Embed Size (px)
Citation preview

Case ReportA Retroperitoneal Leiomyosarcoma Presenting as an AdrenalIncidentaloma in a Subject on Warfarin
Ishrat N. Khan,1 Mohamed A. Adlan,1
Michael J. Stechman,2 and Lakdasa D. Premawardhana1,3
1Section of Endocrinology, Ysbyty Ystrad Fawr, Ystrad Fawr Way, Hengoed, Caerphilly CF82 7EP, UK2Department of Endocrine Surgery, University Hospital of Wales, Heath Park, Cardiff CF14 4XN, UK3Department of Endocrinology, University Hospital of Wales, Heath Park, Cardiff CF14 4XN, UK
Correspondence should be addressed to Lakdasa D. Premawardhana; [email protected]
Received 6 December 2014; Revised 15 April 2015; Accepted 16 April 2015
Academic Editor: Hidetoshi Ikeda
Copyright © 2015 Ishrat N. Khan et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Adrenal incidentalomas (AIs) are mostly benign and nonsecretory. Management algorithms lack sensitivity when assessingmalignant potential, although functional status is easier to assess. We present a subject whose AI was a retroperitonealleiomyosarcoma (RL). Case Presentation. A woman on warfarin with SLE and the antiphospholipid syndrome, presented with leftloin pain. She was normotensive and clinically normal. Ultrasound scans demonstrated left kidney scarring, but CT scans revealedan AI. MRI scans later confirmed the AI without significant fat and no interval growth. Cortisol after 1mg dexamethasone, urinaryfree cortisol and catecholamines, plasma aldosterone renin ratio, and 17-hydroxyprogesterone were within the reference range.Initially, adrenal haemorrhage was diagnosed because of warfarin therapy and the acute presentation. However, she underwentadrenalectomy because of interval growth of the AI. Histology confirmed an RL. The patient received adjuvant radiotherapy.Discussion. Our subject presented with an NSAI. However, we highlight the following: (a) the diagnosis of adrenal haemorrhage inthis anticoagulated woman was revised because of interval growth; (b) the tumour, an RL, was relatively small at diagnosis; (c) thissubject has survived well over 60 months despite an RL perhaps because of her acute presentation and early diagnosis of a smalllocalised tumour.
1. Introduction
Adrenal incidentalomas (AIs) are a modern phenomenon [1]and several algorithms are available for theirmanagement [2–4]. Cliniciansmanaging anAI have two decisions tomake: (a)is it secretory and (b) is it malignant? Surgical interventionis indicated if clinical, laboratory, or radiological features ofeither or both are present. The functional status of AI isrelatively straightforward to assess. If nonsecretory adrenalincidentalomas (NSAI) do not fulfil size and radiologicalcriteria [5], a “wait and see” policy with interval scanning isrecommended. Such a policy is not fail safe and may occa-sionally lead to undesirable outcomes. This is particularly sowhen the patient has comorbidities and is on drugs whichmay contribute to diagnostic confusion.
AIs are usually benign and nonsecretory [2]. The currentguidelines for surgery for NSAI are based on tumour size and
appearance on CT scanning (MRI or PET if used) (Table 1).For NSAI that do not fulfil size criteria at presentation,features such as increasing size and an unfavourable imaging“phenotype” may indicate the need for surgery [6]. The lipidcontent of benign NSAI is high and CT “attenuation” valuesare significantly lower than that for adrenal carcinomas,metastases, or pheochromocytomas [7]. Noncontrasted CTattenuation values of <10 HU are typical of benign lesions,but lipid poor benign NSAI (10–40% of benign adenomas)may occasionally showhigher values. Contrast washout tendsto be lower (<40%) in carcinomas compared to benignadenomas. Furthermore, malignant lesions may demonstratelocal invasion, necrosis, heterogeneous appearances, irreg-ular borders, and regional lymphadenopathy [8]. However,neither tumour size nor the imaging “phenotype” is sensitiveenough to differentiate between benign andmalignant lesionsin every patient [9]. These appearances may be distorted
Hindawi Publishing CorporationCase Reports in EndocrinologyVolume 2015, Article ID 830814, 4 pageshttp://dx.doi.org/10.1155/2015/830814

2 Case Reports in Endocrinology
Table 1: Adrenal imaging modalities and their utility.
Scan type Diagnostic characteristics CommentsContrast enhancedultrasound
Arterial enhancement and rapid washout seen innonadenomatous lesions Not commonly used
Unenhanced CT scan(a) Presence of macroscopic fat seen in myelolipoma(b) Attenuation of less than 10 Hounsfield units (HU) seenin benign adrenal adenomas
Commonly used scan mode but 30–40%benign lesions are lipid poor
Multiphase CT (a) Rapid washout, benign lesions(b) Slower washout, malignant lesions Useful when unenhanced CT is equivocal
MRI Chemical shift imaging is helpful in differentiating betweenlipid poor adenomas and malignant adrenal lesions
Helpful when CT is contraindicated orwashout values are equivocal
Positron emission tomography(PET) and PET-CT
Differentiate benign from malignant lesions with highsensitivity and specificity
Combine HU measurement withfunctional activity
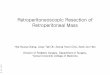
Figure 1: A CT scan of the abdomen showing a well encapsulated“adrenal” mass (solid white arrow).
particularly in subjects who have had a haemorrhage into thelesion, either spontaneously or complicating anticoagulanttherapy. Rarely NSAIs are malignant, primary or metastatic(renal, lung, gastrointestinal, and bladder). Leiomyosarcomaspresenting as NSAI are very uncommon.
We present a subject who had a very rare high-graderetroperitoneal leiomyosarcoma (RL) presenting as an NSAI.She also had the antiphospholipid syndrome and was onwarfarin therapy.
2. Case Presentation
A 40-year-old woman with SLE and the antiphospholipidsyndrome presented acutely with sudden onset left sided loinpain. She was on life-longwarfarin therapy formultiple DVTsand pulmonary emboli and hydroxychloroquine. Ultrasoundscans showed a 10mm focal area in the left kidney dueto scarring or a small angiomyolipoma. A CT scan severalmonths later showed a 2.7× 3.9 cm left adrenal incidentaloma(Figure 1), and she was referred to the endocrine clinic.
On examination, she was normotensive and had noclinical signs of endocrinopathy. Investigations includingcortisol after 1 mg dexamethasone suppression overnight,urinary free cortisol (twice), urinary catecholamines (twice),aldosterone renin ratio, 17-hydroxyprogesterone, and chro-mogranins were all within the reference range. MRI scans
Figure 2: Microscopic appearances of the leiomyosarcoma on theright (solid white arrow) and normal adrenal gland on the left(haematoxylin and eosin staining). The cells were strongly positivefor smooth muscle actin and desmin on immunostaining (notshown).
showed a solid left adrenal lesion measuring 2.4 × 4 cm.without significant fat and no interval growth. However, inview of the phenotype and size of the adrenal mass she wasreferred to the endocrine surgeons. Following a review of herhistory of loin pain, and imaging, it was decided that she had alikely benign NSAI (uniform soft tissue signal intensity, well-defined margins, no local invasion, appropriate size, and nointerval growth over 3 months), who may have developedacute symptoms as a result of haemorrhage into the lesion.Therefore a conservative approach was adopted with scans tobe repeated in 3–6 months. Although the size of the lesioninitially remained stable, imaging one year later revealed thatit had increased in size to 3 × 5.4 cm. The patient thereforehad left laparoscopic adrenalectomy. At surgery, there was nomacroscopic invasion of adjacent structures and the lesionwas excised with periadrenal fat.
Histology revealed a nonencapsulated high-grade leiom-yosarcoma thought to have arisen from connective tissue butseparate from the adrenal gland, that is, a retroperitonealleiomyosarcoma (RL).There were atypical pleomorphic spin-dle cells forming a herringbone pattern in areas (Figure 2).These cells had cigar shaped nuclei with some multinucle-ated forms. Immunostaining revealed strong expression of

Case Reports in Endocrinology 3
smooth muscle actin and desmin. There was no AE1/AE3,S100, CD117, CD34, or CD99 expression. Proliferation frac-tion on Ki67 immunostaining was approximately 30%. Stag-ing CT confirmed only localised disease. She had radiother-apy as recommended by the Sarcoma MDT.
3. Discussion
We have described a 40-year-old woman who presented withwhat appeared to be a benign NSAI. It was later confirmedthat the “NSAI” was actually an RL and separate from theadrenal gland. As far as we are aware, this is the first reportof an RL presenting as an AI. Retroperitoneal sarcomas arerare and RL evenmore so [10].They are largely asymptomaticand therefore grow to a large size before presentation—50%are more than 15 cm in diameter. They have a very poorprognosis. Their large size and spread to surrounding struc-tures at presentation, and technical difficulties in surgicalremoval, contribute to this poor prognosis [11]. RL usuallyarises from the walls of retroperitoneal veins most often fromthe inferior vena cava and shows no gender disparity. Radicalsurgery followed by radiotherapy and/or chemotherapy isrecommended.
The management of our subject was complicated by herdrug therapy and the nonspecific appearances on imaging.It is noteworthy that her initial abdominal ultrasound scanwas reported to show renal scarring or an angiomyolipomaof the kidney, both benign entities. An AI was only identifiedlater on CT scanning. Endocrine assessment at this stageconfirmed it to be an NSAI, but despite a lack of intervalgrowth, it was felt, on size criteria and a paucity of fat in thelesion on imaging, that surgery should be considered [12].Thecombination of her acute presentation with loin pain on thesame side as the lesion, the absence of worrying radiologicalappearances at that stage, and the inherent risk of surgeryin an anticoagulated woman with the antiphospholipid syn-drome pushed the balance of risks away from immediatesurgery. However, interval growth of the mass during follow-up required a reevaluation of the diagnosis so that urgentresection was pursued.
In conclusion, we would like to highlight the following.
(a) The diagnosis of an adrenal bleed in this anticoagu-lated woman was revised because of interval growthof the mass.
(b) This growth was only detectable 1 year after firstevaluation. Lack of early interval growth does notexclude a malignant lesion in every subject; we sup-port repeating initial negative scans as recommendedin recent algorithms [7].
(c) Surgery should be considered for 4 cm diameter AIsshowing an appropriate noncontrast CT phenotype.
(d) While primary adrenal leiomyosarcomas are very rare(only 20 cases reported so far), RL may very rarelypresent as an NSAI.
(e) This tumour was relatively small compared to typicalRLs described in the literature—50%more than 15 cmin diameter. This was most likely because of her acute
presentation with loin pain, which prompted imagingwhich led to an earlier diagnosis.
(f) This subject has survived for well over 60 monthsdespite a high-grademalignant RL perhaps because ofearly detection and a small localised tumour, resultingfrom her acute presentation.
Conflict of Interests
All authors certify that there is no conflict of interests(financial or other) to declare.
Authors’ Contribution
I. N. Khan and L. D. Premawardhana collected the data andI. N. Khan, M. A. Adlan, M. J. Stechman, and L. D. Prem-awardhana contributed to final review and the writing of thispaper.
References
[1] D. C. Aron, “The adrenal incidentaloma: a disease of moderntechnology and a public health problem,” Reviews in Endocrineand Metabolic Disorders, vol. 2, no. 3, pp. 335–342, 2001.
[2] G. Arnaldi and M. Boscaro, “Adrenal incidentaloma,” BestPractice & Research: Clinical Endocrinology & Metabolism, vol.26, no. 4, pp. 405–419, 2012.
[3] G. Kaltsas, A. Chrisoulidou, G. Piaditis, E. Kassi, and G.Chrousos, “Current status and controversies in adrenal inciden-talomas,” Trends in Endocrinology and Metabolism, vol. 23, no.12, pp. 602–609, 2012.
[4] L. K. Nieman, “Approach to the patient with an adrenalincidentaloma,” Journal of Clinical Endocrinology&Metabolism,vol. 95, no. 9, pp. 4106–4113, 2010.
[5] Italian Association of Clinical Endocrinologists, “AME positionstatement on adrenal incidentalomas,” European Journal ofEndocrinology, vol. 164, pp. 851–870, 2011.
[6] A. Reginelli, G. diGrezia, A. Izzo et al., “Imaging of adrenal inci-dentaloma: our experience,” International Journal of Surgery,vol. 12, pp. S126–S131, 2014.
[7] S. Kannan, E. M. Remer, and A. H. Hamrahian, “Evaluationof patients with adrenal incidentalomas,” Current Opinion inEndocrinology, Diabetes and Obesity, vol. 20, no. 3, pp. 161–169,2013.
[8] J. G. Bittner IV and L. M. Brunt, “Evaluation and managementof adrenal incidentaloma,” Journal of Surgical Oncology, vol. 106,no. 5, pp. 557–564, 2012.
[9] T. J. Cawood, P. J. Hunt, D. O’Shea, D. Cole, and S. Soule, “Rec-ommended evaluation of adrenal incidentalomas is costly, hashigh false-positive rates and confers a risk of fatal cancer thatis similar to the risk of the adrenal lesion becoming malignant;time for a rethink?” European Journal of Endocrinology, vol. 161,no. 4, pp. 513–527, 2009.
[10] T. Shiraev, S. S. Pasricha, P. Choong et al., “Retroperitonealsarcomas: a review of disease spectrum, radiological features,characterisation and management,” Journal of Medical Imagingand Radiation Oncology, vol. 57, no. 6, pp. 687–700, 2013.
[11] W. D. Craig, J. C. Fanburg-Smith, L. R. Henry, R. Guerrero, andJ. H. Barton, “Fat-containing lesions of the retroperitoneum:

4 Case Reports in Endocrinology
radiologic-pathologic correlation,” RadioGraphics, vol. 29, no. 1,pp. 261–290, 2009.
[12] B. K. Lack, C. W. Q. Graham, P. Bitterman, B. J. Rusnock, B.W. O’Brien, and J. H. Lynch, “Primary leiomyosarcoma of theadrenal gland. Case report with immunohistochemical andultrastructural study,”The American Journal of Surgical Pathol-ogy, vol. 15, no. 9, pp. 899–905, 1991.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com