Embed Size (px)
Citation preview

Abstract A case of late sciatic nerve palsy followingavulsion of the biceps femoris muscle from the ischialtuberosity in a 27-year-old athlete is reported.
Introduction
Avulsion fracture of the ischial tuberosity in adolescents,due to sudden strong contractions of the hamstring mus-cles, is a well-recognized clinical entity [4]. However,rupture of the hamstring muscles from the ischial tuberos-ity without fracture is uncommon [2, 6, 8, 9]. We reporthere a case of late sciatic nerve paralysis following rup-ture of the long head of the biceps femoris muscle fromthe ischial tuberosity. No similar case has been reported inthe literature to our knowledge.
Case report
A 27-year-old athlete felt a sharp pain in his right buttock whilelong jumping. The patient lost his balance and landed on his rightleg. His right hip was forcibly flexed, while his right knee wasfixed in full extension. The pain gradually disappeared and within2 weeks he resumed running. Five months after the injury he no-ticed “tingling” in the right foot for the first time. During the fol-lowing month, the tingling sensation extended to his leg and thepatient noticed that he could not dorsiflex the right ankle. Exami-nation at 8 months postinjury revealed paralysis of the sciaticnerve. The movements lost were extension of the ankle and toes(Fig. 1). Hypoesthesia was found on the outer side of the leg andthe entire foot except for the instep. Muscle testing was graded:right hamstrings 5, gastrocnemius 4, tibialis posterior 2, tibialis an-terior 0, peroneus 0, extensor hallucis longus 0, and extensor digi-torum longus 0. There was a palpable defect on the area distal fromthe right ischial tuberosity. A firm mass was palpable on the pos-terior surface of the upper third of the thigh. The mass stood outprominently when the leg was flexed (Fig.2). Normal outline ofthe medial hamstring muscles was visible. There was a positive
Tinel’s sign over the sciatic nerve several centimeters distal to theinfragluteal crease. Roentgenograms showed no abnormality of theright ischial tuberosity.
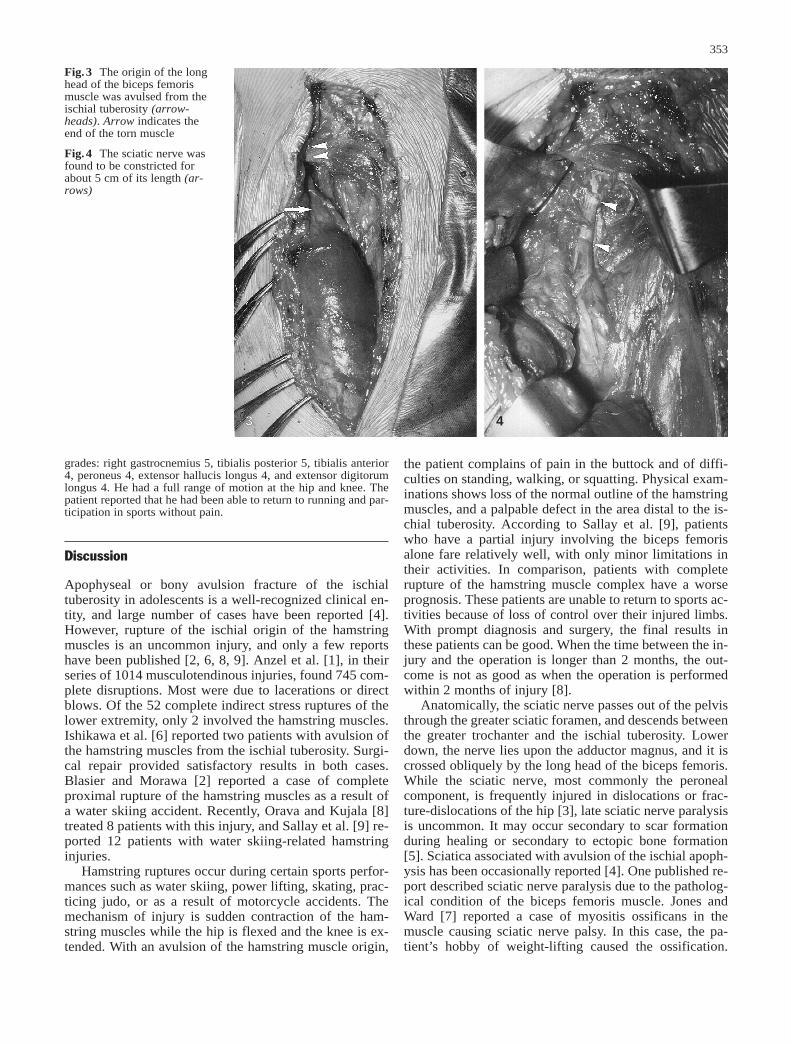
At surgery, the sciatic nerve was dissected out at the proximalpart of the thigh. The long head of the biceps femoris was found tobe ruptured completely near the proximal attachment (Fig. 3). Thefemoral origin of the biceps femoris was uninjured. There was anenormous mass of scar tissue around the torn ends of the muscle.This entrapped the sciatic nerve, causing compression. The nervewas found to be constricted for about 5 cm of its length (Fig. 4).Satisfactory neurolysis was achieved by total excision of the scartissue. The torn muscle was not repaired.
Postoperatively, the area of hypoesthesia gradually decreased.Seven months after the operation, the tibialis anterior began tocontract voluntarily. At 15 months after the neurolysis, the patientwas able to extend the ankle forcibly. He had slight hypoesthesiaover the distal right foot. Muscle testing yielded the following
Hiroshi Takami · Sadao Takahashi · Masashi Ando
Late sciatic nerve palsy following avulsion of the biceps femoris muscle from the ischial tuberosity
Arch Orthop Trauma Surg (2000) 120 :352–354 © Springer-Verlag 2000
Received: 3 September 1997
CURRENT PROBLEM CASE
H. Takami (Y) · S. Takahashi · M. AndoSection of Orthopaedic Surgery, Kanto Rosai Hospital, Nakahara-ku, Kawasaki, Japan Tel.: +81-44-4113131, Fax: +81-44-4333150
Fig.1 Drop foot deformity on admission
Fig.2 A firm mass was palpable on the posterior surface of theupper third of the right thigh. The mass (arrow) stood out promi-nently when the leg was flexed
1
2
grades: right gastrocnemius 5, tibialis posterior 5, tibialis anterior4, peroneus 4, extensor hallucis longus 4, and extensor digitorumlongus 4. He had a full range of motion at the hip and knee. Thepatient reported that he had been able to return to running and par-ticipation in sports without pain.
Discussion
Apophyseal or bony avulsion fracture of the ischialtuberosity in adolescents is a well-recognized clinical en-tity, and large number of cases have been reported [4].However, rupture of the ischial origin of the hamstringmuscles is an uncommon injury, and only a few reportshave been published [2, 6, 8, 9]. Anzel et al. [1], in theirseries of 1014 musculotendinous injuries, found 745 com-plete disruptions. Most were due to lacerations or directblows. Of the 52 complete indirect stress ruptures of thelower extremity, only 2 involved the hamstring muscles.Ishikawa et al. [6] reported two patients with avulsion ofthe hamstring muscles from the ischial tuberosity. Surgi-cal repair provided satisfactory results in both cases.Blasier and Morawa [2] reported a case of completeproximal rupture of the hamstring muscles as a result ofa water skiing accident. Recently, Orava and Kujala [8]treated 8 patients with this injury, and Sallay et al. [9] re-ported 12 patients with water skiing-related hamstringinjuries.
Hamstring ruptures occur during certain sports perfor-mances such as water skiing, power lifting, skating, prac-ticing judo, or as a result of motorcycle accidents. Themechanism of injury is sudden contraction of the ham-string muscles while the hip is flexed and the knee is ex-tended. With an avulsion of the hamstring muscle origin,
the patient complains of pain in the buttock and of diffi-culties on standing, walking, or squatting. Physical exam-inations shows loss of the normal outline of the hamstringmuscles, and a palpable defect in the area distal to the is-chial tuberosity. According to Sallay et al. [9], patientswho have a partial injury involving the biceps femorisalone fare relatively well, with only minor limitations intheir activities. In comparison, patients with completerupture of the hamstring muscle complex have a worseprognosis. These patients are unable to return to sports ac-tivities because of loss of control over their injured limbs.With prompt diagnosis and surgery, the final results inthese patients can be good. When the time between the in-jury and the operation is longer than 2 months, the out-come is not as good as when the operation is performedwithin 2 months of injury [8].
Anatomically, the sciatic nerve passes out of the pelvisthrough the greater sciatic foramen, and descends betweenthe greater trochanter and the ischial tuberosity. Lowerdown, the nerve lies upon the adductor magnus, and it iscrossed obliquely by the long head of the biceps femoris.While the sciatic nerve, most commonly the peronealcomponent, is frequently injured in dislocations or frac-ture-dislocations of the hip [3], late sciatic nerve paralysisis uncommon. It may occur secondary to scar formationduring healing or secondary to ectopic bone formation[5]. Sciatica associated with avulsion of the ischial apoph-ysis has been occasionally reported [4]. One published re-port described sciatic nerve paralysis due to the patholog-ical condition of the biceps femoris muscle. Jones andWard [7] reported a case of myositis ossificans in themuscle causing sciatic nerve palsy. In this case, the pa-tient’s hobby of weight-lifting caused the ossification.
353
Fig.3 The origin of the longhead of the biceps femorismuscle was avulsed from theischial tuberosity (arrow-heads). Arrow indicates theend of the torn muscle
Fig.4 The sciatic nerve wasfound to be constricted forabout 5 cm of its length (ar-rows)
33 4

Two patients with rupture of the hamstring origin hadsymptoms of sciatica or irritation of the sciatic nerve. Inone case, the symptoms of sciatica resolved as theswelling diminished [9]. In the other case, sciatic painpersisted for 14 months after the injury [8].
In the case described here, the patient resumed athleticactivities within 2 weeks of the injury when the soft tissuehealing was immature. We postulate that too early, re-peated contractions of the biceps femoris muscle led toextensive scar tissue formation about the torn ends of themuscle. In this nerve entrapment, the involvement of theperoneal division was more severe than that of the tibialdivision. According to Sunderland [10], the funiculi aremore closely packed in the common peroneal than in thetibial nerve. The reduced amount of protective connectivetissue packing in the former may contribute to the greatersusceptibility to compression as well as to the injury. Wedid not repair the torn biceps femoris muscle in thischronic case because the injury was partial, and thereforethe patient had normal hamstring function. The presentcase demonstrates that late sciatic nerve palsy occurs as acomplication of rupture of the biceps femoris muscle fromthe ischial tuberosity.
References
1.Anzel SH, Covey KW, Weiner AD, et al (1959) Disruption ofmuscles and tendons: an analysis of 1014 cases. Surgery 45 :406–414
2.Blasier RB, Morawa LG (1990) Complete rupture of the ham-string origin from a water skiing injury. Am J Sports Med 18 :435–437
3.Epstein HC (1974) Posterior fracture-dislocations of the hip:long-term follow-up. J Bone Joint Surg [Am] 56 :1103–1127
4.Hamada G, Rida A (1963) Ischial apophysiolysis (IAL): reportof a case and review of the literature. Clin Orthop 31 :117–130
5.Hirasawa Y, Oda R, Nakatani K (1977) Sciatic nerve paralysisin posterior dislocation of the hip: a case report. Clin Orthop126 :172–175
6. Ishikawa K, Kai K, Mizuta H (1988) Avulsion of the hamstringmuscles from the ischial tuberosity: a report of two cases. ClinOrthop 232 :153–155
7. Jones BV, Ward MW (1980) Myositis ossificans in the bicepsfemoris muscles causing sciatic nerve palsy: a case report. J Bone Joint Surg [Br] 62 :506–507
8.Orava S, Kujala UM (1995) Rupture of the ischial origin of thehamstring muscles. Am J Sports Med 23 :702–705
9.Sallay PI, Friedman RL, Coogan PG, et al (1996) Hamstringmuscle injuries among water skiers: functional outcome andprevention. Am J Sports Med 24 :130–136
10.Sunderland S (1968) Nerves and nerve injuries. Livingstone,Edinburgh
354





























