Embed Size (px)
Citation preview

九州大学学術情報リポジトリKyushu University Institutional Repository
Leiomyosarcoma Versus Bizarre and CellularLeiomyomas of the Uterus : A Comparative StudyBased on the MIB-1 and Proliferating CellNuclear Antigen Indices, p53 Expression, DNAFlow Cytometry, and Muscle Specific Actins
尼田, 覚Graduate School of Medical Sciences, Kyushu University
https://doi.org/10.11501/3120485
出版情報:九州大学, 1996, 博士(医学), 課程博士バージョン:権利関係:

[
International Jollrnal of Gynecological Pathology 14:134---142, Raven Press, Ltd .. New York © 1995 International Society of Gynecological Pathologist
Leiomyosarcoma Versus Bizarre and Cellular Leiomyomas
of the Uterus: A Comparative Study Based on the MIB-1 and Proliferating Cell Nuclear Antigen Indices, p53
Expression, DNA Flow Cytometry, and Muscle
Specific Actins
Satoshi Amada, M.D., Hitoo Nakano, M.D., and Masazumi Tsuneyoshi, M.D.
Summary: There is still controversy over the criteria for malignancy of smooth muscle tumors (SMTs) of the uterus. We examined 51 cellular SMTs using immunohistochemistry for MIB-1, proliferating cell nuclear antigen (PCNA), p53, HHF35, a-smooth muscle actin (SMA), and flow cytometry. Morphologically, the 51 cases were classified into 24 leiomyosarcomas (LMS), two uncertain malignant potential, four bizarre leiomyomas, and 21 cellular leiomyomas. The mean values of the MIB-1 and PCNA indices showed significant differences between LMS and benign SMTs. p53 cells were positive in eight of 241eiomyosarcomas, and 12 of 22 were aneuploid. HHF35 and a-SMA showed a diffuse positivity in almost all the benign SMTs. In contrast, I 0 of the 24 LMS were either focally positive or negative for SMA. Using a logistic regression model, at cut-off points of 3.6 on the MlB-1 index and 15.6 on the PCNA index, the LMS and the benign SMTs were classified with an overall accuracy of 92% and 82%, respectively. Moreover, by combining the MIB-1 index and a-SMA positivity, the cut-off point could be established at 0.492 on the probability scale with the highest overall accuracy of 96%. Regarding the prognosis of LMS, p53 positivity wa correlated with survival (p = 0.0357). A combination of the MIB-1 index and a-SMA was helpful in distinguishing between LMS and benign SMT. Moreover, p53 positivity was considered to be a good marker for predicting the prognosis of LMS. Key Words: Leiomyosarcoma-Ki-67-Proliferating cell nuclear antigen-p53-Fiow cytometry-Muscle-specific actins.
Uterine smooth muscle tumors (SMTs) are easily diagnosed in the majority of cases. However, it is difficult to determine whether they are benign or malignant in orne cases because they often include overlapping cases of clinically benign and malignant
From the Second Department of Pathology (S.A., M.T.) and Department of Gynecology and Obstetrics (H.N.), Faculty of Medicine, Kyu hu University, Fukuoka, Japan.
Address correspondence and reprint requests to Prof. Masazumi Tsuneyoshi , Second Department of Pathology, Faculty of Medicine, Kyushu Univcr ity, 3-1-1 Maidashi, Higa hiku, Fukuoka 812, Japan.
134
neoplasms with either aberrant or bland cytological
features ( l ,2). Although some investigators claimed to have established the criteria for malignancy in
the uterine SMTs containing morphological factors with nuclear atypia and mitotic counts (1-8), no accurate diagnostic criteria yet exists for malignancy. Recently, several reports disclosed correlation of the biological behavior with Ki-67 (9, 10), prolifer
ating cell nuclear antigen (PCNA) (11-14), and the
expression of mutant p53 protein (15, 16) using an immunohistochemical assay. This study examines leiomyosarcomas and compare them with benign
SMTs (bizarre and cellular leiomyomas) in order to

LEIOMYOSARCOMA OF THE UTERUS 135
assess the correlation between their biological characteristics and histological findings using both immunohistochemical techniques and flow cytometry.
MATERIALS AND METHODS
Fifty-one cases of uterine cellular SMTs were selected from our files of gynecological neoplasms in the Second Department of Pathology, Kyushu U niversity, from 1977 to 1992. Cases initially labeled as leiomyosarcoma (LMS), cellular leiomyoma (CL), bizarre leiomyoma (BL), and uncertain malignant potential category (UMP) were studied. The clinical information, including follow-up data, was obtained from both the patients' physicians and medical records. Follow-up data for all patients except for one with LMS were available. Hematoxylin and eosin preparations in the proper number for each tumor size were reviewed.
Histologic assessment
The following histologic features were semiquantitatively evaluated. The nuclear atypia of each case was determined by dividing the range of nuclear features from mild to severe. Mildly atypical nuclei possessed regular borders and an even distribution of chromatin, similar to that of benign CL. Severely atypical nuclei were large and pleomorphic, with an irregular nuclear shape, clumped chromatin, and prominent nucleoli. Moderately atypical nuclei ranged between mild and severe. Mitoses were counted and expressed as the number of mitotic figures per I 0 high-power fields (hpf). Count was made on a binocular Olympus BH-2 microscope using 40x S-Plan Apo objective and 10x/20L widefield eyepieces while selecting the most active areas where mitoses were the most frequent. The presence of coagulative tumor necrosis was examined in all the given specimens of each case.
Based on the above histological factors, including the criteria of hypercellularity, cellular atypia, mitotic count, and the presence of tumor necrosis based on previous reports (1-8), the 51 cases were diagnosed into LMS, UMP, BL, and CL. LMS were further classified into four subgroups: (a) moderate to severe nuclear atypia and lO and more mitotic figures/1 0 hpf; (b) moderate to severe nuclear atypia and five to nine mitotic figures/1 0 hpf; (c) mild nuclear atypia and 10 or more mitotic figures/ I 0 hpf; (d) mild nuclear atypia and five to nine mitotic figures/] 0 hpf. LMS and benign SMT (BL and
CL) were used for the immunohistochemical and flow cytometric studies.
Immunohistochemistry
All sections from the formalin-fixed and paraffinembedded specimens were studied immunohistochemically using avidin-biotin complex methodology (17). The primary antibodies and their dilutions are summarized in Table I. All the sections were deparaffinated with xylene and dehydrated in a graded series of alcohol. The sections for Ki-67 (MIB-1) were pretreated with boiling in citrate buffer, pH 6.0, for 30 min. All the sections were incubated in 0.3% hydrogen peroxidase in methanol for 30 min and then were exposed to the primary antibodies at given dilutions by phosphate-buffered saline at room temperature for 90 min. A subsequent reaction was made by using an avidin-biotin-peroxidase kit (Nichirei, Tokyo, Japan). The sections were stained with freshly prepared diaminobenzidine (DAB) solution and then were counterstained with methyl green or hematoxylin.
Assessment of immunohistochemical staining
MIB-1, PCNA, and p53 staining was confined to the nuclei. The MIB-1 and PCNA indices, as the extent of MIB-1 and PCN A positivity in each case, respectively, were evaluated by determining the percentage of positive nuclei counted at high power and more than three fields that were chosen at random. A p53-positive case was defined as a case with positive cells, whereas a case that expressed sporadic positive cells was excluded from the positive category. HHF35 and a-SMA staining were categorized into four grades expressed as negative (- ), focally positive (1 +; <50% of cells had a positive reaction), intermediately positive (2 +; I+ to 3 + ), and diffusely positive (3 +; almost all the tumor cells had a positive reaction).
Flow cytometry
The flow cytometric determination of tumor cell DNA content was performed on paraffin-embedded sections using an earlier published method (18, 19).
TABLE 1. Panel of antibodies
Antibody Source Dilution -- --
Ki-67 (Ml B-1) monoclonal lmmunotech S.A. 1:100 PCNA (PCIO) monoclonal DAKO 1:100 p53 (CMI) polyclonal Novocastra 1:500 HHF35 monoclonal DAKO 1:100 o.-SMA monoclonal Sigma Chemical 1:5000
lnr 1 Cynecol Purhol, Vol. 14. No.2. 1995

136 S. AMADA ET AL.
The cellular DNA content was measured on a FACScan flow cytometer (Becton Dickinson, Sunnyvale, CA) with a 488-nm argon ion laser. Histograms of I x 104 cells were recorded and analyzed with Cell FIT cell-cycle analysis software (Becton Dickinson). The first G0/1 peak was assumed to be a diploid population, and DNA aneuploidy was defined by the presence of a well-defined second peak.
Statistical methods
A logistic regression model of the BMDP statistical Package Program (CBMDP Statistical Software Inc., California) on the IBM system 4381 computer (Armonk, New York, NY) was used to calculate the probabilities of a malignant or benign group (20). From this analysis, the equations and optimal thresholds for classifying the cases into either a malignant or a benign category were calculated (21). The accuracy of classification was determined for each individual parameter (MlB-1 and PCNA indices), and subsequently for more than one variable (adding p53, HHF35, and a-SMA status) to further improve accuracy. The survival rates of the cases with LMS were calculated by the Kaplan-Meier method, and comparisons were made u ing the generalized Wilcoxon test. Other statistical differences were evaluated with the use of either the x2 or the Wilcoxon-Mann- Whitney test.
RESULTS
Histological features
Based on the findings previously mentioned in Materials and Methods, the cellular SMTs were cia ified into 24 LMS, two UMPs, four BLs, and 21 CL . ln the 24 LMS, group A consisted of l 3 c a es; the highest mitotic count was 6 0 mitotic figures/10 hpf, the average 31.8 mitotic figures/tO hpf. Eight of the 13 cases showed severe nuclear atypia, whereas the others exhibited moderate atypia. All but one showed foci of coagulative tumor necrosis. In group B, which con is ted of three cases, two of the three showed severe nuclear atypia and tumor necrosis. Another tumor showed moderate atypia and no necrosis. Group C consisted of five neoplasms with a range of 10-16 mitotic figures/10 hpf. No cases in group C disclosed any necrosis. Group D included three tumors, all of which showed coagulative necrosis. Two neoplasms exhibiting two and three mitotic figures/10 hpf, moderate nuclear atypia, and no tumor cell necrosi were labeled as UMPs, according to the published criteria (1 ,2).
lni J Gynecol Paihol. Vol. 14, No.2. 1995
These two UMPs were excluded from this comparative study (Table 2).
Four BLs exhibited diffuse severe pleomorphism with bizarre giant tumor cells but lacked any mitotic figures. Twenty-one CLs showed minimal to mild nuclear atypia and a range of zero to three mitotic figures/ I 0 hpf. Three CLs contained scattered pleomorphic giant tumor cells. No tumor necrosis was detected in any of the BLs or CLs.
Clinical features
The age range of the patients with LMS was 38-63 years (mean 48.7). All patients with LMS were treated with a total hysterectomy as primary therapy. The initial laparotomy disclosed extrauterine lesions in two women of group A. Twelve women, including the two mentioned above, died of disease at 2-210 months (mean 34.4) after surgery and were from all of the four groups. One woman from group D is now being treated for a recurrent tumor. Both women with UMP are alive without any sign of disease 14 and 59 months after surgery, respectively.
TABLE 2. Histolugical findings of leiomyosarcomas and UMP tumors
Age Case !yr)
Leiomyosarcomas
Atypia Mitoses (110 hpf) Necrosis
Prognosis (mo)
Moderale to se1·ere nuclear atypia and 10 and more mf/10 hpJ I 63 Severe 60 + DOD ( 19) 2 49 Severe 30 + DOD ( 5) 3 62 Severe 30 + DOD ( 48) 4 45 Severe 24 + DOD ( 41) 5 47 Severe 15 DOD ( 2) 6 50 Severe 22 + NED (117) 7 43 Severe 20 + ED ( 77) 8 59 Severe 20 + ED ( 20) 9 54 Moderate 53 + DOD ( 9)
10 54 Moderate 46 + DOD ( 23) II 38 Moderate 41 + NED ( 44) 12 43 Moderate 41 + NED ( 6) 13 45 Moderate 12 + NED (116)
Moderate to sn•ere nuclear atypia and 5-9 mf! 10 hpf 14 49 Severe 8 + DOD ( 22) 15 54 Severe 7 + DOD ( 12) 16 54 Moderate 6 DOD (210)
Mild nuclear cllypia and 10 and more mf/10 hpf 17 40 Mild 13 DOD ( 9) 18 53 Mild 16 19 47 Mild 15 NED ( 35) 20 42 Mild 14 NED ( 5) 21 43 Mild 10 NED ( 61)
Mild nuclear atypia and 5-9 mf/10 hpf 22 49 Mild 8 + DOD ( 13) 23 43 Mild 6 + AWD ( 51) 24 43 Mild 5 + NED ( 86)
UMP tumors 25 32 Moderate 3 NED ( 59) 26 43 Moderate 2 NED ( 14)
UMP. uncertain malignant potential category; mf/10 hpf, mitotic figures/10 hpf: DOD, died of disease: NED, no evidence of disea e; AWD, alive with disease.
LEIOMYOSARCOMA OF THE UTERUS 137
All the patients with benign tumors have undergone either a total hysterectomy or myomectomy for the diagnosis of myoma uteri and are alive without disease after surgery (follow-up period of 28-183 months, mean 70.4).
MIB-1 and PCNA indices
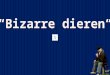
All tumors stained relatively homogeneously for MIB-1 (Fig. I) and PCNA (Fig. 2). The number of counted cells ranged from 600 to 2,000 at the selected fields in each neoplasm. There was little difference in the positivity for MIB-1 or PCNA among the selected fields in each case. The MIB-1 and PCN A indices in the tumors examined were within the ranges of 0.2-47.5 and 0-85, respectively (Figs. 3 and 4). Both the mean indices of LMS and benign SMTs (BLs and CLs) were 19.2 and 1.1, and 35.2 and 6.2, respectively (Table 3). There were significant differences in both indices between LMS and benign SMTs (p < 0.0001).
p53 expression
In the 24 LMS, there were eight neoplasms positive for p53, which expressed >I 0% positive cells in each high power field (Fig. 5), whereas none of the 25 benign BLs and CLs expressed a positive reaction for p53 (p = 0.0016, Table 3).
DNA ploidy pattern
Analyzable DNA histogram s were obtained from 44 of the tumors studied. The mean coefficient of variation was 5.3 (range 1.2-12.5). Twelve of the 22 LMS exhibited a DNA-aneuploid cell population, whereas all the benign SMTs showed a diploid
FIG. 1. lmmunostaining for M I B-1. In the leiomyosarcoma with moderate atypical nuclei and 41 mitotic figure /10 hpf (case 12), 47.5% of the nuclei exhibited a positive reaction.
DNA histogram. The DNA ploidy pattern of the LMS and the benign SMTs (BLs and CLs) significantly differed between themselves (p < 0.0001, Table 3).
Muscle-specific actins
HHF35 and a-SMA were seen almost diffusely (the value exhibited 2 + or 3 +) in all the benign BLs and CLs except for two cases. In contrast, lO of 24 LMS showed either focal or negative immu
noreactivity for HHF35 or a-SMA (0 or 1 + ). The difference of immunostaining for a-SMA was statistically significant between the LMS and the benign SMTs (BLs and CLs) (p = 0.0004) (Table 3).
Logistic regression model
The probability of being an LMS or a benign SMT (BL or CL) was computed using a logistic regression equation with either the MIB- I or PCN A index. To determine the accuracy of classification into LMS and benign SMT (BL or CL), the probability at different cut-off points was tested. For the MIB-1 index, at a cut-off point of 0.492 probability (MIB-1 index 3.6), 87% (21 of 24) of the LMS and 96% (24 of 25) of the benign SMTs, overall 92%, were correctly classified. Regarding the PCN A index, at a cut-off point of probability of 0.525 (PCNA index 15.6), 75% (18 of 24) of LMS and 84% (21 of 25) of the benign SMTs, overall 82%, were also correctly classified (Table 4).
When all possible combinations of more than one parameter (MIB-1 and PCNA indices, p53 and muscle-specific actins) were considered, the highest
lnt J Gynecol Pathol. Vol. 14. o. 2. 1995

138 S. AM ADA ET AL.
overall accuracy was achieved by combining the MIB-l index and a-SMA. At a cut-off probability of 0.492, 96% (23 of 24) of the LMS and 96% (24 of 25) of the benign SMT, 96% overall, were correctly classified (Table 4).
Survival In 23 LMS, there were no differences between
the survival and mitotic count (groups A and C vs. B and D) or nuclear atypia (groups A and B vs. C
and D). Regarding the immunohistochemical and flow cytometric factors, LMS had a tendency to correlate with survival and the p53 positivity with statistical significance (p = 0.0357, Fig. 6). However, there wa no ignificant correlation between
0
-+0 8
& X Q)
-o 30 c §
c:O § � 0
§
� malignant benign
ln=c41 \n=25i
FIG. 3. Distribution of the MIB-1 index. There wa a significant difference between the malignant group (leiomyosarcomas. mean 19.2) and the benign group (bizarre and cellular leiomyomas, mean 1.1) (p < 0.0001).
In! J Gynecol Parhol, Vol. 14, No.2, 1995
FIG. 2. Immunostaining for PCNA. In the leiomyo arcoma with severe atypical nuclei and 20 mitotic figures/ I 0 hpf (case 8), 70% of the nuclei exhibited a positive reaction.
the other factor (MIB-1, PCNA, muscle-specific actins, or DNA ploidy pattern) and the prognosis.
DISCUSSION
Several investigators have reported on the diagnostic criteria for uterine LMS, as shown by hypercellularity, cellular atypia, and numerous mitotic figures (1-8). The most reliable factor of the diag
nosis is believed to be the mitotic count (1 ,3-6). However, there is a small controversial group of the uterine SMTs with cellular atypia and only a slight amount of mitotic activity ( < 10 mitotic figures/ I 0 hpf), in which malignancy is difficult to determine.
Cll �0
� 8 X Cll u
60 -o 0 c
<( 0
z u 40 0 0...
� C>
:w C>
e> C> C>
8 Cl>
0
malignant benign \11=2-ll (11=2'\i
FIG. 4. Distribution'of the PC A index. There was a significant difference between the malignant group (leiomyosarcomas. mean 35.2) and the benign group (bizarre and cellular leiomyomas. mean n.:?.) (p < 0 0001).
LEIOMYOSARCOMA OF THE UTERUS 139
TABLE 3. Comparison of the immunohistochemical and flow cytometric features between leiomyosarcomas
and benign bizarre and cellular leiomyomas
LMS Benign SMT (8L and CL) p
Mean MIB-1 index (range) 19.2 (0.8--47.5) I. I (0 .2-5.0) <0.0001" Mean PCNA score (range) 35.2 (0-85) 6.2 (0-27) <0.0001" p53
+ 8 0 16 25 0.0016"
a-SMA
I+ 2+ 3+
HHF35
I+ 2+ 3+
DNA ploidy pattern Aneuploid Diploid
4 6 7 7
3 3 9 9
12 10
0
22
I 7
IIi
0 22
0.0004"
0.2415"
<0 0001"
LMS. leiomyosarcoma: SMT, smooth muscle tumor: BL. bizarre leiomyoma; CL. cellular leiomyoma.
"Wilcoxon-Mann-Whitney te�t "x" test.
In our experience, six patients who were diagnosed with LMS showed < l 0 mitotic figuresll 0 hpf, and four of them died of the disease at 12-210 months after surgery. In the groups with mild nuclear atypia, two patients died from the disease while histo
logically showing only 13 and eight mitotic figures/ 10 hpf, and one patient with six mitotic figures/10 hpf has a history of a recurrence. On the other hand, no patients with fewer than five mitotic figures/10 hpf had either recurrence or a fatal course. Thus, a definition to distinguish bet ween benign and malignant SMTs might be set at five mitotic figures/ I 0 hpf if one does not need to bother about the problem of accuracy in counting mitosis as discussed in the literature (22-25).
MIB-1 (345 and 395 kDa double band in Western blot analysis) is a new antibody that reacts with the Ki-67 nuclear antigen in paraffin-embedded sec
tions, is associated with cell proliferation, and is found throughout the cell cycle of G I, S, G2, and M phases (26,27). Few studies of MIB-1 on neoplasms have been reported (28). PCNA is a 36-kDa acidic nonhistone nuclear protein that functions as an auxiliary protein for DNA polymerase o and is an ab
solute requirement for DNA synthesis (29). In mesenchymal neoplasms, a large series of PCNA immunostaining has been performed on a few studies of hemangiopericytoma by Yu et al. (12) and synovial sarcoma by Oda et al. (11 ). No series of MIB-1
and PCNA immunostaining have been previously performed on the uterine SMTs. We found a significant difference (p < 0.0001) in the MIB-1 and PCNA indices between the LMS (19.2 and 35.2) and benign SMTs (BLs and CLs) (I. 1 and 6.2). The mitotic count, the most reliable diagnostic morphological factor in previous studies (1 ,3-6), shows only the number of proliferating cells in the M phase. But the proliferating cells occupy several functional
states besides mitosis. Ki-67 is found in proliferating cells of the G 1, S, G2, and M phases (27), and PCNA is synthesized in the late G 1 and S phases (29). Therefore, our results of the MIB-1 and PCNA indices make it clear that the number of proliferating cells is important to discriminate between LMS and benign SMTs. Indeed, at a cut-off point of 3.6 for the MlB-1 index and at 15.6 for the PCNA index, the LMS and benign SMT were predicted with an overall accuracy of 92% and 82%, respectively. Hence, we conclude that the MIB-1 and PCNA indices are useful for the diagnosis of LMS.
The p53 gene encodes a 53-kDa nuclear phosphoprotein involved in the negative regulation of cell growth (30,31 ). The mutations in this gene play an important role in the development of many malignant tumors (32-36). Mutant p53 proteins have a longer half-life than the wild-type proteins and are easily detected by immunohistochemical methods.
Several investigators have demonstrated an overexpression of the p53 protein immunohistochemically in a variety of human malignancies (15, 16). However, no large series of SMTs with p53 evaluation have yet been published. We found p53 protein was expressed in eight of 24 LMS (33%) but in none of the benign SMTs (p = 0.0016). In addition, the p53 positivity statistically correlated with the prognosis of the LMS (p = 0.0357). Recently, mutant p53 has been stressed to be related to cell growth (37) and deviation from apoptosis (38,39). Because the LMS showed cell proliferation more rapid than that of SMTs as demonstrated with our MIB-1 and PCNA indices study, p53 might only be expressed in the LMS. lt is expected that the degree of cell proliferation would correlate with biological behavior of LMS (4-6,40,41 ). Although our studies did not demonstrate a correlation between the mitotic count, MIB-1 or PCNA index, prognosis, and
p53 positivity, in our opinion the p53 expression detects cases with a poor prognosis. p53 might thu be expressed in tumors with a high cell proliferation rate that could not be detected by mitotic count or MIB-1 or PCNA index in the LMS. Therefore, the
Int J Gynecol ?athol, Vvl. 14. No. 2. /995

140 S. AMADA ET AL.
p53 expression is a good marker for predicting po
tential cases with LMS.
A semiquantitative evaluation for muscle-specific
actins in uterine SMTs was compared with their
histological features for the first time. We examined
the characteristics of the tumor cells differentiating
toward smooth muscle while using immunostaining
( 42). In our study, benign B Ls and CLs tended to
TABLE 4. Logistic regression function
1. MlB- 1 index Equation for the probability of being LMS:
Exp(y) p(LMS) = I + Exp(y)
y = - 3.075 -t 0.8487 x MIB-l index
If p > 0.492, the case is predicted to be LMS. Otherwise. if p.::; 0.492. the case is predicted to be benign BL or CL.
2. PCNA index Equation for the probability of being LMS:
Exp(y) p(LMS) =
l + Exp(y)
y = - 1.675 + 0.1141 x PCNA index
If p > 0.525, the case is predicted to be LMS. Otherwise. if p ,::; 0.525, the case is predicted to be benign BL or CL.
3. MIB- 1 index and a-SMA positivity Equation for the probability of being LMS:
Exp(y) p(LMS) =
I + Exp(y)
y = 3.15 + 0.8904 X MIB-1 index 2.839 X o.-SMA positivity (0 if - . 1 if l +. 2 if 2 +, 3 if 3 +)
If p > 0.492. the case i predicted to be LMS. Otherwise, if p .::; 0.492, the case is predicted to be benign BL or CL.
lnt 1 Gynecol P11tlw/, Vol. 14, No.2, 1995
FIG. 5. Immunostaining for p53. The leiomyosarcoma exhibited p53 overexpression with the nuclei showing variable intensities (case 3).
demonstrate more diffuse immunostaining for mus
cle-specific actins than did the LMS. Evans et al.
(43) reported desmin staining in nine uterine SMTs.
Their results were also similar to ours, in which
they described seven leiomyomas as being strongly
positive and two LMS as being negative. Thus, if
there is little or no staining with actin, an SMT
should be regarded with caution. Malignant cells
appear to be heterogenous and lose differentiation
for smooth muscle cells .
A similar analysis for the DNA ploidy patterns of
uterine SMTs was previously reported by Tsushima
et al. (44). They concluded that the DNA ploidy
pattern could not be used diagnostically to distin
guish between malignant and benign SMTs because
(%) 100
:.J . ..
.. t ............. ;
� oL .............................. i p53 negative (n = IS)
<( : .... J ....... J. .......... . 0:: _J :; 50 > 0:: :::> (/)
p53 positive (n = 8)
Q L-----�----------�----�----� 2 3 4 5
(Years) YEARS AFTER SURGERY
FIG. 6. The urvival curves of 23 case· with leiomyosarcoma in relation to the p53 positivity. The positive p53 group had a worse survival rate compared with that of the negative p53 group (p =
0.0357). Kaplan-Meier method, generalized Wilcoxon test.
LEIOMYOSARCOMA OF THE UTERUS 141
of the abnormal DNA ploidy patterns in 12% of
benign SMTs. Our study disclosed no DNA aneu
ploid cases in the benign SMTs, whereas 12 of 22
LMS had DNA aneuploid peaks in our series of
cellular SMTs. Therefore, although why our results
differed from those of Tsushima et al. (44) is still
unclear, the DNA ploidy patterns appear to help in
making a distinction between LMS and benign CLs
and BLs of the uterus.
In this study, the individual immunohistochemi
cal and flow cytometric parameters that we exam
ined proved to be useful in discriminating between
LMS and benign SMT (BL or CL). Moreover, by
combining the MIB- I index and a-SMA positivity,
96.9% of LMS and 96% of benign SMTs were clas
sified with the highest overall accuracy (96%) using
the logi tic regression model. In view of these find
ings, we suggest that the combination of the MIB-1
index and a-SMA positivity is clearly helpful in dis
criminating between LMS and benign SMT.
Acknowledgment: The surgical specimens and clinical data reported herein were obtained from the following institutions: Kyushu University, National Kyushu Cancer Center, Hamanomachi Hospital, Kyushu Welfare Pension Hospital, Fukuoka Red-Cross Hospital, Matsuyama Red-Cross Hospital, Kitakyushu City Medical Center, Kitakyushu City Wakamatsu Hospital, Kitakyushu City Moji Hospital, National Nakatsu Hospital, National Beppu Hospital, Social Insurance Saga Hospital, and Kyushu Central Hospital. We thank these institutes for contributing their cases for this study. We also thank Kouhei Akazawa (Department of Medical Informatic , Faculty of Medicine, Kyushu University) for assistance with statistical analy is and BrianT. Quinn for editing the manuscript. This study was supported by a Grant-in-Aid for Scientific Research (No. 06280 I 05) from the Ministry of Education, Science and Culture, Japan.
REFERENCES
I. Hendrickson MR. Kemp ·on RL. The uterine corpus. In: Sternberg SS, Mill SE, ed. Sur[<icol pathology (�(the female reproductil'e system and peritoneum. ew York: Raven, 1991 : I 05-68.
2. Silverberg SG. Kurman RJ. Tumors of the uterine corpus and gestational trophobla tic disease. In: Rosai J. ed. Atlas of tumor patlwlogy. Washington. DC: AFIP, 1992.
3. Evans HL, Chawla SP, Simpson C. Finn KP. Smooth muscle neopla m of the uteru. other than ordinary leiomyoma . Cancer 1988:62:2239-47.
4. Christopherson WM, Williamson EO. Gray lA. Leiomyosarcoma of the uterus. Concer 1971:29:1512-7.
5. Taylor HB, orris HJ. Me enchymal tumors of the uterus: IV diagno is and prognosis of leiomyosarcoma . Arch Pathol 1966:82:40-4.
6. Kempson RL, Sari W. Uterine sarcomas: clas ·ification. diagnosis and prognosis. Hum Pathol 1970; I :331-49.
7. Spiro RH, Koss LG. Myosarcoma of the uterus: a clinicopathological study. Cancer 1965;18:571-88.
8. Silverberg SG. Leiomyosarcoma of the uterus: a clinicopathologic study. Ohs1et Gynec ol 1971 ;38:613-28.
9. Burger PC, Shibata T, Kleihues P. The use of the monoclonal antibody Ki-67 in the identification of proliferating cells: application to urgical neuropathology. Am J Surg Pa1hol 1986:10:611-7.
10. Gerdes J. Lelle R. Pickartz H, et al. Growth fraction in breast cancers determined in situ with monoclonal antibody Ki-67. J Clin Putlwl 1986:39:977-80.
II. Oda Y, Hashimoto H, Tsu ne yoshi M. The prognostic value of immunohistochemical staining for proliferating cell nuclear antigen (PCNA) in synovial sarcoma. Cancer 1993;72: 478-85.
12. Yu CC-W, Hall PA. Fletcher COM, et al. Haemangiopericytomas: the prognostic value of immunohistochemical staining with a monoclonal antibody to proliferating cell nuclear antigen (PCNA) Histopatholo{<y 1991 ;19:29-33.
13. Robbins BA, Vega D. Ogata K. Tan EM, Nakamura RM. Immunohistochemical detection of proliferating cell nuclear antigen in solid human malignancies. Arch Pathol Lah Med 1987: Il l :841-5.
14. Hall PA. Levi on DA. Wood AL, et al. Proliferating cell nuclear antigen (PCNAI immunolocaliLation in paraffin sections: an index of cell proliferation with evidence of deregulated expression in :.orne neoplasms. J Pathol 1990:162: 285-94.
15. Marks JR, Davidoff AM. Kerns BJ, et al. Overexpression and mutation of p53 in epithelial ovarian cancer. Cancer Res 1991 :51:2979-84.
16. Porter PL. Gown AM. Kramp SG, Coltrera MD. Widepread p53 overexpression in human malignant tumors: an
immunohistochemical study using methacarn-fixed, embedded ti sue. Am J Patholl992;140:145-53.
17. Hsu SM. Raine L, Fanger H. The usc of antiavidin antibody and avidin-biotin-peroxidase complex in immunoperoxidase technics. Am J Clin Patholl981)5:816-21.
18. Hedley DW, Friedlander ML. Taylor lW, Rugg CA, Musgrove EA. Method for analysi of cellular DNA content of paraffin-embedded pathological material using flow cytometry. J Histochem Cytochem 1983:31: 1333-5.
I':J. Schutte B. Reynders MMJ, Bosman FT. Blijham GH. Flow cytometric determination of DNA ploidy level in nuclei i ·alated from paraffin-embedded tissue. Cytometry 1985;6:26-30.
20. Dixon WJ. BMDP stotisticol S(�fiware. Berkeley, CA: University of California Press. 1990.
21. Binder SW, Huang l, Fu YS, Hacker NF. Berek JS. Risk factors for the development of lymph node metastasi in vulvar squamous cell carcinoma. Gynecol Oneal 1990;37:9-16.
22. Silverberg SG. Reproducibility of the mitosi count in the histologic diagnosis of smooth mu cle tumors of the uterus. Hllm Pathol 1976:7:451-4.
23. Scully RE. Editorial: mitosis counting-l. Hum Pathol1976: 7:481-2.
24. Kempson RL. Editorial: mito i counting-11. Hum Pathol 1976;7:482-3.
25. Norris HJ. Editorial: mitosis counting-Ill. Hum Pat hoi 1 ':)76;7:483-4.
26. Key G. Becker MHG, Duchrow M. Schinter C. Gerdes J. ew Ki-67 equivalent murine monoclonal antibodies
(MIB 1-3) prepared against recombinant parts of the Ki-67 antigen. Anal Cell Pathol 1992;4: 181.
27. Gerdes J, Lemke H, Bai ch H. Wacker H-H. Schwab U. Stein H. Cell cycle analysi of a cell proliferation-associated human nuclear antigen defined by the monoclonal antibody Ki-67. J lmmruwll984;133:1710-5.
lnt J Gyneco/ Pathol. Vol. /4, No . 2. 1995

142 S. AMADA ET AL.
28. Kerns B-JM, Jordan PA, Faerman LL. Berchuck A, Bast RC. Layfield LJ. Determination of proliferation index with MlB-1 in advanced ovarian cancer using quantitative image analysis. Am J Clin Pat hoi 1994:101:192-7.
29. Bravo R, Frank R, Blundell PA, Macdonald-Bravo H. Cyclin/PCNA is the auxiliary protein of D A polymerase-c. Nature 1987;326:515-7.
30. Lane DP. Crawford LV. T antigen is bound to a host protein in SV40-transformed cells. Nature 1979;27R:261-3.
31. Miller C, Mohanda T, Wolf D. Prokocimer M, Rotter V, Koeftler HP. Human p53 gene localized to short arm of chromosome 17. Nature 1986;3 19:783-4.
32. Nigro JM. Baker SJ. Preisinger AC, et al. Mutations in the p53 gene occur in diverse human tumour types. Nat111e 1989: 342:705-8.
33. Finlay CA, Hinds PW, Levine AJ. The p53 proto-oncogene can act as a suppressor of transformation. Cell 1989:57:1083-93.
34. lggo R, Gatter K, Bartek J, Lane D. Harris AL. Increased expression of mutant forms of p53 oncogene in primary lung cancer. Lancet 1990:335:675-9.
35. Hollstein M, Sidransky D. Vogelstein B. Harris CC. p53 mutations in human cancers. Science 1991 ;253:49-53.
36. Toguchida J, Yamaguchi T, Ritchie B, et al. Mutation spec-
lnt 1 Gynecol Pathol. Vol. 14. No. 2. 1995
trum of the p53 gene in bone and soft tissue sarcomas. Cancer Res 1992;52:6194-9.
37. Allred DC, Clark GM, Elledge R, et al. Association of p53 protein expression with tumor cell proliferation rate and clinical outcome in node-negative breast cancer. J Nat/ Cancer lnst 1993;85:200-6.
38. Lane DP. A death in the life of p53. Nature 1993;362:786-7. 39. Culotta E. Koshland DE. p53 sweeps through cancer re
search. Science 1993;262: 1958-61. 40. Dihn TV, Woodruff J D. Leiomyosarcoma of the uterus. Am
J Obsret Gyneco/1982;144:817-23. 41. Hannigan EV, Gomez LG. Uterine leiomyosarcoma: a re
view of prognostic clinical and pathologic features. Am J Obsret Gynecol 1979; 134:557--64.
42. Tsukada T, McNutt MA, Ross R, Gown AM. HH F35, a muscle actin-specific monoclonal antibody: II. reactivity in normal. reactive, and neopla tic human tissue. Am J Patho/ 1987; 127:389-402.
43. Evans OJ, Lampert lA, Jacobs M. Intermediate filaments in smooth muscle tumors. J Clin ?athol 1983;36:57--61.
44. Tsushima K. Stanhope CR, Gaffey T A. Lieber MM. Uterine leiomyosarcomas and benign smooth muscle tumors: u efulness of nuclear DNA patterns studied by flow cytometry. Mayo Clin Proc 1988;63:248-55.
\ I