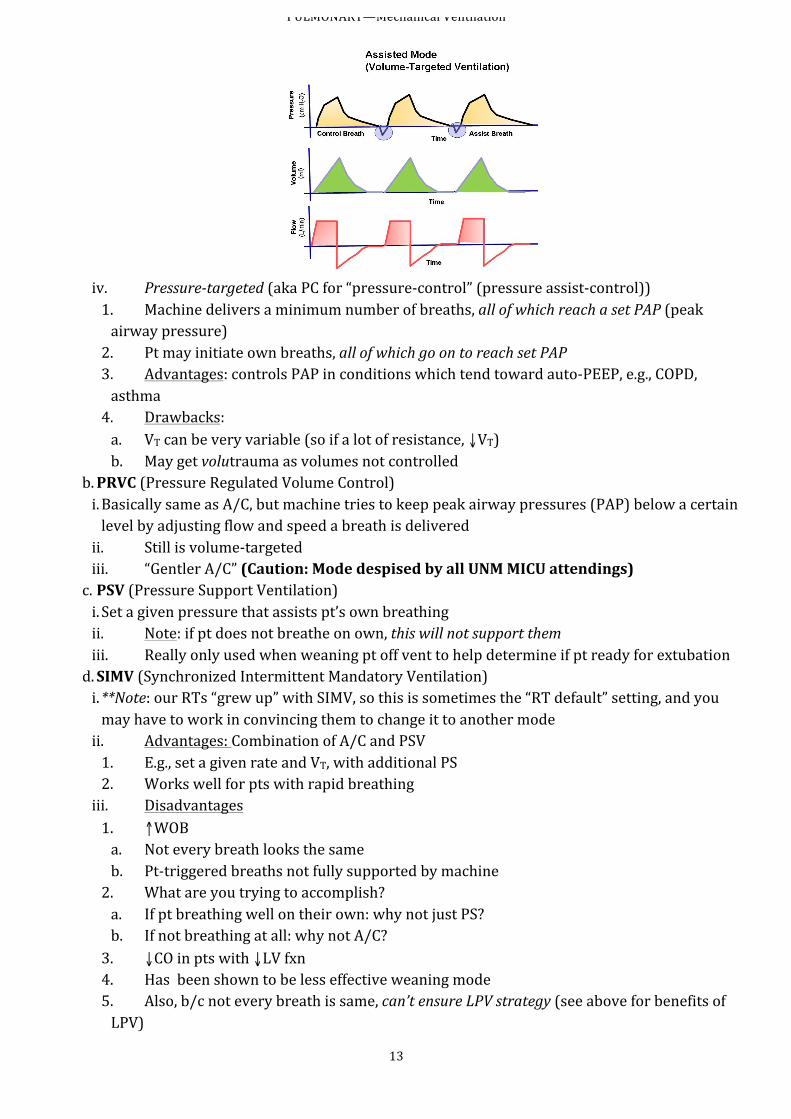
iv. Pressure-‐targeted (aka PC for “pressure-‐control” (pressure assist-‐control)) 1. Machine delivers a minimum number of breaths, all of which reach a set PAP (peak airway pressure) 2. Pt may initiate own breaths, all of which go on to reach set PAP 3. Advantages: controls PAP in conditions which tend toward auto-‐PEEP, e.g., COPD, asthma 4. Drawbacks: a. VT can be very variable (so if a lot of resistance, ↓VT) b. May get volutrauma as volumes not controlled
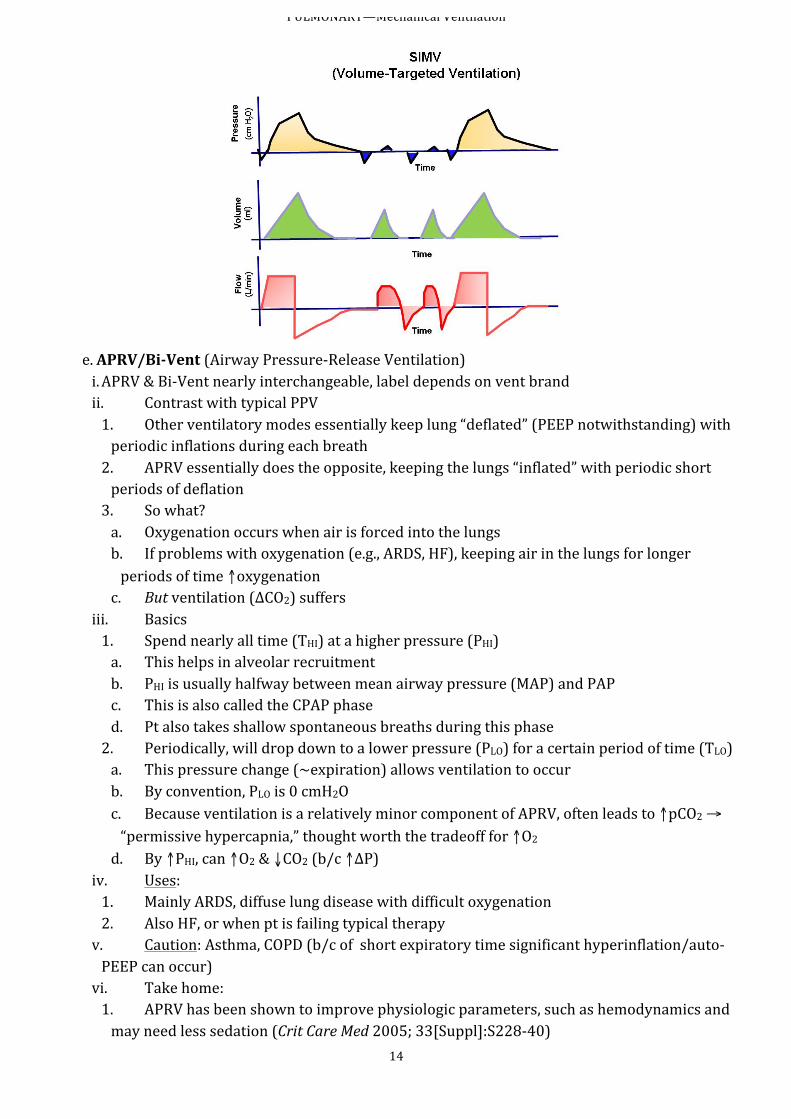
b. PRVC (Pressure Regulated Volume Control) i. Basically same as A/C, but machine tries to keep peak airway pressures (PAP) below a certain level by adjusting flow and speed a breath is delivered ii. Still is volume-‐targeted iii. “Gentler A/C” (Caution: Mode despised by all UNM MICU attendings) c. PSV (Pressure Support Ventilation) i. Set a given pressure that assists pt’s own breathing ii. Note: if pt does not breathe on own, this will not support them iii. Really only used when weaning pt off vent to help determine if pt ready for extubation d. SIMV (Synchronized Intermittent Mandatory Ventilation) i. **Note: our RTs “grew up” with SIMV, so this is sometimes the “RT default” setting, and you may have to work in convincing them to change it to another mode ii. Advantages: Combination of A/C and PSV 1. E.g., set a given rate and VT, with additional PS 2. Works well for pts with rapid breathing iii. Disadvantages 1. ↑WOB a. Not every breath looks the same b. Pt-‐triggered breaths not fully supported by machine 2. What are you trying to accomplish? a. If pt breathing well on their own: why not just PS? b. If not breathing at all: why not A/C? 3. ↓CO in pts with ↓LV fxn 4. Has been shown to be less effective weaning mode 5. Also, b/c not every breath is same, can’t ensure LPV strategy (see above for benefits of LPV)
PULMONARY—Mechanical Ventilation
14
e. APRV/Bi-‐Vent (Airway Pressure-‐Release Ventilation) i. APRV & Bi-‐Vent nearly interchangeable, label depends on vent brand ii. Contrast with typical PPV 1. Other ventilatory modes essentially keep lung “deflated” (PEEP notwithstanding) with periodic inflations during each breath 2. APRV essentially does the opposite, keeping the lungs “inflated” with periodic short periods of deflation 3. So what? a. Oxygenation occurs when air is forced into the lungs b. If problems with oxygenation (e.g., ARDS, HF), keeping air in the lungs for longer periods of time ↑oxygenation c. But ventilation (ΔCO2) suffers
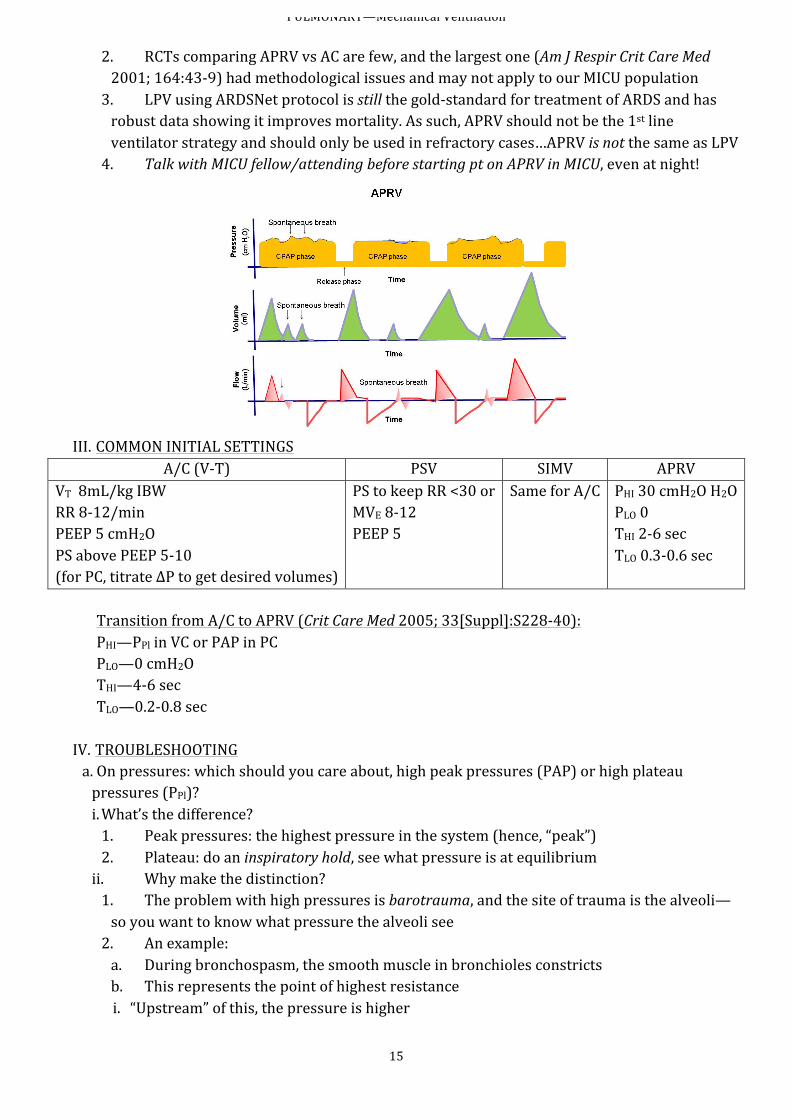
iii. Basics 1. Spend nearly all time (THI) at a higher pressure (PHI) a. This helps in alveolar recruitment b. PHI is usually halfway between mean airway pressure (MAP) and PAP c. This is also called the CPAP phase d. Pt also takes shallow spontaneous breaths during this phase 2. Periodically, will drop down to a lower pressure (PLO) for a certain period of time (TLO) a. This pressure change (~expiration) allows ventilation to occur b. By convention, PLO is 0 cmH2O c. Because ventilation is a relatively minor component of APRV, often leads to ↑pCO2 → “permissive hypercapnia,” thought worth the tradeoff for ↑O2 d. By ↑PHI, can ↑O2 & ↓CO2 (b/c ↑ΔP)
iv. Uses: 1. Mainly ARDS, diffuse lung disease with difficult oxygenation 2. Also HF, or when pt is failing typical therapy v. Caution: Asthma, COPD (b/c of short expiratory time significant hyperinflation/auto-‐PEEP can occur) vi. Take home: 1. APRV has been shown to improve physiologic parameters, such as hemodynamics and may need less sedation (Crit Care Med 2005; 33[Suppl]:S228-‐40)
PULMONARY—Mechanical Ventilation
15
2. RCTs comparing APRV vs AC are few, and the largest one (Am J Respir Crit Care Med 2001; 164:43-‐9) had methodological issues and may not apply to our MICU population 3. LPV using ARDSNet protocol is still the gold-‐standard for treatment of ARDS and has robust data showing it improves mortality. As such, APRV should not be the 1st line ventilator strategy and should only be used in refractory cases…APRV is not the same as LPV 4. Talk with MICU fellow/attending before starting pt on APRV in MICU, even at night!
III. COMMON INITIAL SETTINGS
A/C (V-‐T) PSV SIMV APRV VT 8mL/kg IBW RR 8-‐12/min PEEP 5 cmH2O PS above PEEP 5-‐10 (for PC, titrate ΔP to get desired volumes)
PS to keep RR <30 or MVE 8-‐12 PEEP 5
Same for A/C PHI 30 cmH2O H2O PLO 0 THI 2-‐6 sec TLO 0.3-‐0.6 sec
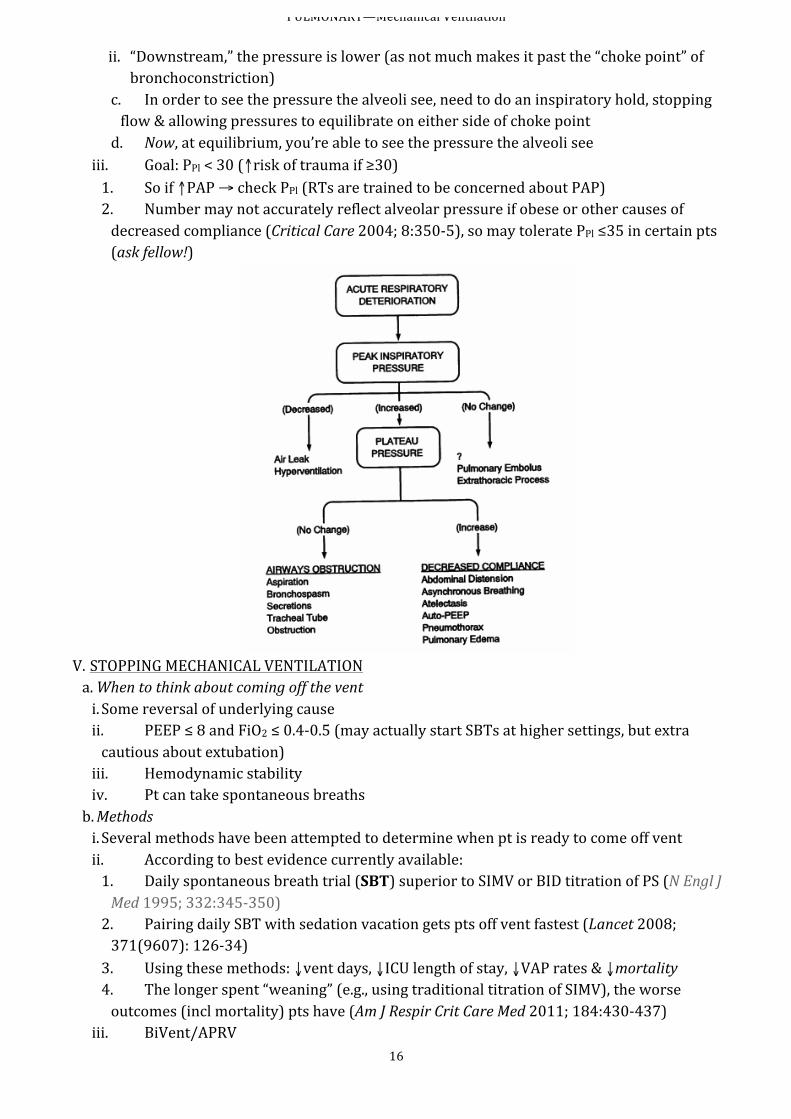
Transition from A/C to APRV (Crit Care Med 2005; 33[Suppl]:S228-‐40): PHI—PPl in VC or PAP in PC PLO—0 cmH2O THI—4-‐6 sec TLO—0.2-‐0.8 sec IV. TROUBLESHOOTING a. On pressures: which should you care about, high peak pressures (PAP) or high plateau pressures (PPl)? i. What’s the difference? 1. Peak pressures: the highest pressure in the system (hence, “peak”) 2. Plateau: do an inspiratory hold, see what pressure is at equilibrium ii. Why make the distinction? 1. The problem with high pressures is barotrauma, and the site of trauma is the alveoli—so you want to know what pressure the alveoli see 2. An example: a. During bronchospasm, the smooth muscle in bronchioles constricts b. This represents the point of highest resistance i. “Upstream” of this, the pressure is higher
PULMONARY—Mechanical Ventilation
16
ii. “Downstream,” the pressure is lower (as not much makes it past the “choke point” of bronchoconstriction)
c. In order to see the pressure the alveoli see, need to do an inspiratory hold, stopping flow & allowing pressures to equilibrate on either side of choke point d. Now, at equilibrium, you’re able to see the pressure the alveoli see
iii. Goal: PPl < 30 (↑risk of trauma if ≥30) 1. So if ↑PAP → check PPl (RTs are trained to be concerned about PAP) 2. Number may not accurately reflect alveolar pressure if obese or other causes of decreased compliance (Critical Care 2004; 8:350-‐5), so may tolerate PPl ≤35 in certain pts (ask fellow!)
V. STOPPING MECHANICAL VENTILATION a. When to think about coming off the vent i. Some reversal of underlying cause ii. PEEP ≤ 8 and FiO2 ≤ 0.4-‐0.5 (may actually start SBTs at higher settings, but extra cautious about extubation) iii. Hemodynamic stability iv. Pt can take spontaneous breaths b. Methods i. Several methods have been attempted to determine when pt is ready to come off vent ii. According to best evidence currently available: 1. Daily spontaneous breath trial (SBT) superior to SIMV or BID titration of PS (N Engl J Med 1995; 332:345-‐350) 2. Pairing daily SBT with sedation vacation gets pts off vent fastest (Lancet 2008; 371(9607): 126-‐34) 3. Using these methods: ↓vent days, ↓ICU length of stay, ↓VAP rates & ↓mortality 4. The longer spent “weaning” (e.g., using traditional titration of SIMV), the worse outcomes (incl mortality) pts have (Am J Respir Crit Care Med 2011; 184:430-‐437)
iii. BiVent/APRV
PULMONARY—Mechanical Ventilation
17
1. Slowly, you “drop and stretch” (↓PHI, ↑THI) 2. Eventually by continuing to drop and stretch, you end up on CPAP of about 15 or so 3. Then can drop CPAP to level of SBT iv. What to look for on SBT 1. RSBI <105 (Rapid Shallow Breathing Index – RR / Vt in L) a. High PPV (80% successful weaning (Am J Respir Crit Care Med 1995; 152:545-‐9)) b. NPV not as high 2. Other signs of distress (↑HR, etc.) 3. What about secretions? Neuro status? (often there are reasons other than respiratory to keep pts on vent)
c. Special considerations i. If COPD reason for intubation, or acquire VAP/HCAP on vent, then there is a mortality benefit in extubation straight to BiPAP, regardless of “how good they look” or whether or not you “think they need it” (Cochrane Database Syst Rev 2010; 8:CD004127, BMJ 2009; 338:b1574) ii. If consistently fail SBTs, think about tracheostomy 1. No real consensus on timing (Chest 2011; 140:1456-‐65) 2. UNM MICU tends to consider trach around day 7-‐14+
d. Failure to wean DDx (FAILTOWEAN) i. Fluid overload → diurese if needed ii. Airway resistance → check ETT: obstructed or too small? iii. Infection → treat appropriately iv. Lying down, bad V/Q mismatch → elevated HOB v. Thyroid, Toxicity of drugs → check TFTs, med list vi. O2 → ↑FiO2 as pt taken off vent vii. Wheezing → nebs viii. Electrolytes, Eating → correct, adequate nutrition ix. Anti-‐inflammatory needed? → consider steroids in asthma/COPD x. Neuromuscular disease e. Consider weaning to NIPPV, esp if from COPD exac (Lancet 2009; 374:1022)
VI. COMPLICATIONS OF VENTILATION a. Oxygen toxicity b. ↓CO? c. VAP, aspiration d. Ventilator-‐dependence e. Laryngeal damage, tracheal necrosis f. Alveolar rupture: PTX, pneumomediastinum/-‐peritoneum, subcutaneous emphysema g. Muscle weakness / deconditioning / loss of mobility
PULMONARY—NIPPV
18
NON-‐INVASIVE POSITIVE PRESSURE VENTILATION (Biphasic Positive Airway Pressure or BiPAP)
(Dr. Gary Iwamoto) I. INDICATIONS a. ABG i. pCO2 >45; pH 7.10-‐7.35 ii. paO2/FiO2 < 200 b. General i. Si/sx of acute respiratory distress ii. Mod-‐severe dyspnea iii. RR >24 iv. Accessory muscle use/paradoxical breathing
II. DIAGNOSES (Respir Care 2009; 54(1):116-‐124) a. COPD b. Acute pulmonary edema (i.e., HF exac) c. Pneumonia (be careful, as often pt would be better served intubated) d. Post-‐extubation respiratory failure III. CONTRAINDICATIONS a. Respiratory arrest (tube them!) b. Trauma/surgery preventing use of mask c. Hemodynamic instability or life-‐threatening arrhythmia (tube them!) d. Excessive secretions or high risk of aspiration (high-‐pressure aspiration bad) e. Impaired mental status (must be able to get mask off, esp if vomit) f. Uncooperative or agitated pt g. Life-‐threatening refractory hypoxemia (e.g., paO2 <60 with FiO2 of 1) IV. MORE LIKELY TO SUCCEED a. Young b. Lower acuity of illness c. Able to cooperate and coordinate breathing with machine d. pCO2 <92; pH 7.10-‐7.35 e. Improvement in gas exchange/HR/RR within 1st 2h, o/w think about intubation V. INITIATION a. HOB at 45o b. Get correct mask size, start with IPAP of 10 cmH2O and EPAP of 0 c. Hold mask to face until pt is comfortable, then secure with head straps d. Slowly ↑EPAP to ≥5 e. ↑IPAP to 10-‐12 to achieve VT 8-‐10 mL/kg f. Evaluate for adequate ventilatory support, consider setting backup rate g. If hypoxic, attempt to titrate FiO2 to <0.6; go up on IPAP to help achieve this h. Adjust according to O2 sats and ABG i. Recheck in 1-‐2h; if no improvement, consider intubation VI. REMEMBER a. BiPAP is a bridge…either to pt improvement or to intubation b. It is not a “bridge to nowhere” i. If pt is DNI must have frank discussion with family prior to initiation

PULMONARY—NIPPV
19
ii. Be prepared to take DNI pt off BiPAP if not improving (may allow for longer than the 2h, but pt should not be on BiPAP for longer than 24h without explicit approval from attending/fellow)
PULMONARY—ARDS
20
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) I. DIAGNOSTIC CRITERIA (“Berlin Definition”: JAMA 2012; 307:2526-‐2533) a. Acute onset of respiratory failure b. Bilateral infiltrates on CXR (nb: some cases of ARDS do present unilaterally or with pleural effusion) c. Absence of clinical evidence of left atrial hypertension i. Not cardiogenic pulmonary edema ii. Normal echo or PCWP ≤18 d. Hypoxia i. Severe ARDS = PaO2/FiO2 < 100 ii. Moderate ARDS = PaO2/FiO2 100-‐200 iii. Mild ARDS = PaO2/FiO2 200-‐300
II. CAUSES Direct Lung Injury Indirect Lung Injury Pneumonia Aspiration Pulmonary contusion Inhalational injury Near-‐drowning Fat Emboli
Sepsis Severe trauma with shock TRALI Pancreatitis Drug overdose Cardiopulmonary Bypass Medications (Amiodarone, chemo etc..)
III. TREATMENT—ARDSNET PROTOCOL (review: Chest 2010; 137:1203-‐16) a. Treat underlying cause b. Vent settings (Chest 2007; 131:921) i. Initial: 1. Use A/C volume-‐targeted mode, VT 6-‐8 cc/kg IBW, PEEP 5-‐12 2. This is called “lung protective ventilation” 3. Start at 8cc/kg, then titrate down to 6cc/kg in a stepwise fashion 4. Low-‐volume/high PEEP settings may be uncomfortable for pt, may need sedation (try to minimize)
ii. Daily vent management: goal is for alveolar recruitment 1. Keep plateau pressure (PPL) ≤ 30 to prevent barotrauma a. If PPL > 30, ↓VT to 5 cc/kg or lower as needed b. If PPL < 25 and VT < 6 cc/kg, ↑ VT until PPL > 25 or VT = 6 cc/kg 2. pH goal 7.30-‐7.45 (“permissive hypercapnia”) 3. pO2 goal 55-‐80, with O2 sats 88-‐95% iii. Other considerations: 1. No real outcome difference between VC & PC modes (Chest 2011; 140(2): 286-‐94) but if PC used, must keep eye on VT to make sure still lung protective 2. APRV may be tried (CPAP phase keeps alveoli open for longer) 3. Prone positioning (i.e., rotating bed) 4. Paralysis (N Engl J Med 2010; 363:1107-‐16) a. Inclusion criteria: i. Severe ARDS (PaO2/FiO2 ≤120) ii. W/in 1st 48h of dx b. Excluded pts included COPD on home O2 & liver pts, among others c. Protocol:

PULMONARY—ARDS
21
i. Cisatracurium: 15mg bolus → 37.5mg/h gtt ii. Paralyzed for 48h straight iii. Do not do sedation vacations while paralyzed! d. Benefit: ↓mortality e. Must be fellow/attending-‐approved
PULMONARY— COPD and Asthma
22
COPD (Thorax 2002; 57(12):1079)
I. GENERAL a. Like any COPD exacerbation, must treat underlying cause (e.g., PNA) b. Don’t forget the use of steroids, etc., just as in other exac c. Key is recognition of need of assisted ventilation, either NIPPV or intubation d. Mucous plugging can be a big deal i. Therapeutic bronch ii. Chest physiotherapy
II. MECHANICAL VENTILATION a. Mostly bedside evaluation (consider work of breathing as an indication for increased support) b. 27% of COPD with pH 7.25-‐7.35 required intubation, compared with 57% of pH < 7.2 c. Think about NIPPV first (see above discussion), especially if pH < 7.3 despite efforts to address underlying etiology i. Uncertain if helps if initial pH < 7.25 ii. Can always progress to intubation (unless DNI); NIPPV fails in up to 30% d. Invasive mechanical ventilation i. Volume-‐targeted 1. Initial settings: VT 8-‐12ml/kg IBW, I:E ratio of 1:2.5—1:3 2. Obstructive disease necessitates ↑expiratory time a. In practice, works by ↓RR. Recommend starting at lower RR (12-‐15) b. Can always adjust, though remember, not aiming for normal pCO2 or pH 3. Avoid use of PEEP (start off with PEEP 0, can always adjust…), as can exacerbate “breath-‐stacking” 4. High risk of ↑PPL → barotrauma → poss PTX, pneumomediastinum, etc ii. Pressure-‐targeted 1. Preferred in obstructive lung disease 2. Goal: PPL < 30 iii. In either case ensure adequate time for exhalation and monitor Auto-‐PEEP. Ignore peak pressures…no relevance to barotrauma…follow plateau.
III. LIBERATION (Lancet 2009; 374:1082) a. Assess for readiness for extubation (SBT) every day (as any other pt) b. Weaning from invasive to NIPPV may help to prevent re-‐intubation
ASTHMA I. GENERAL a. Cont typical treatment for asthma exacerbation: O2, albuterol/ipratropium, ?Mg
PULMONARY— COPD and Asthma
23
b. ABG phases i. Mild: respiratory alkalosis, ↓pCO2, nl or ↑pO2 ii. Mod: normal pH, nearl nl pCO2, ~↓O2 iii. Severe: respiratory acidosis, ↑pCO2, ↓O2 iv. Must be able to recognize that normal ABG in asthma exacerbation, when pt doesn’t look good, is a BAD sign 1. If mild, should be hyperventilating as airway narrowing and subjective dyspnea out of proportion to physiologic derangement 2. As progresses, pt getting tired, so start to retain CO2, which is a sign of impending respiratory failure 3. At this point, start thinking about intubation or (at least) NIPPV
II. ICU a. Use high dose steroids (methylprednisolone 120mg IV q6h) b. NIPPV may ↓ need for intubation c. If need to intubate: large ETT, keep PPL < 30 if possible (treat like COPD) i. Again, like COPD, avoid PEEP if possible so as to avoid air-‐trapping (start PEEP 0) ii. Ensure adequate exhalation time (again, start with lower RR)
III. Rescue Therapies for Status Asthmaticus a. Magnesium 2g IV b. Terbutaline 0.5 mg S/Q q4h / Epinephrine (0.2 mg S/Q q 20-‐60 min) c. Heliox 30-‐40% d. Leukotriene receptor antagonists (Singulair 10 mg po)
Cardiovascular—Post-‐Cardiac Arrest
24
POST-‐CARDIAC ARREST CARE Circulation 2010; 122:S768-‐86
I. General a. For the specifics on what to do during a cardiac arrest, see ACLS b. For all survivors, it is important to go through the “H’s and T’s” of the etiology c. This focuses on post-‐arrest care II. Sedation? a. Avoid sedation to allow better estimation of neuro status, etc. b. If must use, intermittent boluses or short acting agents (propofol or dexmedetomidine): treat symptoms c. If decide to paralyze, should sedate III. To cool, or not to cool? (J Am Coll Cardiol 2012; 59:197-‐210; Circulation 2011; 123:1428-‐35; N
Engl J Med 2010; 363:1256-‐64;) a. Therapeutic hypothermia (TH) is an engaging and fiercely debated topic, on which there is often no clear answer b. What is clear: i. Pts with initial rhythm of VF/VT have better neurologic outcomes if they get TH ii. The longer the time to CPR, the worse the outcome c. What is not clear: i. Pts with PEA/asystole 1. No trial to date has found a benefit to TH in these pts 2. Theoretically, the mechanism of injury to the brain is similar to those with VF/VT 3. There may be a selection bias, as PEA/asytole has a worse prognosis than VF/VT to begin with
ii. How long should TH last (18h, 24h, more?) d. Suggestions on approaching (these are general statements, often attending-‐dependent) i. Note for all: pt must be comatose (GCS ≤8) for consideration. If not in coma, do not need TH ii. If initial rhythm VF/VT → initiate TH protocol (cards should be involved) iii. If initial rhythm PEA/asystole 1. If pt young, no apparent comorbid condition → initiate TH 2. If cause of arrest is an overdose → likely do not cool a. Slows down drug metabolism b. Working against treatment of underlying cause and supportive care 3. If unknown down time → do not cool 4. If down time ≥30min → do not cool 5. If has brain edema on initial CT scan of head → do not cool iv. Clear contraindications 1. Active infection 2. Bleeding v. Call the fellow or attending regarding whether or not to initiate TH, 1. Do not feel obligated to continue TH if initiated in ED 2. Remember, the MICU is the service responsible for managing these pts, and so the ultimate decision is ours
IV. Prognostication post-‐arrest (Neurology 2006; 67:203-‐10, updated 6/23/2009)
Cardiovascular—Post-‐Cardiac Arrest
25
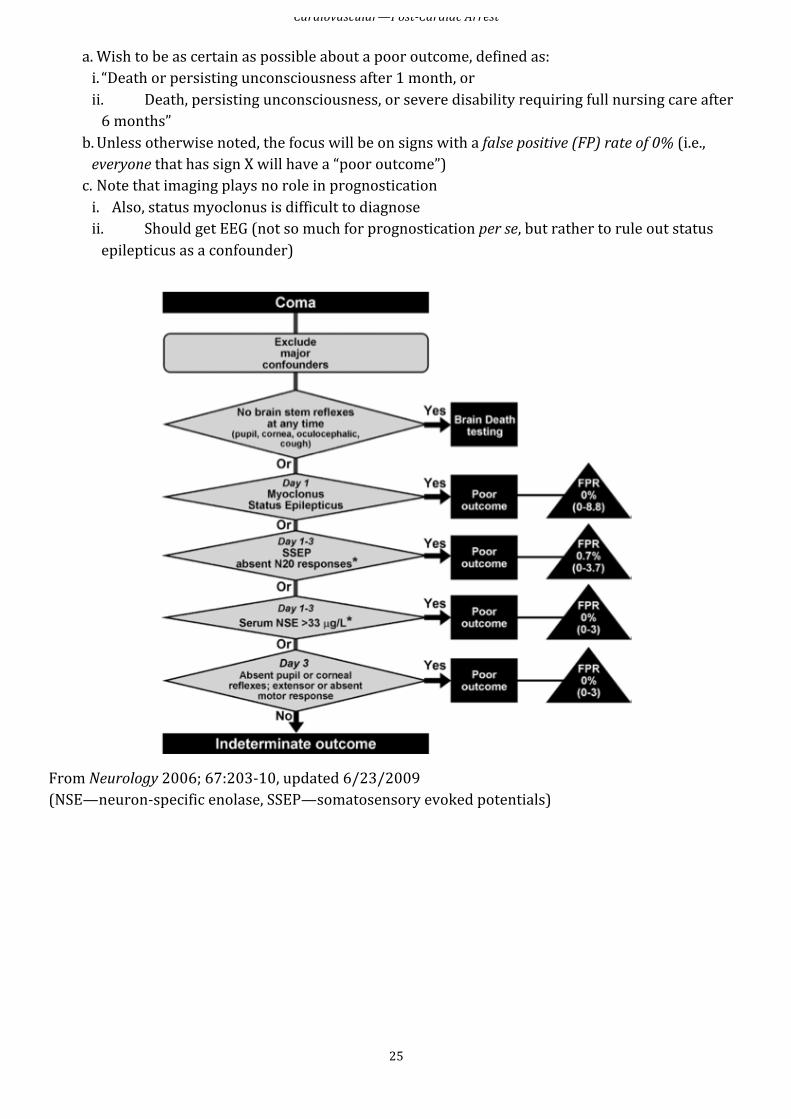
a. Wish to be as certain as possible about a poor outcome, defined as: i. “Death or persisting unconsciousness after 1 month, or ii. Death, persisting unconsciousness, or severe disability requiring full nursing care after 6 months”
b. Unless otherwise noted, the focus will be on signs with a false positive (FP) rate of 0% (i.e., everyone that has sign X will have a “poor outcome”) c. Note that imaging plays no role in prognostication i. Also, status myoclonus is difficult to diagnose ii. Should get EEG (not so much for prognostication per se, but rather to rule out status epilepticus as a confounder)
From Neurology 2006; 67:203-‐10, updated 6/23/2009 (NSE—neuron-‐specific enolase, SSEP—somatosensory evoked potentials)
Cardiovascular—Hypotension and Shock
26
HYPOTENSION AND SHOCK
a. Definition i. Shock: hypotension (usually MAP <55-‐60) WITH evidence of tissue hypoperfusion and hypoxia, i.e., end-‐organ dysfunction (oliguria, CNS sx, lactic acidosis, low SvO2, etc.) ii. Just having “low BP” doesn’t cut it b. Mechanisms: i. “Empty” left heart (i.e., low LV preload, Hypovolemic) 1. True hypovolemia: hemorrhage, dehydration, etc. 2. Effective hypovolemia: a. RV failure b. Tamponade c. Tension PTX d. PE e. High intrathoracic pressure (e.g., PEEP)
ii. Bad pump (Cardiogenic) 1. Bad muscle (e.g., MI) 2. Bad valves 3. Bad rate or rhythm 4. Both bad muscle and bad valves iii. Low SVR 1. Inappropriate loss of vascular tone: “Classic” low SVR shock: a. Cytokine release: TNF, IL-‐1, etc. (e.g., sepsis/SIRS, anaphylaxis) b. Neurogenic (e.g., SAH, acute cord injury, etc.) c. Drug-‐induced (e.g., IL-‐2 therapy) 2. Systemic hyperdynamic/-‐metabolic/-‐catabolic state (RARE) a. Wet beriberi b. DTs c. Thyroid storm 3. Significant peripheral left-‐right shunting (RARE causes) a. Paget’s b. Advanced liver disease
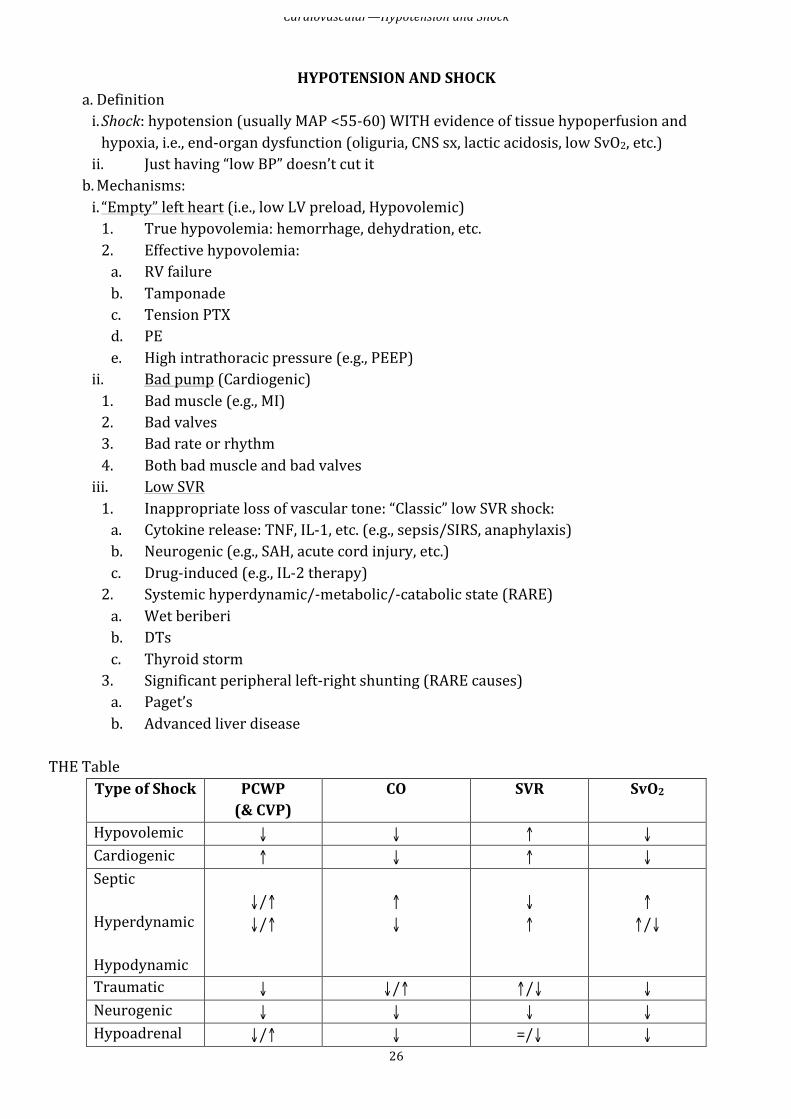
THE Table Type of Shock PCWP
(& CVP) CO SVR SvO2
Hypovolemic ↓ ↓ ↑ ↓ Cardiogenic ↑ ↓ ↑ ↓ Septic Hyperdynamic Hypodynamic
↓/↑ ↓/↑
↑ ↓
↓ ↑
↑ ↑/↓
Traumatic ↓ ↓/↑ ↑/↓ ↓ Neurogenic ↓ ↓ ↓ ↓ Hypoadrenal ↓/↑ ↓ =/↓ ↓
Cardiovascular—Hypotension and Shock
27
Normal values ≤12 mmHg (≤6)
4-‐8 L/min (CI 2.6-‐4.2 L/min/m2)
800-‐1200 dyne-‐sec/cm5
~75%
Pulmonary capillary wedge pressure (PCWP): measure of preload (and roughly central venous pressue (CVP)) Cardiac output (CO)—product of heart rate and stroke volume (SV is affected by preload, afterload, and contractility); cardiac index (CI) = CO/BSA Systemic vascular resistance (SVR) ( = [80 x (MAP – CVP)/CO) Venous O2 saturation (SvO2)—measure of tissue perfusion
HYPOVOLEMIC SHOCK
I. Cause: a. Loss of RBC/plasma: hemorrhage b. Loss of plasma: “third-‐spacing”, GI, urinary, insensible II. Dx: important to differentiate between hypovolemic vs. cardiogenic (manage very different) a. Same: ↓CO, ↑SVR (also tachycardic) b. But: cardiogenic has JVD (↑CVP), rales, S3 gallop
Mild (<20% volume loss) Moderate (20-‐40%) Severe (>40%) Cool extremities ↑ capillary refill time Diaphoresis Collapsed veins Anxiety
Same, plus: Tachycardia Tachypnea Oliguria Postural changes
Same, plus: Hemodynamic instability Marked tachycardia Hypotension MS deterioration (coma)
III. Tx: a. Initial: volume, volume, volume (↑preload: ↑SV, ↑CO) b. If still hemodynamically unstable: i. Ongoing blood loss, Hb <10 → transfuse (if stable, keep Hb >7) ii. Inotropic support: dopamine, vasopressin, dobutamine 1. Problem is getting blood to tissues (not enough blood) 2. So pressors (like NE) make worse by constricting vessels
c. Respiratory support TRAUMATIC SHOCK
I. Usually d/t hypovolemia (consider tension pneumo / tamponade) II. Even when hypovolemia controlled, can third-‐space into injured tissues; exacerbated by secondary microcirculatory injury. Can evolve into distributive.
III. Tx: ABCs, must control hemorrhage; early stabilization of fx, debridement of wounds, evacuation of hematoma all help
NEUROGENIC SHOCK
I. Cause: interruption of sympathetic vasomotor input (bradycardia and ↓SVR) a. Injury to high cervical cord or head b. Inadvertent cephalad migration of spinal anesthesia II. Dx: arterial/venous dilation → warm extremities, venous pooling (so ↓CO by ↓preload) III. Tx:
Cardiovascular—Hypotension and Shock
28
a. Acutely: volume (could be lots, as everything’s blown wide open so could take quite a bit to fill up to give pressure) b. After r/o hemorrhage: pressors (NE or phenylephrine) c. Cervical spine clearance i. If alert & asymptomatic without a distracting injury or neurologic deficit → functional range-‐of-‐motion exam → if no problems can be cleared without any imaging (sens 98.1% NPV 99.8% (J Orthop Trauma 2010; 24:100-‐6) ii. If obtunded & blunt trauma → CT c-‐spine detects 99.75% of clinically significant injury (J Trauma 2010; 68:576-‐82) iii. MRI does not appear to add much to C-‐spine clearance (Am Surg 2012; 78:741-‐4)
HYPOADRENAL SHOCK
I. Cause: adrenocortical insufficiency (Addisonian crisis, idiopathic atrophy, TB, mets, bilateral hemorrhage, amyloidosis, gonococcal (Waterhouse-‐Friderichson)) a. Lose homeostatic mechanisms b. ↓SVR, hypovolemia, ↓CO c. Mineralocorticoids → retain intravascular volume, glucocorticoids → maintain vascular tone II. Dx/Tx: a. Empiric dexamethasone in persistently hemodynamically unstable pt (doesn’t mess up ACTH stim test acutely) b. Corticotropin stim test: if fail, give hydrocortisone, taper as stabilize c. Must have volume and pressors
SEVERE SEPSIS AND SEPTIC SHOCK see also: sepsis
I. Septic shock a. Phases? i. Hyperdyanmic/vasodilatory phase: ↑CO (cardiac compensation for ↓SVR) + impaired tissue oxygen extraction → ↑venous O2 sat ii. Hypodynamic: ↓O2 delivery from depressed myocard, hypovolemia, etc → ↓venous O2 sat
b. Phases may or may not be sequential, and in both can have tissue hypoxia and anaerobic metabolism (i.e., ↑lactate) (cf. Chest 2011; 140(6):1406-‐19)
II. Dx/Clinical Manifestations (recall SIRS) a. Early: hypervent, disorientation, confusion b. Hypotension/DIC → acrocyansois, ischemic necrosis distal tissues c. Cardiopulmonary: i. V/Q mismatch → ↓PO2 → ↑alv cap perm →→ARDS ii. Hypotension from maldistribution of flow d. Renal: oliguria, azotemia, proteinuria, ATN e. Coagulopathy: thrombocytopenia, DIC III. Tx a. Antimicrobials (examples of empiric regimens)
Condition Example Regimen β-‐lactam allergy Immunocompetent Ceftriaxone or pip-‐tazo, add vanc if high MRSA
rate (Cipro or levofloxacin) + clinda (+vanc)

Cardiovascular—Hypotension and Shock
29
Neutropenia Meropenem or (piper-‐tazo +tobra) Splenectomy Ceftriaxone (+vanc if MR pneumococci high) Vanc + (cipro or levo) IVDU Nafcillin (or vanc) + gentamicin Vanc + gent AIDS Pip-‐tazo + tobra Cipro/levo + vanc + tobra
b. Removal of infection source (central lines, tampons for TSST, etc.) c. Hemodynamic, Respiratory, Metabolic support i. Volume CVP ≥8, keep uop >0.5mL/kg/h ii. Goals: MAP > 65 (SBP >90), consider SvO2 > 70% iii. Pressors: norepinephrine, vasopressin; dobutamine if ↓SvO2/lactate clearance 1. Typical order of pressors: a. i. NE appears to be clear 1st line (N Engl J Med 2010; 362:779-‐89; Crit Care Med 2012; 40:725-‐30)
ii. If pt has been on DA for ≥24-‐48h at outside hospital & is responding, consider leaving vs switching over to NE
b. Vasopressin: hits different receptors (V vs α/β) c. 3rd line pressor variablemay consider: i. Dobutamine (if evidence of hypodynamic stage – i.e. low Svo2, poor lactate clearance) ii. Epi (has both inotropic & pressor activity) iii. Phenylephrine (esp if tachycardia is an issue) iv. DA
iv. When to vent: progressive hypoxemia, hypercapnia, neuro deterioration, resp muscle failure v. Think about adrenal insuff (stress dose steroids – HC 100 mg q 8hIV); fix Glc
IV. Progosis: death within 30d: 20-‐35% w/ severe sepsis, 40-‐60% w/ septic shock if they are not adequately resuscitated early (EGDT reduces mortality by ½)
Treatment goals in septic shock: -‐ SaO2 ≥95% -‐ SvO2 ≥ 70% (maybe) (or lactate clearance ≥10% (JAMA 2010 303(8):739)) -‐ Urine output ≥0.5mL/kg/hr (~30cc/h) -‐ pH ≥7.20 -‐ MAP ≥ 65 -‐ HR ≤120 (sinus) -‐ lactic acid ≤3 and/or HCO3 ≥15 -‐ Phos ≥2 -‐ normal mental status -‐ functioning GI tract and normal LFTs -‐ warm/perfused extremities/digits
V. Beyond EGDT: Assessing volume responsiveness (J Intensive Care Med 2009; 24:329-‐37; Ann
Intensive Care 2011; PMID 21906322) a. Clinical question: in this patient with hypotension, would giving fluid (increasing preload) provide the effect of increasing SV and therefore BP?
Cardiovascular—Hypotension and Shock
30
b. Too much fluid may be a bad thing (Crit Care Med 2011; 39:259-‐65; Chest 2008; 133:252-‐63)) i. Positive fluid balance and high CVP are independent markers of mortality in septic shock ii. It’s important to give fluids in the 1st 12h or so, but after that it may be more harm than good iii. CVP is a terrible indicator of volume status, especially outside the window of EGDT (Chest 2008 134:172-‐8)
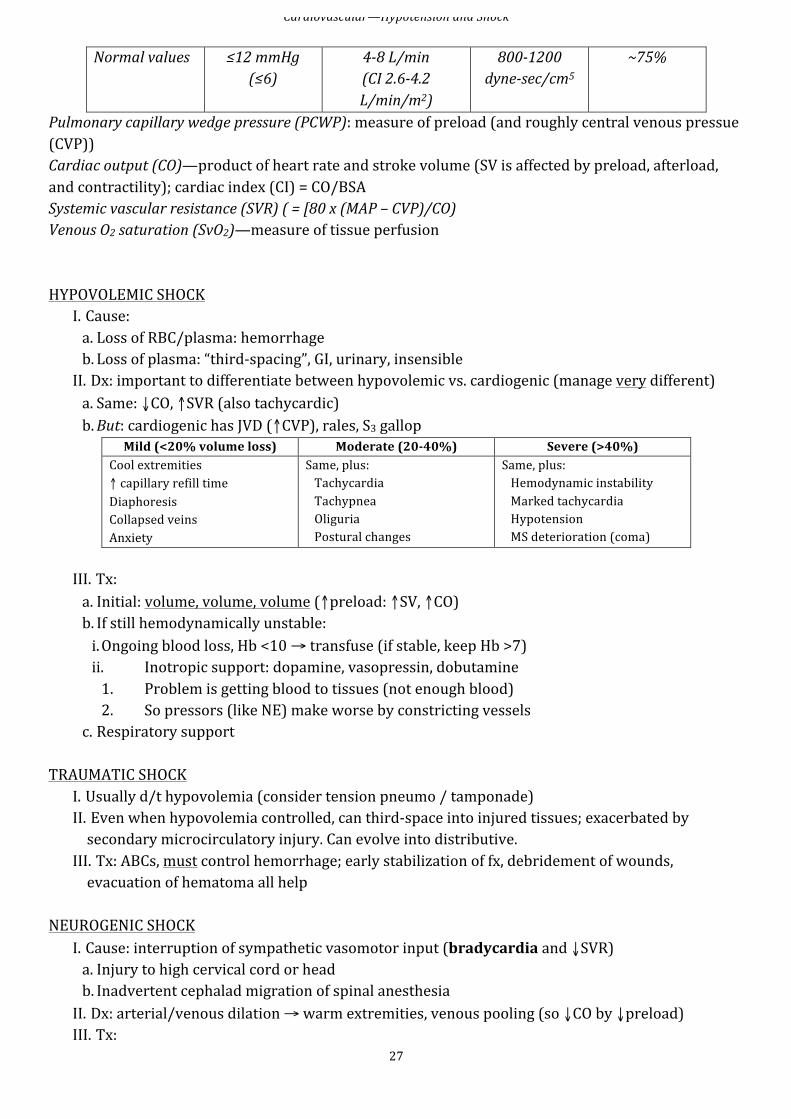
c. You want to give the right amount of IVF to the right pt i. You need to find pts on the ascending limb of the Starling curve, where increasing preload increases SV & CO ii. The “gold standard” is to give a bolus, but can’t always “take that back” (and hence pt may be worse off)
d. Measures of volume responsiveness i. “Static” parameters, like CVP and PCWP aren’t as good as “dynamic” parameters ii. Passive leg raise (PLR) 1. Procedure a. Take baseline measurement of stroke volume, either via echo, Flo-‐Trac,Swan, PiCCO or other means i. Position at baseline: legs flat, head-‐of-‐bed (HOB) elevated to 30-‐45o ii. Should be in that position for minimum 2-‐5 minutes b. Perform PLR i. HOB flat, lift legs to 45o angle with torso (no pt effort: passive), may use wedge pillow, if available
ii. Keep legs raised for minimum 2min iii. Repeat measures of SV 2. +PLR if SV (or CO) ↑15% 3. If +PLR, give IVF, if –PLR, needs pressors for BP 4. Works in ventilated and spontaneously breathing pts (Intensive Care Med 2007; 33: 1111-‐3)
(from: Cardiol Res Pract 2012, PMID: 21918726)
iii. IVC collapsibility (Intensive Care Med 2004; 30:1740-‐6, Intensive Care Med 2004; 30:1834-‐7) 1. Primarily validated for ventilated pts 2. Based on principle that hypovolemic pts are more sensitive to changes in intrathoracic pressure during respiratory cycle
Cardiovascular—Hypotension and Shock
31
3. Measure IVC 2-‐3cm inferior to entrance to RA 4. Predictive of volume responsiveness: a. Collapsibility index: i. Calculate by (max diameter – min)/min ii. Volume responsive: ≥18% b. Alternative calculation i. (max-‐min)/(avg of both) ii. Volume responsive: ≥12%
CARDIOGENIC SHOCK
I. Definition: systemic hypoperfusion caused by severe depression of CI (<2.2 L/min/m2) and sustained arterial hypotension (SBP <90) despite ↑filling pressure (PCWP >18)
II. Cause a. Etiology: Acute MI, PE, CHF, CM, HOCM, Takotsubo, tamponade, etc b. ↓myocardial contractility → ↓CO/BP → ↓perfusion → further ischemia → ↓myocardial contractility → etc.
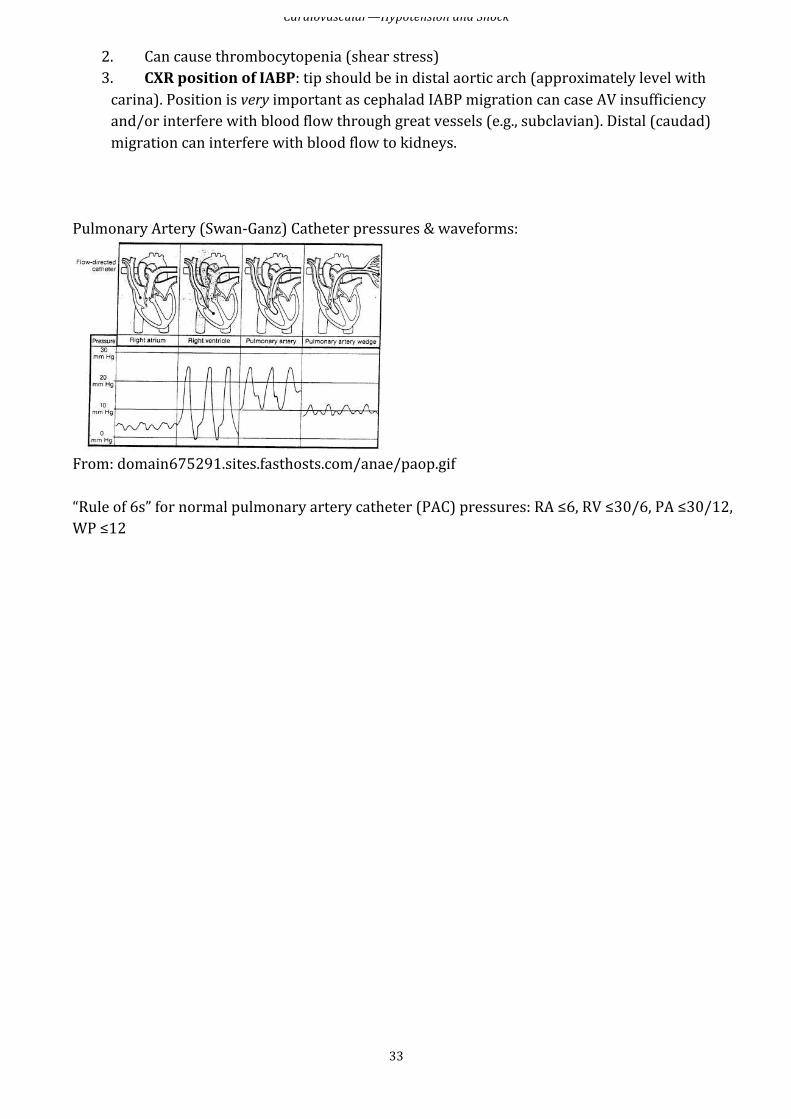
III. Clinical: a. CP, dyspnea, pale, apprehensive, diaphoretic b. Weak, rapid pulse; rales, oliguria c. CXR: pulm vasc congestion +/-‐ pulm edema d. PAC: ↑PCWP, ↓SvO2, if RA = PCWP → tamponade (i.e., equal left and right heart filling pressures) [see diagram below for pulmonary artery catheter pressures]
IV. Tx: a. If d/t acute MI / ischemia → rapid cardiology consultation for PCI, CABG, IABP b. General: maintain adequate perfusion, ↑BP, adjust volume for optimal LV filling pressure c. Vasopressors i. SBP <70: Norepinephrine -‐ ( NEJM 2010:362; pp. 779-‐89 ) ii. SBP 70-‐100 & si/sx shock: Dopamine 1. Low “renal dose”: dilates renal vasculature (questionable) 2. Moderate: +chrono/inotropic 3. High: vasoconstriction iii. SBP 70-‐100, no si/sx shock: Dobutamine 1. Low dose: +ino, minimal +chrono 2. High: +ino, moderate +chrono
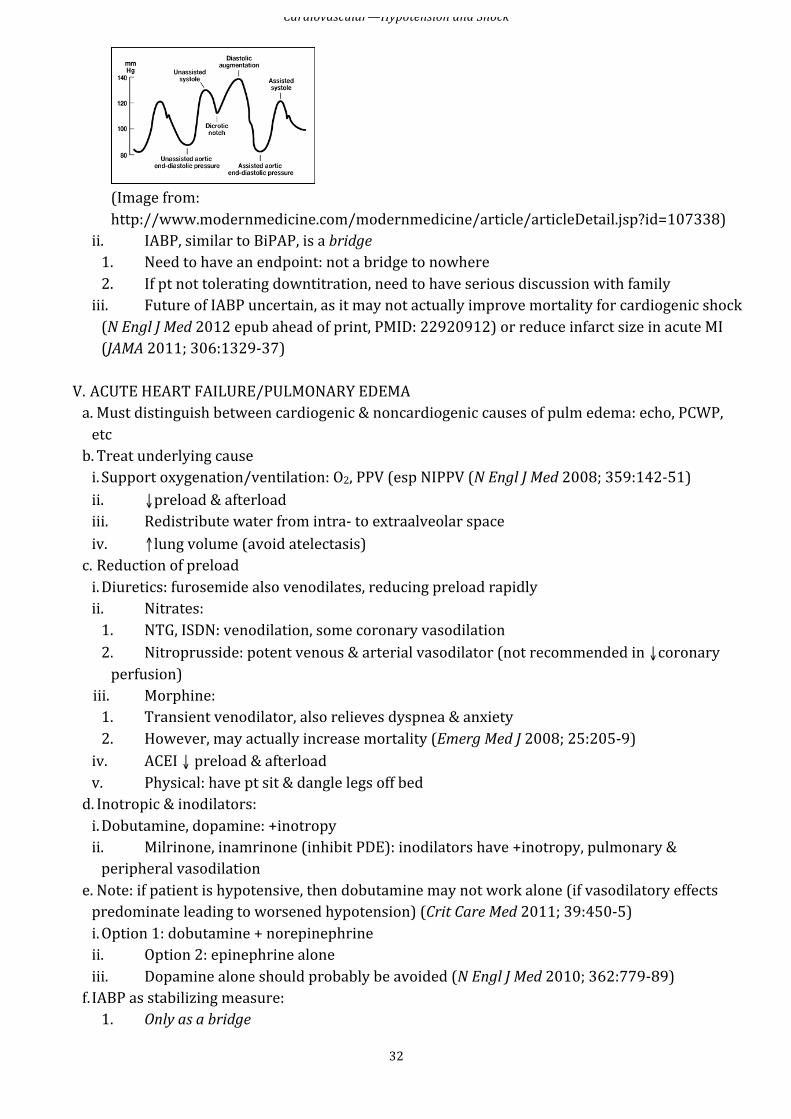
d. May need preload reduction (see below) e. Intraaortic balloon pump (IABP): augments both arterial diastolic pressure & CO (Am J Cardiol 2006; 97: 1391-‐8) i. Mechanism: 1. Collapses in early systole → ↓afterload (vacuum effect) 2. Inflates early diastole → ↑coronary artery flow 3. Recall that MAP = (2xDBP + SBP)/3, so ↑DBP is more than enough to offset the ↓SBP to improve MAP 4. Waveform:
Cardiovascular—Hypotension and Shock
32
(Image from: http://www.modernmedicine.com/modernmedicine/article/articleDetail.jsp?id=107338)
ii. IABP, similar to BiPAP, is a bridge 1. Need to have an endpoint: not a bridge to nowhere 2. If pt not tolerating downtitration, need to have serious discussion with family iii. Future of IABP uncertain, as it may not actually improve mortality for cardiogenic shock (N Engl J Med 2012 epub ahead of print, PMID: 22920912) or reduce infarct size in acute MI (JAMA 2011; 306:1329-‐37)
V. ACUTE HEART FAILURE/PULMONARY EDEMA a. Must distinguish between cardiogenic & noncardiogenic causes of pulm edema: echo, PCWP, etc b. Treat underlying cause i. Support oxygenation/ventilation: O2, PPV (esp NIPPV (N Engl J Med 2008; 359:142-‐51) ii. ↓preload & afterload iii. Redistribute water from intra-‐ to extraalveolar space iv. ↑lung volume (avoid atelectasis) c. Reduction of preload i. Diuretics: furosemide also venodilates, reducing preload rapidly ii. Nitrates: 1. NTG, ISDN: venodilation, some coronary vasodilation 2. Nitroprusside: potent venous & arterial vasodilator (not recommended in ↓coronary perfusion)
iii. Morphine: 1. Transient venodilator, also relieves dyspnea & anxiety 2. However, may actually increase mortality (Emerg Med J 2008; 25:205-‐9) iv. ACEI ↓ preload & afterload v. Physical: have pt sit & dangle legs off bed d. Inotropic & inodilators: i. Dobutamine, dopamine: +inotropy ii. Milrinone, inamrinone (inhibit PDE): inodilators have +inotropy, pulmonary & peripheral vasodilation
e. Note: if patient is hypotensive, then dobutamine may not work alone (if vasodilatory effects predominate leading to worsened hypotension) (Crit Care Med 2011; 39:450-‐5) i. Option 1: dobutamine + norepinephrine ii. Option 2: epinephrine alone iii. Dopamine alone should probably be avoided (N Engl J Med 2010; 362:779-‐89) f. IABP as stabilizing measure: 1. Only as a bridge
Cardiovascular—Hypotension and Shock
33
2. Can cause thrombocytopenia (shear stress) 3. CXR position of IABP: tip should be in distal aortic arch (approximately level with carina). Position is very important as cephalad IABP migration can case AV insufficiency and/or interfere with blood flow through great vessels (e.g., subclavian). Distal (caudad) migration can interfere with blood flow to kidneys.
Pulmonary Artery (Swan-‐Ganz) Catheter pressures & waveforms:
From: domain675291.sites.fasthosts.com/anae/paop.gif “Rule of 6s” for normal pulmonary artery catheter (PAC) pressures: RA ≤6, RV ≤30/6, PA ≤30/12, WP ≤12
Cardiovascular—ACS & Arrhythmias
34
ACUTE CORONARY SYNDROME
If suspect STEMI, call cardiology fellow ST-‐ELEVATION MI (STEMI) (2009 ACCF/AHA guideline update: Circulation 2009; 120:2271-‐2306)
I. Diagnostic Criteria a. ST elevation ≥1mm in 2+ contiguous leads, OR b. (Presumed) new LBBB and history suggestive of acute MI c. Watch out for RV infarct i. If STE in inferior leads (II, III, aVF), get right-‐sided ECG and look for STE in lead V4R ii. RV infarcts very preload-‐dependent—do not give NTG, instead give gentle boluses to maintain BP
II. Intervention a. Early tx can limit infarct size, preserve LV fxn, ↓mortality b. PCI preferable to thrombolysis, esp if thrombolysis contraindicated, pt in cardiogenic shock, or s/p CABG c. Thrombolysis (tPA) used when PCI not available i. Contraindications mainly relate to bleeding ii. ICH in 0.5%
III. Medications a. ASA: 325mg chewable tab b. Clopidogrel: 300mg PO loading dose in anticipation of stent i. Will need 75mg daily thereafter ii. Contraindications: allergy, ↓Plt, high risk for GI bleed c. NTG: i. Start gtt for continued chest pain or pulmonary edema ii. Titrate to pain, watch for hypotension d. β-‐blocker: metoprolol i. PO preferred to IV, less hypotension ii. Target HR = 60 iii. Contraindications: AV block, SBP <100, moderate/severe HF e. ACEI w/in 24h f. Morphine for pain IV. Complications a. Cardiogenic shock, RV/LV falure b. Arrhythmias (VT, VF, AB blocks within 1st 24h) c. Mechanical complications 4-‐7d out (pap musc rupture, free wall rupture, ventricular aneurysm [can see persistent STE])
NON-‐ST-‐ELEVATION MI (NSTEMI) & UNSTABLE ANGINA (UA) (Review: Am J Respir Crit Care Med 2012; 185(9): 924-‐32; 2012 ACCF/AHA guidelines: Circulation 2012; 126:875-‐910)
I. Diagnostic criteria a. NSTEMI: +Tn (→myocardial necrosis) b. UA: neg Tn with classic angina c. Keep in mind this is acute coronary syndrome
Cardiovascular—ACS & Arrhythmias
35
i. Not every +Tn leads down this path ii. Example: +Tn in setting of severe sepsis or septic shock
II. Determine risk a. Critically unstable: persistent severe sx, hemodynamic instability, cardiogenic shock b. High risk: ACS and ≥1 of i. Ongoing ischemic sx despite optimal medical therapy ii. High-‐risk ECG 1. STD >1mm in 2+ contiguous leads 2. Minimal STE (<1mm in 2+ contiguous leads) <20 min in duration 3. Deep TWI in contiguous leads ≥3mm in ≥3 limb leads or ≥4 precordial leads (not counting V1)
iii. ↑Tn iv. TIMI score >2: give 1 point for each
History Presentation -‐ Age >65 -‐ >3 risk factors -‐ Known CAD (stenosis
>50%) -‐ ASA use in past 7d
Severe angina (>2 episodes/24h) STDep >0.5mm +markers
c. General treatment i. Critically unstable/High Risk: urgent cath—call cards! ii. Low risk: conservative medical management, nonurgent cath iii. Timing of cath with UA/NSTEMI often dictated by sx—if chest pain cannot be controlled with meds, call cards to consider earlier coronary angiography regardless of risk factor profile
d. Guideline treatment algorithm i. Give ASA (if ASA-‐intolerant, use clopiogrel as alternative) ii. Select management strategy (cards consult) 1. Conservative or unknown a. Start anticoagulant i. Enoxaparin or UFH ii. Fondaparinux
1. Not generally used at UNMH, especially in MICU 2. Fonda lacks Factor IIa activity, so must be paired with another anticoagulant (e.g., UFH)
iii. UFH generally preferred in MICU, for shorter half-‐life in unstable pts b. Give clopidogrel 2. Invasive a. Start anticoagulant i. Enoxaparin or UFH (again, UFH generally preferred) ii. Bivalirudin b. Before cath: add additional antiplatelet i. Clopidogrel ii. GP IIb/IIIa (e.g., eptifibatide): wary of renal disease c. Additional triage done during angiography i. CABG: cont maintenance ASA ii. PCI
Cardiovascular—ACS & Arrhythmias
36
1. Clopiogrel or prasugrel 2. Possibly GP IIb/IIIa if not already begun
iii. Medical therapy 1. D/c GP IIb/IIIa if begun, cont clopidogrel & ASA
3. Continue with optimal medical therapy per cardiology a. β-‐blocker b. Statin
IF ANY QUESTIONS ABOUT MANAGING NON-‐SURGICAL CARDIOLOGY PATIENTS, DON’T HESITATE TO CALL CARDS!!
ARRHYTHMIAS BRADYCARDIAS, AV BLOCK, AV DISSOCIATION
I. Sinus bradycardia a. Etiology: medications (BB, CCB, amio, Li, dig), ↑vagal tone (includes inferior MI), metabolic (hypoxia, sepsis, myxedema, hypothermia), ↑ICP b. Treatment: usually none, atropine or pacing if symptomatic II. Sick sinus syndrome (SSS) a. Features: unprovoked brady, “tachy-‐brady” syndrome b. Treatment: usually need meds (BB, CCB, etc.) to control tachy and pacer to control brady III. AV block a. 1o: ↑PR b. 2o i. Mobitz I (Wenckebach): ↑ing PR until dropped beat 1. Abnormal AV node: ischemia (inf MI), myocarditis, ↑vagal tone, MV surgery, drugs 2. AVB worsens with carotid massage, improves with atropine 3. No treatment needed ii. Mobitz II: consistent ↑PR with blocked impulse 1. Abnormal His-‐Purkinje system: ischemia (ant MI), infiltrative disease, inflammation, AV surgery, conduction system degeneration 2. AVB improves with carotid massage, worsens with atropine 3. Often progresses to 3o AVB, need pacer
c. 3o: no AV conduction IV. AV Dissociation a. Default: slowing of SA node allows other pacer (e.g., AV node) to take over b. Usurpation: acceleration of other pacer (e.g., junctional rhythm, VT) c. AV block: SA node unable to pace ventricles, other pacer emerges V. Management (Resuscitation 2007; 73:96-‐102, J Emerg Med 2007; 32:105-‐11) a. Treat underlying cause i. In case of drug overdose, may simply need to buy time with pressors/inotropes until drug metabolized ii. See treatment of overdoses in appendix
Cardiovascular—ACS & Arrhythmias
37
b. Pacing i. Think about this for refractory hypotension in the setting of bradycardia ii. Transcutaneous 1. Follow ACLS algorithm 2. Typical HR set is 60-‐70bpm iii. Transvenous 1. This is a fellow-‐level intervention (MICU or cards) 2. Does not appear to be helpful in: a. Asystolic/bradyasystolic cardic arrest b. Traumatic cardiac arrest c. Profound hypothermia or bradydysrhythmias
NARROW-‐COMPLEX TACHYCARDIAS (Postgrad Med J 2009; 85:546-‐51)
I. Regular a. Upright P before QRS i. Sinus tachycardia 1. Cause: pain, fever, hypovolemia, hypoxia, etc. 2. Treatment: treat underlying cause ii. SA Node reentrant tachycardia (RARE, reentrant loop in SA node, rapid start/stop) b. Non-‐sinus P wave(s) before QRS: (ectopic) atrial tachycardia i. See with CAD, COPD, catecholamine surge, EtOH ii. Tx like sinus tach c. No P wave or distorts QRS: AV nodal reentrant tachycardia (AVNRT) i. Cause: reentrant circuit using fast/slow pathways within AVN ii. Tx: vagal maneuvers, CCB/BB, adenosine (caution if AVRT) d. Retrograde P waves after QRS i. AVNRT ii. Atrioventicular reciprocating tachycardia (AVRT) 1. Cause: reentrant circuit using AVN and accessory pathway (e.g., WPW) 2. Tx: BB, amio 3. Avoid AVN blocking agents (e.g., dilt) b/c run risk of starting wide-‐complex tachycardia via accessory pathway
iii. Nonparoxysmal junctional tachycardia (NPJT) 1. Cause: ↑automaticity of AV node, see in myo/endocarditis, surgery, MI, dig 2. Tx: CCB, BB, amio
e. Flutter waves: atrial flutter i. Can be regular or irregular (aflutter with variable block) ii. Flutter waves @300bpm 1. 1:1 conduction = HR 300 2. 2:1 conduction = HR 150 iii. Acute control similar to afib with CCB (e.g., dilt) or BB (e..g, metop)
II. Irregular a. No P waves or fibrillation: atrial fibrillation i. CCB, e.g., dilt 0.25mg/kg IV over 2min, then can start gtt ii. BB, e.g., metop 5-‐15mg IV OR esmolol 500mcg/kg over 1 min, then gtt
Cardiovascular—ACS & Arrhythmias
38
b. ≥3 P wave morphologies before QRS: multifocal atrial tachycardia (MAT) i. Cause: ↑automaticity at several sites in atria ii. Tx: CCB, BB, treat underlying disease
WIDE-‐COMPLEX TACHYCARDIAS (Am J Cardiol 2008; 101:1456-‐66)
I. First decision; whether ventricular or supraventricular origin II. If unstable: ACLS a. Assume all WCT is VT unless proven otherwise! b. If pt presents with spontaneous VT (normal lytes, no drugs, etc.), ALWAYS call cards—VT often precipitated by an ischemic event (ACS, i.e., may need cath)
III. Best predictors that WCT is VT: prior MI, HF, or LV dysfunction IV. Other ECG criteria favoring VT (Circulation 1991; 83:1649) a. AV dissoc (indep P waves, capture or fusion beats) proves VT b. Very wide QRS (>140msec in RBBB-‐type or >160msec in LBBB-‐type) c. Extreme axis deviation d. QRS morphology atypical for BBB e. +Concordance (QRS in all precordial leads with same pattern/direction)
Cardiovascular—HTN Urgency/Emergency and Aortic Dissection
39
HYPERTENSIVE URGENCY AND EMERGENCY
I. Hypertensive emergency is present with evidence of end-‐organ damage Fundoscopic Neurologic Cardiac Renal GI Hemorrhages, exudates, papilledema
h/a, AMS, visual loss, sz, focal deficits
HF, ↑Tn, chest pain
Azotemia/AKI, proteinuria, oliguria
n/v
II. BP usually >200/120 in either case III. Vasodilators listed in APPENDIX: only NTG gtt can be done on SAC IV. Notes: a. Goal should be ↓BP by 20% (NOT normalize) b. Treat underlying cause (need dialysis, pain control, etc.) c. Generally, use IV meds only until BP stable & managed for ~24h, then switch to oral d. Place art line for accurate measurements
AORTIC DISSECTION
I. Classification: a. Proximal: involves ascending aorta (Stanford A, DeBakey I/II) b. Distal: involves descending aorta only (Stanford B, DeBakey III) II. Risk factors: a. HTN b. Connective tissue disease (e.g., Marfan, Ehler-‐Danlos, PCKD, etc.) c. Congential abnormality (e.g., bicuspid AV or coarc) d. Aortitis e. Pregnancy (esp. 3rd trim) f. Trauma (incl IABP) III. Manifestations and Exam (IRAD JAMA 2000;283:897) IV. Diagnosis a. CXR (abnl 60-‐90%, cannot r/o) b. CT: good, but if negative and high suspicion, don’t stop c. TEE (good for proximal) d. MRI/aortography: good but very time-‐consuming V. Treatment a. Proximal: surgical + medical b. Distal: medical i. IV BB first 1. Propranolol, metoprolol, or labetolol 2. Blunt reflex ↑HR/inotropy that comes with vasodilation) ii. Then ↓SBP with vasodilators (e.g., nitroprusside) iii. Consider surgery if progressive, significant arterial branch affected (e.g., renal arteries), uncontrollable HTN or aneurysm
VI. Complications: depend on direction (includes AI) a. Rupture (into pericardium → tamponade; pleural space, mediastinum, retroperitoneal) b. Branch artery obstruction (coronary → MI, carotid → CVA; intestinal → bowel ischemia; renal → AKI)

RENAL—AKI
40
ACUTE KIDNEY INJURY I. General a. Definition: ↑ in Cr ≥0.5 mg/dL above baseline or ↑ Cr ≥20% in ≤2 weeks if baseline >2.5 b. Oliguria: uop 100-‐400 mL/24h; Anuria: uop <100 mL/24h
FENa = (UNa/PNa) / (UCr/PCr) = (UNa x PCr) / (UCr x PNa) if diuretics used FEUN = (UUN/PUN) / (UCr/PCr)
Prerenal Intrinsic Renal Postrenal Causes Underlying: ↓perfusion
-‐ hypovolemia -‐ ↓ cardiac contractility -‐ systemic vasodilation (e.g., sepsis) -‐ renal vasoconstriction: -‐ Rx: NSAIDs, ACEI/ARB -‐ hepatorenal, hyperCa2+ -‐ vascular: -‐ RAS (bilat + ACEI) -‐ thrombosis, embolism, dissection -‐ vasculitis
1) ATN (most common) -‐ ischemia (←prerenal) -‐ toxins: -‐ Rx: AG, ampho, cisplatin -‐ Pigment: Hgb, Mgb -‐ Prot: Ig light chains -‐ CIARF 2) AIN -‐ Allergic: β-‐lactam, sulfa, NSAID -‐ Inf: pyelo -‐ Infil: sarcoid, lymphoma, leukemia 3) Small vessel -‐ cholesterol emboli -‐ thrombotic microangiopathy (HUS/TTP, DIC, pre-‐ecl, malignant HTN, scleroderma renal crisis) 4) Glomerulonephritis
1) Bladder neck -‐ BPH, prostate CA -‐ neurogen bladder -‐ anticholinergics 2) Ureteral -‐ malignancy -‐ LAD -‐ retroperit fibrosis -‐ bilat nephrolith 3) Tubular -‐ ppt crystals
U/A Bland, transparent hyaline casts Muddy brown casts (in 75%, ± in CIARF) ± RBC/protein
Bland ± RBC if nephrolith
FENa FENa < 1% FEurea < 35%
FENa >2% (except pigment & CIARF) FEurea >35%
Normal
Uosm >400 300-‐350 >20 U Na <20 >20 Normal
I. ATN: most common cause of AKI in ICU a. Ischemic: any prolonged prerenal or hypotensive state; vascular obstruction b. Toxic: aminoglyc, amphotericin, rhabdo, hemolysis, Contrast-‐induced c. Sepsis (even without hypotension) II. AIN a. Classic triad: fever, rash, eosinophilia b. Allergic (most common): PCN, cephalosporin, sufla, NSAID, rifampin c. Infection: leptospirosis, hantavirus, strep, CMV, histo, RMSF
RENAL—AKI
41
d. Autoimmune: SLE, Sjogren’s III. ACEI/ARB & NSAIDs a. Normal action: mild hypoperfusion → activate SNS & renin-‐angiotensin-‐aldosterone i. A II → 1) ↑PG synth → afferent glom art vasodil; 2) preferential constriction efferent glom art ii. thus, ↑filtration fraction & maintain GFR b. NSAIDs → block PG synth → afferent vasoconstriction (usually OK, but if hypovol/CKD→tip over to ARF) c. ACEI/ARB → block A II formation/action → cannot use regulatory measures of ↑BP, efferent vasoconstr to maintain GFR
IV. Contrast-‐induced acute renal failure (CIARF) a. Risk Factors: CKD, DM, CHF, age, hypotension, ↑contrast volume b. Prevention: NAC, fluid, hold ACEI/ARB, NSAIDs, diuretics i. NAC: 600mg PO BID day prior to and day of contrast ii. Aggressive hydration if tolerable (3ml/kg/hr NS 1hr before then 1ml/kg/hr x 6h))
V. TREATMENT a. Treat underlying cause b. Avoid renal insults; renal dosing of meds c. Watch for volume overload & electrolyte disturbances d. When to dialyze: (remember, does not replace medical management first) i. Acidemia/acid-‐base disturbances ii. Electrolyte disorders: usually hyperK+, occ hyperCa2+ or tumor lysis syndrome iii. Intoxication: methanol, ethylene glycol, Li, salicylates iv. Overload of volume (CHF) v. Uremia: pericarditis, encephalopathy, bleeding
OLIGURIA/LOW URINE OUTPUT Rarely is Lasix the answer to low urine output in the ICU…think first
I. Normal uop 0.5cc/kg/h II. Do you believe the numbers? a. Flush Foley to make sure not clogged b. If no Foley, check post-‐void residual and daily weights III. Examine pt to assess volume status (make sure CVP >10-‐12 or PCWP >16) IV. Abrupt cessation of uop most often is obstruction; other causes are a. Progression of renal disease b. Renal cortical necrosis c. RPGN V. R/o obstruction by checking PVR VI. Workup as AKI a. If pt not volume overloaded, try fluid challenge (250-‐500cc NS) b. Even if responds, consider hypovolemia, ↓CO, infection/sepsis, CIARF, drug toxicity (most common causes) c. Watch out for volume overload, acidosis, hyperK+ (i.e., reasons for dialysis) VII. If pt has HF or is overloaded, start diuresis; BUT diuresis just to increase uop is pointless—treat pt, not numbers!
RENAL—Electrolytes
42
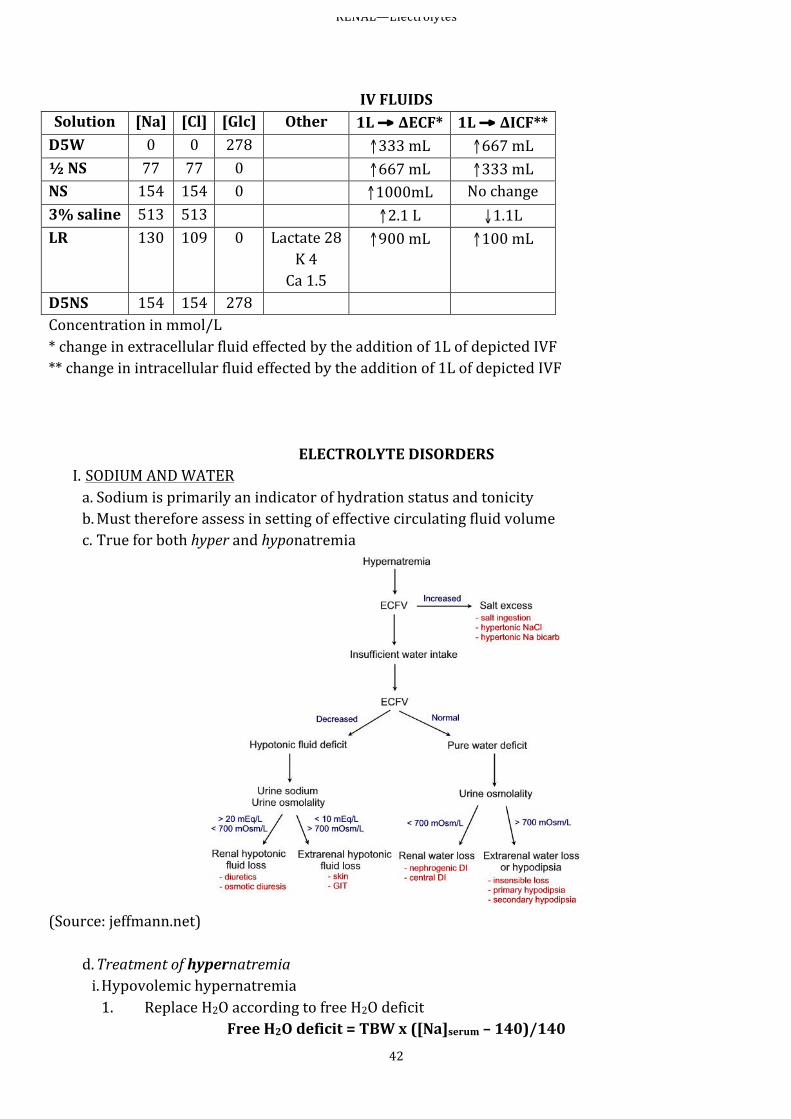
IV FLUIDS Solution [Na] [Cl] [Glc] Other 1L → ΔECF* 1L → ΔICF** D5W 0 0 278 ↑333 mL ↑667 mL ½ NS 77 77 0 ↑667 mL ↑333 mL NS 154 154 0 ↑1000mL No change 3% saline 513 513 ↑2.1 L ↓1.1L LR 130 109 0 Lactate 28
K 4 Ca 1.5
↑900 mL ↑100 mL
D5NS 154 154 278 Concentration in mmol/L * change in extracellular fluid effected by the addition of 1L of depicted IVF ** change in intracellular fluid effected by the addition of 1L of depicted IVF
ELECTROLYTE DISORDERS I. SODIUM AND WATER a. Sodium is primarily an indicator of hydration status and tonicity b. Must therefore assess in setting of effective circulating fluid volume c. True for both hyper and hyponatremia
(Source: jeffmann.net)
d. Treatment of hypernatremia i. Hypovolemic hypernatremia 1. Replace H2O according to free H2O deficit
Free H2O deficit = TBW x ([Na]serum – 140)/140
RENAL—Electrolytes
43
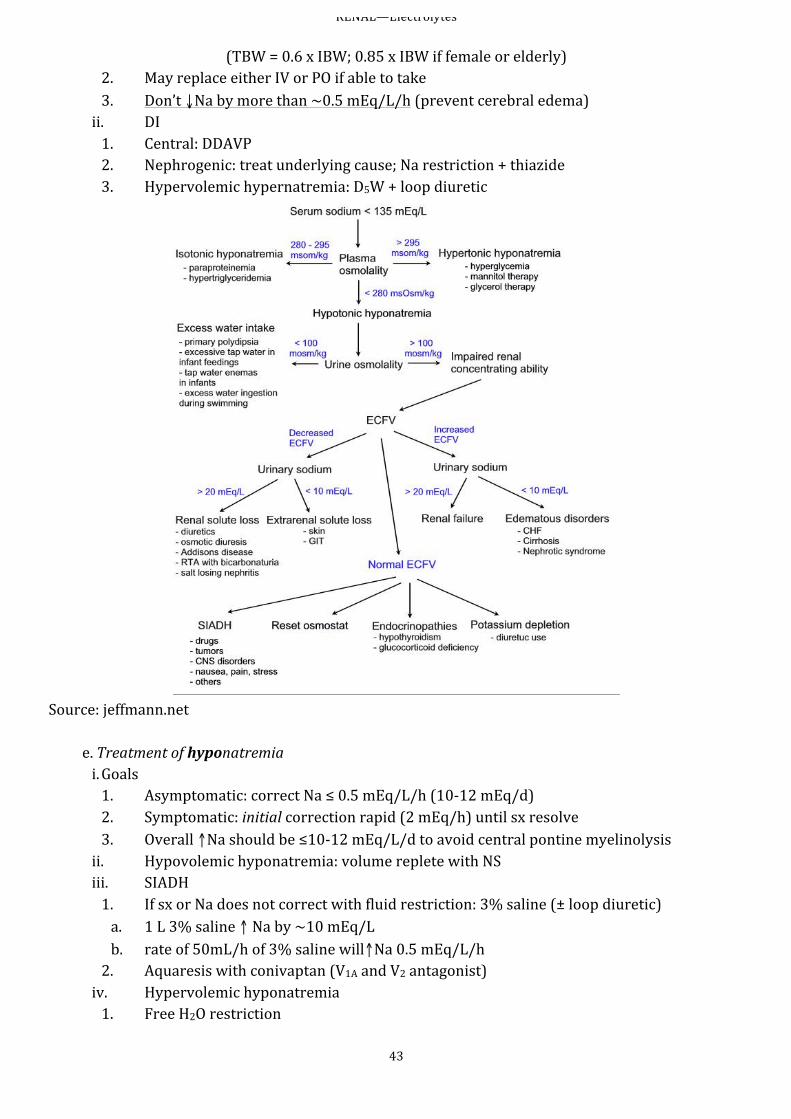
(TBW = 0.6 x IBW; 0.85 x IBW if female or elderly) 2. May replace either IV or PO if able to take 3. Don’t ↓Na by more than ~0.5 mEq/L/h (prevent cerebral edema) ii. DI 1. Central: DDAVP 2. Nephrogenic: treat underlying cause; Na restriction + thiazide 3. Hypervolemic hypernatremia: D5W + loop diuretic
Source: jeffmann.net
e. Treatment of hyponatremia i. Goals 1. Asymptomatic: correct Na ≤ 0.5 mEq/L/h (10-‐12 mEq/d) 2. Symptomatic: initial correction rapid (2 mEq/h) until sx resolve 3. Overall ↑Na should be ≤10-‐12 mEq/L/d to avoid central pontine myelinolysis ii. Hypovolemic hyponatremia: volume replete with NS iii. SIADH 1. If sx or Na does not correct with fluid restriction: 3% saline (± loop diuretic) a. 1 L 3% saline ↑ Na by ~10 mEq/L b. rate of 50mL/h of 3% saline will↑Na 0.5 mEq/L/h 2. Aquaresis with conivaptan (V1A and V2 antagonist) iv. Hypervolemic hyponatremia 1. Free H2O restriction
RENAL—Electrolytes
44
2. ↑effective arterial volume [EAV] (e.g., vasodilators and loop diuretics to ↑CO in HF; give colloids in cirrhosis) 3. ?aquaresis with tolvaptan (V2 antagonist)
II. POTASSIUM a. Hyperkalemia i. Sx: weakness, nausea, paresthesias ii. ECG: peaked T → ↑PR → ↑ QRS → sine wave → PEA iii. R/o transcellular shifts (acidemia, ↓insulin, BB, etc.) & ↓GFR iv. Transtubular potassium gradient (TTKG) differentiates renal from nonrenal causes if normal GFR 1. TTKG = (UK/PK)/(Uosm/Posm) 2. TTKG > 7 → nl aldosterone a. ↓EAV b. HF, cirrhosis, excessive K intake 3. TTKG < 7 → hypoaldosteronism a. Same etiologies as Type IV RTA b. ↓renin: diabetic nephro, NSAID, chronic interstitial nephritis, HIV c. nl renin, ↓aldo synth: 1o adrenal d/o, ACEI/ARB, heparin d. ↓response to aldo: i. Meds: K-‐sparing diurectics, TMP-‐SMX, pentamadine, calcineurin inhib ii. Tubulointerstitial dz: sickle cell, SLE, amyloid, DM
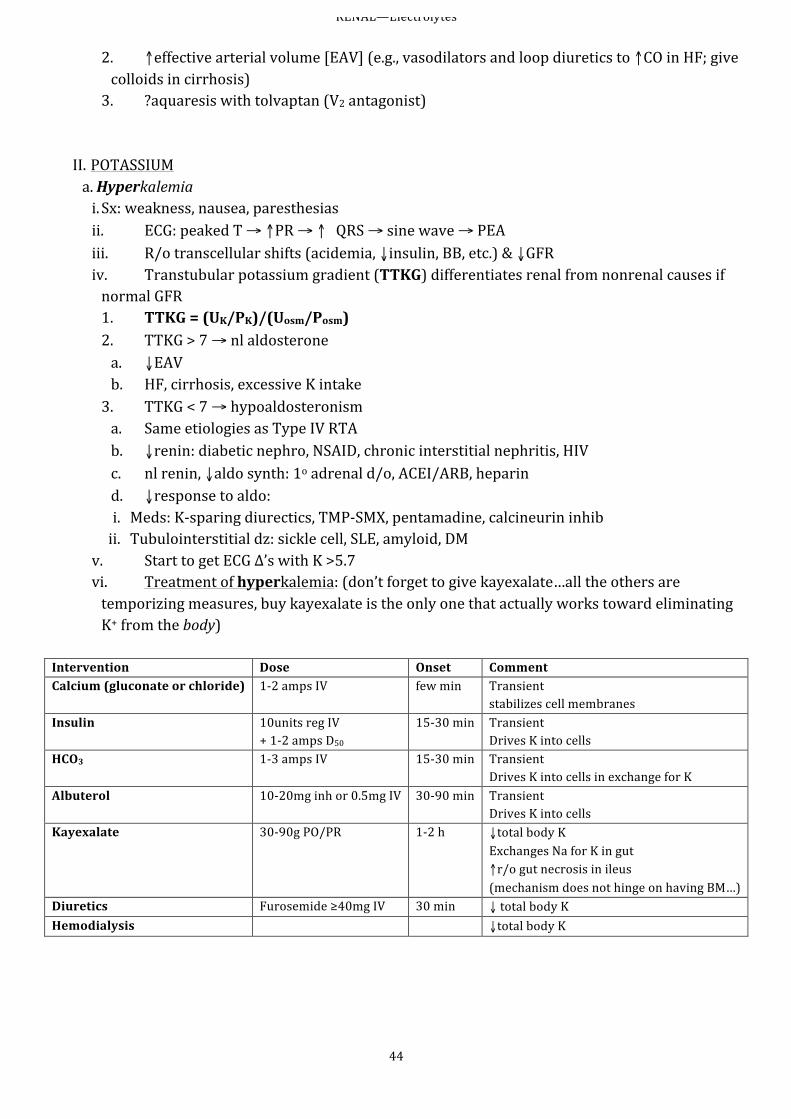
v. Start to get ECG Δ’s with K >5.7 vi. Treatment of hyperkalemia: (don’t forget to give kayexalate…all the others are temporizing measures, buy kayexalate is the only one that actually works toward eliminating K+ from the body)
Intervention Dose Onset Comment Calcium (gluconate or chloride) 1-‐2 amps IV few min Transient
stabilizes cell membranes Insulin 10units reg IV
+ 1-‐2 amps D50 15-‐30 min Transient
Drives K into cells HCO3 1-‐3 amps IV 15-‐30 min Transient
Drives K into cells in exchange for K Albuterol 10-‐20mg inh or 0.5mg IV 30-‐90 min Transient
Drives K into cells Kayexalate 30-‐90g PO/PR 1-‐2 h ↓total body K
Exchanges Na for K in gut ↑r/o gut necrosis in ileus (mechanism does not hinge on having BM…)
Diuretics Furosemide ≥40mg IV 30 min ↓ total body K Hemodialysis ↓total body K
RENAL—Electrolytes
45
b. Hypokalemia i. Sx: n/v, weakness, muscle cramps ii. ECG: U waves, ± ↑QT → ventricular ectopy (PVC, VT, VF) iii. R/o transcellular shifts (alkalemia, insulin, catecholamines, etc.) iv. Renal vs GI losses 1. Renal: 24o UK > 30 mEq, TTKG >7 a. Hypo-‐/normal BP i. Acidosis: DKA, RTA ii. Alkalosis: diuretics, vomiting/NGT drain (2o/t hyperaldo), Bartter’s, Gitelman’s iii. ↓Mg b. HTN: mineralocorticoid excess i. 1o/2o hyperaldo (Conn’s, renovascular dz, renin-‐secreting tumor) ii. Nonaldosterone mineralocorticoid (Cushing’s, Liddle’s, exogenous) 2. GI: 24o UK < 25 mEq, TTKG <3 a. GI loss + metabolic acidosis: diarrhea, laxatives, villous adenoma b. Vomiting/NGT drainage usually lead to renal loss of K
v. Treatment 1. Treat underlying cause 2. 1 mEq/L ↓ in K means ~ 200 mEq total body loss 3. 10 mEq K repletion should ↑Kserum by ~0.1 mEq/L, unless K< 3.0, in which case must recheck after giving and continue to replete 4. Repletion not effective if ↓Mg 5. Remember: normal is normal! a. Goal K+: 3.5-‐4.5 (JAMA 2012; 307:157-‐64) i. Like nearly all K+ studies, done in acute MI pts ii. Found U-‐shaped mortality curve according to K+, with nadir in 3.5-‐4.5 range b. Repleting to ≥4 doesn’t help outcomes c. If concerned, can always recheck later
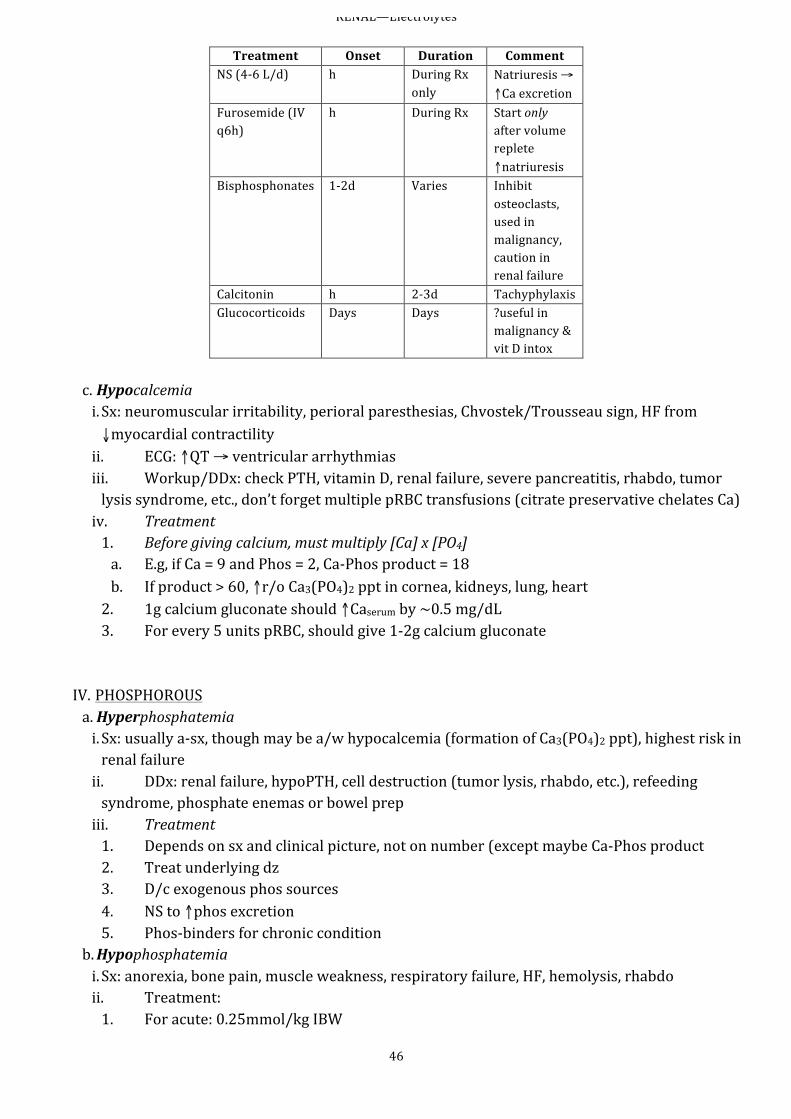
III. CALCIUM a. Must correct calcium according to albumin i. Corrected Ca = Ca (mg/dL) + [0.8 x (4 – albumin (g/dL)] ii. Or can measure ionized (free) Ca directly iii. Note: alkalosis cause albumin to bind more Ca (so total wnl, but iCa↓) b. Hypercalcemia i. Sx: 1. Hypercalcemic crisis (Ca usu 13-‐15): polyuria, dehydration, AMS 2. Renal stones, nephrogenic DI, abd pain, anorexia, n/v/constip, pancreatitis 3. Calciphylaxis a/w uremia: poor prognosis overall ii. ECG: ↓QT, pts on dig more prone to arrhythmias iii. Main causes: hyperparathyroidism or malignancy (combined 90% etiology) 1. Hyper-‐PTH: more likely if a-‐sx or chronic 2. Malignancy: more likely if acute or sx iv. Acute Treatment
RENAL—Electrolytes
46
Treatment Onset Duration Comment NS (4-‐6 L/d) h During Rx
only Natriuresis → ↑Ca excretion
Furosemide (IV q6h)
h During Rx Start only after volume replete ↑natriuresis
Bisphosphonates 1-‐2d Varies Inhibit osteoclasts, used in malignancy, caution in renal failure
Calcitonin h 2-‐3d Tachyphylaxis Glucocorticoids Days Days ?useful in
malignancy & vit D intox
c. Hypocalcemia i. Sx: neuromuscular irritability, perioral paresthesias, Chvostek/Trousseau sign, HF from ↓myocardial contractility ii. ECG: ↑QT → ventricular arrhythmias iii. Workup/DDx: check PTH, vitamin D, renal failure, severe pancreatitis, rhabdo, tumor lysis syndrome, etc., don’t forget multiple pRBC transfusions (citrate preservative chelates Ca) iv. Treatment 1. Before giving calcium, must multiply [Ca] x [PO4] a. E.g, if Ca = 9 and Phos = 2, Ca-‐Phos product = 18 b. If product > 60, ↑r/o Ca3(PO4)2 ppt in cornea, kidneys, lung, heart 2. 1g calcium gluconate should ↑Caserum by ~0.5 mg/dL 3. For every 5 units pRBC, should give 1-‐2g calcium gluconate
IV. PHOSPHOROUS a. Hyperphosphatemia i. Sx: usually a-‐sx, though may be a/w hypocalcemia (formation of Ca3(PO4)2 ppt), highest risk in renal failure ii. DDx: renal failure, hypoPTH, cell destruction (tumor lysis, rhabdo, etc.), refeeding syndrome, phosphate enemas or bowel prep iii. Treatment 1. Depends on sx and clinical picture, not on number (except maybe Ca-‐Phos product 2. Treat underlying dz 3. D/c exogenous phos sources 4. NS to ↑phos excretion 5. Phos-‐binders for chronic condition
b. Hypophosphatemia i. Sx: anorexia, bone pain, muscle weakness, respiratory failure, HF, hemolysis, rhabdo ii. Treatment: 1. For acute: 0.25mmol/kg IBW
RENAL—Electrolytes
47
2. For chronic: 0.5mmol/kg IBW 3. 0.25mmol/kg should ↑Phosserum by ~1.2 mg/dL 4. IV repletion options: a. KPhos: 6mmol/100mL over 4h b. NaPhos: 10mmol/100mL over 4h
V. MAGNESIUM (Rev Endocr Metab Disord 2003; 4:195-‐206) a. Hypermagnesemia i. Sx 1. Neuromuscular: loss of DTR, paralysis, apnea, ileus, urinary retention 2. Cardiac: bradycardia, hypotension, ↑PR, ↑QRS ↑QTc, Vfib ii. Causes (in brief) 1. Decreased renal excretion (GFR <30) 2. ↑intake iii. Treatment (if severe/symptomatic) 1. 100-‐200mg elementral calcium 2. Loop diuretics/saline (↑renal excretion) 3. HD (rarely needed)
b. Hypomagnesemia (J Am Soc Nephrol 1999; 10:1616-‐22) i. Sx: 1. Hypokalemia (occurs in 40-‐60% of hypoMg) 2. Hypocalcemia 3. Cardiac: a. QRS widening b. Peaked T c. PR prolongation d. Ventricular arrhythmias (esp in acute MI) 4. Very low levels (<1.2mg/dL) can cause tetany & seizures ii. Causes (in brief) 1. GI loss 2. Renal loss (loop & thiazide diuretics, hyperCa, primary renal wasting) iii. Treatment 1. IV: a. If hypoMg/hypoK arrhythmias: give 50mEq Mg slowly over 8-‐24h b. IV is generally used in most MICU pts (1-‐2g MagSulfate doses) 2. PO if asymptomatic
RENAL—Acid-‐base
48
ACID-‐BASE DISORDERS
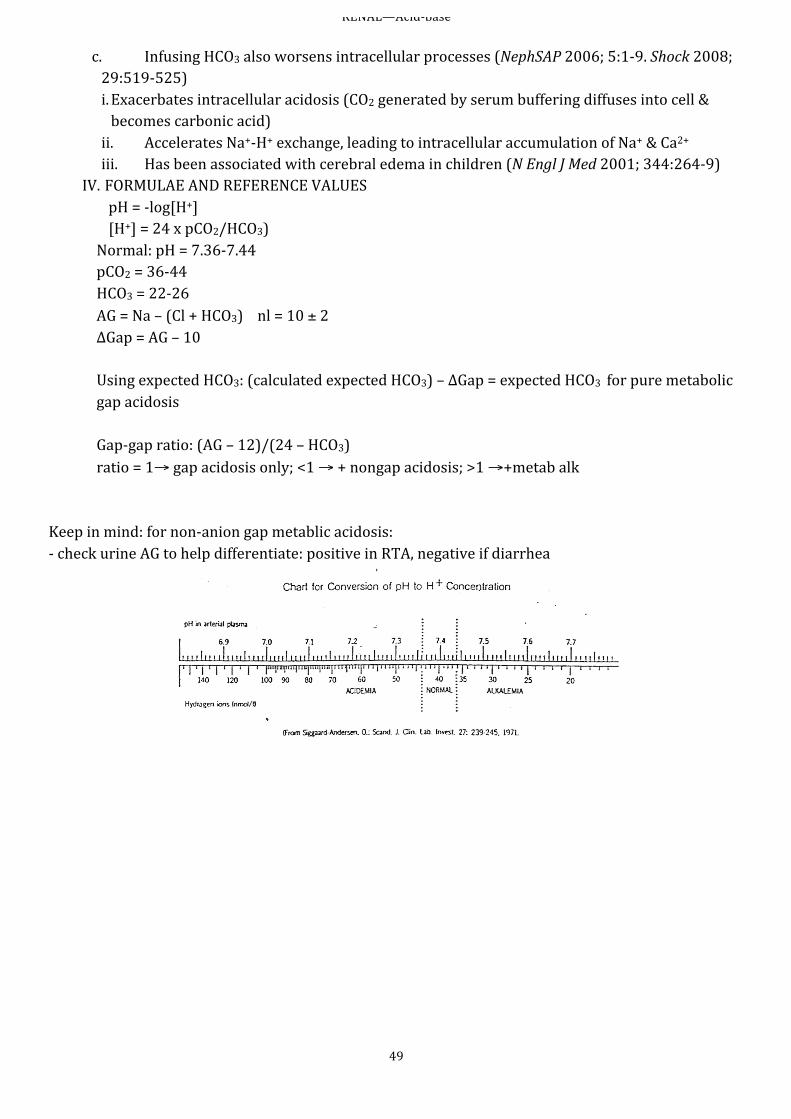
I. SUGGESTIONS ON HOW TO APPROACH a. “Do the numbers make sense?” i. HCO3 from ABG is a calculated value from the pH & pCO2 (from Henderson-‐Hasselbach : [H+] = 24 x (pCO2/HCO3)), so you need to use the HCO3 from BMP as it is independent ii. Convert pH to [H+] using: 10-‐pH = [H+], or you could use the a scale iii. Then calculate [H+] independently using [H+] = 24 x (pCO2/HCO3), making sure to use HCO3 from BMP iv. If H+ = H+ (approximately) using both methods, then proceed v. If H+≠ H+ then stop and redraw ABG and BMP b. Is there an acidemia or alkalemia? i. Just based on pH alone ii. If pH is wnl, then go to pCO2 (K+ could be hint, as ↑K+ in acidemias (opposite in alkalemia) d/t transcellular shift)
c. Determine the 1o disturbance. i. Use the rules above for pH and pCO2 ii. There might not be a primary disturbance if two equal things d. Determine whether the compensation is appropriate. i. Recall metabolic disturbances compensated by lungs in minutes ii. Respiratory disturbances compensated by kidneys in hours (acute) to days (fully) iii. If inappropriately compensated, what is 2o problem? iv. If metabolic acidosis involved, on to next step e. What is the anion gap? Check to see if metabolic gap acidosis (hidden or not) f. Calculate the Δgap & determine if HCO3 is appropriate. (for metabolic gap acidosis only) II. THE VENT AS YOUR FRIEND a. Remember, with the vent you can effectively control pCO2 b. So… i. If pt is acidotic, you can ↑MVE (by ↑either RR or VT) to blow off more CO2 1. This would cause a respiratory alkalosis 2. Raising pH ii. If alkalotic, ↓MVE 1. This is more important 2. Alkalemia can cause great harm, though acidemia is tolerated fairly well
c. Keep in mind that if the primary problem is respiratory acidosis or alkalosis, you effectively solve it with controlling the vent
III. A Note on Bicarbonate Use (Nat Rev Nephrol 2010; 6: 274-‐285) a. Sometimes in the setting of acute severe metabolic acidosis (pH <7.15), HCO3 gtt is suggested b. Most of the studies have been in lactic acidosis and ketoacidosis (the most common causes of metabolic acidosis in ICU) i. No reduction in morbidity or mortality (NephSAP 2006; 5:1-‐9. Am J Kidney Dis 2001; 38:703-‐27; Chest 2000; 117:260-‐7) ii. No improvement in hemodynamics (Ann Intern Med 1990; 112:492-‐8. Crit Care Med 1991; 19:1352-‐6)
RENAL—Acid-‐base
49
c. Infusing HCO3 also worsens intracellular processes (NephSAP 2006; 5:1-‐9. Shock 2008; 29:519-‐525) i. Exacerbates intracellular acidosis (CO2 generated by serum buffering diffuses into cell & becomes carbonic acid) ii. Accelerates Na+-‐H+ exchange, leading to intracellular accumulation of Na+ & Ca2+ iii. Has been associated with cerebral edema in children (N Engl J Med 2001; 344:264-‐9)
IV. FORMULAE AND REFERENCE VALUES pH = -‐log[H+] [H+] = 24 x pCO2/HCO3)
Normal: pH = 7.36-‐7.44 pCO2 = 36-‐44 HCO3 = 22-‐26 AG = Na – (Cl + HCO3) nl = 10 ± 2 ΔGap = AG – 10 Using expected HCO3: (calculated expected HCO3) – ΔGap = expected HCO3 for pure metabolic gap acidosis Gap-‐gap ratio: (AG – 12)/(24 – HCO3) ratio = 1→ gap acidosis only; <1 → + nongap acidosis; >1 →+metab alk
Keep in mind: for non-‐anion gap metablic acidosis: -‐ check urine AG to help differentiate: positive in RTA, negative if diarrhea
RENAL—Acid-‐base
50
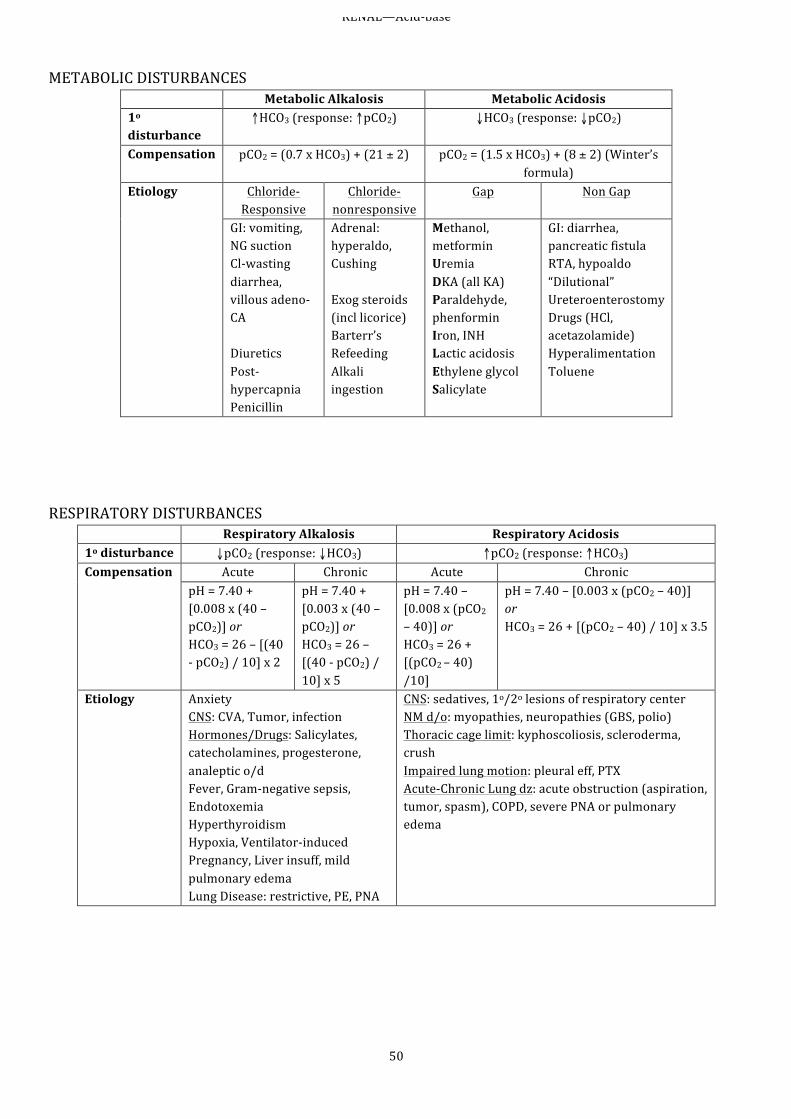
METABOLIC DISTURBANCES
Metabolic Alkalosis Metabolic Acidosis 1o disturbance
↑HCO3 (response: ↑pCO2) ↓HCO3 (response: ↓pCO2)
Compensation pCO2 = (0.7 x HCO3) + (21 ± 2)
pCO2 = (1.5 x HCO3) + (8 ± 2) (Winter’s formula)
Etiology Chloride-‐Responsive
Chloride-‐nonresponsive
Gap Non Gap
GI: vomiting, NG suction Cl-‐wasting diarrhea, villous adeno-‐CA Diuretics Post-‐hypercapnia Penicillin
Adrenal: hyperaldo, Cushing Exog steroids (incl licorice) Barterr’s Refeeding Alkali ingestion
Methanol, metformin Uremia DKA (all KA) Paraldehyde, phenformin Iron, INH Lactic acidosis Ethylene glycol Salicylate
GI: diarrhea, pancreatic fistula RTA, hypoaldo “Dilutional” Ureteroenterostomy Drugs (HCl, acetazolamide) Hyperalimentation Toluene
RESPIRATORY DISTURBANCES
Respiratory Alkalosis Respiratory Acidosis 1o disturbance ↓pCO2 (response: ↓HCO3) ↑pCO2 (response: ↑HCO3) Compensation Acute Chronic Acute Chronic
pH = 7.40 + [0.008 x (40 – pCO2)] or HCO3 = 26 – [(40 -‐ pCO2) / 10] x 2
pH = 7.40 + [0.003 x (40 – pCO2)] or HCO3 = 26 – [(40 -‐ pCO2) / 10] x 5
pH = 7.40 – [0.008 x (pCO2 – 40)] or HCO3 = 26 + [(pCO2 – 40) /10]
pH = 7.40 – [0.003 x (pCO2 – 40)] or HCO3 = 26 + [(pCO2 – 40) / 10] x 3.5
Etiology Anxiety CNS: CVA, Tumor, infection Hormones/Drugs: Salicylates, catecholamines, progesterone, analeptic o/d Fever, Gram-‐negative sepsis, Endotoxemia Hyperthyroidism Hypoxia, Ventilator-‐induced Pregnancy, Liver insuff, mild pulmonary edema Lung Disease: restrictive, PE, PNA
CNS: sedatives, 1o/2o lesions of respiratory center NM d/o: myopathies, neuropathies (GBS, polio) Thoracic cage limit: kyphoscoliosis, scleroderma, crush Impaired lung motion: pleural eff, PTX Acute-‐Chronic Lung dz: acute obstruction (aspiration, tumor, spasm), COPD, severe PNA or pulmonary edema
GI and Metabolism—GI Bleed
51
UPPER GI BLEED I. GENERAL a. Etiologies i. PUD (50%): H. pylori, NSAIDs, etc ii. Varices (10-‐30%): esophageal ± gastric; present in 40-‐60% of cirrhotics iii. Mallory-‐Weiss (10%) iv. Gastritis/gastropathy (15%): NSAIDs, ASA, EtOH, etc. v. Esophagitis (10%): GERD/Barrett’s, XRT (CMV, HSV, Candida if compromised). vi. Vascular malformation (5%) b. Manifestations: n/v, hematemesis, coffee-‐ground emesis, etc. +NG lavage, melena (not all “dark” stool = melena: do a rectal and see what’s in there! (GI will ask))
II. GENERAL MANAGEMENT a. Call GI ASAP to make them aware and get recommendations, while doing the following… b. Transfuse to goal Hgb 7mg/dL (N Engl J Med; 2013:11-‐21) i. Higher transfusion goals (e.g., 10mg/dL) increases mortality and risk of rebleeding ii. If Hgb >10, puts ↑pressure in portal system (esp if variceal bleed) (Hepatology 2007; 46(3): 922-‐38) (J Hepatol 2010; 53:762-‐8) iii. If transfuse ≥ 5 pRBC, give calcium (if anticipate, used massive transfusion order set) iv. Remember, Hct may be wnl early on before equilibration v. How much blood was lost? (1 Hgb/3Hct = 1 unit blood → ~300-‐500cc) 1. If tachy → 10% volume loss 2. Orthostatic hypotension → 20% 3. Shock → 30% a. Remember, pts don’t die of anemia b. They die of hypovolemic shock
c. Correct coagulopathy d. If not sure whether variceal… (World J Gastroenterol 2009; 15(9):1099-‐1104) i. Variceal likely: 1. Previous dx of cirrhosis (not just “drinks a lot”) 2. Signs of cirrhosis: spider angiomata, palmar erythema, gynecomastia, testricular atrophy, parotid gland enlargement, ascites, splenomegaly
ii. If none of the above, NPV 96% for not having variceal bleed iii. Upon initial presentation, all pts should have PPI until talk to GI e. If actively bleeding a lot… i. Consider giving erythromycin 250mg IV x1 30-‐60 min prior to EGD as motility agent to get blood out ii. May need prophylactic intubation prior to EGD for airway protection, esp if withdrawing or hepatic encephalopathy
III. VARICEAL BLEEDING (N Engl J Med 2010; 362:823) a. Risk of bleeding i. If varices & Child B/C: 1y rate of variceal bleed is 12% ii. 1y rate of recurrent bleeding 60% b. Treatments i. Octreotide 50 mcg IV push → 50 mcg/h gtt, for 72h ii. Abx (ceftriaxone or ciprofloxacin) for SBP prophylaxis iii. EGD with either band ligation or sclerotherapy
GI and Metabolism—GI Bleed
52
iv. If EGD fails with severe bleed, may insert Blakemore tube as temporary measure (fellow-‐level procedure) v. If above fails, will need TIPS or other portal decompression therapy
IV. PEPTIC ULCER a. Most common cause of UGIB b. Treatment i. Pantoprazole 80mg IV push → 8 mg/h (↓r/o rebleeding) ii. EGD with sclerotherapy /clipping / BiCAP c. Will likely switch to PO PPI after EGD if no intervention (if intervention then 72h of PPI IV) V. OTHER CAUSES a. Mallory-‐Weiss: usually stops spontaneously, EGD if active b. Esophagitis/gastritis: PPI or H2B
LOWER GI BLEED I. ETIOLOGIES a. Diverticular (33%, though 60% of diverticular bleeding in right colon) b. Angiodysplasia (8%, commonly cecum/ascending colon) c. Neoplasm (19%, usually occult bleeding) d. Colitis (18%): infection, ischemic, radiation, IBD [UC] e. Anorectal (4%): hemorrhoids, anal fissues II. MANIFESTATIONS: diarrhea, tenesmus, BRBPR or maroon stools (BRBPR can also represent
rapid UGI bleeding) III. LOCALIZATION:
If unclear if upper orlower, or to localizae the hemicolon bleeding is coming from (i.e. pre-‐op) tagged RBC scan may be helpful (will only detect if bleeding rate > 0.1-‐0.4 ml/min).
IV. TREATMENT a. Diverticular i. 75% stop spontaneously ii. Endoscopy (with sclerotherapy, etc.), arterial vasopressin/embolization, surgery b. Angiodysplasia i. 85% stop spontaneously ii. Endoscopy, arterial vasopression/embolization, surgery iii. Estrogen or Amicar in select cases
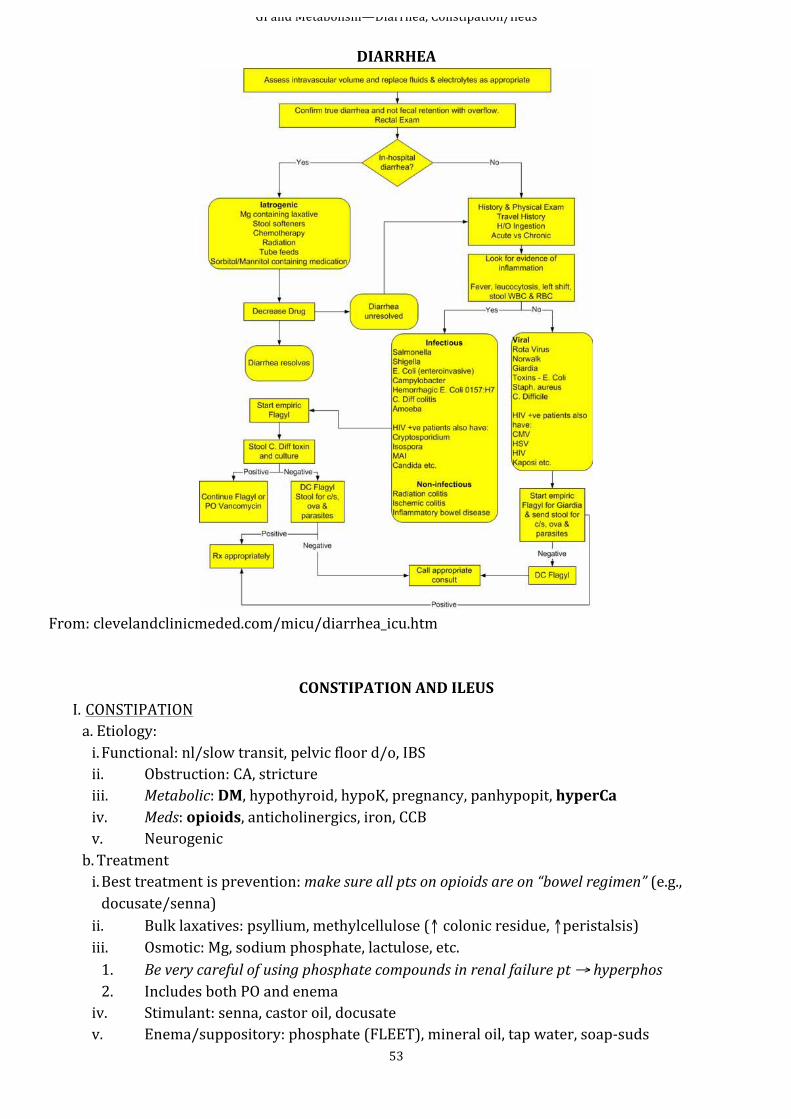
GI and Metabolism—Diarrhea, Constipation/Ileus
53
DIARRHEA
From: clevelandclinicmeded.com/micu/diarrhea_icu.htm
CONSTIPATION AND ILEUS I. CONSTIPATION a. Etiology: i. Functional: nl/slow transit, pelvic floor d/o, IBS ii. Obstruction: CA, stricture iii. Metabolic: DM, hypothyroid, hypoK, pregnancy, panhypopit, hyperCa iv. Meds: opioids, anticholinergics, iron, CCB v. Neurogenic b. Treatment i. Best treatment is prevention: make sure all pts on opioids are on “bowel regimen” (e.g., docusate/senna) ii. Bulk laxatives: psyllium, methylcellulose (↑ colonic residue, ↑peristalsis) iii. Osmotic: Mg, sodium phosphate, lactulose, etc. 1. Be very careful of using phosphate compounds in renal failure pt → hyperphos 2. Includes both PO and enema iv. Stimulant: senna, castor oil, docusate v. Enema/suppository: phosphate (FLEET), mineral oil, tap water, soap-‐suds
GI and Metabolism—Diarrhea, Constipation/Ileus
54
II. ADYNAMIC ILEUS (small bowel) a. Etiologies i. Intra-‐abd process (surgery, pancreatitis, peritonitis) ii. Severe illness (sepsis, PNA) iii. Ischemia iv. Meds (opioids) v. Electrolyte abnl b. Manifestations: abd pain, abdominal distention, decreased BS, n/v, hiccups (can see on vent). Can have gasless abdomen on KUB or air fluid levels. R/O obstruction as cause (obstruction requires surgery eval.) c. Treatment i. Treat underlying cause, ↓/avoid opioids (switch to NSAIDs for pain if possible, esp post-‐op) ii. NPO, NGT (suction or not) to decompress iii. Prokinetic agents: erythromycin or metoclopramide of questionable value
III. OGILVIE’S SYNDROME (colonic pseudo obstruction) a. Etiologies i. Electrolyte abnormalities ii. Severe illness (CHF, shock) iii. Hypothyroidism iv. Meds (opioids, anticholinergics) v. b. Manifestations: abdominal distention, decreased BS, Dilated colon on KUB. R/O obstruction as cause with gastrograffin enema or CT as req (obstruction requires surgery eval.) c. Treatment i. Treat underlying cause, ↓/avoid opioids (switch to NSAIDs for pain if possible, esp post-‐op) ii. Mobilize patient, ideally to a prone on bed iii. NPO, NGT (suction or not) to decompress iv. Prokinetic agents: neostigmine (requires monitoring) v. N-‐methyl naltrexone if opiod induced vi. Gastrograffin enema may be therapeutic (under fluro) vii. Colonoscopy with suction as a last resort
GI and Metabolism—LFTs, Acute Liver Failure, SBP
55
PANCREATITIS
I. ETIOLOGIES a. Alcohol (30%, esp men) b. Gallstones (35%, esp women) c. Many other relatively minor causes (hyper triglycerides, hypercalcemia, viruses) II. WORKUP a. Lab i. ↑amylase >3x ULN suggestive, but dx not based on lab value (i.e., if no abd pain, not pancreatitis) ii. lipase may be more specific b. Imaging i. U/S to look for gallstones, CBD dilation, ascites, pseudocyst ii. CT not required unless using to r/o other dx
III. TREATMENT a. Fluid resuscitation with crystalloid, consider albumin if serum level < 3, NPO initially, but start enteral ASAP (feed when hungry, until then consider NJ tube, TPN only if needed when very prolonged time without nutrition) b. Pain control extremely important c. Follow intrabdominal pressures d. Surgical consultation if patient not improving / sepsis IV. COMPLICATIONS a. Systemic: shock, ARDS, renal failure, GI bleed, DIC b. Metabolic: hypoCa, hyperGlc, hyperTG c. Acute fluid collection (30-‐50% of pts): early, no capsule, no treatment needed d. Pseudocyst (10-‐20%): encapsulated e. Sterile pancreatic necrosis f. Infection i. Infected pancreatic necrosis → must have surgical debridement (100% mortality if not debrided) ii. Pancreatic abscess: abx, CT-‐guided drainage
V. PROGNOSIS Ranson’s criteria Prognosis: At Diagnosis At 48 hours Age >55 Hct ↓ >10% WBC >16k BUN ↑ >5 Glc >200 Base deficit >4 AST >250 Ca <8 LDH >350 PaO2 <60 Fluid seques >6L
#Criteria Mortality ≤2 <5 % 3-‐4 15-‐20% 5-‐6 40% ≥7 >99%
GI and Metabolism—LFTs, Acute Liver Failure, SBP
56
Liver Function Tests
I. AST/ALT—indicative of hepatocellular injury a. Etiologies: viral, AIH, drugs/toxins, NAFLD, vascular, systemic (HHC, A1AT, Wilson’s, celiac sprue) b. Sensitive i. AST: liver, heat, muscle, kidneys, brain, pancreas, lungs, WBC, RBC ii. ALT: liver c. Poor correlation between degree of damage & elevation i. Up to 300 nonspecific (most common fatty liver disease) d. Patterns: i. AST/ALT >2:1 suggests EtOH; >3:1 strongly suggests EtOH ii. >1000 = viral, toxin, ischemic (shock or portal vein thrombosis), gallstones
II. Alk phos/T bili—obstruction a. Etiologies: hepatitis, cirrhosis, meds (sex hormones, EPO), sepsis, PBC, PSC, etc b. Alk phos in /near bile canicular membrane i. Sources: liver, bone, placenta, small intestine ii. “Red herrings” (nonliver): >60yo, blood type O & B, post meal, pregnancy, bone dz c. T bili i. Indirect (red herrings): hemolysis, Crigler-‐Najjar, Gilbert’s ii. Direct implies liver or biliary tract dz (rate-‐limiting step is transport into canaliculi)
III. Protein/albumin—cirrhosis/hepatic insufficiency a. Albumin made only by liver i. Usually albumin ~ ½ protein ii. If larger, e.g., (protein – albumin) ≥ 4, consider MM b. Long half-‐life (18-‐20d) i. Only minimal change in acute disease (if albumin < 3, think of chronic liver disease) ii. Red herrings of low albumin: protein malnutrition, nephrotic syndrome, protein-‐losing enteropathies
IV. Coagulation factors a. All except VIII made by liver b. Short half-‐life: 6h (VII) to 5d (fibrinogen) c. PT: II, V, VII, X d. K-‐dep (warfarin): II, VII, IX, X V. “Infiltrative pattern”: ↑↑alk phos, near nl bili/AST/ALT a. CA: HCC, metastatic, lymphoma b. Granuloma: TB, sarcoid, histo c. Abscess: amoebic, bacterial
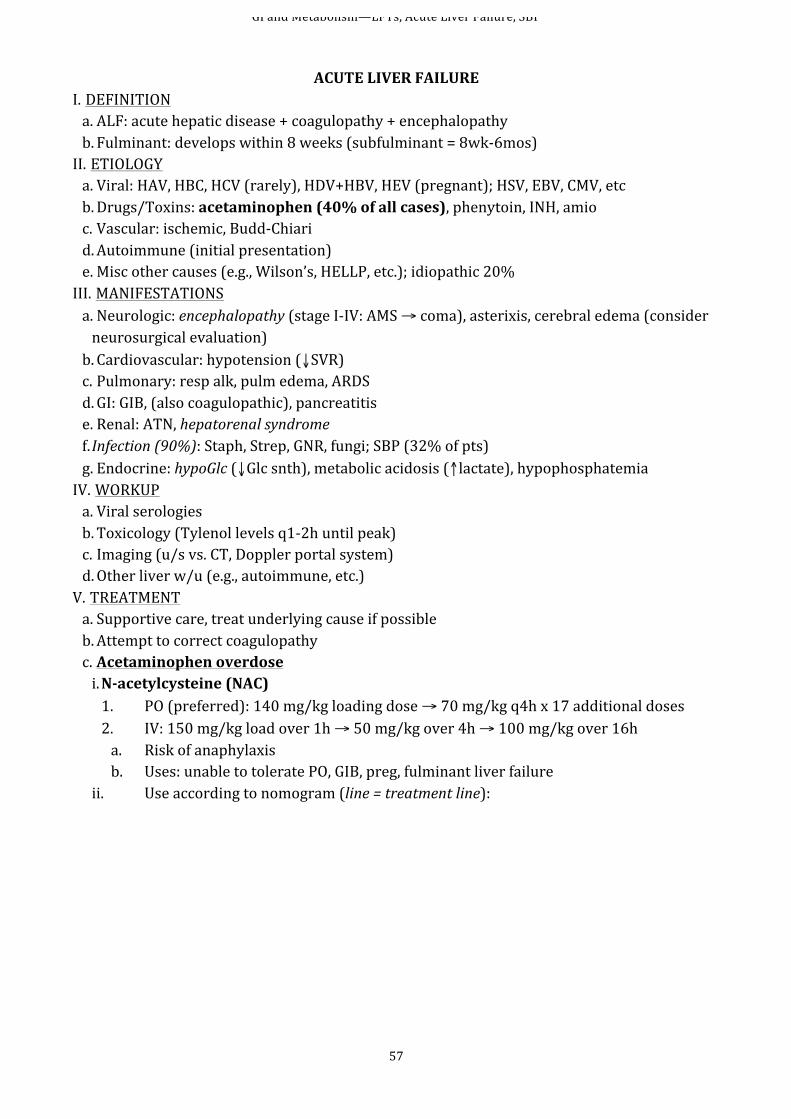
GI and Metabolism—LFTs, Acute Liver Failure, SBP
57
ACUTE LIVER FAILURE
I. DEFINITION a. ALF: acute hepatic disease + coagulopathy + encephalopathy b. Fulminant: develops within 8 weeks (subfulminant = 8wk-‐6mos) II. ETIOLOGY a. Viral: HAV, HBC, HCV (rarely), HDV+HBV, HEV (pregnant); HSV, EBV, CMV, etc b. Drugs/Toxins: acetaminophen (40% of all cases), phenytoin, INH, amio c. Vascular: ischemic, Budd-‐Chiari d. Autoimmune (initial presentation) e. Misc other causes (e.g., Wilson’s, HELLP, etc.); idiopathic 20% III. MANIFESTATIONS a. Neurologic: encephalopathy (stage I-‐IV: AMS → coma), asterixis, cerebral edema (consider neurosurgical evaluation) b. Cardiovascular: hypotension (↓SVR) c. Pulmonary: resp alk, pulm edema, ARDS d. GI: GIB, (also coagulopathic), pancreatitis e. Renal: ATN, hepatorenal syndrome f. Infection (90%): Staph, Strep, GNR, fungi; SBP (32% of pts) g. Endocrine: hypoGlc (↓Glc snth), metabolic acidosis (↑lactate), hypophosphatemia IV. WORKUP a. Viral serologies b. Toxicology (Tylenol levels q1-‐2h until peak) c. Imaging (u/s vs. CT, Doppler portal system) d. Other liver w/u (e.g., autoimmune, etc.) V. TREATMENT a. Supportive care, treat underlying cause if possible b. Attempt to correct coagulopathy c. Acetaminophen overdose i. N-‐acetylcysteine (NAC) 1. PO (preferred): 140 mg/kg loading dose → 70 mg/kg q4h x 17 additional doses 2. IV: 150 mg/kg load over 1h → 50 mg/kg over 4h → 100 mg/kg over 16h a. Risk of anaphylaxis b. Uses: unable to tolerate PO, GIB, preg, fulminant liver failure
ii. Use according to nomogram (line = treatment line):
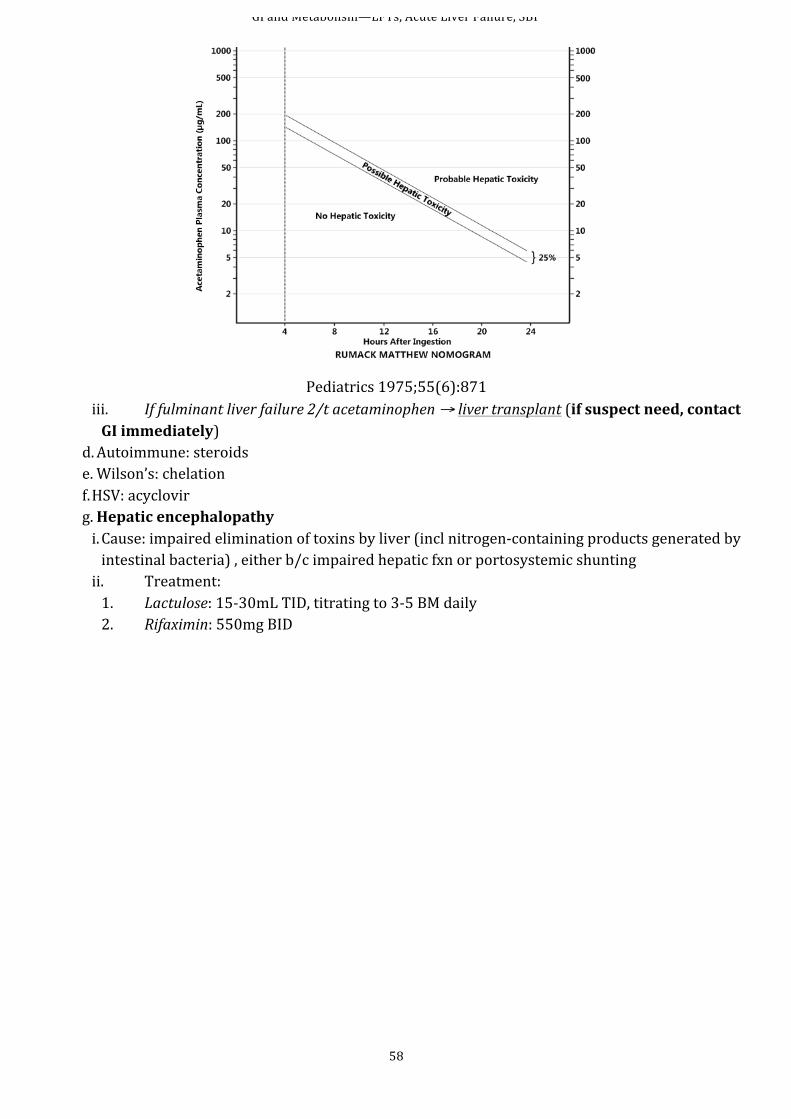
GI and Metabolism—LFTs, Acute Liver Failure, SBP
58
Pediatrics 1975;55(6):871 iii. If fulminant liver failure 2/t acetaminophen → liver transplant (if suspect need, contact GI immediately)
d. Autoimmune: steroids e. Wilson’s: chelation f. HSV: acyclovir g. Hepatic encephalopathy i. Cause: impaired elimination of toxins by liver (incl nitrogen-‐containing products generated by intestinal bacteria) , either b/c impaired hepatic fxn or portosystemic shunting ii. Treatment: 1. Lactulose: 15-‐30mL TID, titrating to 3-‐5 BM daily 2. Rifaximin: 550mg BID
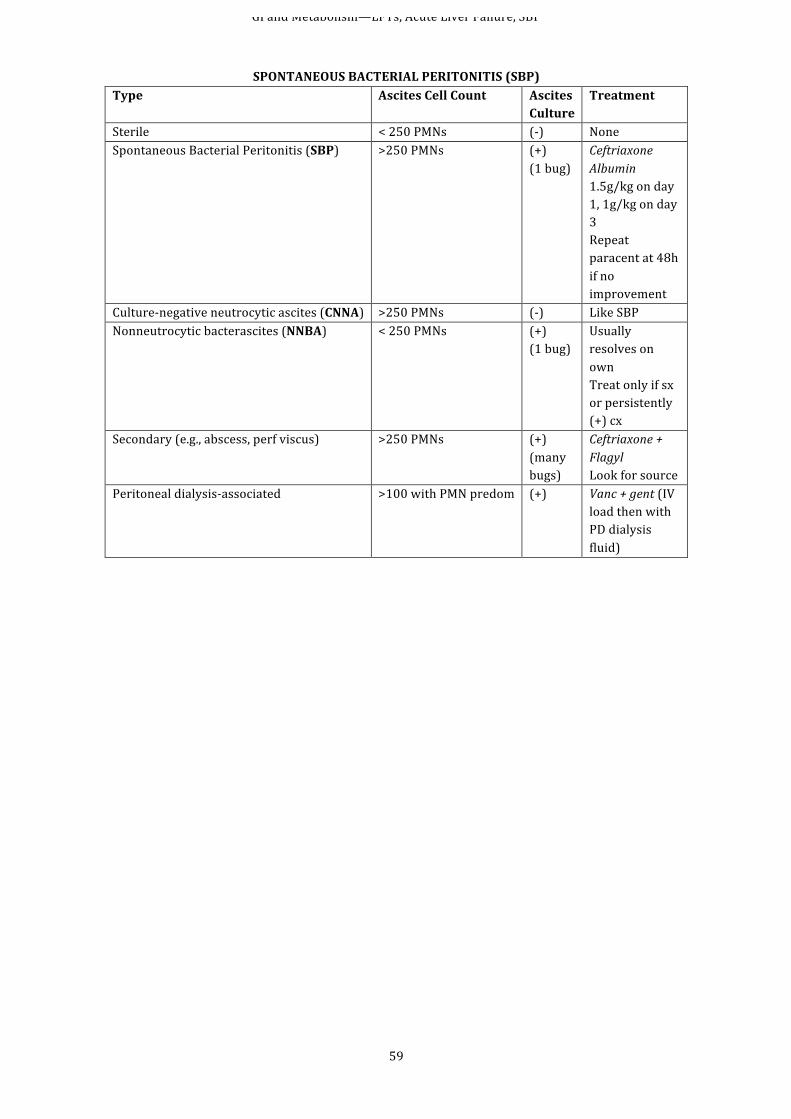
GI and Metabolism—LFTs, Acute Liver Failure, SBP
59
SPONTANEOUS BACTERIAL PERITONITIS (SBP)
Type Ascites Cell Count Ascites Culture
Treatment
Sterile < 250 PMNs (-‐) None Spontaneous Bacterial Peritonitis (SBP) >250 PMNs (+)
(1 bug) Ceftriaxone Albumin 1.5g/kg on day 1, 1g/kg on day 3 Repeat paracent at 48h if no improvement
Culture-‐negative neutrocytic ascites (CNNA) >250 PMNs (-‐) Like SBP Nonneutrocytic bacterascites (NNBA) < 250 PMNs (+)
(1 bug) Usually resolves on own Treat only if sx or persistently (+) cx
Secondary (e.g., abscess, perf viscus) >250 PMNs (+) (many bugs)
Ceftriaxone + Flagyl Look for source
Peritoneal dialysis-‐associated >100 with PMN predom (+) Vanc + gent (IV load then with PD dialysis fluid)
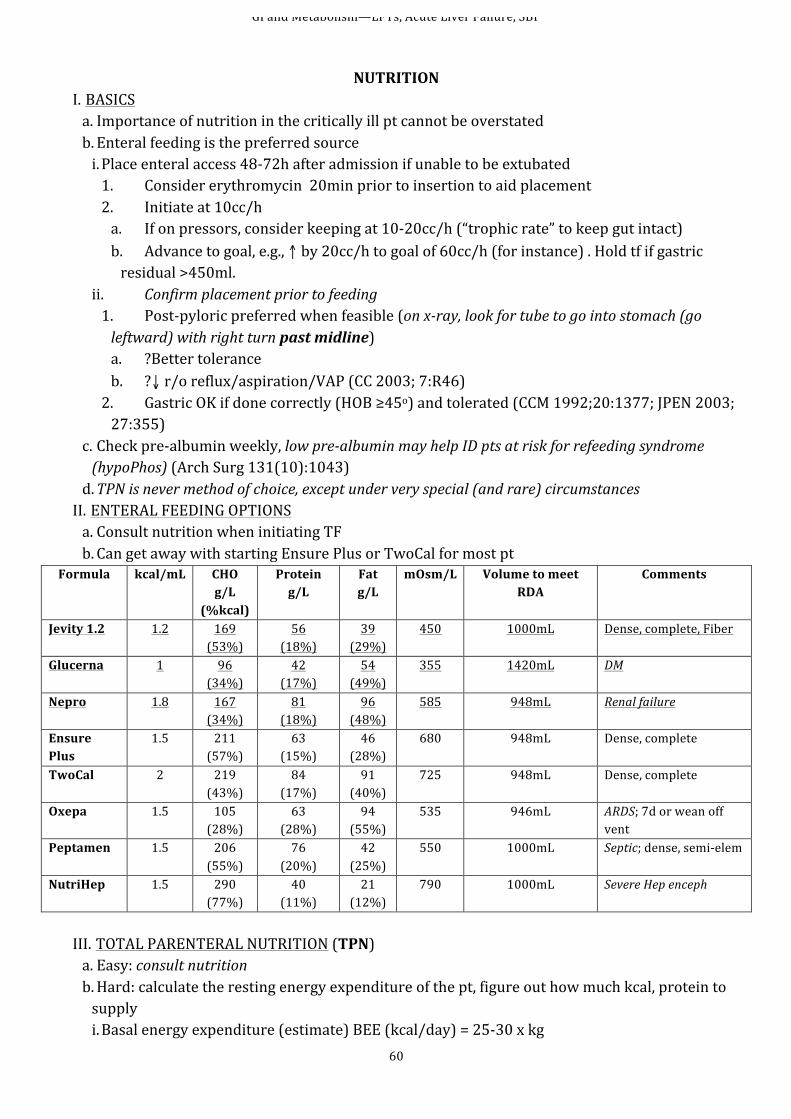
GI and Metabolism—LFTs, Acute Liver Failure, SBP
60
NUTRITION
I. BASICS a. Importance of nutrition in the critically ill pt cannot be overstated b. Enteral feeding is the preferred source i. Place enteral access 48-‐72h after admission if unable to be extubated 1. Consider erythromycin 20min prior to insertion to aid placement 2. Initiate at 10cc/h a. If on pressors, consider keeping at 10-‐20cc/h (“trophic rate” to keep gut intact) b. Advance to goal, e.g., ↑ by 20cc/h to goal of 60cc/h (for instance) . Hold tf if gastric residual >450ml.
ii. Confirm placement prior to feeding 1. Post-‐pyloric preferred when feasible (on x-‐ray, look for tube to go into stomach (go leftward) with right turn past midline) a. ?Better tolerance b. ?↓ r/o reflux/aspiration/VAP (CC 2003; 7:R46) 2. Gastric OK if done correctly (HOB ≥45o) and tolerated (CCM 1992;20:1377; JPEN 2003; 27:355)
c. Check pre-‐albumin weekly, low pre-‐albumin may help ID pts at risk for refeeding syndrome (hypoPhos) (Arch Surg 131(10):1043) d. TPN is never method of choice, except under very special (and rare) circumstances II. ENTERAL FEEDING OPTIONS a. Consult nutrition when initiating TF b. Can get away with starting Ensure Plus or TwoCal for most pt
Formula kcal/mL
CHO g/L
(%kcal)
Protein g/L
Fat g/L
mOsm/L Volume to meet RDA
Comments
Jevity 1.2 1.2 169 (53%)
56 (18%)
39 (29%)
450 1000mL Dense, complete, Fiber
Glucerna 1 96 (34%)
42 (17%)
54 (49%)
355 1420mL DM
Nepro 1.8 167 (34%)
81 (18%)
96 (48%)
585 948mL Renal failure
Ensure Plus
1.5 211 (57%)
63 (15%)
46 (28%)
680 948mL Dense, complete
TwoCal 2 219 (43%)
84 (17%)
91 (40%)
725 948mL Dense, complete
Oxepa 1.5 105 (28%)
63 (28%)
94 (55%)
535 946mL ARDS; 7d or wean off vent
Peptamen 1.5 206 (55%)
76 (20%)
42 (25%)
550 1000mL Septic; dense, semi-‐elem
NutriHep 1.5 290 (77%)
40 (11%)
21 (12%)
790 1000mL Severe Hep enceph
III. TOTAL PARENTERAL NUTRITION (TPN) a. Easy: consult nutrition b. Hard: calculate the resting energy expenditure of the pt, figure out how much kcal, protein to supply i. Basal energy expenditure (estimate) BEE (kcal/day) = 25-‐30 x kg

GI and Metabolism—LFTs, Acute Liver Failure, SBP
61
1. BEE does not take into account thermal effect of food intake 2. Can adjust for hypermetabolic conditions a. Fever: BEE x 1.1(for each oC above 37) b. Stress: mild (x1.2), moderate (x1.4), severe (x1.6)
ii. Estimate daily protein calories 1. Normal metabolism: 0.8-‐1 g/kg 2. Hypercatabolism: 1.2-‐1.6 g/kg iii. Figure out how to give protein 1. Final product has 1000mL and often has 6% (6g/100mL, or 60g/L) amino acids and 20% dextrose (20g/100mL, or 200g/L) a. Volume of TPN = (calculated protein requirement g/day) / (60 g/L) = X L/day b. Divide by 24h to get hourly infusion rate
iv. Figure out how many calories given by dextrose (200g/L) daily 1. Dextrose cal = X g/day x 3.4kcal/g 2. This likely will not cover the daily caloric requirement calculated above 3. Supply remaining calories with IV lipid emulsion v. 10% lipid emulsion (1 kcal/mL) used to infuse remainder 1. Comes in volumes of 50mL, so round off to nearest 50 2. Infuse at half the max rate (50mL/h) to prevent lipemic serum vi. Walkthrough calculations 1. Let’s say for 70kg pt, daily cal req is 25 kcal/kg and protein 1.4g/kg a. Calorie = 25kcal/kg x 70kg = 1750 kcal/day b. Protein = 1.4 g/day x 70kg = 98g/day 2. How much 6% aa 20% Dex TPN to give protein? a. Volume of TPN = (98g/day) / (50g/L) = 1.63L/day b. 1630ml/24h = 68mL/h (round to 70) 3. How much calories are supplied by dextrose, and how much is still left? a. Amount of dextrose being given = 200g/L x 1.68L/day = 336g/day b. Calories from dextrose = 336g/day x 3.4kcal/g = 1142kcal/day c. Add calories from protein (4 kcal/g ptn X 98g/day protein) = 392 kcal d. This leaves 216 kcal/day to be supplied by lipids (1750 total required minus the 1142 supplied by dextrose minus the 392 supplied by protein)
4. How much of a 10% lipid emulsion (1 kcal/mL) to be given per day? a. 216kcal needed → 216mL b. Round to nearest 50mL → 200 mL of 10% lipid 5. Final order? a. Standard 6%aa and D20 to run at 70mL/h b. Add standard electrolytes, multivitamins, and trace elements c. Give 10% Intralipid: 200 mL to infuse over 6h
c. Complications of parenteral nutrition i. General 1. Mucosal atrophy → bacterial translocation → sepsis of bowel origin 2. Acalculous cholecystitis ii. Carbohydrate infusions: HyperGlc, hypoPhos, fatty liver, ↑pCO2 (from ↑carb breakdown) iii. Lipid: ↑r/o oxidation-‐induced cell injury
GI and Metabolism—LFTs, Acute Liver Failure, SBP
62
iv. Consider metabolic cart if concerned about hyperglycemia or hypercarbia. IV. FOR ALL NON-‐INTUBATED PTS IN ICU, ASESS SWALLOWING a. For relatively low-‐risk pts (not neurologically compromised), may do bedside eval by having them sip H2O through a straw without coughing (= fail) b. For others (i.e., most ICU pts), get a formal swallow eval c. Try to start “regular” diet ASAP
Endocrinology—DKA
63
Diabetic Ketoacidosis (DKA) and
Hyperosmolar Hyperglycemic State (HHS, or Hyperosmolar Nonketotic State [HONK]) (Ann Intern Med 2010; 152(1):ITC-‐1)
I. Precipitants a. Infection b. Intoxication: alcohol, drugs (esp. amphetamines, cocaine) c. Psychological stress d. Pregnancy e. Cardiovascular events (e.g., MI, CVA, mesenteric ischemia) f. Trauma g. Cushing’s disease h. Medications (e.g., corticosteroids,) i. Acute GI dz (e.g., pancreatitis, obstruction II. Epidemiology a. Mostly type 1 DM b. 22% have type 2 DM III. HHS/HONK: very similar in precipitants and treatment; primary differentiation is Glc (typically
>600 in HHS) IV. Differential Disease Characteristics Notes
Starvation ketosis Pts may have intercurrent illness and quite ill, usu clear h/o not eating and poss n/v
Glc can be nl, ↑, or little ↑. Does not lead to acidosis; HCO3 usu >18
Alcoholic ketoacidosis
h/o excessive EtOH w/ long-‐term abuse Glc: nl of ↓ with ketonemia and metabolic acidosis. Osmolar gap can occur
Lactic acidosis Lactate usu ≥5mmol/L Can co-‐occur w/ DKA Suspect if h/o metformin
Salicylate intoxication
Anion gap metabolic acidosis, often with 1o resp alkalosis
Glc usu not elevated, may be ↓. Measure salicylate level
Methanol intox Ketones not signif ↑, sx incl blurry vision & abd pain, but anion gap & osmolar gap are typically high
Glc nl/↑. Measure methanol level
Ethylene glycol intox
Ketones not usu ↑, but anion gap & osmolar gap are typically high
Glc variable; calcium oxalate and hippurate crystals can be seen in urine. Measure ethylene glycol
Chronic renal failure
Mild acidosis w/ slight ↑ in AG, ketones not ↑ h/o ↑Cr
Pseudoketosis Paraldehyde or isopropyl alcohol ingestion Nl pH and nl AG, high osmolar gap Rhabdomyolysis CK usu very ↑. Causes of rhabdo may be present
(statins, trauma, heat stroke, etc.) pH ↓, Glc nl, ketones nl with AG and myoglobinuria
V. Treatment a. Use DKA protocol & GIVE FLUIDS! i. Algorithms below gives basics of therapy ii. Don’t forget about insulin affecting K+ b. In ICU, consider placement of art line for frequent ABGs
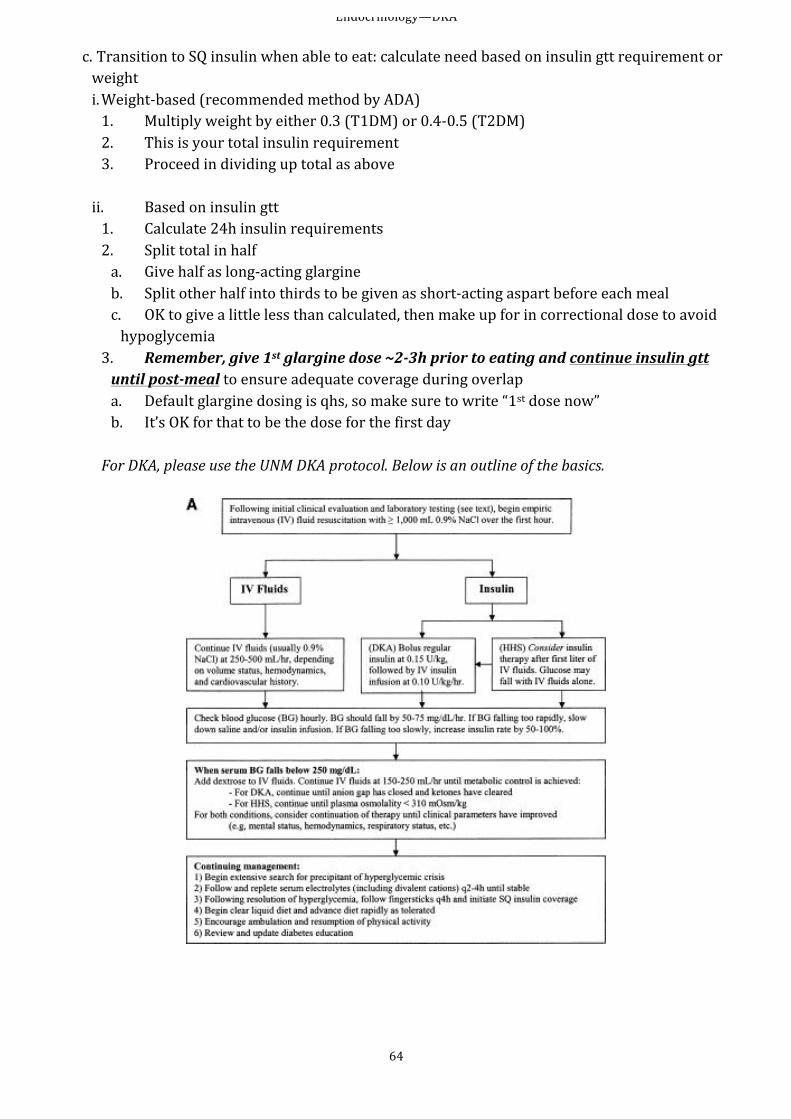
Endocrinology—DKA
64
c. Transition to SQ insulin when able to eat: calculate need based on insulin gtt requirement or weight i. Weight-‐based (recommended method by ADA) 1. Multiply weight by either 0.3 (T1DM) or 0.4-‐0.5 (T2DM) 2. This is your total insulin requirement 3. Proceed in dividing up total as above
ii. Based on insulin gtt 1. Calculate 24h insulin requirements 2. Split total in half a. Give half as long-‐acting glargine b. Split other half into thirds to be given as short-‐acting aspart before each meal c. OK to give a little less than calculated, then make up for in correctional dose to avoid hypoglycemia
3. Remember, give 1st glargine dose ~2-‐3h prior to eating and continue insulin gtt until post-‐meal to ensure adequate coverage during overlap a. Default glargine dosing is qhs, so make sure to write “1st dose now” b. It’s OK for that to be the dose for the first day For DKA, please use the UNM DKA protocol. Below is an outline of the basics.
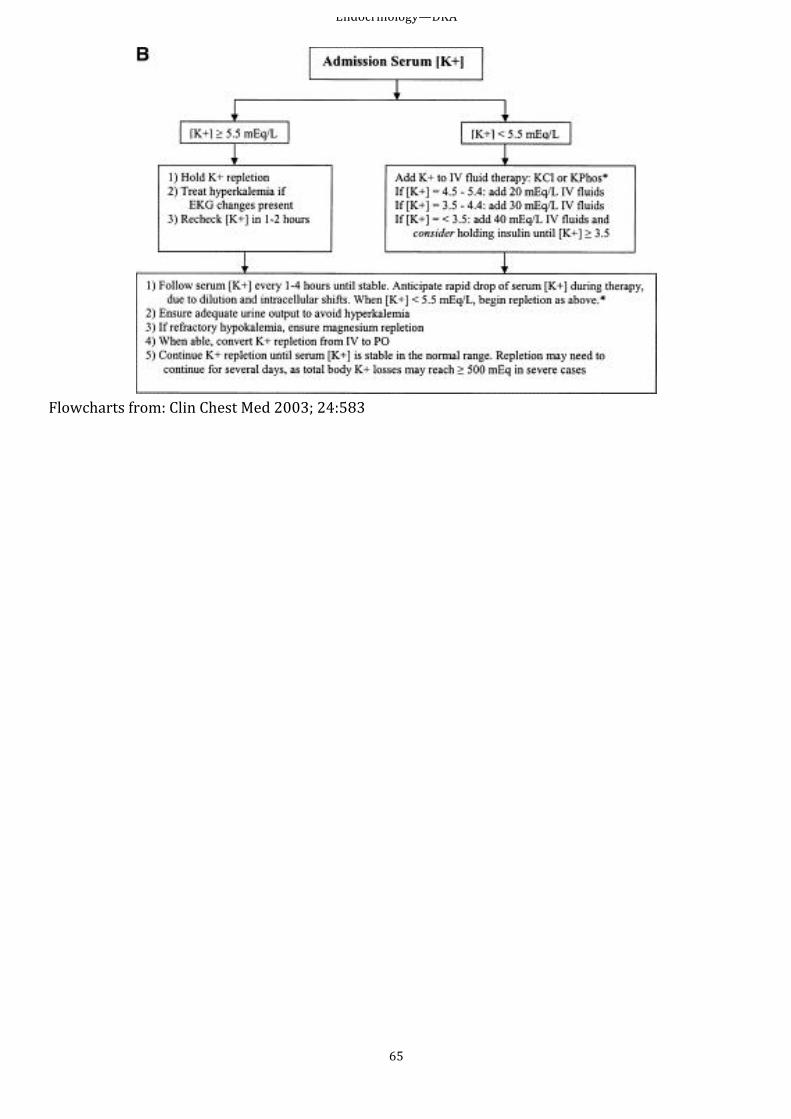
Endocrinology—DKA
65
Flowcharts from: Clin Chest Med 2003; 24:583
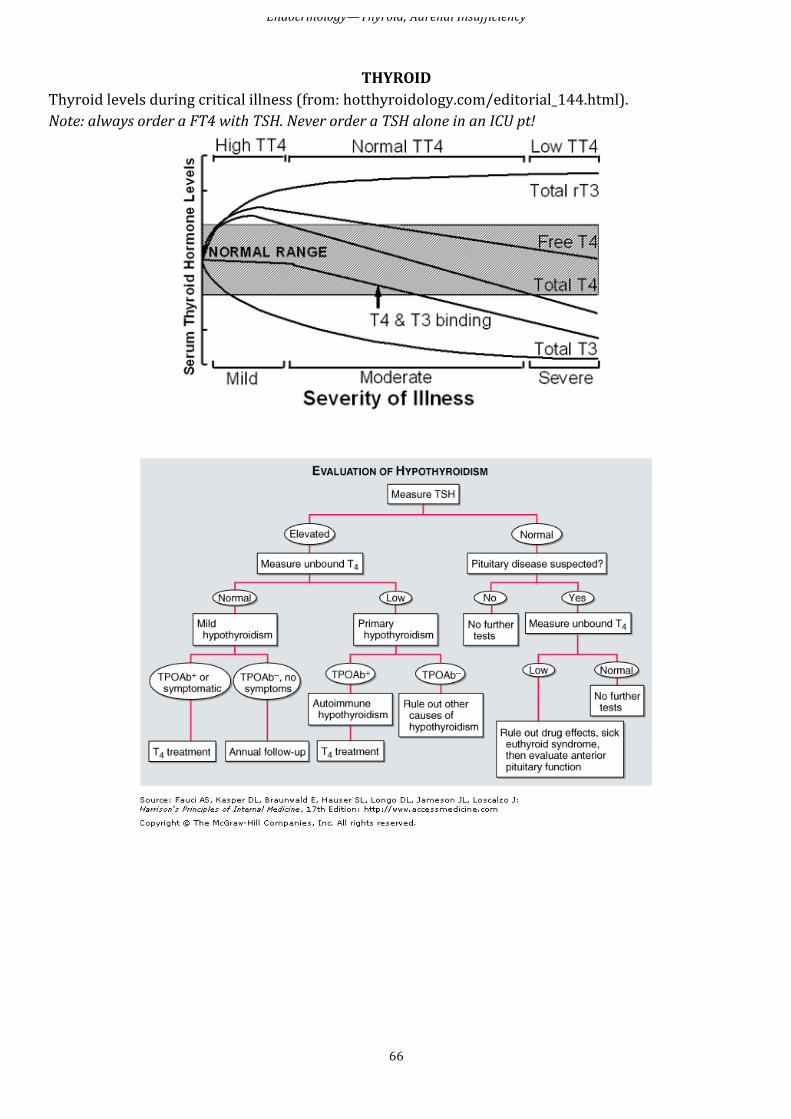
Endocrinology—Thyroid; Adrenal Insufficiency
66
THYROID
Thyroid levels during critical illness (from: hotthyroidology.com/editorial_144.html). Note: always order a FT4 with TSH. Never order a TSH alone in an ICU pt!
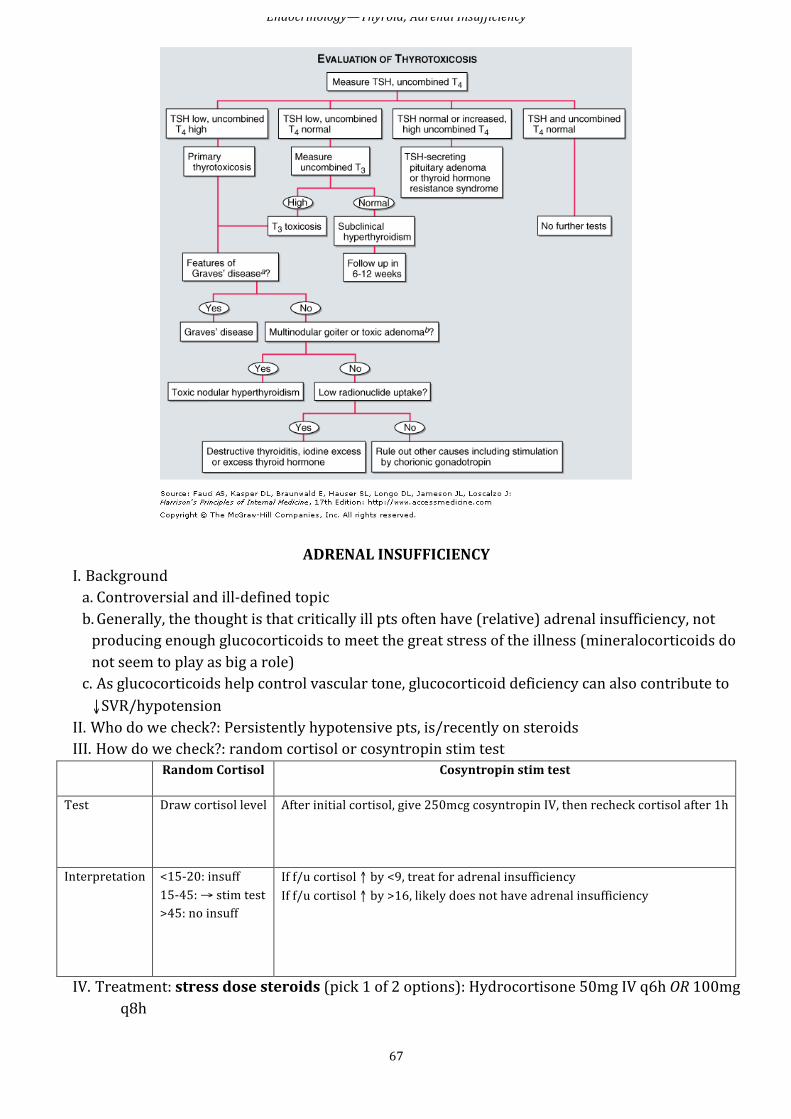
Endocrinology—Thyroid; Adrenal Insufficiency
67
ADRENAL INSUFFICIENCY I. Background a. Controversial and ill-‐defined topic b. Generally, the thought is that critically ill pts often have (relative) adrenal insufficiency, not producing enough glucocorticoids to meet the great stress of the illness (mineralocorticoids do not seem to play as big a role) c. As glucocorticoids help control vascular tone, glucocorticoid deficiency can also contribute to ↓SVR/hypotension
II. Who do we check?: Persistently hypotensive pts, is/recently on steroids III. How do we check?: random cortisol or cosyntropin stim test Random Cortisol Cosyntropin stim test
Test Draw cortisol level After initial cortisol, give 250mcg cosyntropin IV, then recheck cortisol after 1h
Interpretation <15-‐20: insuff 15-‐45: → stim test >45: no insuff
If f/u cortisol ↑ by <9, treat for adrenal insufficiency If f/u cortisol ↑ by >16, likely does not have adrenal insufficiency
IV. Treatment: stress dose steroids (pick 1 of 2 options): Hydrocortisone 50mg IV q6h OR 100mg q8h
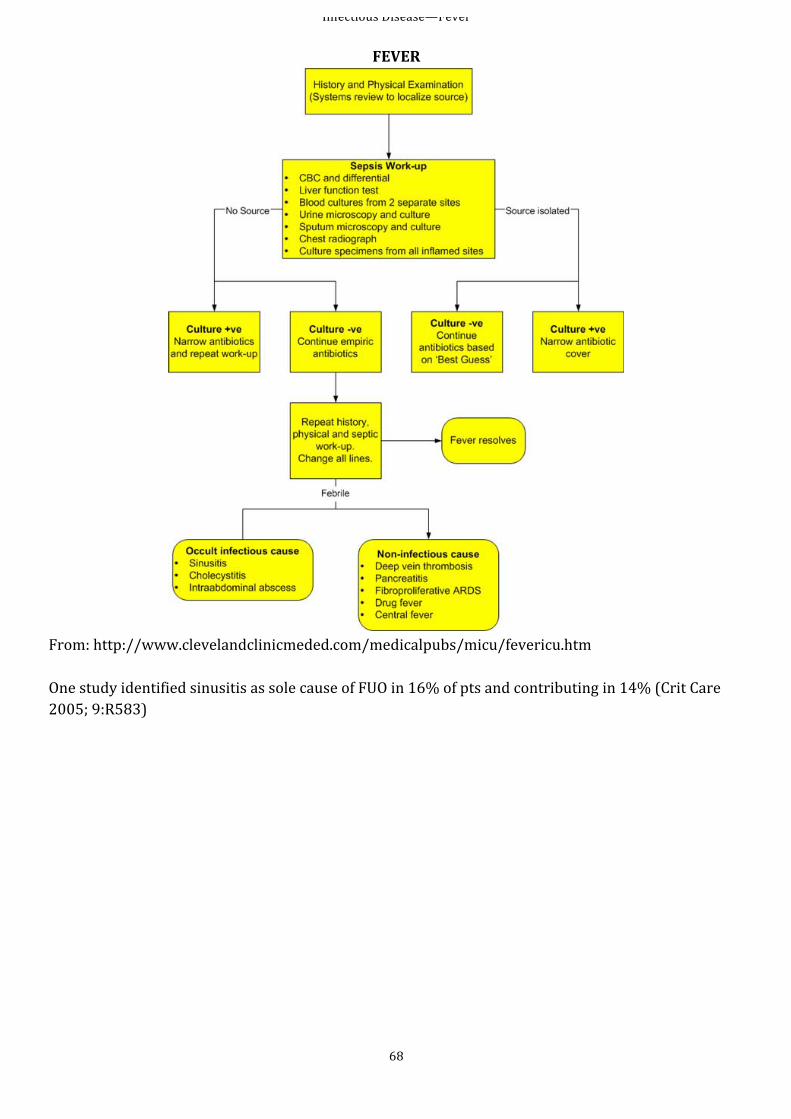
Infectious Disease—Fever
68
FEVER
From: http://www.clevelandclinicmeded.com/medicalpubs/micu/fevericu.htm One study identified sinusitis as sole cause of FUO in 16% of pts and contributing in 14% (Crit Care 2005; 9:R583)
Infectious Disease—Sepsis & Empiric Abx
69
SEPSIS
See also: “Septic Shock” I. Definitions a. Bacteremia—bacteria in blood (i.e., +blood cx) b. Systemic inflammatory response syndrome (SIRS)— ≥2 of following: i. Temp >38oC or <36 ii. RR >20 or pCO2 <32 iii. HR >90 iv. WBC <4k or >12k or >10% banded neutrophils c. Sepsis—SIRS that has proven or suspected microbial etiology d. Severe sepsis—sepsis with 1+ signs of organ dysfunction e. Septic shock—sepsis with hypotension (SBP <90) after intitial bolus or need for vasopressors to maintain SBP >90 f. Note: the latest surviving sepsis guidelines (Crit Care Med 2013; 41:580-‐637) do not clearly define sepsis in relations to SIRS, leaving the definition more broad. Nevertheless, SIRS is a useful rubric for evaluation.
II. Pathogenesis a. Bacteria, fungi, or exotoxins → system-‐wide inflammation (i.e., SIRS) i. Pro-‐inflammatory molecules → ↑blood flow to infected tissue, ↑permeability of local blood vessels, recruit neutrophils, elicit pain ii. TNF-‐α is central mediator iii. Intravascular thrombosis locally walls off infected tissue; if systemic → DIC b. Organ dysfunction & shock i. Endothelial injury → cytokines, procoagulants, PAF, NO, etc → ↑vasc perm, microvasc thrombosis, DIC, hypotension ii. Tissue oxygenation 1. May ↓ as number of functional capillaries ↓ (d/t thrombosis, etc) 2. May ↓ by “hibernation” period d/t mitochondrial dysfxn caused by NO
III. Treatment a. Use “Adult sepsis/SMITe” order set: ensures abx to be delivered stat i. If possible, try to obtain blood cx (2 sets) prior to abx, but don’t delay treatment too long ii. Abx not ordered using this order set are routine by default: make sure get abx STAT b. Initial therapy focused on appropriate (broad-‐spectrum) abx and surgical intervention as needed (e.g., drain abscess) i. See empiric regimens below ii. Why is it important to get it right the 1st time?
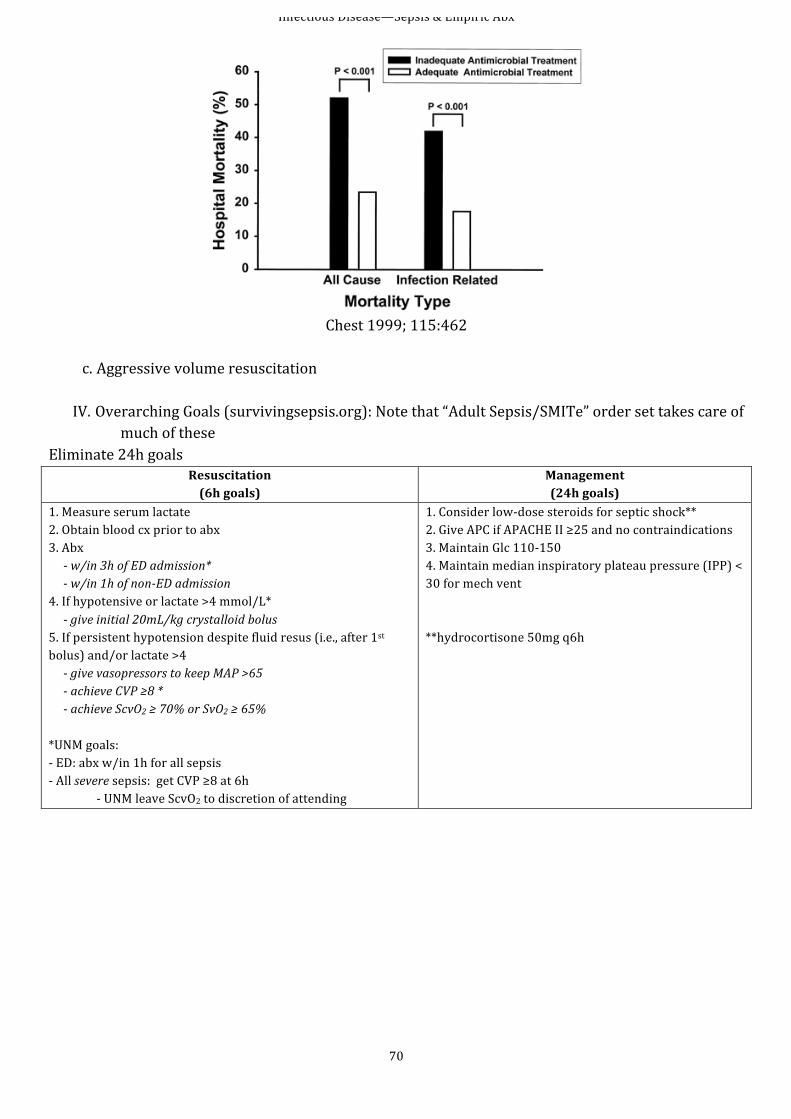
Infectious Disease—Sepsis & Empiric Abx
70
Chest 1999; 115:462
c. Aggressive volume resuscitation
IV. Overarching Goals (survivingsepsis.org): Note that “Adult Sepsis/SMITe” order set takes care of much of these
Eliminate 24h goals Resuscitation (6h goals)
Management (24h goals)
1. Measure serum lactate 2. Obtain blood cx prior to abx 3. Abx -‐ w/in 3h of ED admission* -‐ w/in 1h of non-‐ED admission 4. If hypotensive or lactate >4 mmol/L* -‐ give initial 20mL/kg crystalloid bolus 5. If persistent hypotension despite fluid resus (i.e., after 1st bolus) and/or lactate >4 -‐ give vasopressors to keep MAP >65 -‐ achieve CVP ≥8 * -‐ achieve ScvO2 ≥ 70% or SvO2 ≥ 65% *UNM goals: -‐ ED: abx w/in 1h for all sepsis -‐ All severe sepsis: get CVP ≥8 at 6h
-‐ UNM leave ScvO2 to discretion of attending
1. Consider low-‐dose steroids for septic shock** 2. Give APC if APACHE II ≥25 and no contraindications 3. Maintain Glc 110-‐150 4. Maintain median inspiratory plateau pressure (IPP) < 30 for mech vent **hydrocortisone 50mg q6h
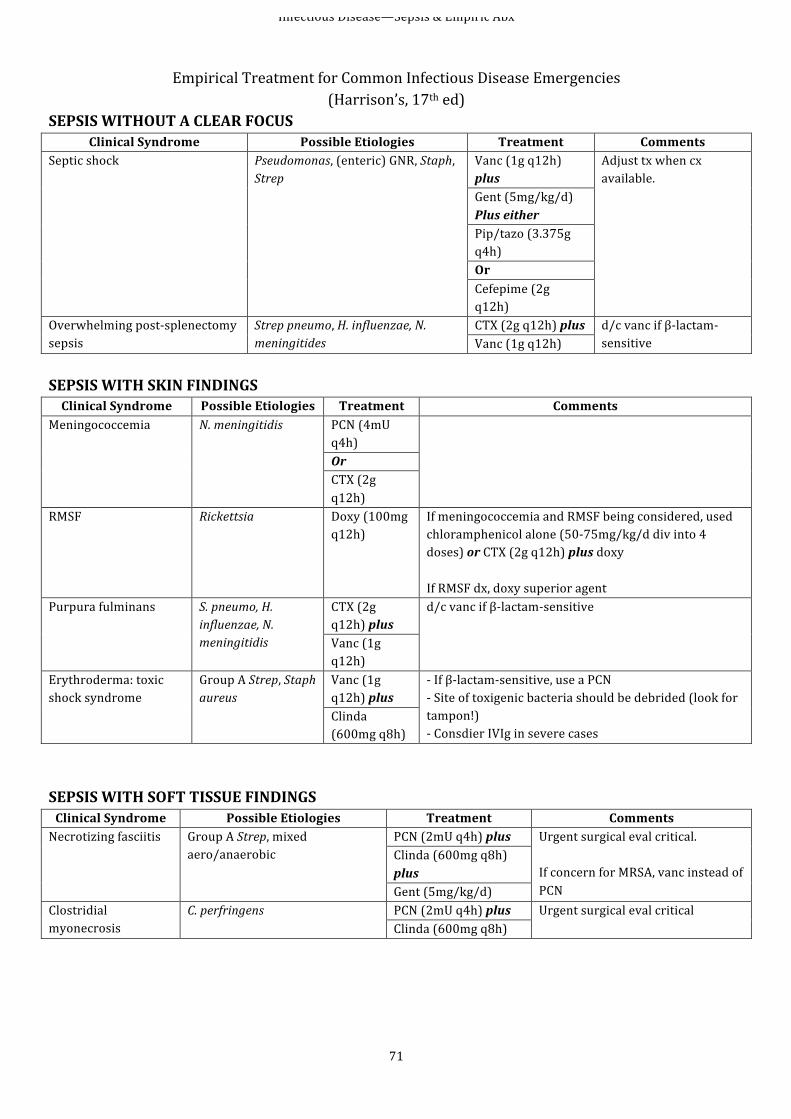
Infectious Disease—Sepsis & Empiric Abx
71
Empirical Treatment for Common Infectious Disease Emergencies
(Harrison’s, 17th ed) SEPSIS WITHOUT A CLEAR FOCUS
Clinical Syndrome Possible Etiologies Treatment Comments Septic shock Pseudomonas, (enteric) GNR, Staph,
Strep Vanc (1g q12h) plus
Adjust tx when cx available. Gent (5mg/kg/d)
Plus either Pip/tazo (3.375g q4h) Or Cefepime (2g q12h)
Overwhelming post-‐splenectomy sepsis
Strep pneumo, H. influenzae, N. meningitides
CTX (2g q12h) plus d/c vanc if β-‐lactam-‐sensitive Vanc (1g q12h)
SEPSIS WITH SKIN FINDINGS Clinical Syndrome Possible Etiologies Treatment Comments
Meningococcemia N. meningitidis PCN (4mU q4h)
Or CTX (2g q12h)
RMSF Rickettsia Doxy (100mg q12h)
If meningococcemia and RMSF being considered, used chloramphenicol alone (50-‐75mg/kg/d div into 4 doses) or CTX (2g q12h) plus doxy If RMSF dx, doxy superior agent
Purpura fulminans S. pneumo, H. influenzae, N. meningitidis
CTX (2g q12h) plus
d/c vanc if β-‐lactam-‐sensitive
Vanc (1g q12h)
Erythroderma: toxic shock syndrome
Group A Strep, Staph aureus
Vanc (1g q12h) plus
-‐ If β-‐lactam-‐sensitive, use a PCN -‐ Site of toxigenic bacteria should be debrided (look for tampon!) -‐ Consdier IVIg in severe cases
Clinda (600mg q8h)
SEPSIS WITH SOFT TISSUE FINDINGS Clinical Syndrome Possible Etiologies Treatment Comments Necrotizing fasciitis Group A Strep, mixed
aero/anaerobic PCN (2mU q4h) plus Urgent surgical eval critical.
If concern for MRSA, vanc instead of PCN
Clinda (600mg q8h) plus Gent (5mg/kg/d)
Clostridial myonecrosis
C. perfringens PCN (2mU q4h) plus Urgent surgical eval critical Clinda (600mg q8h)
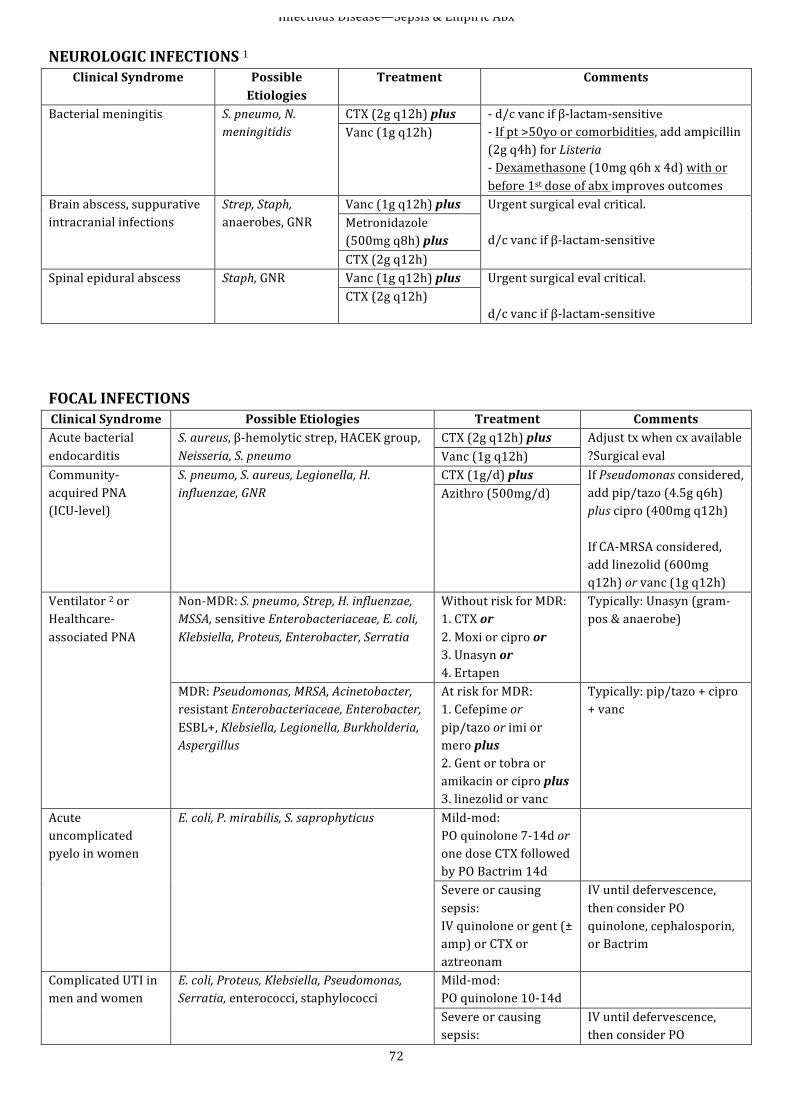
Infectious Disease—Sepsis & Empiric Abx
72
NEUROLOGIC INFECTIONS 1 Clinical Syndrome Possible
Etiologies Treatment Comments
Bacterial meningitis S. pneumo, N. meningitidis
CTX (2g q12h) plus -‐ d/c vanc if β-‐lactam-‐sensitive -‐ If pt >50yo or comorbidities, add ampicillin (2g q4h) for Listeria -‐ Dexamethasone (10mg q6h x 4d) with or before 1st dose of abx improves outcomes
Vanc (1g q12h)
Brain abscess, suppurative intracranial infections
Strep, Staph, anaerobes, GNR
Vanc (1g q12h) plus Urgent surgical eval critical. d/c vanc if β-‐lactam-‐sensitive
Metronidazole (500mg q8h) plus CTX (2g q12h)
Spinal epidural abscess Staph, GNR Vanc (1g q12h) plus Urgent surgical eval critical. d/c vanc if β-‐lactam-‐sensitive
CTX (2g q12h)
FOCAL INFECTIONS Clinical Syndrome Possible Etiologies Treatment Comments Acute bacterial endocarditis
S. aureus, β-‐hemolytic strep, HACEK group, Neisseria, S. pneumo
CTX (2g q12h) plus Adjust tx when cx available ?Surgical eval Vanc (1g q12h)
Community-‐acquired PNA (ICU-‐level)
S. pneumo, S. aureus, Legionella, H. influenzae, GNR
CTX (1g/d) plus If Pseudomonas considered, add pip/tazo (4.5g q6h) plus cipro (400mg q12h) If CA-‐MRSA considered, add linezolid (600mg q12h) or vanc (1g q12h)
Azithro (500mg/d)
Ventilator 2 or Healthcare-‐associated PNA
Non-‐MDR: S. pneumo, Strep, H. influenzae, MSSA, sensitive Enterobacteriaceae, E. coli, Klebsiella, Proteus, Enterobacter, Serratia
Without risk for MDR: 1. CTX or 2. Moxi or cipro or 3. Unasyn or 4. Ertapen
Typically: Unasyn (gram-‐pos & anaerobe)
MDR: Pseudomonas, MRSA, Acinetobacter, resistant Enterobacteriaceae, Enterobacter, ESBL+, Klebsiella, Legionella, Burkholderia, Aspergillus
At risk for MDR: 1. Cefepime or pip/tazo or imi or mero plus 2. Gent or tobra or amikacin or cipro plus 3. linezolid or vanc
Typically: pip/tazo + cipro + vanc
Acute uncomplicated pyelo in women
E. coli, P. mirabilis, S. saprophyticus Mild-‐mod: PO quinolone 7-‐14d or one dose CTX followed by PO Bactrim 14d
Severe or causing sepsis: IV quinolone or gent (± amp) or CTX or aztreonam
IV until defervescence, then consider PO quinolone, cephalosporin, or Bactrim
Complicated UTI in men and women
E. coli, Proteus, Klebsiella, Pseudomonas, Serratia, enterococci, staphylococci
Mild-‐mod: PO quinolone 10-‐14d
Severe or causing sepsis:
IV until defervescence, then consider PO
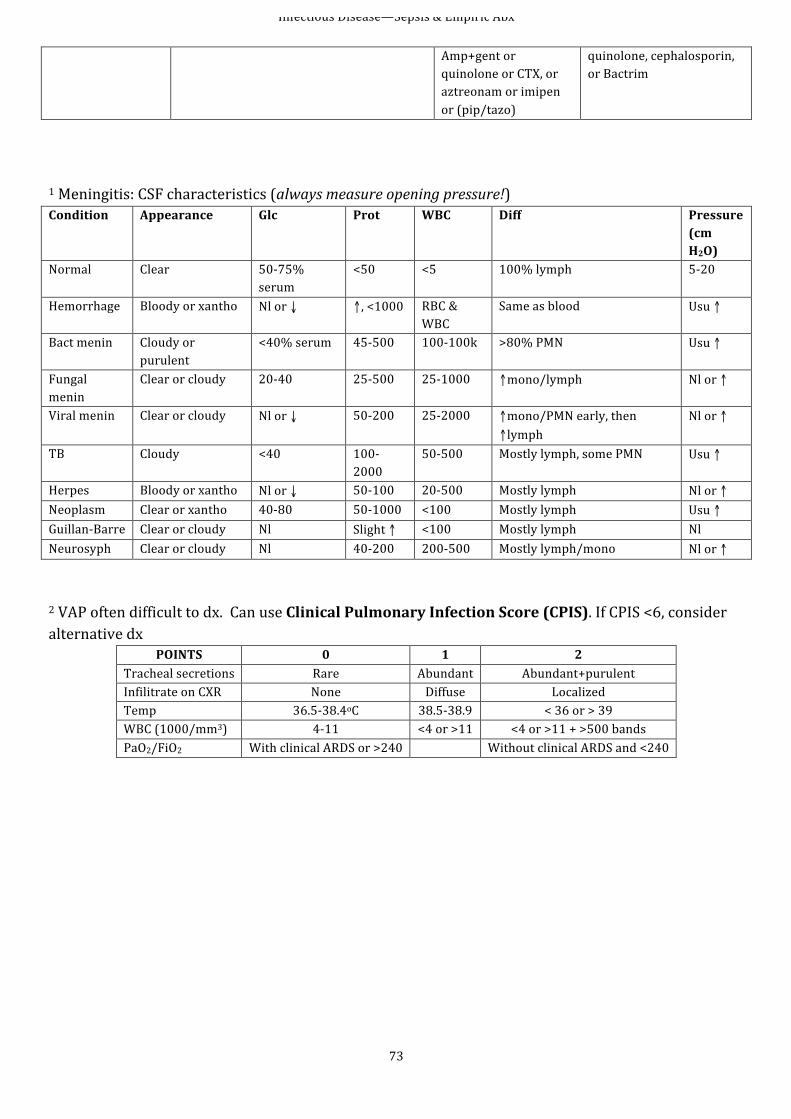
Infectious Disease—Sepsis & Empiric Abx
73
Amp+gent or quinolone or CTX, or aztreonam or imipen or (pip/tazo)
quinolone, cephalosporin, or Bactrim
1 Meningitis: CSF characteristics (always measure opening pressure!) Condition Appearance Glc Prot WBC Diff Pressure
(cm H2O)
Normal Clear 50-‐75% serum
<50 <5 100% lymph 5-‐20
Hemorrhage Bloody or xantho Nl or ↓ ↑, <1000 RBC & WBC
Same as blood Usu ↑
Bact menin Cloudy or purulent
<40% serum 45-‐500 100-‐100k >80% PMN Usu ↑
Fungal menin
Clear or cloudy 20-‐40 25-‐500 25-‐1000 ↑mono/lymph Nl or ↑
Viral menin Clear or cloudy Nl or ↓ 50-‐200 25-‐2000 ↑mono/PMN early, then ↑lymph
Nl or ↑
TB Cloudy <40 100-‐2000
50-‐500 Mostly lymph, some PMN Usu ↑
Herpes Bloody or xantho Nl or ↓ 50-‐100 20-‐500 Mostly lymph Nl or ↑ Neoplasm Clear or xantho 40-‐80 50-‐1000 <100 Mostly lymph Usu ↑ Guillan-‐Barre Clear or cloudy Nl Slight ↑ <100 Mostly lymph Nl Neurosyph Clear or cloudy Nl 40-‐200 200-‐500 Mostly lymph/mono Nl or ↑ 2 VAP often difficult to dx. Can use Clinical Pulmonary Infection Score (CPIS). If CPIS <6, consider alternative dx
POINTS 0 1 2 Tracheal secretions Rare Abundant Abundant+purulent Infilitrate on CXR None Diffuse Localized Temp 36.5-‐38.4oC 38.5-‐38.9 < 36 or > 39 WBC (1000/mm3) 4-‐11 <4 or >11 <4 or >11 + >500 bands PaO2/FiO2 With clinical ARDS or >240 Without clinical ARDS and <240
Infectious Disease—Hanta
74
HANTAVIRUS INFECTION
(Hantavirus Cardiopulmonary Syndrome, HCPS) The Basics
I. Etiology/Pathogenesis a. Spread by infection after contact with aerosolized deermice urine (e.g., cleaning abandoned sheds) b. Suspect in patient who presents with fever, myalgias and thrombocytopenia esp if also. hemoconcentration c. Progresses to Pulmonary edema and Cardiogenic Shock.
II. Diagnosis (Am J Clin Pathol 2001; 116:665-‐72) a. Initial Diagnosis based on peripheral smear criteria: i. Hct >50 (48 in women) ii. Plt <150 iii. Absence of toxic granulation in neutrophils, iv. Bands (myelocytes) >10% of neutrophils v. Immunoblasts >10% of circulating lymphocytes (requires hem/path to interpret) b. 4/5 criteria = HCPS (sensitivity 96%, specificity 99%)
III. Treatment a. Withhold all IV fluids. b. Use vasopressors to support blood pressure if necessary. c. Contact MICU attending, who will alert ECMO team and hem/path in suspected cases
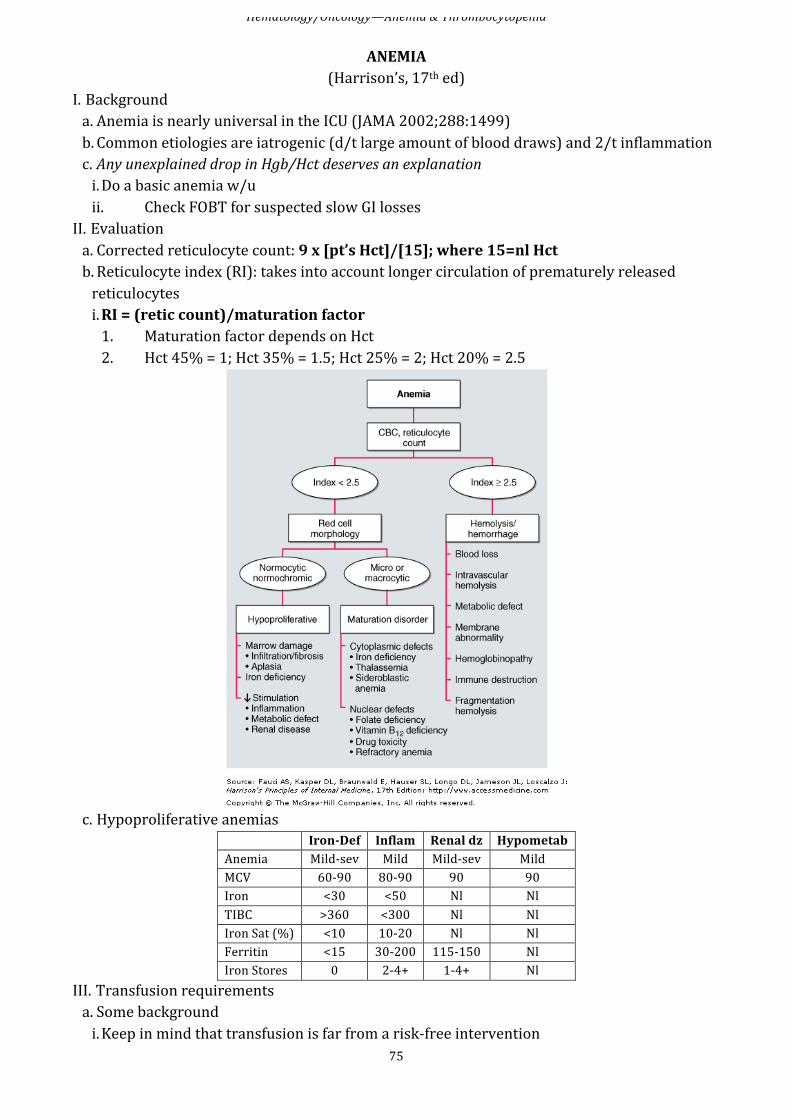
Hematology/Oncology—Anemia & Thrombocytopenia
75
ANEMIA (Harrison’s, 17th ed)
I. Background a. Anemia is nearly universal in the ICU (JAMA 2002;288:1499) b. Common etiologies are iatrogenic (d/t large amount of blood draws) and 2/t inflammation c. Any unexplained drop in Hgb/Hct deserves an explanation i. Do a basic anemia w/u ii. Check FOBT for suspected slow GI losses
II. Evaluation a. Corrected reticulocyte count: 9 x [pt’s Hct]/[15]; where 15=nl Hct b. Reticulocyte index (RI): takes into account longer circulation of prematurely released reticulocytes i. RI = (retic count)/maturation factor 1. Maturation factor depends on Hct 2. Hct 45% = 1; Hct 35% = 1.5; Hct 25% = 2; Hct 20% = 2.5
c. Hypoproliferative anemias
Iron-‐Def Inflam Renal dz Hypometab Anemia Mild-‐sev Mild Mild-‐sev Mild MCV 60-‐90 80-‐90 90 90 Iron <30 <50 Nl Nl TIBC >360 <300 Nl Nl Iron Sat (%) <10 10-‐20 Nl Nl Ferritin <15 30-‐200 115-‐150 Nl Iron Stores 0 2-‐4+ 1-‐4+ Nl
III. Transfusion requirements a. Some background i. Keep in mind that transfusion is far from a risk-‐free intervention
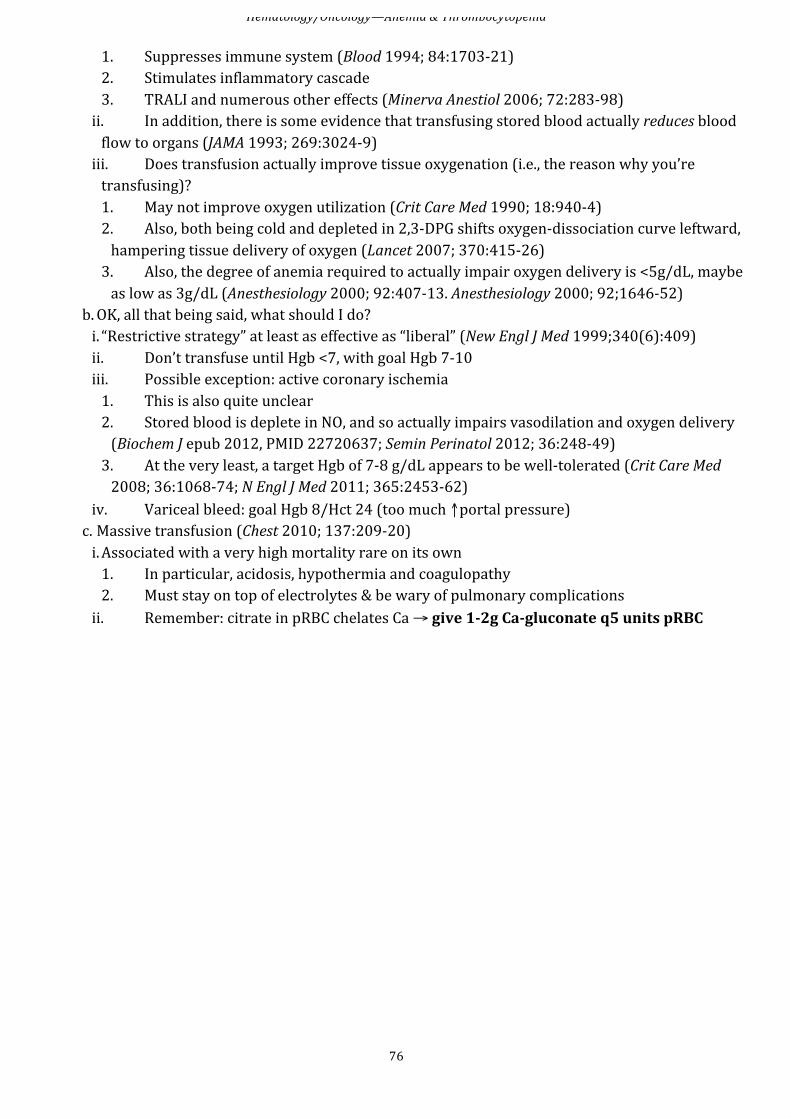
Hematology/Oncology—Anemia & Thrombocytopenia
76
1. Suppresses immune system (Blood 1994; 84:1703-‐21) 2. Stimulates inflammatory cascade 3. TRALI and numerous other effects (Minerva Anestiol 2006; 72:283-‐98) ii. In addition, there is some evidence that transfusing stored blood actually reduces blood flow to organs (JAMA 1993; 269:3024-‐9) iii. Does transfusion actually improve tissue oxygenation (i.e., the reason why you’re transfusing)? 1. May not improve oxygen utilization (Crit Care Med 1990; 18:940-‐4) 2. Also, both being cold and depleted in 2,3-‐DPG shifts oxygen-‐dissociation curve leftward, hampering tissue delivery of oxygen (Lancet 2007; 370:415-‐26) 3. Also, the degree of anemia required to actually impair oxygen delivery is <5g/dL, maybe as low as 3g/dL (Anesthesiology 2000; 92:407-‐13. Anesthesiology 2000; 92;1646-‐52)
b. OK, all that being said, what should I do? i. “Restrictive strategy” at least as effective as “liberal” (New Engl J Med 1999;340(6):409) ii. Don’t transfuse until Hgb <7, with goal Hgb 7-‐10 iii. Possible exception: active coronary ischemia 1. This is also quite unclear 2. Stored blood is deplete in NO, and so actually impairs vasodilation and oxygen delivery (Biochem J epub 2012, PMID 22720637; Semin Perinatol 2012; 36:248-‐49) 3. At the very least, a target Hgb of 7-‐8 g/dL appears to be well-‐tolerated (Crit Care Med 2008; 36:1068-‐74; N Engl J Med 2011; 365:2453-‐62)
iv. Variceal bleed: goal Hgb 8/Hct 24 (too much ↑portal pressure) c. Massive transfusion (Chest 2010; 137:209-‐20) i. Associated with a very high mortality rare on its own 1. In particular, acidosis, hypothermia and coagulopathy 2. Must stay on top of electrolytes & be wary of pulmonary complications ii. Remember: citrate in pRBC chelates Ca → give 1-‐2g Ca-‐gluconate q5 units pRBC
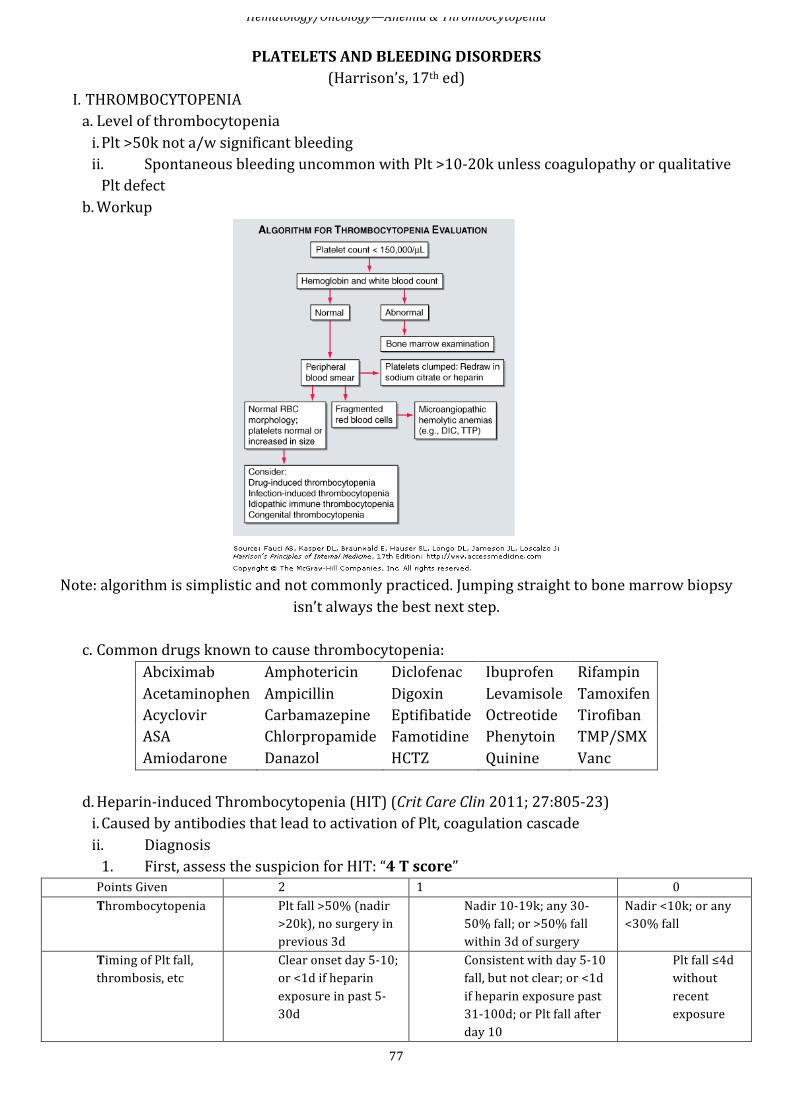
Hematology/Oncology—Anemia & Thrombocytopenia
77
PLATELETS AND BLEEDING DISORDERS (Harrison’s, 17th ed)
I. THROMBOCYTOPENIA a. Level of thrombocytopenia i. Plt >50k not a/w significant bleeding ii. Spontaneous bleeding uncommon with Plt >10-‐20k unless coagulopathy or qualitative Plt defect
b. Workup
Note: algorithm is simplistic and not commonly practiced. Jumping straight to bone marrow biopsy
isn’t always the best next step.
c. Common drugs known to cause thrombocytopenia: Abciximab Amphotericin Diclofenac Ibuprofen Rifampin Acetaminophen Ampicillin Digoxin Levamisole Tamoxifen Acyclovir Carbamazepine Eptifibatide Octreotide Tirofiban ASA Chlorpropamide Famotidine Phenytoin TMP/SMX Amiodarone Danazol HCTZ Quinine Vanc
d. Heparin-‐induced Thrombocytopenia (HIT) (Crit Care Clin 2011; 27:805-‐23) i. Caused by antibodies that lead to activation of Plt, coagulation cascade ii. Diagnosis 1. First, assess the suspicion for HIT: “4 T score” Points Given 2 1 0 Thrombocytopenia Plt fall >50% (nadir
>20k), no surgery in previous 3d
Nadir 10-‐19k; any 30-‐50% fall; or >50% fall within 3d of surgery
Nadir <10k; or any <30% fall
Timing of Plt fall, thrombosis, etc
Clear onset day 5-‐10; or <1d if heparin exposure in past 5-‐30d
Consistent with day 5-‐10 fall, but not clear; or <1d if heparin exposure past 31-‐100d; or Plt fall after day 10
Plt fall ≤4d without recent exposure
Hematology/Oncology—Anemia & Thrombocytopenia
78
Thrombosis or other sequelae
New proven thrombosis, skin necrosis, anaphylaxis after IV bolus; adrenal hemorrhage
Progressive or recurrent thrombosis; erythematous skin lesions; suspected thrombosis
None
Other cause of ↓Plt not evident
No other cause evident
Possible other cause evident
Definite other cause is present
a. Interpretation of score: i. High: 6-‐8 ii. Intermediate: 4-‐5 iii. Low: 0-‐3 b. Should have intermediate or high suspicion to send assay 2. Then send serotonin release assay (include the 4T score in the order comments to expedite)
iii. Treatment/Management 1. Stop and avoid all heparin 2. Use non-‐heparin anticoagulant (e.g., bivalirudin, dabigatran, etc.) a. Because HIT is a hypercoaguable state, may need initial therapeutic dosing b. This is controversial 3. Avoid/postpone warfarin therapy 4. Test for HIT Ab (above) 5. Image to look for clot 6. Avoid Plt transfusions
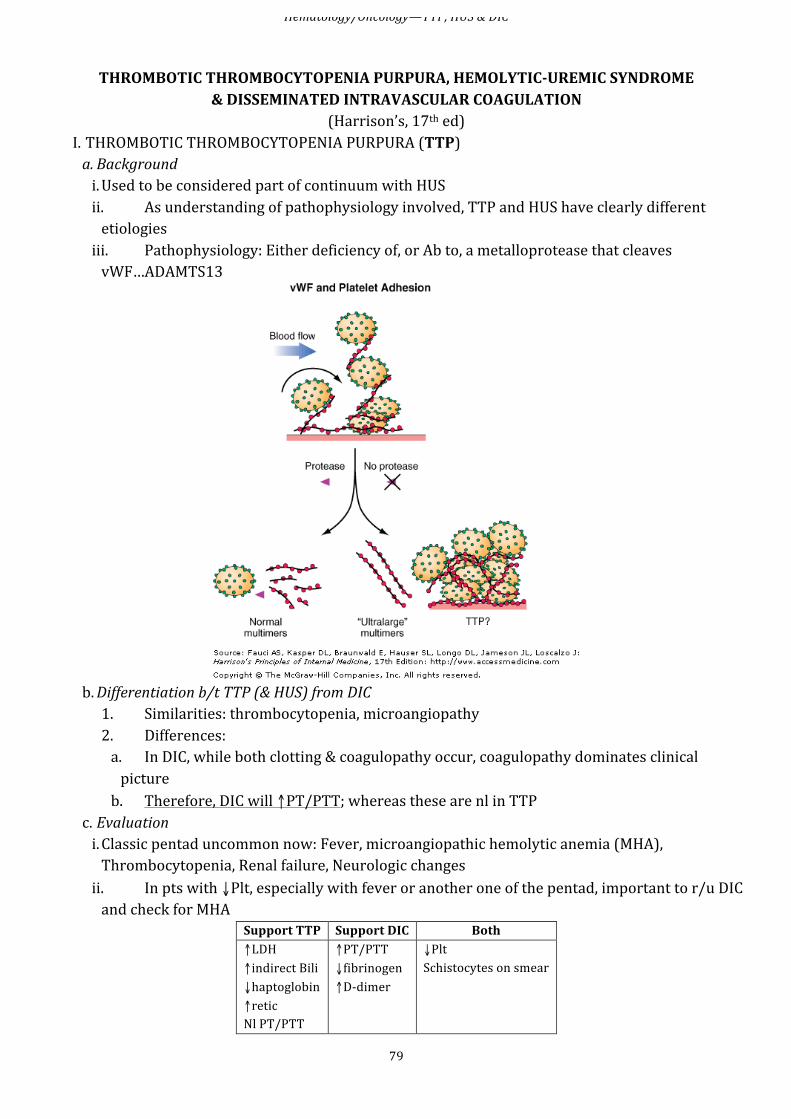
Hematology/Oncology—TTP, HUS & DIC
79
THROMBOTIC THROMBOCYTOPENIA PURPURA, HEMOLYTIC-‐UREMIC SYNDROME
& DISSEMINATED INTRAVASCULAR COAGULATION (Harrison’s, 17th ed)
I. THROMBOTIC THROMBOCYTOPENIA PURPURA (TTP) a. Background i. Used to be considered part of continuum with HUS ii. As understanding of pathophysiology involved, TTP and HUS have clearly different etiologies iii. Pathophysiology: Either deficiency of, or Ab to, a metalloprotease that cleaves vWF…ADAMTS13
b. Differentiation b/t TTP (& HUS) from DIC 1. Similarities: thrombocytopenia, microangiopathy 2. Differences: a. In DIC, while both clotting & coagulopathy occur, coagulopathy dominates clinical picture b. Therefore, DIC will ↑PT/PTT; whereas these are nl in TTP
c. Evaluation i. Classic pentad uncommon now: Fever, microangiopathic hemolytic anemia (MHA), Thrombocytopenia, Renal failure, Neurologic changes ii. In pts with ↓Plt, especially with fever or another one of the pentad, important to r/u DIC and check for MHA
Support TTP Support DIC Both ↑LDH ↑indirect Bili ↓haptoglobin ↑retic Nl PT/PTT
↑PT/PTT ↓fibrinogen ↑D-‐dimer
↓Plt Schistocytes on smear
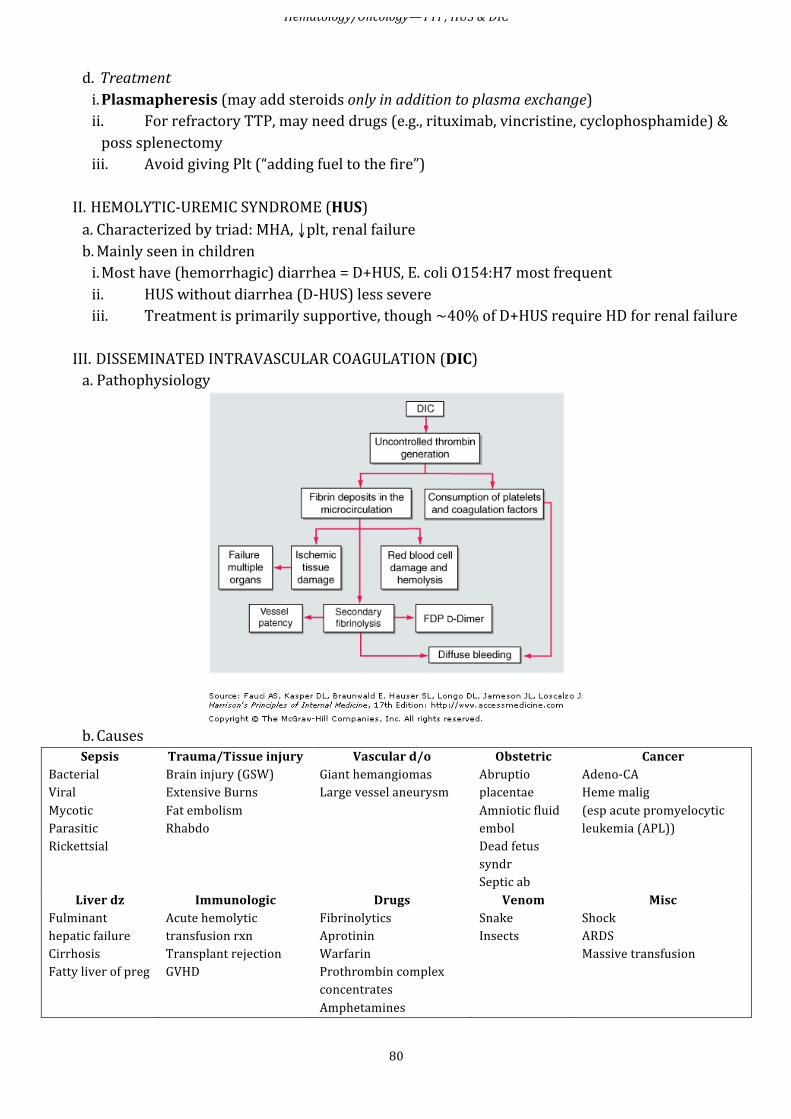
Hematology/Oncology—TTP, HUS & DIC
80
d. Treatment i. Plasmapheresis (may add steroids only in addition to plasma exchange) ii. For refractory TTP, may need drugs (e.g., rituximab, vincristine, cyclophosphamide) & poss splenectomy iii. Avoid giving Plt (“adding fuel to the fire”)
II. HEMOLYTIC-‐UREMIC SYNDROME (HUS) a. Characterized by triad: MHA, ↓plt, renal failure b. Mainly seen in children i. Most have (hemorrhagic) diarrhea = D+HUS, E. coli O154:H7 most frequent ii. HUS without diarrhea (D-‐HUS) less severe iii. Treatment is primarily supportive, though ~40% of D+HUS require HD for renal failure
III. DISSEMINATED INTRAVASCULAR COAGULATION (DIC) a. Pathophysiology
b. Causes Sepsis
Bacterial Viral Mycotic Parasitic Rickettsial
Trauma/Tissue injury Brain injury (GSW) Extensive Burns Fat embolism Rhabdo
Vascular d/o Giant hemangiomas Large vessel aneurysm
Obstetric Abruptio placentae Amniotic fluid embol Dead fetus syndr Septic ab
Cancer Adeno-‐CA Heme malig (esp acute promyelocytic leukemia (APL))
Liver dz Fulminant hepatic failure Cirrhosis Fatty liver of preg
Immunologic Acute hemolytic transfusion rxn Transplant rejection GVHD
Drugs Fibrinolytics Aprotinin Warfarin Prothrombin complex concentrates Amphetamines
Venom Snake Insects
Misc Shock ARDS Massive transfusion
Hematology/Oncology—TTP, HUS & DIC
81
c. Evaluation i. “DIC screen order set” order: has PT/PTT, fibrinogen, D-‐dimer ii. See above for labs in DIC vs TTP d. Treatment i. Treat underlying disorder ii. Bleeding management 1. Give FFP to ↓INR 2. If ↓fibrinogen, give cryoprecipitate (10U of cryo for every 2-‐3U FFP) 3. If Plt <20-‐30k, give 1-‐2U/10kg Plt transfusion 4. Clotting factor concentrates not recommended iii. Clotting management 1. Heparin a. In acute DIC, heparin likely to aggravate bleeding sx b. Low dose heparin gtt (5-‐10U/kg/h) may be effective in: i. Low-‐grade DIC a/w solid tumor or APL or recognized thrombosis ii. Also used in purpura fulminans, resection of giant hemangiomas, removal of dead fetus 2. Activing protein C (APC) may be used for purpura fulminans in acquired protein C deficiency or meningococcemia 3. Antithrombin III is another option 4. Antifibrinolytics, EACA, or tranexemic acid to prevent fibrin degradation may ↓bleeding in pts with DIC & confirmed fibrinolysis a. Since ↑r/o thrombosis, also need heparin gtt b. Use mainly limited to APL or chronic DIC from giant hemangiomas
REVERSING COAGULOPATHY Problem Solution Starting Dose Amount Correction
↑INR FFP (± vit K)
FFP: 2 units Vit K: 5mg PO/IV
INR Mean INR Change per FFP Unit1
1.3-‐1.7
0.1
1.7-‐2.3
0.2
2.4-‐2.9
0.4
3-‐4.3 0.7 4.4-‐20
3.5
↓Plt Plt transfusion 1 unit (= one 6-‐pk) ↑Plt 5-‐10k per unit2 ↓Fibrinogen Cryoprecipitate 10 units Uremia / VW disease DDAVP ~30mcg IV x1
1 http://www.clinlabnavigator.com/transfusion/Flash/FreshFrozenPlasma.swf 2 http://www.scbcinfo.org/publications/bulletin_v2_n2.htm
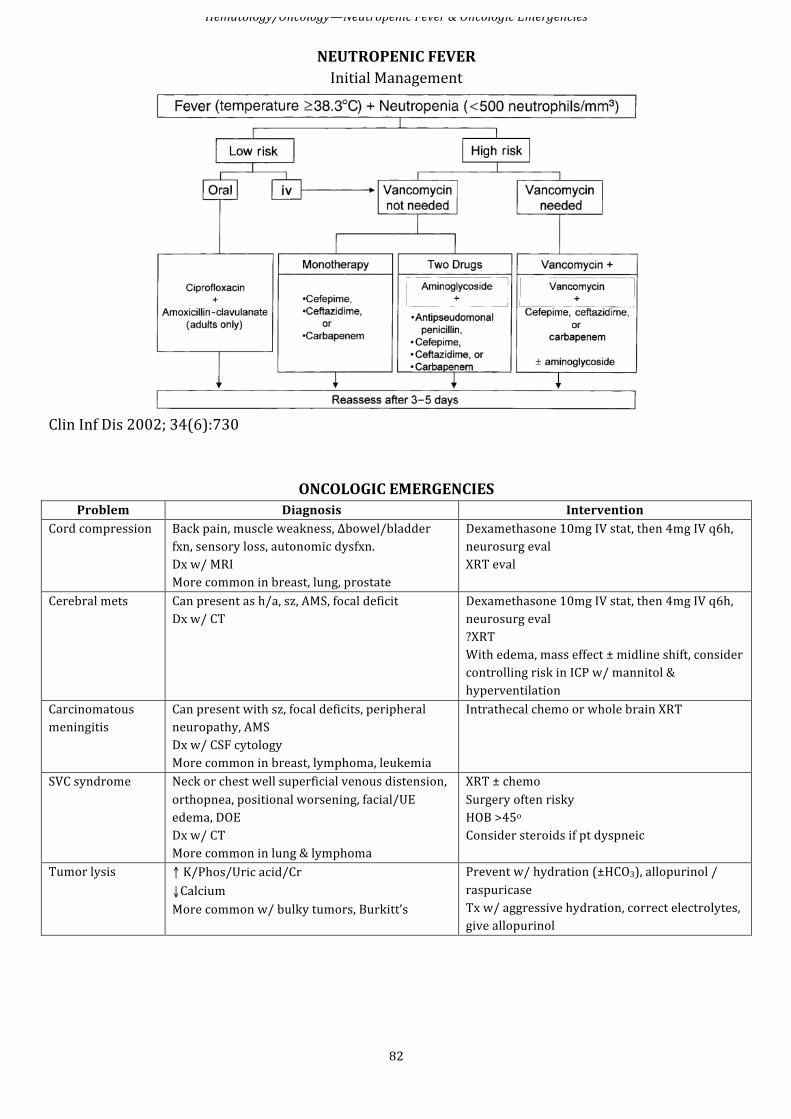
Hematology/Oncology—Neutropenic Fever & Oncologic Emergencies
82
NEUTROPENIC FEVER Initial Management
Clin Inf Dis 2002; 34(6):730
ONCOLOGIC EMERGENCIES Problem Diagnosis Intervention
Cord compression Back pain, muscle weakness, Δbowel/bladder fxn, sensory loss, autonomic dysfxn. Dx w/ MRI More common in breast, lung, prostate
Dexamethasone 10mg IV stat, then 4mg IV q6h, neurosurg eval XRT eval
Cerebral mets Can present as h/a, sz, AMS, focal deficit Dx w/ CT
Dexamethasone 10mg IV stat, then 4mg IV q6h, neurosurg eval ?XRT With edema, mass effect ± midline shift, consider controlling risk in ICP w/ mannitol & hyperventilation
Carcinomatous meningitis
Can present with sz, focal deficits, peripheral neuropathy, AMS Dx w/ CSF cytology More common in breast, lymphoma, leukemia
Intrathecal chemo or whole brain XRT
SVC syndrome Neck or chest well superficial venous distension, orthopnea, positional worsening, facial/UE edema, DOE Dx w/ CT More common in lung & lymphoma
XRT ± chemo Surgery often risky HOB >45o Consider steroids if pt dyspneic
Tumor lysis ↑ K/Phos/Uric acid/Cr ↓Calcium More common w/ bulky tumors, Burkitt’s
Prevent w/ hydration (±HCO3), allopurinol / raspuricase Tx w/ aggressive hydration, correct electrolytes, give allopurinol
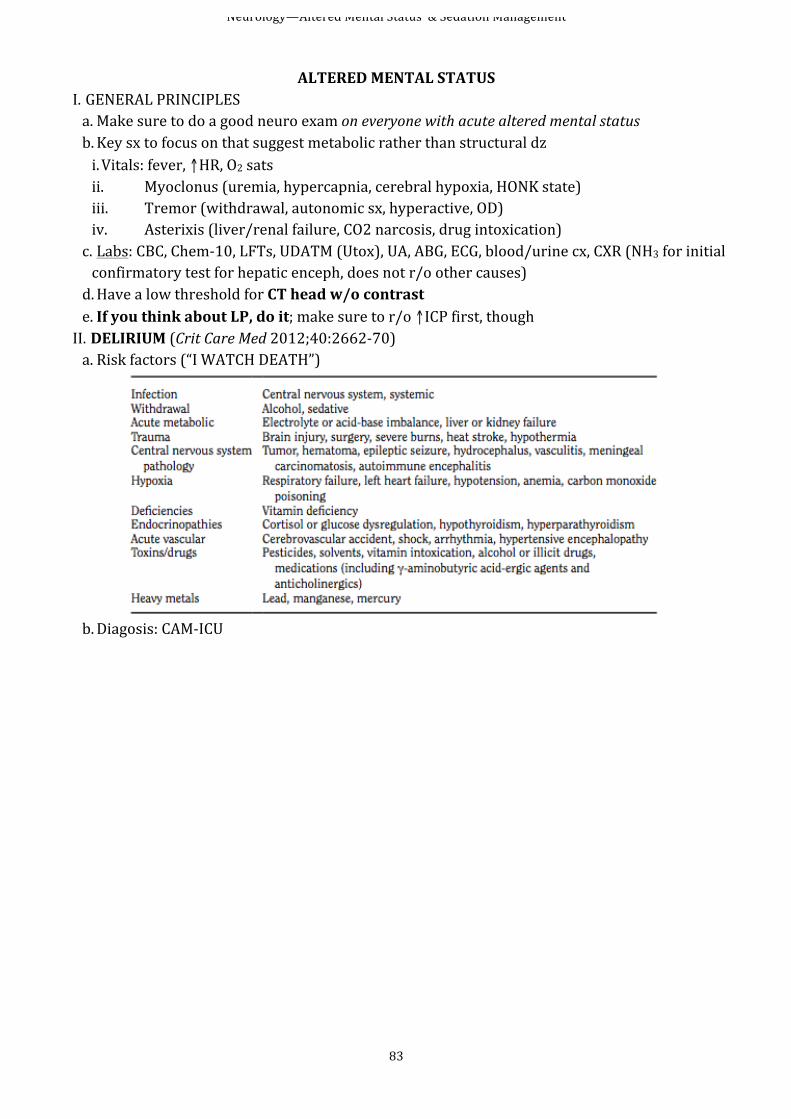
Neurology—Altered Mental Status & Sedation Management
83
ALTERED MENTAL STATUS
I. GENERAL PRINCIPLES a. Make sure to do a good neuro exam on everyone with acute altered mental status b. Key sx to focus on that suggest metabolic rather than structural dz i. Vitals: fever, ↑HR, O2 sats ii. Myoclonus (uremia, hypercapnia, cerebral hypoxia, HONK state) iii. Tremor (withdrawal, autonomic sx, hyperactive, OD) iv. Asterixis (liver/renal failure, CO2 narcosis, drug intoxication) c. Labs: CBC, Chem-‐10, LFTs, UDATM (Utox), UA, ABG, ECG, blood/urine cx, CXR (NH3 for initial confirmatory test for hepatic enceph, does not r/o other causes) d. Have a low threshold for CT head w/o contrast e. If you think about LP, do it; make sure to r/o ↑ICP first, though II. DELIRIUM (Crit Care Med 2012;40:2662-‐70) a. Risk factors (“I WATCH DEATH”)
b. Diagosis: CAM-‐ICU

Neurology—Altered Mental Status & Sedation Management
84
c. Treatment i. Haloperidol is the mainstay of treatment 1. Tends to cause less QTc prolongation than other antipsychotics (Am J Psychiatry 2001; 158:1774-‐82) 2. IV causes less extrapyramidal side effects vs PO/IM ((Drugs 2003; 63:493-‐512) ii. Dexmedetomidine may help if on vent (Crit Care 2009; 13:R75)
SEDATION MANAGEMENT a. Careful with sedation 1. Avoid BZDs as much as possible a. ≥20mg/day of lorazepam virtually guarantees delirium in ICU (Anesthesiology 2006; 104:21-‐6) b. Try only intermittent boluses of BZD if needed, avoid BZD gtt 2. Propofol and dexmedetomidine drips preferred a. Both have drawbacks of hypotension b. Dexmedetomidine is very costly
b. Minimize anticholinergies c. Manage pain i. Not all opioids are alike ii. Morphine not very deliriogenic iii. Meperidine and tramadol are much worse iv. Again, intermittent boluses are vastly preferred to continuous drips d. Promote normal sleep-‐wake cycle i. Do not “snow” pts at night: this Is not the same as sleep!
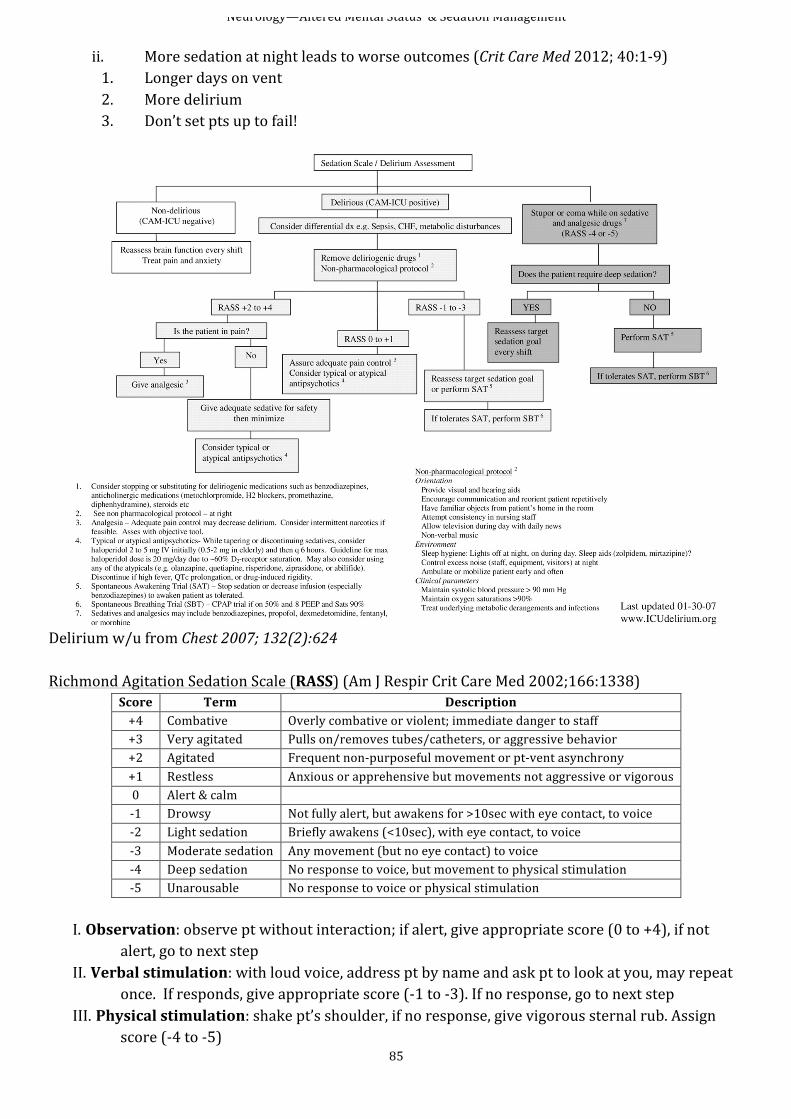
Neurology—Altered Mental Status & Sedation Management
85
ii. More sedation at night leads to worse outcomes (Crit Care Med 2012; 40:1-‐9) 1. Longer days on vent 2. More delirium 3. Don’t set pts up to fail!
Delirium w/u from Chest 2007; 132(2):624 Richmond Agitation Sedation Scale (RASS) (Am J Respir Crit Care Med 2002;166:1338)
Score Term Description +4 Combative Overly combative or violent; immediate danger to staff +3 Very agitated Pulls on/removes tubes/catheters, or aggressive behavior +2 Agitated Frequent non-‐purposeful movement or pt-‐vent asynchrony +1 Restless Anxious or apprehensive but movements not aggressive or vigorous 0 Alert & calm -‐1 Drowsy Not fully alert, but awakens for >10sec with eye contact, to voice -‐2 Light sedation Briefly awakens (<10sec), with eye contact, to voice -‐3 Moderate sedation Any movement (but no eye contact) to voice -‐4 Deep sedation No response to voice, but movement to physical stimulation -‐5 Unarousable No response to voice or physical stimulation
I. Observation: observe pt without interaction; if alert, give appropriate score (0 to +4), if not
alert, go to next step II. Verbal stimulation: with loud voice, address pt by name and ask pt to look at you, may repeat
once. If responds, give appropriate score (-‐1 to -‐3). If no response, go to next step III. Physical stimulation: shake pt’s shoulder, if no response, give vigorous sternal rub. Assign
score (-‐4 to -‐5)
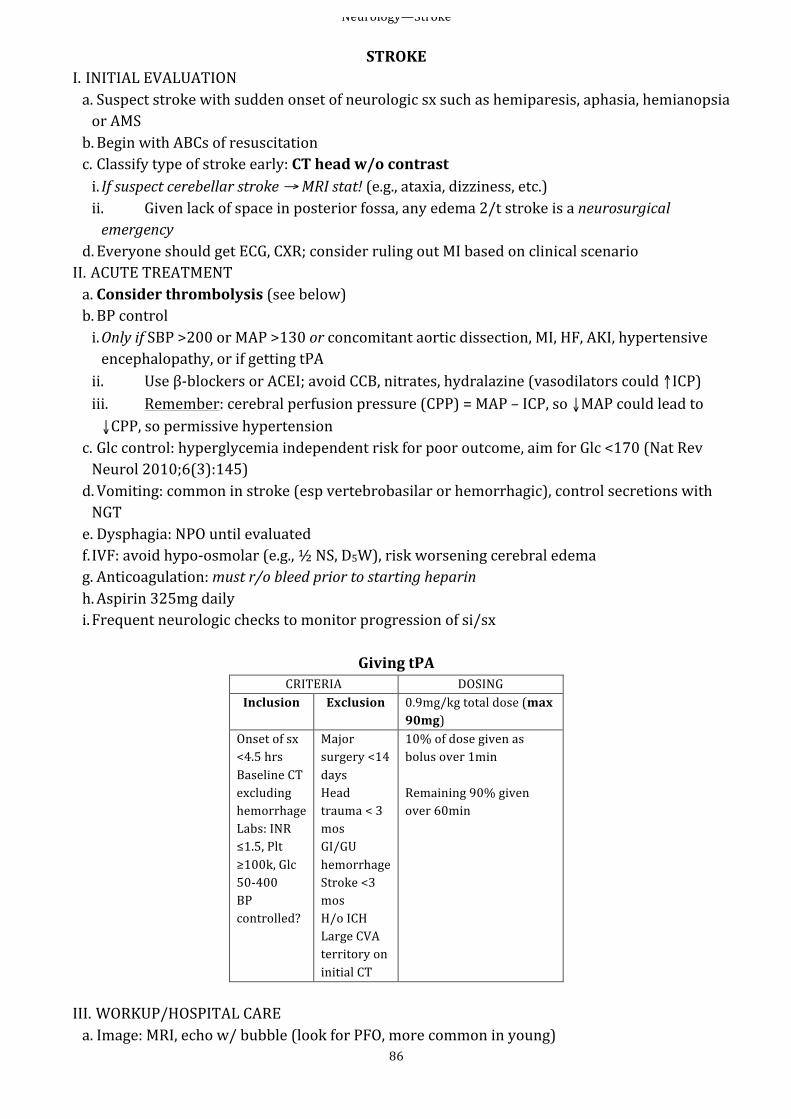
Neurology—Stroke
86
STROKE I. INITIAL EVALUATION a. Suspect stroke with sudden onset of neurologic sx such as hemiparesis, aphasia, hemianopsia or AMS b. Begin with ABCs of resuscitation c. Classify type of stroke early: CT head w/o contrast i. If suspect cerebellar stroke → MRI stat! (e.g., ataxia, dizziness, etc.) ii. Given lack of space in posterior fossa, any edema 2/t stroke is a neurosurgical emergency
d. Everyone should get ECG, CXR; consider ruling out MI based on clinical scenario II. ACUTE TREATMENT a. Consider thrombolysis (see below) b. BP control i. Only if SBP >200 or MAP >130 or concomitant aortic dissection, MI, HF, AKI, hypertensive encephalopathy, or if getting tPA ii. Use β-‐blockers or ACEI; avoid CCB, nitrates, hydralazine (vasodilators could ↑ICP) iii. Remember: cerebral perfusion pressure (CPP) = MAP – ICP, so ↓MAP could lead to ↓CPP, so permissive hypertension
c. Glc control: hyperglycemia independent risk for poor outcome, aim for Glc <170 (Nat Rev Neurol 2010;6(3):145) d. Vomiting: common in stroke (esp vertebrobasilar or hemorrhagic), control secretions with NGT e. Dysphagia: NPO until evaluated f. IVF: avoid hypo-‐osmolar (e.g., ½ NS, D5W), risk worsening cerebral edema g. Anticoagulation: must r/o bleed prior to starting heparin h. Aspirin 325mg daily i. Frequent neurologic checks to monitor progression of si/sx
Giving tPA
CRITERIA DOSING Inclusion Exclusion 0.9mg/kg total dose (max
90mg) Onset of sx <4.5 hrs Baseline CT excluding hemorrhage Labs: INR ≤1.5, Plt ≥100k, Glc 50-‐400 BP controlled?
Major surgery <14 days Head trauma < 3 mos GI/GU hemorrhage Stroke <3 mos H/o ICH Large CVA territory on initial CT
10% of dose given as bolus over 1min Remaining 90% given over 60min
III. WORKUP/HOSPITAL CARE a. Image: MRI, echo w/ bubble (look for PFO, more common in young)
Neurology—Stroke
87
b. Fasting lipid panel c. PT/OT, consider speech for swallow eval d. Remember, half of deaths d/t stroke are 2/t medical complications i. W/u fever aggressively, give anti-‐pyretics ii. Sz occur in ~5% of ischemic stroke iii. Prevent DVT, PE, PNA (e.g,, ↑HOB), UTI, decub ulcers
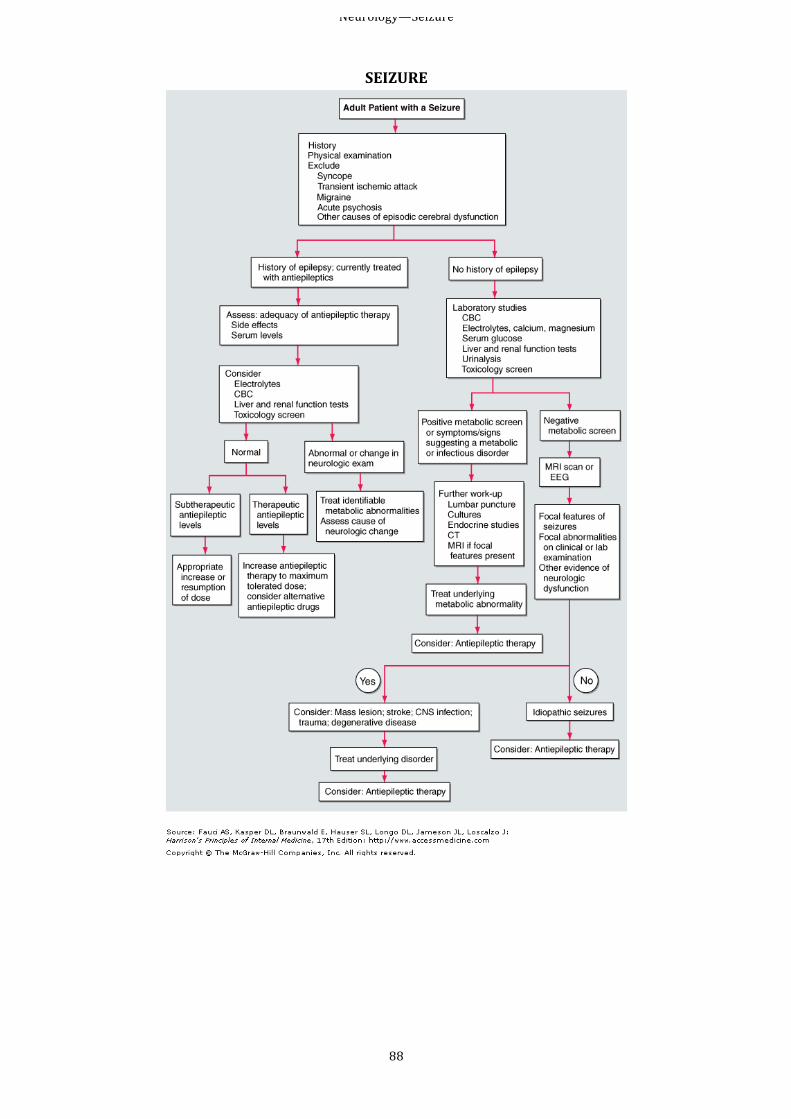
Neurology—Seizure
88
SEIZURE
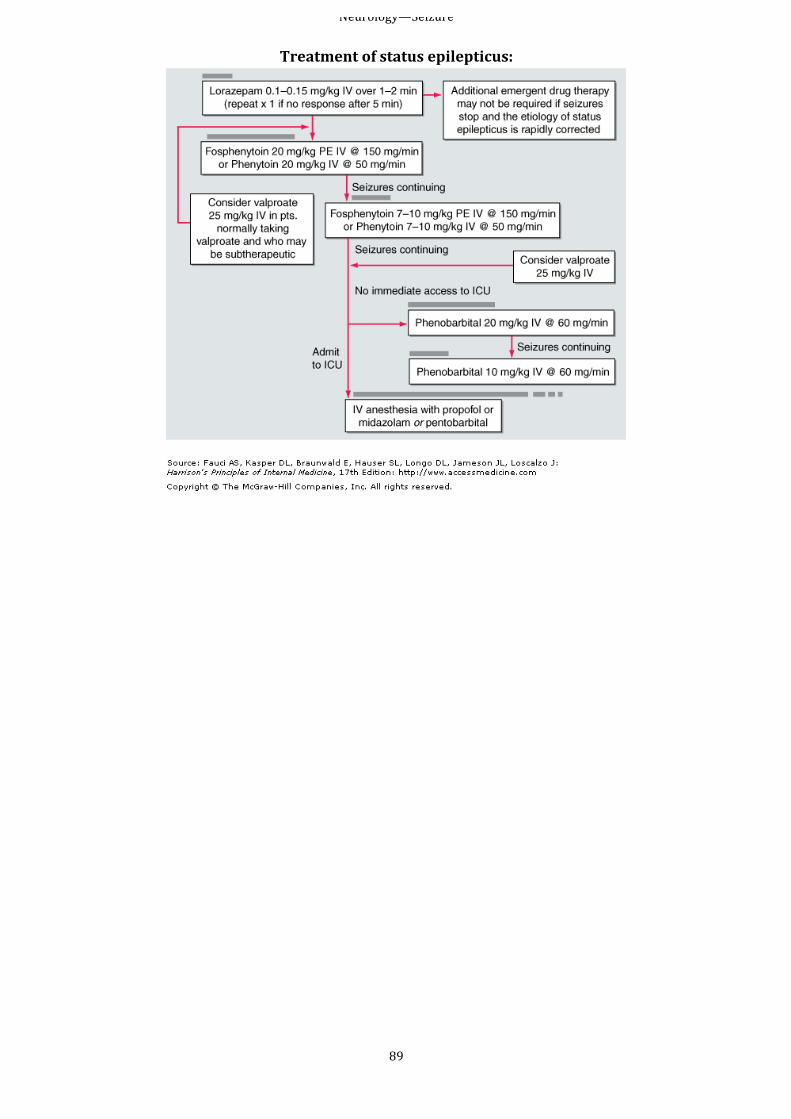
Neurology—Seizure
89
Treatment of status epilepticus:
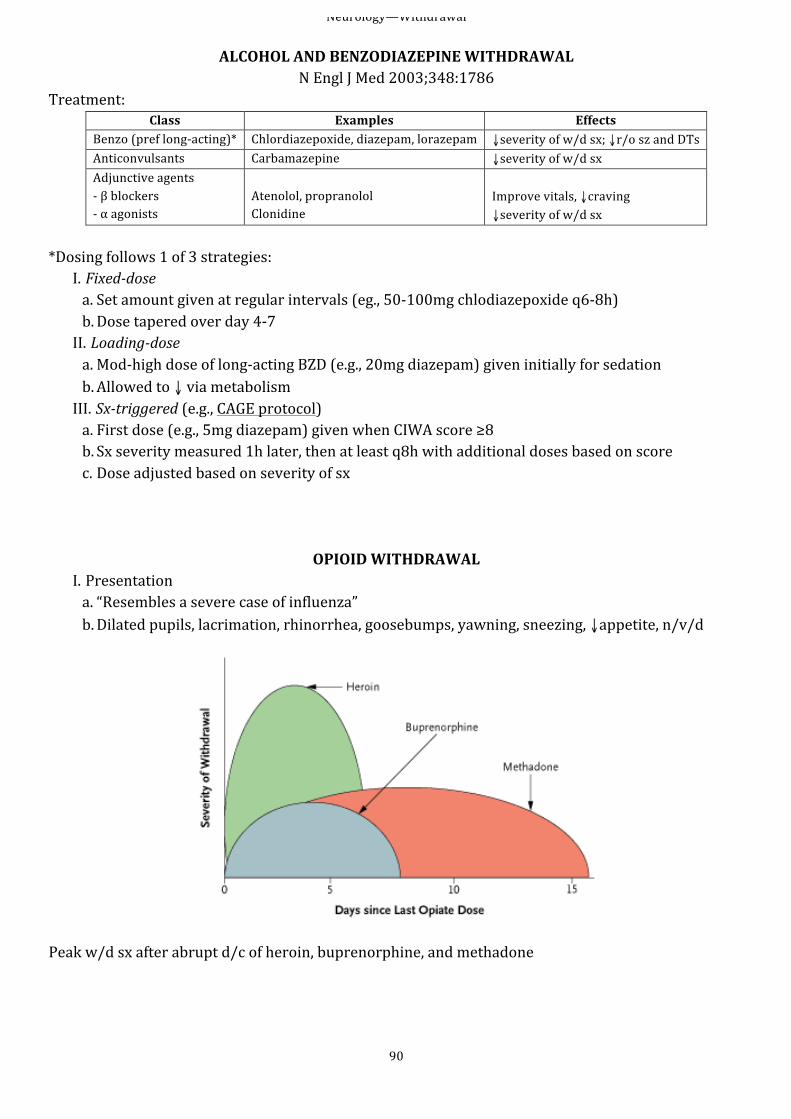
Neurology—Withdrawal
90
ALCOHOL AND BENZODIAZEPINE WITHDRAWAL N Engl J Med 2003;348:1786
Treatment: Class Examples Effects
Benzo (pref long-‐acting)* Chlordiazepoxide, diazepam, lorazepam ↓severity of w/d sx; ↓r/o sz and DTs Anticonvulsants Carbamazepine ↓severity of w/d sx Adjunctive agents -‐ β blockers -‐ α agonists
Atenolol, propranolol Clonidine
Improve vitals, ↓craving ↓severity of w/d sx
*Dosing follows 1 of 3 strategies:
I. Fixed-‐dose a. Set amount given at regular intervals (eg., 50-‐100mg chlodiazepoxide q6-‐8h) b. Dose tapered over day 4-‐7 II. Loading-‐dose a. Mod-‐high dose of long-‐acting BZD (e.g., 20mg diazepam) given initially for sedation b. Allowed to ↓ via metabolism III. Sx-‐triggered (e.g., CAGE protocol) a. First dose (e.g., 5mg diazepam) given when CIWA score ≥8 b. Sx severity measured 1h later, then at least q8h with additional doses based on score c. Dose adjusted based on severity of sx
OPIOID WITHDRAWAL I. Presentation a. “Resembles a severe case of influenza” b. Dilated pupils, lacrimation, rhinorrhea, goosebumps, yawning, sneezing, ↓appetite, n/v/d
Peak w/d sx after abrupt d/c of heroin, buprenorphine, and methadone
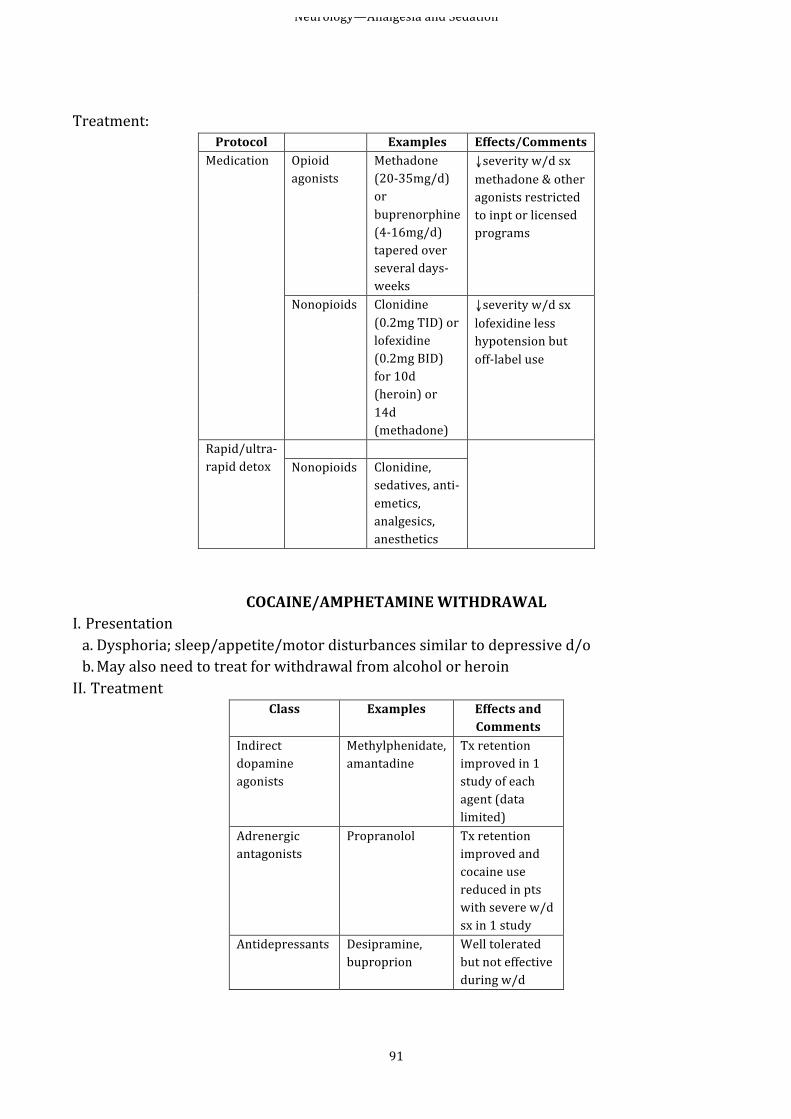
Neurology—Analgesia and Sedation
91
Treatment:
Protocol Examples Effects/Comments Medication Opioid
agonists Methadone (20-‐35mg/d) or buprenorphine (4-‐16mg/d) tapered over several days-‐weeks
↓severity w/d sx methadone & other agonists restricted to inpt or licensed programs
Nonopioids Clonidine (0.2mg TID) or lofexidine (0.2mg BID) for 10d (heroin) or 14d (methadone)
↓severity w/d sx lofexidine less hypotension but off-‐label use
Rapid/ultra-‐rapid detox
Nonopioids Clonidine,
sedatives, anti-‐emetics, analgesics, anesthetics
COCAINE/AMPHETAMINE WITHDRAWAL I. Presentation a. Dysphoria; sleep/appetite/motor disturbances similar to depressive d/o b. May also need to treat for withdrawal from alcohol or heroin II. Treatment
Class Examples Effects and Comments
Indirect dopamine agonists
Methylphenidate, amantadine
Tx retention improved in 1 study of each agent (data limited)
Adrenergic antagonists
Propranolol Tx retention improved and cocaine use reduced in pts with severe w/d sx in 1 study
Antidepressants Desipramine, buproprion
Well tolerated but not effective during w/d
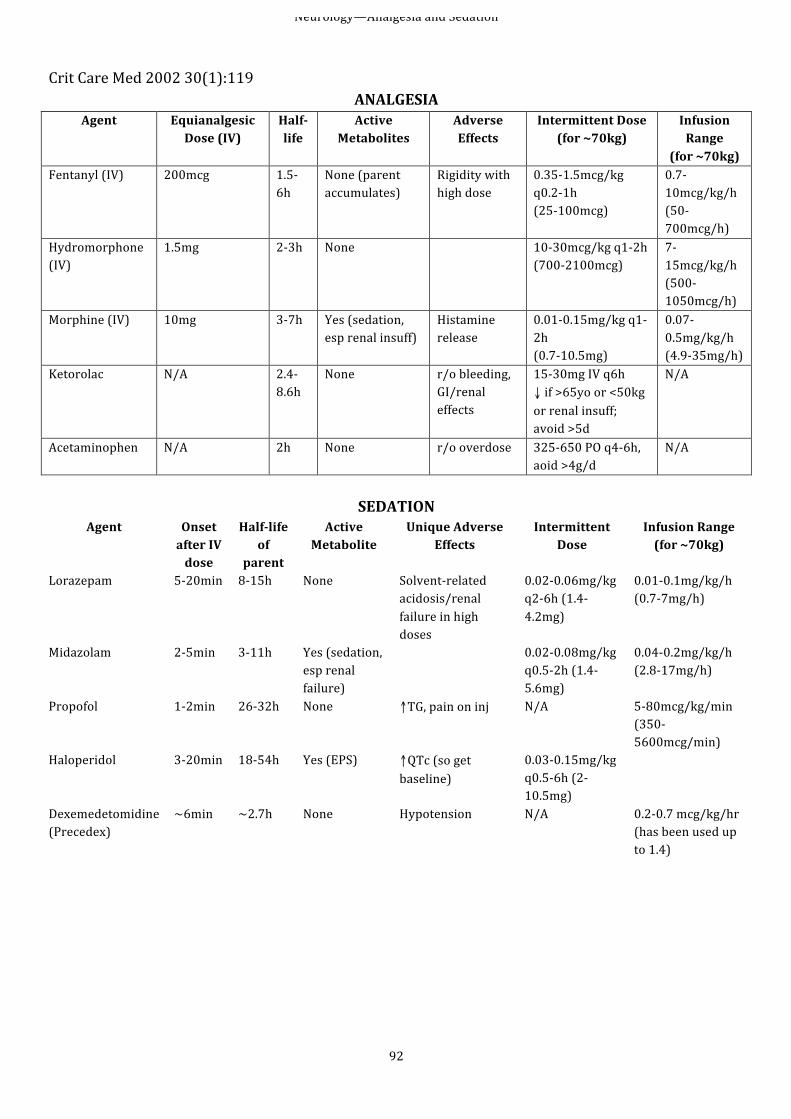
Neurology—Analgesia and Sedation
92
Crit Care Med 2002 30(1):119
ANALGESIA Agent Equianalgesic
Dose (IV) Half-‐life
Active Metabolites
Adverse Effects
Intermittent Dose (for ~70kg)
Infusion Range
(for ~70kg) Fentanyl (IV) 200mcg 1.5-‐
6h None (parent accumulates)
Rigidity with high dose
0.35-‐1.5mcg/kg q0.2-‐1h (25-‐100mcg)
0.7-‐10mcg/kg/h (50-‐700mcg/h)
Hydromorphone (IV)
1.5mg 2-‐3h None 10-‐30mcg/kg q1-‐2h (700-‐2100mcg)
7-‐15mcg/kg/h (500-‐1050mcg/h)
Morphine (IV) 10mg 3-‐7h Yes (sedation, esp renal insuff)
Histamine release
0.01-‐0.15mg/kg q1-‐2h (0.7-‐10.5mg)
0.07-‐0.5mg/kg/h (4.9-‐35mg/h)
Ketorolac N/A 2.4-‐8.6h
None r/o bleeding, GI/renal effects
15-‐30mg IV q6h ↓ if >65yo or <50kg or renal insuff; avoid >5d
N/A
Acetaminophen N/A 2h None r/o overdose 325-‐650 PO q4-‐6h, aoid >4g/d
N/A
SEDATION
Agent Onset after IV dose
Half-‐life of
parent
Active Metabolite
Unique Adverse Effects
Intermittent Dose
Infusion Range (for ~70kg)
Lorazepam 5-‐20min 8-‐15h None Solvent-‐related acidosis/renal failure in high doses
0.02-‐0.06mg/kg q2-‐6h (1.4-‐4.2mg)
0.01-‐0.1mg/kg/h (0.7-‐7mg/h)
Midazolam 2-‐5min 3-‐11h Yes (sedation, esp renal failure)
0.02-‐0.08mg/kg q0.5-‐2h (1.4-‐5.6mg)
0.04-‐0.2mg/kg/h (2.8-‐17mg/h)
Propofol 1-‐2min 26-‐32h None ↑TG, pain on inj N/A 5-‐80mcg/kg/min (350-‐5600mcg/min)
Haloperidol 3-‐20min 18-‐54h Yes (EPS) ↑QTc (so get baseline)
0.03-‐0.15mg/kg q0.5-‐6h (2-‐10.5mg)
Dexemedetomidine (Precedex)
~6min ~2.7h None Hypotension N/A 0.2-‐0.7 mcg/kg/hr (has been used up to 1.4)
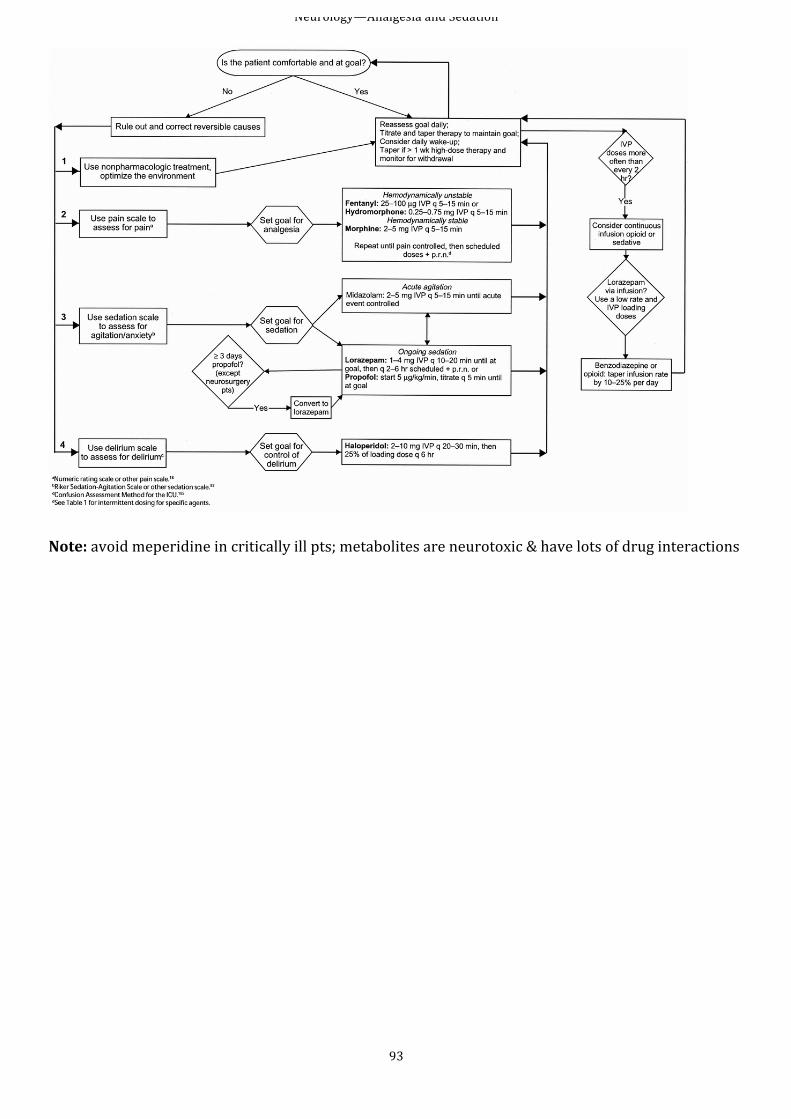
Neurology—Analgesia and Sedation
93
Note: avoid meperidine in critically ill pts; metabolites are neurotoxic & have lots of drug interactions
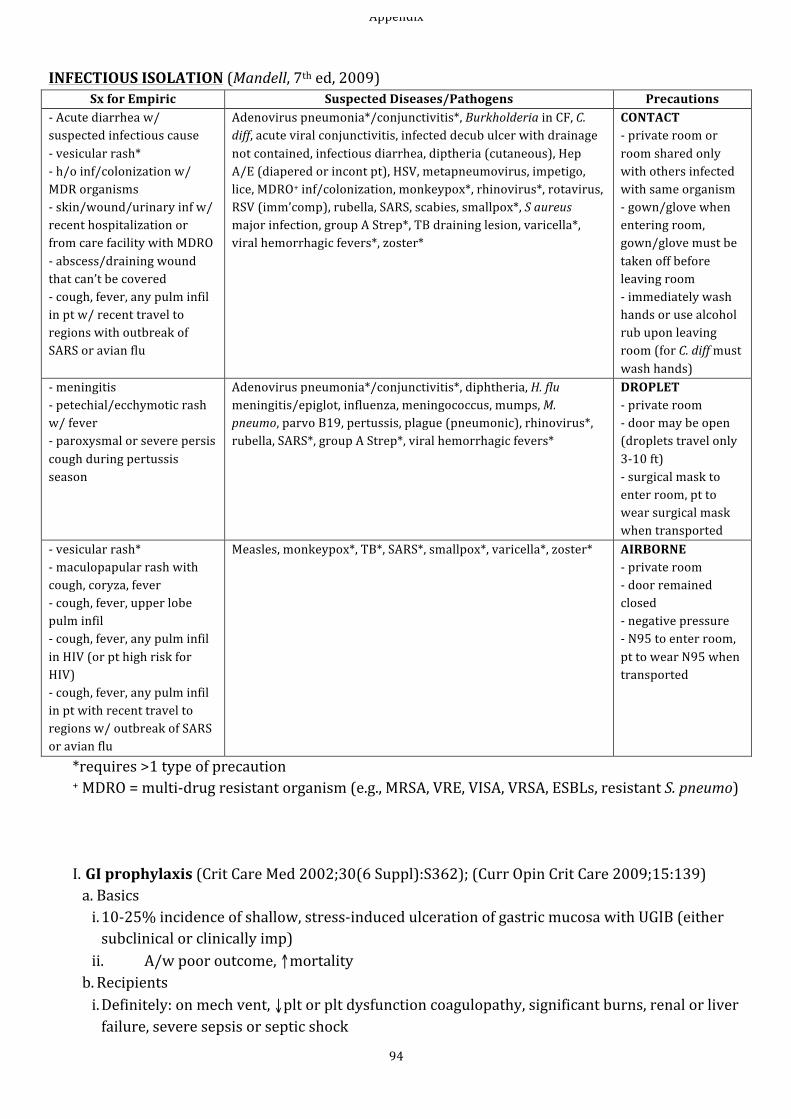
Appendix
94
INFECTIOUS ISOLATION (Mandell, 7th ed, 2009)
Sx for Empiric Suspected Diseases/Pathogens Precautions -‐ Acute diarrhea w/ suspected infectious cause -‐ vesicular rash* -‐ h/o inf/colonization w/ MDR organisms -‐ skin/wound/urinary inf w/ recent hospitalization or from care facility with MDRO -‐ abscess/draining wound that can’t be covered -‐ cough, fever, any pulm infil in pt w/ recent travel to regions with outbreak of SARS or avian flu
Adenovirus pneumonia*/conjunctivitis*, Burkholderia in CF, C. diff, acute viral conjunctivitis, infected decub ulcer with drainage not contained, infectious diarrhea, diptheria (cutaneous), Hep A/E (diapered or incont pt), HSV, metapneumovirus, impetigo, lice, MDRO+ inf/colonization, monkeypox*, rhinovirus*, rotavirus, RSV (imm’comp), rubella, SARS, scabies, smallpox*, S aureus major infection, group A Strep*, TB draining lesion, varicella*, viral hemorrhagic fevers*, zoster*
CONTACT -‐ private room or room shared only with others infected with same organism -‐ gown/glove when entering room, gown/glove must be taken off before leaving room -‐ immediately wash hands or use alcohol rub upon leaving room (for C. diff must wash hands)
-‐ meningitis -‐ petechial/ecchymotic rash w/ fever -‐ paroxysmal or severe persis cough during pertussis season
Adenovirus pneumonia*/conjunctivitis*, diphtheria, H. flu meningitis/epiglot, influenza, meningococcus, mumps, M. pneumo, parvo B19, pertussis, plague (pneumonic), rhinovirus*, rubella, SARS*, group A Strep*, viral hemorrhagic fevers*
DROPLET -‐ private room -‐ door may be open (droplets travel only 3-‐10 ft) -‐ surgical mask to enter room, pt to wear surgical mask when transported
-‐ vesicular rash* -‐ maculopapular rash with cough, coryza, fever -‐ cough, fever, upper lobe pulm infil -‐ cough, fever, any pulm infil in HIV (or pt high risk for HIV) -‐ cough, fever, any pulm infil in pt with recent travel to regions w/ outbreak of SARS or avian flu
Measles, monkeypox*, TB*, SARS*, smallpox*, varicella*, zoster* AIRBORNE -‐ private room -‐ door remained closed -‐ negative pressure -‐ N95 to enter room, pt to wear N95 when transported
*requires >1 type of precaution + MDRO = multi-‐drug resistant organism (e.g., MRSA, VRE, VISA, VRSA, ESBLs, resistant S. pneumo)
I. GI prophylaxis (Crit Care Med 2002;30(6 Suppl):S362); (Curr Opin Crit Care 2009;15:139) a. Basics i. 10-‐25% incidence of shallow, stress-‐induced ulceration of gastric mucosa with UGIB (either subclinical or clinically imp) ii. A/w poor outcome, ↑mortality b. Recipients i. Definitely: on mech vent, ↓plt or plt dysfunction coagulopathy, significant burns, renal or liver failure, severe sepsis or septic shock
Appendix
95
ii. If eating, that is enough for most patients c. Regimens: i. Sucralfate (?↓ r/o PNA, poss less effective) ii. Ranitidine 150mg IV q8-‐12h or famotidine 20mg IV q12h (adjust for renal insuff) iii. Pantoprazole 40mg IV qday for 5-‐7d, then consider Δ to PO pantop or omep
II. VTE prophylaxis (Chest 2001;119(1 Suppl):132S) a. Basics i. Risk of DVT/PE in ICU 15-‐50% w/o some type of prophylaxis ii. Risk ↑ by stasis (immobilization), hypercoaguable state, infection, local venous trauma, etc.
b. Recipients: all pts in ICU c. Regimens: i. No bleeding risk 1. Heparin 5000 SQ q8h (use in renal insuff) 2. Fondaparinux 2.5mg SQ qday (caution in renal insuff) 3. Enoxaparin 40mg SQ qday or 30mg SQ q12h for ortho pt (caution in renal insuff) 4. May also add SCDs ii. Bleeding risk: SCDs
III. VAP prophylaxis (N ENGL J MED 1999; 340(8):627) a. Initiate “VAP bundle” at UNM b. Examples of measures
Non-‐pharmacologic Pharmacologic -‐ Remove NG or ETT as soon as possible -‐ Elevate HOB -‐ Hand-‐washing -‐ Avoid gastric overdistension -‐ Continuous subglottic suctioning (not routinely done at UNM)
-‐ Chlorhexadine oral rinse
IV. Sinusitis prophylaxis (Clin Inf Dis 1997; 25:1441) a. Basics i. Sinusitis common cause of fever in ICU ii. Intubated pts and those with NG tubes predisposed iii. Prophylaxis controversial b. Regimen: i. Saline spray (“Ocean spray”) ii. Nasal steroids (e.g., flunisolide or budesonide) iii. Possibly short-‐term α-‐adrenergic agents (e.g., oxymetazoline)
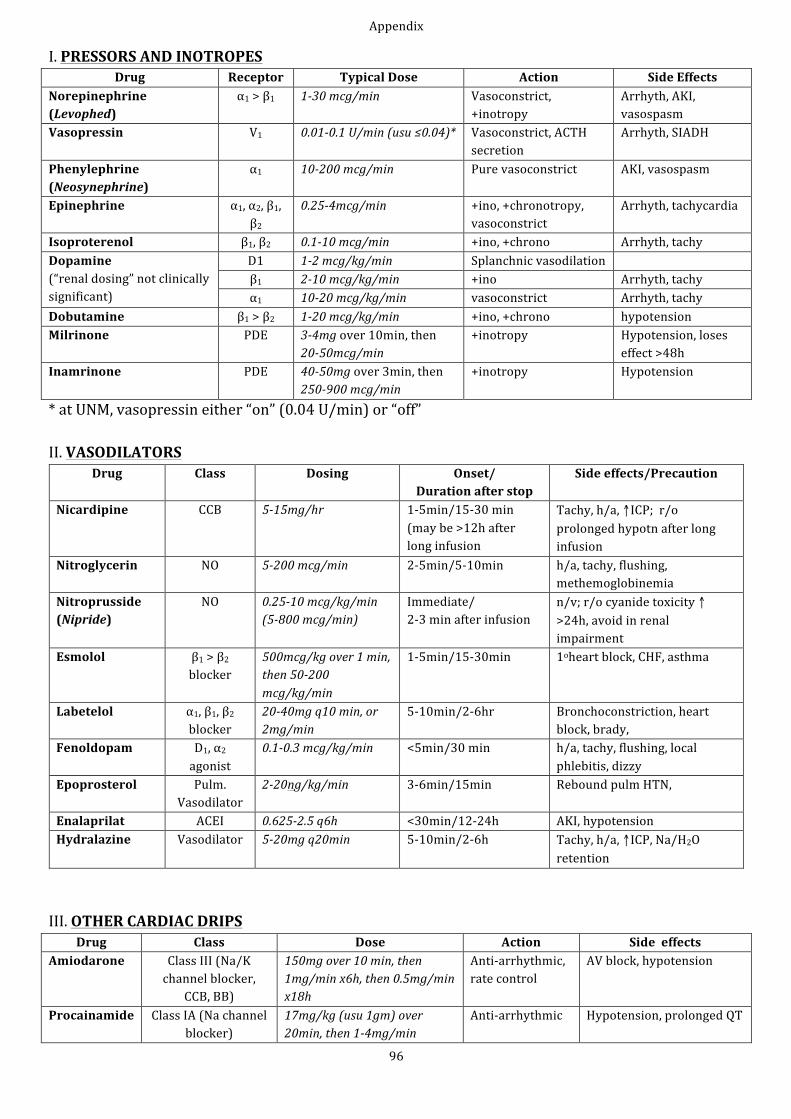
Appendix
96
I. PRESSORS AND INOTROPES Drug Receptor Typical Dose Action Side Effects
Norepinephrine (Levophed)
α1 > β1 1-‐30 mcg/min Vasoconstrict, +inotropy
Arrhyth, AKI, vasospasm
Vasopressin V1 0.01-‐0.1 U/min (usu ≤0.04)* Vasoconstrict, ACTH secretion
Arrhyth, SIADH
Phenylephrine (Neosynephrine)
α1 10-‐200 mcg/min Pure vasoconstrict AKI, vasospasm
Epinephrine α1, α2, β1, β2
0.25-‐4mcg/min +ino, +chronotropy, vasoconstrict
Arrhyth, tachycardia
Isoproterenol β1, β2 0.1-‐10 mcg/min +ino, +chrono Arrhyth, tachy Dopamine (“renal dosing” not clinically significant)
D1 1-‐2 mcg/kg/min Splanchnic vasodilation β1 2-‐10 mcg/kg/min +ino Arrhyth, tachy α1 10-‐20 mcg/kg/min vasoconstrict Arrhyth, tachy
Dobutamine β1 > β2 1-‐20 mcg/kg/min +ino, +chrono hypotension Milrinone PDE 3-‐4mg over 10min, then
20-‐50mcg/min +inotropy Hypotension, loses
effect >48h Inamrinone PDE 40-‐50mg over 3min, then
250-‐900 mcg/min +inotropy Hypotension
* at UNM, vasopressin either “on” (0.04 U/min) or “off” II. VASODILATORS
Drug Class Dosing Onset/ Duration after stop
Side effects/Precaution
Nicardipine CCB 5-‐15mg/hr 1-‐5min/15-‐30 min (may be >12h after long infusion
Tachy, h/a, ↑ICP; r/o prolonged hypotn after long infusion
Nitroglycerin NO 5-‐200 mcg/min 2-‐5min/5-‐10min h/a, tachy, flushing, methemoglobinemia
Nitroprusside (Nipride)
NO 0.25-‐10 mcg/kg/min (5-‐800 mcg/min)
Immediate/ 2-‐3 min after infusion
n/v; r/o cyanide toxicity ↑ >24h, avoid in renal impairment
Esmolol β1 > β2 blocker
500mcg/kg over 1 min, then 50-‐200 mcg/kg/min
1-‐5min/15-‐30min 1oheart block, CHF, asthma
Labetelol α1, β1, β2 blocker
20-‐40mg q10 min, or 2mg/min
5-‐10min/2-‐6hr Bronchoconstriction, heart block, brady,
Fenoldopam D1, α2 agonist
0.1-‐0.3 mcg/kg/min <5min/30 min h/a, tachy, flushing, local phlebitis, dizzy
Epoprosterol Pulm. Vasodilator
2-‐20ng/kg/min 3-‐6min/15min Rebound pulm HTN,
Enalaprilat ACEI 0.625-‐2.5 q6h <30min/12-‐24h AKI, hypotension Hydralazine Vasodilator 5-‐20mg q20min 5-‐10min/2-‐6h Tachy, h/a, ↑ICP, Na/H2O
retention III. OTHER CARDIAC DRIPS
Drug Class Dose Action Side effects Amiodarone Class III (Na/K
channel blocker, CCB, BB)
150mg over 10 min, then 1mg/min x6h, then 0.5mg/min x18h
Anti-‐arrhythmic, rate control
AV block, hypotension
Procainamide Class IA (Na channel blocker)
17mg/kg (usu 1gm) over 20min, then 1-‐4mg/min
Anti-‐arrhythmic Hypotension, prolonged QT
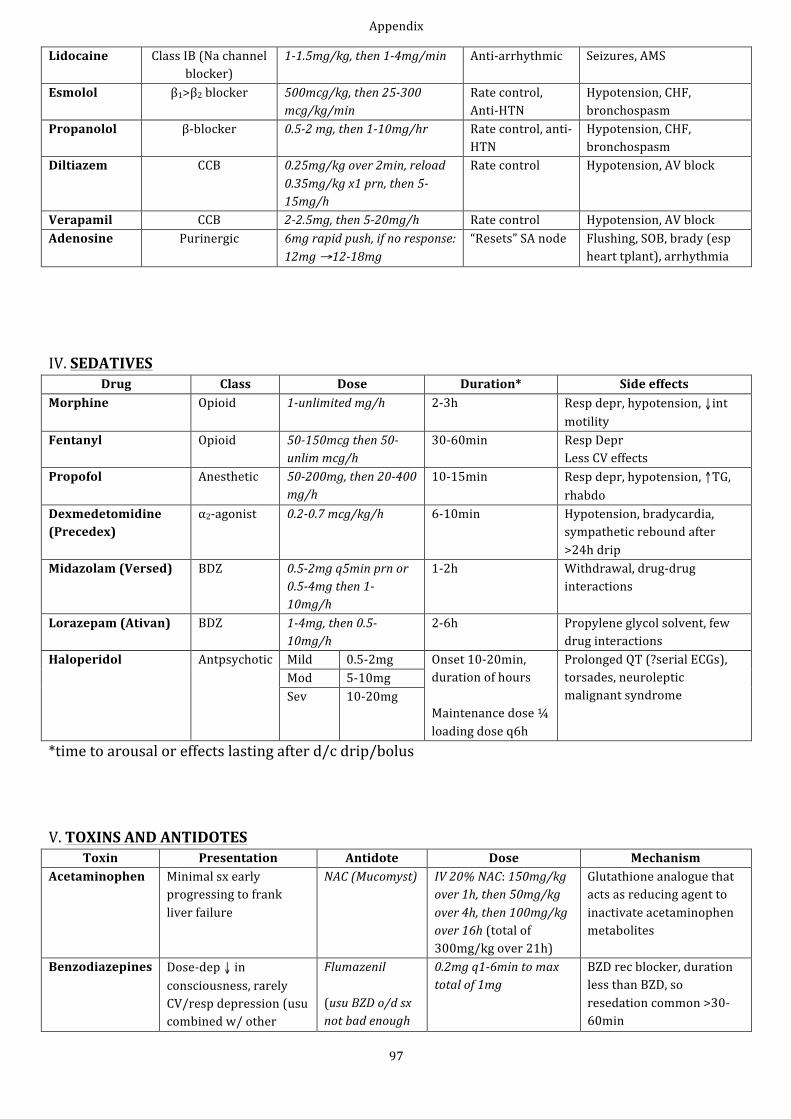
Appendix
97
Lidocaine Class IB (Na channel blocker)
1-‐1.5mg/kg, then 1-‐4mg/min Anti-‐arrhythmic Seizures, AMS
Esmolol β1>β2 blocker 500mcg/kg, then 25-‐300 mcg/kg/min
Rate control, Anti-‐HTN
Hypotension, CHF, bronchospasm
Propanolol β-‐blocker 0.5-‐2 mg, then 1-‐10mg/hr Rate control, anti-‐HTN
Hypotension, CHF, bronchospasm
Diltiazem CCB 0.25mg/kg over 2min, reload 0.35mg/kg x1 prn, then 5-‐15mg/h
Rate control Hypotension, AV block
Verapamil CCB 2-‐2.5mg, then 5-‐20mg/h Rate control Hypotension, AV block Adenosine Purinergic 6mg rapid push, if no response:
12mg →12-‐18mg “Resets” SA node Flushing, SOB, brady (esp
heart tplant), arrhythmia IV. SEDATIVES
Drug Class Dose Duration* Side effects Morphine Opioid 1-‐unlimited mg/h 2-‐3h Resp depr, hypotension, ↓int
motility Fentanyl Opioid 50-‐150mcg then 50-‐
unlim mcg/h 30-‐60min Resp Depr
Less CV effects Propofol Anesthetic 50-‐200mg, then 20-‐400
mg/h 10-‐15min Resp depr, hypotension, ↑TG,
rhabdo Dexmedetomidine (Precedex)
α2-‐agonist 0.2-‐0.7 mcg/kg/h 6-‐10min Hypotension, bradycardia, sympathetic rebound after >24h drip
Midazolam (Versed) BDZ 0.5-‐2mg q5min prn or 0.5-‐4mg then 1-‐10mg/h
1-‐2h Withdrawal, drug-‐drug interactions
Lorazepam (Ativan) BDZ 1-‐4mg, then 0.5-‐10mg/h
2-‐6h Propylene glycol solvent, few drug interactions
Haloperidol Antpsychotic Mild 0.5-‐2mg Onset 10-‐20min, duration of hours Maintenance dose ¼ loading dose q6h
Prolonged QT (?serial ECGs), torsades, neuroleptic malignant syndrome
Mod 5-‐10mg Sev 10-‐20mg
*time to arousal or effects lasting after d/c drip/bolus V. TOXINS AND ANTIDOTES
Toxin Presentation Antidote Dose Mechanism Acetaminophen Minimal sx early
progressing to frank liver failure
NAC (Mucomyst) IV 20% NAC: 150mg/kg over 1h, then 50mg/kg over 4h, then 100mg/kg over 16h (total of 300mg/kg over 21h)
Glutathione analogue that acts as reducing agent to inactivate acetaminophen metabolites
Benzodiazepines Dose-‐dep ↓ in consciousness, rarely CV/resp depression (usu combined w/ other
Flumazenil (usu BZD o/d sx not bad enough
0.2mg q1-‐6min to max total of 1mg
BZD rec blocker, duration less than BZD, so resedation common >30-‐60min
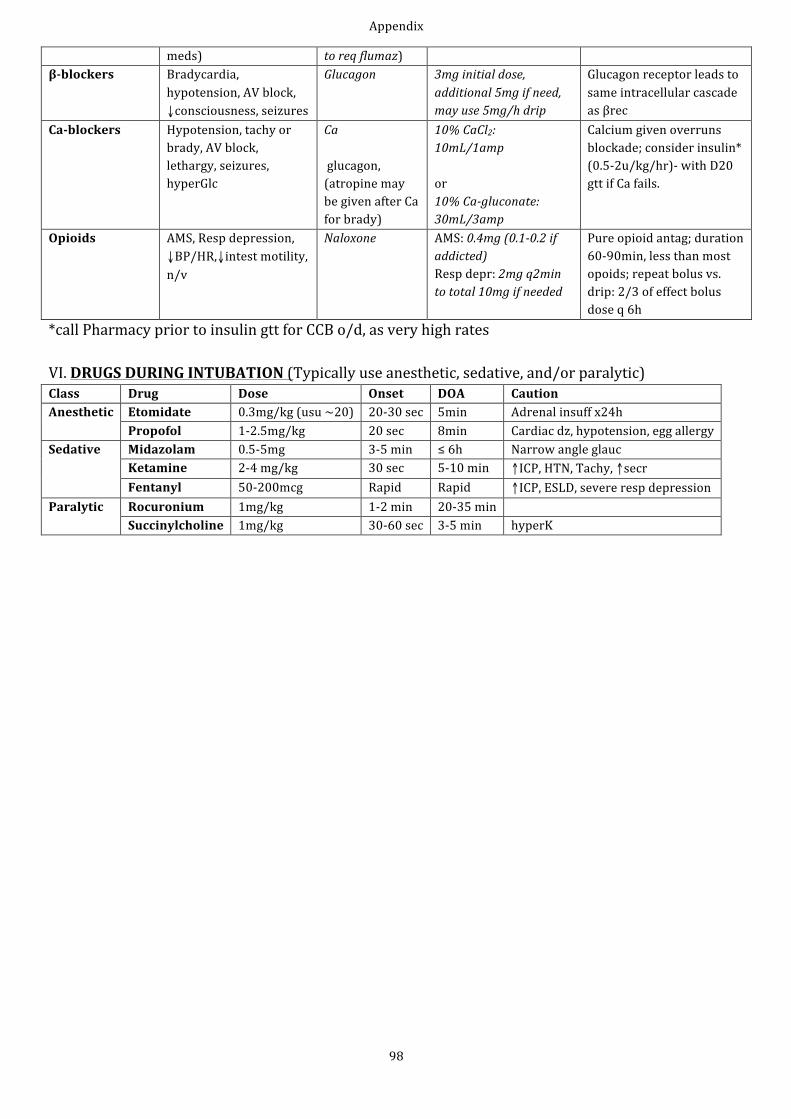
Appendix
98
meds) to req flumaz) β-‐blockers Bradycardia,
hypotension, AV block, ↓consciousness, seizures
Glucagon 3mg initial dose, additional 5mg if need, may use 5mg/h drip
Glucagon receptor leads to same intracellular cascade as βrec
Ca-‐blockers Hypotension, tachy or brady, AV block, lethargy, seizures, hyperGlc
Ca glucagon, (atropine may be given after Ca for brady)
10% CaCl2: 10mL/1amp or 10% Ca-‐gluconate: 30mL/3amp
Calcium given overruns blockade; consider insulin* (0.5-‐2u/kg/hr)-‐ with D20 gtt if Ca fails.
Opioids AMS, Resp depression, ↓BP/HR,↓intest motility, n/v
Naloxone AMS: 0.4mg (0.1-‐0.2 if addicted) Resp depr: 2mg q2min to total 10mg if needed
Pure opioid antag; duration 60-‐90min, less than most opoids; repeat bolus vs. drip: 2/3 of effect bolus dose q 6h
*call Pharmacy prior to insulin gtt for CCB o/d, as very high rates VI. DRUGS DURING INTUBATION (Typically use anesthetic, sedative, and/or paralytic) Class Drug Dose Onset DOA Caution Anesthetic Etomidate 0.3mg/kg (usu ~20) 20-‐30 sec 5min Adrenal insuff x24h
Propofol 1-‐2.5mg/kg 20 sec 8min Cardiac dz, hypotension, egg allergy Sedative Midazolam 0.5-‐5mg 3-‐5 min ≤ 6h Narrow angle glauc
Ketamine 2-‐4 mg/kg 30 sec 5-‐10 min ↑ICP, HTN, Tachy, ↑secr Fentanyl 50-‐200mcg Rapid Rapid ↑ICP, ESLD, severe resp depression
Paralytic Rocuronium 1mg/kg 1-‐2 min 20-‐35 min Succinylcholine 1mg/kg 30-‐60 sec 3-‐5 min hyperK
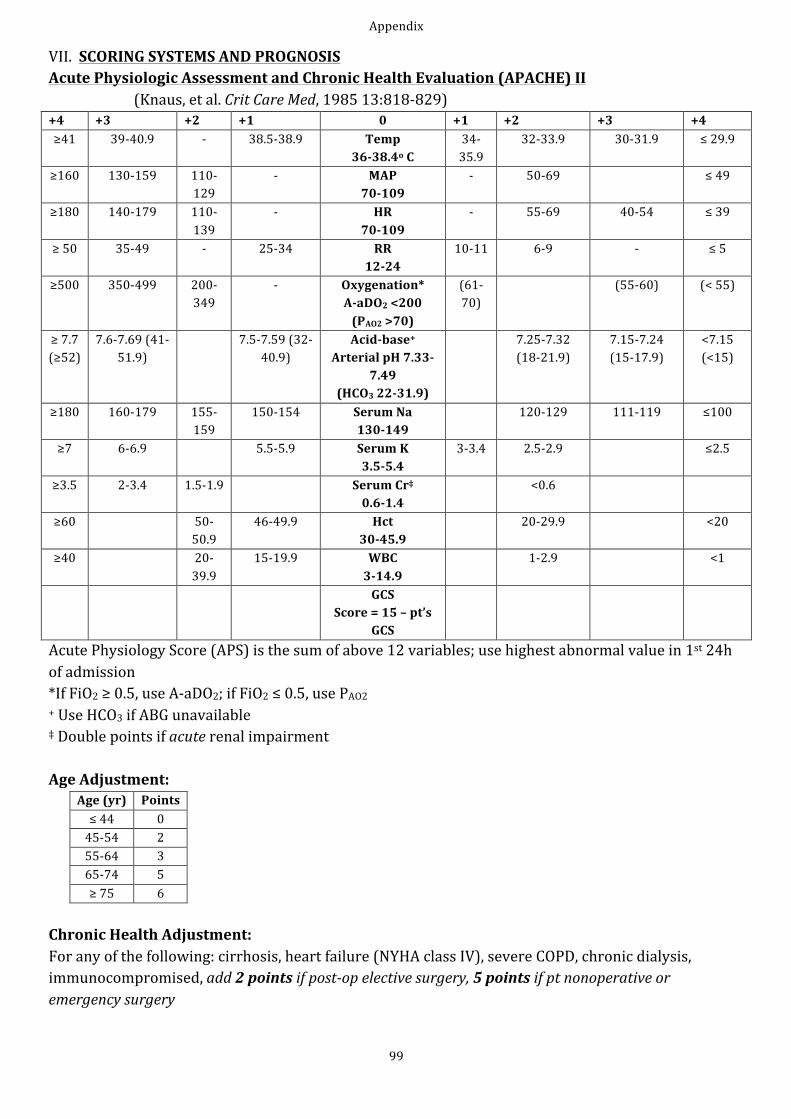
Appendix
99
VII. SCORING SYSTEMS AND PROGNOSIS Acute Physiologic Assessment and Chronic Health Evaluation (APACHE) II (Knaus, et al. Crit Care Med, 1985 13:818-‐829) +4 +3 +2 +1 0 +1 +2 +3 +4 ≥41 39-‐40.9 -‐ 38.5-‐38.9 Temp
36-‐38.4o C 34-‐35.9
32-‐33.9 30-‐31.9 ≤ 29.9
≥160 130-‐159 110-‐129
-‐ MAP 70-‐109
-‐ 50-‐69 ≤ 49
≥180 140-‐179 110-‐139
-‐ HR 70-‐109
-‐ 55-‐69 40-‐54 ≤ 39
≥ 50 35-‐49 -‐ 25-‐34 RR 12-‐24
10-‐11 6-‐9 -‐ ≤ 5
≥500 350-‐499 200-‐349
-‐ Oxygenation* A-‐aDO2 <200 (PAO2 >70)
(61-‐70)
(55-‐60) (< 55)
≥ 7.7 (≥52)
7.6-‐7.69 (41-‐51.9)
7.5-‐7.59 (32-‐40.9)
Acid-‐base+ Arterial pH 7.33-‐
7.49 (HCO3 22-‐31.9)
7.25-‐7.32 (18-‐21.9)
7.15-‐7.24 (15-‐17.9)
<7.15 (<15)
≥180 160-‐179 155-‐159
150-‐154 Serum Na 130-‐149
120-‐129 111-‐119 ≤100
≥7 6-‐6.9 5.5-‐5.9 Serum K 3.5-‐5.4
3-‐3.4 2.5-‐2.9 ≤2.5
≥3.5 2-‐3.4 1.5-‐1.9 Serum Cr‡ 0.6-‐1.4
<0.6
≥60 50-‐50.9
46-‐49.9 Hct 30-‐45.9
20-‐29.9 <20
≥40 20-‐39.9
15-‐19.9 WBC 3-‐14.9
1-‐2.9 <1
GCS Score = 15 – pt’s
GCS
Acute Physiology Score (APS) is the sum of above 12 variables; use highest abnormal value in 1st 24h of admission *If FiO2 ≥ 0.5, use A-‐aDO2; if FiO2 ≤ 0.5, use PAO2 + Use HCO3 if ABG unavailable ‡ Double points if acute renal impairment Age Adjustment:
Age (yr) Points ≤ 44 0 45-‐54 2 55-‐64 3 65-‐74 5 ≥ 75 6
Chronic Health Adjustment: For any of the following: cirrhosis, heart failure (NYHA class IV), severe COPD, chronic dialysis, immunocompromised, add 2 points if post-‐op elective surgery, 5 points if pt nonoperative or emergency surgery
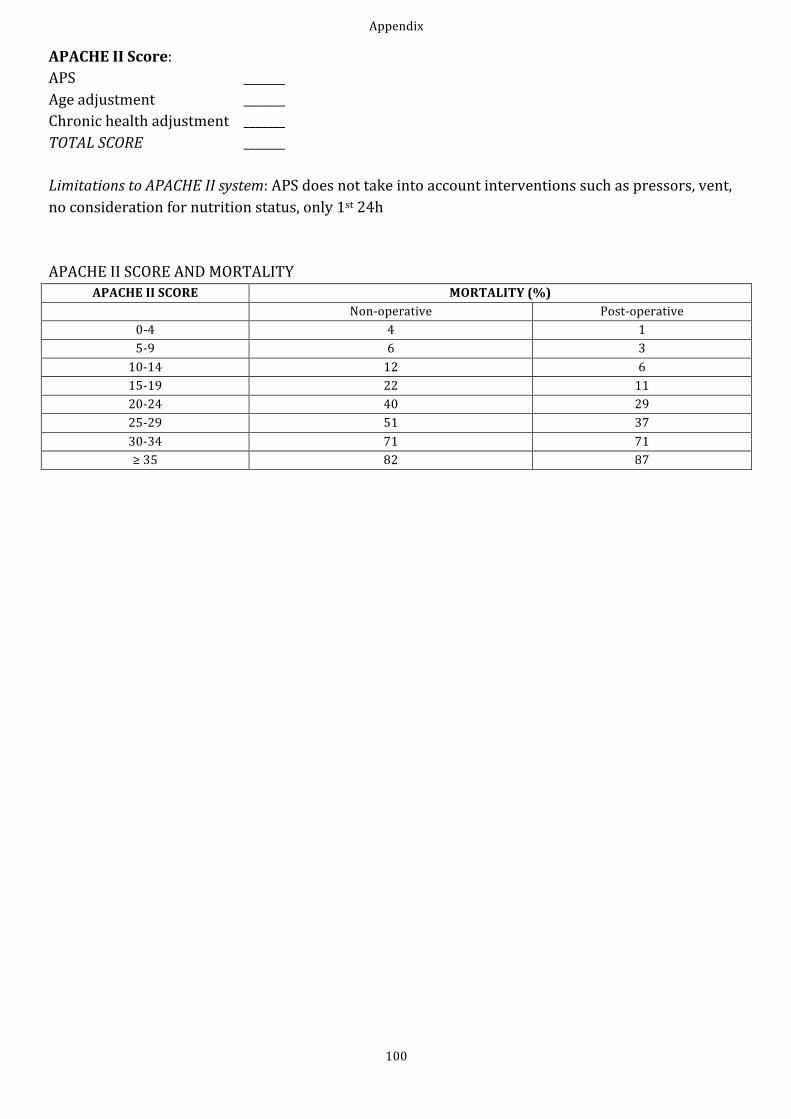
Appendix
100
APACHE II Score: APS _______ Age adjustment _______ Chronic health adjustment _______ TOTAL SCORE _______ Limitations to APACHE II system: APS does not take into account interventions such as pressors, vent, no consideration for nutrition status, only 1st 24h APACHE II SCORE AND MORTALITY
APACHE II SCORE MORTALITY (%) Non-‐operative Post-‐operative
0-‐4 4 1 5-‐9 6 3 10-‐14 12 6 15-‐19 22 11 20-‐24 40 29 25-‐29 51 37 30-‐34 71 71 ≥ 35 82 87
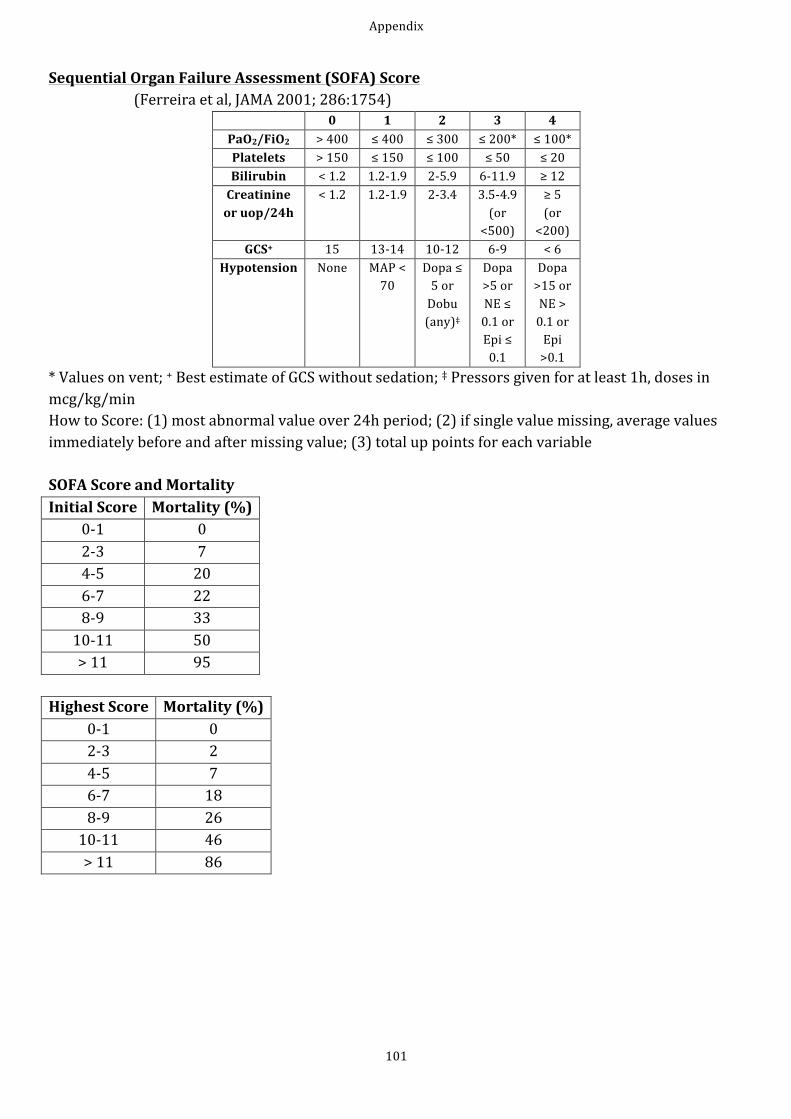
Appendix
101
Sequential Organ Failure Assessment (SOFA) Score (Ferreira et al, JAMA 2001; 286:1754)
0 1 2 3 4 PaO2/FiO2 > 400 ≤ 400 ≤ 300 ≤ 200* ≤ 100* Platelets > 150 ≤ 150 ≤ 100 ≤ 50 ≤ 20 Bilirubin < 1.2 1.2-‐1.9 2-‐5.9 6-‐11.9 ≥ 12 Creatinine or uop/24h
< 1.2 1.2-‐1.9 2-‐3.4 3.5-‐4.9 (or <500)
≥ 5 (or <200)
GCS+ 15 13-‐14 10-‐12 6-‐9 < 6 Hypotension None MAP <
70 Dopa ≤ 5 or Dobu (any)‡
Dopa >5 or NE ≤ 0.1 or Epi ≤ 0.1
Dopa >15 or NE > 0.1 or Epi >0.1
* Values on vent; + Best estimate of GCS without sedation; ‡ Pressors given for at least 1h, doses in mcg/kg/min How to Score: (1) most abnormal value over 24h period; (2) if single value missing, average values immediately before and after missing value; (3) total up points for each variable SOFA Score and Mortality Initial Score Mortality (%)
0-‐1 0 2-‐3 7 4-‐5 20 6-‐7 22 8-‐9 33 10-‐11 50 > 11 95
Highest Score Mortality (%)
0-‐1 0 2-‐3 2 4-‐5 7 6-‐7 18 8-‐9 26 10-‐11 46 > 11 86
Appendix
102
VIII. BASIC MEDICO-‐LEGAL INFORMATION (http://law.justia.com/newmexico/codes/nmrc/jd_ch24art7a-‐acff.html) Medicial decision making hierarchy in NM: 1. Pt 2. POA or person pt declares to provider to be his/her surrogate (including who pt tells doctor should make their medical decisions) 3. Spouse or person “fulfilling the traditional role of a spouse” (unless legally separated or pending annulment, divorce, etc.) 4. Person in long-‐term relation of indefinite duration with pt demonstrating commitment to pt similar to commitment of a spouse
5. Adult child 6. Parent 7. Adult sibling 8. Grandparent 9. In the event no relative, an adult with special concern Notes: -‐ important: when admitting a lucid pt, don’t ask who their “contact person” is, instead, ask “If you couldn’t make your own medical decisions, who would you want to make those decisions for you?” and document this as such
-‐ pt at any time may disqualify any person, including family, from acting as surrogate either by signed writing or personally informing provider
-‐ if >1 member of a class is present, must go with majority decision; if class is evenly divided and provider so informed, that class and all lower are disqualified
ACKNOWLEDGMENTS -‐ Dr. Michel Boivin, who supervised and edited the final content matter -‐ Dr. R. S. Morehead at the University of Kentucky, who provided the UK MICU Guidebook that served as a basic template for this endeavor -‐ Drs. Nathan Boyer, Jens Langsjoen and Lana Melendres, who provided feedback for earlier editions -‐ Drs. Erik Kraai and Shozab Ahmed, who helped with this edition Remember, medicine is an ever-‐changing discipline. This guide is meant as a help, and not to replace keeping up with the literature! Hope this helps, -‐-‐Jarrod Frizzell, MD





























