Embed Size (px)
Citation preview
MASH – Work-Package 6
‐ 1 ‐
MASH
- Mass casualties and Health care following the release of
toxic chemicals or radioactive material –
WP 6 – Final Report
V Meineke, DH Graessle, E Schanbacher
Institut für Radiobiologie der Bundeswehr
in Verbindung mit der Universität Ulm
MASH – Work-Package 6
‐ 2 ‐
Background
Within the EU MASH program WP 6 was designed to study the individual state of preparedness in the 27 EU Member States with respect to the management of mass casualties following the release of radioactive material. This includes a survey of the national guidelines of the member states for triage, decontamination and initial medical counter measures at the scene. A template had to be developed which itemizes key attributes of emergency preparedness plans. The template information had to be collated for as many state plans as possible so that key attributes may easily be compared across states.
Therefore the key organizations/institutions supervising the specialized medical responses in case of release of toxic chemicals or radioactive material had to be identified, contacted and asked for cooperation in order to verify the individual state of preparation.
By compiling and analyzing the various national practices, a common understanding was to be assessed in order to recommend and highlight information useful in generic preparedness planning. These common understandings will be used as the basis for the future projection undertaken in WPs7-9.
As outlined in the “description of the action” there was uncertainty about attracting enough member states and getting access to national preparedness planning, therefore a number of fifteen partners was seen as the critical number for the reference group. Hence, it was great success that by the end of 2008 25 representatives from 20 countries had declared their preparedness to participate.
Time schedule
Spring 2008 (during the MASH “kick off” meeting in Umea, Sweden): Definition of detailed data for investigating the state of preparation in the 27 EU Members States.
May 2008- August 2008: Identification of contact points (individuals, organizations, institutions) in all 27 Member States of the European Union
June 2008- October 2008: Configuration of a questionnaire enquiring the pre-clinical and clinical algorithms available
October 2008: Setup of an online accessible platform on a security server to gather information regarding the organizational structure and individual preparedness for radiation mass casualty management in the EU 27.

MASH – Work-Package 6
‐ 3 ‐
November 2008 - February 2009: Potential key organizations supervising the specialized medical response in case of radiological/dirty bomb disaster and/or were identified. 107 contact points (up to 9 per country) were informed about the research project and asked to participate or to help in identifying responsible persons/groups assigned responsibility for RN Medical Planning. They were informed about the questionnaire and invited to participate in the forthcoming European Symposium on the management of mass incidents caused by release of toxic chemicals or radioactive materials in February 2009 in Munich.
38 organizations with expertise in radiation medicine or radiobiology declared their principle preparedness to participate in the questionnaire survey. They were provided with an individual password and username to access the questionnaire and fill in and save their data. They were asked to complete the questionnaire until the end of January; however, this date could not be met by all participants.
Finally, 25 representatives from 20 countries of the 27 EU Member States replied to the questionnaire.
February 11th, 2009: Workshop on radiation mass casualty management in the European Union in Munich.
This workshop was conducted as a joint seminar on CR (WP 5 and 6) best practices of today and embedded into the “18th Medizinische A-Schutz-Tagung”. 170 scientists with different emphasis in radiobiology and radiation accident management from all over the world participated in this Symposium and gave presentations about new methods of radiation protection and diagnosis and therapy of the acute radiation syndrome. The symposium provided an excellent possibility for the MASH-representatives to establish new contacts to experts from all over the world. It was the key step in developing the essential network and provided an opportunity for partners to meet relevant end-users, a wider dissemination of results and valuable and practical insight from both authorities and end-users. It served as a platform for developing networks and relationships through direct contact. 17 cooperators in the questionnaire attended the meeting. They gave oral or poster presentations about the structure of their respective institutions/organizations, expertise, national organizational/institutional structure, ongoing activities, publications and specified the need for further improvement in various areas. This information enhanced the survey of the national guidelines of the Member States for triage, decontamination and initial medical counter measures at the scene of chemical and radiological disasters provided by the questionnaires. First results from the questionnaire survey/evaluation were presented. The completion of the questionnaire could not be accomplished by all participants until February and although the results were preliminary, the necessity to harmonize radiation accident management in Europe could be stated as a first result. The result of the final discussion was the specified need for a
MASH – Work-Package 6
‐ 4 ‐
European Network. The initiative for „EMRAM” (European Medical Radiation Accident Management) was discussed and approved. Following the symposium, the presentations were uploaded on the MASH website and all participants in the questionnaire were given a username and password to access the symposium site so that the information provided within the symposium was also accessible for the representatives of the Members States that could not participate in the symposium. March 2009 up to now: Ongoing gathering of information from the 27 countries.
Structure of the questionnaire
1: Organizational structures
- Personal information - Structure of the emergency system - Responsible institutions - Networking with international institutions (IAEA, REMPAN (WHO)
2: Health care system
- Pre hospital triage, Monitoring in the case of a radiation accident - Decontamination - Clinical diagnosis - Biological dosimetry - Physical dosimetry - Therapy, follow-up - Guidelines
Evaluation of the Responses to the Questionnaires
Number of received filled questionnaires: 25
Number of countries represented: 20
(Some countries were represented by several institutions)
MASH – Work-Package 6
‐ 5 ‐
I Organizational Structure Questions 1 to 22: contact data of the person filling in the questionnaire, expertise and request to name additional responsible organizations.
15 additional contact data sets of responsible persons could be acquired.
16 contact data sets of interested collaboration partners were received within the questionnaires.
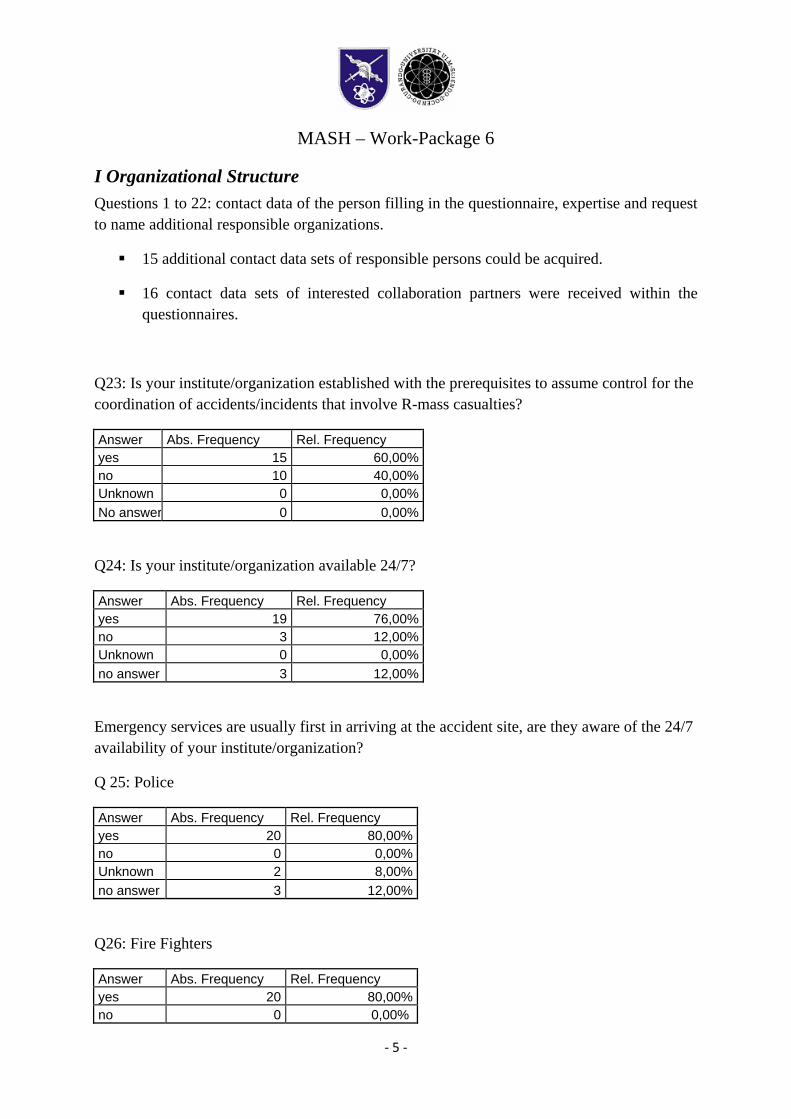
Q23: Is your institute/organization established with the prerequisites to assume control for the coordination of accidents/incidents that involve R-mass casualties?
Answer Abs. Frequency Rel. Frequency yes 15 60,00%no 10 40,00%Unknown 0 0,00%No answer 0 0,00%
Q24: Is your institute/organization available 24/7?
Answer Abs. Frequency Rel. Frequency yes 19 76,00%no 3 12,00%Unknown 0 0,00%no answer 3 12,00%
Emergency services are usually first in arriving at the accident site, are they aware of the 24/7 availability of your institute/organization?
Q 25: Police
Answer Abs. Frequency Rel. Frequency yes 20 80,00%no 0 0,00%Unknown 2 8,00%no answer 3 12,00%
Q26: Fire Fighters
Answer Abs. Frequency Rel. Frequency yes 20 80,00%no 0 0,00%
MASH – Work-Package 6
‐ 6 ‐
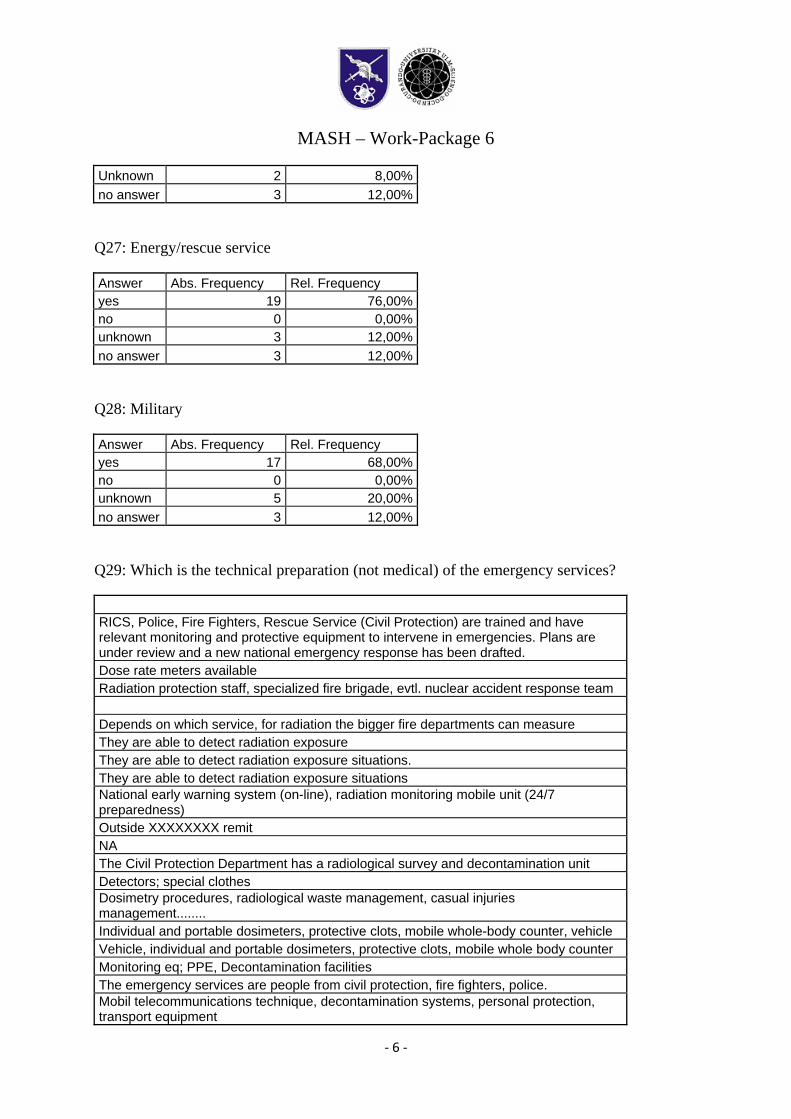
Unknown 2 8,00%no answer 3 12,00%
Q27: Energy/rescue service
Answer Abs. Frequency Rel. Frequency yes 19 76,00%no 0 0,00%unknown 3 12,00%no answer 3 12,00%
Q28: Military
Answer Abs. Frequency Rel. Frequency yes 17 68,00%no 0 0,00%unknown 5 20,00%no answer 3 12,00%
Q29: Which is the technical preparation (not medical) of the emergency services?
RICS, Police, Fire Fighters, Rescue Service (Civil Protection) are trained and have relevant monitoring and protective equipment to intervene in emergencies. Plans are under review and a new national emergency response has been drafted. Dose rate meters available Radiation protection staff, specialized fire brigade, evtl. nuclear accident response team Depends on which service, for radiation the bigger fire departments can measure They are able to detect radiation exposure They are able to detect radiation exposure situations. They are able to detect radiation exposure situations National early warning system (on-line), radiation monitoring mobile unit (24/7 preparedness) Outside XXXXXXXX remit NA The Civil Protection Department has a radiological survey and decontamination unit Detectors; special clothes Dosimetry procedures, radiological waste management, casual injuries management........ Individual and portable dosimeters, protective clots, mobile whole-body counter, vehicle Vehicle, individual and portable dosimeters, protective clots, mobile whole body counter Monitoring eq; PPE, Decontamination facilities The emergency services are people from civil protection, fire fighters, police. Mobil telecommunications technique, decontamination systems, personal protection, transport equipment
MASH – Work-Package 6
‐ 7 ‐
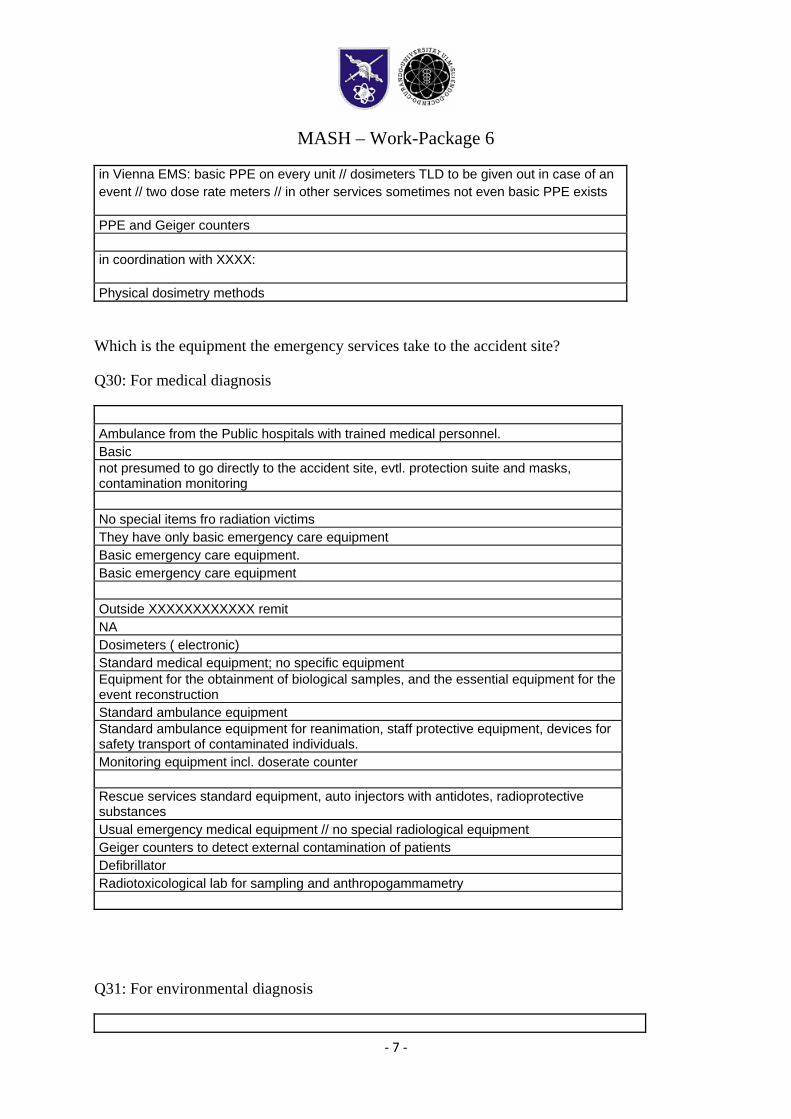
in Vienna EMS: basic PPE on every unit // dosimeters TLD to be given out in case of an event // two dose rate meters // in other services sometimes not even basic PPE exists
PPE and Geiger counters in coordination with XXXX:
Physical dosimetry methods
Which is the equipment the emergency services take to the accident site?
Q30: For medical diagnosis
Ambulance from the Public hospitals with trained medical personnel. Basic not presumed to go directly to the accident site, evtl. protection suite and masks, contamination monitoring No special items fro radiation victims They have only basic emergency care equipment Basic emergency care equipment. Basic emergency care equipment Outside XXXXXXXXXXXX remit NA Dosimeters ( electronic) Standard medical equipment; no specific equipment Equipment for the obtainment of biological samples, and the essential equipment for the event reconstruction Standard ambulance equipment Standard ambulance equipment for reanimation, staff protective equipment, devices for safety transport of contaminated individuals. Monitoring equipment incl. doserate counter Rescue services standard equipment, auto injectors with antidotes, radioprotective substances Usual emergency medical equipment // no special radiological equipment Geiger counters to detect external contamination of patients Defibrillator Radiotoxicological lab for sampling and anthropogammametry
Q31: For environmental diagnosis
MASH – Work-Package 6
‐ 8 ‐
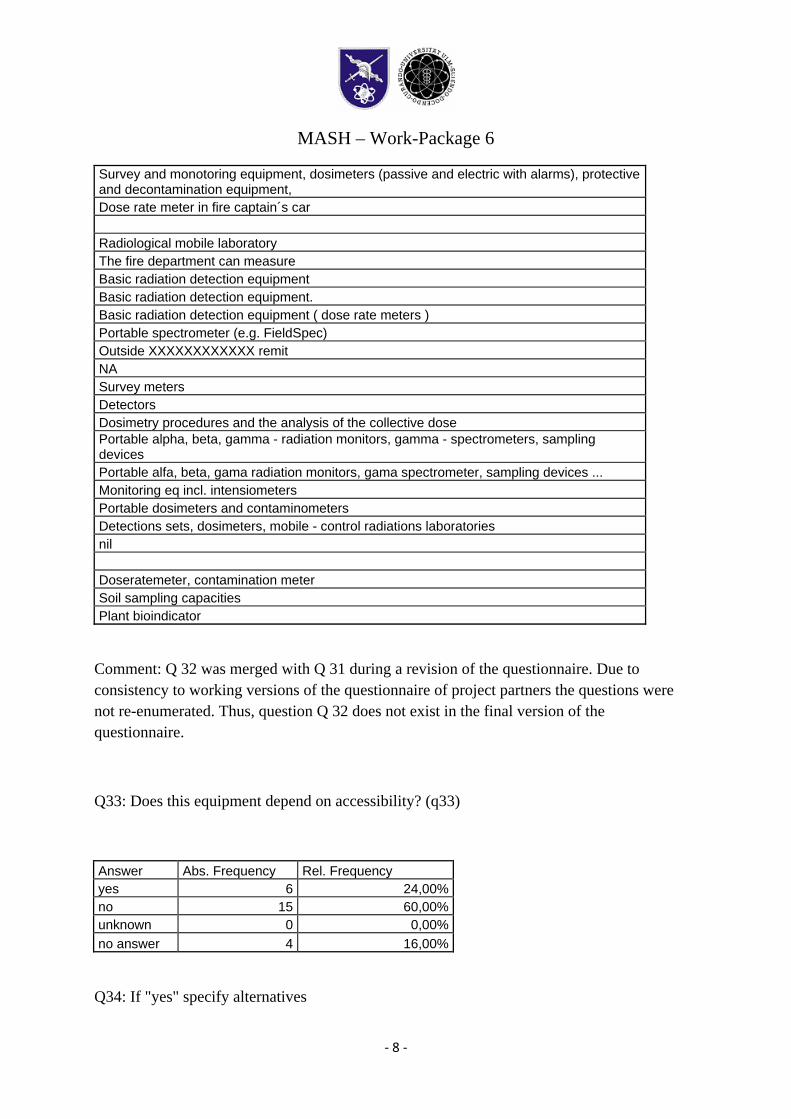
Survey and monotoring equipment, dosimeters (passive and electric with alarms), protective and decontamination equipment, Dose rate meter in fire captain´s car Radiological mobile laboratory The fire department can measure Basic radiation detection equipment Basic radiation detection equipment. Basic radiation detection equipment ( dose rate meters ) Portable spectrometer (e.g. FieldSpec) Outside XXXXXXXXXXXX remit NA Survey meters Detectors Dosimetry procedures and the analysis of the collective dose Portable alpha, beta, gamma - radiation monitors, gamma - spectrometers, sampling devices Portable alfa, beta, gama radiation monitors, gama spectrometer, sampling devices ... Monitoring eq incl. intensiometers Portable dosimeters and contaminometers Detections sets, dosimeters, mobile - control radiations laboratories nil Doseratemeter, contamination meter Soil sampling capacities Plant bioindicator
Comment: Q 32 was merged with Q 31 during a revision of the questionnaire. Due to consistency to working versions of the questionnaire of project partners the questions were not re-enumerated. Thus, question Q 32 does not exist in the final version of the questionnaire.
Q33: Does this equipment depend on accessibility? (q33)
Answer Abs. Frequency Rel. Frequency yes 6 24,00%no 15 60,00%unknown 0 0,00%no answer 4 16,00%
Q34: If "yes" specify alternatives
MASH – Work-Package 6
‐ 9 ‐
In XXXXXXXXXXXX, one car is equipped for monitoring dangerous agents, including identification of radionuclides not all fire fighters have the measuring device for radiation Outside XXXXXXXXXXXX remit
NA Number of eq-units are limiting Particulary yes, it depends of disposition in concrete location in territory. I do not understand the question
Q35: Which are the communication systems used (GSM, UMTS, GPS, dedicated ….)?
Dedicated wireless, GSM, UMTS TETRA-based public authorities network Gsm, gps Dedicated Dedicated. Dedicated GSM, dedicated radio system (operated by Civil Protection) Outside XXXXXXX remit XXXXXXX GSM, Local wireless, GPS GSM radiotransmission;GSM
MASH – Work-Package 6
‐ 10 ‐
GPS GSM, GPS, fax, e-mail GSM, GPS, fax, e-mail GSM, TETRA, GPS, dedicated radionetwork; military telephone network; Internet; different Intranet GSM, GPS, UMTS Standard communication systems, mobile phones Radio, GSM Dedicated radio, GSM, Tetra GSM, GPS no applicable
Q36: Is the information gathered, saved or transmitted?
Saved in paper and electronic form, Transmitted to XXXXX and the emergency operations centre Depending on specific instructions Saved and transmitted yes Yes. Yes Saved and transmitted to the seat of organisation (XXXXXXXX)
Outside XXXXXXXXX remit Not clear transmitted yes yes saved preliminary data for environmental monitoring and propose urgent protective measure to MH Saved preliminary date for environmental monitoring and propose urgent protective measure to Ministry of Health Some info are saved in data loggs, e.g. patient information in standard patient information files. Usually transmitted, but also saved. Information are both saved and transmitted. no Gathered no applicable
MASH – Work-Package 6
‐ 11 ‐
Q37: Where is it saved or where it is transmitted to?
Saved in paper and electronic form, Transmitted to XXXXXXXXX and the eemrgency operations centre Local emergency service command center XXXXXXXXXX for Emergency Situations XXXXXXXXXXX for Emergency Situations. XXXXXXXXXX for Emergency Situations Written down in the form and transmitted to the seat of organisation (XXXXX) Outside XXXXXXX remit Not clear transmitted to control room of civil protection unit centre of emergency coordination service To the XXXXXXXXX and to the reference hospital XXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXX Local, regional and national compent authorities Transmitted to decision makers, saved for own purposes. The information is transmitted and saved by XXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXXX
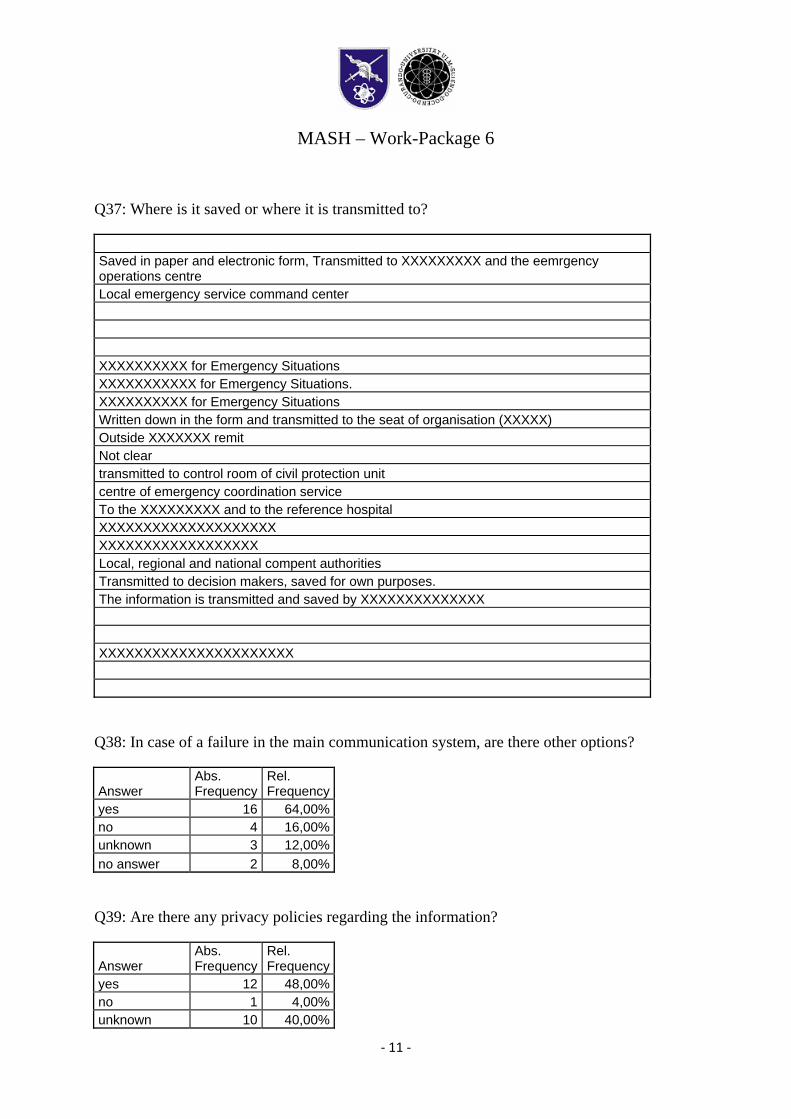
Q38: In case of a failure in the main communication system, are there other options?
Answer Abs. Frequency
Rel. Frequency
yes 16 64,00%no 4 16,00%unknown 3 12,00%no answer 2 8,00%
Q39: Are there any privacy policies regarding the information?
Answer Abs. Frequency
Rel. Frequency
yes 12 48,00%no 1 4,00%unknown 10 40,00%
MASH – Work-Package 6
‐ 12 ‐
no answer 2 8,00%
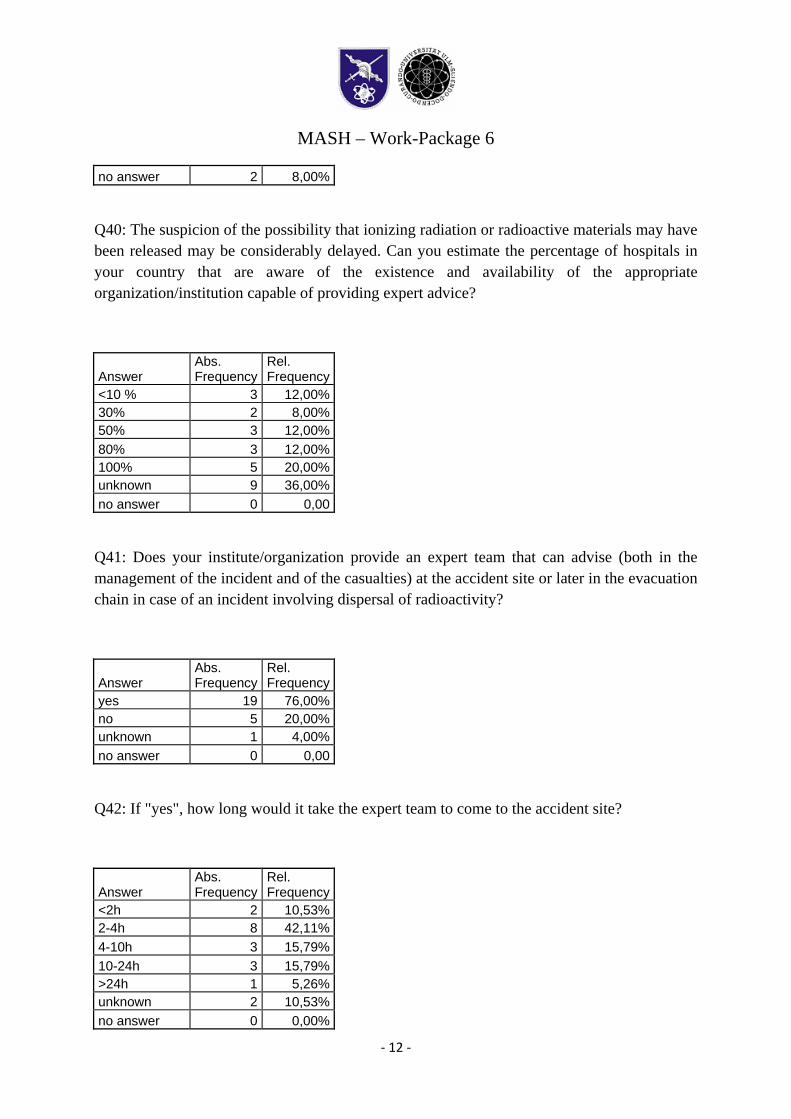
Q40: The suspicion of the possibility that ionizing radiation or radioactive materials may have been released may be considerably delayed. Can you estimate the percentage of hospitals in your country that are aware of the existence and availability of the appropriate organization/institution capable of providing expert advice?
Answer Abs. Frequency
Rel. Frequency
<10 % 3 12,00%30% 2 8,00%50% 3 12,00%80% 3 12,00%100% 5 20,00%unknown 9 36,00%no answer 0 0,00
Q41: Does your institute/organization provide an expert team that can advise (both in the management of the incident and of the casualties) at the accident site or later in the evacuation chain in case of an incident involving dispersal of radioactivity?
Answer Abs. Frequency
Rel. Frequency
yes 19 76,00%no 5 20,00%unknown 1 4,00%no answer 0 0,00
Q42: If "yes", how long would it take the expert team to come to the accident site?
Answer Abs. Frequency
Rel. Frequency
<2h 2 10,53%2-4h 8 42,11%4-10h 3 15,79%10-24h 3 15,79%>24h 1 5,26%unknown 2 10,53%no answer 0 0,00%
MASH – Work-Package 6
‐ 13 ‐
[Evaluator Comment: numbers in relation to “yes” answers in q41]]
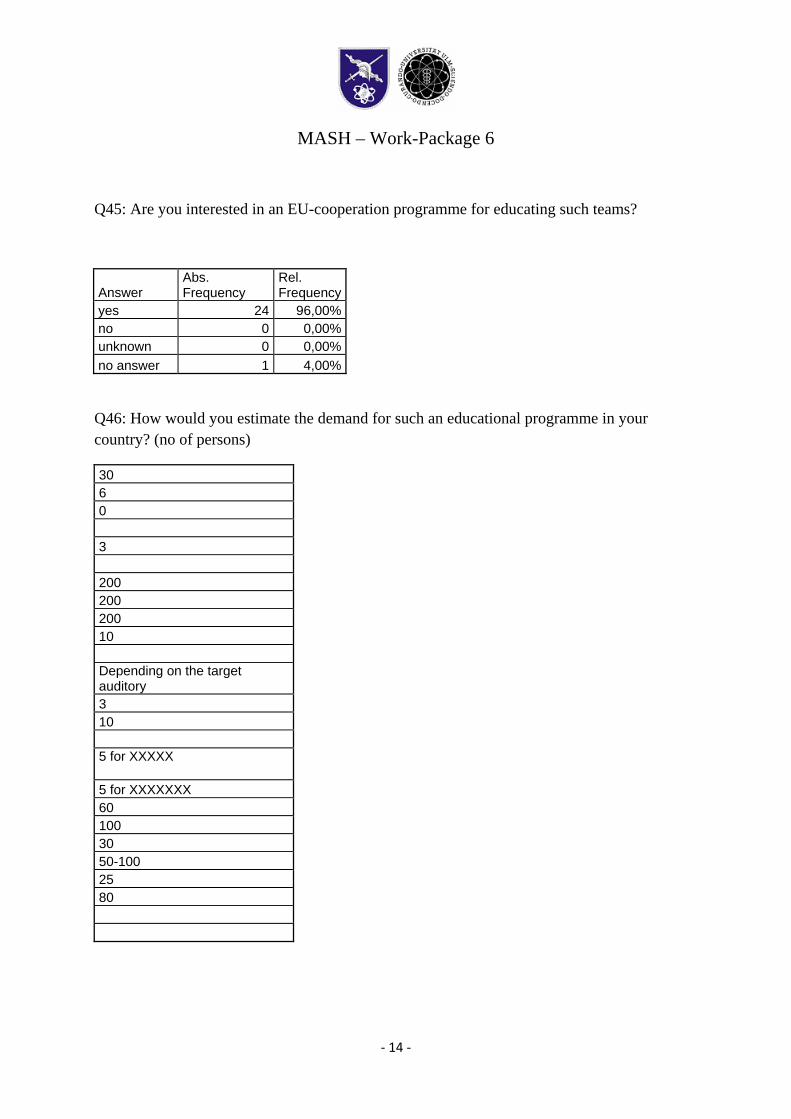
Q43: Please specify tasks the expert team could provide at the accident site (advise, conduct sampling, decontamination, triage etc.)
advice, conduct sampling, decontamination, physical dosimetry, biodosimetry advice, conduct sampling, decontamination Advice, direct measurements, identification of nuclides, sampling advise, conduct sampling, decontamination, triage advise, conduct sampling,dose-rate mapping,thyroid contamination measurements advice,conduct sampling Advice, conduct sampling and triage. Technical advice, conduct sampling and triage advise and measure radioactivity, sampling and detailed measurements will be performed by national mobile radiation monitoring team Time to deploy dependent on a number of factors inclduing location. XXXXXXXX can provide advice and radiological monitoring capability
Advice medical treatment advise, sampling, detection,triage advise, conduct sampling, triage etc advice on the health status of the victims and triage; conducting samples for biologycal dosimetry, blood cell count, urine analisys and clinical chemistry; environmental sampling Advise on the health status of the victims and triage. Conducting sample for: biological dosimetry, cells blood count, standard urine analysis, clinical chemistry. Environmental sampling. Advises on monitoring, triage, decontamination, treatment, resources etc advice, radioactive source search and identification, radiation monitoring All above mentioned (=. advise, conduct sampling, decontamination, triage etc.) all that is listed advise, conduct sampling, triage, hospitalisation in a specific service
Q44: If "no": Do you consider that the presence of an expert team is essential?
Answer Abs. Frequency
Rel. Frequency
yes 4 80,00%no 0 0,00%unknown 0 0,00%no answer 1 20,00%[Evaluator Comment: numbers in relation to “no” answers in q41]
MASH – Work-Package 6
‐ 14 ‐
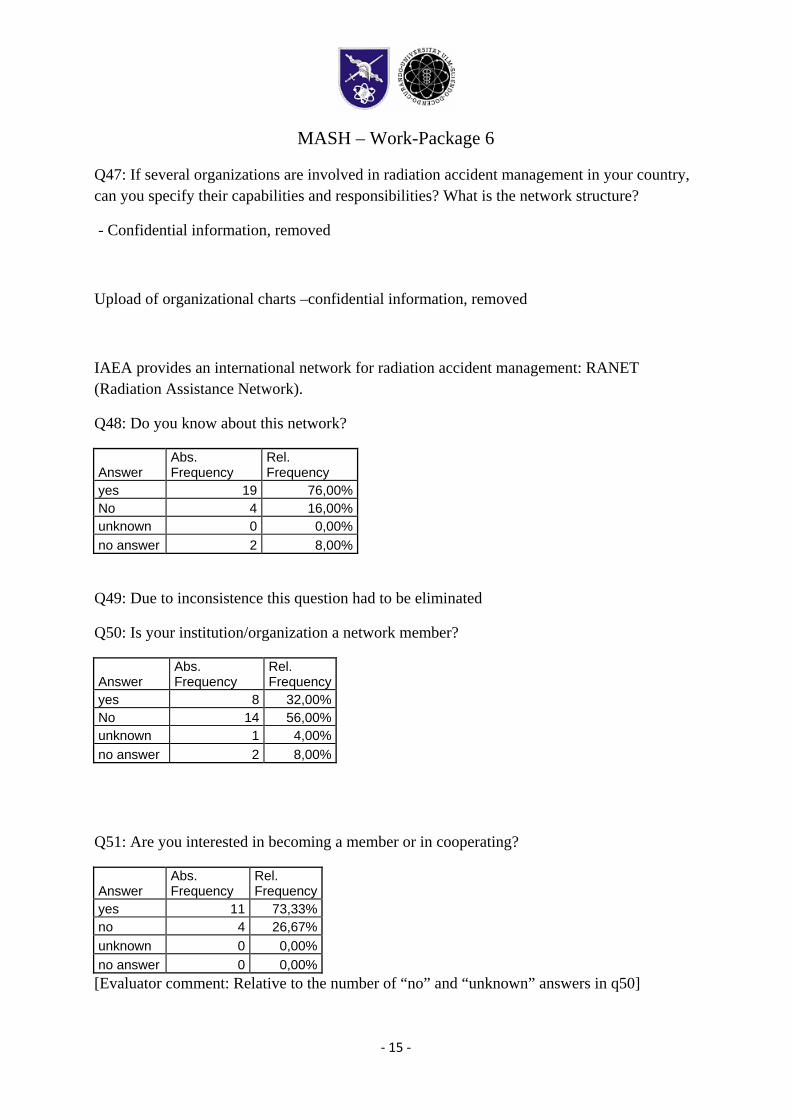
Q45: Are you interested in an EU-cooperation programme for educating such teams?
Answer Abs. Frequency
Rel. Frequency
yes 24 96,00%no 0 0,00%unknown 0 0,00%no answer 1 4,00%
Q46: How would you estimate the demand for such an educational programme in your country? (no of persons)
30 6 0 3 200 200 200 10 Depending on the target auditory 3 10 5 for XXXXX
5 for XXXXXXX 60 100 30 50-100 25 80
MASH – Work-Package 6
‐ 15 ‐
Q47: If several organizations are involved in radiation accident management in your country, can you specify their capabilities and responsibilities? What is the network structure?
- Confidential information, removed
Upload of organizational charts –confidential information, removed
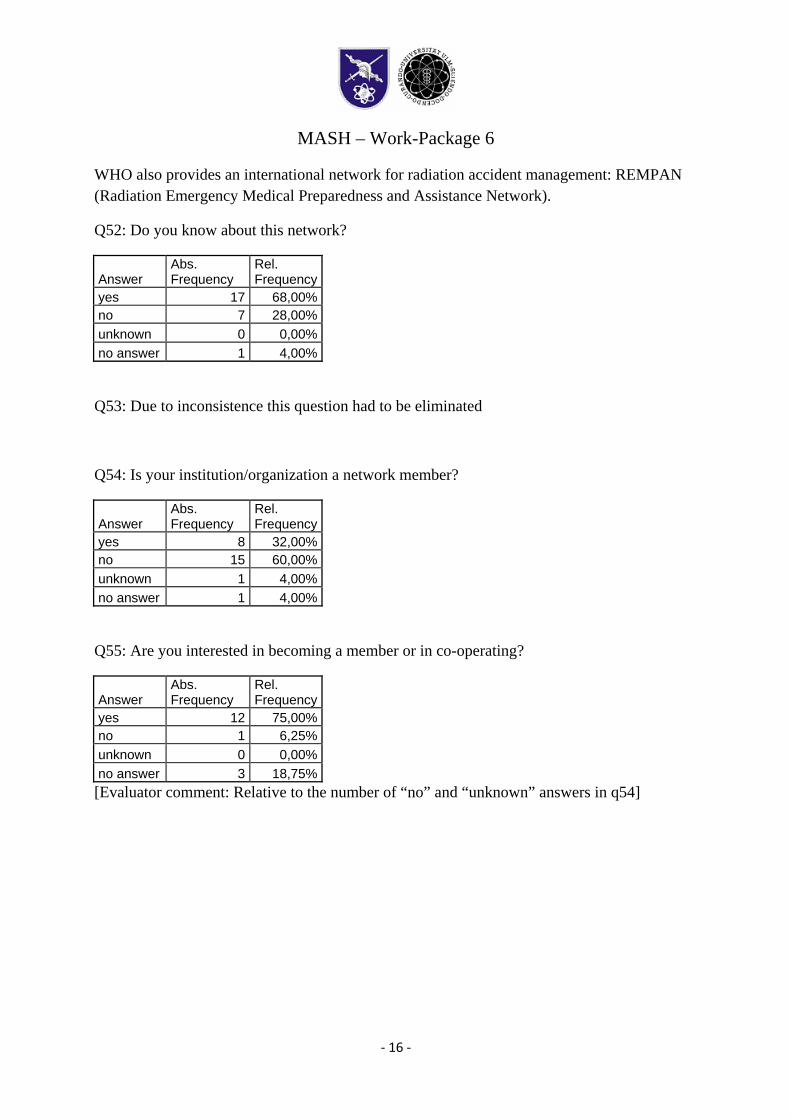
IAEA provides an international network for radiation accident management: RANET (Radiation Assistance Network).
Q48: Do you know about this network?
Answer Abs. Frequency
Rel. Frequency
yes 19 76,00%No 4 16,00%unknown 0 0,00%no answer 2 8,00%
Q49: Due to inconsistence this question had to be eliminated
Q50: Is your institution/organization a network member?
Answer Abs. Frequency
Rel. Frequency
yes 8 32,00%No 14 56,00%unknown 1 4,00%no answer 2 8,00%
Q51: Are you interested in becoming a member or in cooperating?
Answer Abs. Frequency
Rel. Frequency
yes 11 73,33% no 4 26,67% unknown 0 0,00% no answer 0 0,00% [Evaluator comment: Relative to the number of “no” and “unknown” answers in q50]
MASH – Work-Package 6
‐ 16 ‐
WHO also provides an international network for radiation accident management: REMPAN (Radiation Emergency Medical Preparedness and Assistance Network).
Q52: Do you know about this network?
Answer Abs. Frequency
Rel. Frequency
yes 17 68,00% no 7 28,00% unknown 0 0,00% no answer 1 4,00%
Q53: Due to inconsistence this question had to be eliminated
Q54: Is your institution/organization a network member?
Answer Abs. Frequency
Rel. Frequency
yes 8 32,00% no 15 60,00% unknown 1 4,00% no answer 1 4,00%
Q55: Are you interested in becoming a member or in co-operating?
Answer Abs. Frequency
Rel. Frequency
yes 12 75,00% no 1 6,25% unknown 0 0,00% no answer 3 18,75% [Evaluator comment: Relative to the number of “no” and “unknown” answers in q54]
MASH – Work-Package 6
‐ 17 ‐
2. Health system
[Evaluator’s comment:
The questions of part 2 are dealing with country based information. Therefore, the answers of the different person/institution based questionnaires had to be grouped by country. The first evaluation of these data showed that there are differences between questionnaires within the same country. The merging of these data was done using certain rules to provide transparency how the data were processed from the individual questionnaire to the country data set.
The following rules were applied:
A given valid answer dominates “no answer” or “unknown”.
If numbers were requested, the most optimistic number was used. The underlying assumption is that if e.g. expert A knows 2 specialized laboratories whereas expert B only knows 1, expert A has superior knowledge to expert B and the best information is the answer of expert A.
If for certain numbers the answer was e.g. “at least 1” this number was translated to exactly “1”. The underlying assumption is that if an expert knows at least 1 this means that he does not know 2, and thus the correct answer is 1.
The number of countries represented was 20. Therefore, percentages in part 2 are based on the number of 20 countries. ]
2.1. Pre-hospital triage/ Monitoring in case of a radiation accident
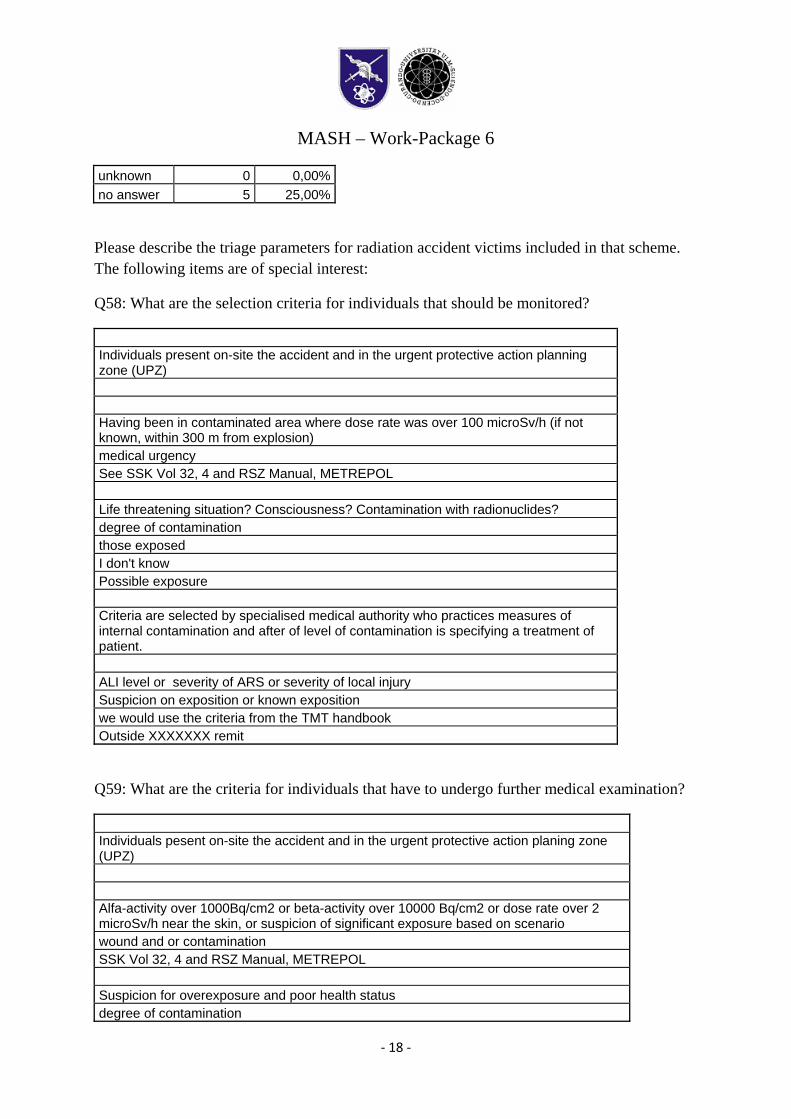
Q56: Is a scheme for pre-hospital examination/triage of patients available in your country?
Answer Abs. Frequency
Rel. Frequency
yes 14 70,00%no 4 20,00%unknown 0 0,00%no answer 2 10,00%
Q57: Is it standardized throughout the country?
Answer Abs. Frequency
Rel. Frequency
yes 9 45,00%no 6 30,00%
MASH – Work-Package 6
‐ 18 ‐
unknown 0 0,00%no answer 5 25,00%
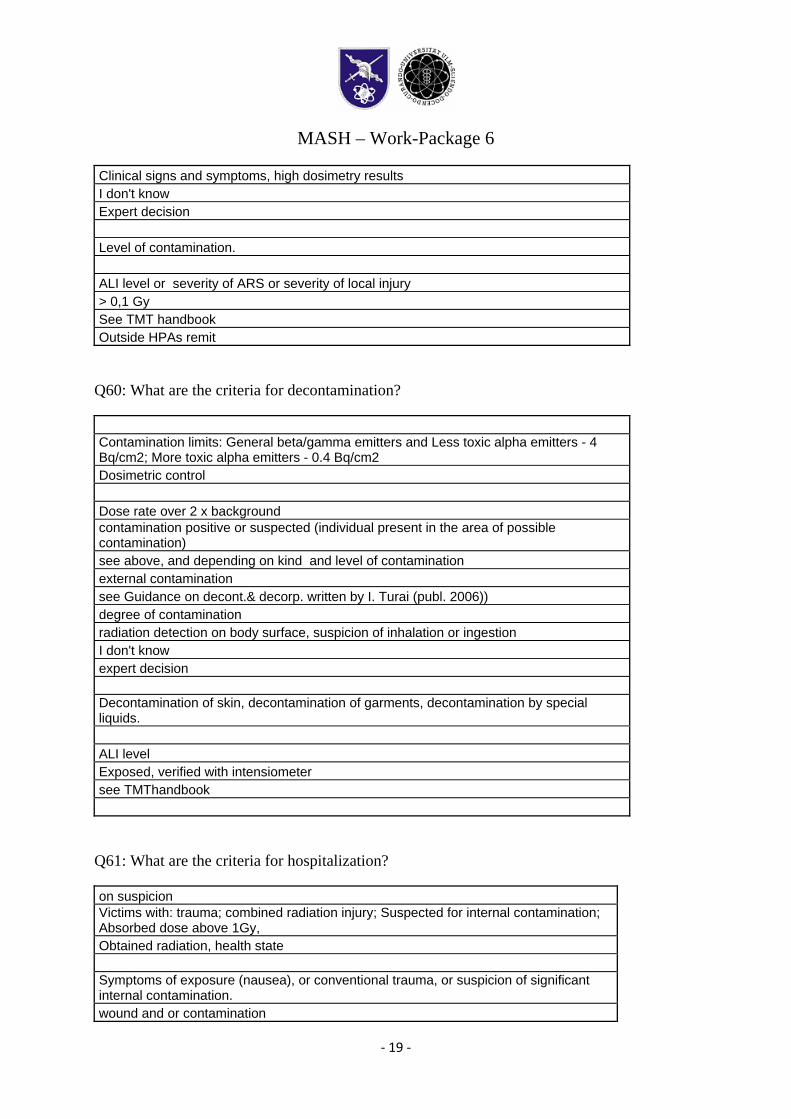
Please describe the triage parameters for radiation accident victims included in that scheme. The following items are of special interest:
Q58: What are the selection criteria for individuals that should be monitored?
Individuals present on-site the accident and in the urgent protective action planning zone (UPZ)
Having been in contaminated area where dose rate was over 100 microSv/h (if not known, within 300 m from explosion) medical urgency See SSK Vol 32, 4 and RSZ Manual, METREPOL Life threatening situation? Consciousness? Contamination with radionuclides? degree of contamination those exposed I don't know Possible exposure Criteria are selected by specialised medical authority who practices measures of internal contamination and after of level of contamination is specifying a treatment of patient. ALI level or severity of ARS or severity of local injury Suspicion on exposition or known exposition we would use the criteria from the TMT handbook Outside XXXXXXX remit
Q59: What are the criteria for individuals that have to undergo further medical examination?
Individuals pesent on-site the accident and in the urgent protective action planing zone (UPZ)
Alfa-activity over 1000Bq/cm2 or beta-activity over 10000 Bq/cm2 or dose rate over 2 microSv/h near the skin, or suspicion of significant exposure based on scenario wound and or contamination SSK Vol 32, 4 and RSZ Manual, METREPOL Suspicion for overexposure and poor health status degree of contamination
MASH – Work-Package 6
‐ 19 ‐
Clinical signs and symptoms, high dosimetry results I don't know Expert decision Level of contamination. ALI level or severity of ARS or severity of local injury > 0,1 Gy See TMT handbook Outside HPAs remit
Q60: What are the criteria for decontamination?
Contamination limits: General beta/gamma emitters and Less toxic alpha emitters - 4 Bq/cm2; More toxic alpha emitters - 0.4 Bq/cm2 Dosimetric control Dose rate over 2 x background contamination positive or suspected (individual present in the area of possible contamination) see above, and depending on kind and level of contamination external contamination see Guidance on decont.& decorp. written by I. Turai (publ. 2006)) degree of contamination radiation detection on body surface, suspicion of inhalation or ingestion I don't know expert decision Decontamination of skin, decontamination of garments, decontamination by special liquids. ALI level Exposed, verified with intensiometer see TMThandbook
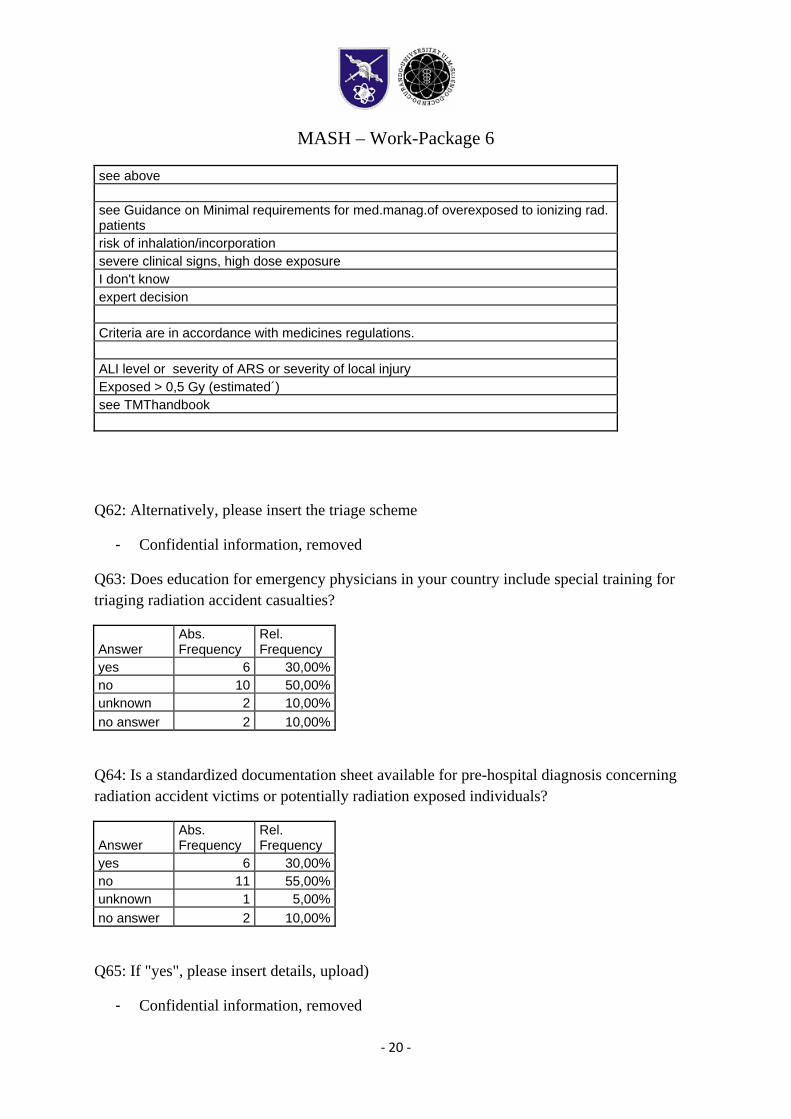
Q61: What are the criteria for hospitalization?
on suspicion Victims with: trauma; combined radiation injury; Suspected for internal contamination; Absorbed dose above 1Gy, Obtained radiation, health state Symptoms of exposure (nausea), or conventional trauma, or suspicion of significant internal contamination. wound and or contamination
MASH – Work-Package 6
‐ 20 ‐
see above see Guidance on Minimal requirements for med.manag.of overexposed to ionizing rad. patients risk of inhalation/incorporation severe clinical signs, high dose exposure I don't know expert decision Criteria are in accordance with medicines regulations. ALI level or severity of ARS or severity of local injury Exposed > 0,5 Gy (estimated´) see TMThandbook
Q62: Alternatively, please insert the triage scheme
- Confidential information, removed
Q63: Does education for emergency physicians in your country include special training for triaging radiation accident casualties?
Answer Abs. Frequency
Rel. Frequency
yes 6 30,00%no 10 50,00%unknown 2 10,00%no answer 2 10,00%
Q64: Is a standardized documentation sheet available for pre-hospital diagnosis concerning radiation accident victims or potentially radiation exposed individuals?
Answer Abs. Frequency
Rel. Frequency
yes 6 30,00%no 11 55,00%unknown 1 5,00%no answer 2 10,00%
Q65: If "yes", please insert details, upload)
- Confidential information, removed
MASH – Work-Package 6
‐ 21 ‐
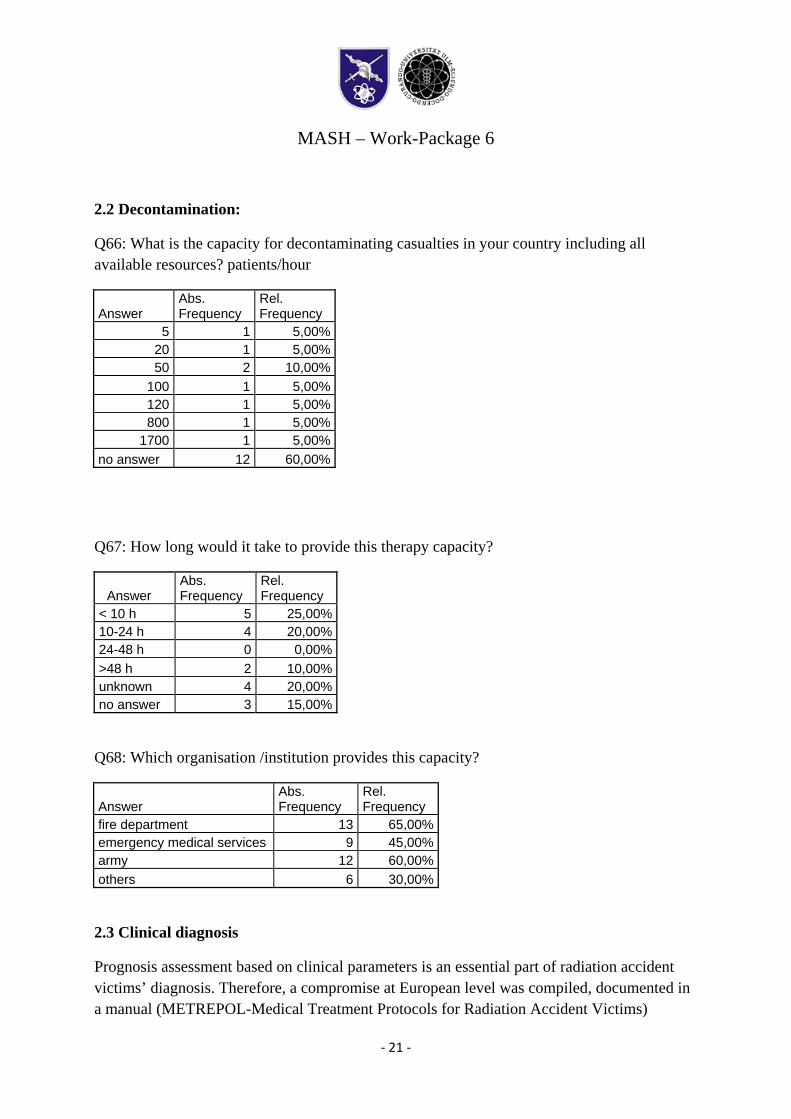
2.2 Decontamination:
Q66: What is the capacity for decontaminating casualties in your country including all available resources? patients/hour
Answer Abs. Frequency
Rel. Frequency
5 1 5,00%20 1 5,00%50 2 10,00%
100 1 5,00%120 1 5,00%800 1 5,00%
1700 1 5,00%no answer 12 60,00%
Q67: How long would it take to provide this therapy capacity?
Answer Abs. Frequency
Rel. Frequency
< 10 h 5 25,00%10-24 h 4 20,00%24-48 h 0 0,00%>48 h 2 10,00%unknown 4 20,00%no answer 3 15,00%
Q68: Which organisation /institution provides this capacity?
Answer Abs. Frequency
Rel. Frequency
fire department 13 65,00%emergency medical services 9 45,00%army 12 60,00%others 6 30,00%
2.3 Clinical diagnosis
Prognosis assessment based on clinical parameters is an essential part of radiation accident victims’ diagnosis. Therefore, a compromise at European level was compiled, documented in a manual (METREPOL-Medical Treatment Protocols for Radiation Accident Victims)
MASH – Work-Package 6
‐ 22 ‐
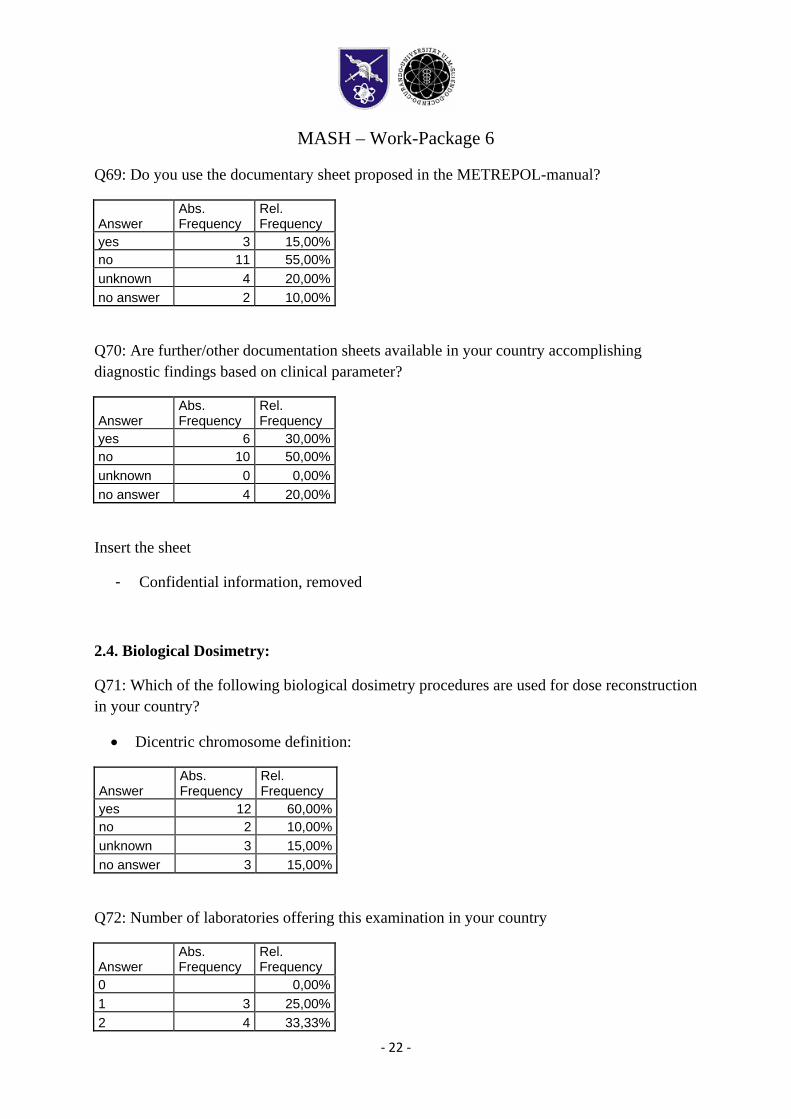
Q69: Do you use the documentary sheet proposed in the METREPOL-manual?
Answer Abs. Frequency
Rel. Frequency
yes 3 15,00%no 11 55,00%unknown 4 20,00%no answer 2 10,00%
Q70: Are further/other documentation sheets available in your country accomplishing diagnostic findings based on clinical parameter?
Answer Abs. Frequency
Rel. Frequency
yes 6 30,00%no 10 50,00%unknown 0 0,00%no answer 4 20,00%
Insert the sheet
- Confidential information, removed
2.4. Biological Dosimetry:
Q71: Which of the following biological dosimetry procedures are used for dose reconstruction in your country?
• Dicentric chromosome definition:
Answer Abs. Frequency
Rel. Frequency
yes 12 60,00%no 2 10,00%unknown 3 15,00%no answer 3 15,00%
Q72: Number of laboratories offering this examination in your country
Answer Abs. Frequency
Rel. Frequency
0 0,00%1 3 25,00%2 4 33,33%
MASH – Work-Package 6
‐ 23 ‐
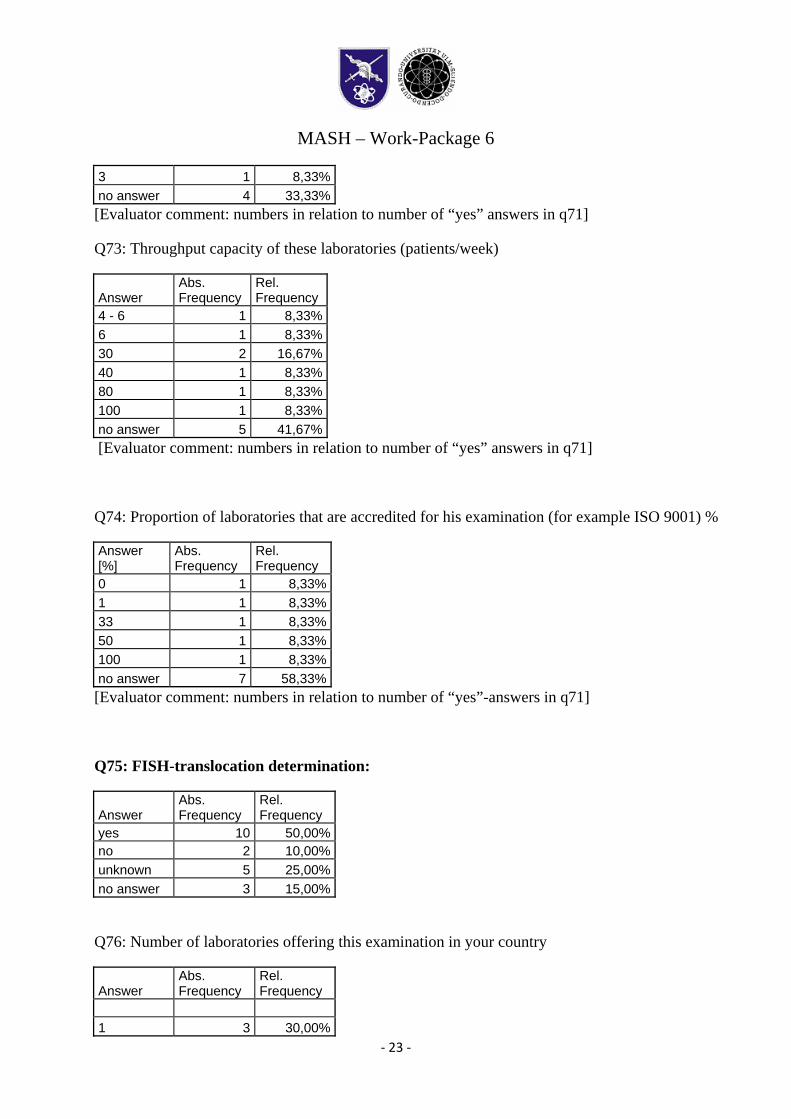
3 1 8,33%no answer 4 33,33%[Evaluator comment: numbers in relation to number of “yes” answers in q71]
Q73: Throughput capacity of these laboratories (patients/week)
Answer Abs. Frequency
Rel. Frequency
4 - 6 1 8,33% 6 1 8,33% 30 2 16,67% 40 1 8,33% 80 1 8,33% 100 1 8,33% no answer 5 41,67% [Evaluator comment: numbers in relation to number of “yes” answers in q71]
Q74: Proportion of laboratories that are accredited for his examination (for example ISO 9001) %
Answer [%]
Abs. Frequency
Rel. Frequency
0 1 8,33% 1 1 8,33% 33 1 8,33% 50 1 8,33% 100 1 8,33% no answer 7 58,33% [Evaluator comment: numbers in relation to number of “yes”-answers in q71]
Q75: FISH-translocation determination:
Answer Abs. Frequency
Rel. Frequency
yes 10 50,00%no 2 10,00%unknown 5 25,00%no answer 3 15,00%
Q76: Number of laboratories offering this examination in your country
Answer Abs. Frequency
Rel. Frequency
1 3 30,00%
MASH – Work-Package 6
‐ 24 ‐
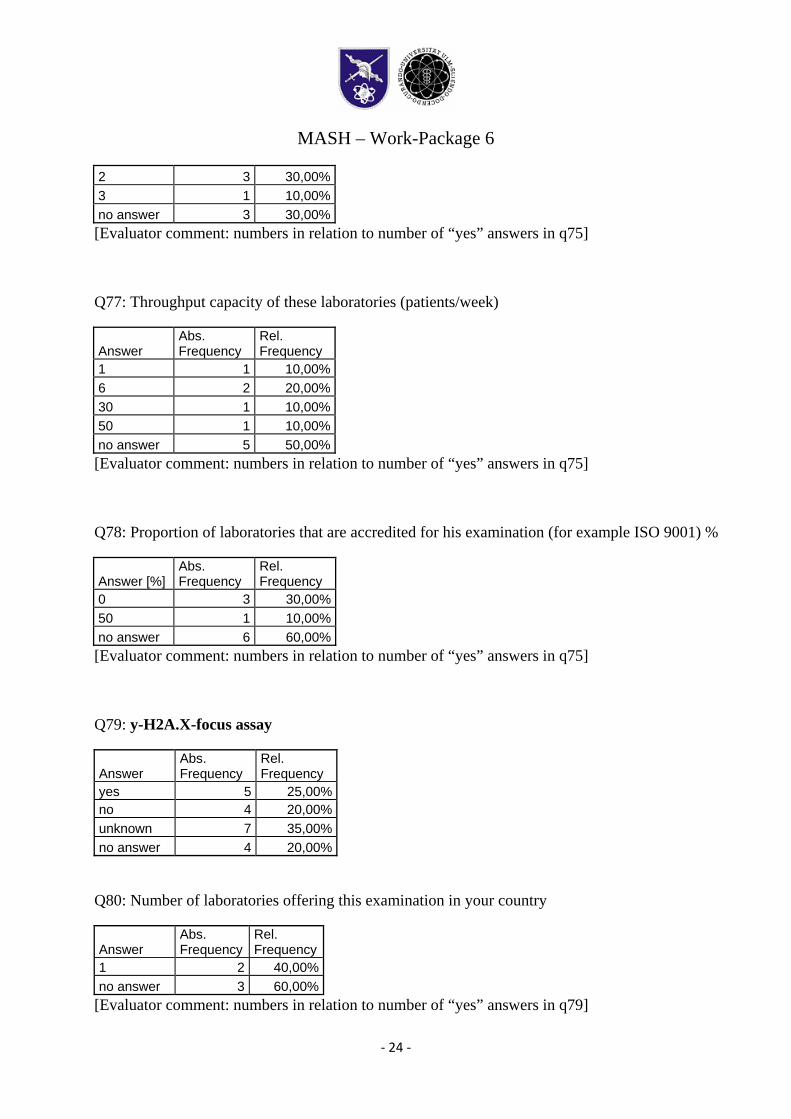
2 3 30,00%3 1 10,00%no answer 3 30,00%[Evaluator comment: numbers in relation to number of “yes” answers in q75]
Q77: Throughput capacity of these laboratories (patients/week)
Answer Abs. Frequency
Rel. Frequency
1 1 10,00%6 2 20,00%30 1 10,00%50 1 10,00%no answer 5 50,00%[Evaluator comment: numbers in relation to number of “yes” answers in q75]
Q78: Proportion of laboratories that are accredited for his examination (for example ISO 9001) %
Answer [%] Abs. Frequency
Rel. Frequency
0 3 30,00%50 1 10,00%no answer 6 60,00%[Evaluator comment: numbers in relation to number of “yes” answers in q75]
Q79: y-H2A.X-focus assay
Answer Abs. Frequency
Rel. Frequency
yes 5 25,00%no 4 20,00%unknown 7 35,00%no answer 4 20,00%
Q80: Number of laboratories offering this examination in your country
Answer Abs. Frequency
Rel. Frequency
1 2 40,00% no answer 3 60,00%
[Evaluator comment: numbers in relation to number of “yes” answers in q79]
MASH – Work-Package 6
‐ 25 ‐
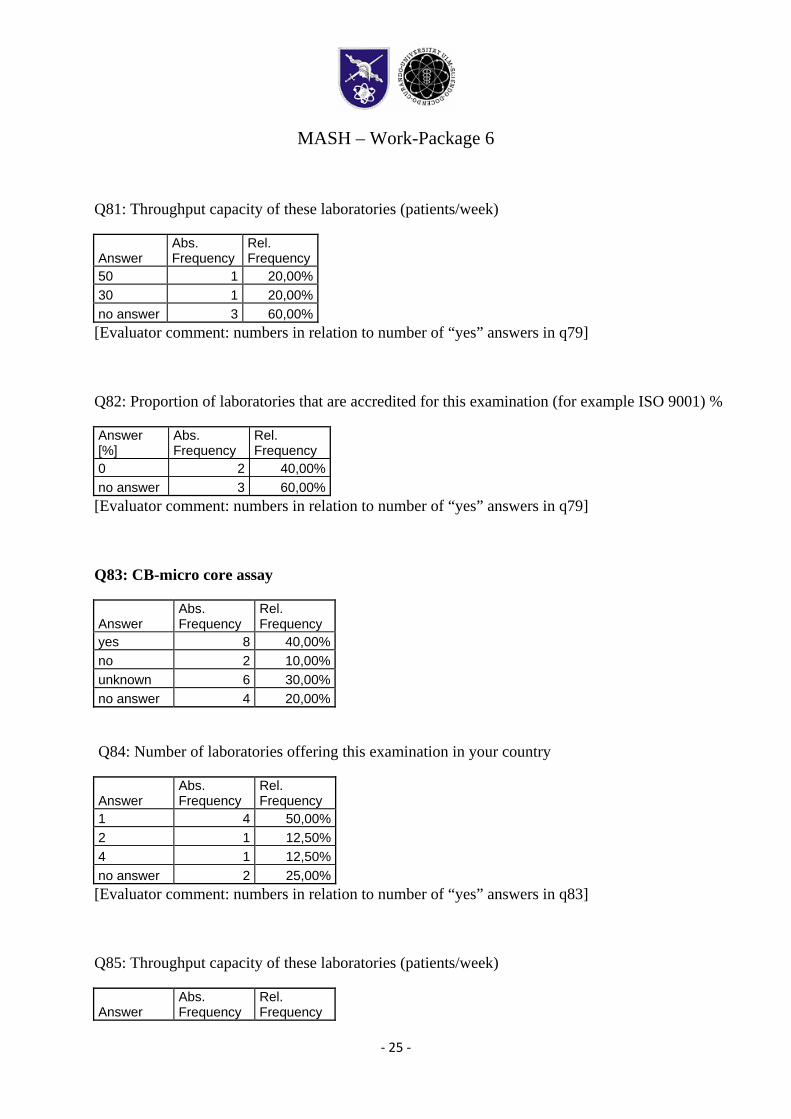
Q81: Throughput capacity of these laboratories (patients/week)
Answer Abs. Frequency
Rel. Frequency
50 1 20,00% 30 1 20,00% no answer 3 60,00% [Evaluator comment: numbers in relation to number of “yes” answers in q79]
Q82: Proportion of laboratories that are accredited for this examination (for example ISO 9001) %
Answer [%]
Abs. Frequency
Rel. Frequency
0 2 40,00% no answer 3 60,00% [Evaluator comment: numbers in relation to number of “yes” answers in q79]
Q83: CB-micro core assay
Answer Abs. Frequency
Rel. Frequency
yes 8 40,00%no 2 10,00%unknown 6 30,00%no answer 4 20,00%
Q84: Number of laboratories offering this examination in your country
Answer Abs. Frequency
Rel. Frequency
1 4 50,00%2 1 12,50%4 1 12,50%no answer 2 25,00%[Evaluator comment: numbers in relation to number of “yes” answers in q83]
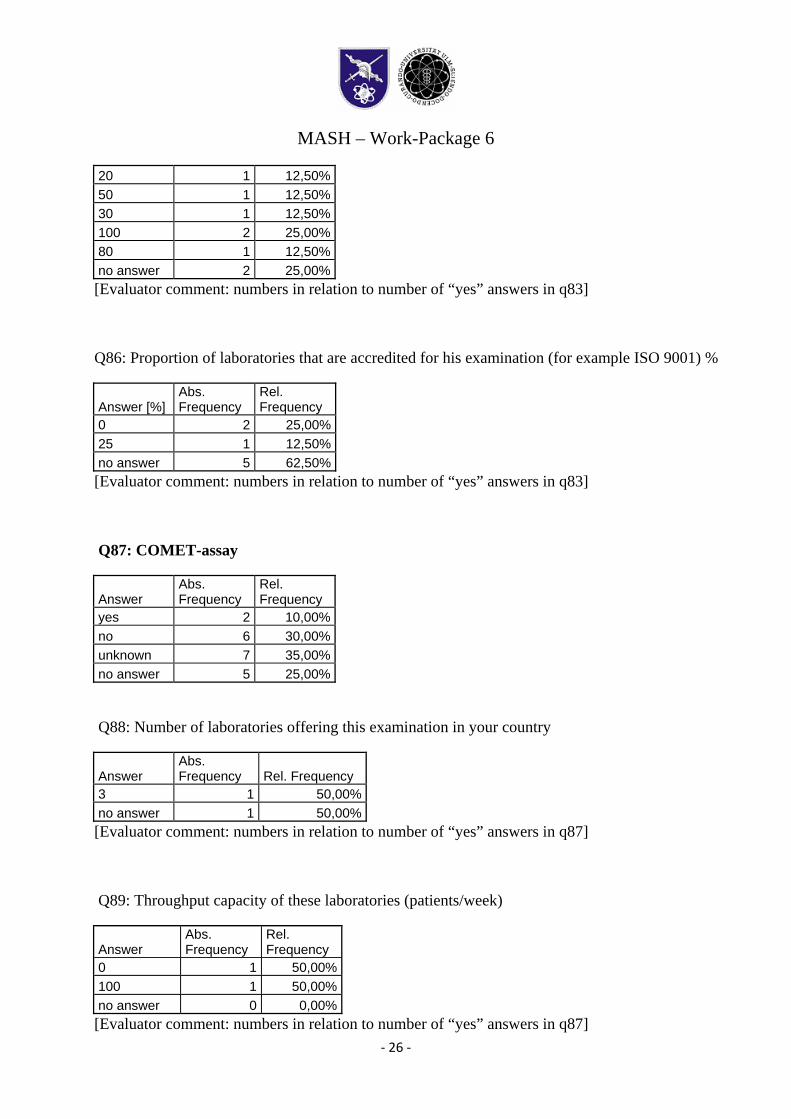
Q85: Throughput capacity of these laboratories (patients/week)
Answer Abs. Frequency
Rel. Frequency
MASH – Work-Package 6
‐ 26 ‐
20 1 12,50%50 1 12,50%30 1 12,50%100 2 25,00%80 1 12,50%no answer 2 25,00%[Evaluator comment: numbers in relation to number of “yes” answers in q83]
Q86: Proportion of laboratories that are accredited for his examination (for example ISO 9001) %
Answer [%] Abs. Frequency
Rel. Frequency
0 2 25,00%25 1 12,50%no answer 5 62,50%[Evaluator comment: numbers in relation to number of “yes” answers in q83]
Q87: COMET-assay
Answer Abs. Frequency
Rel. Frequency
yes 2 10,00%no 6 30,00%unknown 7 35,00%no answer 5 25,00%
Q88: Number of laboratories offering this examination in your country
Answer Abs. Frequency Rel. Frequency
3 1 50,00%no answer 1 50,00%[Evaluator comment: numbers in relation to number of “yes” answers in q87]
Q89: Throughput capacity of these laboratories (patients/week)
Answer Abs. Frequency
Rel. Frequency
0 1 50,00%100 1 50,00%no answer 0 0,00%[Evaluator comment: numbers in relation to number of “yes” answers in q87]
MASH – Work-Package 6
‐ 27 ‐
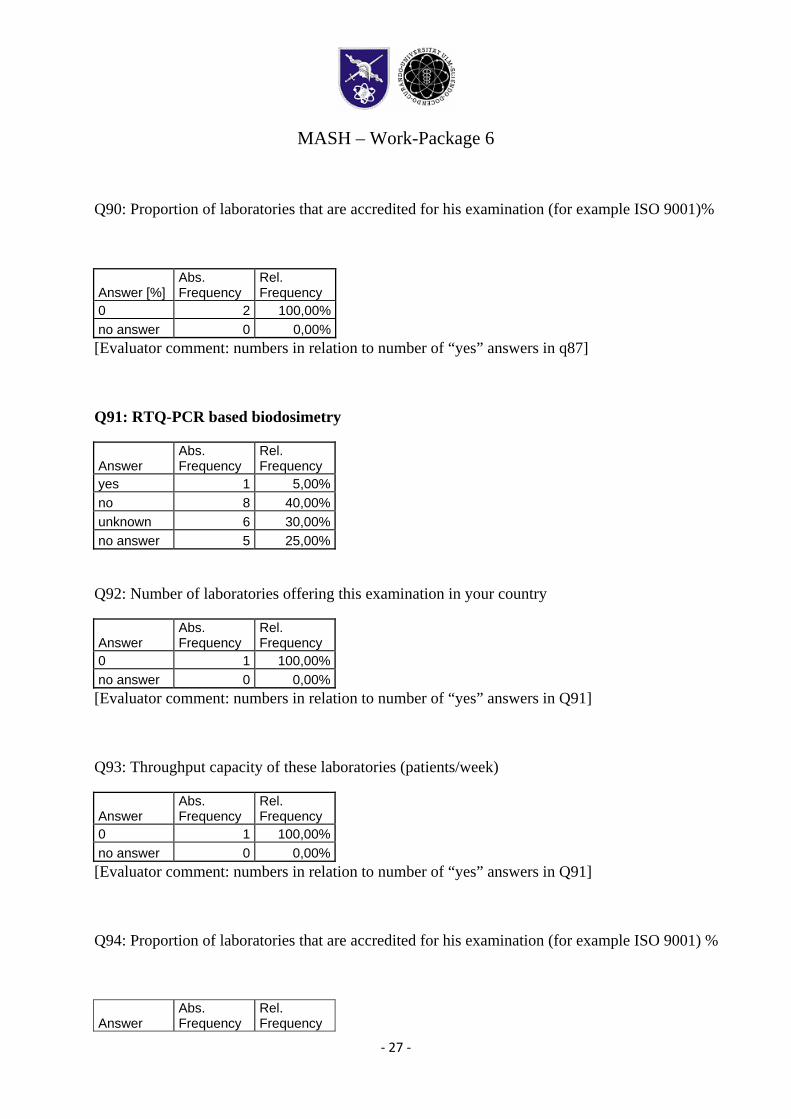
Q90: Proportion of laboratories that are accredited for his examination (for example ISO 9001)%
Answer [%] Abs. Frequency
Rel. Frequency
0 2 100,00%no answer 0 0,00%[Evaluator comment: numbers in relation to number of “yes” answers in q87]
Q91: RTQ-PCR based biodosimetry
Answer Abs. Frequency
Rel. Frequency
yes 1 5,00%no 8 40,00%unknown 6 30,00%no answer 5 25,00%
Q92: Number of laboratories offering this examination in your country
Answer Abs. Frequency
Rel. Frequency
0 1 100,00%no answer 0 0,00%[Evaluator comment: numbers in relation to number of “yes” answers in Q91]
Q93: Throughput capacity of these laboratories (patients/week)
Answer Abs. Frequency
Rel. Frequency
0 1 100,00%no answer 0 0,00%[Evaluator comment: numbers in relation to number of “yes” answers in Q91]
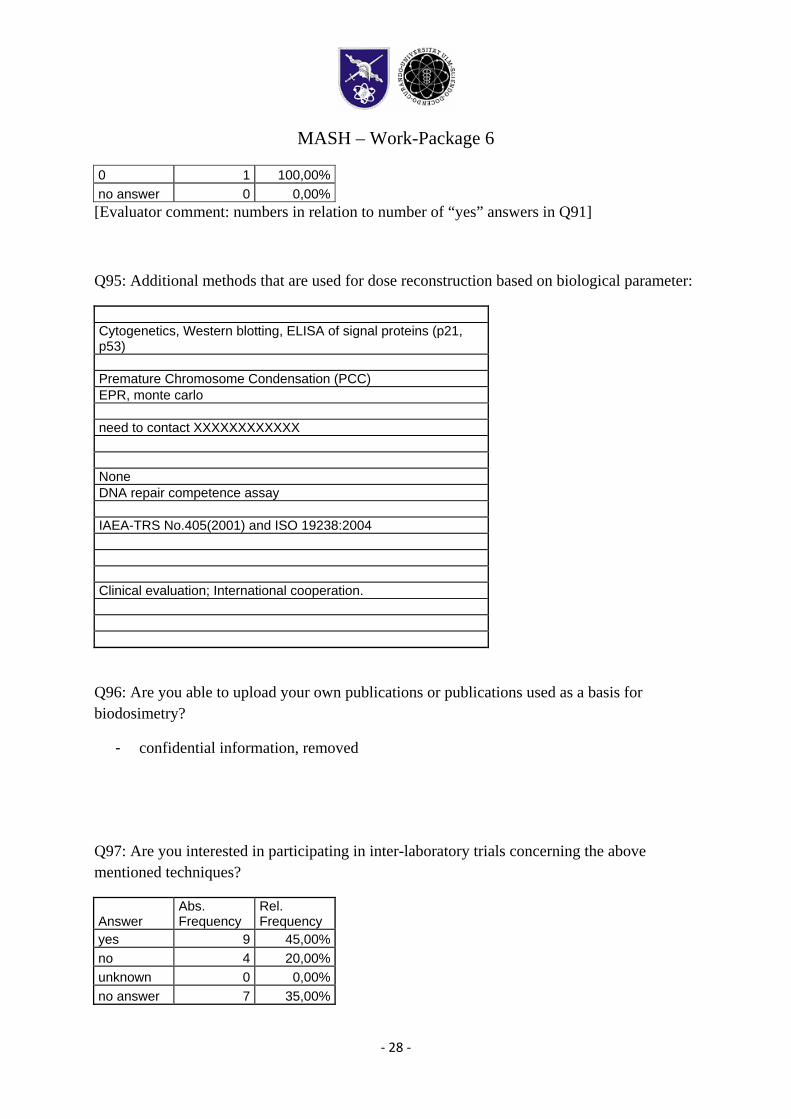
Q94: Proportion of laboratories that are accredited for his examination (for example ISO 9001) %
Answer Abs. Frequency
Rel. Frequency
MASH – Work-Package 6
‐ 28 ‐
0 1 100,00%no answer 0 0,00%[Evaluator comment: numbers in relation to number of “yes” answers in Q91]
Q95: Additional methods that are used for dose reconstruction based on biological parameter:
Cytogenetics, Western blotting, ELISA of signal proteins (p21, p53) Premature Chromosome Condensation (PCC) EPR, monte carlo need to contact XXXXXXXXXXXX None DNA repair competence assay IAEA-TRS No.405(2001) and ISO 19238:2004 Clinical evaluation; International cooperation.
Q96: Are you able to upload your own publications or publications used as a basis for biodosimetry?
- confidential information, removed
Q97: Are you interested in participating in inter-laboratory trials concerning the above mentioned techniques?
Answer Abs. Frequency
Rel. Frequency
yes 9 45,00%no 4 20,00%unknown 0 0,00%no answer 7 35,00%
MASH – Work-Package 6
‐ 29 ‐
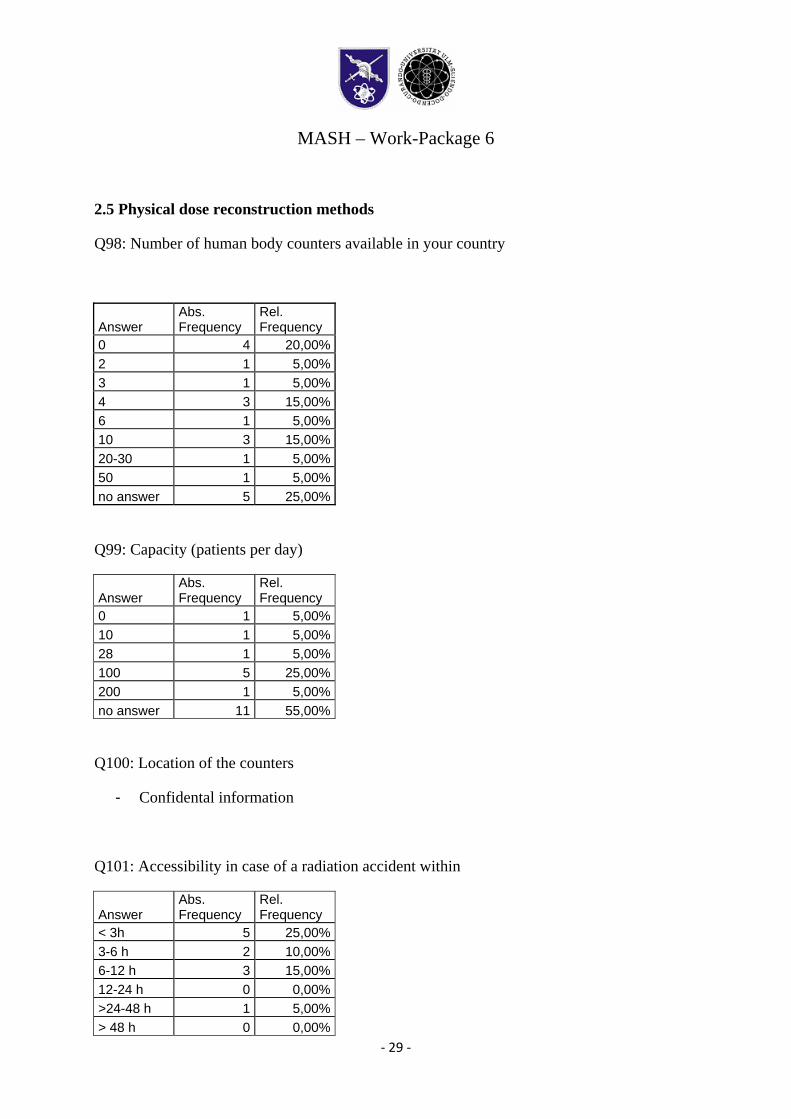
2.5 Physical dose reconstruction methods
Q98: Number of human body counters available in your country
Answer Abs. Frequency
Rel. Frequency
0 4 20,00%2 1 5,00%3 1 5,00%4 3 15,00%6 1 5,00%10 3 15,00%20-30 1 5,00%50 1 5,00%no answer 5 25,00%
Q99: Capacity (patients per day)
Answer Abs. Frequency
Rel. Frequency
0 1 5,00%10 1 5,00%28 1 5,00%100 5 25,00%200 1 5,00%no answer 11 55,00%
Q100: Location of the counters
- Confidental information
Q101: Accessibility in case of a radiation accident within
Answer Abs. Frequency
Rel. Frequency
< 3h 5 25,00%3-6 h 2 10,00%6-12 h 3 15,00%12-24 h 0 0,00%>24-48 h 1 5,00%> 48 h 0 0,00%
MASH – Work-Package 6
‐ 30 ‐
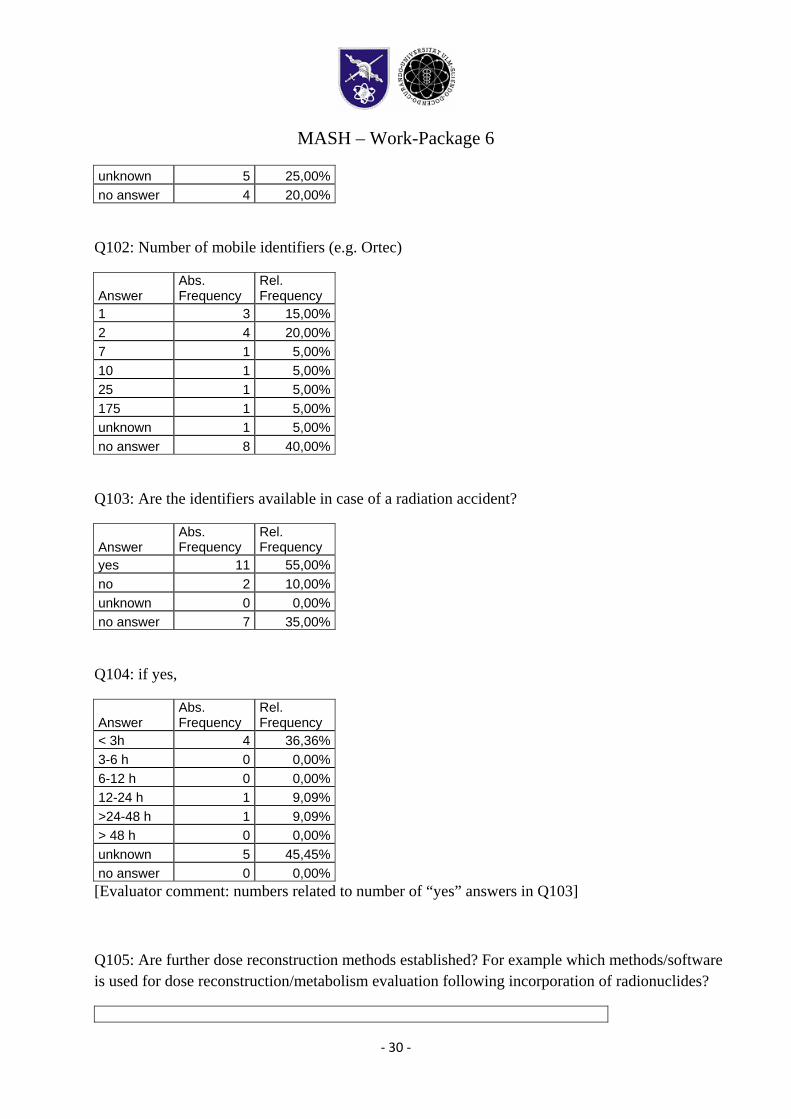
unknown 5 25,00%no answer 4 20,00%
Q102: Number of mobile identifiers (e.g. Ortec)
Answer Abs. Frequency
Rel. Frequency
1 3 15,00%2 4 20,00%7 1 5,00%10 1 5,00%25 1 5,00%175 1 5,00%unknown 1 5,00%no answer 8 40,00%
Q103: Are the identifiers available in case of a radiation accident?
Answer Abs. Frequency
Rel. Frequency
yes 11 55,00%no 2 10,00%unknown 0 0,00%no answer 7 35,00%
Q104: if yes,
Answer Abs. Frequency
Rel. Frequency
< 3h 4 36,36%3-6 h 0 0,00%6-12 h 0 0,00%12-24 h 1 9,09%>24-48 h 1 9,09%> 48 h 0 0,00%unknown 5 45,45%no answer 0 0,00%[Evaluator comment: numbers related to number of “yes” answers in Q103]
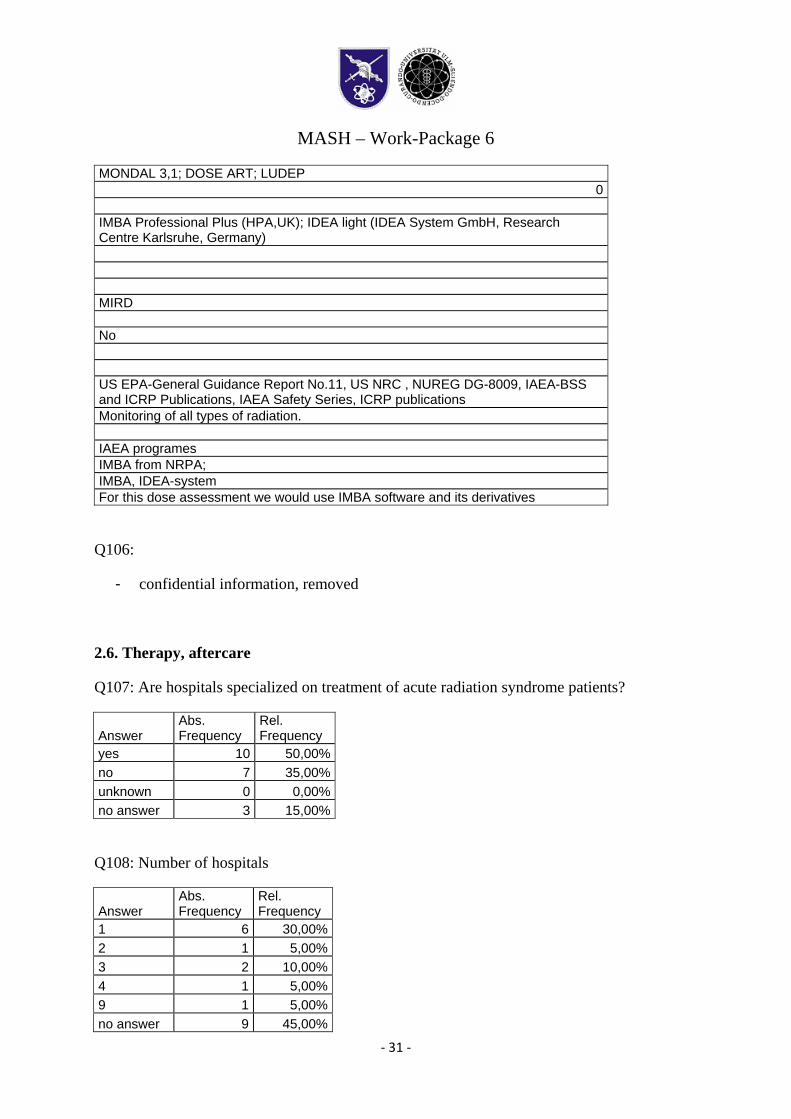
Q105: Are further dose reconstruction methods established? For example which methods/software is used for dose reconstruction/metabolism evaluation following incorporation of radionuclides?
MASH – Work-Package 6
‐ 31 ‐
MONDAL 3,1; DOSE ART; LUDEP 0
IMBA Professional Plus (HPA,UK); IDEA light (IDEA System GmbH, Research Centre Karlsruhe, Germany) MIRD No US EPA-General Guidance Report No.11, US NRC , NUREG DG-8009, IAEA-BSS and ICRP Publications, IAEA Safety Series, ICRP publications Monitoring of all types of radiation. IAEA programes IMBA from NRPA; IMBA, IDEA-system For this dose assessment we would use IMBA software and its derivatives
Q106:
- confidential information, removed
2.6. Therapy, aftercare
Q107: Are hospitals specialized on treatment of acute radiation syndrome patients?
Answer Abs. Frequency
Rel. Frequency
yes 10 50,00%no 7 35,00%unknown 0 0,00%no answer 3 15,00%
Q108: Number of hospitals
Answer Abs. Frequency
Rel. Frequency
1 6 30,00%2 1 5,00%3 2 10,00%4 1 5,00%9 1 5,00%no answer 9 45,00%
MASH – Work-Package 6
‐ 32 ‐
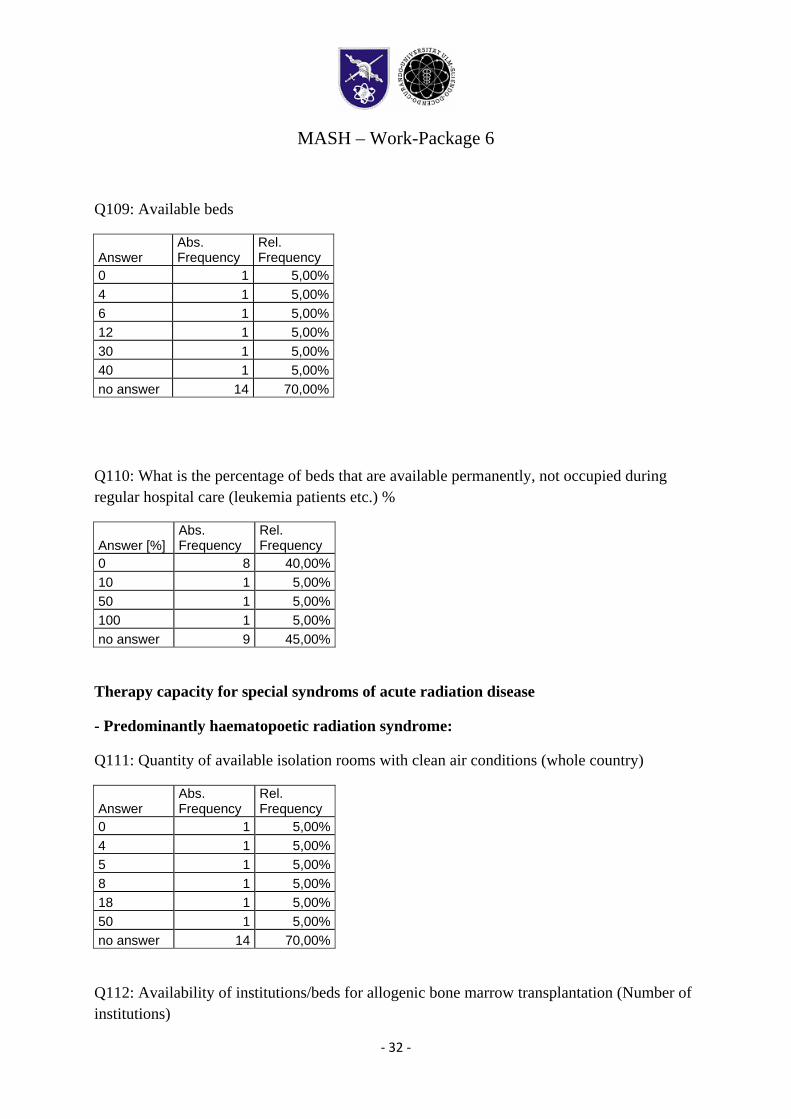
Q109: Available beds
Answer Abs. Frequency
Rel. Frequency
0 1 5,00%4 1 5,00%6 1 5,00%12 1 5,00%30 1 5,00%40 1 5,00%no answer 14 70,00%
Q110: What is the percentage of beds that are available permanently, not occupied during regular hospital care (leukemia patients etc.) %
Answer [%] Abs. Frequency
Rel. Frequency
0 8 40,00%10 1 5,00%50 1 5,00%100 1 5,00%no answer 9 45,00%
Therapy capacity for special syndroms of acute radiation disease
- Predominantly haematopoetic radiation syndrome:
Q111: Quantity of available isolation rooms with clean air conditions (whole country)
Answer Abs. Frequency
Rel. Frequency
0 1 5,00%4 1 5,00%5 1 5,00%8 1 5,00%18 1 5,00%50 1 5,00%no answer 14 70,00%
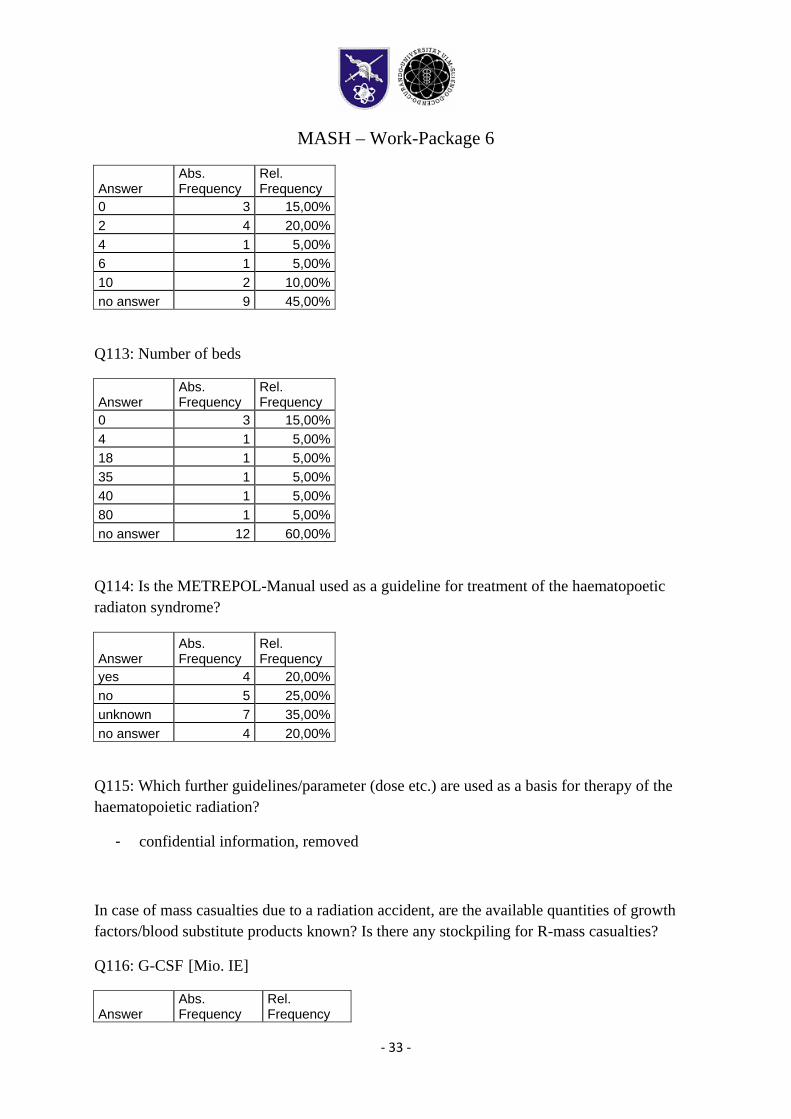
Q112: Availability of institutions/beds for allogenic bone marrow transplantation (Number of institutions)
MASH – Work-Package 6
‐ 33 ‐
Answer Abs. Frequency
Rel. Frequency
0 3 15,00%2 4 20,00%4 1 5,00%6 1 5,00%10 2 10,00%no answer 9 45,00%
Q113: Number of beds
Answer Abs. Frequency
Rel. Frequency
0 3 15,00%4 1 5,00%18 1 5,00%35 1 5,00%40 1 5,00%80 1 5,00%no answer 12 60,00%
Q114: Is the METREPOL-Manual used as a guideline for treatment of the haematopoetic radiaton syndrome?
Answer
Abs. Frequency
Rel. Frequency
yes 4 20,00%no 5 25,00%unknown 7 35,00%no answer 4 20,00%
Q115: Which further guidelines/parameter (dose etc.) are used as a basis for therapy of the haematopoietic radiation?
- confidential information, removed
In case of mass casualties due to a radiation accident, are the available quantities of growth factors/blood substitute products known? Is there any stockpiling for R-mass casualties?
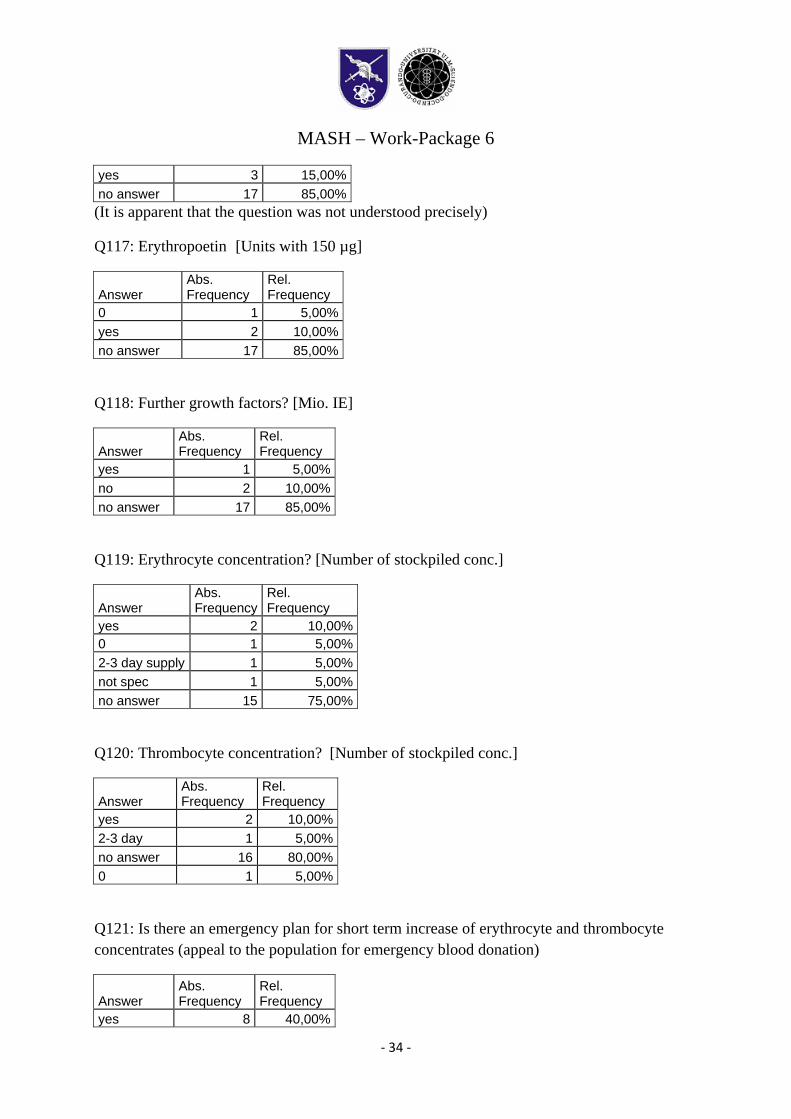
Q116: G-CSF [Mio. IE]
Answer Abs. Frequency
Rel. Frequency
MASH – Work-Package 6
‐ 34 ‐
yes 3 15,00%no answer 17 85,00%(It is apparent that the question was not understood precisely)
Q117: Erythropoetin [Units with 150 µg]
Answer Abs. Frequency
Rel. Frequency
0 1 5,00%yes 2 10,00%no answer 17 85,00%
Q118: Further growth factors? [Mio. IE]
Answer Abs. Frequency
Rel. Frequency
yes 1 5,00%no 2 10,00%no answer 17 85,00%
Q119: Erythrocyte concentration? [Number of stockpiled conc.]
Answer Abs. Frequency
Rel. Frequency
yes 2 10,00%0 1 5,00%2-3 day supply 1 5,00%not spec 1 5,00%no answer 15 75,00%
Q120: Thrombocyte concentration? [Number of stockpiled conc.]
Answer Abs. Frequency
Rel. Frequency
yes 2 10,00%2-3 day 1 5,00%no answer 16 80,00%0 1 5,00%
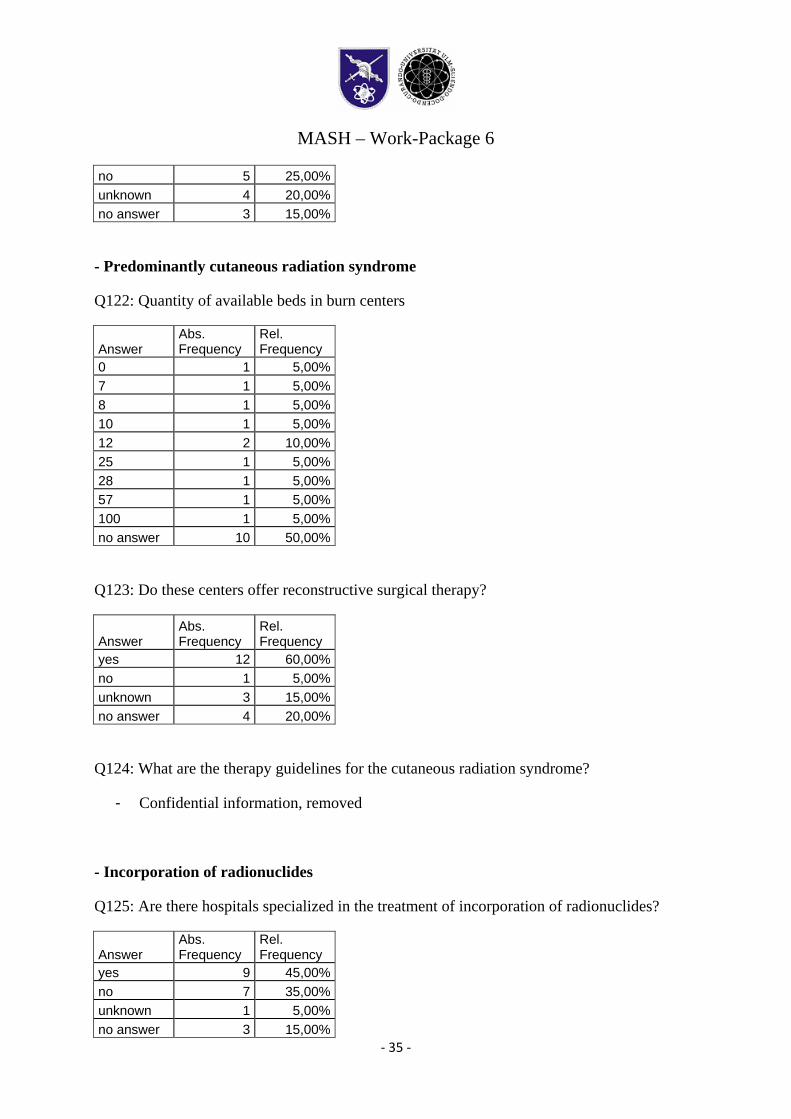
Q121: Is there an emergency plan for short term increase of erythrocyte and thrombocyte concentrates (appeal to the population for emergency blood donation)
Answer
Abs. Frequency
Rel. Frequency
yes 8 40,00%
MASH – Work-Package 6
‐ 35 ‐
no 5 25,00%unknown 4 20,00%no answer 3 15,00%
- Predominantly cutaneous radiation syndrome
Q122: Quantity of available beds in burn centers
Answer Abs. Frequency
Rel. Frequency
0 1 5,00%7 1 5,00%8 1 5,00%10 1 5,00%12 2 10,00%25 1 5,00%28 1 5,00%57 1 5,00%100 1 5,00%no answer 10 50,00%
Q123: Do these centers offer reconstructive surgical therapy?
Answer
Abs. Frequency
Rel. Frequency
yes 12 60,00%no 1 5,00%unknown 3 15,00%no answer 4 20,00%
Q124: What are the therapy guidelines for the cutaneous radiation syndrome?
- Confidential information, removed
- Incorporation of radionuclides
Q125: Are there hospitals specialized in the treatment of incorporation of radionuclides?
Answer Abs. Frequency
Rel. Frequency
yes 9 45,00%no 7 35,00%unknown 1 5,00%no answer 3 15,00%
MASH – Work-Package 6
‐ 36 ‐
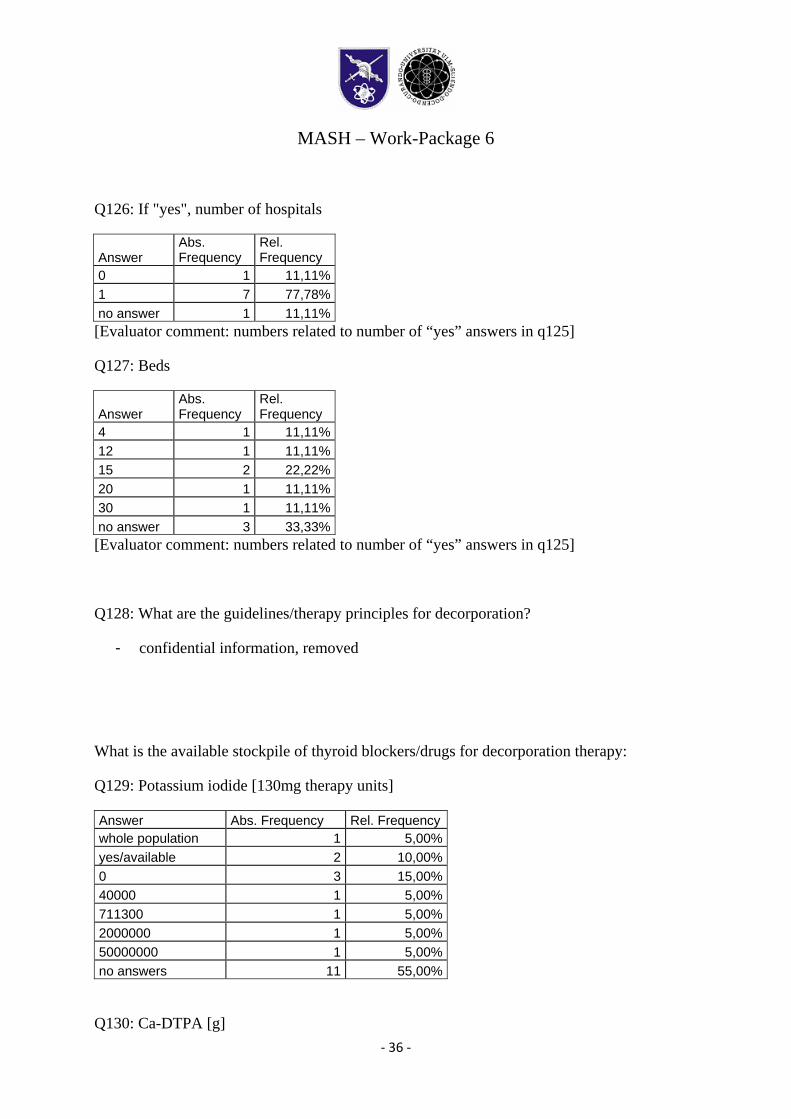
Q126: If "yes", number of hospitals
Answer Abs. Frequency
Rel. Frequency
0 1 11,11%1 7 77,78%no answer 1 11,11%[Evaluator comment: numbers related to number of “yes” answers in q125]
Q127: Beds
Answer Abs. Frequency
Rel. Frequency
4 1 11,11%12 1 11,11%15 2 22,22%20 1 11,11%30 1 11,11%no answer 3 33,33%[Evaluator comment: numbers related to number of “yes” answers in q125]
Q128: What are the guidelines/therapy principles for decorporation?
- confidential information, removed
What is the available stockpile of thyroid blockers/drugs for decorporation therapy:
Q129: Potassium iodide [130mg therapy units]
Answer Abs. Frequency Rel. Frequencywhole population 1 5,00%yes/available 2 10,00%0 3 15,00%40000 1 5,00%711300 1 5,00%2000000 1 5,00%50000000 1 5,00%no answers 11 55,00%
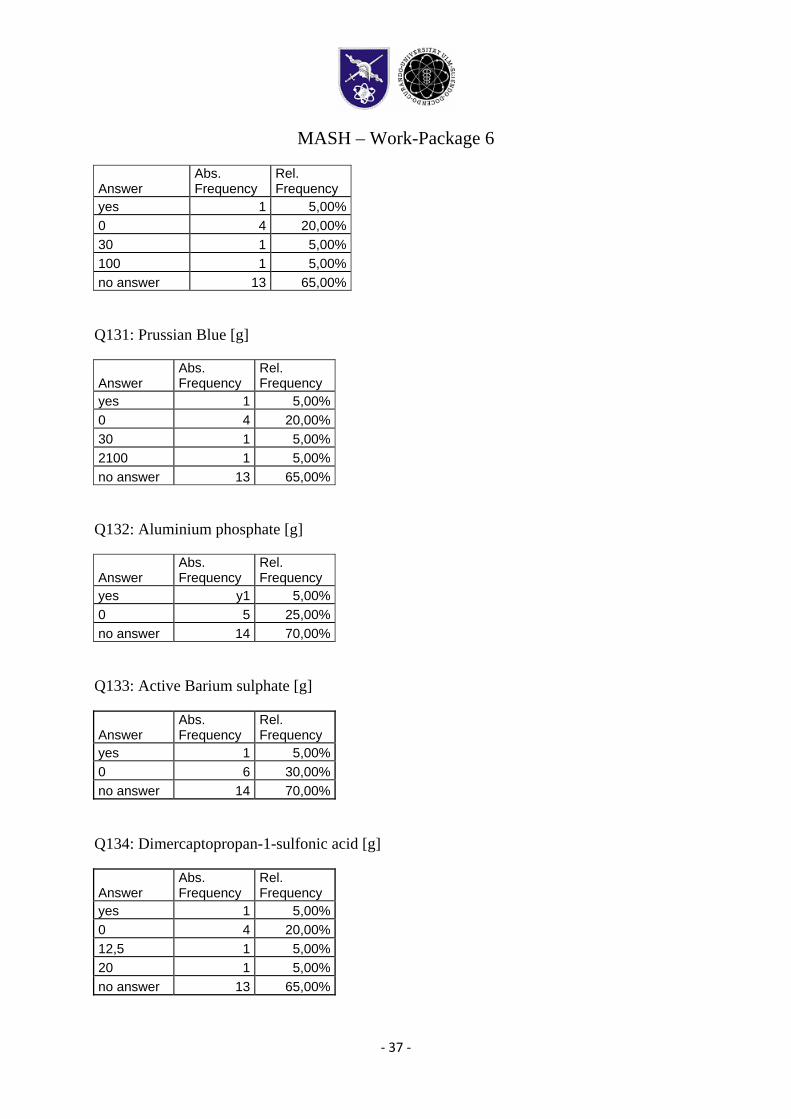
Q130: Ca-DTPA [g]
MASH – Work-Package 6
‐ 37 ‐
Answer Abs. Frequency
Rel. Frequency
yes 1 5,00%0 4 20,00%30 1 5,00%100 1 5,00%no answer 13 65,00%
Q131: Prussian Blue [g]
Answer Abs. Frequency
Rel. Frequency
yes 1 5,00%0 4 20,00%30 1 5,00%2100 1 5,00%no answer 13 65,00%
Q132: Aluminium phosphate [g]
Answer Abs. Frequency
Rel. Frequency
yes y1 5,00%0 5 25,00%no answer 14 70,00%
Q133: Active Barium sulphate [g]
Answer Abs. Frequency
Rel. Frequency
yes 1 5,00%0 6 30,00%no answer 14 70,00%
Q134: Dimercaptopropan-1-sulfonic acid [g]
Answer Abs. Frequency
Rel. Frequency
yes 1 5,00%0 4 20,00%12,5 1 5,00%20 1 5,00%no answer 13 65,00%
MASH – Work-Package 6
‐ 38 ‐
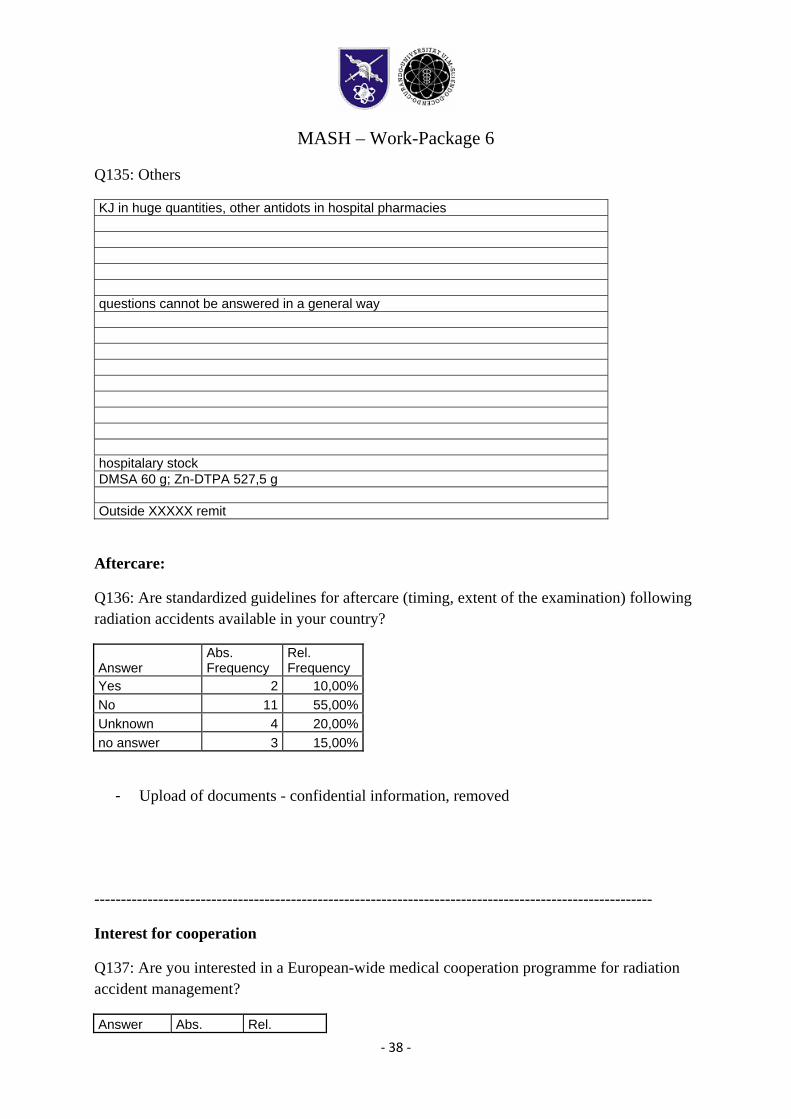
Q135: Others
KJ in huge quantities, other antidots in hospital pharmacies
questions cannot be answered in a general way hospitalary stock DMSA 60 g; Zn-DTPA 527,5 g Outside XXXXX remit
Aftercare:
Q136: Are standardized guidelines for aftercare (timing, extent of the examination) following radiation accidents available in your country?
Answer Abs. Frequency
Rel. Frequency
Yes 2 10,00%No 11 55,00%Unknown 4 20,00%no answer 3 15,00%
- Upload of documents - confidential information, removed
---------------------------------------------------------------------------------------------------------
Interest for cooperation
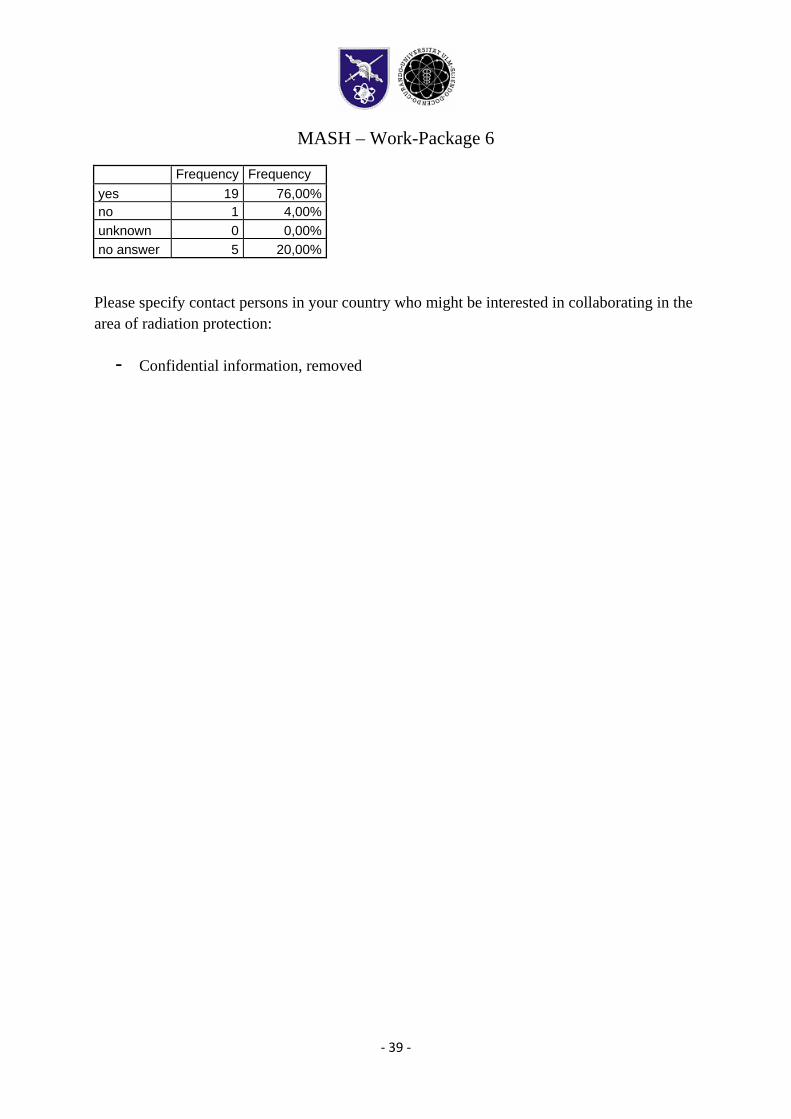
Q137: Are you interested in a European-wide medical cooperation programme for radiation accident management?
Answer Abs. Rel.
MASH – Work-Package 6
‐ 39 ‐
Frequency Frequency yes 19 76,00% no 1 4,00% unknown 0 0,00% no answer 5 20,00%
Please specify contact persons in your country who might be interested in collaborating in the area of radiation protection:
- Confidential information, removed
MASH – Work-Package 6
‐ 40 ‐
Interpretation of the received data.
Introductory remarks
It is not intended to give interpretation to every single point of the questionnaire. This is the task of different experts in different fields of science and disaster preparedness. Instead, this interpretation will concentrate more on the meta information that can be extracted out of received data and what conclusions can be drawn from that.
Response to the questionnaire
About 40 organizations that are involved directly or indirectly in the radiation mass casualty management in the 27 Member States of the European Union declared their preparedness to to fill in the questionnaire. Finally, 25 Representatives from 20 countries replied to the questionnaire. 8 announced their interest to participate but did not provide any information despite repeated requests.
Only a minority of the participants was able to answer all questions.
I Organizational Structures:
60 % of the contacted institutions are able to assume control for the coordination of R-mass casualties. Also, for 60% of the countries covered by the received questionnaires there was an institution capable to assume control of R-mass casualties (Q23). That implies directly, that 40% of the countries can not be assessed by the WP6 questionnaires, since it is not apparent if there are such institutions or not. Further work should be done on that question.
70%-80% (q25-q28) of the responding institutions are known to the main emergency services for their availability in the case of an accent. 76% of the responding institutions can provide expert teams for radiation accidents (Q41). Thus, the contacted institutions hold a high level of “reputation” in the field of radiation accidents and can be regarded to be experts in their field.
About 30% of the contacted institutions are members of RANET or REMPAN, 75% of the nonmembers are interested in participating in these networks. Thus, international cooperation is seen as an essential factor in radiation emergency preparedness. (q48 ff)
MASH – Work-Package 6
‐ 41 ‐
II Health System
In a surprisingly high fraction of 70% of the responding countries there are schemes for pre-hospital examination available, whereas only in 45% of these countries one standardized scheme is used for the whole country.
The more detailed questions of part II identify all over a great lack of knowledge on the real quantitative characteristics of the R-mass casualty reaction systems on the national level. Some of these questions could be - in principle – be answered on a national level if a responsible or an insitution would gather all the distributed information among e.g. bloodbanks and other suitable health care institutions.
Many questions dealing with exact capacities in numbers could not be answered by a great part of the responders.
In 60% of the responding countries, no decontamination capacity was entered.
Especially for biological dosimetry, the lack of precise knowledge is obvious: Only 70% of the countries have reported capacities for dicentric chromosome method, 50% FISH and for other methods the rate drops below 25%.
The questionnaire requested detailed information on stockpiling of decorporation drugs. Only a minority of 30 % of the participating institutions was able to provide detailed information on stockpiling. 10 % had information, that there is some stockpiling in their country but were not able to provide detailed information. About 60 % were not able to provide any information on stockpiling.
REMPAN network (WHO): About 70 % of the participants are aware of this network, 35 % are members of the network and 85 % of the rest are interest in a membership.
RANET (IAEA): About 80 % of the participants are aware of this network, 40 % are members of this network and 60 % of the rest is interested in a membership.
A majority of more than 90 % of the participants is interested in a European cooperation programme for a radiation accident management system.
Contact Data Sets
15 additional contact data sets of responsible persons could be acquired.
16 contact data sets of interested collaboration persons were received within the questionnaires.
MASH – Work-Package 6
‐ 42 ‐
Concluding Remarks
- Although we were able to gather information from 25 organizations from 20 countries of the EU 27, only very few were able to answer all questions of our questionnaire.
- Reasons which can be responsible for this lack of information: o The contacted institution may be not able to provide the information. o The contacted institution does not have motivation to provide the information o The contacted institution is not willing or is not allowed to provide information
due to reasons of internal politics, classification rules or other reasons. - The essential prerequisites to handle radiation mass casualties (expert teams,
decontamination units, biological dosimetry etc.) are available in most participating countries. Further training and especially standardization of the documentation is necessary.
- Capacities for new approaches in biodosimetry especially with the possibility to offer quick information (Gene expression and gamma-H2AX) have to be established in many countries
- There is a clear lack of information on stockpiling of decorporating drugs in most participating institutions.
- The participating institutions do have a great interest in European wide cooporation programmes for radiation mass casualty management
Conclusion and perspectives:
The study was up until now able to collect a set of very informative and important data on the level of preparation to radiation mass casualties in 20 European countries. These data sets can not be regarded to be complete as well as the set of addressed countries is not complete. At the present stage, there is still a big lack of knowledge regarding the established points of the radiation questionnaire. Thus, there should be a second phase of the data acquisition in which this lack of data should be systematically analyzed and the deficit corrected.