Embed Size (px)
Citation preview
Dr A P Naveen KumarChief Specialist
VSGH
38 maleRecently detected T2DMBP 140/94Lipids 206 / 174 /32 /123Smoker , no exercise
52 female Obese Newly detected T2DM Family h/o premature CAD Known HTN on treatment Lipids 212 / 376 / 32 / 96
56 female T2DM 15 yrs.Obese and HTNBP 130/82Lipids 168/178/36/94FBS 96 PPBS 156 Sr. Crea. 0.9ECG - LVHRetinopathy ,neuropathy +H/O TIAOn OHA ,ACEI ,Aspirin ,Statin
A majority of patients with T2DM either die from or acquire serious manifestations of CV disease.
The risk of a patient with T2DM suffering a major adverse cardioarvascular event (MACE) of either myocardial infarction (MI), stroke, or heart failure (HF) and subsequent CV death is more than double that of a person without T2DM

Beneficial effect of blood glucose lowering on macrovascular events (ie, MACE) is very limited
UKPDS - followed for up to 20 years, a significant effect on CV mortality emerged
ACCORD, ADVANCE, and VADT trials failed to show sig. benefits on lowering the incidence of macrovascular events.
Lifestyle changes (diet, exercise, not smoking) and controlling dyslipidemia and high blood pressure, with the use of statins and antihypertensive medications respectively, are thought to be proportionately more important than glycemic control in reducing MACE events in patients with T2DM
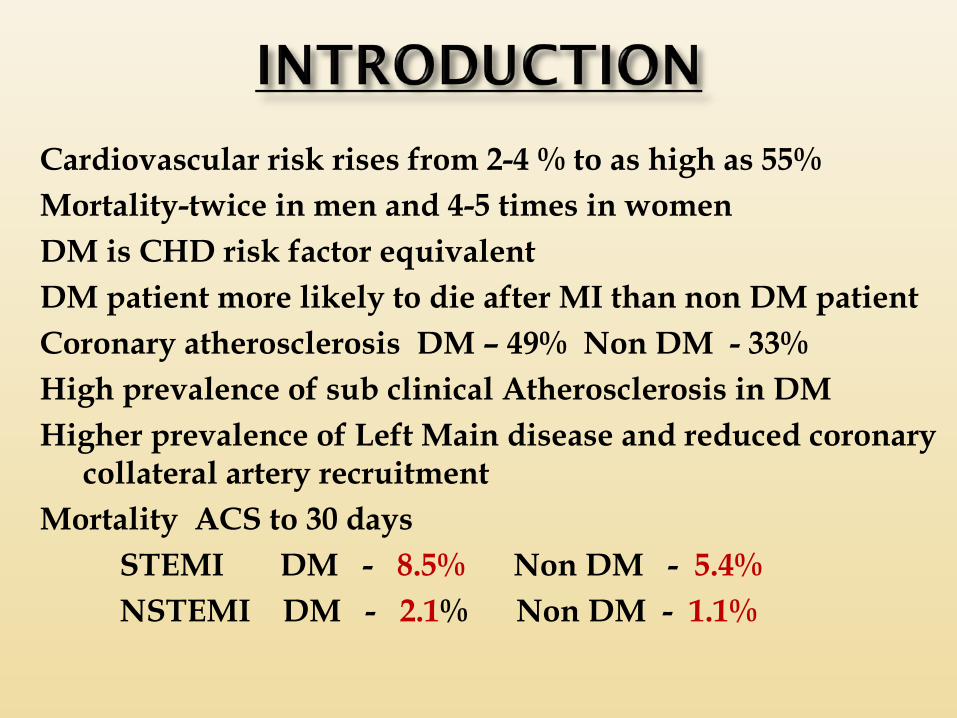
Cardiovascular risk rises from 2-4 % to as high as 55%Mortality-twice in men and 4-5 times in womenDM is CHD risk factor equivalentDM patient more likely to die after MI than non DM patientCoronary atherosclerosis DM – 49% Non DM - 33%High prevalence of sub clinical Atherosclerosis in DMHigher prevalence of Left Main disease and reduced coronary
collateral artery recruitmentMortality ACS to 30 days STEMI DM - 8.5% Non DM - 5.4% NSTEMI DM - 2.1% Non DM - 1.1%
CVD is increased two- to threefold in patients with DM
In a meta-analysis involving 447,064 patients, the rate of fatal coronary heart disease in patients with DM was reported to be 5.4% versus 1.6% in nondiabetic subjects.
Diabetic females had a significantly higher relative fatal cardiovascular risk than males
The factors responsible for DM being a CVD risk factor are insulin resistance, HTN, lipid abnormalities, endothelial dysfunction, inflammation, and procoagulant factors.
Screening and diagnosis
Blood pressure should be measured at every routine visit B
Patients found to have elevated blood pressure should have blood pressure confirmed on a separate day B
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S49
Goals People with diabetes and hypertension should be treated to a
systolic blood pressure goal of <140 mmHg A
Lower systolic targets, such as <130 mmHg, may be appropriate for certain individuals, such as younger patients, if it can be achieved without undue treatment burden C
Patients with diabetes should be treated to a diastolic blood pressure <90 mmHg A
Lower diastolic targets, such as <80 mmHg, may be appropriate for certain individuals, such as younger patients, if it can be achieved without undue treatment burden B
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S49

Treatment (2)
Lifestyle therapy for elevated blood pressure B
Weight loss if overweight DASH-style dietary pattern including reducing
sodium, increasing potassium intake Moderation of alcohol intake Increased physical activity
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S49
Action to Control Cardiovascular Risk in Diabetes (ACCORD):
Does SBP <120 provide better cardiovascular protection than SBP 130-140? No.
ADVANCE-BP: Significant risk reduction
American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2016; 39 (Suppl. 1): S60-S71
Treatment (3)
Pharmacological therapy for patients with diabetes and hypertension comprise a regimen that includes
either an ACE inhibitor or angiotensin II receptor blocker Bif one class is not tolerated, substitute the other C
Multiple drug therapy (two or more agents at maximal doses) generally required to achieve blood pressure targets B
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S50
Treatment (4)
If ACE inhibitors, ARBs, or diuretics are used, serum creatinine/eGFR and potassium levels should be monitored E
In pregnant patients with diabetes and chronic hypertension, blood pressure target goals of 110–129/65–79 mmHg are suggested in interest of long-term maternal health and minimizing impaired fetal growth;
ACE inhibitors, ARBs, contraindicated during pregnancy E
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S50
Screening
In adults, a screening lipid profile is reasonable E
At first diagnosis
At the initial medical evaluation
And/or at age 40 years and periodically (e.g., every 1-2 years) thereafter
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S51
Treatment recommendations and goals
To improve lipid profile in patients with diabetes, recommend lifestyle modification A, focusing on
Reduction of saturated fat, trans fat, cholesterol intakeIncrease of n-3 fatty acids, viscous fiber,plant stanols/sterolsWeight loss (if indicated)Increased physical activity
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S51
Treatment recommendations and goals
Intensify lifestyle therapy and optimize glycemic control for patients with C
Triglyceride levels >150 mg/Dl (1.7 mmol/L) and/or HDL cholesterol <40 mg/dL (1.0 mmol/L) in men and <50 mg/dL (1.3 mmol/L) in women
For patients with fasting triglyceride levels > 500 mg/dL (5.7 mmol/L), evaluate for secondary causes and consider medical therapy to reduce the risk of pancreatitis C
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S52
Treatment recommendations and goals
In clinical practice, providers may need to adjust intensity of statin therapy based on individual patient response to medication (e.g. side effects, tolerability, LDL cholesterol levels.) E
Cholesterol laboratory testing may be helpful in monitoring adherence to therapy but may not be needed once the patient is stable on therapy E
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S52
Treatment recommendations and goals
Combination therapy has been shown not to provide additional cardiovascular benefit above statin therapy alone and is not generally recommended A
Statin therapy is contraindicated in pregnancy B
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S52
Consider aspirin therapy (75–162 mg/day) C
As a primary prevention strategy in those with type 1 or type 2 diabetes at increased cardiovascular risk (10-year risk >10%)
Includes most men >50 years of age or women >60 years of age who have at least one additional major risk factor
Family history of CVD Hypertension Smoking Dyslipidemia Albuminuria
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S54
Aspirin should not be recommended for CVD prevention for adults with diabetes at low CVD risk, since potential adverse effects from bleeding likely offset potential benefits C
Low risk: 10-year CVD risk <5%, such as in men <50 years, women <60 years with no major additional CVD risk factors
• In patients in these age groups with multiple other risk factors (10-year risk 5–10%), clinical judgment is
required E
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S54
Use aspirin therapy (75–162 mg/day) Secondary prevention strategy in those with
diabetes with a history of CVD A
For patients with CVD and documented aspirin allergy Clopidogrel (75 mg/day) should be used B
Dual antiplatelet therapy is reasonable for up to a year after an acute coronary syndrome B
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S54
Screening
In asymptomatic patients, routine screening for CAD is not recommended because it does not improve outcomes as long as CVD risk factors are treated A
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S55
Treatment :
To reduce risk of cardiovascular events in patients with known CVD, consider
ACE inhibitor CAspirin* AStatin therapy* A
In patients with a prior MIβ-blockers should be continued for at least
2 years after the event B
*If not contraindicated.
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S55
Treatment
In patients with symptomatic heart failure, thiazolidinedione treatment should not be used A
In patients with stable CHF, metformin BMay be used if renal function is normalShould be avoided in unstable or hospitalized
patients with CHF
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S55
: The 2014, ACC/AHA guidelines strongly advocate use of statins for primary and secondary prevention in all patients with diabetes.
The expert panel observed that there was no strong evidence to set any LDL and non-HDL goals for such patients.
The patients should not be evaluated for cardiovascular risk and diabetes alone is sufficient justification for use of moderate to high intensity statins.
These guidelines are more patient specific and focused than ACC/AHA guidelines and suggest the following:
• For patients with diabetes aged < 40 years with additional CV risk factors, consider using moderate or high intensity statin with lifestyle therapy.
• For patients with diabetes aged 40–75 without CV risk factor consider moderate intensity statin with lifestyle therapy.
CARDS trial showed CV event reduction by 38%
• For patients with diabetes aged 40–75 with additional CV risk factor consider high intensity statin with lifestyle therapy.
• For patients with diabetes > 75 years of age without
CV risk factor consider mod. intensity statin with lifestyle therapy.
• For patients with diabetes > 75 years of age with additional CV risk factor consider moderate or high intensity statin with lifestyle therapy.
• Combination therapy of statin+ fibrates or statin + niacin has not been shown to have any additional cardiovascular benefits over and above statins alone and generally not recommended.
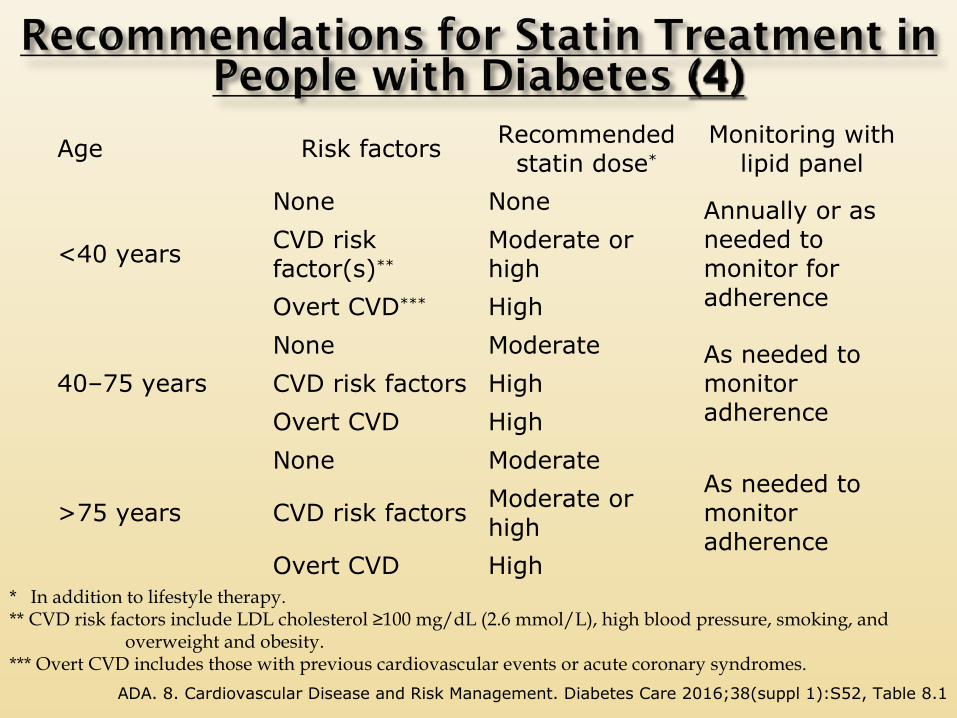
Age Risk factors Recommended statin dose*
Monitoring with lipid panel
<40 years
None None Annually or as needed to monitor for adherence
CVD risk factor(s)**
Moderate or high
Overt CVD*** High
40–75 years
None Moderate As needed to monitor adherence
CVD risk factors High
Overt CVD High
>75 years
None ModerateAs needed to monitor adherence
CVD risk factors Moderate or high
Overt CVD High* In addition to lifestyle therapy. ** CVD risk factors include LDL cholesterol ≥100 mg/dL (2.6 mmol/L), high blood pressure, smoking, and overweight and obesity. *** Overt CVD includes those with previous cardiovascular events or acute coronary syndromes.
ADA. 8. Cardiovascular Disease and Risk Management. Diabetes Care 2016;38(suppl 1):S52, Table 8.1
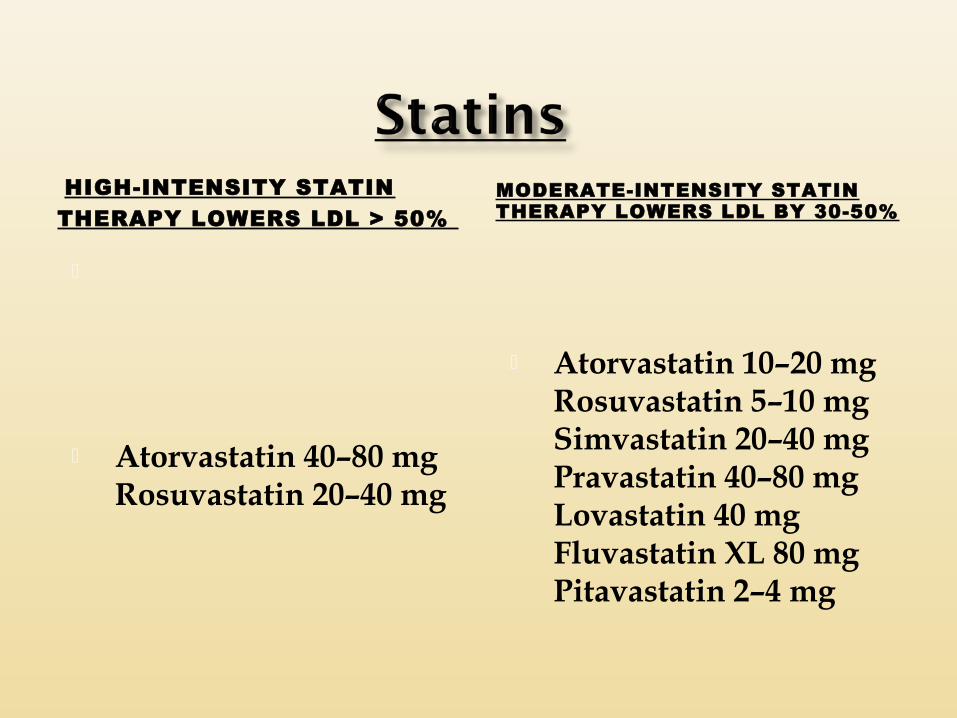
HIGH-INTENSITY STATIN THERAPY LOWERS LDL > 50%
Atorvastatin 40–80 mg Rosuvastatin 20–40 mg
MODERATE-INTENSITY STATIN THERAPY LOWERS LDL BY 30-50%
Atorvastatin 10–20 mg Rosuvastatin 5–10 mg Simvastatin 20–40 mg Pravastatin 40–80 mg Lovastatin 40 mg Fluvastatin XL 80 mg Pitavastatin 2–4 mg
The non–HDL-C level is the number of circulating atherogenic particles (chylomicrons ,LDL,Lp –a,IDL,VLDL and their remnants)
It is a more precise therapeutic target than LDL-C when the triglyceride level is above 200 mg/Dl.
Reaching ideal goals for non–HDL-C, especially in persons with diabetes, is one of the most significant means of reducing cardiovascular events.
LDL goal is achieved with optimal statin therapy, non-statin agent may be considered for uncontrolled non-HDL cholesterol level
Non HDL
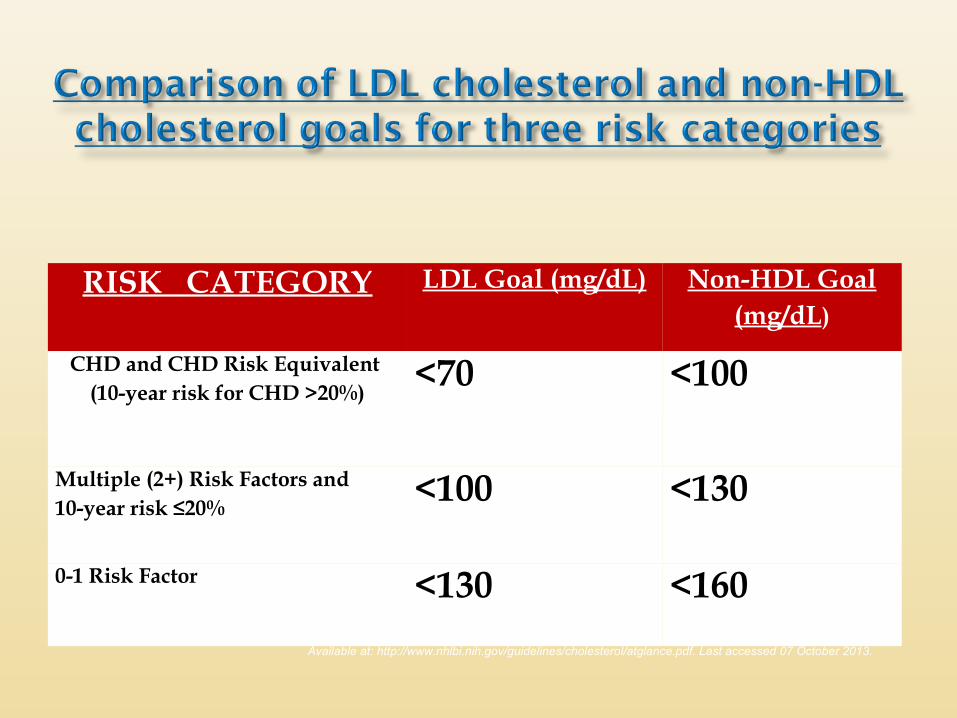
RISK CATEGORY LDL Goal (mg/dL) Non-HDL Goal (mg/dL)
CHD and CHD Risk Equivalent (10-year risk for CHD >20%)
<70 <100
Multiple (2+) Risk Factors and10-year risk ≤20%
<100 <130
0-1 Risk Factor <130 <160
Available at: http://www.nhlbi.nih.gov/guidelines/cholesterol/atglance.pdf. Last accessed 07 October 2013.
In conclusion, among statin-treated patients, levels of LDL-C, and non–HDL-C, was strongly associated with the risk of major cardiovascular events
Non–HDL-C was more strongly associated than LDL-C.
Non–HDL-C may be a more appropriate target for statin therapy than LDL-C.
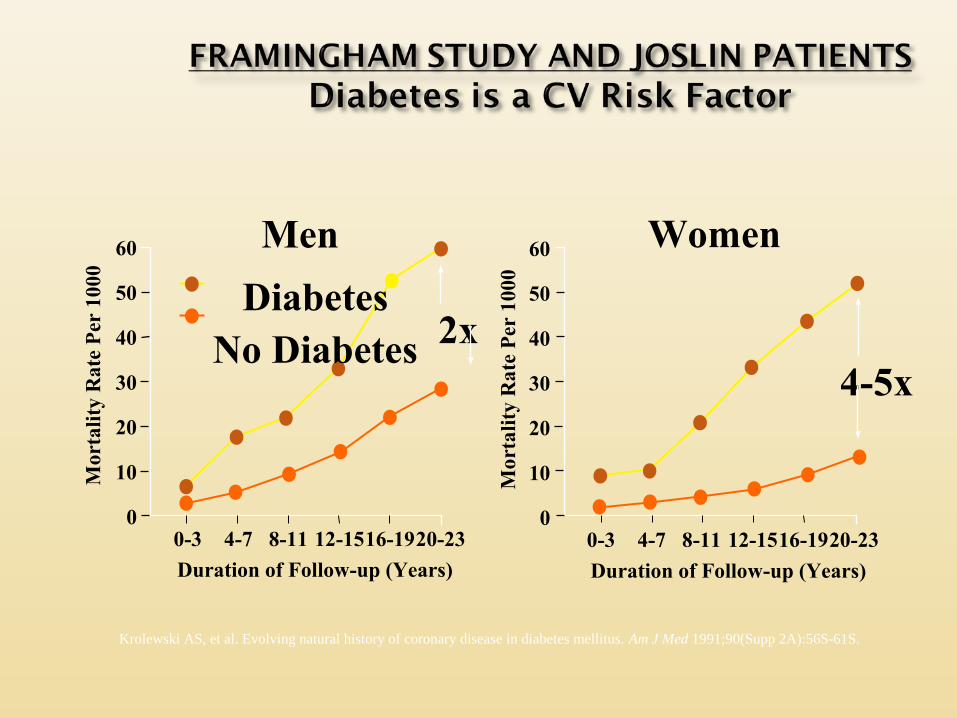
Krolewski AS, et al. Evolving natural history of coronary disease in diabetes mellitus. Am J Med 1991;90(Supp 2A):56S-61S.
DiabetesNo Diabetes
60 Men
0-3
Duration of Follow-up (Years)
50
40
30
20
10
0
Women
4-7 8-11 12-1516-1920-23
60
0-3
Duration of Follow-up (Years)
50
40
30
20
10
04-7 8-11 12-1516-1920-23
Mor
tali
ty R
ate
Per
100
0
Mor
talit
y R
ate
Per
100
0
2x4-5x
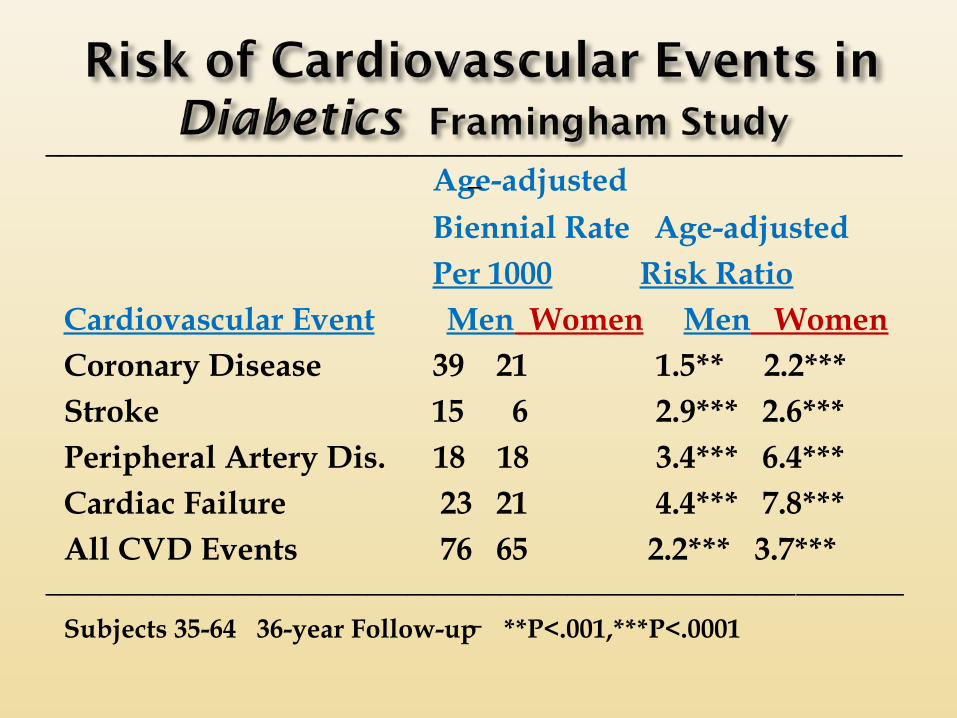
Age-adjusted Biennial Rate Age-adjusted
Per 1000 Risk RatioCardiovascular Event Men Women Men WomenCoronary Disease 39 21 1.5** 2.2***Stroke 15 6 2.9*** 2.6***Peripheral Artery Dis. 18 18 3.4*** 6.4***Cardiac Failure 23 21 4.4*** 7.8***All CVD Events 76 65 2.2*** 3.7***
Subjects 35-64 36-year Follow-up **P<.001,***P<.0001
_________________________________________________________________
_________________________________________________________________
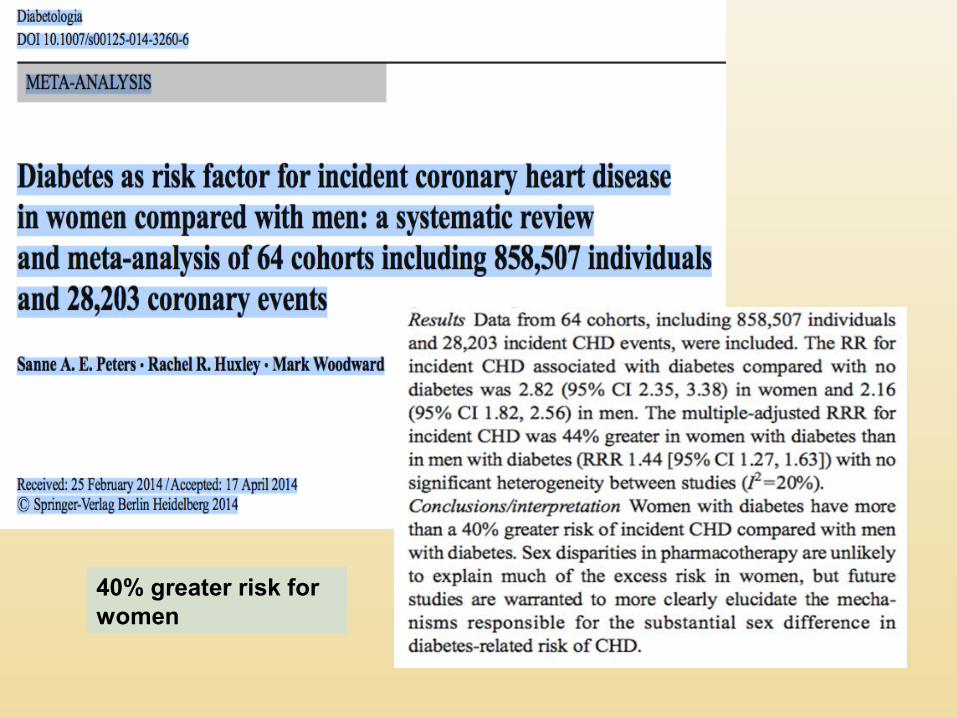
40% greater risk for women
Inherent biological risk [ hormonal]
CV risk factors like obesity, visceral adiposity, hypertension, prediabetes , dyslipidemia
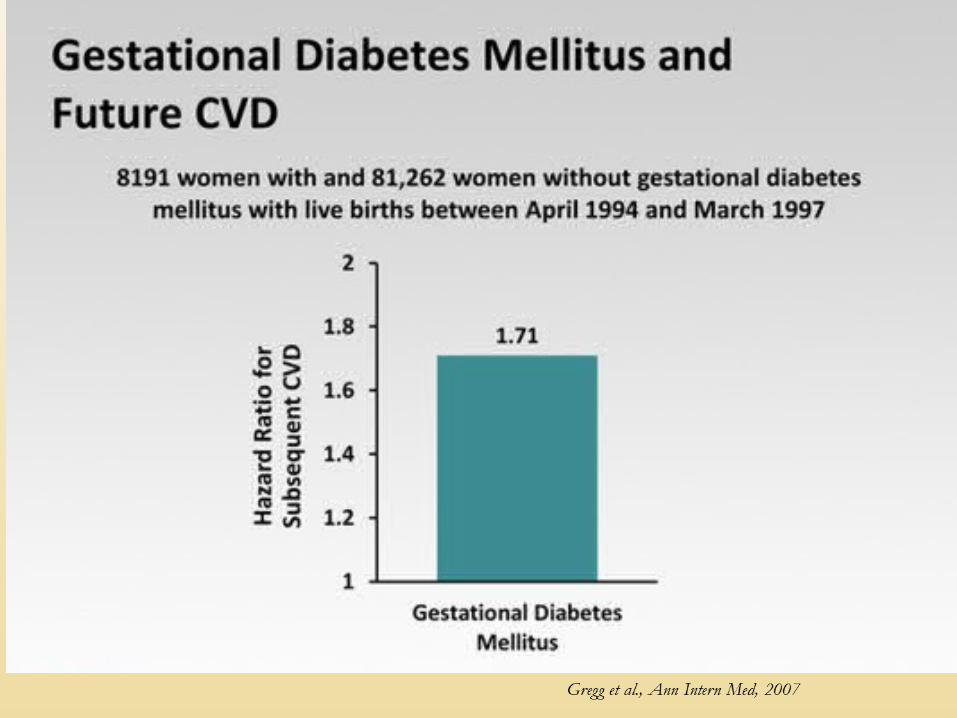
GDM
Varied clinical presentation
Aggressive screening for prediabetes among women
Awareness of excess CV risk even among IFG or IGT category among women, with need for aggressive monitoring and control - ? Impact on CV risk
45
38% of women experiencing a heart attack will die within one year compared to 25% of men.
35% of women heart attack survivors will have another heart attack compared to 18% of men.
Women are almost twice as likely as men to die after bypass surgery.
Consider aspirin therapy (75–162 mg/day) As a primary prevention strategy in
those with type 1 or type 2 diabetes at increased cardiovascular risk (10-year risk >10%)
women >60 years of age who have at least one additional major risk factor Family history of CVD Hypertension Smoking Dyslipidemia Albuminuria
For patients with CVD and documented aspirin allergy Clopidogrel (75 mg/day) should be used
ADA. VI. Prevention, Management of Complications. Diabetes Care 2014;37(suppl 1):S40
Women with diabetes ARE at high risk of CVD and strokeAge, menopausal status not protectiveScreen all women with diabetes for CV risk factors and
treat aggressively Use internationally accepted targets
A1C <7.0%*
Blood pressure <140/80 mmHg†
Lipids: LDL cholesterol
<100 mg/dL (<2.6 mmol/L)‡
Statin therapy for those with history of MI or age >40+ or other risk factors
Women with diabetes are at very high for CVD and Cer.VD
Aggressive search for risk factors and risk stratification is necessary
Targets are the same as for men
Presenting symptoms may be different
Avoid medications that can increase CHF/ Ischemia/ weight/ hypoglycemia
Depression, dental health, obstructive sleep apnea linked to CVD
Advise all patients not to smoke or use tobacco products
Include smoking cessation counseling and other forms of treatment as a routine component of diabetes care
ADA. VI. Prevention, Management of Complications. Diabetes Care 2014;37(suppl 1):S41
STENO-2
STENO-2
The Steno-2 study was designed in 1990
There was no evidence base for the treatment of type 2 diabetes
Some diabetes educators were suffering from therapeutic nihilism
Intervention studies including the UKPDS were ongoing
STENO-2
An attempt to validate the efficacy of daily clinical practice, i.e. the
multifactorial treatment of type 2 diabetes
High risk type 2 diabetes patients
A single center study
An organisation which allowed for intensive intervention
Longterm intervention
STENO-2
To investigate the impact on microvascular and cardiovascular disorders of a target driven behaviour modification and polypharmacy
as compared to a conventional multifactorial treatment of
high-risk type 2 diabetic patients with the metabolic syndrome including microalbuminuria
STENO-2
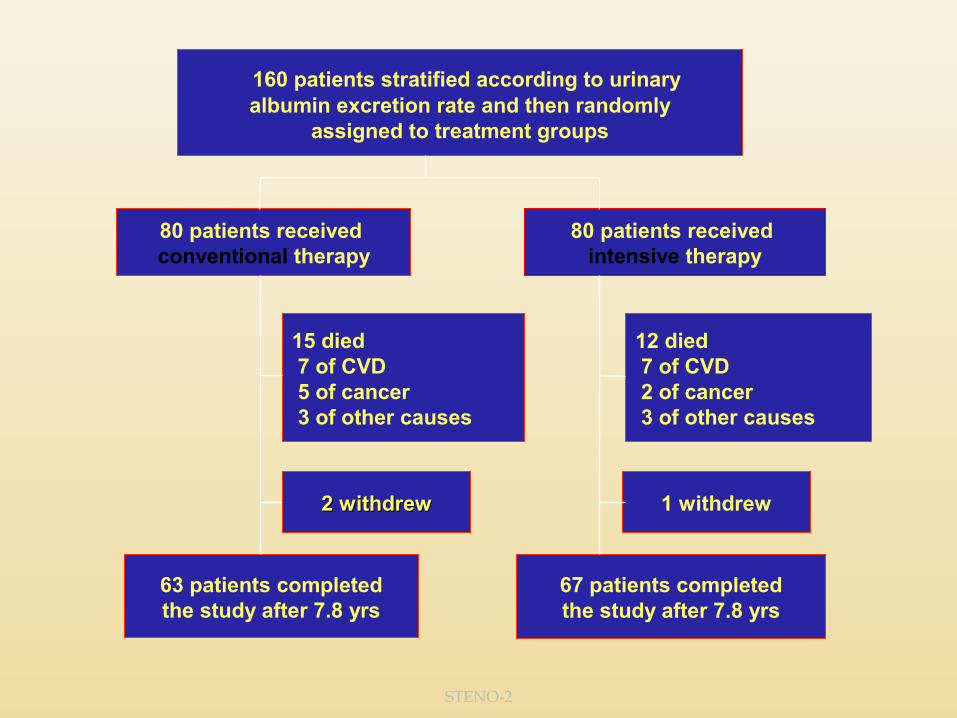
160 patients stratified according to urinaryalbumin excretion rate and then randomly
assigned to treatment groups
80 patients received conventional therapy
80 patients received intensive therapy
15 died 7 of CVD 5 of cancer 3 of other causes
12 died 7 of CVD 2 of cancer 3 of other causes
2 withdrew2 withdrew 1 withdrew
63 patients completed the study after 7.8 yrs
67 patients completedthe study after 7.8 yrs
STENO-2
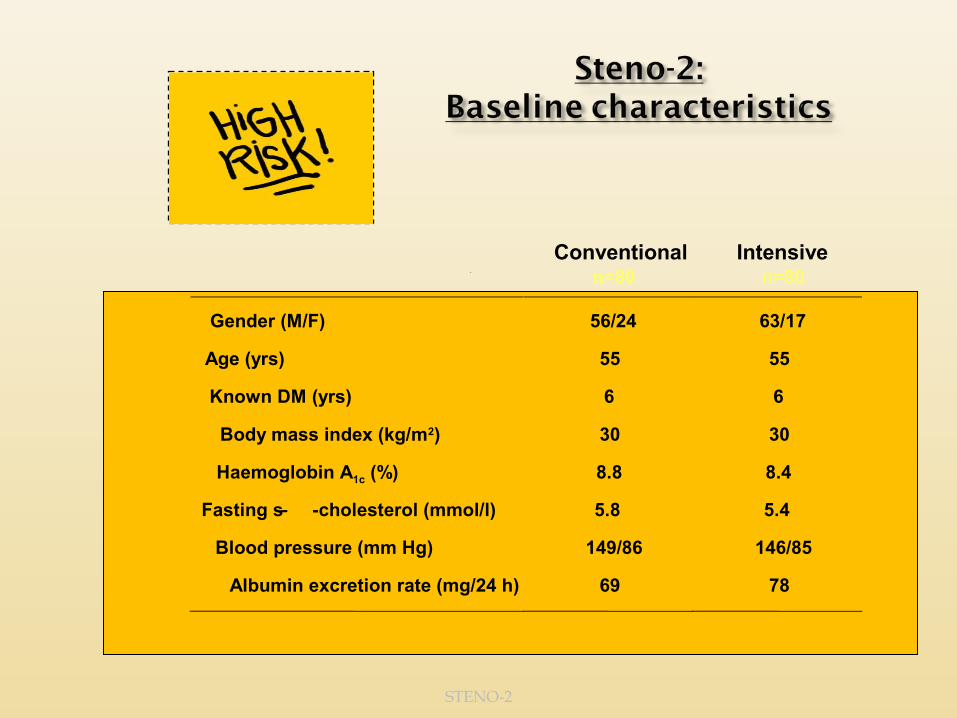
Conventional n=80
Intensive n=80
Gender (M/F) 56/24 63/17
Age (yrs) 55 55
Known DM (yrs) 6 6
Body mass index (kg/m2) 30 30
Haemoglobin A1c (%) 8.8 8.4
Fasting s- -cholesterol (mmol/l) 5.8 5.4
Blood pressure (mm Hg) 149/86 146/85
Albumin excretion rate (mg/24 h) 69 78
STENO-2
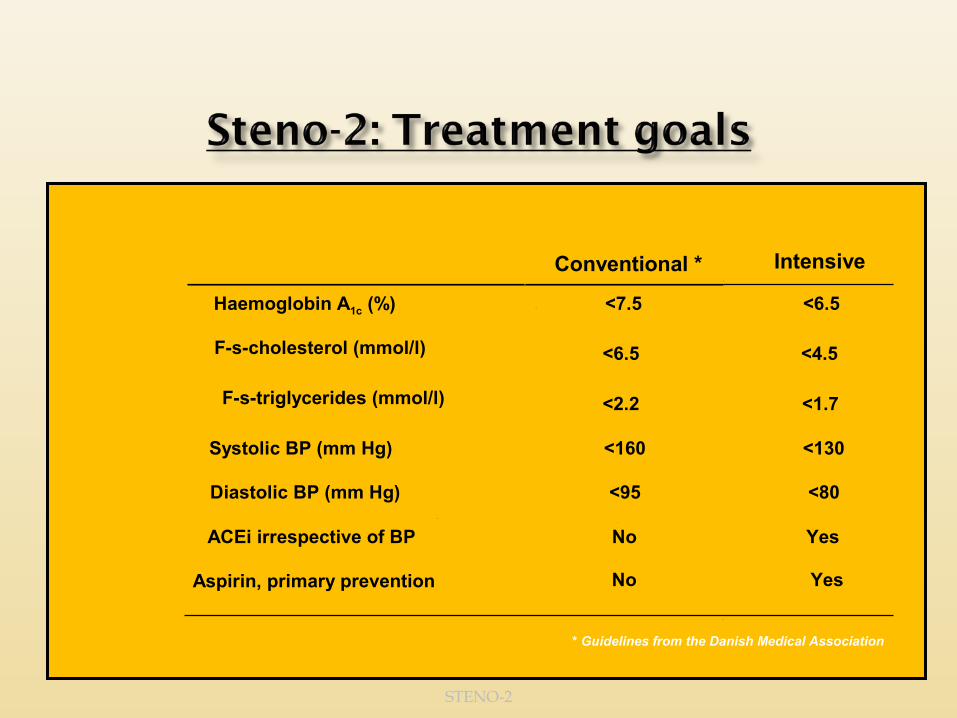
Conventional * Intensive
Haemoglobin A1c (%) <7.5 <6.5
F-s-cholesterol (mmol/l) <6.5 <4.5
F-s-triglycerides (mmol/l) <2.2 <1.7
Systolic BP (mm Hg) <160 <130
Diastolic BP (mm Hg) <95 <80
ACEi irrespective of BP No Yes
Aspirin, primary prevention No
Yes
* Guidelines from the Danish Medical Association

STENO-2
Patients and spouses were motivated to join smoking cessation courses
Nicotine substitutes were given for free
STENO-2
Have some kind of seafood every day
Cut down on animal fat
STENO-2
5-6 servings of vegetables and fruits/day
STENO-2
Enjoy physical performance more than 150 min/week
STENO-2
ACE inhibitor/Angiotensin II antagonist
Diuretics
Calcium antagonist
ß-blocker
OtherSeverity of hypertension
Stepwise approach Stepwise approach to the treatment of to the treatment of
hypertension hypertension
STENO-2
Primary: Cardiovascular diseasePrimary: Cardiovascular disease• Cardiovascular mortality• Non-fatal myocardial infarction• Coronary artery bypass graft• Non-fatal stroke• Revascularization• Amputation Secondary: Microvascular diseaseSecondary: Microvascular disease• Progression to nephropathy• Development of/progression in retinopathy• Development of/progression in neuropathy

STENO-2
PCI or CABG
Vascular surgery Amputation
StrokeCVD deathMyocardial infarction
Number of eventsNumber of events
Intensive Conventional
STENO-2
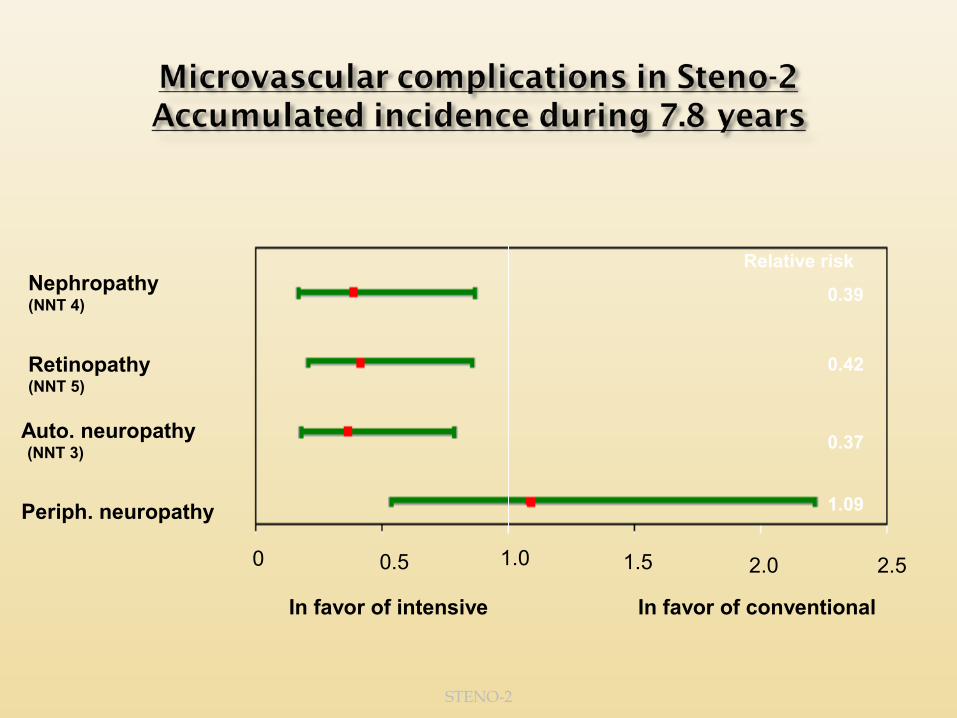
0.50 2.52.01.51.0
Nephropathy(NNT 4)
Retinopathy(NNT 5)
Auto. neuropathy (NNT 3)
Periph. neuropathy
Relative risk
0.39
0.42
0.37
1.09
In favor of intensive In favor of conventional
STENO-2
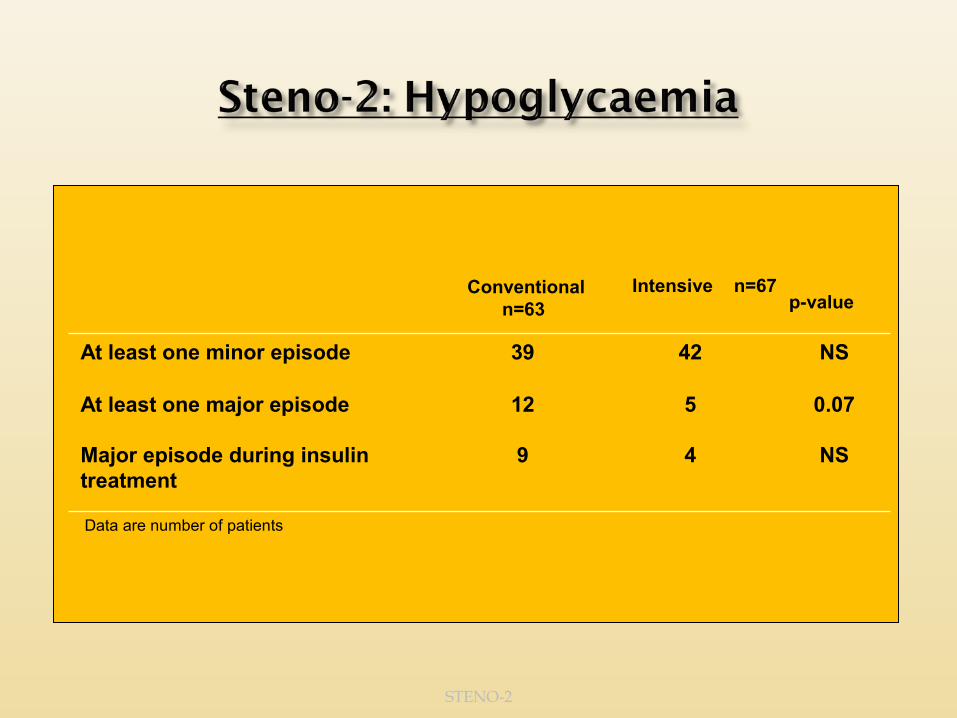
Conventional n=63
Intensive n=67 p-value
NS4239At least one minor episode
NS49Major episode during insulin treatment
0.07512At least one major episode
Data are number of patients
Our study was not designed to identify which elements of intensive diabetes therapy contributed most to the reduction in cardiovascular risk.
However, using a risk calculator based on epidemiologic and interventional data from patients with type 2 diabetes in the United Kingdom Prospective Diabetes Study
we concluded that the use of statins and antihypertensive drugs might have had the largest effect in reducing cardiovascular risk during the 7.8 years of intervention
with hypoglycemic agents and aspirin the next most important interventions.24
STENO-2
Compared with a conventional multifactorial Compared with a conventional multifactorial treatment an intensive and target driven treatment an intensive and target driven
behaviour modelling and polypharmacy for 7.8 yrs behaviour modelling and polypharmacy for 7.8 yrs
induced an absolute risk reduction of induced an absolute risk reduction of 20%20% (RRR (RRR 0.53; NNT 4) in CVD in patients with type 2 DM and 0.53; NNT 4) in CVD in patients with type 2 DM and
the metabolic syndrome incl. microalbuminuriathe metabolic syndrome incl. microalbuminuria
The RRR’s found for microvascularThe RRR’s found for microvascularevents after 4 years were main-events after 4 years were main-tained at a similar level after 7.8 tained at a similar level after 7.8
years of intervention: nephropathy years of intervention: nephropathy 61%, retinopathy 58% and autono-61%, retinopathy 58% and autono-
mic neuropathy 63%mic neuropathy 63%
Do we screen asymptomatic people (men or women) for CVD
ADA – NO ACC – coronary artery calcium score
can be used
Consider investigations for coronary artery disease in the presence of any of the following:
1. Atypical cardiac symptoms (e.g., unexplained dyspnea, chest discomfort)
2. Signs or symptoms of associated vascular disease including carotid bruits, transient ischemic attack, stroke, claudication, or peripheral arterial disease
3. Electrocardiogram abnormalities (e.g., Q waves).
1. Resting ECG
2. Exercise stress testing with ECHO cardiography
3. Those who cannot exercise we van use pharmacological stress echo
4. For those with baseline ECG abnormalities we can use pharmacological stress echo or nuclear imaging
5. Coronary artery Calcium score can also be considered in women > 40
Complex lesions - CABG
Lower disease complexity - PCI
Left main - CABG
SYNTAX score < 22 - PCI
Secondary risk reduction with guideline directed therapies for HTN,Cholesterol ,Smoking and HbA1c
38 maleRecently detected T2DMBP 130/90Lipids 206 / 174 /32 /123Smoker , no exercise

52 female Obese Newly detected T2DM Family h/o premature CAD Known HTN on treatment Lipids 212 / 376 / 32 / 96
56 female T2DM 15 yrs.Obese and HTNBP 130/82Lipids 168/178/36/94FBS 96 PPBS 156 Sr. Crea. 0.9ECG - LVHRetinopathy ,neuropathy +H/O TIAOn OHA ,ACEI ,Aspirin ,Statin
Lifestyle changes (diet, exercise, not smoking) and controlling dyslipidemia and high blood pressure, with the use of statins and antihypertensive medications respectively are important than glycemic control in reducing MACE events in patients with T2DM
Treat women as aggresively as men if not more
High dose statins in certain patients
Anti-platelets according to guidelines
CABG better in multiple lesions

THANK YOU





![HISO 10071:2019 cvd risk assessment data standard · Web viewiv [TITLE] HISO 10071:2019 cvd risk assessment data standard 9 30 HISO 10071:2019 cvd risk assessment data standard HISO](https://img.dokumen.tips/doc/110x75/60af119b3ec8762eec607c48/hiso-100712019-cvd-risk-assessment-data-standard-web-view-iv-title-hiso-100712019.jpg)