Embed Size (px)
Citation preview
Looking Forward: Looking Forward: Imagining New Models of CareImagining New Models of Care
Eric A. Coleman, MD, MPHAssociate ProfessorDivisions of Geriatric Medicine and Health Care Policy and ResearchUniversity of Colorado Health Sciences Center
Frame the DiscussionFrame the Discussion
Focus is on the interface between new models that improve geriatric care and strategies that overcome the aging workforce shortage
DisclaimerDisclaimer
lConceptual rather than evidence-based approachl Illustrative examples will be offered of
models under development

Assertions:Assertions:
l Business as usual will not sufficel Need a fundamental shift to promote changel Defenders of the status quo are powerfull The distinguished IOM platform is needed
to chart a course for meaningful change

Pipeline or Funnel?Pipeline or Funnel?
Resources committed to conduct study
Good ideas
Reached study recruitment goals
Rigorous evaluation approach
Positive results
Results appeal to decision makers
Adopted in “real world”

Looking Into Our Crystal BallLooking Into Our Crystal Ball……

Strategic PartnershipsStrategic Partnerships……

Model End Adopters:Model End Adopters:A Moving TargetA Moving Target
l Attracted to “cutting edge” technologyl Reliance on evidence-based practice variesl Expect a short turnaround to achieve ROIl Recognize benefits do not always accrue to
those who make the investment in the model

Partnerships Between Model Partnerships Between Model Developers and EndDevelopers and End--AdoptersAdopters
lToo often operate in isolationlNo formal mechanism to foster collaboration

Need for a Collaborative TriadNeed for a Collaborative Triad
Funders
Model Developers
End Adopters
Variation On A ThemeVariation On A Theme
Payors
Model Developers
End Adopters

Medicare Chronic Care Medicare Chronic Care Practice Research NetworkPractice Research Network
l Led by Cheryl Schraeder, RN, PhD Carle Clinicl Legislation sponsors: Sen Obama and Sen Derbinl Fundamental changes to CMS’ research approach

Limitations of the Current CMS Limitations of the Current CMS Demonstration MechanismDemonstration Mechanism
1) A mismatch between project duration and rate at which benefits accrue to different populations
2) Delayed feedback about program performance makes midstream project adjustments impossible
3) Insufficient means to validate care management best practices to ensure replicability & scalability

Goals of the NetworkGoals of the Network
1) To improve our understanding of which care management interventions achieve the greatest benefit at the lowest possible cost
2) To provide a reproducible, reliable and scalable framework to implement effective standardized care management services nationwide
3) To implement a comprehensive evaluation to assess the impact of care management that has implications for current and future policy
Network ActivitiesNetwork Activities
1) Collaboration between CMS and select group of care providers (Medicare Care Coord Demos)
2) To function as “laboratories” to develop, test, adjust, and re-test new approaches
3) To rigorously assess coordinated care management interventions
4) To enable feedback loops between local organizations and policy makers to accelerate practice and policy refinements

The The AnemicAnemic Aging WorkforceAging Workforce

The Anemic Aging WorkforceThe Anemic Aging Workforce
1. Inadequate red blood cells produced in the “factory” (i.e., health professional schools)
2. Loss of red blood cells (i.e., leaving the field or retirement)
3. Sequestration of red blood cells (i.e., workers’ roles leave them unavailable to effectively care for older adults)

Sequestration: Sequestration: The Spleen of Health Care DeliveryThe Spleen of Health Care Delivery
‘‘All Assessed Up and No Where to GoAll Assessed Up and No Where to Go ‘‘
l Assessment often over-emphasized relative to need for execution of care plan
l Enormous drain on health professionals’ time and providers’ resources
l Ties into IOM goals for greater efficiencyl Need to decrease both the number of assessments
and the length of assessments
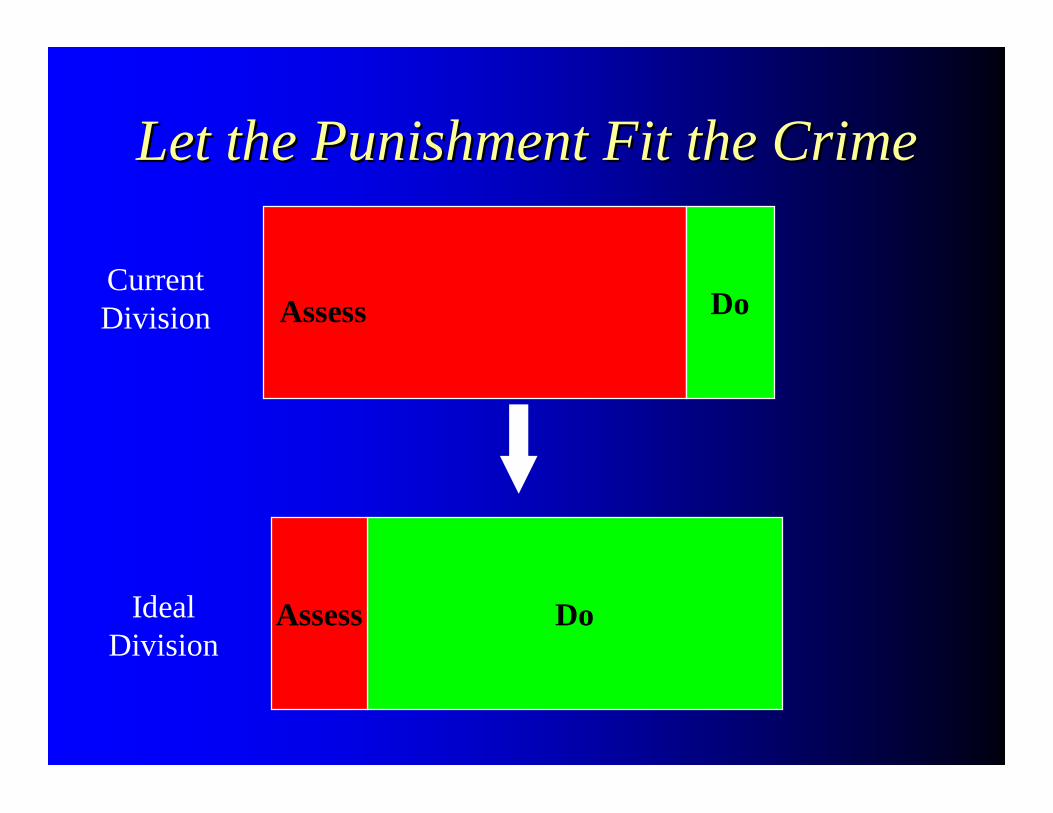
Let the Punishment Fit the CrimeLet the Punishment Fit the Crime
DoAssess
DoAssess
Current Division
Ideal Division
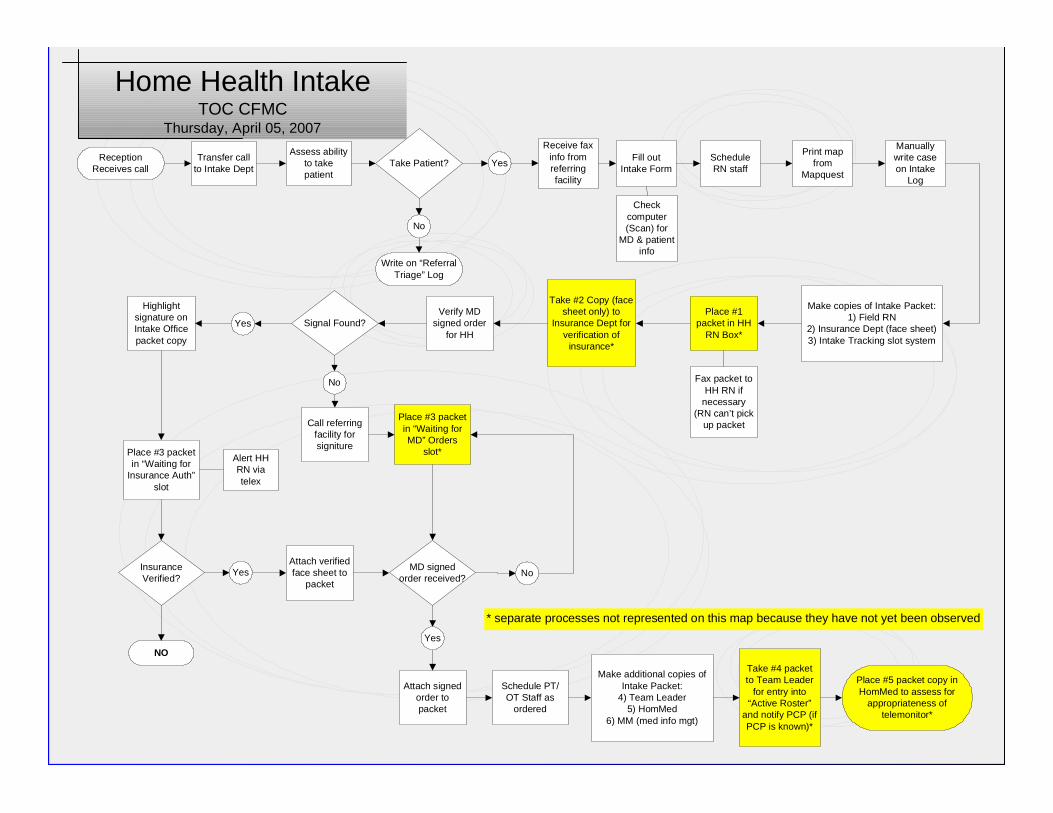
Process MappingProcess Mapping
l Led by Jane Brock, MD, Medical Director of Colorado Foundation for Medical Care
l CMS Special Study to CFMC and UCHSCl Applied principles of lean thinking to intake
and discharge processes for hospital, skilled nursing facilities, and home health care

DisclaimerDisclaimer
Disclaimer: “This material was prepared by CFMC PM-415-076 CO 2007, the Medicare Quality Improvement Organization for Colorado, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy.
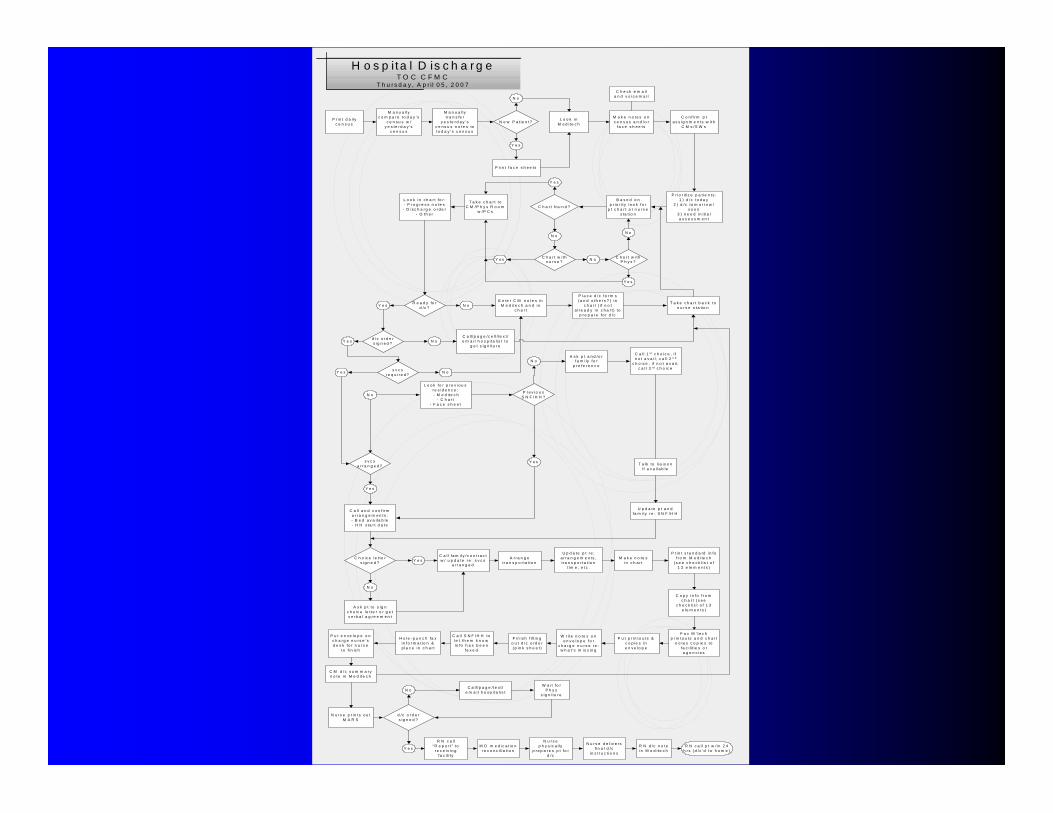
H o s p i ta l D is c h a r g eT O C C F M C
T h u r s d a y , A p r i l 0 5 , 2 0 0 7
P r in t d a i lyc e n s u s
M a n u a l lyc o m p a r e t o d a y ’s
c e n s u s w /y e s te r d a y ’s
c e n s u s
M a n u a l lyt r a n s fe r
y e s te r d a y ’sc e n s u s n o te s tot o d a y ’s c e n s u s
N e w P a t ie n t?
Y e s
N o
L o o k inM e d i t e c h
C h e c k e m a i la n d v o ic e m a i l
M a k e n o te s o nc e n s u s a n d /o r
f a c e s h e e t s
C o n f i r m p ta s s ig n m e n ts w i t h
C M s /S W s
P rin t f a c e s h e e t s
P r io r i tiz e p a t ie n t s :1 ) d / c t o d a y
2 ) d / c t o m o r r o w /s o o n
3 ) n e e d in i t ia la s s e s s m e n t
B a s e d o np r io r i t y lo o k f o r
p t c h a r t a t n u r s es ta t io n
C h a r t f o u n d ?
Y e s
N o
T a k e c h a r t t oC M /P h y s R o o m
w /P C s
C h a r t w i t hn u r s e ?Y e s N o C h a r t w i t h
P h y s ?
Y e s
N o
L o o k in c h a r t f o r :- P r o g r e s s n o te s- D is c h a r g e o r d e r
- O th e r
R e a d y fo rd / c ?Y e s N o
d /c o r d e rs ig n e d ?Y e s N o
E n te r C M n o te s inM e d i t e c h a n d in
c h a r t
P la c e d / c f o r m s( a n d o th e r s ? ) in
c h a r t ( i f n o ta l r e a d y in c h a r t ) t o
p r e p a r e f o r d / c
T a k e c h a r t b a c k t on u r s e s t a tio n
C a ll / p a g e / c e l l / te x t /e m a i l h o s p i t a l is t t o
g e t s ig n i t u r e
s v c sr e q u i r e d ?
Y e s N o
s v c sa r r a n g e d ?
N o
Y e s
L o o k f o r p r e v io u sr e s id e n c e : - M e d it e c h
- C h a r t- F a c e s h e e t
C a l l a n d c o n f i r ma r r a n g e m e n ts :- B e d a v a i la b le- H H s ta r t d a te
P r e v io u sS N F /H H ?
Y e s
N oA s k p t a n d /o r
f a m i ly f o rp r e fe r e n c e
T a lk t o l ia is o ni f a v a i la b le
C a l l 1 s t c h o ic e , i fn o t a v a i l , c a l l 2 n d
c h o ic e , i f n o t a v a i l ,c a l l 3 r d c h o ic e
U p d a te p t a n dfa m i ly r e : S N F /H H
C h o ic e le t t e rs ig n e d ? Y e s
N o
A s k p t t o s ig nc h o ic e le t t e r o r g e tv e r b a l a g r e e m e n t
C a l l f a m i ly / c o n t r a c tw / u p d a te r e : s v c s
a r r a n g e d
A r r a n g et r a n s p o r t a tio n
U p d a te p t r e :a r r a n g e m e n ts ,t ra n s p o r t a t io n
t im e , e t c .
M a k e n o te sin c h a r t
P r in t s t a n d a rd in f of r o m M e d i te c h
( s e e c h e c k l is t o f1 3 e le m e n ts )
C o p y in f o f r o mc h a r t ( s e e
c h e c k l is t o f 1 3e le m e n ts )
F a x M ’ t e c hp r in t o u t s a n d c h a r t
n o te s c o p ie s t of a c i li t ie s o ra g e n c ie s
P u t p r in t o u t s &c o p ie s ine n v e lo p e
W r i t e n o te s o ne n v e lo p e f o r
c h a r g e n u r s e r e :w h a t ’s m is s in g
C M d / c s u m m a r yn o te in M e d i t e c h
F in is h f i l l in go u t d / c o rd e r( p in k s h e e t )
C a l l S N F /H H tole t t h e m k n o win fo h a s b e e n
fa x e d
H o le - p u n c h fa xin f o r m a t io n &p la c e in c h a r t
P u t e n v e lo p e o nc h a r g e n u r s e ’sd e s k f o r n u r s e
to f in is h
N u r s e p r in t s o u tM A R S
d /c o r d e rs ig n e d ?
N o
Y e s
C a l l / p a g e / t e x t /e m a i l h o s p i t a l is t
W a i t f o rP h y s
s ig n i t u r e
R N c a l l“ R e p o r t ” t o
r e c e iv in gfa c i l i t y
N u r s ep h y s ic a l ly
p r e p a r e s p t f o rd / c
N u r s e d e l iv e r sf in a l d / c
in s t r u c t io n s
R N d / c n o tein M e d i t e c h
M D m e d ic a t io nr e c o n c i l ia t io n
R N c a l l p t w / in 2 4h r s ( d / c ’d t o h o m e )
Transfer callto Intake Dept
Assess abilityto takepatient
Home Health IntakeTOC CFMC
Thursday, April 05, 2007
Take Patient?ReceptionReceives call
Write on “ReferralTriage” Log
Receive faxinfo fromreferringfacility
Fill outIntake Form
Checkcomputer(Scan) for
MD & patientinfo
ScheduleRN staff
Print mapfrom
Mapquest
Manuallywrite caseon Intake
Log
Make copies of Intake Packet:1) Field RN
2) Insurance Dept (face sheet)3) Intake Tracking slot system
Place #1packet in HH
RN Box*
Fax packet toHH RN if
necessary(RN can’t pick
up packet
Take #2 Copy (facesheet only) to
Insurance Dept forverification of
insurance*
Verify MDsigned order
for HHSignal Found?
Call referringfacility forsigniture
Place #3 packetin “Waiting forMD” Orders
slot*
MD signedorder received?
Highlightsignature onIntake Officepacket copy
Place #3 packetin “Waiting for
Insurance Auth”slot
Alert HHRN viatelex
InsuranceVerified?
NO
Attach verifiedface sheet to
packet
Attach signedorder topacket
Schedule PT/OT Staff as
ordered
Take #4 packetto Team Leader
for entry into“Active Roster”
and notify PCP (ifPCP is known)*
Make additional copies ofIntake Packet:
4) Team Leader5) HomMed
6) MM (med info mgt)
* separate processes not represented on this map because they have not yet been observed
Place #5 packet copy inHomMed to assess for
appropriateness oftelemonitor*
No
No
No
Yes
Yes
Yes
Yes

What If We ReWhat If We Re--Invested the Time Invested the Time and Resources Dedicated to: and Resources Dedicated to:
l Joint Commission AccreditationlMDS/OASIS/IRF-PAIlHIPAA Compliance

Continuity Assessment Record Continuity Assessment Record and Evaluation (CARE) and Evaluation (CARE)
l CMS tasked to create under Deficit Reduction Actl Cross-setting assessment tool initiated upon
hospital discharge to post-acute carel Three primary purposes:
– Improve information transfer– Longitudinal outcomes assessment– Promote payment reform
CMS contracted awarded to RTI to develop
Sequestration ContinuedSequestration Continued……
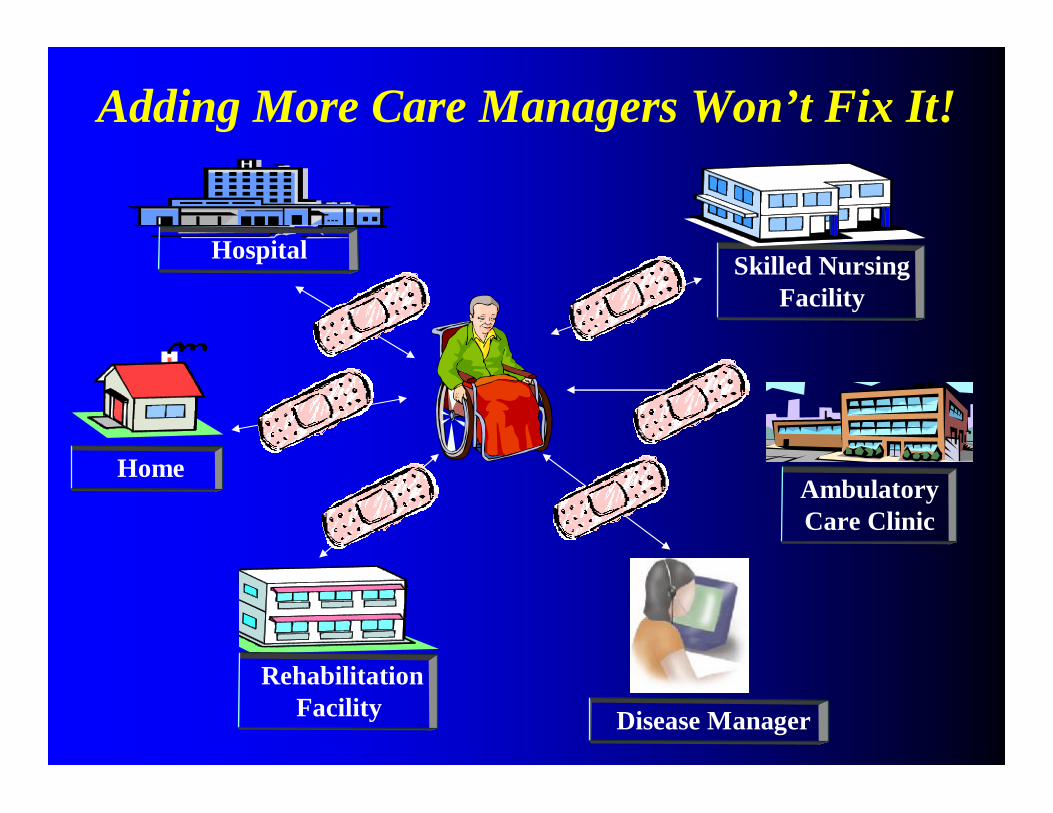
Hospital
HomeAmbulatory Care Clinic
Skilled Nursing Facility
SNF
Rehabilitation Facility Disease Manager
Adding More Care Managers Won’t Fix It!
PolyPoly--Management SyndromeManagement Syndrome
l Physicians deal with multiple care managers– Health plan– Disease category
l Patients deal with multiple care managers– Provider-based– Disease-based– Special programs
Attribution to Cheryl Phillips, MD, CMD
Affect on Older AdultsAffect on Older Adults
l Confused by multiple case/disease managers l Cannot identify their case managerl Become more passive or disengage

Too Many CooksToo Many Cooks……..
Need a care manager for the care managers!
A Solution: Sutter Health SystemA Solution: Sutter Health System
l Formal mechanism for cross referral between health plan and provider programs
l Designate one care manager (ideally with a continuous relationship) to serve as lead, obtaining input of other mangers to create a single plan of care with patient and family
Attribution to Cheryl Phillips, MD, CMD
Returning to Our Analogy Returning to Our Analogy Workforce = Red Blood CellsWorkforce = Red Blood Cells


Need for ChampionsNeed for Champions……
Geriatric Resource NursesGeriatric Resource Nurses
l Nurses Improving Care for Health System Eldersl RNs with enhanced skills in care of older adults l Valuable resource on geriatric best practicesl Improve management of pain, incontinencel Reduce readmission rates
John A. Hartford Foundation Institute for Geriatric Nursing

One Patient, Many Places:
Managing Health Care Transitions
A Report from the HMO Care Management Workgroup
Supported by the Robert Wood Johnson Foundation

Practice Change FellowsPractice Change Fellows
l Build leadership capacity among health care professionals with operational responsibility for aging programs & geriatric service lines
l 10 selected each yearl Nurses, Physicians, Social Workersl Foster national network and platform for change
Supported by Atlantic Philanthropies & John A. Hartford Foundation
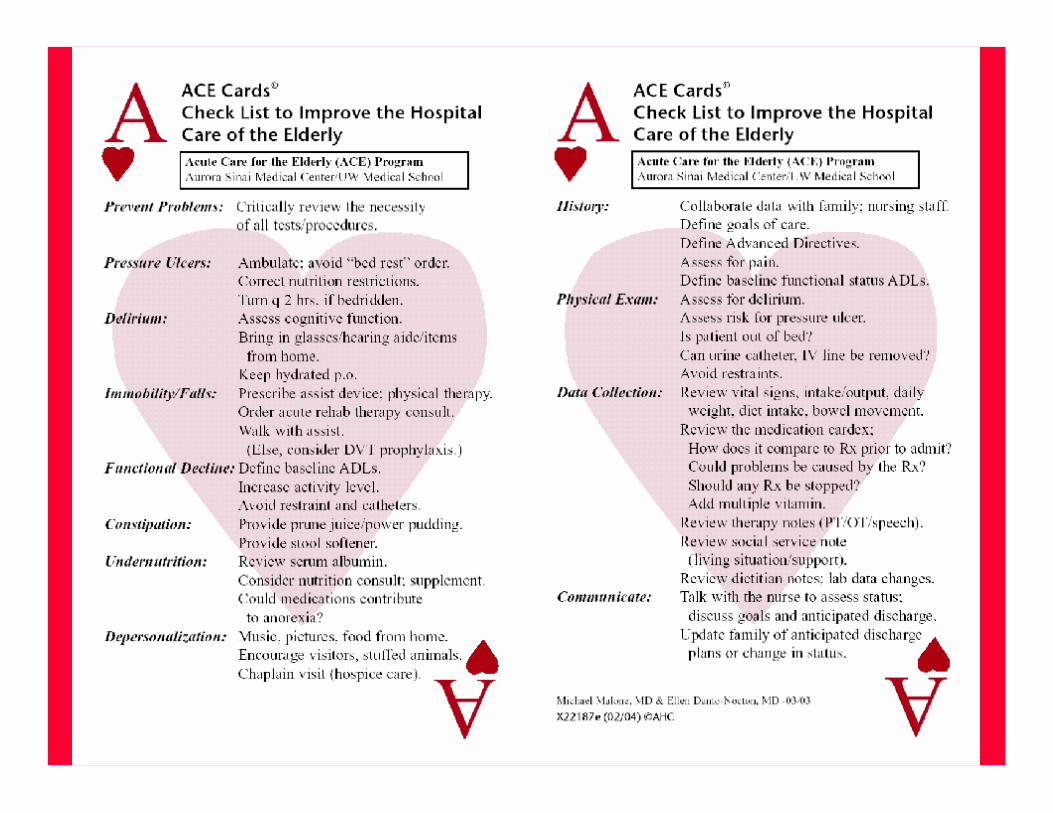
eGeriatricianeGeriatrician and ACE Trackerand ACE Trackerl Cannot build and/or staff
enough ACE unitsl Incorporate principles
into all programsl Reach seniors in urban
and rural settings
Michael L. Malone, MD
Aurora Sinai, Milwaukee WI

ACE TrackerACE Tracker-- PurposePurpose
l To identify vulnerable hospitalized seniors
l To provide focus for interdisciplinary rounds
l To promote care planning
Michael L. Malone, MD

ACE TrackerACE Tracker-- DescriptionDescriptionl Who? Team members
enter data into EMRl What? Daily reportsl Where? 12 hospitalsl Why? Focus on reducing
complications
Michael L. Malone, MD

eGeriatricianeGeriatricianl Urban and rural hospitals
connect via conference call with the “e-Geriatrician”.
Michael L. Malone, MD

GeriatricizeGeriatricize Other DisciplinesOther Disciplines
l “Hospitalists are geriatricians in denial”– Eric Segal, MD Madison Wisconsin
l John A. Hartford Foundation is supporting Society for Hospital Medicine to improve care transitions for older adults
l Develop toolkits to foster adoption amongst hospitalists across the country

Advanced Care Medical HomeAdvanced Care Medical Home
l ACP White Paper: Re-invigorate primary carelMedicare Medical Home Demonstration
– 3 years duration– Urban/rural/underserved areas– Small physician practice encouraged
Components of a Medical HomeComponents of a Medical Home
l Advocates for and provides ongoing support, oversight, and guidance to implement a care plan
l Uses clinical decision support toolsl Develop a health assessment tooll Uses health information technologyl Provides support for self-managementl Promote patient access to health information

Will Physician Practices Join the Party?Will Physician Practices Join the Party?
l External entity would certify medical homesl Amount of compensation to practice unclearl Specialists could qualify to be medical homel Patients choose their medical home

Models That Elicit and Honor Models That Elicit and Honor Patient PreferencesPatient Preferences
Advanced Illness Coordinated Care Advanced Illness Coordinated Care (AICC) Program(AICC) Program
l Developed by Dan Tobin MD (Albany VA) and Dale Larson PhD (UC Santa Clara)
l Approach used for people with advanced illness in all settings
l Continuity across hospital, home based and office based care
Conducted in partnership with SUNY Albany and the Life Institute in Albany with support from the Garfield Memorial Trust
MethodologyMethodology
l Targeted people with heart failure, renal failure, or chronic obstructive lung disease
l Patients identified with “surprise question”l Referred to AICC social worker or RN

AICC Program DescriptionAICC Program Description
l Social worker guides patients with advanced illness as they transition into end-of-life
l AICC program evaluates the patient's ability to confront diagnosis and fears
l Focuses on practical issues such as legal planning and completion of advance directives
AICC: 6 SessionsAICC: 6 Sessions
1. Understand perspective in terms of curative, uncertain, or palliative
2. Assess understanding of condition and prognosis3. Inquire about fears, worries, concerns4. Elicit values, goals and preferences5. Planning for the future 6. Coordinate and support per care plan
Preliminary OutcomesPreliminary Outcomes
l Psycho-social outcomes positivel Cost and utilization will be complete by Fall 2007
– Fewer ICU days– Less intensive care
Hebrew Senior Life Center Hebrew Senior Life Center Green House Green House
l Green House founded as a social model l HSL recognize a subgroup whose move was
prompted by a change in health status and need for more support with chronic illness care
lWeave in elements of a medical model but try to make invisible or at the very least, non intrusive
Attributed to Robert Schreiber, MD
HSL Green HouseHSL Green House
l Integrated medical model into environment in non-obtrusive manner-- “behind the scenes”
l CNA driven model with less visible RN & MDl Home visits using cart with wireless EMR
Attributed to Robert Schreiber, MD
HSL Green House: HSL Green House: Preliminary Findings:Preliminary Findings:
lWeight gain among persons losing weight l Reduced number of medications takenl Fewer fallsl Improved depression scoresl Escaped nosocomial Norwalk virus epidemicl High satisfaction among residents
Attributed to Robert Schreiber, MD
HSL Green House: HSL Green House: Impact on WorkforceImpact on Workforce
l Higher satisfaction and retentionl Career ladder for CNA’s
– Support to obtain English equivalency– Paid during pursuit of LPN degree– Nurse mentor program
l New campus opens 2009--all units will adopt approachl Rigorous measurement strategy to capture outcomes
Attributed to Robert Schreiber, MD

Aliens Did Aliens Did NotNot Build The PyramidsBuild The Pyramids……

And Case Managers Do And Case Managers Do NotNot PerformPerformThe Majority of Care CoordinationThe Majority of Care Coordination……

Family Caregivers As Formal Members Family Caregivers As Formal Members of the Interdisciplinary Team of the Interdisciplinary Team
l Silent partners/care coordinatorsl Tremendous financial offset on health care costsl Role not recognized (i.e., not part of JCAHO
hospital surveys)

Expanding EvidenceExpanding Evidence
l Coordination between formal providers and caregivers improves caregiver preparation to provide care
l Positively associated with patients’ pain control, functional status, and mental health.
D. Weinberg et al., “Coordination Between Formal Providers and Informal Caregivers” . Health Care Manage Rev 2007 32(2) 1-10.

United Health Care United Health Care Caregiver CollegeCaregiver College
l Six 2.5 hour seminars led by professionalsl Held at community based organizationsl Respite dollars available
Attribution to Danielle Butin, OTR and Kathy Alsgaard, RN

UHC Caregiver College:UHC Caregiver College:ObjectivesObjectives
1. To increase caregiver efficacy 2. To increase services and community support3. To increase understanding of benefit plans4. Decrease caregiver burden5. Decrease unnecessary healthcare utilization
Attribution to Danielle Butin, OTR and Kathy Alsgaard, RN

UHC Caregiver College:UHC Caregiver College:Core TopicsCore Topics
l Symptom managementl Self-care managementlMedication managementl Emergency managementl Emotional copingl End of life planning
Attribution to Danielle Butin, OTR and Kathy Alsgaard, RN

One Final Look at SequestrationOne Final Look at Sequestration
Electronic Health Electronic Health Information ExchangeInformation Exchange
l Interoperability is a worthy goall Adoption of HIT particularly low among
nursing homes and home health care agenciesl Lack of data standards for physical and
cognitive function, roles of family caregivers

Health Information Exchange Across Health Information Exchange Across Acute, PostAcute, Post--Acute, & LongAcute, & Long--Term CareTerm Care
l Business case needs to be more compellinglWorkflow concerns as challenging as technologyl Use of national data standards not a high priority
Supported by the Office of the Assistant Secretary of Planning and Evaluation, Department of Health and Human Services

State of Indiana: State of Indiana: Docs4DocsDocs4Docs
l Facilitators:– Unique patient identifier– Statewide e-prescribing– Leadership and financing of hospitals
l Information available:– Laboratory and radiology reports– Pharmacy data– Discharge summaries
Standardize Communication For Standardize Communication For Family Caregiver Role (s)Family Caregiver Role (s)
T= Primary Tumor Description
N= Nodal Involvement
M= Metastasis
F= Financial
A= Advocacy
C= Care Coordination
E= Emotional Support
D= Direct Care Provision























![Looking back and looking forward[1]](https://img.dokumen.tips/doc/110x75/5559ad0dd8b42aa4288b511b/looking-back-and-looking-forward1.jpg)





