Embed Size (px)
Citation preview

CHAPTER I
INTRODUCTION
Worldwide more than 285 million people are affected by diabetes mellitus.
This number is expected to increase to 439 million by 2030 according to the
International Diabetes Federation.1
A cataract is present when the transparency of the lens is reduced to the
point that the patient’s vision is impaired. The term cataract comes from the Greek
word katarraktes (downrushing; waterfall) because earlier it was thought that the
cataract was a congealed fluid from the brain that had flowed in front of the lens.
Cataract is considered a major cause of visual impairment in diabetic patients as
the incidence and progression of cataract is elevated in patients with diabetes
mellitus. The association between diabetes and cataract formation has been shown
in clinical epidemiological and basic research studies. Due to increasing numbers
of type 1 and type 2 diabetics worldwide, the incidence of diabetic cataracts
steadily rises. Even though cataract surgery, the most common surgical
ophthalmic procedure worldwide, is an effective cure, the elucidation of
pathomechanisms to delay or prevent the development of cataract in diabetic
patients remains a challenge. Furthermore, patients with diabetes mellitus have
higher complication rates from cataract surgery. Both diabetes and cataract pose
an enormous health and economic burden, particularly in developing countries,
where diabetes treatment is insufficient and cataract surgery often inaccessible.2

CHAPTER II
LITERATURE REVIEW
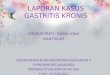
1.1. Anatomy and Physiology of the Lens
The lens is one of the essential refractive media of the eye and focuses
incident rays of light on the retina. It adds a variable element to the eye’s total
refractive power (10 – 20 diopters, depending on individual accommodation) to
the fixed refractive power of the cornea (approximately 43 diopters).
The fully developed lens is a biconvex, transparent structure. The curvature
of the posterior surface, which has a radius of 6 mm, is greater than that of the
anterior surface, which has a radius of 10 mm. The lens is approximately 4 mm
thick , and its weight increases with age to five times its weight at birth. An adult
lens weighs about 220 mg.
The lens lies in the posterior chamber of the eye between the posterior
surface of the iris and the vitreous body in a saucer-shape d depression of the
vitreous body known as the hyaloid fossa. Together with the iris it forms an
optical diaphragm that separates the anterior and posterior chambers of the eye.
Radially arranged zonule fibers that insert into the lens around its equator connect
the lens to the ciliary body. These fibers hold the lens in position and transfer the
tensile force of the ciliary muscle
Pict 1. Anatomy of the lens

1.2. Definition of Cataract
Cataract is a opacity of the lens of the eye, which occurs when fluid gathers
between the lens fibres. The refractive index alters and causes light scatter with
resultant blurred vision.. These zones of opacity may be subcapsular, cortical, or
nuclear and may be anterior or posterior in location. In addition to of the nucleus
and cortex, there may be a yellow or amber color change to the lens. A cataract
also can be described in terms of its stage of development. A cataract with a clear
cortex remaining is immature. A mature cataract has a totally opacified cortex.
Picture 2. Lens in Cataract
1.3. Epidemiology
In 2002, the World Health Organization calculated that the number of
visually impaired people worldwide was in excess of 161 million. Cataract is the
leading cause, accounting for 47.8% of all cases. The estimated global costs of
blindness and low vision in 2000 was estimated at US$42 billion. There are also
hidden costs of cataract blindness. Each person who is blind requires a caregiver,
placing demands on one tenth of their time so reducing their economic activity.
Over the next 20 years it is estimated that the world’s population will increase by
about one third, this growth occurring predominantly in developing countries.
During the same period, the number of people over the age of 65 years will more
than double. Therefore, there will be approximate doubling in the incidence of
cataract, visual morbidity, and need for cataract surgery. But questions remain,
such as, how much cataract is enough to warrant surgery, how should it be
performed and delivered, and how should it be paid for? In the developed world,
the threshold for cataract surgery is now 20/30 (6/9) or less, which has resulted in
a three- to fourfold increase in patients receiving surgery with an associated
increased need for resources and funding. The challenge is to determine at what

visual acuity level a government or insurer should pay for surgery, and how to
allocate resources appropriately.
1.4. Etiology
Cataract can be caused by many etiology that have manifestation in opacity
in lens, such as:
a. Age
b. Trauma
c. Systemic disorders (diabetes, galaktosemia)
d. Ocular diseases
e. Toxic causes (steroid, anticholinesterase)
f. Congenital (dominant, sporadic or part of a syndrome, abnormal
galactose metabolism, hypoglycaemia)
g. Associated with inherited abnormality (myotonic dystrophy,
h. Central nervous system disorders
1.5. Symptoms
Development of the cataract and its symptoms is generally an occult
process. Patients experience the various symptoms such as seeing only shades of
gray, visual impairment, blurred vision, distorted vision, glare or star bursts,
monocular diplopia, altered color perception, etc. to varying degrees, and these
symptoms will vary with the specific type of cataract.

Picture 3. Symptom Cataract
1.6. Classification
Cataracts may be classified according to time of occurence and maturity.
From classified by time, there are acquired cataract (senile cataract, cataract with
systemic disease, secondary and complicated cataract, traumatic and toxic
cataract) that cause 99% etiology of cataract and congenital cataract thta less than
1% of all cataract etiology.
a. Senile cataract
In the fourth decade of life, the pressure of peripheral lens fiber
production causes hardening of the entire lens, especially t he nucleus. The

nucleus takes on a yellowish brown color (brunescent nuclear cataract).This
may range from re ddish brown to nearly black discoloration of the entire
lens (black cataract). Because they increase t he refractive power of t he
lens, nuclear cataracts lead to lenticular myopia and occasionally produce a
second focal point in the lens with resulting monocular diplopia.
Nuclear cataracts are of ten associate d with changes in the lens cortex. It is
interesting to note that patients with cortical cataracts tend to have acquired
hyperopia in contrast to patients with nuclear cataracts, who tend to be
myopic.
b. Cataract with systemic disease
Diabetic cataract. The typical diabetic cataract is rare in young diabetic
patients. Transient metabolic decompensation promotes the occurrence of a
typical radial snowflake pattern of cortical opacities (snowflake cataract).
Transient hyperopia and myopia can occur. Diabetic cataract progresses
rapidly. Senile cataracts are observed about five times as often in older
diabetics as in patients the same age with normal metabolism. These
cataracts usually also occur two to three years earlier.
Galactosemic cataract. This deep posterior cortical opacity begins after
birth. Galactosemia is a rare cause of early cataract in children lacking an
enzyme required to metabolize galactose. The newborn receives ample
amounts of galactose in the mother’s milk . Due a lack of uridyl transferase,
or less frequently galactokinase, galactose cannot be metabolized to glucose,
and the body becomes inundated with galactose or with galactose and
galactose-1-phosphate. If the disorder is diagnosed promptly and the child is
maintained on a galactose-free diet, the opacities of the first few week s of
life will be reversible. Galactosemic cataract is the only form of cataract that
responds to conservative therapy.
Dialysis cataract. Hemodialysis to eliminate metabolic acidosis in renal
insufficiency can disturb the osmotic equilibrium of lens metabolism and
cause swelling of t he cortex of the lens.

Cataract with myotonic dystrophy. Opacities f irst occur between the ages
of 30 and 50, initially in a thin layer of the anterior cortex and later also in
the subcapsular posterior cortex in the form of rosettes. Detecting these
opacities is important for differential diagnosis as cataracts do not occur in
Thomsen’s disease (myotonia congenita) or Erb’s progressive muscular
dystrophy. Symptoms that confirm the diagnosis include cataract, active
signs of myotonia (delayed opening of the f ist), and passive signs of
myotonia (decreased relaxation of muscles in the extremities following
direct percussion of the muscle and absence of reflexes).
Tetany cataract. The opacity lies within a broad zone inferior to the
anterior lens capsule and consists of a series of gray punctate lesions.
Symptoms that confirm the diagnosis include low blood calcium levels, a
positive hyperventi-lation test, and signs of tetany: positive Chvostek,
Trousseau, and Erb signs.
Dermatogenous cataract. This may occur with chronic neurodermatitis, less
frequently with other skin disorders s uch as scleroderma, poikiloderma,and
chromic eczema. Characteristic signs include an anterior c rest-shaped
thickening of the protruding center of the capsule.
c. Complicated Cataracts
This form of cataract can occur as a complication of any protracted
intraocular inflammation, especially heterochromia, chronic iridocyclitis,
retinal vasculitis, and retinitis pigmentosa. The result is a pumice-like
posterior subcapsular cataract that progresses axially toward the nucleus.
This form of cataract produces extreme light scattering.
d. Cataract after Surgery
Cataracts usually develop earlier in the operated eye as compared to
the opposite, non-operated eye after intraocular surgery. This applies
especially to f iltering operations. A secondar y cataract will generally occur
following vitrectomy and silicone oil tamponade.
e. Traumatic Cataract

The incidence of these lens opacities is higher in men than in women due to
occupational and sports injuries.
Contusion cataract: Contusion of t he eyeball will produce a rosette-
shaped subcapsular opacity on the anterior surface of the lens. I t will
normally remain unchanged but will migrate into the deeper cortex over
time due to the apposition of new fibers
Infrared radiation cataract (glassblower’s cataract): This type of cataract
occurs af ter decades of prolonged exposure to the infrared radiation of fire
without eye protection. Characteristic findings include splitting of the
anterior lens capsule, whose edges will be observed to curl up and float in
the anterior chamber. Occupational safety regulations have drastically
reduced the incidence of t his t ype of cataract.
Picture 4. Radiation on eye
Electrical injury: This dense subcapsular cataract can be caused by
lightning or high-voltage electrical shock.
Then classified by maturity, there are insipient cataract, immature cataract,
mature cataract, and hypermature cataract.
a. Insipient Cataract

In this stadium opacity start from marginal equator to anterior and
posterior cortex. This opacity can arised poliopia because refraction index is
not same in the all of lens.
b. Immature Cataract
Opacity at a part of lens. In this stadium lens volume will increase that
is caused by increased of osmotic pressure. Subsequently, lens become more
convex and can block the flow of aqueous humor and finally result on
secondary glaucoma.
Picture 5. Immature cataract
c. Mature Cataract
Opacity can found in all of lens. This opacity can occur because there
is calcium depotitions in the lens. Fluid in the lens will remove out so that
lens will back at normal size, anterior chambers back at normal depth and
there isn’t iris image at the opaque lens so shadow test is negative.
Picture 6. Mature Cataract
d. Hipermature Cataract

If a mature cataract progresses to the point of complete liquification of
the cortex, the dense brown nucleus will subside within the capsule. Its
superior margin will then be visible in the pupil as a dark brown silhouette
against the surrounding grayish white cortex. The pressure in the lens
capsule decreases. The contents of the limp and wrinkled capsular bag
gravitate within the capsule. This condition, referred to as Morgagni’s
cataract , is the final stage in a cataract that has usually develope d over the
course of two decades.
Picture 7. Hypermature Cataract
1.7. Pathogenesis of Diabetic Cataract
The enzyme aldose reductase (AR) catalyzes the reduction of glucose to
sorbitol through the polyol pathway, a process linked to the development of
diabetic cataract. Extensive research has focused on the central role of the AR
pathway as the initiating factor in diabetic cataract formation.
It has been shown that the intracellular accumulation of sorbitol leads to
osmotic changes resulting in hydropic lens fibers that degenerate and form sugar
cataracts. In the lens, sorbitol is produced faster than it is converted to fructose by
the enzyme sorbitol dehydrogenase. In addition, the polar character of sorbitol
prevents its intracellular removal through diffusion. The increased accumulation
of sorbitol creates a hyperosmotic effect that results in an infusion of fluid to
countervail the osmotic gradient. Animal studies have shown that the intracellular
accumulation of polyols leads to a collapse and liquefaction of lens fibers, which
ultimately results in the formation of lens opacities. These findings have led to the

“Osmotic Hypothesis” of sugar cataract formation, emphasizing that the
intracellular increase of fluid in response to AR-mediated accumulation of polyols
results in lens swelling associated with complex biochemical changes ultimately
leading to cataract formation.
Furthermore, studies have shown that osmotic stress in the lens caused by
sorbitol accumulation induces apoptosis in lens epithelial cells (LEC) leading to
the development of cataract. Transgenic hyperglycemic mice overexpressing AR
and phospholipase D (PLD) genes became susceptible to develop diabetic cataract
in contrast to diabetic mice overexpressing PLD alone, an enzyme with key
functions in the osmoregulation of the lens. These findings show that impairments
in the osmoregulation may render the lens susceptible to even small increases of
AR-mediated osmotic stress, potentially leading to progressive cataract formation.
The role of osmotic stress is particularly important for the rapid cataract
formation in young patients with type 1 diabetes mellitus due to the extensive
swelling of cortical lens fibers. A study performed by Oishi et al. investigated
whether AR is linked to the development of adult diabetic cataracts. Levels of AR
in red blood cells of patients under 60 years of age with a short duration of
diabetes were positively correlated with the prevalence of posterior subcapsular
cataracts. A negative correlation has been shown in diabetic patients between the
amount of AR in erythrocytes and the density of lens epithelial cells, which are
known to be decreased in diabetics compared to nondiabetics suggesting a
potential role of AR in this pathomechanism.
The polyol pathway has been described as the primary mediator of diabetes-
induced oxidative stress in the lens. Osmotic stress caused by the accumulation of
sorbitol induces stress in the endoplasmic reticulum (ER), the principal site of
protein synthesis, ultimately leading to the generation of free radicals. ER stress
may also result from fluctuations of glucose levels initiating an unfolded protein
response (UPR) that generates reactive oxygen species (ROS) and causes
oxidative stress damage to lens fibers. There are numerous recent publications that
describe oxidative stress damage to lens fibers by free radical scavengers in
diabetics. However, there is no evidence that these free radicals initiate the

process of cataract formation but rather accelerate and aggravate its development.
Hydrogen peroxide (H2O2) is elevated in the aqueous humor of diabetics and
induces the generation of hydroxyl radicals (OH–) after entering the lens through
processes described as Fenton reactions. The free radical nitric oxide (NO),
another factor elevated in the diabetic lens and in the aqueous humor, may lead to
an increased peroxynitrite formation, which in turn induces cell damage due to its
oxidizing properties.
Furthermore, increased glucose levels in the aqueous humor may induce
glycation of lens proteins, a process resulting in the generation of superoxide
radicals () and in the formation of advanced glycation endproducts (AGE). By
interaction of AGE with cell surface receptors such as receptor for advanced
glycation endproducts in the epithelium of the lens further and H2O2 are
generated.
In addition to increased levels of free radicals, diabetic lenses show an
impaired antioxidant capacity, increasing their susceptibility to oxidative stress.
The loss of antioxidants is exacerbated by glycation and inactivation of lens
antioxidant enzymes like superoxide dismutases. Copper-zink superoxide
dismutase 1 (SOD1) is the most dominant superoxide dismutase isoenzyme in the
lens, which is important for the degradation of superoxide radicals () into
hydrogen peroxide (H2O2) and oxygen. The importance of SOD1 in the protection
against cataract development in the presence of diabetes mellitus has been shown
in various in vitro and in vivo animal studies.
In conclusion, a variety of publications support the hypothesis that the
initiating mechanism in diabetic cataract formation is the generation of polyols
from glucose by AR, which results in increased osmotic stress in the lens fibers
leading to their swelling and rupture.
1.8. Examination
a. Reduced Visual Acuity
A reduction in visual acuity can, of course, be an early sign of cataract
formation but this is not always the case. Some patients see surpris-ingly

well through marked lens opacities, and the effect on visual acuity as
measured by the Snellen test type depends as much on the pos-ition of the
opacities in the lens as on the density of the opacities.
b. Findings of Ophthalmoscopy
The best way of picking up a cataract in its early stages is to view the
pupil through the ophthal-moscope from a distance of about 50 cm. In this
way, the red reflex is clearly seen. The red reflex is simply the reflection of
light from the fundus. When using the ophthalmoscope, the opacities in the
lens are often seen as black spokes against the red reflex. It is important to
focus one’s eyes onto the plane of the patient’s pupil if the cataract is to be
well seen, and it is preferable to dilate the pupil beforehand or at least
examine in a darkened room. Typical age-related lens opacities are wedge-
shaped, pointing towards the centre of the pupil. At the same time, the
central nucleus of the lens can take on a yellowish-brown colour, the
appearance being termed “lens sclerosis”, and ultimately, the lens can
become nearly black in some instances.
Picture 8. Cataract in ofthalmoskop

1.9. Management
At the present time, there is no effective medical treatment for cataract.
Cataract extraction with the insertion of an intraocular lens is the treatment of
choice. Cataract extraction surgery can be divided into 2 form, that is
intracapsular cataract extraction and extracapsular cataract extraction.
Until the mid 1980s, intracapsular cataract extraction was the method of
choice. Today intracapsular cataract extraction is used only with subluxation or
dislocation of the lens. The entire lens is frozen in its capsule with a cryophake
and removed from the eye through a large superior corneal incision.
Picture 9. Intracapsular cataract extraction
Extracapsular cataract extraction with implantation of a posterior chamber
intraocular lens is now the method of choice. In this technique, the anterior
capsule is opened (capsulor rhexis). Then only the cortex and nucleus of the lens
are removed (extracapsular extraction); the posterior capsule and zonule
suspension remain intact. This provides a stable base for implantation of the
posterior chamber intraocular lens.

Picture 10. Extraocular Cataract Extraction
Today phacoemulsification (emulsifying and aspirating the nucleus of the
lens with a high-frequency ultrasonic needle) is the preferred technique for
removing the nucleus. Where the nucleus is very hard, the entire nucleus is
expressed or aspirated. Then the softer portions of the cortex are removed by
suction with an aspirator/ir rigator attachment in an aspiration/irrigation
maneuver. The posterior capsule is then polished, and an intraocular lens (IOL) is
implanted in the empty capsular bag. Phacoemulsification and IOL implantation
require an incision only 3 – 6 mm in length. Where a tunnel technique is used to
make this incision, no suture will be necessary as the wound will close itself.
Picture 11. Phacoemulsification surgery

CHAPTER III
CASE
1. Patient identity
Name : Mrs. M
Sex : Female
Age : 50 years old
Address : Jln Khatulistiwa Gg. Flora Batu Layang
Ethnic : -
Job : House wife
Religion : Islam
Patient was examined on April 8, 2014
2. Anamnesis
Main complaint :
Blur of vision in the right eye.
History of disease :
Patient came to opthalmologist with mayor complain blurred of vision in the
right eye from a year ago. At the first time, patient felt like there was cloudy in
his sight and then her vision become worse and more blurred than before.
Now, she claimed that her right eye cannot see everything properly. Patient
have had diabetes mellitus for two years and take the diabetic medication
routinely. There were no history of eye trauma and no complaint about pain in
the eyes. She did not consume any drug before to treat her eyes.
Past clinical history :
Patient claim that she has diabetes mellitus for two years and take the
diabetic medication routinely.
Family history :
She claim that no one of her family member has the eye symptom like her.
Her mother has diabetes mellitus also.

3. General Physical Assestment
General condition : good
Awareness : compos mentis, GCS= 15
Vital sign :
a. Blood Pressure : 140/90 mmHg
b. Heart rate : 68 x/ minute/ regular
c. RR : 18 x/minute
d. Temperature : 36,80 C
4. Ophthalmological status
Visual acuity :
a. OD : 1/60 good projection
b. OS : 6/6 f
OD OS
Ortho Eye ball position Ortho
Eye Movement
Movement (+), ptosis (-), lagoftalmos
(-), oedem(-)
Palpebra Movement (+), ptosis (-),
lagoftalmos (-), oedem (-)
redness (-), discharge (-), injection(-),
ulcer (-), foreign body (-)
Conjungtiva Redness (-), discharge (-), injection
(-), ulcer (-), foreign body (-)
Oedem (-), ulcer (-) Cornea Oedem (-), ulcer (-)
Clear, deep impression Anterior chamber Clear, deep impression
Iris colour : brown, direct light reflect
(+), indirect light refelct (+)
Circular pupil, isochore,
Iris/pupil Iris colour : brown, direct light
reflect (+), indirect light refelct (+)
Circular pupil, isochore,

Opacity (+) Lens Clear
Can not be described Vitreous Clear
Can not be described Fundus Optic disk and vaskular saw no
problem, there was not hemorragic
• Shadow test :
• OD : negatif
• OS : negatif
• Tonometri
• OD : normal (palpation)
• OS : normal (palpation)
• Eye field test (Confrontation test)
• OD : can not be examined
• OS : normal
5. Resume
Patient came to opthalmologist with mayor complain blurred of vision in
the right eye from a year ago. At the first time, patient felt like there was
cloudy in his sight and then her vision become worse and more blurred than
before. Now, she claimed that her right eye cannot see everything properly.
Patient have had diabetes mellitus for two years and take the diabetic
medication routinely. There were no history of eye trauma and no complaint
about pain in the eyes. She did not consume any drug before to treat her eyes.
In ophtalmology examination, visual acuity in the right eye is 1/60 with a
good projection and the left eye is 6/6 f. There is a high opacity on the right
eye and shadow test (-).
6. Diagnose
Working Diagnose:
OD : Diabetic cataract

OS : Normal
DDx:
OD : Senil Cataract, cataract traumatica, cataract complikata.
OS : -
7. Plan for examination
Hemotology,
Blood sugar in time, to know the etiology is diabetic or not
Routine hematology, bleding and cloting time to preparation surgery
Result:
Blood sugar in time: 220 ( Normal: 70-150)
Routine hematology : no result
8. Treatment
a.OD: Extracapsular cataract extraction with an implantation of posterior
chamber intraoculer lens.
b.OS: No treatment
9. Prognosis
OD:
a. Ad vitam : bonam
b. Ad functionam : dubia et bonam
c. Ad sanactionam : dubia et bonam
OS:
a. Ad vitam : bonam
b. Ad functionam : bonam
c. Ad sanactionam : bonam

CHAPTER IV
DISCUSSION
In this case Patient came to opthalmologist with mayor complain blurred
of vision in the right eye from a year ago. At the first time, patient felt like there
was cloudy in her sight and then her vision become worse and more blurred than
before. Now, she claimed that her right eye cannot see everything properly.
Patient have had diabetes mellitus for two years and take the diabetic medication
routinely. There were no history of eye trauma and no complaint about pain in the
eyes. She did not consume any drug before to treat her eyes. In ophtalmology
examination, visual acuity in the right eye is 1/60 with a good projection and the
left eye is 6/6 f. There is a high opacity on the right eye and shadow test (-).
From the data above, the diagnose for the right eye is mature cataract et
causa diabetes mellitus. This patient said that she has diabetes mellitus for two
years and began get the blurry in her right eye for the first time a year ago. This
diagnostic based on symptoms that patient had complaint with the same
characteristic with the symptoms of cataract such as: blurry vision with slowly
onset. In this case the most probably etiology is diabetes mellitus because she has
the diabetic history for 2 years, and she did not have traumatic history in the eyes
that can cause traumatic cataract or get radiation such as infrared or others.
From the examination, lens appeared opacity in all part of the lens. This
opacity can occur because there is ion calcium depositions in the lens. Opacity of
the lens will make disrupting the refraction media so the light can not focus to
retina, finally produce blurred vision. Vision slowly blurred because the
progression of lenses opacification (thickness of opacity influence the degree of
vision lost). Because of opacity of the lens, we can not see the fundus with
ofthalmoskop. This cataract classify to mature cataract because all of the lens was
clouded and from the shadow test is negatif that diffrent with immatur cataract.
From the result of laboratorium hematology test, patient had a bad control of
blood sugar, and has history for diabetes mellitus for 2 years, so cataract may
cause from diabetic mellitus she had.

The patogenesis of diabetic cataract is the enzyme aldose reductase (AR)
catalyzes the reduction of glucose to sorbitol through the polyol pathway, a
process linked to the development of diabetic cataract. Extensive research has
focused on the central role of the AR pathway as the initiating factor in diabetic
cataract formation.
It has been shown that the intracellular accumulation of sorbitol leads to
osmotic changes resulting in hydropic lens fibers that degenerate and form sugar
cataracts. In the lens, sorbitol is produced faster than it is converted to fructose by
the enzyme sorbitol dehydrogenase. In addition, the polar character of sorbitol
prevents its intracellular removal through diffusion. The increased accumulation
of sorbitol creates a hyperosmotic effect that results in an infusion of fluid to
countervail the osmotic gradient. Animal studies have shown that the intracellular
accumulation of polyols leads to a collapse and liquefaction of lens fibers, which
ultimately results in the formation of lens opacities. These findings have led to the
“Osmotic Hypothesis” of sugar cataract formation, emphasizing that the
intracellular increase of fluid in response to AR-mediated accumulation of polyols
results in lens swelling associated with complex biochemical changes ultimately
leading to cataract formation.
The treatment for the patient is surgery, becauase there was no effective
medical treatment for cataract. The definitive management for mature senile
cataract is lens extraction through surgery. The type of the surgery that
recommend for this patient is extracapsular cataract extraction (ECCE). we attend
to choose this type rather than intracapsular cataract extraction (ICCE) because
extracapsular cataract extraction maintains the integrity of the anterior and
posterior chambers of the eye, and the vitreous body cannot prolapse anterior as
after intracapsular cataract extraction. At 0.1 – 0.2 %, the incidence of retinal
detachment after extracapsular cataract extraction is about ten times less than after
intracapsular cataract extraction, which has an incidence of 2 – 3 %.
Prognosis cataract for patient after surgery may be good. Patient can see
clearly after removal the old lens and changed with syntetyc lens (Intra Ocular
Lens/ IOL). After surgery, eye’s patient had pseudofakhia from examination

ofthalmoskop. But then, because of the etiology for this case is diabetes mellitus,
the patient should control her blood sugar level in a good term to not make any
complication anymore.

CHAPTER V
CONCLUSION
From the case above, we can make a conclution about cataract are:
1. This patient suffer from diabetic cataract, because from the anamnesis and
examination it clearly pinpoint the cataract and also she has diabetes
mellitus for over 2 years.
2. A cataract is present when the transparency of the lens is reduced to the
point that the patient’s vision is impaired
3. Diagnostic of cataract based on anamnesis, examination, and laboratorium.
In anamnesis, we should to know abaout history of disease. In
examination, we have to see the opacity of lens and other examination. In
the laboratorium, we have to know abaut the etiology of cataract such as
diabetic that can see from blood sugar.
4. The efecctive tratment for catarac is surgery, there are many types of
surgery that can be used; extracapsular cataract extraction (ECCE) and
intracapsular cataract extraction (ICCE) but it was so rare to use nowdays.