-
Duty ReportAugust 11-17, 2014Consultants :dr. St. Finekri
Abidin, OBGYN (C)dr. Bintari Puspasari, OBGYNdr. T. Indang Dewi,
OBGYN (C)
RSGS Team August 2014
-
Reporting4 Caesarean sections
-
CAESAREAN SECTION #1
-
Day S OAP11/8/14DAY I22.15SCTPP
Mrs. Ella Sofhia, 41 yoMR. 129632
CC: Referred from RS Bersalin Pasutri with suspected severe
preeclampsia.
Patient admitted 9 month pregnancy. Her LMP 4/12/13 (unsured)
EDD 11/9/14~ 35-36 wga. ANC regularly at OBGYN (Bogor). USG at
every visit, baby in good condition.Contraction (-), water broke
(-), bloody show (-)
Blood pressure elevated since 2 months (140/90 mmHg), not given
drugs.Frontal headache (-), nausea / vomiting (-), blurred vision
(-)Active fetal movement
Menarche 12 yo, reguler, GP 3x/day, dysmenorrhea (-)
Married 1xObs history: G5P2A21999, boy 3800 g, spontaneous
delivery at RSPAD2007, miscarriage, curettage at RS Bogor2009, girl
3000 g, SC at RSPAD due to cord entanglement2011, miscarriage,
curettage at RS BogorThis pregnancyPhysical examinationCompos
mentis, BP : 170/100 mmHg, P: 86x/m, FR 20x/m, T : 36OCBB: 90 kg,
TB 169 cm: BMI 31.5 kg/m2Gen. state: Pale conjungtive -/-, abd ~
pregnancy
Obstetrical Status: FH 36 cm, head presentation, head 4/5, FHR
152I: V/U wnl Io: smooth portio, closed ostium, flr (-), flx
(-).Vt: portio firm, posterior, t 3cm, closed, H I
CTG: Category 1Lab:CBC (11/8/14)9.9/31/9200/182000SGOT 35 SGPT
20 Alb 3.6Ur 19 Cr 0.6 RBG 115Na 138 K 3.6 Cl 108Ul protein +2
US exam (7/7/14)Singleton live head presentation, placenta
implanted at fundus, normal implantationBPD 9,4/HC 36 / AC 37/ FL
7.4/ AFI normal/ EFW 4075G5P2A2 Term Pregnancy, singleton live
fetus, previous C-section 1x, superimposed preeclampsia, susp
macrosomia, not in labor
P: Observe hemodynamics, contractions, FHRObserve worsening of
preeclampsia
Emergency CSMgSO4Nifedipine 4 x 10 mgNAC 3 x 600 mg POVit C 2 x
400 mg IV
02.00 03.00LUS free of adhesionBorn baby boy, 4050 gr, 54 cm AS
8/9Clear amniotic fluidPlacenta born completely
FP : Tubectomy Pomeroy
Hb Post op: 9.8 g/dl
Outcome:Now patient (130/90 mmHg) and baby are in good
condition, already discharged
-
CAESAREAN SECTION #2
-
Day S OAP11/8/14DAY I14.00SCTPP
Mrs. Dwi Novianti, 33 yoMR. 242324
CC: irreguler contraction since 5 hours before admission
Patient admitted 9 months pregnancy. Her LMP 12/11/13 (unsure)
EDD 19/8/14~ 39 wga. ANC regularly at KesDip Tangerang then
referred to RSGS. USG 4x, baby in good condition.Contraction (-),
water broke (-), active fetal movement
Blood pressure elevated since previous pregnancy. In RSGS
policlinic patient got Methyldopa 3x500 mg and was already
consulted to internal medicine dept, already plan for elective
c-section at 18/8/2014
Frontal headache (-), nausea / vomiting (-), blurred vision
(-)
Menarche 12 yo, reguler, GP 3x/day, dysmenorrhea (-)
Married 1xObs history: G2P12005, SC at RSPAD due to breech
presentation, girl 2500 g.This pregnancyPhysical examinationCompos
mentis, BP : 160/110 mmHg, P: 84x/m, FR 18x/m, T : 36OCGen. state:
Pale conjungtive -/-, abd ~ pregnancy
Obstetrical Status : FH 30 cm, head presentation, head 4/5, FHR
146I: V/U wnl Io: smooth portio, closed ostium, flr (-), flx
(-).Vt: portio firm, posterior, t 3cm, closed, H I
CTG: Category 1Lab:CBC (11/8/14)10.7/32/14000/395000SGOT 16 SGPT
19 Alb 3.9Ur 19 Cr 0.6 RBG 83Na 140 K 3.9 Cl 106Ul protein +2
US exam (7/7/14)Singleton live head presentation, placenta
implanted at right corpus, normal implantationBPD 8.8/HC 314/ AC
330/ FL 76/ AFI 3.5 SP / EFW 3000G2P1 38 wga, singleton live fetus,
severe preeclampsia, previous CS 1x
P: Observe hemodynamics, contractions, FHRObserve worsening of
preeclampsia
Emergency CSMgSO4 Nifedipine 4 x 10 mgNAC 3 x 600 mg POVit C 2 x
400 mg IV
12/8/1414.30 15.30Anterior part of uterus was adhered to omentum
AdhesiolysisBorn baby girl, 2780 gr, 49 cm AS 8/9Clear amniotic
fluidPlacenta born completely
FP: IUD TC
Hb Post op: 11.8 g/dl
Outcome:Now patient (BP 130/90 mmHg) and baby are in good
condition, ready for rooming in
-
CAESAREAN SECTION #3
-
Day S OAP13/8/14DAY I15.00SCTPP
Mrs. Arum A, 31 yoMR. 419713
CC: irreguler contractions and bloody show since 1 day before
admission
Patient admitted 9 months pregnancy. Her LMP 10/11/13 EDD
17/8/14~ 39 wga. ANC regularly at RSGS. USG 3x, baby in good
condition. Planned for elective CS on 19/8/2014 due to
HbsAg(+)Water broke (-), active fetal movement
Menarche 13 yo, reguler, GP 2-3x/day, dysmenorrhea (-)
Married 1xObs history: G3P1A12008, miscarriage2011, girl 2600 g,
spontaneous delivery at RSAL.This pregnancyPhysical
examinationCompos mentis, BP : 100/70 mmHg, P: 92x/m, FR 18x/m, T :
36OCGen. state: Pale conjungtive -/-, abd ~ pregnancy
Obstetrical Status : FH 32 cm, head presentation, head 4/5, FHR
146, his 1-2 x/10/40I: V/U wnl Io: smooth portio, closed ostium,
flr (-), flx (+).Vt: portio firm, axial, t 2 cm, 2 cm dilatation,
head H I-II
CTG: Category 1Lab:CBC (7/8/14)10.6/31/11830/221000SGOT 20 SGPT
19 Ur 14 Cr 0.6 RBG 79Ul wnl
US exam (7/7/14)Singleton live head presentation, placenta
implanted at leftcorpus, normal implantationBPD 90/HC 311/ AC 344/
FL 71/ AFI 12 / EFW 3159Latent phase of labor in G3P1A1 38 wga,
singleton live fetus, HbsAg reactive
P: Observe hemodynamics, contractions, FHR
Emergency CSConsult to perinatology for HepB Ig
12/8/1420.00 21.00Born baby boy, 3100 gr, 50 cm AS 8/9Clear
amniotic fluidPlacenta born completely
Hb Post op: 10.4 g/dl
Outcome:Now patient and baby are in good condition, already
discharged
-
The mechanism of MTCT remains unclear. Most MTCTs likely occur
perinatally by microperfusion of maternal blood to the fetal
circulation during the uterine contractions and tearing of the
placenta at birth. Other possible modes of infection include
swallowing amniotic fluid, vaginal secretions, or exposure to
maternal blood during VD.
-
CAESAREAN SECTION #4
-
Day S OAP13/8/14DAY I20.30SCTPP
Mrs. Grace A, 26 yoMR. 440720
CC: Referred from Tebet PHC due to prolonged active phase of
labor
Patient admitted 9 months pregnancy. Her LMP 29/10/13 EDD
5/8/14~ 41 wga. ANC regularly at PHC. Contraction (+) since 10
hours, water broke (+) 18 hours. Active fetal movement
Patient was given oxytocin drip 24 drip/minute for 12 hours at
PHC. Dilatation 4 cm 6 cm 7 cm 7 cm (every 4 hours)
Menarche 12 yo, reguler, GP 3x/day, dysmenorrhea (-)
Married 1xObs history: G1This pregnancyPhysical
examinationCompos mentis, BP : 110/50 mmHg, P: 90x/m, FR 18x/m, T :
36.5OCGen. state: Pale conjungtive -/-, abd ~ pregnancy
Obstetrical Status : FH 33 cm, head presentation, head 2/5, FHR
156, his 1-2x/10/45I: V/U wnl Vt: portio thin, 7 cm dilatation,
head H II-III, small fontanel left-transverse
CTG: Category 1Lab:CBC (13/8/14)12.6/36/24000/226000SGOT 3 SGPT
20 Ur 15 Cr 0.6 RBG 108Ul protein wnl
US exam (7/7/14)Singleton live head presentation, placenta
implanted at anterior corpus, normal implantationBPD 91/HC 314/ AC
310/ FL 79/ AFI 4.1 / EFW 3100Inertia of active phase of labor in
G1 40-41 wga, singleton live fetus
P: Observe hemodynamics, contractions, FHRObserve signs of
intrauterine infection and cord compression
Initial plan: vaginal deliveryAcceleration with Oxytocin 5
IU/500 cc RL, start at 8 tpm, escalated 4 tpm/30 mins until
adequate contractions or max 40 tpm.
Ceftriaxone 1 x 2 g IV
-
Day S OAP13/8/14DAY I21.00
13/8/14DAY I22.00
13/8/14DAY I24.00
14/8/1402.00
Oxytocin drip is administered (8 tpm)
Frequent contractions, active fetal movement
Frequent contractions, active fetal movement
Frequent contractions, active fetal movement
His 3-4 x /10 / 45FHR 142 dpm
Physical examinationCompos mentis, BP : 110/70 mmHg, P: 86x/m,
FR 18x/m, T : 36.5OCGen. state: wnlObstetrical Status : FHR 150,
his 4x/10/45I: V/U wnl Vt: complete cm dilatation, head H III,
small fontanel left-transverse
Physical examinationCompos mentis, BP : 120/80 mmHg, P: 90x/m,
FR 18x/m, T : 36.5OCGen. state: wnlObstetrical Status : FHR 150,
his 4x/10/45I: V/U wnl Vt: complete cm dilatation, head H III,
caput H III+, small fontanel posterior
Adequate contractions on active phase of labor in G1 40-41 wga,
singleton live fetus
Second stage of labor in G1 40-41 wga, singleton live fetus
Distosia of second stage of labor in G1 40-41 wga, singleton
live fetus
Sustain oxytocin drip, evaluate after 3 hours
Observe hemodynamics, contractions, FHR
Management of second stage
Emergency CS
03:00Born baby girl, 3150 gr, 50 cm AS 8/9Nil amniotic
fluidPlacenta born completely
Now patient and baby are in good condition already
discharged
-
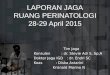
Partograph from PHC Tebet
-
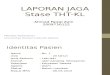
CTG Category 1
-
THANK YOU
*****