Embed Size (px)
Citation preview

LYMPHOID TISSUES I N NEOPLASIA A Pilot Study and Review IRVING I. KESSLER, MD, DRPH"
Relationships between cancer and prior appendectomy and tonsillectomy were studied in a series of 919 consecutive autopsies as well as by interview and physical examination of 461 cancer patients and 223 controls. In the autopsy series, 11.0 appendectomies were expected among the male cancer patients compared with 7 observed. Among female cancer patients, 11.0 appendec- tomies were expected, while 10 were observed. Neither of these differences was statistically significant. In the interview series, the appropriately weighted relative risk of appendectomy was 0.72 in men and 1.12 in women with cancer. Neither value deviated significantly from the null value, 1.00. For tonsillec- tomy, the relative risks were 1.26 and 1.06, respectively, both insignificantly increased. There is no evidence from the present study that prior lymphoid tissue surgery substantially affects the subsequent risk of cancer. However, sample sizes in this as well as 9 other studies which were reviewed are in- adequate to permit rejection of an actual two- or threefold relative risk devia- tion in patients with certain types of cancer. Restrospective and prospective approaches for subsequent investigation of the role of lymphoid tissues in neoplasia are suggested.
HE VIRAL ETIOLOGY OF CERTAIN HUMAN T malignancies has long been suspected but, despite a theoretical consistency with animal models, remains unproven. Nevertheless, there is considerable evidence suggesting that viruses
From the Department of Environmental Medicine and Community Health, Downstate Medical Center, State University of New York, Brooklyn, N.Y., and the De artment of Chronic Diseases, School of Hygiene an! Public Health, The Johns Hopkins University, Baltimore, Md.
+ Presently Assistant Professor in the Department of Chronic Diseases, School of Hygiene and Public Health, The Johns Hopkins University.
Supported by United States Public Health Service General Research Support Grant 5 SO1 FR5401-05, and National Cancer Institute, Cancer Epidemiology Re- search Training Program Grant 5 TO1 CA05165.
Address for reprints: I. I. Kessler, MD, School of Hygiene and Public Health, The Johns Hopkins Uni- versity, 615 N. Wolfe St., Baltimore, Md. 21205.
The author acknowledges with gratitude the assist- ance of Chester Babat, Karl Green, and Michael Schack- man, who were then senior medical students a t Down- state. For technical assistance he is grateful to Mr. Hamilton Harriss, Assistant in the Department of En- vironmental Medicine and Community Health a t Downstate and to Mrs. Helen Schmerler, Assistant in the Department of Chronic Diseases at Johns Hopkins. He is also indebted to the following for their kind co- operation: Dr. Duncan w. Clark, Dr. Stanley M. Aron- son, Dr. David L. Benninghoff, Dr. Richard Rosen, the Division of Radiotherapy and the Department of Pathology of the Downstate Medical Center; Kings County Hospital Center, and the Brooklyn Veterans Administration Hos ital.
Received for pubfiation August 22, 1969.
and the immunologic responses to them are implicated in the carcinogenic process.23 Re- cent elucidation of the role of the thymus in bodily defense mechanisms has led to in- creased interest in the lymphatic system and its relationships to normal and abnormal growth processes.ll.20 In his Flexner Lecture- ship at Vanderbilt University in 1958, Sir MacFarlane Burnet reflected briefly on the possible immunologic roles of the vermiform appendix and the palatine tonsil: ". . . If histology is any guide, lymphocytes and their products must continually be oozing into the cavity of the appendix and the crypts of the tonsil-presumably for a purpose. . . . Of even greater interest is the possible role of the tonsils and the appendix as two strategically situated major sources for the liberation of what might almost be called antiseptic paint for the protection of the walls of the adjacent cesspools."3 While Burnet limited his specula- tions to local immune responses, recent fmd- ings suggest that the tonsils may function as a central lymphoid organ in the general pro- duction of antibodies and interferon.6e14 A similar role for the appendix has been dem- onstrated in rabbits, though not in humans.'. 8
An epidemiologic model of viral carcino- genesis might attribute the initiation of the process to a virus or virus component and its
510
No. 3 LYMPHOID TISSUFS IN NEOPLASIA * Kessler 51 1
subsequent suppression or enhancement to the adequacy of the host's immune response mech- anisms. Such a model might be tested by ob- serving whether the risk of developing cancer is affected by the prior removal of immuno- logically active lymphoid tissues. In man, only 3 lymphoid tissues are subject to routine extir- pation and, accordingly, are suitable for testing this hypothesis: the vermiform appendix and the palatine and pharyngeal tonsils. At least 9 studies of the relationships between these tissues and neoplasia have been published to date.
PREVIOUSLY PUBLISHED STUDIES
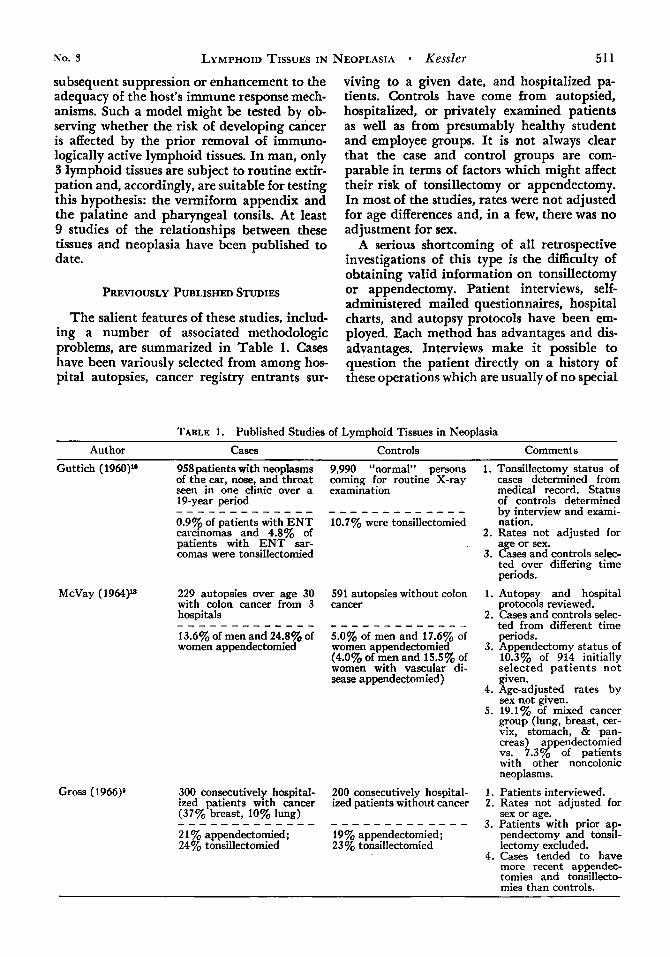
The salient features of these studies, includ- ing a number of associated methodologic problems, are summarized in Table 1. Cases have been variously selected from among hos- pital autopsies, cancer registry entrants sur-
viving to a given date, and hospitalized pa- tients. Controls have come from autopsied, hospitalized, or privately examined patients as well as from presumably healthy student and employee groups. It is not always clear that the case and control groups are com- parable in terms of factors which might affect their risk of tonsillectomy or appendectomy. In most of the studies, rates were not adjusted for age differences and, in a few, there was no adjustment for sex.
A serious shortcoming of all retrospective investigations of this type is the difficulty of obtaining valid information on tonsillectomy or appendectomy. Patient interviews, self- administered mailed questionnaires, hospital charts, and autopsy protocols have been em- ployed. Each method has advantages and dis- advantages. Interviews make it possible to question the patient directly on a history of these operations which are usually of no special
TABLE 1. Published Studies of Lymphoid Tissues in Neoplasia
Author Cases Controls Comments
Guttich (1960)" 958 patients with neoplasms of the ear, nose, and throat seen in one clinic over a 19-year period
0.9% of patients with E N T carcinomas and 4.8% of patients with E N T sar- comas were tonsillectomied
- - - - - - - - - - - - -
McVay (1964)1* 229 autopsies over age 30 with colon cancer from 3 hospitals
13.6% of men and 24.8% of women appendectomied
- - - - - - - - - - - - -
Gross (1966)g 300 consecutively hospital- ized patients with cancer (37% breast, 10% lung)
2 1 % appendectomied; 24% tonsillectomied
- - - - - - - - - - - - -
9,990 "normal" persons coming for routine X-ray examination
- - - - - - - - - - - - - 10.7% were tonsillectomied
591 autopsies without colon cancer
- - - - - - - - - - - - _ 5.0% of men and 17.6% of women appendectomied (4.0% of men and 15.5% of women with vascular di- sease appendectomied)
200 consecutively hospital- ized patients without cancer
19% appendectomied; 23% tonsillectomied
- - - - - - - - - - - - -
1. Tonsillectomy status of cases determined from medical record. Status of controls determined by interview and exami- nation.
2. Rates not adjusted for age or sex.
3. Cases and controls selec- ted over differing time periods.
1. Autopsy and hospital protocols reviewed.
2. Cases and controls selec- ted from different time periods.
3. Appendectomy status of 10.3% of 914 initially selected pat ients not even.
4. Age-adjusted rates by sex not given.
5 . 19.1% of mixed cancer gfoup (lung, breast, cer- vix, stomach, & pan- creas) appendectomied vs. 7.3% of patients with other noncolonic neoplasms.
1. Patients interviewed. 2. Rates not adjusted for
sex or age. 3. Patients with prior ap-
pendectomy and tonsil- lectomy excluded.
4. Cases tended to have more recent appendec- tomies and tonsillecto- mies than controls.
5 12 CANCER March 1970 Vol. 25
TABLE 1 . (Continued)
Author Cases Controls Comments
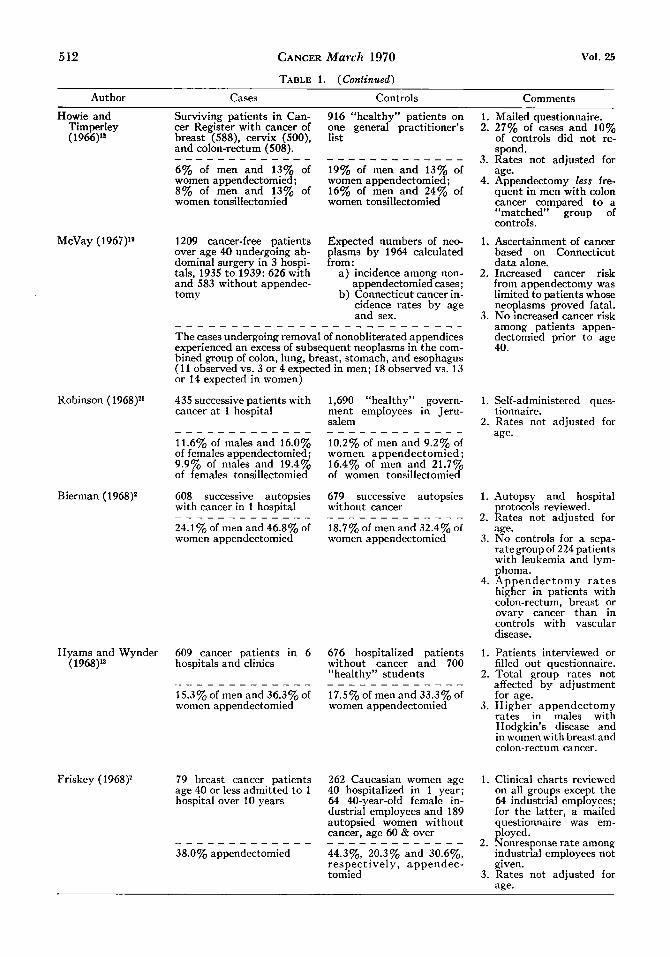
Howie and Surviving patients in Can- 916 “healthy” patients on Timperley cer Register with cancer of one general practitioner’s (1966)’* breast (588), cervix ( S O O ) , list
and colon-rectum (508).
6% of men and 13% of 19% of men and 13% of women appendectomied; women appendectomied; 8% of men and 13% of 16% of men and 24% of women tonsillectomied women tonsillectomied
- - - - - - - - - - - - - - - - - - - - - - _ _ _ _
McVay ( 1967)19 1209 cancer-free patients Expected numbers of neo- over age 40 undergoing ab- plasms by 1964 calculated dominal surgery in 3 hospi- from: tals, 1935 t o 1939: 626 with a ) incidence among non- and 583 without appendec- appendectomied cases; tomy b) Connecticut cancer in-
cidence rates by age and sex.
The cases undergoing removal of nonobliterated appendices experienced an excess of subsequent neoplasms in the com- bined group of colon, lung, breast, stomach, and esophagus (1 1 observed vs. 3 or 4 expected in men; 18 observed vs. 13 or 14 expected in women)
_ _ _ _ _ _ _ _ _ - _ _ - _ - _ - - _ _ _ _ _ _ _ _
1. Mailed questionnaire. 2. 27% of cases and 10%
of controls did not re- spond.
3. Rates not adjusted for age.
4. Appendectomy less fre- quent in men with colon cancer compared to a “matched” group of controls.
1. Ascertainment of cancer based on Connecticut data alone.
2. Increased cancer risk from appendectomy was limited to patients whose neoplasms proved fatal.
3. No increased cancer risk among patients appen- dectomied prior to age 40.
Robinson ( 1968)21 435 successive patients with 1,690 “healthy” govern- 1. Self-administered ques-
2. Rates not adjusted for cancer a t 1 hospital ment employees in Jeru- tionnaire.
Salem
11.6% of males and 16.0% 10.2% of men and 9.2% of of females appendectomied; women appendectomied ; 9.9% of males and 19.4% 16.4% of men and 21.7% of females tonsillectomied of women tonsillectomied
age. _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Bierman ( 1968)2 608 successive autopsies 679 successive autopsies without cancer
18.7% of men and 32.4% of
with cancer in 1 hospital
24.1% of men and 46.8% of women appendectomied women appendectomied
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Hyams and Wynder 609 cancer patients in 6 676 hospitalized patients ( 1968)13 hospitals and clinics without cancer and 700
“healthy” students
17.5% of men and 33.3% of _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ 15.3% of men and 36.3% of women appendectomied women appendectomied
Friskey (1968)T 79 breast cancer patients 262 Caucasian women age age 40 or less admitted to 1 40 hospitalized in 1 year; hospital over 10 years 64 40-year-old female in-
dustrial employees and 189 autopsied women without cancer, age 60 & over
44.3%, 20.3% and 30.6%, respectively, appendec- tomied
_ _ _ _ _ _ _ _ _ _ _ _ _ - - _ - _ - _ _ _ _ _ _ _ 38.0% appendectomied
1. Autopsy and hospital
2. Rates not adjusted for protocols reviewed.
age. 3. No controls for a sepa-
rategroup of 224 patients with leukemia and Ivm- phoma.
4. Appendectomy r a t e s higher in patients with colon-rectum, breast or ovary cancer than in controls with vascular disease.
1. Patients interviewed or filled out questionnaire.
2. Total group rates not affected by adiustment -~ for age.
3. Higher. appendectomy rates in males with Hodgkin’s disease and in women with breast and colon-rectum cancer.
1. Clinical charts reviewed on all groups except the 64 industrial employees; for the latter, a mailed questionnaire was em- ployed.
2. Nonresponse rate among industrial employees not given.
3. Rates not adjusted for age.
No. 3 LYMPHOID TISSUES IN
interest to physicians taking medical histories in the hospital. Mailed questionnaires permit the sampling of other than hospitalized pa- tients, but are subject to large nonresponse rates. Of course, both interviews and question- naires depend upon the memory and coopera- tion of the respondents themselves. Nonre- sponse is not a problem with hospital records but variability in history-taking procedures is. A serious problem is deciding how to deal with the usual high proportion of charts in which no mention is made of either opera- tion: the conservative approach would be to assume that the relevant history was not taken. Autopsy series could, theoretically, provide definitive evidence for the presence or absence of particular lymphoid tissues. However, ton- sils are not usually examined postmortem and the appendix is rarely sought as assiduously as are other organs more commonly associated with disease. Autopsy procedures can be modi- fied to permit a detailed study of lymphoid tissues, but the problem of the selective na- ture of autopsied populationslst 17 will remain.
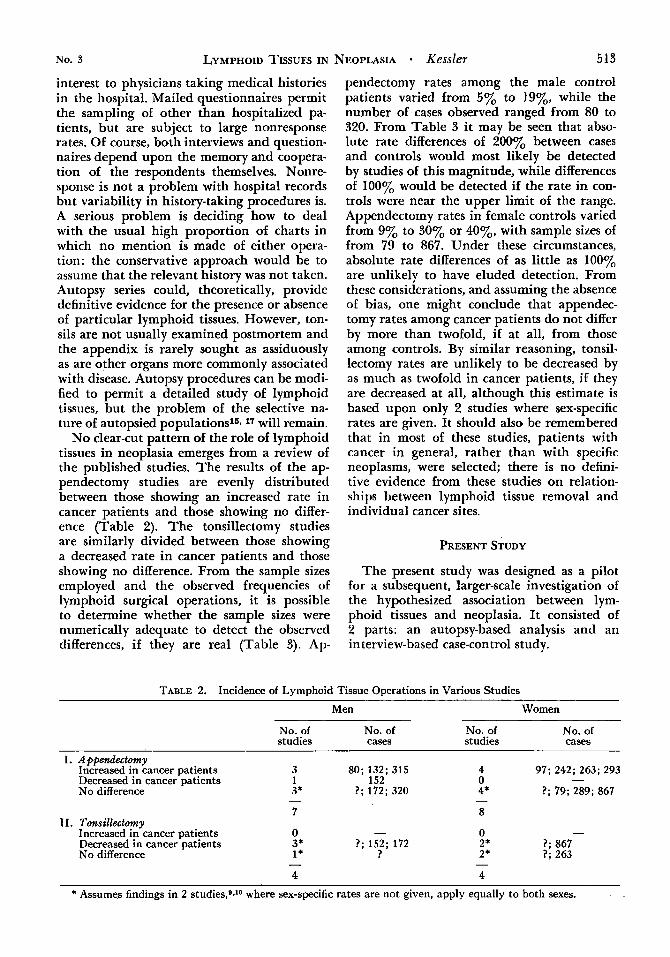
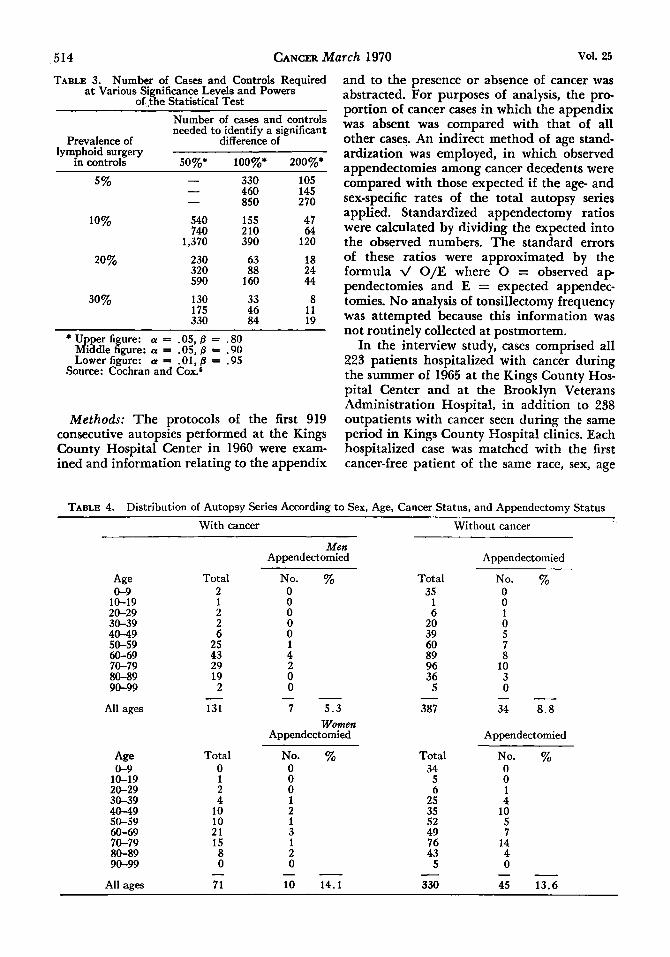
No clear-cut pattern of the role of lymphoid tissues in neoplasia emerges from a review of the published studies. The results of the ap- pendectomy studies are evenly distributed between those showing an increased rate in cancer patients and those showing no differ- ence (Table 2). The tonsillectomy studies are similarly divided between those showing a decreased rate in cancer patients and those showing no difference. From the sample sizes employed and the observed frequencies of lymphoid surgical operations, it is possible to determine whether the sample sizes were numerically adequate to detect the observed differences, if they are real (Table 3). Ap-
NEOPLASIA * Kessler 513
pendectomy rates among the male control patients varied from 5% to 19%, while the number of, cases observed ranged from 80 to 320. From Table 3 it may be seen that abso- lute rate differences of ZOOYO between cases and controls would most likely be detected by studies of this magnitude, while differences of 1 0 0 ~ o would be detected if the rate in con- trols were near the upper limit of the range. Appendectomy rates in female controls varied from 9% to 30% or 40%, with sample sizes of from 79 to 867. Under these circumstances, absolute rate differences of as little as 100% are unlikely to have eluded detection. From these considerations, and assuming the absence of bias, one might conclude that appendec- tomy rates among cancer patients do not differ by more than twofold, if at all, from those among controls. By similar reasoning, tonsil- lectomy rates are unlikely to be decreased by as much as twofold in cancer patients, if they are decreased at all, although this estimate is based upon only 2 studies where sex-specific rates are given. It should also be remembered that in most of these studies, patients with cancer in general, rather than with specific neoplasms, were selected; there is no defini- tive evidence from these studies on relation- ships between lymphoid tissue removal and individual cancer sites.
PRESENT STUDY
The present study was designed as a pilot for a subsequent, larger-scale investigation of the hypothesized association between lym- phoid tissues and neoplasia. It consisted of 2 parts: an autopsy-based analysis and an interview-based case-control study.
TABLE 2. Incidence of Lymphoid Tissue Operations in Various Studies
Men Women
No. of No. of No. of No. of studies cases studies cases
I. Apfiendectomy Increased in cancer patients 3 80;132;315 4 97; 242; 263; 293
No difference 3* ?; 172; 320 4* ?; 79; 289; 867 - Decreased in cancer patients 1 152 0
- - 7 8
0 11. Tonsillectomy - - Increased in cancer patients 0
Decreased in cancer patients 3* ?; 152; 172 2* 1; 867 No difference 1* ? 2* 1; 263
- - 4 4
* Assumes findings in 2 studies,gJO where sex-specific rates are not given, apply equally to both sexes.
CANCER March 1970 Vol. 25
TABLE 3. Number of Cases and Controls Required at Various Significance Levels and Powers
of. $he Statistical Test Number of cases and controls needed to identify a significant
Prevalence of difference of lymphoid surgery
in controls SO%* loo%* 200%*
- 330 - 460 - 850
540 155 740 210
1,370 390
5%
10%
20% 230 63 320 88 590 160
130 33 175 46 330 84
30%
105 145 270
47 64
120
18 24 44
8 11 19
* Upper fi * a = .05,0 = .80 Middle &:;: a = .05, 0 = .90 Lower figure: a = = .95
Source: Cochran and Cox.
Methods: The protocols of the first 919 consecutive autopsies performed at the Kings County Hospital Center in 1960 were exam- ined and information relating to the appendix
and to the presence or absence of cancer was abstracted. For purposes of analysis, the pro- portion of cancer cases in which the appendix was absent was compared with that of all other cases. An indirect method of age stand- ardization was employed, in which observed appendectomies among cancer decedents were compared with those expected if the age- and sex-specific rates of the total autopsy series applied. Standardized appendectomy ratios were calculated by dividing the expected into the observed numbers. The standard errors of these ratios were approximated by the formula V O/E where 0 = observed a p pendectomies and E = expected appendec- tomies. No analysis of tonsillectomy frequency was attempted because this information was not routinely collected at postmortem.
In the interview study, cases comprised all 223 patients hospitalized with cancer during the summer of 1965 at the Kings County Hos- pital Center and at the Brooklyn Veterans Administration Hospital, in addition to 238 outpatients with cancer seen during the same period in Kings County Hospital clinics. Each hospitalized case was matched with the first cancer-free patient of the same race, sex, age
TABLE 4. Distribution of Autopsy Series According to Sex, Age, Cancer Status, and Appendectomy Status ~~
With cancer Without cancer
Men Appendectomied Appendectomied
Age Total No. % Total No. % 0-9
10-19 20-29 30-39 40-49 50-59 60-69 70-79 80-89 90-99
All ages
Age 0-9
10-19 20-29 30-39
2 1 2 2 6
25 43 ~~
29 19
2 - 131
Total 0 1 2 4
40-49 10 50-59 10 60-69 21 70-79 15 80-89 8
0 0 0 0 0 1 4 2 0 0
7 5.3 - -
Women Appendectomied
No. % 0 0 0 1
35 1 6
20 39 60 89 96 36
5
387
0 0 1 0 5 7 8
10 3 0 - - 34 8.8
Appendectomied
Total 34
5 6
25
No. % 0 0 1 4
43 4 0 - - 0 5 - - - 0 - 90-99
All ages 71 10 14.1 330 45 13.6

No. 3 LYMPHOID TISSUES IN NEOPLASIA Kessler 515 (zk 5 years), and marital status who was TABLE 5. Distribution of Autopsied Cancer Patients identified from the patient roster, utilizing a random selection procedure. As a rule, controls were selected from the same wards Men Women
as cases. However, patients admitted to cancer Appendec- Appendec- therapy wards were matched to cancer-free site tomied tomied admissions to general surgery wards. Hospital charts, surgical pathology reports, and hema- tology reports were reviewed to confirm the diagnosis of cancer in cases and to exclude it in controls. Lymphoid tissue status was Large intestine 12
According to Sex, Cancer Site, and Appendectomy Status
Buccal cavity
g:&Lynx Stomach small intestine
5 1 2 0 10 1 1 0 9 1 3 2
0 0 0 2 7 1
ascertained by physical examination as well Rectum 1 0 2 0 as by personal interview. The oropharynx Liver 6 1 4 0 was carefully visualized and the presence or Pancreas 4 0 3 0
2 0 1 0 41 0 4 0
0 1 0
absence, size, and condition of the palatine tonsils were determined. The abdominal wall was then examined and the size and location
Nose, Sinuses* and larynx
Lung Mediastinurn
of all surgical scars was recorded. Finally, a Breast 0 0 13 3 personal interview was conducted in order to Cervix uteri 0 0 4 0 obtain demographic and socioeconomic in- Corpus uteri 0 0 4 1
and tonsillectomy. adnexae 0 0 3 0 formation as well as a history of appendectomy
Summary relative risks of lymphoid tissue
Ovary and
Prostate 8 0 0 0 Other male
and controls were calculated by a formula Kidne and surgery as determined by interview of cases genitalia 1 0 0 0
suggested by Mantel and Haenszel.16 This gives bladdk 6 0 2 0 a weighted average of age- and sex-specific Skin 1 0 0 0
significant deviation of the summary relative Lymphoma 4 0 6 0
combining 2 x 2 contingency tables was uti- lized. Calculations of the summary relative A*1 sites 131 7 71 10
Central nervous
Connective
Fggka
4 0 0 0 relative risks in which the weights are propor- tional to the precision of the relative risks for each subclassification. In order to test for tissue 1 0 0 0
2 0 2 1 risks from unity, Mantel and Haenszel’P 1 9 2 modification of Cochran’s4 f statistic for Leukemia 13
system
- - - -
TABLE 6. Distribution of the Autopsied Controls According to Disease for which Hospitalized Total ICD Rubric* Disease category Men Women
001-138 Infective & parasitic 3 0 3 210-229 Benign neoplasms 0 10 10 240-289 Allergic, endocrine, etc. 10 5 15 300-326 Mental etc. 4 1 5 330-398 Nervous system etc. 3 4 7
470-527 Respiratory system 9 1 10 530-587 Digestive system 45 19 64 590-637 Genito-urinary system 20 8 28
3 3 640-689 Pregnancy, childbirth, etc. - 690-7 16 Skin and cellular tissue 2 2 4 720-749 Bones and organs of movement 3 2 5 780-795 Symptoms, senility & ill-defined 6 2 8
N800-N999 Accidents etc. 4 11 15
TOTAL 139 84 223
400-468 Circulatory system 30 16 46
- - -
* Three-digit categories of the Manual of the International Statistical Classification of Diseases, Injuries and Cause of Death, vol. 1. World Health Organization, Geneva, 1957.
516 CANCER March 1970 Vol. 25
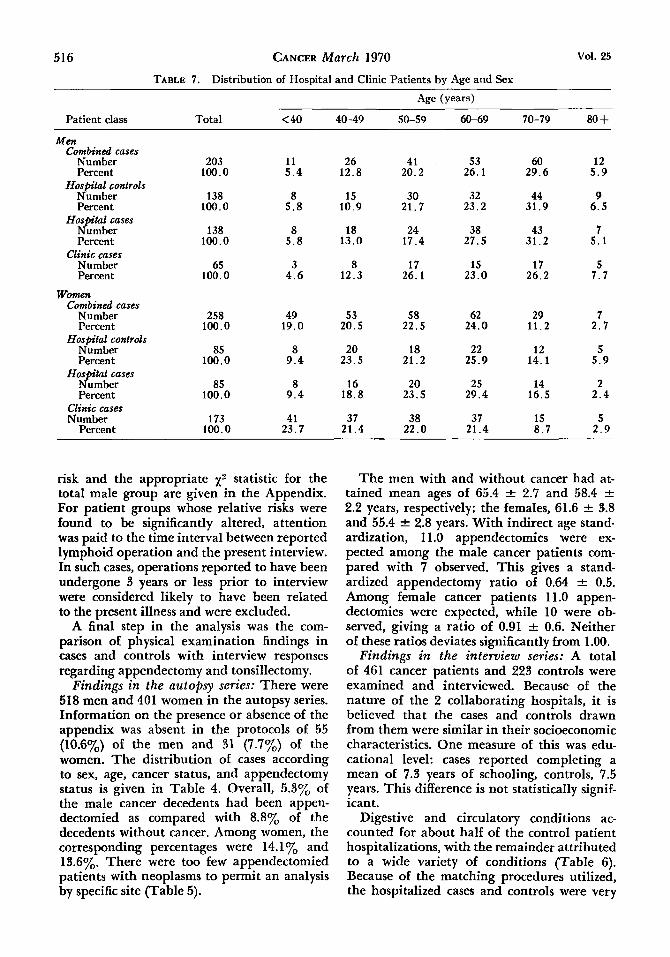
TABLE 7. Distribution of Hospital and Clinic Patients by Age and Sex
Age (years)
Patient class Total < 40 40-49 50-59 60-69 70-79 80 + MCn
Combined cases Number Percent
Number Percent
Hospital cases Number Percent
Clinic cases Number Percent
Hospitul controls
Women Combined cases
Number Percent
Number Percent
Hospitul cases Number Percent
Clinic cases Number
Percent
Hospital controls
203 100.0
138 100.0
138 100.0
65 100.0
258 100.0
85 100.0
85 100.0
173 100.0
11 5 . 4
8 5 . 8
8 5 . 8
3 4 . 6
49 19.0
8 9 .4
8 9 . 4
41 23.7
26 12.8
15 10.9
18 13.0
8 12.3
53 20.5
20 23.5
16 18.8
37 21.4
41 20.2
30 21.7
24 17.4
17 26.1
58 22.5
18 21.2
20 23.5
38 22.0
53 26.1
32 23.2
38 27.5
15 23.0
62 24.0
22 25.9
25 29.4
37 21.4
60 29.6
44 31.9
43 31.2
17 26.2
29 11.2
12 14.1
14 16.5
15 8.7
12 5 . 9
9 6.5
7 5 . 1
5 7 . 7
7 2.7
5 5 . 9
2 2 .4
5 2 .9
risk and the appropriate x 2 statistic for the total male group are given in the Appendix. For patient groups whose relative risks were found to be significantly altered, attention was paid to the time interval between reported lymphoid operation and the present interview. In such cases, operations reported to have been undergone 3 years or less prior to interview were considered likely to have been related to the present illness and were excluded.
A final step in the analysis was the com- parison of physical examination findings in cases and controls with interview responses regarding appendectomy and tonsillectomy.
Findings in the autopsy series: There were 518 men and 401 women in the autopsy series. Information on the presence or absence of the appendix was absent in the protocols of 55 (10.6%) of the men and 31 (7.7%) of the women. The distribution of cases according to sex, age, cancer status, and appendectomy status is given in Table 4. Overall, 5.3y0 of the male cancer decedents had been appen- dectomied as compared with 8.8% of the decedents without cancer. Among women, the corresponding percentages were 14.1y0 and 13.6%. There were too few appendectomied patients with neoplasms to permit an analysis by specific site (Table 5).
The men with and without cancer had at- tained mean ages of 65.4 & 2.7 and 58.4 +- 2.2 years, respectively; the females, 61.6 f 3.8 and 55.4 f 2.8 years. With indirect age stand- ardization, 11.0 appendectomies were ex- pected among the male cancer patients com- pared with 7 observed. This gives a stand- ardized appendectomy ratio of 0.64 f 0.5. Among female cancer patients 11.0 appen- dectomies were expected, while 10 were ob- served, giving a ratio of 0.91 k 0.6. Neither of these ratios deviates significantly from 1.00.
Findings in the interview series: A total of 461 cancer patients and 223 controls were examined and interviewed. Because of the nature of the 2 collaborating hospitals, it is believed that the cases and controls drawn from them were similar in their socioeconomic characteristics. One measure of this was edu- cational level: cases reported completing a mean of 7.3 years of schooling, controls, 7.5 years. This difference is not statistically signif- icant.
Digestive and circulatory conditions ac- counted for about half of the control patient hospitalizations, with the remainder attributed to a wide variety of conditions (Table 6). Because of the matching procedures utilized, the hospitalized cases and controls were very
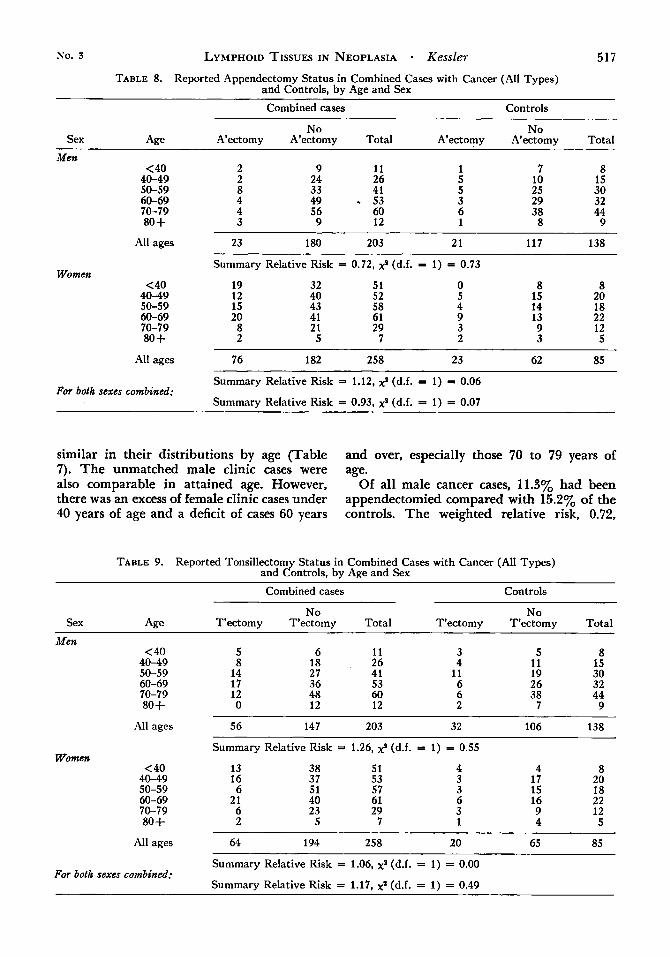
No. 3 LYMPHOID TISSUES IN NEOPLASIA - Kessler 517 TABLE 8. Reported Appendectomy Status in Combined Cases with Cancer (All Types)
and Controls, by Age and Sex
Combined cases Controls
No No Sex Age A’ectomy A’ectomy Total A’ectomy A’ectomy Total
Men < 40
4 0 4 9 50-59 60-69 70-79 80 +
2 2 8 4 4 3
9 24 33 49 56 9
11 26 41 - 53 60 12
7 8 10 15 25 30 29 32 38 44 8 9
Women
All ages 23 180 203 2 1 117 138
Summary Relative Risk = 0.72, x* (d.f. = 1) = 0.73
<40 4 0 4 9 50-59 60-69 70-79 80 +
All ages -
19 32 51 0 8 8 12 40 52 5 15 20 15 43 58 4 14 18 20 41 61 9 13 22
8 21 29 3 9 12 2 5 7 2 3 5
76 182 258 23 62 85 -
Summary Relative Risk = 1.12, X* (d.f. = 1) = 0.06
Summary Relative Risk = 0.93, X* (d.f. =I 1) = 0.07 For both sexes combined:
similar in their distributions by age (Table 7). The unmatched male clinic cases were also comparable in attained age. However, there was an excess of female clinic cases under 40 years of age and a deficit of cases 60 years
and over, especially those 70 to 79 years of age.
Of all male cancer cases, 11.3% had been appendectomied compared with 15.2% of the controls. The weighted relative risk, 0.72,
TABLE 9. Reported Tonsillectomy Status in Combined Cases with Cancer (All Types) and Controls, by Age and Sex Combined cases Controls
No No Sex Age T’ectomy T’ectomy Total T’ectomy T’ectomy Total
Men <40 5 6 11 3 5 8
40-49 8 50-59 14 60-69 17 70-79 12 80 + 0
18 26 ~~ ~~
27 41 36 53 48 60 12 12
4 11 6 6 2
11 15 19 30 26 32 38 44
7 9
Women
~ ~
All ages 56 147 203 32 106 138
Summary Relative Risk = 1.26, x* (d.f. = 1) = 0.55
< 40 40-49 50-59
13 16 6
60-69 21 70-79 6 80 + 2
38 51 37 53 51 57 40 61 23 29
5 7
4 3 3 6 3 1
4 8 17 20 15 18 16 22 9 12 4 5
All ages 64 194 258 20 65 85
Summary Relative Risk = 1.06, x* (d.f. = 1) = 0.00
Summary Relative Risk = 1.17, xa (d.f. = 1) = 0.49 For both sexes combined:

518 CANCER March 1970 Vol. 25
TABLE 10. Proportions Appendectomied Among Combined Cases and Controls, by Sex and Cancer Type ~~
Combined cases Controls
Cancer type Sex No. % A'ectomy No. % A'ectomy Buccal cavity
Esophagus, stomach, & small intestine
Colon & rectum
Liver, pancreas & other gastrointestinal
Respiratory
Breast
Prostate & other male
Uterus & other female
Kidney & bladder
genitalia
genitalia
Lymphatic & hematopoietic
All other cancer
TOTAL CANCER
F M
Total M F
Total M F
Total M F
-
__
Total
M F
Total M F
Total M
F
M F
-
Total M F
Total M F
-
Total
M F
Total -
31 10
41 1 1 6
17 31 14
45 5 1
6 54 4
58 2 89
91 11
92
21 8
29 22 18
40 15 16
31 203 258
461
-
-
-
-
-
-
-
-
-
-
6.5 10.0
7.3 9.1 16.7
11.8 6.5 21.4
-
-
11.1 0.0
100.0
16.7 14.8 25.0
-
15.5 50.0 29.2
29.7 9.1
33.7
14.3 62.5
-
27.6 18.2 16.7
17.5 6.7 25.0
16.1 11.3 29.5
-
21.5
19 5
24 10 5
15 25 9
34 5 1
6 36
1
37 1 18
19 8
35
11 2
13 14 5
19 9 4
13 138 85
223
-
-
-
--
-
-
-
-
-
-
15.8 60.0
25.0 0.0 60.0
20.0 16.0 33.3
20.6 40.0 0.0
33.3 13.9 100.0
16.2 0.0 27.8
-
26.3 12.5
11.4
18.2 50.0
23.1 14.3 40.0
21.1 22.2 25.0
-
-
23.1 15.2 27.1
19.7 -
TABLE 11. Relative Risks of Appendectomy in was not significantly reduced (p>.40), Table 8. Among women, 29.5% of all cases and 27.1% of controls were appendectomied. The
relative associated relative risk, 1.12, was not signif-
Selected Patient Groups
Summary
Cancer type Sex risk x2(d.f. = 1) P icantly increased (p>.80). The summar; re- lative risk for both sexes combined was 0.93, 0.55 >.40 insignificantly reduced from unity (p>.80). Buccal cavity M 0.27
O." >." Approximately 27.6% of the men with can- Colon and rectum M 0.44
Respiratory M 1.09 0.03 >.80 cer reported a tonsillectomy as compared with Breast F 1.34 0.05 >.80 23.2% of the controls. The summarv relative Uterus & other risk 'of 1.26 was not significantly increased
(p>.40), Table 9. Among women, 24.8% of 4.49 <.05 genitalia F 3.82
No. 3 LYMPHOID TISSUES IN NEOPLASIA - Kesslel- 519
TABLE 12. Proportions Tonsillectomied Among Combined Cases and Controls, by Sex and Cancer Type
Controls Combined cases
Cancer type Sex No. yo T'ectomy No. yo T'ectomy
Buccal cavity
Esophagus, stomach, & small intestine
Colon & rectum
M F
Total
M F
Total M F
-
-
Liver, pancreas, & other gastrointestinal
Respiratory
Total
M F
Total
M F
-
Breast
Total M F
Prostate & other male
Uterus & other female
Kidney & bladder
genitalia
genitalia
Lymphatic & hematopoietic
Total M
F
M F
Total
M F
-
All other cancer
TOTAL CANCER
Total M F
Total M F
-
31 10
41
11 6
17 31 14
45 5 1
6
54 4
58 2
89
-
-
-
-
-
91 11
92
21 8
29 22 18
40 15 16
31 203 258
-
-
-
38.7 40.0
39.0
18.2 16.7
17.6 35.5 35.7
-
-
19 5
24
10 5
15
25 9
-
-
35.6 40.0
100.0
50.0
27.8 50.0
-
29.3
0.0 32.6
31.9 27.3
15.2
23.8 0.0
17.2 13.6 27.8
20.0 20.0 18.8
19.4 27.6 24.8
-
Total 461 26.0
34 5 1
6
36 1
37 1
18
19 8
35
11 2
13
14 5
19 9 4
-
-
-
-
-
31.6 0.0
25.0
10.0 80.0
~
33.3 20.0 22 .2
20.6 20.0 0.0
16.7 22.2
100.0
24.3
0.0 33.3
31.6 25.0
17.1
18.2 50.0
23.1 21.4 0.0
-
-
-
-
15.8 44.4 0.0
13
138 85
223 -
30.8 23.2 23.5
23.3 -
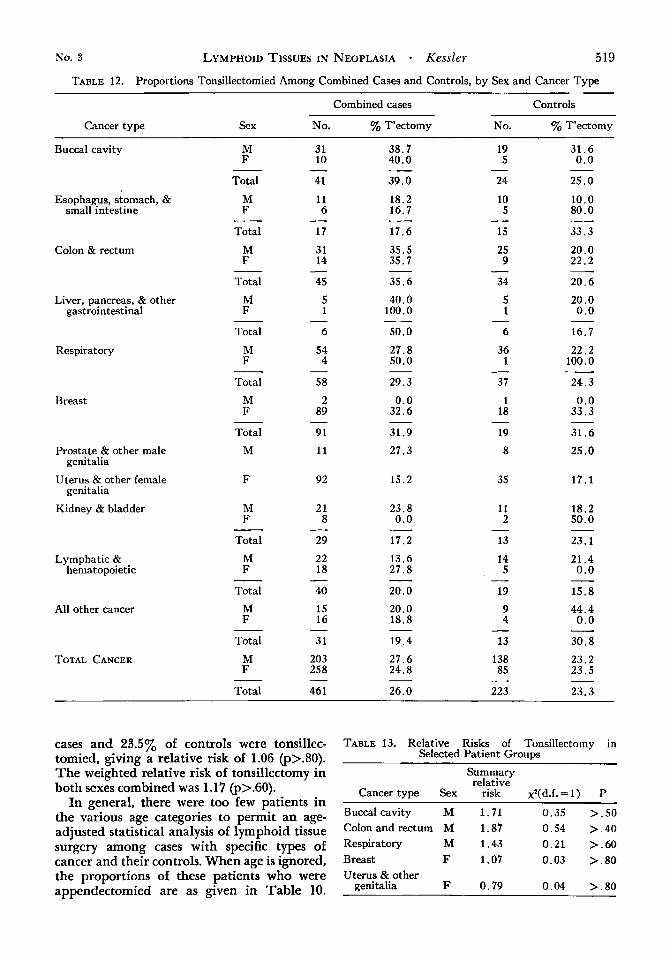
cases and 23.501, of controls were tonsillec- tomied, giving a relative risk of 1.06 (p>.80). The weighted relative risk of tonsillectomy in both sexes combined was 1.17 (p>.60).
In general, there were too few patients in the various age categories to permit an age- adjusted statistical analysis of lymphoid tissue surgery among cases with specific types of cancer and their controls. When age is ignored, the proportions of these patients who were appendectomied are as given in Table 10.
TABLE 13. Relative Risks of Tonsillectomy in Selected Patient Groups
Summary relative
Cancer type Sex risk xZ(d.f.=l) P
Buccalcavity M 1.71 0.35 >.SO Colon and rectum M 1.87 0.54 >.40 Respiratory M 1.43 0.21 >.60 Breast F 1.07 0.03 > . 8 0 Uterus & other
genitalia F 0.79 0.04 >.80
520 CANCER March 1970 Vol. 25
TAnLE 14. Operative Scars on Right or Midline of Abdomen in Cases and Controls According t o
Reported Appendectomy History*
Appendectomy Reported Cases Controls
Sex No. %Scarred No. %Scarred
M 23 100.0 21 100.0 F 76 94.7 23 95.7 - - - -
TOTAL 99 96.0 44 97.7
Appendectomy Denied Cases Controls
Sex No. %Scarred No. %Scarred
M 171 36.8 117 39 .3 159 49 .1 62 5 0 . 0 F
TOTAL 330 42 .7 179 4 3 . 0 - - - -
* Excludes 32 cases with incomplete examinations.
No consistent pattern is evident, either in men or women, except for a higher rate of appendectomy among women. It was possible to calculate age-weighted summary relative risks for 5 groups of cancer patients and their controls, viz. men with buccal, colon-rectum, and respiratory cancer and women with breast and uterus cancer (Table 11). The relative risk was significantly increased (3.82, p < .05) only in the patients with uterine cancer. How- ever, 18 out of the 31 appendectomied cases had undergone appendectomy 3 years or less prior to interview. When these are excluded, the difference between cases and controls ceases to be significant.
Proportions of patients tonsillectomied, by type of cancer, are given in Table 12. Overall, there is no difference between the sexes in
TABLE 15. Visualization of Palatine Tonsils in Cases and Controls According to Reported
Tonsillectomy History* -
Tonsillectomy Reported Cases Controls
Sex No. yo Absent No. % Absent
M 56 5 3 . 6 32 53 .1 64 56 .3 20 45 .0 F
TOTAL 120 53 .3 52 50 .0 - - - -
Tonsillectomy Denied Cases Controls
Sex No. % Absent No. % Absent
M 138 2 . 9 102 4 . 9 1 . 6 F 185 2 . 2 64
TOTAL 323 2 . 5 166 3 . 6 - - - -
* Excludes 18 cases and 5 controls with incomplete examinations.
rate of tonsillectomy. Risks according to can- cer type do not show any consistent pattern. As was done for appendectomy, age-weighted summary relative risks were calculated for the 5 largest groups of cancer patients and their controls (Table 13). None deviated signifi- cantly from unity.
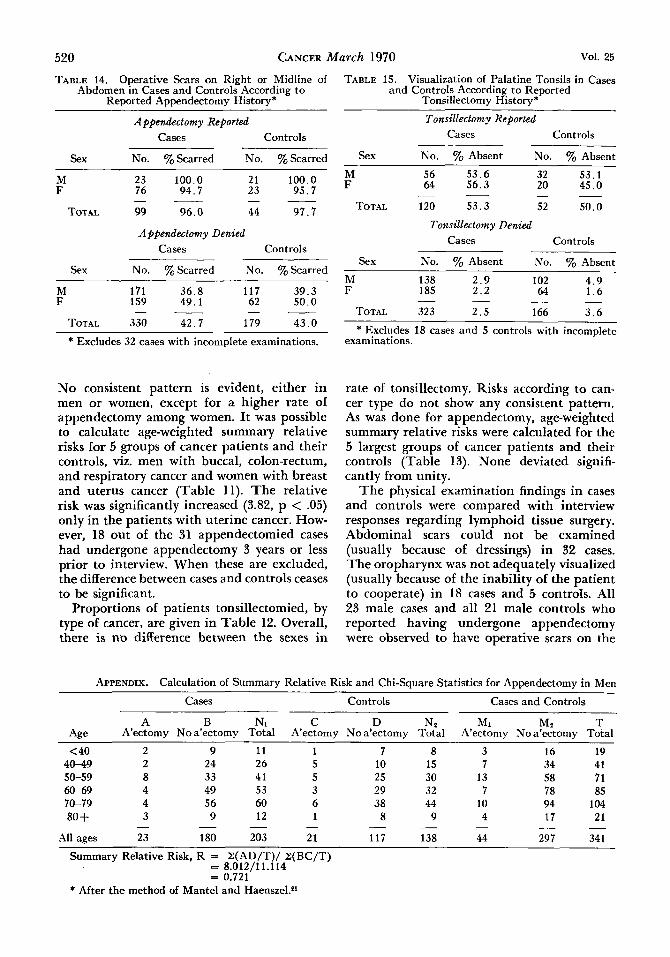
T h e physical examination findings in cases and controls were compared with interview responses regarding lymphoid tissue surgery. Abdominal scars could not be examined (usually because of dressings) in 32 cases. The oropharynx was not adequately visualized (usually because of the inability of the patient to cooperate) in 18 cases and 5 controls. All 23 male cases and all 21 male controls who reported having undergone appendectomy were observed to have operative scars on the
APPENDIX. Calculation of Summary Relative Risk and Chi-square Statistics for Appendectomy in Men
Cases Controls Cases and Controls
A B N1 C D Nz Mi Mz T Age A’ectomy No a’ectomy Total A’ectomy No a’ectomy Total A’ectomy No a’ectomy Total
< 40 2 40-49 2 50-59 8 60-69 4 70-79 4
3 80 + All ages 23
-
9 24 33 49 56 9
180 -
11 1 26 5 41 5 53 3 60 6 12 1
203 21 - -
7 8 10 15 25 30 29 32 38 44
9
1 1 7 138 -
8 -
3 7
13 7
10 4
44 -
16 19 34 41 58 7 1 78 85 94 104
21 17
297 34 1 - -
Summary Relative Risk, R = Z(AD/T)/ z(BC/T) = 8.012/11.114 = 0.721
* After the method of Mantel and Haensze1.P’
No. 3 LYMPHOID TISSUES IN
right or midline of the abdomen. Of the 76 female cases and 23 female controls reporting appendectomy, the corresponding figures were 72 (94.7%) and 22 (95.7%). By way of con- trast, only 43% of cases or controls denying appendectomy had right or midline scars (Table 14). Among cancer patients denying appendectomy, the prevalence of such scars ranged from 20yo or less for those with buccal cavity and lung cancer to 70% or more for those with colon-rectum, liver, and other gas- trointestinal cancer. Intermediate scar fre- quencies were observed in patients with all other cancers.
Of patients who reported a tonsillectomy, 53.3% of the cases and 50.0% of the controls were found to have tonsils absent on physical examination (Table 15). The proportions among men were 53.6y0 in cases and 53.1y0 in controls; among women, 56.3y0 and 45.0y0, respectively. The proportions among cases reporting the operation were quite stable, ranging upward from a low of 43.8% in those with cancer of the buccal cavity to 66.7y0 in patients with prostatic and upper gastrointes- tinal cancer to 100% of the 3 patients with liver cancer. Very few patients who denied tonsillectomy showed evidence of the opera- tion, viz. 2.5% of cases and 3.6Y0 of controls, with slightly higher frequencies in men than in women.
DISCUSSION
There is no evidence from the present study that prior appendectomy or tonsillectomy affects the subsequent risk of cancer. The autopsy series and the interview series are consistent in showing no significant differences
with Cancer (All Types) and Their Controls*
1.737 6.737 0.650 0,737 0.474 4.439 12.439 1.380 0.488 2.927 7.507 24.507 2.628 2.817 2.324 4.365 29.365 1.526 1.365 1.729 5.769 39.769 2.227 1.462 3.231 2.286 7.286 0.833 1.143 0.429
26.103 120.103 9.244 8.012 11.114 - _ _ _ - --
Chi-Square,x2(d.f. = 1 ) = (I ZA - ZE(A)I - 0.5)2/V(A) = (123 -26.1031 -0.5)'/9.244 = 0.733
NEOPLASIA - Kessler 52 1
in rates of prior appendectomy or tonsillec- tomy among cancer patients when compared with suitably matched controls. However, the relatively small sample sizes of patients with particular neoplasms do not permit the re- jection of the possibility that a two- or three- fold deviation in relative risk actually exists for patients with certain types of cancer. To test such an hypothesis, it would be necessary to assemble an adequate number of cases (200, perhaps) with the cancer in question as well as an appropriately selected control grOUP.
The effect of selectivity factors on study variables is exemplified by a comparison of 2 findings in the autopsy and interview series. In both series, the proportion of women (ir- respective of case or control status) reporting appendectomy was 2 to 3 times that of men. This finding is consistent with most, though not all, previously published studies. On the other hand, for both male and female cases and controls, the proportions reporting appen- dectomy were approximately twice as high in the interview series as in the autopsy series. Differing methods of ascertainment (live inter- view vs. autopsy protocol) have undoubtedly played a role here, bu t differences in age distribution as well as other factors which bring patients to autopsy or to particular hospitals may also be implicated.
The cases and controls of the interview series are believed to be comparable in socio- economic status by virtue of their attained edu- cational level and their admission to a muni- cipal hospital lacking a private service. No adjustment was made for possible differences in country of birth. Although a higher rate of primary appendectomy in American-born as compared with foreign-born women has been reported in one study,13 the 2 groups differed by more than 4 years in mean age, and there was no significant difference among men.
Previously published reports29 131 18, 19 of sig- nificantly increased appendectomy rates among patients with cancers of the colon-rectum, lung, breast, and uterus could not be con- firmed by this investigation. The same is true of the reported decrease in tonsillectomy prevalence among patients with ear, nose, and throat cancers.10 The methodologic character- istics of these studies, which may have influ- enced their findings, have already been dis- cussed.
The difficulties inherent in attempting to validate reported appendectomies and tonsil-
522 CANCER March 1970 Vol. 25
lectomies in retrospective studies are well known. The physical examination findings in the present study suggest that inspection of the abdomen and oropharynx offer no solution to this problem. About 43% of the patients denying appendectomy had right or midline abdominal scars, while only about half of those who reported tonsillectomy could have this confirmed on examination.
Two promising approaches are open to subsequent investigators of the possible role of lymphoid tissues in neoplasia. First, one might design a well-controlled retrospective study of appendectomy status in persons with
and without cancers of specified types. Such a study should have sufficient numbers of cases and controls to assure an adequate test of the hypothesis. It should also provide for an in- dependent validation of reported appendec- tomy or tonsillectomy status, perhaps through a review of all existing hospital records. A second approach would be the prospective follow-up of a suitably large cohort of persons appendectomied or tonsillectomied several decades ago, as well as suitable control groups. The true risk of cancer in each group could then be calculated. Studies of these types are presently being developed.
REFERENCES
1. Archer, Olga K., Sutherland, D. E. R., and Good, R. A.: The developmental biology of lymphoid tissue in the rabbit: consideration of the role of thymus and appendix. Lab. Invest. 13:259-271, 1964.
2. Bierman, H. R.: Human appendix and neoplasia. Cancer 21:109-118,1968.
3. Burnet, M.: The Clonal Selection Theory of Ac- quired Immunity. Nashville, Vanderbilt University Press, 1959; pp. 84-86.
4. Cochran, W. G.: Some methods for strengthening the common x 2 tests. Biornetrics 10417-151, 1954.
5. - , and Cox, Gertrude M.: Experimental De- signs. New York, John Wiley & Sons, 1962; p. 24.
6. Drabe, J.: Experimentelle Untersuchungen zur Frage der Antikorperbildung in den Tonsillen. Portschr. Hals-Nus-Ohrenheilk. 7217-292, 1961.
7. Friskey, 1. W.: Appendectomy prevalence in ho- mogeneous populations. J. Chronic Dis. 21 :387-389, 1968.
8. Good, R. A., and Papermaster, B. W.: Ontogeny and phylogeny of adaptive immunity. In Advances in Immunology, F. J. Dixon, Jr., and . H. Humphrey, eds. New York, Academic Press, 196d; pp. 1-115.
9. Gross, L.: Incidence of appendectomies and ton- sillectomies in cancer patients. Cancer 19:84%852, 1966.
10. Guttich, H.: Erkranken Tonsillecktomierte sel- tener am Carcinom der oberen Luft- und Speisewege? HNO 94749,1960.
11. Holborow, E. J.: An ABC of Modern Immunol- ogy. London, The Lancet Ltd., 1968.
12. Howie, J. G. R., and Tim erley, W. R.: Cancer and appendectomy. Cancer 19:11!&-1142, 1966.
13. Hyams, L., and Wynder, E. L.: Appendectomy and cancer risk: an epidemiological evaluation. J . Chronic Dis. 21:391-415, 1968.
14. Kocsard-Varo, G.: The physiological role of the tonsils, adenoids and appendix in immunity. Med. J . A w t . 2:873-874, 1964.
15. Mainland, D.: The risk of fallacious conclusions from autopsy data on the incidence of diseases with applications to heart disease. Amer. Heart J . 45:644- 654, 1953.
16. Mantel, N., and Haenszel, W.: Statistical aspects of the analysis of data from retrospective studies of disease. J . Nut. Cancer Inst. 22:719-748, 1959.
17. McMahan, C. A.: Age-sex distributions of selected groups of human autopsied cases. Arch. Path. 73:4047, 1962.
18. McVay, J. R., Jr.: The appendix in relation to neoplastic disease. Cancer 17:929-937, 1964.
19. -- . Deaths from appendicitis and appendicec- tomy. Lancet 1:439, 1967 (letter).
20. Nakakuki, K., Shisa, H., and Nishizuka, Y.: Pre- vention of AKR leukemia by thymectomy at varying ages. Acta Haemat. 38:317-323, 1967.
21. Robinson, E.: The incidence of appendectomies, tonsillectomies and adenoidectomies in cancer patients. Brit. J. Cancer 22:25&252, 1968.
22. Shapiro, S. L.: Tonsillectomy: once-routine, but attitudes shifting, In Current Medical News, 1966; p. 13.
23. Viruses and Cancer, WHO Technical Report No. 295, 1965. Geneva.