-
8/12/2019 Lifestyle,DM,CVD Risk Factors
1/11
n engl j med 351;26 w w w. ne jm . org d ec em be r 23, 2004
2683
The
new englandjournal of
medicine
established in 1812
december
23
, 2004
vol. 3 51 no. 26
Lifestyle, Diabetes, and Cardiovascular Risk Factors 10
Yearsafter Bariatric Surgery
Lars Sjstrm, M.D., Ph.D., Anna-Karin Lindroos, Ph.D., Markku
Peltonen, Ph.D., Jarl Torgerson, M.D., Ph.D.Claude Bouchard, Ph.D.,
Bjrn Carlsson, M.D., Ph.D., Sven Dahlgren, M.D., Ph.D., Bo Larsson,
M.D., Ph.D.,Kristina Narbro, Ph.D., Carl David Sjstrm, M.D., Ph.D.,
Marianne Sullivan, Ph.D., and Hans Wedel, Ph.D.,
for the Swedish Obese Subjects Study Scientific Group*
abs t r ac t
From the Departments of Body Composi-tion and Metabolism (L.S.,
A.-K.L., B.C.,K.N., M.S.) and Anesthesiology (B.L.,C.D.S.),
Sahlgrenska University Hospital,Gteborg, Nordic University of
PublicHealth (H.W.), Gteborg; the Medical De-partment, Norra
lvsborgs Lns Hospital,Trollhttan (J.T.); and Brjegatan 10B,Uppsala
(S.D.) all in Sweden; the De-partment of Epidemiology and Health
Pro-motion, National Public Health Institute,Helsinki, Finland
(M.P.); and PenningtonBiomedical Research Center, Louisiana
State University, Baton Rouge (C.B.). Ad-dress reprint requests
to Dr. Lars Sjstrmat SOS Secretariat, Sahlgrenska
UniversityHospital, S-413 45 Gteborg, Sweden.
*The members of the Swedish Obese Sub-jects (SOS) Study
Scientific Group are list-ed in the Appendix.
N Engl J Med 2004;351:2683-93.
Copyright 2004 Massachusetts Medical Society.
background
Weight loss is associated with short-term amelioration and
prevention of metabolicand cardiovascular risk, but whether these
benefits persist over time is unknown.
methods
The prospective, controlled Swedish Obese Subjects Study
involved obese subjects whounderwent gastric surgery and
contemporaneously matched, conventionally treatedobese control
subjects. We now report follow-up data for subjects (mean age, 48
years;mean body-mass index, 41) who had been enrolled for at least
2 years (4047 subjects)or 10 years (1703 subjects) before the
analysis (January 1, 2004). The follow-up rate forlaboratory
examinations was 86.6 percent at 2 years and 74.5 percent at 10
years.
results
After two years, the weight had increased by 0.1 percent in the
control group and haddecreased by 23.4 percent in the surgery group
(P
-
8/12/2019 Lifestyle,DM,CVD Risk Factors
2/11
n engl j med 351;26
w ww.n ej m. org d ec em b er 23
, 2004
The
new england journal of
medicine
2684
besity is associated with in-
creased morbidity and mortality.
1
The in-creased morbidity is assumed to be me-
diated mainly by insulin resistance, diabetes,hypertension, and
lipid disturbances conditionsthat affect one quarter of the North
American pop-
ulation.
2,3
Over the short term (one to three years),lifestyle changes
resulting in weight loss result inimprovements in insulin
resistance,
4
diabetes,
5-7
hypertension,
8
and lipid disturbances
9-11
or in theprevention of these conditions. In contrast,
several(but not all
12
) observational epidemiologic studieshave suggested that weight
loss is associated withincreased overall mortality and mortality
from car-diovascular causes, not only among thin
13
and nor-mal-weight
14
subjects, but also among obese sub- jects.
15-17
One overall aim of the Swedish Obese Subjects(SOS) Study was to
address this apparent discrep-
ancy between the effects of weight loss on risk fac-tors and
hard end points. In the current study, weassessed changes in
cardiovascular risk factors overfollow-up periods of 2 and 10 years
in surgically treated subjects and contemporaneously
matched,conventionally treated control subjects. Changes inenergy
intake and physical activity over the 10-yearperiod were also
evaluated.
study design
The SOS Study was a prospective, nonrandomized,intervention
trial involving 4047 obese subjects. Theoutcomes in a surgically
treated group were com-pared with those in a contemporaneously
matched,conventionally treated control group.
18 For the pur-poses of this report, all subjects who had been
en-rolled at least 2 years (4047 subjects) or 10 years(1703
subjects) before the date of the analysis (Jan-uary 1, 2004) were
included. The 4047 subjects wereall those who were finally enrolled
in the SOS inter- vention study.
The seven ethics review boards involved in theSOS Study approved
the protocol. Informed consent was obtained both from the subjects
in the registry study and from those in the intervention study.
Registry Examination
As a result of recruitment campaigns through themass media and
at 480 primary health care centersin Sweden, 11,453 subjects living
in participating
counties (18 of the 24 counties in Sweden) sent stan-dardized
application forms to the SOS secretariat between September 1987 and
November 2000. All8966 applicants who fulfilled age and
weight-for-height criteria were provided written informationabout
the surgical and nonsurgical treatments of-
fered by the SOS Study. They also completed ques-tionnaires and
were asked whether they wanted toparticipate as surgically treated
or medically treatedsubjects. All 7593 subjects who returned their
ques-tionnaires were offered participation in the registry
examination, and 6905 completed that examina-tion. According to
individual treatment preferencesand data obtained from the registry
examination,eligible subjects were assigned either to the surgery
group of the intervention study or to a pool of poten-tial control
subjects.
Surgical Visit
The eligibility of candidates for surgery was deter-mined by
computer, and the result was manually checked by the examining
surgeon. If a candidate was eligible, an operation was scheduled.
On aver-age, the surgical visit occurred eight months afterthe
registry examination and five months before theoperation itself,
which marked the start of the inter- vention study. Eight weeks
before a subject under- went surgery, an optimal matched control
was se-lected, on the basis of variables described below,from among
the subjects in the pool of potentialcontrols. Thus, matching was
contemporaneousand was based on registry data, both for the
surgi-cally treated subjects and for the control subjects.
Inclusion Examination
The inclusion examination for subjects for whomsurgery was
planned and for their matched controls was undertaken 4 weeks
before surgery (i.e., 4 weeksbefore the start of the intervention
study), on aver-age 13 months after the registry examination.
Thisdelay was a consequence of the waiting time for sur-gery at the
25 participating surgical departments.The controls underwent their
manual eligibility check at the time of the inclusion
examination.
Intervention Study
The intervention study for a surgically treated sub- ject and
his or her matched control began on the day of the surgically
treated subjects operation. Thedates of all subsequent examinations
(at 0.5, 1.0,2.0, 3.0, 4.0, 6.0, 8.0, and 10.0 years) for both
sub-
o
m e t h o d s
Copyright 2004 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org on May 23, 2005 . This
article is being provided free of charge for use in Indonesia.
-
8/12/2019 Lifestyle,DM,CVD Risk Factors
3/11
n engl j med 351;26
w ww.n ej m. org d ec em b er 23, 2004
long-term weight loss and changes in cardiovascular risk
factors
2685
jects were calculated in relation to the date of sur-gery.
Inclusion criteria for the intervention study were a body-mass
index (calculated as the weight in kilograms divided by the square
of the height inmeters) of 34 or more (for men) or 38 or more (for
women) and an age of 37 to 60 years. Exclusion cri-
teria, described elsewhere,
18
were minimal and were aimed at ensuring that the subjects in the
sur-gery group could tolerate the operation. Identicalinclusion and
exclusion criteria were used in the twostudy groups. Subjects with
diabetes, hypertension,or lipid disturbances were not excluded, nor
weresubjects who had had a myocardial infarction or astroke more
than six months before inclusion.
Matching
The SOS Study was not randomized; rather, sub- jects were
matched according to the method of se-quential treatment
assignment,
19
with balancing
of confounding factors measured at baseline in pro-spective,
nonrandomized intervention trials. Thefollowing 18 matching
variables were considered
18
:sex, age, weight, height, waist and hip circumfer-ences,
systolic blood pressure, serum cholesteroland triglyceride levels,
smoking status, diabetes,menopausal status, four psychosocial
variables withdocumented associations with the risk of death,
andtwo personality traits related to treatment preferenc-es. The
investigators had no influence on the com-puterized matching
process.
Clinical and Biochemical Assessments
At each visit, measurements of weight, height, waist
circumference, and blood pressure were obtained.In addition, energy
intake (in kilocalories per day) was estimated with use of the
validated SOS Dietary Questionnaire.
20,21
Subjects were also asked to ratetheir physical activity during
leisure and work timeon a scale from 1 to 4, in which 1 denotes
sedentary activity and 4 regular strenuous exercise.
20,22
In thecurrent report, ratings were dichotomized; a ratingof 1
corresponded to physically inactive and ratingsof 2, 3, or 4 to
physically active.
Biochemical variables were measured at the reg-istry
examination, at the inclusion examination(year 0 of the
intervention study), and at years 2 and10 of the intervention study
(Table 1). All bloodsamples, which were obtained in the morning
aftera 10-to-12-hour fast, were analyzed at the CentralLaboratory
of Sahlgrenska University Hospital (ac-credited according to
European Norm EN45001).
The schedule, questionnaires, blood pressure andanthropometric
measurements, and laboratory ex-aminations were identical for
surgically treated sub- jects and their matched controls.
treatments
The surgically treated subjects underwent fixed or variable
banding, vertical banded gastroplasty, orgastric bypass.
23
The contemporaneously matchedcontrols received the nonsurgical
treatment for obe-sity that was customary for the center at which
they were registered. No attempt was made to standard-ize the
nonsurgical treatment, which ranged fromsophisticated lifestyle
intervention and behaviormodification to, in some practices, no
treatment whatsoever. No antiobesity drugs were approved inSweden
until 1998.
criteria for health and disease
Criteria for health and disease were based on cutoff values or
the use of medication for the condition inquestion, according to
principles specified else- where.
11
However, in the course of the study, thecriterion for diagnosing
diabetes decreased to a fast-ing blood glucose level of 110 mg per
deciliter (6.1mmol per liter) or greater, corresponding to a
fast-ing plasma glucose level of 126 mg per deciliter(7.0 mmol per
liter) or greater, in accordance withthe new criteria of the
American Diabetes Associa-tion.
24
Similarly, the criterion for diagnosing hy-pertension decreased
to a systolic pressure of 140mm Hg or greater or a diastolic
pressure of 90mm Hg or greater.
25
Other criteria included thefollowing: hypercholesterolemia
(cholesterol level,201 mg per deciliter [5.2 mmol per liter] or
great-er
26
); hypertriglyceridemia (triglyceride level, 150mg per deciliter
[1.7 mmol per liter] or greater
26
);a low level of high-density-lipoprotein (HDL) cho-lesterol
(less than 39 mg per deciliter [1.0 mmolper liter]
26
); and hyperuricemia (uric acid level, 7.6mg per deciliter [450
mol per liter] or greater inmen and 5.7 mg per deciliter [340 mol
per liter] orgreater in women).
outcome variables
The primary outcome variable in the SOS Study as a whole was
overall mortality. Three secondary out-come variables are described
in this report. The first was the difference between the surgery
group andthe control group with respect to changes in body weight,
risk factors, energy intake, and the propor-
Copyright 2004 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org on May 23, 2005 . This
article is being provided free of charge for use in Indonesia.
-
8/12/2019 Lifestyle,DM,CVD Risk Factors
4/11
n engl j med 351;26
w ww.n ej m. org d ec em b er 23
, 2004
The
new england journal of
medicine
2686
tion of subjects who were physically active. Thesecalculations
included all the subjects and did not take medication use or
baseline disease into ac-count. The next secondary outcome was the
dif-ference between the two groups in the incidence of risk
conditions over 2- and 10-year periods amongthe subjects unaffected
by those risk conditions at baseline (i.e., the primary preventive
effect of weight loss). The final secondary outcome was the
differ-
ence between the two groups in the rate of recovery from risk
conditions over 2- and 10-year periodsamong those who had been
affected by those con-ditions at baseline.
statistical analysis
The intervention study had 80 percent power (at an alpha level
of 0.05) to detect a difference in totalmortality between a group
of 2000 surgically treat-
* Plusminus values are means SD. To convert the values for
glucose to milligrams per deciliter, divide by 0.05551. To convert
the values forinsulin to picomoles per liter, multiply by 7.175. To
convert the values for uric acid to milligrams per deciliter,
divide by 59.48. To convert thevalues for triglycerides to
milligrams per deciliter, divide by 0.01129. To convert the values
for cholesterol to milligrams per deciliter, divideby 0.02586. HDL
denotes high-density lipoprotein.
Among the subjects who did not complete 10 years of the study,
the controls were older and had higher systolic blood pressure than
the sur-gically treated subjects, whereas the surgically treated
subjects were heavier and had a larger waist circumference (P
values not shown).
P values are for the comparison with data for subjects in the
control group under the indicated conditions. P values are for the
comparison with matching data for subjects in the control group who
completed the 10-year examination. P values are for the comparison
with matching data for subjects in the surgically treated group who
completed the 10-year examination. P
-
8/12/2019 Lifestyle,DM,CVD Risk Factors
5/11
n engl j med 351;26
w ww.n ej m. org d ec em b er 23, 2004
long-term weight loss and changes in cardiovascular risk
factors
2687
ed subjects and a group of 2000 controls followedfor 10
years.
18
To evaluate the originally chosentreatment strategy according to
pragmatic clinical-treatment principles,
27
subjects in the surgery group who completed 10 years of the
study and who un-derwent reoperation (band removal in 15
subjects
and conversion to another type of surgical treatment in 62) or
who had a spontaneous band disruption(in 2 subjects) were
considered surgically treatedand remained in their original
treatment subgroup.Similarly, control subjects who later underwent
bar-iatric surgery (34 subjects) were considered controlsthroughout
the study. All analyses presented hereare based on data from
subjects who completed 2 or10 years of the study. However, for
confirmatory rea-sons, additional calculations were performed by
re-placing all missing data with baseline data, accord-ing to the
baseline observation carried forwardmethod.
28
Mean values and standard deviations are used todescribe the
baseline characteristics of the two treat-ment groups. Analysis of
covariance was used to test for differences in changes in risk
factors betweenthe two treatment groups. Treatment group was
in-cluded as a covariate, as were sex, age, body-massindex, and the
baseline level of each studied varia-ble. Adjusted differences,
with 95 percent confi-dence intervals, are reported. Logistic
regression was used to compare the incidence of disease andrates of
recovery. The data were adjusted for sex,age, and body-mass index
at baseline, and the re-sulting differences in risk are reported as
odds ra-tios with 95 percent confidence intervals. All report-ed P
values are two-sided. Statistical analyses werecarried out with use
of the Stata statistical package(version 7.0).
29
subjects
At least 10 years before the date of the current analy-sis, 851
surgically treated subjects had been enrolledin the SOS Study. The
surgically treated subjects hadbeen contemporaneously matched with
852 obesecontrol subjects. The matching resulted in twogroups that
were not significantly different with re-spect to sex distribution,
height, blood pressure,blood glucose level, serum lipid levels, or
serum uricacid level (data not shown). At the time of matching,the
surgically treated subjects were slightly young-er than the control
subjects (46.1 vs. 47.4 years of
age, P=0.005), were heavier (119.2 vs. 116.1 kg,P
-
8/12/2019 Lifestyle,DM,CVD Risk Factors
6/11
n engl j med 351;26
w ww.n ej m. org d ec em b er 23
, 2004
The
new england journal of
medicine
2688
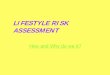
gastroplasty (Fig. 1). The fractions of subjects who,after
completing 10 years of the study, had a loss of less than 5 percent
of their initial weight were 72.7percent (control group), 8.8
percent (gastric-bypasssubgroup), 13.8 percent
(vertical-banded-gastro-plasty subgroup), and 25.0 percent (banding
sub-group). The fractions of subjects achieving 20 per-cent weight
loss or more over the 10-year period were 3.8 percent (control
group), 73.5 percent (gas-tric-bypass subgroup), 35.2 percent
(vertical-band-ed-gastroplasty subgroup), and 27.6 percent
(band-ing subgroup).
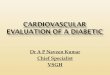
lifestyle changes
Mean energy intake at the time of inclusion in theintervention
study was 2882 kcal per day among thesurgically treated subjects,
as compared with 2526kcal per day among the controls. As Figure 2
andTable 2 indicate, the baseline adjusted energy intake was
significantly lower in the surgery group than inthe control group
over the 10-year period. Similar-ly, the fraction of subjects
physically active during
leisure time was higher in the surgery group overthe 10-year
period, and the fraction of those physi-cally active during work
time was higher in the sur-gery group for the first 6 years of the
intervention.
effects on anthropometric variablesand mean risk-factor
values
Table 2 shows the changes in risk factors for allavailable
subjects, independent of baseline statusand medication use. The
waist circumference wasreduced more in the surgery group than in
the con-trol group after 2 and 10 years. Glucose and insulinlevels
increased in the control group, whereas sub-stantial decreases were
seen in the surgically treat-ed group after both 2 and 10 years of
observation.Similarly, changes in uric acid, triglyceride, andHDL
cholesterol levels were more favorable in thesurgically treated
group than in the control groupafter 2 and 10 years. Systolic blood
pressure was re-duced by more in the surgery group at two
yearsonly. Diastolic blood pressure and total cholesterol were
reduced by more in the surgery group than in
Figure 1. Weight Changes among Subjects in the SOS Study over a
10-Year Period.
All data are for subjects who completed 10 years of the study.
The average weight change in the entire group of surgicallytreated
subjects was almost identical to that in the subgroup of subjects
who underwent vertical banded gastroplasty.TheI
bars represent the 95 percent confidence intervals.
5
W e i g h
t C h a n g e
( % )
5
0
10
15
25
30
40
20
35
450.0 1.00.5 2.0 3.0 4.0 6.0 8.0 10.0
Control
Banding
Vertical bandedgastroplasty
Gastricbypass
Years of Follow-up
No. of SubjectsControlBandingVertical banded gastroplastyGastric
bypass
62715645134
53514440129
54214741232
56315041732
57714942933
58715343834
58515043834
59415443834
62715645134
Copyright 2004 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org on May 23, 2005 . This
article is being provided free of charge for use in Indonesia.
-
8/12/2019 Lifestyle,DM,CVD Risk Factors
7/11
n engl j med 351;26
w ww.n ej m. org d ec em b er 23, 2004
long-term weight loss and changes in cardiovascular risk
factors
2689
* D a t a a r e
f o r a l
l s u b
j e c t s w
h o c o m p l e t e d
2 a n
d 1 0 y e a r s o f
t h e s t u d y a n
d a r e
i n d e p e n
d e n t o f
d i a g n o s i s a n
d m e d
i c a t
i o n
s a t o r a f
t e r
b a s e
l i n e .
T h e c h a n g e s w
i t h i n e a c h
t r e a
t m e n
t g r o u p a r e
u n a d
j u s t e d , w
h e r e a s
t h e
d i f f e r e n c e s
b e t w e e n
t h e g r o u p s
i n t h e c h a n g e s
h a v e
b e e n a d
j u s t e d
f o r s e x , a g e ,
b o d y - m a s s
i n d e x
( B M I )
, a n d
t h e
b a s e
l i n e
l e v e
l o f t h e r e s p e c t
i v e v a r i a b
l e . C
I d e -
n o t e s c o n f
i d e n c e
i n t e r v a l , a
n d H D L h i g h - d e n s i
t y l i p o p r o
t e i n
.
F o r v a l u e s w
i t h i n e a c h g r o u p , m
i n u s s i g n s
d e n o
t e d e c r e a s e s ;
f o r d
i f f e r e n c e s
b e t w e e n
t h e g r o u p s , m
i n u s s i g n s
d e n o
t e s m a l
l e r r e d u c
t i o n s o r
( i n
t h e c a s e o f
H D L c h o l e s t e r o l
) l a r g e r
i n c r e a s -
e s i n t h e s u r g
i c a l g r o u p
t h a n
i n t h e c o n t r o
l g r o u p .
P v a
l u e s a r e
f o r
t h e c o m p a r i s o n w
i t h t h e
b a n d
i n g s u
b g r o u p .
P < 0 . 0 0 1 .
P < 0 . 0 5
.
P < 0 . 1 0
.
T a b l e
2 . P e r c e n
t a g e
C h a n g e s
i n W e i g h
t , A n t
h r o p o m e t r i c
V a r i a b
l e s ,
R i s k F a c t o r s , a n
d E n e r g y
I n t a k e a t
2 a n
d 1 0 Y e a r s .
*
V a r i a b
l e
C h a n g e s a t
2 Y r
C h a n g e s a t
1 0 Y r
C h a n g e s a t
1 0 Y r
i n S u r g e r y S u b g r o u p s
C o n
t r o l
G r o u p
( N =
1 6 6 0 )
S u r g e r y
G r o u p
( N = 1
8 4 5 )
D i f f e r e n c e
( 9 5 % C I )
C o n
t r o l
G r o u p
( N =
6 2 7 )
S u r g e r y
G r o u p
( N =
6 4 1 )
D i f f e r e n c e
( 9 5 % C I )
B a n
d i n g
( N = 1
5 6 )
V e r
t i c a
l B a n
d e d
G a s
t r o p
l a s t y
( N = 4
5 1 )
G a s
t r i c B y p a s s
( N = 3
4 )
p e r c e n t
p e r c e n t
p e r c e n t
W e i g h
t
0 . 1
2 3 . 4
2 2 . 2
( 2 1 . 6 t o 2 2 . 8 )
1 . 6
1 6 . 1
1 6 . 3
( 1 4 . 9 t o 1 7
. 6 )
1 3 . 2
1 6 . 5
2 5 . 0
H e i g h
t
0 . 0
1
0 . 0
6
0 . 0 6 ( 0
. 0 2 t o 0
. 1 0 )
0 . 3
0 . 3
0 . 0 1
( 0 . 1 2 t o 0 . 1 0 )
0 . 2
0 . 3
0 . 8
B M I
0 . 1
2 3 . 3
2 2 . 1
( 2 1 . 5 t o 2 2 . 7 )
2 . 3
1 5 . 7
1 6 . 5
( 1 5 . 1 t o 1 7
. 8 )
1 2 . 8
1 6 . 0
2 3 . 8
W a i s t
0 . 2
1 6 . 9
1 6 . 0
( 1 5 . 4 t o 1 6 . 5 )
2 . 8
1 0 . 1
1 1 . 3
( 1 0 . 3 t o 1 2
. 4 )
7 . 6
1 0 . 2
1 9 . 3
S y s t o l
i c b l o o
d p r e s s u r e
0 . 5
4 . 4
2 . 8 ( 2
. 1 t o 3 . 6 )
4 . 4
0 . 5
1 . 1 ( 0 . 3 t o 2 . 6 )
2 . 1
0 . 4
4 . 7
D i a s t o l
i c b l o o
d p r e s s u r e
0 . 3
5 . 2
3 . 2 ( 2
. 4 t o 3 . 9 )
2 . 0
2 . 6
2 . 3
( 3 . 5 t o 1 . 0
)
1 . 4
2 . 5
1 0 . 4
P u l s e p r e s s u r e
3 . 2
0 . 6
0 . 5
( 2 . 3 t o 1 . 3 )
1 8 . 0
1 0 . 8
3 . 5 ( 0
. 1 t o 6 . 9 )
1 3 . 8
1 0 . 1
6 . 3
G l u c o s e
5 . 1
1 3 . 6
1 6 . 6
( 1 5 . 0 t o 1 8 . 3 )
1 8 . 7
2 . 5
1 8 . 4
( 1 4 . 7 t o 2 2
. 1 )
0 . 8
2 . 5
1 0 . 0
I n s u
l i n
1 0 . 3
4 6 . 2
5 1 . 4
( 4 8 . 0 t o 5 4 . 8 )
1 2 . 3
2 8 . 2
3 0 . 3
( 2 3 . 9 t o 3 6
. 6 )
2 5 . 3
2 7 . 2
5 4 . 0
U r i c a c
i d
0 . 4
1 4 . 9
1 3 . 5
( 1 2 . 5 t o 1 4 . 6 )
3 . 9
6 . 2
8 . 8 ( 6
. 4 t o 1 1
. 1 )
5 . 2
6 . 1
1 2 . 3
T r i g l y c e r i
d e s
6 . 3
2 7 . 2
2 9 . 9
( 2 7 . 4 t o 3 2 . 5 )
2 . 2
1 6 . 3
1 4 . 8
( 1 0 . 4 t o 1 9
. 1 )
1 8 . 0
1 4 . 9
2 8 . 0
H D L c h o l e s
t e r o
l
3 . 5
2 2 . 0
1 8 . 7 ( 2 0
. 1 t o 1
7 . 3 )
1 0 . 8
2 4 . 0
1 3 . 6 ( 1 6
. 5 t o 1
0 . 6 )
2 0 . 4
2 3 . 5
4 7 . 5
T o t a l c h o l e s t e r o l
0 . 1
2 . 9
1 . 0 ( 0
. 1 t o 1 . 9 )
6 . 0
5 . 4
2 . 0
( 0 . 2 t o 3 . 8
)
5 . 0
5 . 0
1 2 . 6
E n e r g y
i n t a k e
2 . 8
2 8 . 6
1 9 . 1
( 1 6 . 0 t o 2 2 . 2 )
1 . 0
2 0 . 7
1 1 . 6
( 8 . 1
t o 1 5
. 0 )
1 9 . 7
2 1 . 6
1 2 . 6
Copyright 2004 Massachusetts Medical Society. All rights
reserved.Downloaded from www.nejm.org on May 23, 2005 . This
article is being provided free of charge for use in Indonesia.
-
8/12/2019 Lifestyle,DM,CVD Risk Factors
8/11
n engl j med 351;26
w ww.n ej m. org d ec em b er 23
, 2004
The
new england journal of
medicine
2690
the control group after 2 years but less reduced af-ter 10
years. The pulse-pressure increase was less
pronounced in the surgery group than in the con-trol group after
10 years (Table 2).
The 10-year changes in weight, body-mass in-dex, and waist
circumference were larger for sub- jects who underwent vertical
banded gastroplasty and gastric bypass than for those who underwent
banding. Insulin, triglyceride, HDL cholesterol, andtotal
cholesterol levels were more improved amongthe subjects who
underwent gastric bypass thanamong those who underwent banding
(Table 2).
effects on incidence of and recoveryfrom risk conditions
As Figure 3 shows, the incidence rates of hyper-triglyceridemia,
diabetes, and hyperuricemia weremarkedly lower in the surgically
treated group thanin the control group after 2 and 10 years. The
inci-dence of low HDL cholesterol was significantly low-er in the
surgical group after 2 years but not after 10 years. The incidence
of hypertension and hyper-cholesterolemia did not differ between
the groupsover the 2- and 10-year periods (Fig. 3).
Recovery from hypertension, diabetes, hyper-triglyceridemia, a
low HDL cholesterol level, and hy-peruricemia was more frequent in
the surgical group
than in the control group, both at 2 and 10 years(Fig. 4). The
rates of recovery from hypercholester-olemia did not differ between
the two groups aftereither 2 or 10 years.
E n e r g y
I n t a k e ( k c a
l / d a y )
0 1.00.5 2.0 3.0 4.0 6.0 8.0 10.0
Years of Follow-up
0 1.00.5 2.0 3.0 4.0 6.0 8.0 10.0Years of Follow-up
0 1.00.5 2.0 3.0 4.0 6.0 8.0 10.0
Years of Follow-up
Control
Surgery
P r o p o r
t i o n
A c t
i v e
d u r i n g
L e i s u r e
T i m e
( % )
Control
Surgery
P r o p o r
t i o n
A c t
i v e a t
W o r
k ( % )
20
0
40
80
60
100
20
0
40
80
60
100
500
0
1000
2500
2000
1500
3000
Control
Surgery
A
B
C
** * * ** * **
** * * ** * *
* *
Figure 2. Lifestyle Changes among the Subjectsin the SOS Study
over a 10-Year Period.
Mean energy intake (in kilocalories per day) (Panel A)and the
percentage of subjects who were physically ac-tive during leisure
time and at work (Panels B and C, re-spectively) are shown. Energy
intake and the proportionof active subjects at baseline (year 0)
are unadjustedvalues, whereas the values during the follow-up
havebeen adjusted for sex, age, body-mass index, and energyintake
or physical activity at baseline. All data are fromsubjects who
completed 10 years of the study. The num-bers of subjects at each
time point are the same as thoseshown in Figure 1. Asterisks denote
P
-
8/12/2019 Lifestyle,DM,CVD Risk Factors
9/11
n engl j med 351;26
w ww.n ej m. org d ec em b er 23, 2004
long-term weight loss and changes in cardiovascular risk
factors
2691
baseline observations carried forward
In additional calculations, all missing observations were
replaced by baseline observations. The conclu-sions with respect to
mean risk-factor values, inci-dence rates, and rates of recovery
for subjects whocompleted the study remained the same in the
analy-
sis in which baseline observations were carried for- ward (data
not shown).
death and other adverse events
Five of the 2010 subjects who underwent surgery (0.25 percent)
died postoperatively. As reportedelsewhere for 1164 patients,
23
151 (13.0 percent)had 193 postoperative complications (bleeding
in0.5 percent, embolism or thrombosis in 0.8 per-cent, wound
complications in 1.8 percent, deep in-fections [leakage or abscess]
in 2.1 percent, pul-monary complications in 6.1 percent, and
othercomplications in 4.8 percent). In 26 patients (2.2
percent), the postoperative complications were se-rious enough
to require reoperation. The study isongoing with respect to
analyses of mortality andthe incidence of myocardial infarction,
stroke, andcancer. The safety monitoring committee found noreason
to interrupt the study prematurely becauseof positive effects or
harm.
The surgically treated subjects in this study hadgreater weight
loss, more physical activity, and low-er energy intake than the
control subjects over a 10- year period. Furthermore, the 2- and
10-year ratesof recovery from all the studied risk factors, except
hypercholesterolemia, were more favorable in thesurgery group than
in the control group, as werethe 2- and 10-year incidence rates of
hypertriglycer-idemia, diabetes, and hyperuricemia. All
reportedresults are based on subjects who completed 2 or10 years of
the study. However, the conclusions re-mained the same when data
from all included sub- jects were used and missing follow-up data
werereplaced by baseline data, according to the conser- vative
baseline observation carried forward pro-cedure.
28
The mean changes in weight and risk factors were more favorable
among the subjects treated by gastric bypass than among those
treated by band-ing or vertical banded gastroplasty. The low
num-ber of subjects who were followed for 10 years after
gastric bypass prohibited incidence and recovery calculations,
but the technique appears to be a cur-rent method of choice. The
large weight loss aftergastric bypass, as compared with that after
the oth-er types of surgery, may be related to altered gut-to-brain
signaling.
30,31
Most intervention studies with one to three yearsof follow-up
are in agreement with our two-year ob-
d i s c u s s i o n
Figure 3. Incidence of Diabetes, Lipid Disturbances,
Hypertension, and Hy-peruricemia among Subjects in the SOS Study
over 2- and 10-Year Periods.
Data are for subjects who completed 2 years and 10 years of the
study. Thebars and the values above the bars indicate unadjusted
incidence rates;I
barsrepresent the corresponding 95 percent confidence intervals
(CIs). The oddsratios, 95 percent CIs for the odds ratios, and P
values have been adjusted forsex, age, and body-mass index at the
time of inclusion in the intervention study.
60
I n c i
d e n c e
( % o f s u
b j e c
t s )
40
30
10
50
20
0
Hypertriglyceridemia Low HDL Cholesterol
Hypercholesterolemia
No. of subjectsControlSurgery
Odds ratio95% CIP value
2 Yr 10 Yr
1881351.16
0.691.950.57
5965041.27
0.951.690.11
2 Yr 10 Yr
4404310.57
0.291.150.12
117412930.21
0.140.32
-
8/12/2019 Lifestyle,DM,CVD Risk Factors
10/11
n engl j med 351;26
w ww.n ej m. org d ec em b er 23
, 2004
The
new england journal of
medicine
2692
servations concerning the effects of weight loss onblood
pressure,
8,32,33
lipids,
9,34,35
uric acid,
36
anddiabetes.
5-7
In contrast, to our knowledge there havebeen no controlled,
prospective intervention trialsagainst which our long-term results
can be com-pared. In a retrospective, nine-year analysis,
gastric
bypass surgery was found to have a dramatic effect on the
incidence of type 2 diabetes and overall mor-tality.
37
Sixteen-year observational data on weight loss from the
Framingham Study
38
are in agreement with the primary preventive effect on diabetes
that we found over a 10-year period. In contrast, observa-tional,
epidemiologic 12-to-15-year data on weight loss indicated a primary
preventive effect on hyper-tension in the Nurses Health Study,
39
but this find-ing could not be confirmed in our controlled
10-yearintervention. Our results indicate that the long-termeffects
(effects at 10 years) of maintained weight loss on risk factors
cannot always be estimated from
short-term observations (up to 2 years).The main limitation of
the SOS Study is that it
was not randomized. When it was approved as amatched,
prospective intervention study in 1987, sixof the seven involved
ethics review boards in Swe-den considered the high mortality rate
after gastricsurgery for obesity (1 to 5 percent in the 1970s
and1980s
40
) unacceptable for randomization.In summary, this study
indicates that bariatric
surgery is a favorable option in the treatment of se- vere
obesity. That not all obesity-associated risk fac-tors were
improved by sustained weight loss under-scores the importance of
obtaining long-term dataconcerning the effect of weight loss on
overall mor-tality and on the incidence rates of myocardial
in-farction, stroke, and cancer.
Supported by a grant (05239) from the Swedish Medical
ResearchCouncil and by grants from HoffmannLa Roche, Basel,
Switzer-land (to Dr. Sjstrm), and Bristol-Myers Squibb (to Dr.
Bouchard).
Dr. Carlsson reports holding equity in AstraZeneca.We are
indebted to the staff members at the 480 primary health
care centers and 25 surgical departments that participated in
thestudy.
append ix
The SOS Study Scientific Group consists of L. Sjstrm (chair), L.
Backman, C. Bengtsson, C. Bouchard, B. Carlsson, L. Carlsson, S.
Dahl-gren, P. Jacobsson, E. Jonsson, K. Karason, J. Karlsson, B.
Larsson, A.-K. Lindroos, L. Lnn, H. Lnnroth, K. Narbro, I. Nslund,
M. Pel-tonen, A. Rydn, C.D. Sjstrm, K. Stenlf, M. Sullivan, C.
Taft, J. Torgerson, and H. Wedel.
r e f e r ences
1.
Sjstrm LV. Mortality of severely obesesubjects. Am J Clin Nutr
1992;55:Suppl:516S-523S.
2.
Mokdad AH, Ford ES, Bowman BA, et al. Prevalence of obesity,
diabetes, and obe-sity-related health risk factors, 2001.
JAMA2003;289:76-9.
3.
Ford ES, Giles WH, Dietz WH. Preva-lence of the metabolic
syndrome among USadults: findings from the Third NationalHealth and
Nutrition Examination Survey. JAMA 2002;287:356-9.
4.
Bjrntorp P, De Jounge K, Sjstrm L,Sullivan L. The effect of
physical training on
insulin production in obesity. Metabolism1970;19:631-8.
5.
Knowler WC, Barrett-Connor E, FowlerSE, et al. Reduction in the
incidence of type 2diabetes with lifestyle intervention or
met-formin. N Engl J Med 2002;346:393-403.
6.
Tuomilehto J, Lindstrm J, Eriksson JG,
Figure 4. Recovery from Diabetes, Lipid Disturbances,
Hypertension,and Hyperuricemia over 2 and 10 Years in Surgically
Treated Subjectsand Their Obese Controls.
Data are for subjects who completed 2 years and 10 years of the
study. Thebars and the values above the bars indicate unadjusted
rates of recovery;I barsrepresent the corresponding 95 percent
confidence intervals (CIs). The oddsratios, 95 percent CIs for the
odds ratios, and P values have been adjusted forsex, age, and
body-mass index at the time of inclusion in the intervention
study.
100
R a t e o f
R e c o v e r y
( % o f s u
b j e c
t s )
60
40
80
20
0
No. of subjectsControlSurgery
Odds ratio95% CIP value
2 yr 10 yr
4354981.30
0.921.830.14
104813271.22
0.981.510.07
2 yr 10 yr
1661692.35
1.443.840.001
3964455.28
3.857.23
-
8/12/2019 Lifestyle,DM,CVD Risk Factors
11/11
n engl j med 351;26 w ww.n ej m. org d ec em b er 23, 2004
long-term weight loss and changes in cardiovascular risk
factors
2693
et al. Prevention of type 2 diabetes mellitusby changes in
lifestyle among subjects withimpaired glucose tolerance. N Engl J
Med2001;344:1343-50.7. Torgerson JS, Hauptman J, Boldrin
MN,Sjostrom L. XENical in the prevention of di-abetes in obese
subjects (XENDOS) study:a randomized study of orlistat as an ad-
junct to lifestyle changes for the preventionof type 2 diabetes in
obese patients. Diabe-tes Care 2004;27:155-61. [Erratum, Diabe-tes
Care 2004;27:856.]8. Stevens VJ, Obarzanek E, Cook NR, et al.
Long-term weight loss and changes inblood pressure: results of the
Trials of Hy-pertension Prevention, phase II. Ann InternMed
2001;134:1-11.9. Wood PD, Stefanick ML, Dreon DM, et al. Changes in
plasma lipids and lipopro-teins in overweight men during weight
lossthrough dieting as compared with exercise.N Engl J Med
1988;319:1173-9.10. Sjstrm CD, Lissner L, Sjstrm L. Re-lationships
between changes in body com-position and changes in cardiovascular
risk factors: the SOS Intervention Study. ObesRes 1997;5:519-30.11.
Sjstrm CD, Lissner L, Wedel H,Sjstrm L. Reduction in incidence of
diabe-tes, hypertension and lipid disturbances af-ter intentional
weight loss induced by bari-atric surgery: the SOS Intervention
Study.Obes Res 1999;7:477-84.12. Saudicani P, Hein HO, Gyntelberg
F.Weight changes and risk of ischemic heart disease for middle aged
and elderly men: an8-year follow-up in the Copenhagen MaleStudy. J
Cardiovasc Risk 1997;4:25-32.13. Sidney S, Friedman GD, Siegelaub
AB.Thinness and mortality. Am J Public Health1987;77:317-22.14.
Higgins M, DAgostino R, Kannel W,Cobb J, Pinsky J. Benefits and
adverse effectsof weight loss: observations from the Fra-mingham
Study. Ann Intern Med 1993;119:758-63. [Erratum, Ann Intern Med
1993;119:1055.]15. Cornoni-Huntley JC, Harris TB, Everett DF, et
al. An overview of body weight of olderpersons, including the
impact on mortality:the National Health and Nutrition Examina-tion
Survey I Epidemiologic Follow-upStudy. J Clin Epidemiol
1991;44:743-53.16. Pamuk ER, Williamson DF, Madans J,Serdula MK,
Kleinman JC, Byers T. Weight
loss and mortality in a national cohort of adults, 1971-1987. Am
J Epidemiol 1992;136:686-97.17. Pamuk ER, Williamson DF, Serdula
MK,Madans J, Byers TE. Weight loss and subse-quent death in a
cohort of U.S. adults. AnnIntern Med 1993;119:744-8.18. Sjstrm L,
Larsson B, Backman L, et al.Swedish Obese Subjects (SOS):
recruitment for an intervention study and a selected de-scription
of the obese state. Int J Obes Relat Metab Disord
1992;16:465-79.19. Pocock SJ, Simon R. Sequential treat-ment
assignment with balancing for prog-nostic factors in the controlled
clinical trial.Biometrics 1975;31:103-15.20. Lindroos AK, Lissner
L, Sjstrm L. Va-lidity and reproducibility of a self-adminis-tered
dietary questionnaire in obese andnon-obese subjects. Eur J Clin
Nutr 1993;47:461-81.21. Lindroos AK, Lissner L, Sjstrm L.Does
degree of obesity influence the validity of reported energy and
protein intake? Re-sults from the SOS Dietary Questionnaire.Eur J
Clin Nutr 1999;53:375-8.22. Larsson I, Lissner L, Nslund I,
LindroosAK. Leisure and occupational physical activi-ty in relation
to body mass index in men and women. Scand J Nutr
2004;48:165-72.23. Sjstrm L. Surgical intervention as astrategy for
treatment of obesity. Endocrine2000;13:213-30.24. Report of the
Expert Committee on theDiagnosis and Classification of
DiabetesMellitus. Diabetes Care 2003;26:Suppl 1:S5-S24.25. 1999
World Health OrganizationInternational Society of Hypertension
Guide-lines for the Management of Hypertension:Guidelines
Subcommittee. J Hypertens 1999;19:151-83.26. Expert Panel on
Detection, Evaluation,and Treatment of High Blood Cholesterol
inAdults. Executive Summary of The Third Re-port of The National
Cholesterol EducationProgram (NCEP) Expert Panel on
Detection,Evaluation, and Treatment of High BloodCholesterol in
Adults (Adult Treatment Pan-el III). JAMA 2001;285:2486-97.27.
Tunis SR, Stryer DB, Clancy CM. In-creasing the value of clinical
research for de-cision making in clinical and health policy. JAMA
2003;290:1624-32.28. Ware JH. Interpreting incomplete data
in studies of diet and weight loss. N Engl J Med
2003;348:2136-7.29. Stata statistical software: release 7.0.College
Station, Tex.: Stata, 2001.30. Cummings DE, Weigle DS, Frayo RS, et
al. Plasma ghrelin levels after diet-induced weight loss or gastric
bypass surgery. N Engl J Med 2002;346:1623-30.31. Fruhbeck G, Diez
Caballero A, Gil MJ.Fundus functionality and ghrelin
concentra-tions after bariatric surgery. N Engl J
Med2004;350:308-9.32. Foley EF, Benotti PN, Borlase BC,
Hol-lingshead J, Blackburn GL. Impact of gastricrestrictive surgery
on hypertension in themorbidly obese. Am J Surg 1992;163:294-7.33.
Carson JL, Ruddy ME, Duff AE, HolmesNJ, Cody RP, Brolin RE. The
effect of gastricbypass surgery on hypertension in morbidly obese
patients. Arch Intern Med 1994;154:193-200. [Erratum, Arch Intern
Med 1994;154:1770.]34. Dattilo AM, Kris-Etherton PM. Effectsof
weight reduction on blood lipids andlipoproteins: a meta-analysis.
Am J ClinNutr 1992;56:320-8.35. Wadden TA, Anderson DA, Foster
GD.Two-year changes in lipids and lipoproteinsassociated with the
maintenance of a 5% to10% reduction in initial weight: some
find-ings and some questions. Obes Res 1999;7:170-8.36. Nakanishi
N, Nakamura K, Suzuki K,Matsuo Y, Tatara K. Relation of body weight
change to changes in atherogenic traits:a study of middle-aged
Japanese obese maleoffice workers. Ind Health 2000;38:233-8.37.
MacDonald KG Jr, Long SD, SwansonMS, et al. The gastric bypass
operation re-duces the progression and mortality of
non-insulin-dependent diabetes mellitus. J Gas-trointest Surg
1997;1:213-20.38. Moore LL, Visioni AJ, Wilson PW, DAg-ostino RB,
Finkle WD, Ellison RC. Can sus-tained weight loss in overweight
individualsreduce the risk of diabetes mellitus? Epide-miology
2000;11:269-73.39. Huang Z, Willett WC, Manson JE, et al.Body
weight, weight change, and risk forhypertension in women. Ann
Intern Med1998;128:81-8.40. Brolin RE. Results of obesity
surgery.Gastroenterol Clin North Am 1987;16:317-38.Copyright 2004
Massachusetts Medical Society.
journal index
The index to volume 351 of the Journal will be available on
February 17, 2005. Atthat time, it can be downloaded free in PDF
format from www.nejm.org or canbe ordered in a printed and bound
format. To order a bound copy, please call1-800-217-7874 from the
United States and Canada (call 651-582-3800 from othercountries) or
e-mail [email protected].
Downloaded from www nejm org on May 23 2005 This article is
being provided free of charge for use in Indonesia