Embed Size (px)
Citation preview
Kentucky Application for
Provider Evaluation and Reevaluation
April 2009
KAPER-l (04/2009)

Kentucky Department of Insurance
Kentucky Application for Provider Evaluation and Reevaluation – 2009
Introduction. Development of a uniform application form and guidelines for the evaluation and reevaluation of health care providers, including psychologists, was mandated under KRS 304.17 A-545 (5). In response to the requirement, the Department of Insurance developed the form entitled Kentucky Application for Provider Evaluation and Reevaluation in December 2005. The form has undergone several modifications since that time. However, the current KAPER-1 (04/2009) consists of two (2) parts, including Part A and Part B. The KAPER-1, Part A was adopted with consent from the Council for Affordable Quality Healthcare form entitled "Provider Application." All health insurers offering managed care plans in Kentucky are required to use either the CAQH provider application or the KAPER-1 (04/2009), Part A, for the evaluation (credentialing) and reevaluation (recredentialing) of health care providers, including psychologists, who will be on their lists of participating providers. The KAPER-1 (04/2009), Part A is also used by the Cabinet for Health and Family Services (CHFS) pursuant to KRS 205.560. The KAPER-1, Part B was initially developed in collaboration with health care providers, insurers, and the CHFS. This part is for use by Kentucky hospitals and health care facilities and consists of two (2) sections, including Part B, Section 1, used for initial evaluation (credentialing) of a physician or allied health professional, and Part B, Section 2, used for reevaluation (recredentialing) of a physician or allied health professional. The KAPER-1(04/2009), Part B is also used by the CHFS pursuant to KRS 216B.155. The KAPER-1 (04/2009) may be accessed on the Department’s Web site at http://insurance.ky.gov or obtained directly from the Kentucky Department of Insurance, Division of Health Insurance Policy and Managed Care, P. O. Box 517, Frankfort, KY 40602- 0517. Reproduction of the form without any changes is allowed.
i

KAPER-l (04/2009), Part A
For Evaluation (Credentialing) and Reevaluation (Recredentialing) of Health Care Providers Desiring Participation in Kentucky Managed Care
Plans and the Kentucky Medicaid Program.
ii
Commonwealth of Kentucky Instructions - Form KAPER-l (04/2009), Part A
A. Uniform Kentucky Application for Evaluation (Credentialing) and Reevaluation (recredentialing) Form. Following is the KAPER-l (04/2009), Part A, which was adopted with consent of the Council for Affordable Quality Health Care pursuant to KRS 304.17 A-545(5). A complete KAPER-l (04/2009), Part A, with required attachments, as specified in item C of this instruction, must be accepted by an insurer offering a managed care plan in Kentucky for the evaluation (credentialing) and reevaluation (recredentialing) of a health care provider who will be on the insurer's list of participating providers. "Health care provider" is defined in 806 KAR 17:480, Section 1. The KAPER-l (04/2009), Part A, which must be accepted by the insurer in an electronic or handwritten format, is available on the Web site of the Department of Insurance http://insurance.ky.gov or at a location identified by the health insurer. Prior to completing the KAPER-l (04/2009), it is advised that a health care provider desiring participation in a managed care plan contact the insurer for information regarding electronic or handwritten submission of the form with required attachments, as specified in item C of this instruction, and cover letter, as applicable. Prior to completing the KAPER-1 (04/2009), it is advised that a health care provider desiring participation in the Kentucky Medicaid Program contact the KY Cabinet for Health and Family Services for submission of required attachments, as specified in item C of this instruction, and cover letter, as applicable. B. Cover Letter. If a complete KAPER-l (04/2009), Part A is submitted to an insurer, a cover letter signed and dated by the health care provider requesting consideration of evaluation or revaluation may be required by the insurer. C. Required Attachments. Unless otherwise specified in this instruction, one (1) photocopy of each of the following eight (8) supporting documents shall be on 8 ½” X 11” paper, labeled, and attached to the complete KAPER-l (04/2009), Part A in the following order. 1. Drug enforcement agency (DEA) registration certificate; 2. State controlled dangerous substance (CDS) certificate, if applicable; 3. W-9 of each tax identification number; 4. Workers’ compensation certificate of coverage; 5. Current professional liability insurance policy face sheet (showing expiration dates, limits and health care provider's name); 6. Signed and dated authorization, attestation and release form; 7. Supplemental forms, if any, in page number order; and 8. Additional pages, if indicated (e.g. lists, etc.).
iii
SECTION 1
Provider Type
NameDo not use nicknamesor initials, unless theyare part of your legalname.
3076
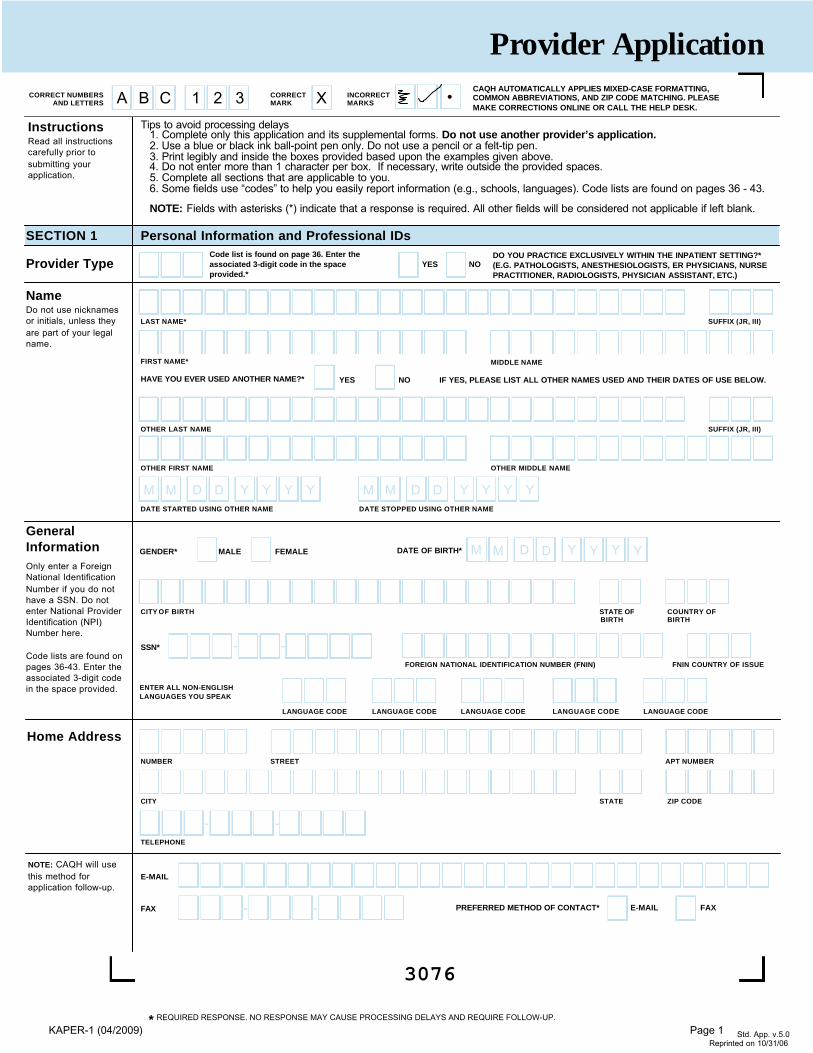
Tips to avoid processing delays 1. Complete only this application and its supplemental forms. Do not use another provider’s application. 2. Use a blue or black ink ball-point pen only. Do not use a pencil or a felt-tip pen. 3. Print legibly and inside the boxes provided based upon the examples given above. 4. Do not enter more than 1 character per box. If necessary, write outside the provided spaces.5. Complete all sections that are applicable to you.6. Some fields use “codes” to help you easily report information (e.g., schools, languages). Code lists are found on pages 36 - 43.
NOTE: Fields with asterisks (*) indicate that a response is required. All other fields will be considered not applicable if left blank.
LAST NAME* SUFFIX (JR, III)
FIRST NAME* MIDDLE NAME
CORRECT NUMBERS AND LETTERS
Personal Information and Professional IDs
CORRECTMARK
INCORRECTMARKSA B C 1 2 3 •X
HAVE YOU EVER USED ANOTHER NAME?* YES NO IF YES, PLEASE LIST ALL OTHER NAMES USED AND THEIR DATES OF USE BELOW.
GENDER* MALE FEMALE
*
OTHER LAST NAME SUFFIX (JR, III)
OTHER FIRST NAME OTHER MIDDLE NAME
DATE STARTED USING OTHER NAME DATE STOPPED USING OTHER NAME
M M D D Y Y Y Y M M D D Y Y Y Y
M M D D Y Y Y Y
FOREIGN NATIONAL IDENTIFICATION NUMBER (FNIN) FNIN COUNTRY OF ISSUE
SSN*
DATE OF BIRTH*
--
InstructionsRead all instructionscarefully prior tosubmitting yourapplication.
REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Provider Application
GeneralInformationOnly enter a ForeignNational IdentificationNumber if you do nothave a SSN. Do notenter National ProviderIdentification (NPI)Number here.
Code lists are found onpages 36-43. Enter theassociated 3-digit codein the space provided.
Std. App. v.5.0
Reprinted on 10/31/06
ENTER ALL NON-ENGLISHLANGUAGES YOU SPEAK
LANGUAGE CODE LANGUAGE CODE LANGUAGE CODE LANGUAGE CODE LANGUAGE CODE
DO YOU PRACTICE EXCLUSIVELY WITHIN THE INPATIENT SETTING?*(E.G. PATHOLOGISTS, ANESTHESIOLOGISTS, ER PHYSICIANS, NURSEPRACTITIONER, RADIOLOGISTS, PHYSICIAN ASSISTANT, ETC.)
CAQH AUTOMATICALLY APPLIES MIXED-CASE FORMATTING,COMMON ABBREVIATIONS, AND ZIP CODE MATCHING. PLEASEMAKE CORRECTIONS ONLINE OR CALL THE HELP DESK.
YES NO
CITY OF BIRTH STATE OF COUNTRY OFBIRTH BIRTH
Code list is found on page 36. Enter theassociated 3-digit code in the spaceprovided.*
NOTE: CAQH will usethis method forapplication follow-up.
NUMBER STREET APT NUMBER
CITY STATE ZIP CODE
FAX - - PREFERRED METHOD OF CONTACT* E-MAIL FAX
Home Address
TELEPHONE
- -
KAPER-1 (04/2009) Page 1
3077
Personal Information and Professional IDs (Continued)
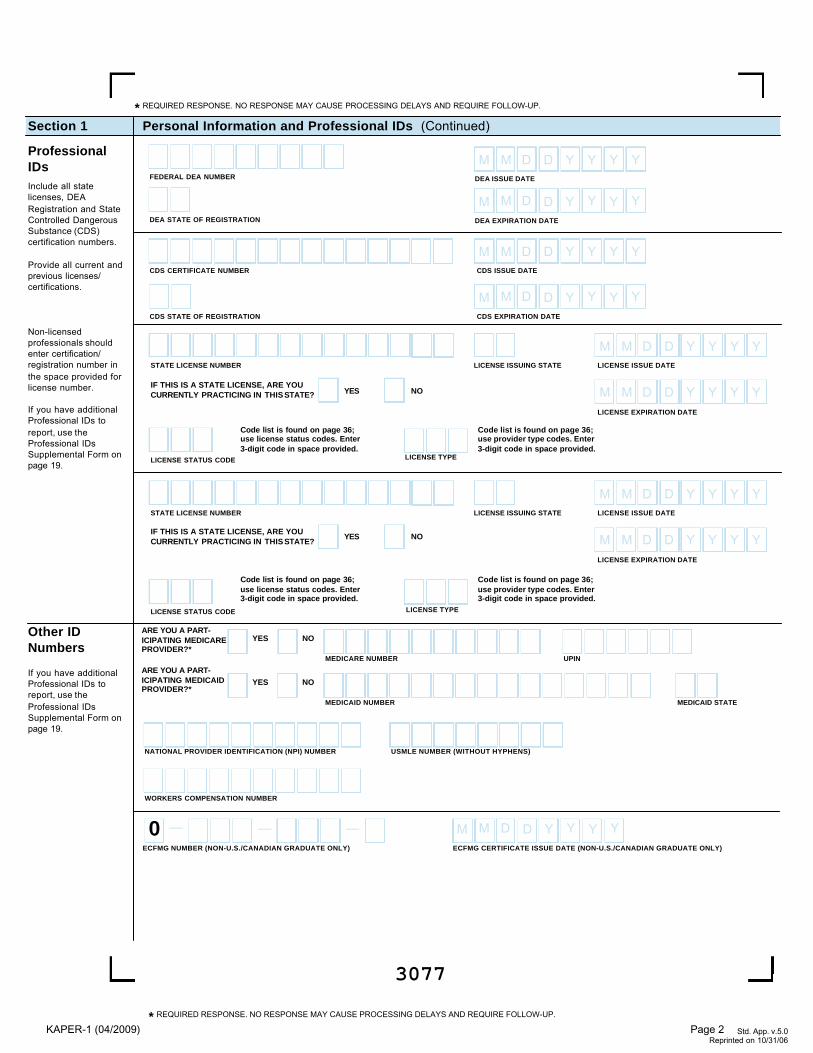
ProfessionalIDsInclude all statelicenses, DEARegistration and StateControlled DangerousSubstance (CDS)certification numbers.
Provide all current andprevious licenses/certifications.
Non-licensedprofessionals shouldenter certification/registration number inthe space provided forlicense number.
If you have additionalProfessional IDs toreport, use theProfessional IDsSupplemental Form onpage 19.
FEDERAL DEA NUMBER
DEA STATE OF REGISTRATION
CDS STATE OF REGISTRATION
DEA EXPIRATION DATE
M M D D Y Y Y Y
DEA ISSUE DATE
M M D D Y Y Y Y
CDS EXPIRATION DATE
M M D D Y Y Y Y
CDS ISSUE DATE
M M D D Y Y Y Y
Section 1
CDS CERTIFICATE NUMBER
LICENSE ISSUING STATE LICENSE ISSUE DATE
M M D D Y Y Y Y
LICENSE EXPIRATION DATE
M M D D Y Y Y Y
LICENSE ISSUE DATE
M M D D Y Y Y Y
LICENSE EXPIRATION DATE
M M D D Y Y Y Y
STATE LICENSE NUMBER
LICENSE STATUS CODE
LICENSE STATUS CODE
LICENSE ISSUING STATESTATE LICENSE NUMBER
IF THIS IS A STATE LICENSE, ARE YOUCURRENTLY PRACTICING IN THIS STATE? YES NO
IF THIS IS A STATE LICENSE, ARE YOUCURRENTLY PRACTICING IN THIS STATE?
YES NO
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0Reprinted on 10/31/06
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
MEDICAID NUMBER
Other IDNumbers
If you have additionalProfessional IDs toreport, use theProfessional IDsSupplemental Form onpage 19.
UPIN
ARE YOU A PART-ICIPATING MEDICAREPROVIDER?*
ARE YOU A PART-ICIPATING MEDICAIDPROVIDER?*
YES NO
MEDICARE NUMBER
MEDICAID STATE
NATIONAL PROVIDER IDENTIFICATION (NPI) NUMBER
WORKERS COMPENSATION NUMBER
USMLE NUMBER (WITHOUT HYPHENS)
ECFMG CERTIFICATE ISSUE DATE (NON-U.S./CANADIAN GRADUATE ONLY)
M M D D Y Y Y Y—— —ECFMG NUMBER (NON-U.S./CANADIAN GRADUATE ONLY)
0
YES NO
Code list is found on page 36; use provider type codes. Enter3-digit code in space provided.
Code list is found on page 36; use provider type codes. Enter3-digit code in space provided.
Code list is found on page 36; use license status codes. Enter3-digit code in space provided.
Code list is found on page 36; use license status codes. Enter3-digit code in space provided.
LICENSE TYPE
LICENSE TYPE
KAPER-1 (04/2009) Page 2
3078
Education and TrainingSection 2
UndergraduateSchool(s)Provide the appropriateinformation for theschool that issued yourundergraduate degreeand all schoolsattended.
ProfessionalSchool(s)Provide the appropriateinformation for theschool that issued yourprofessional degree.
Fifth Pathway Graduatesplease complete thefollowing sections: U.S.School that issued yourcertificate, the Non-U.S.School where youattended, and the FifthPathway institutionwhere you completedyour training onSupplemental Page 20.
Code lists are found onpages 36-43. Enter theassociated 3-digit codein the space provided.
If you have additionalUndergraduate orProfessional Schools toreport, use theEducation SupplementalForm on page 20.
UNDERGRADUATE SCHOOL
DEGREE AWARDEDSTART DATE END DATE (GRADUATION DATE)
M M Y Y Y YM M Y Y Y Y
OFFICIAL NAME OF UNDERGRADUATE SCHOOL
DID YOU COMPLETE YOURUNDERGRADUATE EDUCATIONAT THIS SCHOOL?
YES NO
DID YOU COMPLETE YOURGRADUATE EDUCATION AT THISSCHOOL?
YES NO
DID YOU COMPLETE YOURGRADUATE EDUCATION AT THISSCHOOL?
YES NO
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
ADDRESS
CITY STATE ZIP/POSTAL CODE
COUNTRY CODE TELEPHONE
- -FAX
- -
DEGREE AWARDEDSTART DATE* END DATE (GRADUATION DATE)*
M M Y Y Y YM M Y Y Y Y
U.S. OR CANADIAN SCHOOL
NON - U.S. OR CANADIAN SCHOOL
CITY COUNTRY CODE POSTAL CODE
ADDRESS
DEGREE AWARDEDSTART DATE* END DATE (GRADUATION DATE)*
M M Y Y Y YM M Y Y Y Y
OFFICIAL NAME OF NON-U.S. PROFESSIONAL SCHOOL
SCHOOL CODE (U.S./CANADIAN ONLY)
NAME OF U.S./CANADIAN SCHOOL:
U.S. OR CANADIAN GRADUATE FIFTH PATHWAY GRADUATE
GRADUATE TYPE*:
NON-U.S./CANADIAN GRADUATE
KAPER-1 (04/2009) Page 3
3080
Education and Training (Continued)Section 2
Training
List all trainingprograms youattended. Use onesection per institution.
If you have additionalpost-graduate trainingprograms, use theSupplemental TrainingForm on page 21.
Please explain on theSupplementalProfessional / WorkHistory Gap Form onpage 33 any traininggap(s) of three (3)months or greater, orany gap(s) of a shorterduration if required bythe organization forwhich you are beingcredentialed.
Code lists are found onpages 36-43. Enter theassociated 3-digit codein the space provided.
INSTITUTION/HOSPITAL NAME (USE BOTH LINES IF REQUIRED)
START DATE END DATE
M M Y Y Y YM M Y Y Y Y
SCHOOL CODE (E.G.,AFFILIATED MEDICALSCHOOL)
INTERNSHIP/RESIDENCY FELLOWSHIP OTHER
DEPARTMENT/SPECIALTY (DO NOT ABBREVIATE)
NAME OF DIRECTOR
NAME OF DIRECTOR
NAME OF DIRECTOR
List eachdepartment
separately, ifapplicable.
ListInternship/Residency,Fellowshipand Otherprograms
separately.INTERNSHIP/RESIDENCY FELLOWSHIP OTHER
DEPARTMENT/SPECIALTY (DO NOT ABBREVIATE)
START DATE END DATE
M M Y Y Y YM M Y Y Y Y
INTERNSHIP/RESIDENCY
FELLOWSHIP OTHER
DEPARTMENT/SPECIALTY (DO NOT ABBREVIATE)
START DATE END DATE
M M Y Y Y YM M Y Y Y Y
NUMBER STREET SUITE/BUILDING
CITY STATE ZIP/POSTAL CODE
COUNTRY CODE TELEPHONE
- -FAX
- -
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
DID YOU COMPLETE THIS TRAINING PROGRAM AT THISINSTITUTION?
(IF NOT, PLEASE USE THE SPACE BELOW TO EXPLAIN.)
YES NO
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
KAPER-1 (04/2009) Page 4
3081
PrimarySpecialty
Code lists are found onpages 36-43. Enter theassociated 3-digit codein the space provided.
SPECIALTY CODE
BOARD CERTIFIED? YES NO
CERTIFYING BOARD CODE
RECERTIFICATION DATE
(IF APPLICABLE)M M D D Y Y Y Y
EXPIRATION DATE (IF APPLICABLE) M M D D Y Y Y Y
INITIAL CERTIFICATION
DATE M M D D Y Y Y Y YES NO
DO YOU WISH TOBE LISTED INTHE DIRECTORYUNDER THISSPECIALTY?
YES NO
YES NO
HMO
PPO
POS
IF NOTBOARD CERTIFIED(SELECTONE)
I HAVE TAKENEXAM, RESULTSPENDING FOR
CERTIFYING BOARD CODE
IF YOU INDICATED THAT YOU DID NOT INTEND TO TAKE A CERTIFYING BOARD EXAM, PLEASE USE THEFOLLOWING SPACE TO EXPLAIN, OTHERWISE LEAVE THE SPACE BLANK.
I INTEND TO SIT FOR ANEXAM ON
M M D D Y Y Y Y
I DO NOT INTEND TO TAKEA CERTIFYING BOARD EXAM.
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP. Std. App. v.5.0
Reprinted on 10/31/06
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
IF YOU INDICATED THAT YOU DID NOT INTEND TO TAKE A CERTIFYING BOARD EXAM, PLEASE USE THEFOLLOWING SPACE TO EXPLAIN, OTHERWISE LEAVE THE SPACE BLANK.
Professional / Medical Specialty InformationSection 3
SecondarySpecialty
Code lists are found onpages 36-43. Enter theassociated 3-digit codein the space provided.
If you have additionalProfessional / MedicalSpecialties to report,use the AdditionalSpecialtiesSupplemental Form onpage 22.
SPECIALTY CODE
BOARD CERTIFIED?
YES NO
CERTIFYING BOARD CODE
RECERTIFICATION DATE
(IF APPLICABLE)M M D D Y Y Y Y
EXPIRATION DATE (IF APPLICABLE) M M D D Y Y Y Y
INITIAL CERTIFICATION
DATE M M D D Y Y Y Y YES NO
DO YOU WISH TOBE LISTED INTHE DIRECTORYUNDER THISSPECIALTY?
YES NO
YES NO
HMO
PPO
POS
IF NOTBOARD CERTIFIED(SELECTONE)
I HAVE TAKENEXAM, RESULTSPENDING FOR
CERTIFYING BOARD CODE
I INTEND TO SIT FOR ANEXAM ON
M M D D Y Y Y Y
I DO NOT INTEND TO TAKEA CERTIFYING BOARD EXAM.
KAPER-1 (04/2009) Page 5
3082
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
Professional / Medical Specialty Information (Continued)Section 3
PracticeInterestsProvide additionalareas of professionalpractice interest,activities, procedures,diagnoses orpopulations.
CertificationsEXPIRATION DATE EXPIRATION DATE
BASIC LIFESUPPORT?*
YES NO
CPR?* YES NO
ADVCARDIAC LIFE SPT?*
YES NO
Do you hold the following certifications? If yes, provide expiration dates.
M M D D Y Y Y Y
M M D D Y Y Y Y
M M D D Y Y Y Y
NEONATALADVANCEDLIFE SPT?*
YES NO M M D D Y Y Y Y
ADV LIFESUPPORT INOB?*
YES NO
ADV TRAUMALIFE SUPPORT?*
YES NO
PEDIATRICADVANCEDLIFE SPT?*
YES NO
M M D D Y Y Y Y
M M D D Y Y Y Y
M M D D Y Y Y Y
PrimaryCredentialingContact
CHECK HERE TOUSE THE OFFICEMANAGER ANDADDRESS OF THEPRIMARY PRACTICELOCATION AS THECREDENTIALINGINFORMATION.
CITY
LAST NAME
FIRST NAME
NUMBER STREET SUITE/BUILDING
E-MAIL ADDRESS
TELEPHONE
- -FAX
- -
M.I.
STATE ZIP CODE
NOTE:
Even if you checkedthe boxes above,please provide thee-mail address, ifavailable.
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
KAPER-1 (04/2009) Page 6
3083
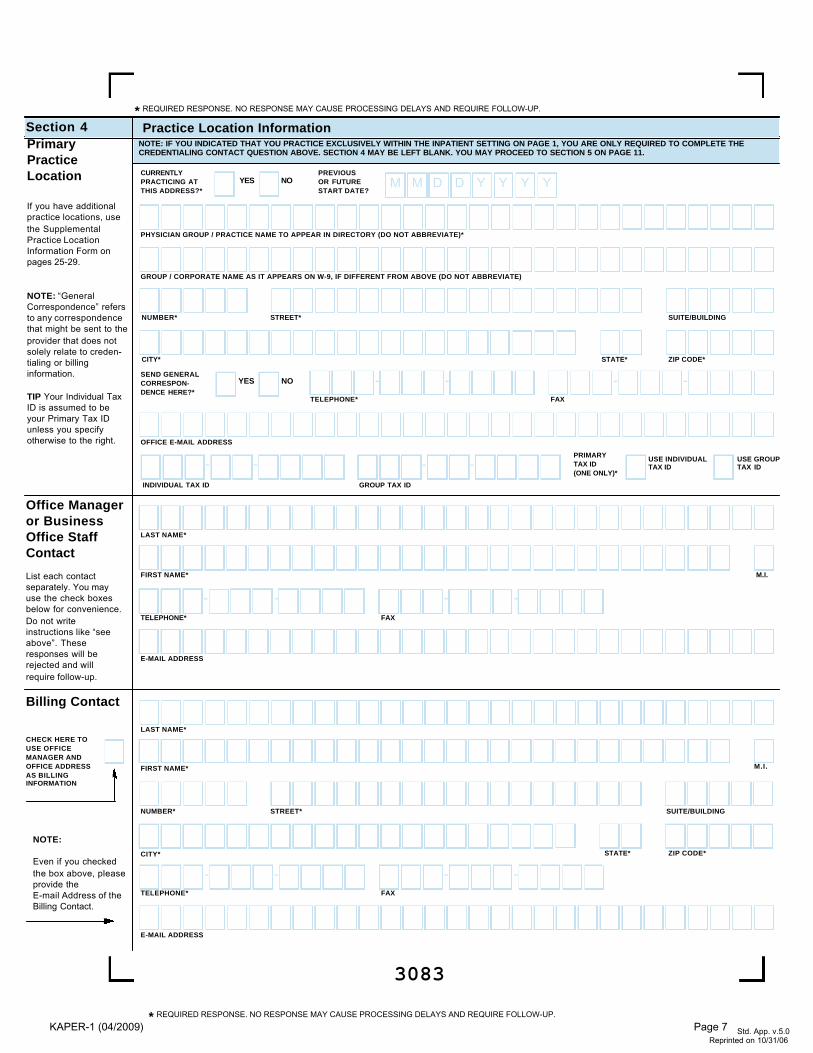
Practice Location InformationSection 4
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
NOTE: IF YOU INDICATED THAT YOU PRACTICE EXCLUSIVELY WITHIN THE INPATIENT SETTING ON PAGE 1, YOU ARE ONLY REQUIRED TO COMPLETE THECREDENTIALING CONTACT QUESTION ABOVE. SECTION 4 MAY BE LEFT BLANK. YOU MAY PROCEED TO SECTION 5 ON PAGE 11.
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
NUMBER* STREET* SUITE/BUILDING
CITY* STATE* ZIP CODE*
PHYSICIAN GROUP / PRACTICE NAME TO APPEAR IN DIRECTORY (DO NOT ABBREVIATE)*
GROUP / CORPORATE NAME AS IT APPEARS ON W-9, IF DIFFERENT FROM ABOVE (DO NOT ABBREVIATE)
TELEPHONE*
- -FAX
- -
OFFICE E-MAIL ADDRESS
SEND GENERALCORRESPON-DENCE HERE?*
YES NO
CURRENTLYPRACTICING AT THIS ADDRESS?*
YES NO M M D D Y Y Y YPREVIOUSOR FUTURESTART DATE?
INDIVIDUAL TAX ID
--GROUP TAX ID
PRIMARYTAX ID (ONE ONLY)*
-- USE INDIVIDUAL TAX ID
USE GROUP TAX ID
LAST NAME*
E-MAIL ADDRESS
FIRST NAME*
TELEPHONE*
- -FAX
- -
M.I.
Office Manageror BusinessOffice StaffContact
List each contactseparately. You mayuse the check boxesbelow for convenience.Do not writeinstructions like “seeabove”. Theseresponses will berejected and willrequire follow-up.
PrimaryPracticeLocation
If you have additionalpractice locations, usethe SupplementalPractice LocationInformation Form onpages 25-29.
NOTE: “GeneralCorrespondence” refersto any correspondencethat might be sent to theprovider that does notsolely relate to creden-tialing or billinginformation.
TIP Your Individual TaxID is assumed to beyour Primary Tax IDunless you specifyotherwise to the right.
CITY*
LAST NAME*
FIRST NAME*
NUMBER* STREET* SUITE/BUILDING
E-MAIL ADDRESS
TELEPHONE*
- -FAX
- -
Billing Contact
M.I.
STATE* ZIP CODE*
CHECK HERE TOUSE OFFICEMANAGER ANDOFFICE ADDRESSAS BILLINGINFORMATION
NOTE:
Even if you checkedthe box above, pleaseprovide theE-mail Address of theBilling Contact.
KAPER-1 (04/2009) Page 7
3084
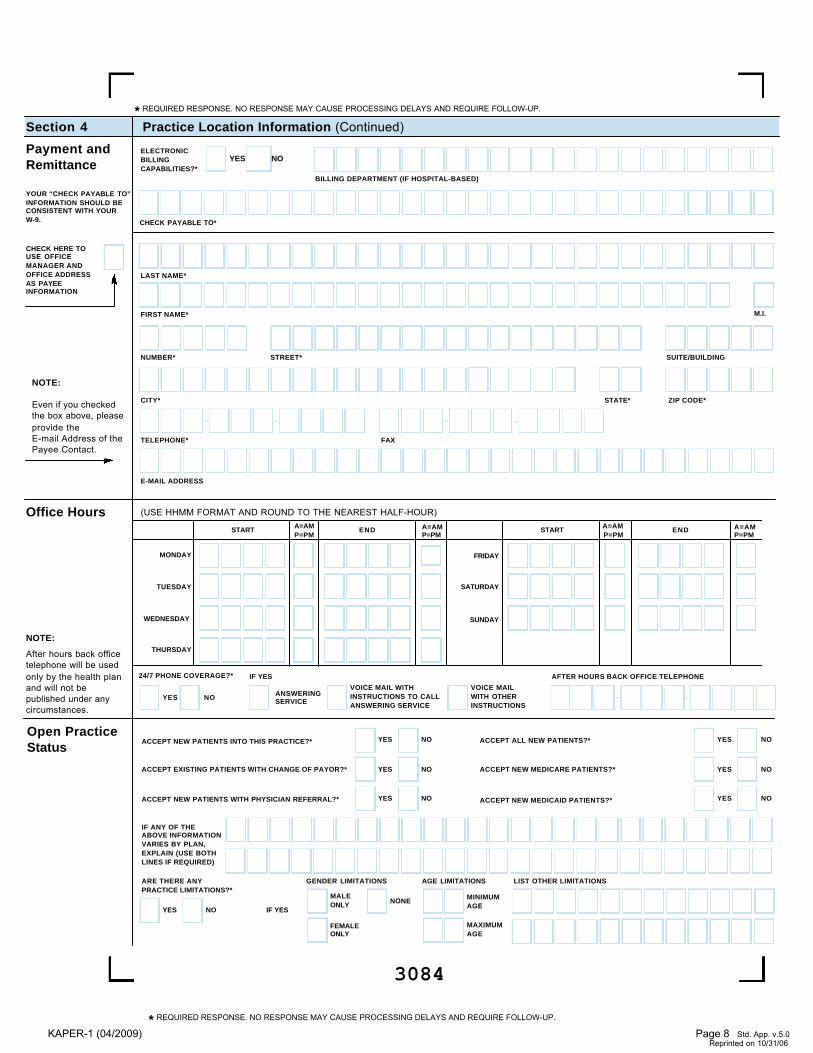
Practice Location Information (Continued)Section 4
BILLING DEPARTMENT (IF HOSPITAL-BASED)
CHECK PAYABLE TO*
ELECTRONIC BILLINGCAPABILITIES?*
YES NOPayment andRemittance
CITY*
NUMBER* STREET* SUITE/BUILDING
E-MAIL ADDRESS
TELEPHONE*
- -FAX
- -
STATE* ZIP CODE*
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP. Std. App. v.5.0
Reprinted on 10/31/06
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Office Hours
NOTE:
After hours back officetelephone will be usedonly by the health planand will not bepublished under anycircumstances.
(USE HHMM FORMAT AND ROUND TO THE NEAREST HALF-HOUR)
MONDAY
TUESDAY
WEDNESDAY
THURSDAY
FRIDAY
SATURDAY
SUNDAY
START END
24/7 PHONE COVERAGE?*
YES NO ANSWERINGSERVICE
IF YES
VOICE MAIL WITH INSTRUCTIONS TO CALLANSWERING SERVICE
VOICE MAIL WITH OTHERINSTRUCTIONS
AFTER HOURS BACK OFFICE TELEPHONE
- -
A=AMP=PM
A=AMP=PM
START ENDA=AMP=PM
A=AMP=PM
LAST NAME*
FIRST NAME* M.I.
CHECK HERE TOUSE OFFICEMANAGER ANDOFFICE ADDRESSAS PAYEEINFORMATION
YOUR “CHECK PAYABLE TO”INFORMATION SHOULD BECONSISTENT WITH YOURW-9.
NOTE:
Even if you checkedthe box above, pleaseprovide theE-mail Address of thePayee Contact.
Open PracticeStatus
ACCEPT NEW PATIENTS INTO THIS PRACTICE?* YES NO
ACCEPT EXISTING PATIENTS WITH CHANGE OF PAYOR?*
IF ANY OF THEABOVE INFORMATIONVARIES BY PLAN,EXPLAIN (USE BOTHLINES IF REQUIRED)
YES NO
ACCEPT NEW PATIENTS WITH PHYSICIAN REFERRAL?*
ACCEPT NEW MEDICARE PATIENTS?*
ACCEPT NEW MEDICAID PATIENTS?* YES NO
ARE THERE ANYPRACTICE LIMITATIONS?*
YES NO
MALE ONLY
FEMALEONLY
NONEIF YES
YES NO
GENDER LIMITATIONS
MINIMUM AGE
MAXIMUM AGE
AGE LIMITATIONS LIST OTHER LIMITATIONS
YES NO
ACCEPT ALL NEW PATIENTS?* YES NO
KAPER-1 (04/2009) Page 8
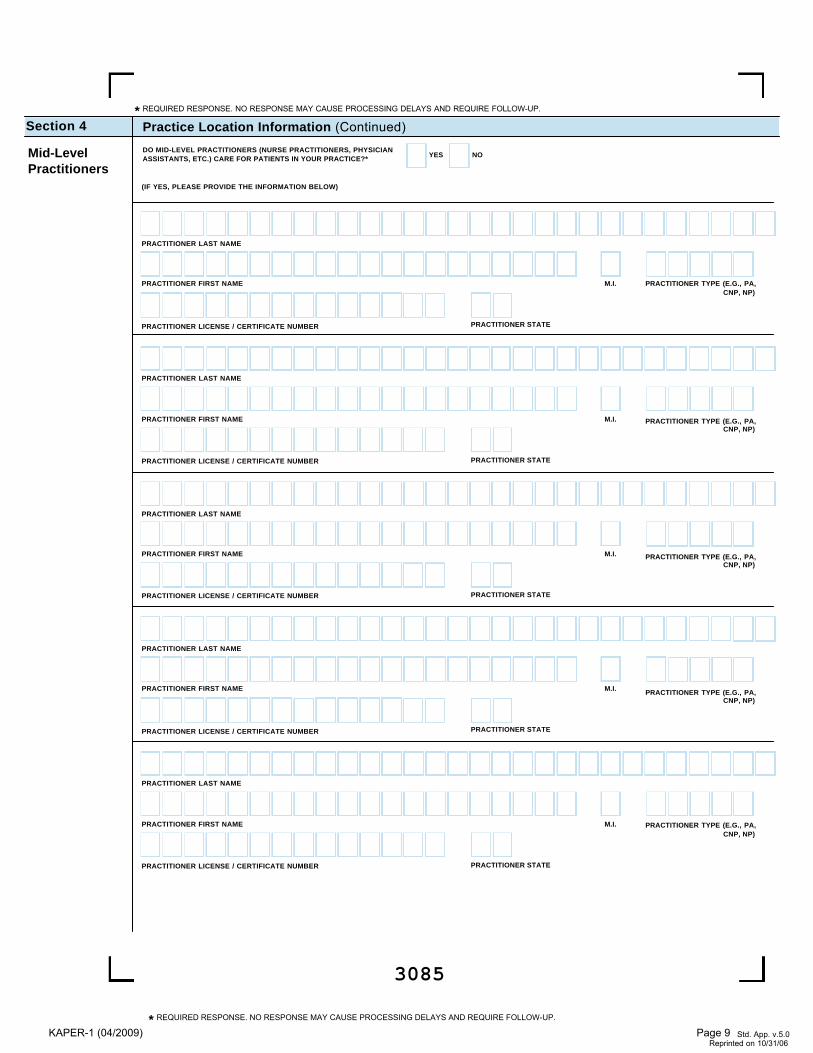
DO MID-LEVEL PRACTITIONERS (NURSE PRACTITIONERS, PHYSICIANASSISTANTS, ETC.) CARE FOR PATIENTS IN YOUR PRACTICE?*
3085
Practice Location Information (Continued)Section 4
Mid-LevelPractitioners
YES NO
(IF YES, PLEASE PROVIDE THE INFORMATION BELOW)
PRACTITIONER LAST NAME
PRACTITIONER FIRST NAME PRACTITIONER TYPE (E.G., PA,CNP, NP)
PRACTITIONER TYPE (E.G., PA,CNP, NP)
PRACTITIONER TYPE (E.G., PA,CNP, NP)
PRACTITIONER TYPE (E.G., PA,CNP, NP)
PRACTITIONER TYPE (E.G., PA,CNP, NP)
PRACTITIONER LICENSE / CERTIFICATE NUMBER PRACTITIONER STATE
M.I.
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
PRACTITIONER LAST NAME
PRACTITIONER FIRST NAME
PRACTITIONER LICENSE / CERTIFICATE NUMBER PRACTITIONER STATE
PRACTITIONER LAST NAME
PRACTITIONER FIRST NAME
PRACTITIONER LICENSE / CERTIFICATE NUMBER PRACTITIONER STATE
M.I.
M.I.
PRACTITIONER LAST NAME
PRACTITIONER FIRST NAME
PRACTITIONER LICENSE / CERTIFICATE NUMBER PRACTITIONER STATE
PRACTITIONER LAST NAME
PRACTITIONER FIRST NAME
PRACTITIONER LICENSE / CERTIFICATE NUMBER PRACTITIONER STATE
M.I.
M.I.
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
KAPER-1 (04/2009) Page 9
3086
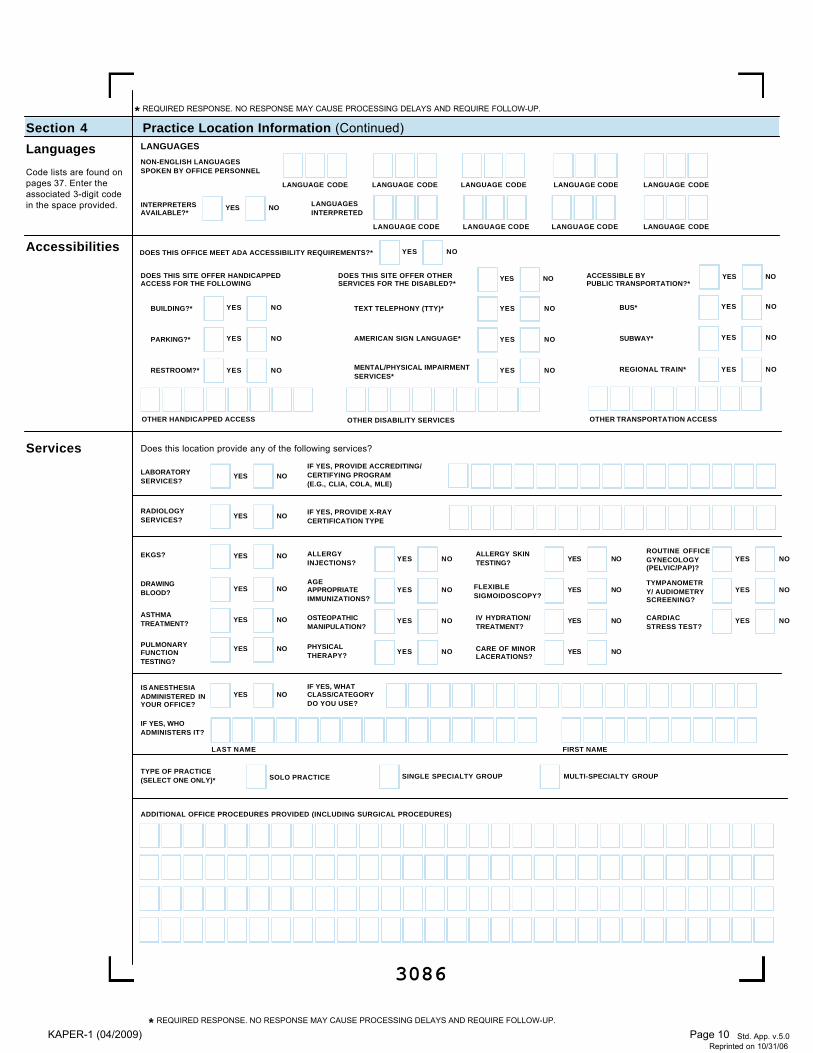
Practice Location Information (Continued)Section 4
Languages
Code lists are found onpages 37. Enter theassociated 3-digit codein the space provided.
Accessibilities
Services
NON-ENGLISH LANGUAGES SPOKEN BY OFFICE PERSONNEL
LANGUAGE CODE LANGUAGE CODE LANGUAGE CODE LANGUAGE CODE LANGUAGE CODE
LANGUAGES INTERPRETED
LANGUAGE CODE LANGUAGE CODE LANGUAGE CODE LANGUAGE CODE
INTERPRETERSAVAILABLE?*
YES NO
LANGUAGES
DOES THIS OFFICE MEET ADA ACCESSIBILITY REQUIREMENTS?* YES NO
YES NO YES NODOES THIS SITE OFFER HANDICAPPED ACCESS FOR THE FOLLOWING
DOES THIS SITE OFFER OTHER SERVICES FOR THE DISABLED?*
ACCESSIBLE BY PUBLIC TRANSPORTATION?*
BUILDING?* YES NO
PARKING?* YES NO
RESTROOM?* YES NO
OTHER HANDICAPPED ACCESS
BUS* YES NO
SUBWAY* YES NO
REGIONAL TRAIN* YES NO
OTHER TRANSPORTATION ACCESS
TEXT TELEPHONY (TTY)* YES NO
AMERICAN SIGN LANGUAGE* YES NO
MENTAL/PHYSICAL IMPAIRMENTSERVICES*
YES NO
OTHER DISABILITY SERVICES
RADIOLOGYSERVICES? YES NO
DRAWINGBLOOD? YES NO
LABORATORYSERVICES?
YES NO
ALLERGYINJECTIONS? YES NO
AGEAPPROPRIATEIMMUNIZATIONS?
YES NO
ALLERGY SKINTESTING? YES NO
FLEXIBLESIGMOIDOSCOPY?
YES NO
ROUTINE OFFICEGYNECOLOGY(PELVIC/PAP)?
YES NO
TYMPANOMETRY/ AUDIOMETRYSCREENING?
YES NO
ASTHMATREATMENT? YES NO
PHYSICALTHERAPY?
OSTEOPATHICMANIPULATION?
YES NO IV HYDRATION/TREATMENT?
YES NO CARDIACSTRESS TEST?
YES NO
IF YES, PROVIDE ACCREDITING/CERTIFYING PROGRAM(E.G., CLIA, COLA, MLE)
IF YES, PROVIDE X-RAYCERTIFICATION TYPE
IF YES, WHATCLASS/CATEGORYDO YOU USE?
IF YES, WHOADMINISTERS IT?
IS ANESTHESIAADMINISTERED INYOUR OFFICE?
YES NO
EKGS? YES NO
PULMONARYFUNCTIONTESTING?
YES NO YES NO
Does this location provide any of the following services?
LAST NAME FIRST NAME
CARE OF MINORLACERATIONS?
YES NO
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP. Std. App. v.5.0
Reprinted on 10/31/06
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
TYPE OF PRACTICE(SELECT ONE ONLY)* SOLO PRACTICE SINGLE SPECIALTY GROUP MULTI-SPECIALTY GROUP
ADDITIONAL OFFICE PROCEDURES PROVIDED (INCLUDING SURGICAL PROCEDURES)
KAPER-1 (04/2009) Page 10
3087
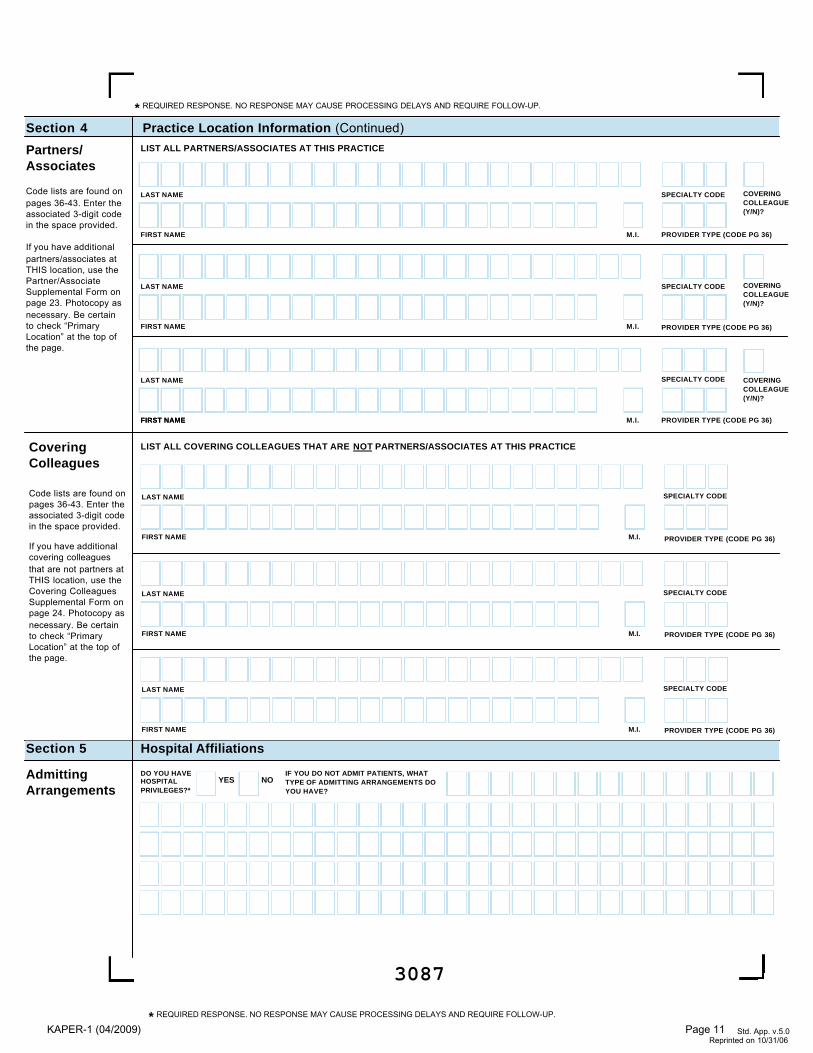
Practice Location Information (Continued)Section 4
Partners/Associates
Code lists are found onpages 36-43. Enter theassociated 3-digit codein the space provided.
If you have additionalpartners/associates atTHIS location, use thePartner/AssociateSupplemental Form onpage 23. Photocopy asnecessary. Be certainto check “PrimaryLocation” at the top ofthe page.
CoveringColleagues
Code lists are found onpages 36-43. Enter theassociated 3-digit codein the space provided.
If you have additionalcovering colleaguesthat are not partners atTHIS location, use theCovering ColleaguesSupplemental Form onpage 24. Photocopy asnecessary. Be certainto check “PrimaryLocation” at the top ofthe page.
FIRST NAME
LAST NAME
FIRST NAME
LAST NAME
FIRST NAME
SPECIALTY CODE
M.I.
LIST ALL COVERING COLLEAGUES THAT ARE NOT PARTNERS/ASSOCIATES AT THIS PRACTICE
LIST ALL PARTNERS/ASSOCIATES AT THIS PRACTICE
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
M.I.
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
M.I.
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
M.I.
M.I.
SPECIALTY CODE
LAST NAME
FIRST NAME M.I.
SPECIALTY CODE
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Hospital AffiliationsSection 5
AdmittingArrangements
DO YOU HAVEHOSPITALPRIVILEGES?*
YES NOIF YOU DO NOT ADMIT PATIENTS, WHATTYPE OF ADMITTING ARRANGEMENTS DOYOU HAVE?
KAPER-1 (04/2009) Page 11
3088
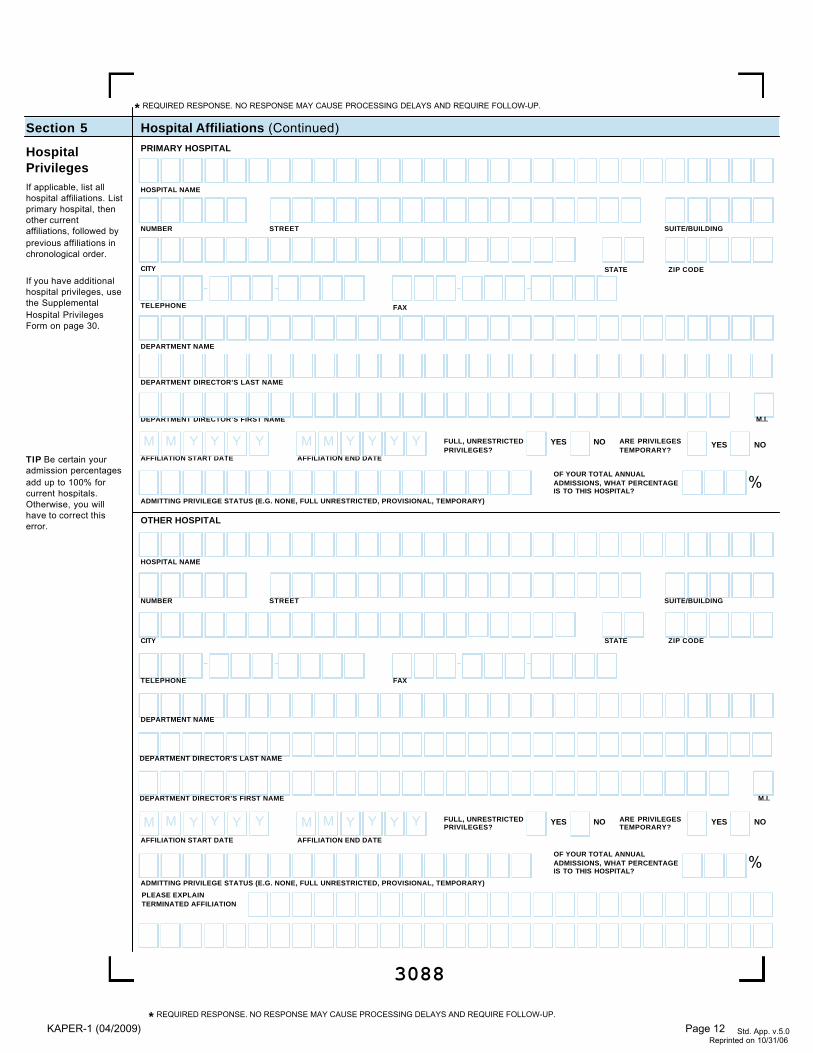
Hospital Affiliations (Continued)Section 5
HospitalPrivilegesIf applicable, list allhospital affiliations. Listprimary hospital, thenother currentaffiliations, followed byprevious affiliations inchronological order.
If you have additionalhospital privileges, usethe SupplementalHospital PrivilegesForm on page 30.
TIP Be certain youradmission percentagesadd up to 100% forcurrent hospitals.Otherwise, you willhave to correct thiserror.
PRIMARY HOSPITAL
HOSPITAL NAME
DEPARTMENT NAME
NUMBER STREET SUITE/BUILDING
TELEPHONE
- -FAX
- -
FULL, UNRESTRICTEDPRIVILEGES?
ARE PRIVILEGESTEMPORARY?
YES NO
ADMITTING PRIVILEGE STATUS (E.G. NONE, FULL UNRESTRICTED, PROVISIONAL, TEMPORARY)
ADMITTING PRIVILEGE STATUS (E.G. NONE, FULL UNRESTRICTED, PROVISIONAL, TEMPORARY)
OF YOUR TOTAL ANNUALADMISSIONS, WHAT PERCENTAGEIS TO THIS HOSPITAL?
%
STATE ZIP CODECITY
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
YES NO
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
AFFILIATION START DATE
M M Y Y Y Y
OTHER HOSPITAL
HOSPITAL NAME
DEPARTMENT NAME
NUMBER STREET SUITE/BUILDING
TELEPHONE
- -FAX
- -
OF YOUR TOTAL ANNUALADMISSIONS, WHAT PERCENTAGEIS TO THIS HOSPITAL?
%
STATE ZIP CODECITY
AFFILIATION END DATE
M M Y Y Y Y
FULL, UNRESTRICTEDPRIVILEGES?
ARE PRIVILEGESTEMPORARY?
YES NOYES NO
AFFILIATION START DATE
M M Y Y Y YAFFILIATION END DATE
M M Y Y Y Y
PLEASE EXPLAINTERMINATED AFFILIATION
DEPARTMENT DIRECTOR’S LAST NAME
DEPARTMENT DIRECTOR’S FIRST NAME M.I.
DEPARTMENT DIRECTOR’S LAST NAME
DEPARTMENT DIRECTOR’S FIRST NAME M.I.
KAPER-1 (04/2009) Page 12
3089
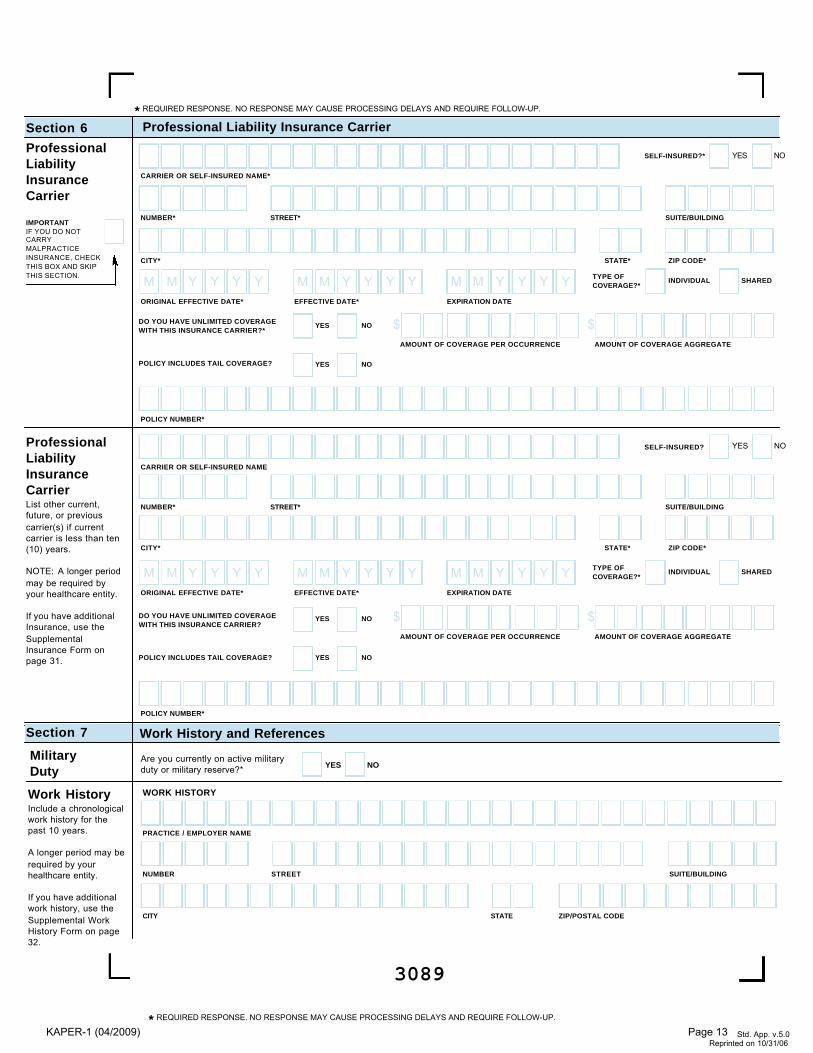
ProfessionalLiabilityInsuranceCarrier
Professional Liability Insurance CarrierSection 6
SELF-INSURED? YES NO
CARRIER OR SELF-INSURED NAME
ProfessionalLiabilityInsuranceCarrierList other current,future, or previouscarrier(s) if currentcarrier is less than ten(10) years.
NOTE: A longer periodmay be required byyour healthcare entity.
If you have additionalInsurance, use theSupplementalInsurance Form onpage 31.
SELF-INSURED?* YES NO
CARRIER OR SELF-INSURED NAME*
NUMBER* STREET* SUITE/BUILDING
EFFECTIVE DATE* EXPIRATION DATE
M M Y Y Y YM M Y Y Y Y
DO YOU HAVE UNLIMITED COVERAGEWITH THIS INSURANCE CARRIER?*
YES NO
DO YOU HAVE UNLIMITED COVERAGEWITH THIS INSURANCE CARRIER?
YES NO
POLICY INCLUDES TAIL COVERAGE? YES NO
, ,$AMOUNT OF COVERAGE PER OCCURRENCE
, ,$AMOUNT OF COVERAGE AGGREGATE
POLICY INCLUDES TAIL COVERAGE? YES NO
, ,$
AMOUNT OF COVERAGE PER OCCURRENCE, ,
$AMOUNT OF COVERAGE AGGREGATE
STATE* ZIP CODE*CITY*
POLICY NUMBER*
POLICY NUMBER*
ORIGINAL EFFECTIVE DATE*
M M Y Y Y Y
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP. Std. App. v.5.0
Reprinted on 10/31/06
NUMBER* STREET* SUITE/BUILDING
EFFECTIVE DATE* EXPIRATION DATE
M M Y Y Y YM M Y Y Y Y TYPE OFCOVERAGE?*
INDIVIDUAL SHARED
TYPE OFCOVERAGE?*
INDIVIDUAL SHARED
STATE* ZIP CODE*CITY*
ORIGINAL EFFECTIVE DATE*
M M Y Y Y Y
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Work History and ReferencesSection 7
Work HistoryInclude a chronologicalwork history for thepast 10 years.
A longer period may berequired by yourhealthcare entity.
If you have additionalwork history, use theSupplemental WorkHistory Form on page32.
WORK HISTORY
PRACTICE / EMPLOYER NAME
Military Duty
Are you currently on active militaryduty or military reserve?* YES NO
NUMBER STREET SUITE/BUILDING
CITY STATE ZIP/POSTAL CODE
IMPORTANTIF YOU DO NOTCARRYMALPRACTICEINSURANCE, CHECKTHIS BOX AND SKIPTHIS SECTION.
KAPER-1 (04/2009) Page 13
3090
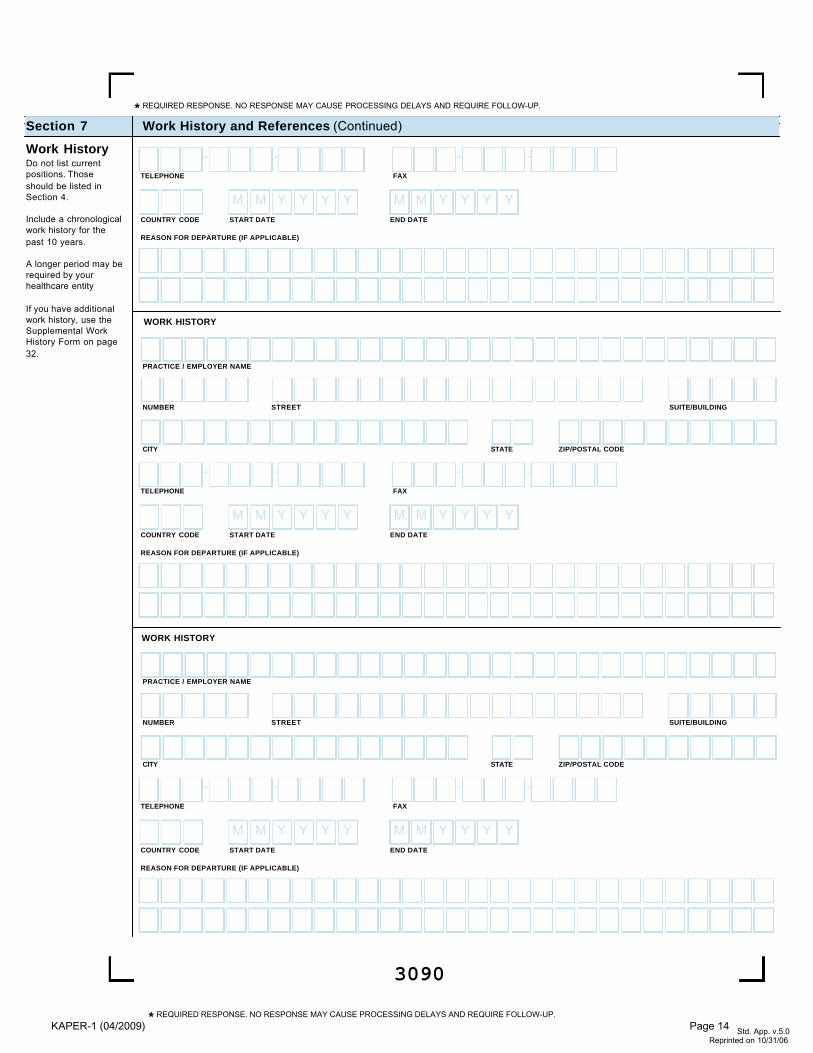
Work History and References (Continued)Section 7
Work HistoryDo not list currentpositions. Thoseshould be listed inSection 4.
Include a chronologicalwork history for thepast 10 years.
A longer period may berequired by yourhealthcare entity
If you have additionalwork history, use theSupplemental WorkHistory Form on page32.
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
START DATECOUNTRY CODE
REASON FOR DEPARTURE (IF APPLICABLE)
END DATE
M M Y Y Y YM M Y Y Y Y
TELEPHONE
- -FAX
- -
START DATECOUNTRY CODE
REASON FOR DEPARTURE (IF APPLICABLE)
END DATE
M M Y Y Y YM M Y Y Y Y
TELEPHONE
- -FAX
- -
PRACTICE / EMPLOYER NAME
NUMBER STREET SUITE/BUILDING
CITY STATE ZIP/POSTAL CODE
START DATECOUNTRY CODE
REASON FOR DEPARTURE (IF APPLICABLE)
END DATE
M M Y Y Y YM M Y Y Y Y
TELEPHONE
- -FAX
- -
PRACTICE / EMPLOYER NAME
NUMBER STREET SUITE/BUILDING
CITY STATE ZIP/POSTAL CODE
WORK HISTORY
WORK HISTORY
KAPER-1 (04/2009) Page 14
3091
Work History and References (Continued)Section 7
Gaps inProfessional /Work History
If you have additionalprofessional / workhistory gaps, use theSupplementalProfessional WorkHistory Gaps Form onpage 33.
GAP START DATE
PLEASE EXPLAIN ANY TIME PERIODS OR GAPS IN TRAINING OR WORK HISTORY THAT HAVE OCCURRED SINCE GRADUATION FROM PROFESSIONAL SCHOOL AND ARELONGER THAN THREE MONTHS IN DURATION OR OF A SHORTER DURATION IF REQUIRED BY THE ORGANIZATION FOR WHICH YOU ARE BEING CREDENTIALED.
GAP END DATE M M Y Y Y YM M Y Y Y Y
LAST NAME*
FIRST NAME*
NUMBER* STREET* APT/SUITE/BUILDING
NUMBER* STREET* APT/SUITE/BUILDING
NUMBER* STREET* APT/SUITE/BUILDING
LAST NAME*
FIRST NAME*
LAST NAME*
FIRST NAME*
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
STATE* ZIP CODE*CITY*
STATE* ZIP CODE*CITY*
STATE* ZIP CODE*CITY*
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
TELEPHONE
- -FAX
- -
TELEPHONE
- -FAX
- -
TELEPHONE
- -FAX
- -
ProfessionalReferencesProvide threeprofessional referencesto whom you are notrelated or are notpartners in yourpractice.
Code lists are found onpages 36-43. Enter theassociated 3-digit codefor provider type.
NOTE:
You are required toprovide exactly 3references. Yourapplication will not becomplete without thisinformation.
Please check withcredentialing entity forany specialrequirements.
KAPER-1 (04/2009) Page 15
3092
Disclosure QuestionsSection 8
DisclosureQuestionsAnswer all questions.For any “Yes”response, provide anexplanation on theSupplementalDisclosure QuestionExplanation Form onpage 34.
Allied HealthProvidersIf you are an AlliedHealth Provider andyou do not believe aquestion is applicableto you, you shouldanswer the question“NO”.
Has your license, registration or certification to practice in your profession, ever been voluntarily or involuntarily relinquished,denied, suspended, revoked, restricted, or have you ever been subject to a fine, reprimand, consent order, probation or any con-ditions or limitations by any state or professional licensing, registration or certification board?*
YES NO1.
Has there been any challenge to your licensure, registration or certification?*YES NO2.
Have your clinical privileges or medical staff membership at any hospital or healthcare institution, voluntarily or involuntarily, everbeen denied, suspended, revoked, restricted, denied renewal or subject to probationary or to other disciplinary conditions (forreasons other than non-completion of medical record when quality of care was not adversely affected) or have proceedingstoward any of those ends been instituted or recommended by any hospital or healthcare institution, medical staff or committee,or governing board?*
YES NO3.
Have you voluntarily or involuntarily surrendered, limited your privileges or not reapplied for privileges while under investigation?*YES NO4.
Have you ever been terminated for cause or not renewed for cause from participation, or been subject to any disciplinary action,by any managed care organizations (including HMOs, PPOs, or provider organizations such as IPAs, PHOs)?*
5.
LICENSURE
HOSPITAL PRIVILEGES AND OTHER AFFILIATIONS
Were you ever placed on probation, disciplined, formally reprimanded, suspended or asked to resign during an internship, resi-dency, fellowship, preceptorship or other clinical education program? If you are currently in a training program, have you beenplaced on probation, disciplined, formally reprimanded, suspended or asked to resign?*
YES NO6.
Have you ever, while under investigation or to avoid an investigation, voluntarily withdrawn or prematurely terminated your statusas a student or employee in any internship, residency, fellowship, preceptorship, or other clinical education program?*
YES NO7.
Have any of your board certifications or eligibility ever been revoked?*YES NO8.
EDUCATION, TRAINING AND BOARD CERTIFICATION
Have you ever chosen not to re-certify or voluntarily surrendered your board certification(s) while under investigation?*YES NO9.
Have your Federal DEA and/or State Controlled Dangerous Substances (CDS) certificate(s) or authorization(s) ever been chal-lenged, denied, suspended, revoked, restricted, denied renewal, or voluntarily or involuntarily relinquished?*
YES NO
DEA OR STATE CONTROLLED SUBSTANCE REGISTRATION
10.
Have you ever been disciplined, excluded from, debarred, suspended, reprimanded, sanctioned, censured, disqualified or other-wise restricted in regard to participation in the Medicare or Medicaid program, or in regard to other federal or state governmentalhealthcare plans or programs?*
YES NO
MEDICARE, MEDICAID OR OTHER GOVERNMENTAL PROGRAM PARTICIPATION
11.
YES NO
Are you currently the subject of an investigation by any hospital, licensing authority, DEA or CDS authorizing entities, educa-tion or training program, Medicare or Medicaid program, or any other private, federal or state health program or a defendantin any civil action that is reasonably related to your qualifications, competence, functions, or duties as a medical professionalfor alleged fraud, an act of violence, child abuse or a sexual offense or sexual misconduct?*
YES NO
OTHER SANCTIONS OR INVESTIGATIONS
12.
To your knowledge, has information pertaining to you ever been reported to the National Practitioner Data Bank or HealthcareIntegrity and Protection Data Bank?*
YES NO13.
Have you ever received sanctions from or are you currently the subject of investigation by any regulatory agencies (e.g., CLIA,OSHA, etc.)?*
YES NO14.
Have you ever been convicted of, pled guilty to, pled nolo contendere to, sanctioned, reprimanded, restricted, disciplined orresigned in exchange for no investigation or adverse action within the last ten years for sexual harassment or other illegalmisconduct?*
YES NO15.
Are you currently being investigated or have you ever been sanctioned, reprimanded, or cautioned by a military hospital, facility, oragency, or voluntarily terminated or resigned while under investigation or in exchange for no investigation by a hospital or health-care facility of any military agency?*
YES NO16.
Has your professional liability coverage ever been cancelled, restricted, declined or not renewed by the carrier based on yourindividual liability history?*
YES NO
PROFESSIONAL LIABILITY INSURANCE INFORMATION AND CLAIMS HISTORY
17.
Have you ever been assessed a surcharge, or rated in a high-risk class for your specialty, by your professional liability insurancecarrier, based on your individual liability history?*
YES NO18.
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
KAPER-1 (04/2009) Page 16
3093
Disclosure Questions (Continued)Section 8
DisclosureQuestionsAnswer all questions.For any “Yes”response, provide anexplanation on theSupplementalDisclosure QuestionExplanation Form onpage 34.
IMPORTANTIf you answered “Yes”to question #19, youmust complete theSupplementalMalpractice ClaimsExplanation Form onpage 35 for eachmalpractice claim.
Have you ever been convicted of, pled guilty to, or pled nolo contendere to any felony?*YES NO
CRIMINAL/CIVIL HISTORY
20.
In the past ten years have you been convicted of, pled guilty to, or pled nolo contendere to any misdemeanor (excluding minortraffic violations) or been found liable or responsible for any civil offense that is reasonably related to your qualifications, compe-tence, functions, or duties as a medical professional, or for fraud, an act of violence, child abuse or a sexual offense or sexualmisconduct?*
YES NO21.
Have you ever been court-martialed for actions related to your duties as a medical professional?*YES NO22.
Are you currently engaged in the illegal use of drugs?*("Currently" means sufficiently recent to justify a reasonable belief that the use of drugs may have an ongoing impact onone's ability to practice medicine. It is not limited to the day of, or within a matter of days or weeks before the date of applica-tion, rather that it has occurred recently enough to indicate the individual is actively engaged in such conduct. "Illegal use ofdrugs" refers to drugs whose possession or distribution is unlawful under the Controlled Substances Act, 21 U.S.C. § 812.22.It "does not include the use of a drug taken under supervision by a licensed health care professional, or other uses author-ized by the Controlled Substances Act or other provision of Federal law." The term does include, however, the unlawful use ofprescription controlled substances.)
YES NO
ABILITY TO PERFORM JOB
23.
Do you use any chemical substances that would in any way impair or limit your ability to practice medicine and perform the func-tions of your job with reasonable skill and safety?*
YES NO24.
Do you have any reason to believe that you would pose a risk to the safety or well being of your patients?*YES NO25.
Are you unable to perform the essential functions of a practitioner in your area of practice even with reasonableaccommodation?*
YES NO26.
Have you had any professional liability actions (pending, settled, arbitrated, mediated or litigated) within the past 10 years?*If yes, provide information for each case.
YES NO
MALPRACTICE CLAIMS HISTORY
19.
Note: A criminal record will not necessarily be a bar to acceptance. Decisions will be made by each health plan orcredentialing organization based upon all the relevant circumstances, including the nature of the crime.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
KAPER-1 (04/2009) Page 17
Standard Authorization, Attestation and Release(Not for Use for Employment Purposes)
I understand and agree that, as part of the credentialing application process for participation, membership and/or clinical privileges (hereinafter, referred to as"Participation") at or with each healthcare organization indicated on the "List of Authorized Organizations" that accompanies this Provider Application (hereinafter,each healthcare organization on the "List of Authorized Organizations" is individually referred to as the "Entity"), and any of the Entity's affiliated entities, I am requiredto provide sufficient and accurate information for a proper evaluation of my current licensure, relevant training and/or experience, clinical competence, health status,character, ethics, and any other criteria used by the Entity for determining initial and ongoing eligibility for Participation. Each Entity and its representatives, employ -ees, and agent(s) acknowledge that the information obtained relating to the application process will be held confidential to the extent permitted by law.
I acknowledge that each Entity has its own criteria for acceptance, and I may be accepted or rejected by each independently. I further acknowledge and understandthat my cooperation in obtaining information and my consent to the release of information do not guarantee that any Entity will grant me clinical privileges or contractwith me as a provider of services. I understand that my application for Participation with the Entity is not an application for employment with the Entity and thatacceptance of my application by the Entity will not result in my employment by the Entity.
Authorization of Investigation Concerning Application for Participation. I authorize the following individuals including, without limitation, the Entity, its representa-tives, employees, and/or designated agent(s); the Entity's affiliated entities and their representatives, employees, and/or designated agents; and the Entity's designat -ed professional credentials verification organization (collectively referred to as "Agents"), to investigate information, which includes both oral and written statements,records, and documents, concerning my application for Participation. I agree to allow the Entity and/or its Agent(s) to inspect and copy all records and documentsrelating to such an investigation.
Authorization of Third-Party Sources to Release Information Concerning Application for Participation. I authorize any third party, including, but not limited to,individuals, agencies, medical groups responsible for credentials verification, corporations, companies, employers, former employers, hospitals, health plans, healthmaintenance organizations, managed care organizations, law enforcement or licensing agencies, insurance companies, educational and other institutions, militaryservices, medical credentialing and accreditation agencies, professional medical societies, the Federation of State Medical Boards, the National Practitioner DataBank, and the Health Care Integrity and Protection Data Bank, to release to the Entity and/or its Agent(s), information, including otherwise privileged or confidentialinformation, concerning my professional qualifications, credentials, clinical competence, quality assurance and utilization data, character, mental condition, physicalcondition, alcohol or chemical dependency diagnosis and treatment, ethics, behavior, or any other matter reasonably having a bearing on my qualifications forParticipation in, or with, the Entity. I authorize my current and past professional liability carrier(s) to release my history of claims that have been made and/or are cur-rently pending against me. I specifically waive written notice from any entities and individuals who provide information based upon this Authorization, Attestation andRelease.
Authorization of Release and Exchange of Disciplinary Information. I hereby further authorize any third party at which I currently have Participation or hadParticipation and/or each third party's agents to release "Disciplinary Information," as defined below, to the Entity and/or its Agent(s). I hereby further authorize theAgent(s) to release Disciplinary Information about any disciplinary action taken against me to its participating Entities at which I have Participation, and as may beotherwise required by law. As used herein, "Disciplinary Information" means information concerning (i) any action taken by such health care organizations, theiradministrators, or their medical or other committees to revoke, deny, suspend, restrict, or condition my Participation or impose a corrective action plan; (ii) any otherdisciplinary action involving me, including, but not limited to, discipline in the employment context; or (iii) my resignation prior to the conclusion of any disciplinary pro -ceedings or prior to the commencement of formal charges, but after I have knowledge that such formal charges were being (or are being) contemplated and/or were(or are) in preparation.
Release from Liability. I release from all liability and hold harmless any Entity, its Agent(s), and any other third party for their acts performed in good faith and with-out malice unless such acts are due to the gross negligence or willful misconduct of the Entity, its Agent(s), or other third party in connection with the gathering,release and exchange of, and reliance upon, information used in accordance with this Authorization, Attestation and Release. I further agree not to sue any Entity,any Agent(s), or any other third party for their acts, defamation or any other claims based on statements made in good faith and without malice or misconduct of suchEntity, Agent(s) or third party in connection with the credentialing process. This release shall be in addition to, and in no way shall limit, any other applicable immuni-ties provided by law for peer review and credentialing activities. In this Authorization, Attestation and Release, all references to the Entity, its Agent(s), and/or otherthird party include their respective employees, directors, officers, advisors, counsel, and agents. The Entity or any of its affiliates or agents retains the right to allowaccess to the application information for purposes of a credentialing audit to customers and/or their auditors to the extent required in connection with an audit of thecredentialing processes and provided that the customer and/or their auditor executes an appropriate confidentiality agreement. I understand and agree that thisAuthorization, Attestation and Release is irrevocable for any period during which I am an applicant for Participation at an Entity, a member of an Entity's medical orhealth care staff, or a participating provider of an Entity. I agree to execute another form of consent if law or regulation limits the application of this irrevocable authori-zation. I understand that my failure to promptly provide another consent may be grounds for termination or discipline by the Entity in accordance with the applicablebylaws, rules, and regulations, and requirements of the Entity, or grounds for my termination of Participation at or with the Entity. I agree that information obtained inaccordance with the provisions of this Authorization, Attestation and Release is not and will not be a violation of my privacy.
I certify that all information provided by me in my application is current, true, correct, accurate and complete to the best of my knowledge and belief, and is furnishedin good faith. I will notify the Entity and/or its Agent(s) within 10 days of any material changes to the information (including any changes/challenges to licenses, DEA,insurance, malpractice claims, NPDB/HIPDB reports, discipline, criminal convictions, etc.) I have provided in my application or authorized to be released pursuant tothe credentialing process. I understand that corrections to the application are permitted at any time prior to a determination of Participation by the Entity, and must besubmitted online or in writing, and must be dated and signed by me (may be a written or an electronic signature). I acknowledge that the Entity will not process anapplication until they deem it to be a complete application and that I am responsible to provide a complete application and to produce adequate and timely informa-tion for resolving questions that arise in the application process. I understand and agree that any material misstatement or omission in the application may constitutegrounds for withdrawal of the application from consideration; denial or revocation of Participation; and/or immediate suspension or termination of Participation. Thisaction may be disclosed to the Entity and/or its Agent(s). I further acknowledge that I have read and understand the foregoing Authorization, Attestation and Releaseand that I have access to the bylaws of applicable medical staff organizations and agree to abide by these bylaws, rules and regulations. I understand and agree thata facsimile or photocopy of this Authorization, Attestation and Release shall be as effective as the original.
Name (print)*
3094
Signature*
DATE SIGNED*
M M D D Y Y Y Y
Std. App. v.5.0
Reprinted on 10/31/06* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
KAPER-1 (04/2009) Page 18
3095
Professional IDsSupplemental Form
Personal Information and Professional IDs Section 1
ProfessionalIDs
Include all additionalstate licenses, DEARegistration and StateControlled DangerousSubstance (CDS)certification numbers.
Provide all current andprevious licenses/certifications.
If you need to reportadditional ProfessionalIDs, photocopy thispage as needed andsubmit as instructed.
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
FEDERAL DEA NUMBER
DEA STATE OF REGISTRATION DEA EXPIRATION DATE
M M D D Y Y Y Y
DEA ISSUE DATE
M M D D Y Y Y Y
FEDERAL DEA NUMBER
DEA STATE OF REGISTRATION DEA EXPIRATION DATE
M M D D Y Y Y Y
DEA ISSUE DATE
M M D D Y Y Y Y
CDS STATE OF REGISTRATION CDS EXPIRATION DATE
M M D D Y Y Y Y
CDS ISSUE DATE
M M D D Y Y Y YCDS CERTIFICATE NUMBER
CDS STATE OF REGISTRATION CDS EXPIRATION DATE
M M D D Y Y Y Y
CDS ISSUE DATE
M M D D Y Y Y YCDS CERTIFICATE NUMBER
LICENSE ISSUING STATE LICENSE ISSUE DATE
M M D D Y Y Y Y
M M D D Y Y Y Y
STATE LICENSE NUMBER
IF THIS IS A STATE LICENSE, ARE YOUCURRENTLY PRACTICING IN THIS STATE?
YES NO
LICENSE ISSUING STATE LICENSE ISSUE DATE
M M D D Y Y Y Y
LICENSE EXPIRATION DATE
M M D D Y Y Y Y
STATE LICENSE NUMBER
IF THIS IS A STATE LICENSE, ARE YOUCURRENTLY PRACTICING IN THIS STATE?
YES NO
LICENSE STATUS CODE
Code list is found on page 36; use provider type codes. Enter3-digit code in space provided.
Code list is found on page 36; use license status codes. Enter3-digit code in space provided.
LICENSE TYPE
LICENSE EXPIRATION DATE
LICENSE STATUS CODE
Code list is found on page 36; use provider type codes. Enter3-digit code in space provided.
Code list is found on page 36; use license status codes. Enter3-digit code in space provided.
LICENSE TYPE
KAPER-1 (04/2009) Page 19
Other Relevant EducationSupplemental Form
3079
Education and TrainingSection 2
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Other RelevantEducation
If you need to reportadditional Education,photocopy this page asneeded and submit asinstructed.
Fifth PathwayEducation
NUMBER STREET SUITE/BUILDING
CITY STATE ZIP/POSTAL CODE
INSTITUTION/SCHOOL ISSUING DEGREE (DO NOT ABBREVIATE)
DEGREE AWARDEDSTART DATECOUNTRY CODE END DATE (GRADUATION DATE)
M M Y Y Y YM M Y Y Y Y
START DATE END DATE (GRADUATION DATE)
M M Y Y Y YM M Y Y Y Y
CITY
ADDRESS
INSTITUTION/HOSPITAL WHERE U.S. CLINICAL TRAINING WAS PERFORMED (DO NOT ABBREVIATE)
ZIP CODESTATE
FIFTH PATHWAY GRADUATES ONLY
TELEPHONE
- -FAX
- -
TELEPHONE
- -FAX
- -
DID YOU COMPLETE YOUREDUCATION AT THIS SCHOOL? YES NO
DID YOU COMPLETE YOUREDUCATION AT THIS SCHOOL? YES NO
DID YOU COMPLETE YOUREDUCATION AT THIS SCHOOL? YES NO
NUMBER STREET SUITE/BUILDING
CITY STATE ZIP/POSTAL CODE
INSTITUTION/SCHOOL ISSUING DEGREE (DO NOT ABBREVIATE)
DEGREE AWARDEDSTART DATECOUNTRY CODE END DATE (GRADUATION DATE)
M M Y Y Y YM M Y Y Y Y
TELEPHONE
- -FAX
- -
KAPER-1 (04/2009) Page 20
Training
List all postgraduatetraining programs youattended. Use onesection per institution.
If you need to reportadditional Training,photocopy this page asneeded and submit asinstructed.
Code lists are found onpages 36-43. Enter theassociated 3-digit codein the space provided.
Education and Training Section 2
NUMBER STREET SUITE/BUILDING
INSTITUTION / HOSPITAL NAME (USE BOTH LINES IF REQUIRED)
SCHOOL CODE (E.G.,AFFILIATED MEDICALSCHOOL)
Other TrainingSupplemental Form
COUNTRY CODE
3096
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
CITY STATE ZIP/POSTAL CODE
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
TELEPHONE
- -FAX
- -
START DATE END DATE
M M Y Y Y YM M Y Y Y YINTERNSHIP/RESIDENCY FELLOWSHIP OTHER
DEPARTMENT/SPECIALTY (DO NOT ABBREVIATE)
NAME OF DIRECTOR
NAME OF DIRECTOR
NAME OF DIRECTOR
List eachdepartmentseparately, ifapplicable.
ListInternship/Residency,Fellowshipand Otherprograms
separately.INTERNSHIP/RESIDENCY FELLOWSHIP OTHER
DEPARTMENT/SPECIALTY (DO NOT ABBREVIATE)
START DATE END DATE
M M Y Y Y YM M Y Y Y Y
INTERNSHIP/RESIDENCY FELLOWSHIP OTHER
DEPARTMENT/SPECIALTY (DO NOT ABBREVIATE)
START DATE END DATE
M M Y Y Y YM M Y Y Y Y
DID YOU COMPLETE THIS TRAINING PROGRAM AT THISINSTITUTION?
(IF NOT, PLEASE USE THE SPACE BELOW TO EXPLAIN.)
YES NO
KAPER-1 (04/2009) Page 21
Professional / Medical Specialty InformationSection 3
Additional SpecialtySupplemental Form
3097
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
AdditionalSpecialty
Code lists are found onpages 36-43. Enter theassociated 3-digit codein the space provided.
SPECIALTY CODE
BOARD CERTIFIED? YES NO
CERTIFYING BOARD CODE
RECERTIFICATION DATE
(IF APPLICABLE)M M D D Y Y Y Y
EXPIRATION DATE (IF APPLICABLE) M M D D Y Y Y Y
INITIAL CERTIFICATION
DATE M M D D Y Y Y Y YES NO
DO YOU WISH TOBE LISTED INTHE DIRECTORYUNDER THISSPECIALTY?
YES NO
YES NO
HMO
PPO
POS
IF NOTBOARD CERTIFIED(SELECTONE)
I HAVE TAKENEXAM, RESULTSPENDING FOR
CERTIFYING BOARD CODE
I INTEND TO SIT FOR ANEXAM ON
M M D D Y Y Y Y
I DO NOT INTEND TO TAKEA CERTIFYING BOARD EXAM
AdditionalSpecialty
Code lists are found onpages 36-43. Enter theassociated 3-digit codein the space provided.
If you need to reportadditional Specialties,photocopy this page asneeded and submit asinstructed.
SPECIALTY CODE
BOARD CERTIFIED? YES NO
CERTIFYING BOARD CODE
RECERTIFICATION DATE
(IF APPLICABLE)M M D D Y Y Y Y
EXPIRATION DATE (IF APPLICABLE) M M D D Y Y Y Y
INITIAL CERTIFICATION
DATE M M D D Y Y Y Y YES NO
DO YOU WISH TOBE LISTED INTHE DIRECTORYUNDER THISSPECIALTY?
YES NO
YES NO
HMO
PPO
POS
IF NOTBOARD CERTIFIED(SELECTONE)
I HAVE TAKENEXAM, RESULTSPENDING FOR
CERTIFYING BOARD CODE
I INTEND TO SIT FOR ANEXAM ON
M M D D Y Y Y Y
I DO NOT INTEND TO TAKEA CERTIFYING BOARD EXAM.
IF YOU INDICATED THAT YOU DID NOT INTEND TO TAKE A CERTIFYING BOARD EXAM, PLEASE USE THEFOLLOWING SPACE TO EXPLAIN, OTHERWISE LEAVE THE SPACE BLANK.
IF YOU INDICATED THAT YOU DID NOT INTEND TO TAKE A CERTIFYING BOARD EXAM, PLEASE USE THEFOLLOWING SPACE TO EXPLAIN, OTHERWISE LEAVE THE SPACE BLANK.
KAPER-1 (04/2009) Page 22
3098
PRIMARY PRACTICE
Partner/AssociatesUse this page toreport additionalpartners/associates atthe designatedpractice location.
IMPORTANT
In the box provided,indicate to whichpractice location thispage belongs.
Check “CoveringColleague?” if he/sheprovides coverage foryou at THIS location.
Code lists are foundon pages 36-43. Enterthe associated 3-digitcode in the spaceprovided.
If you need to reportadditionalpartners/associates,photocopy this pageas needed and submitas instructed.
Practice Location Information Section 4SPECIFY PRACTICE LOCATION INDICATE THE PRACTICE LOCATION TO WHICH YOU ARE ASSOCIATING THESE PROVIDERS.
LOCATION #PRACTICE NAME
PRACTICE ADDRESS
FIRST NAME
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
M.I.
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
M.I.
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
M.I.
FIRST NAME
LAST NAME SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
M.I.
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
M.I.
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
M.I.
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
M.I.
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
M.I.
Partners/AssociatesSupplemental Form
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
KAPER-1 (04/2009) Page 23
PRIMARY PRACTICE
3099
Covering ColleaguesSupplemental Form
CoveringColleaguesInclude all colleaguesproviding regularcoverage and his/herspecialty, including ifhe/she is a partner inone or more of yourpractice locations.
IMPORTANT
In the box provided,indicate to whichpractice location thispage belongs.
Code lists are found onpages 36-43. Enter theassociated 3-digit codein the space provided.
If you need to reportadditional CoveringColleagues, photocopythis page as neededand submit asinstructed.
Practice Location Information Section 4
LAST NAME
FIRST NAME
LAST NAME
FIRST NAME
SPECIALTY CODE
SPECIALTY CODE
LAST NAME
FIRST NAME
LAST NAME
FIRST NAME
LAST NAME
FIRST NAME
SPECIALTY CODE
SPECIALTY CODE
SPECIALTY CODE
M.I.
M.I.
M.I.
M.I.
M.I.
LAST NAME
FIRST NAME
LAST NAME
FIRST NAME
LAST NAME
FIRST NAME
SPECIALTY CODE
SPECIALTY CODE
SPECIALTY CODE
M.I.
M.I.
M.I.
SPECIFY PRACTICE LOCATION INDICATE THE PRACTICE LOCATION TO WHICH YOU ARE ASSOCIATING THESE PROVIDERS.
LOCATION #PRACTICE NAME
PRACTICE ADDRESS
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
KAPER-1 (04/2009) Page 24
3100
Practice Location InformationSupplemental Form
Practice Location Information - Page 1 of 5Section 4
AdditionalPracticeLocation
IMPORTANT
In the box provided,indicate to whichpractice location thispage belongs.
For example, if youpractice at threelocations, the primarylocation is reported inthe main applicationand remaininglocations would bereported onSupplemental Formsas Location 2 andLocation 3.
TIP Your Individual TaxID is assumed to beyour Primary Tax IDunless you specifyotherwise to the right.
LOCATION* #
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Office Manageror BusinessOffice Contact
List each contactseparately. You mayuse the check boxesbelow for convenience.Do not writeinstructions like “seeabove”. Theseresponses will berejected and willrequire follow-up.
CHECK HERE TOUSE OFFICEMANAGER ANDOFFICE ADDRESSAS BILLINGINFORMATION
NOTE:
Even if you checkedthe boxes above,please provide thee-mail address of theBilling Contact, ifavailable.
NUMBER* STREET* SUITE/BUILDING
CITY* STATE* ZIP CODE*
PHYSICIAN GROUP / PRACTICE NAME TO APPEAR IN DIRECTORY (DO NOT ABBREVIATE)*
GROUP / CORPORATE NAME AS IT APPEARS ON W-9, IF DIFFERENT FROM ABOVE (DO NOT ABBREVIATE)
TELEPHONE*
- -FAX
- -
OFFICE E-MAIL ADDRESS
SEND GENERALCORRESPON-DENCE HERE?*
YES NO
CURRENTLYPRACTICING AT THIS ADDRESS?*
YES NO M M D D Y Y Y YPREVIOUSOR FUTURESTART DATE?
INDIVIDUAL TAX ID
--GROUP TAX ID
PRIMARYTAX ID (ONE ONLY)*
-- USE INDIVIDUAL TAX ID
USE GROUP TAX ID
LAST NAME*
E-MAIL ADDRESS
FIRST NAME*
TELEPHONE*
- -FAX
- -
M.I.
CITY*
LAST NAME*
FIRST NAME*
NUMBER* STREET* SUITE/BUILDING
E-MAIL ADDRESS
TELEPHONE*
- -FAX
- -
Billing Contact
M.I.
STATE* ZIP CODE*
KAPER-1 (04/2009) Page 25
Practice Location InformationSupplemental Form
Practice Location Information - Page 2 of 5Section 4
3101
Add’l PracticeLocation (Cont.)
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
LOCATION* #
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
NOTE:
Even if you checkedthe boxes above,please provide theE-mail Address,Department Name,Electronic Billing andCheck Payable To, ifapplicable.
Office Hours
NOTE:
After hours back officetelephone will be usedonly by the health planand will not bepublished under anycircumstances.
Open PracticeStatus
CHECK HERE TOUSE OFFICEMANAGER ANDOFFICE ADDRESSAS BILLINGINFORMATION
BILLING DEPARTMENT (IF HOSPITAL-BASED)
CHECK PAYABLE TO*
ELECTRONIC BILLINGCAPABILITIES?*
YES NO
CITY*
NUMBER* STREET* SUITE/BUILDING
E-MAIL ADDRESS
TELEPHONE*
- -FAX
- -
STATE* ZIP CODE*
LAST NAME*
FIRST NAME* M.I.
(USE HHMM FORMAT AND ROUND TO THE NEAREST HALF-HOUR)
MONDAY
TUESDAY
WEDNESDAY
THURSDAY
FRIDAY
SATURDAY
SUNDAY
START END
24/7 PHONE COVERAGE?*
YES NO ANSWERINGSERVICE
IF YES
VOICE MAIL WITH INSTRUCTIONS TO CALLANSWERING SERVICE
VOICE MAIL WITH OTHERINSTRUCTIONS
AFTER HOURS BACK OFFICE TELEPHONE
- -
A=AMP=PM
A=AMP=PM
START ENDA=AMP=PM
A=AMP=PM
ACCEPT NEW PATIENTS INTO THIS PRACTICE?* YES NO
ACCEPT EXISTING PATIENTS WITH CHANGE OF PAYOR?*
IF ANY OF THEABOVE VARIES BYPLAN, EXPLAIN
YES NO
ACCEPT NEW PATIENTS WITH PHYSICIAN REFERRAL?*
ACCEPT NEW MEDICARE PATIENTS?*
ACCEPT NEW MEDICAID PATIENTS?* YES NO
ARE THERE ANYPRACTICE LIMITATIONS?*
YES NO
MALE ONLY
FEMALEONLY
NONEIF YES
YES NO
GENDER LIMITATIONS
MINIMUM AGE
MAXIMUM AGE
AGE LIMITATIONS LIST OTHER LIMITATIONS
YES NO
ACCEPT ALL NEW PATIENTS?* YES NO
Payment andRemittance
YOUR “CHECK PAYABLE TO”INFORMATION SHOULD BECONSISTENT WITH YOURW-9.
KAPER-1 (04/2009) Page 26
3102
Practice Location InformationSupplemental Form
Practice Location Information - Page 3 of 5Section 4
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
LOCATION* #
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Mid-LevelPractitioners
AdditionalPracticeLocation(Continued)
IMPORTANT
In the box provided,indicate to whichpractice location thispage belongs.
DO MID-LEVEL PRACTITIONERS (NURSE PRACTITIONERS, PHYSICIANASSISTANTS, ETC.) CARE FOR PATIENTS IN YOUR PRACTICE?* YES NO
(IF YES, PLEASE PROVIDE THE INFORMATION BELOW)
PRACTITIONER LAST NAME
PRACTITIONER FIRST NAME PRACTITIONER TYPE (E.G., PA,CNP, NP)
PRACTITIONER TYPE (E.G., PA,CNP, NP)
PRACTITIONER TYPE (E.G., PA,CNP, NP)
PRACTITIONER TYPE (E.G., PA,CNP, NP)
PRACTITIONER TYPE (E.G., PA,CNP, NP)
PRACTITIONER LICENSE / CERTIFICATE NUMBER PRACTITIONER STATE
M.I.
PRACTITIONER LAST NAME
PRACTITIONER FIRST NAME
PRACTITIONER LICENSE / CERTIFICATE NUMBER PRACTITIONER STATE
PRACTITIONER LAST NAME
PRACTITIONER FIRST NAME
PRACTITIONER LICENSE / CERTIFICATE NUMBER PRACTITIONER STATE
M.I.
M.I.
PRACTITIONER LAST NAME
PRACTITIONER FIRST NAME
PRACTITIONER LICENSE / CERTIFICATE NUMBER PRACTITIONER STATE
PRACTITIONER LAST NAME
PRACTITIONER FIRST NAME
PRACTITIONER LICENSE / CERTIFICATE NUMBER PRACTITIONER STATE
M.I.
M.I.
KAPER-1 (04/2009) Page 27
Practice Location InformationSupplemental Form
Practice Location Information - Page 4 of 5Section 4
3103
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP. Std. App. v.5.0
Reprinted on 10/31/06
LOCATION* #
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
AdditionalPracticeLocation(Continued)
IMPORTANT
In the box provided,indicate to whichpractice location thispage belongs.
NON-ENGLISH LANGUAGES SPOKEN BY OFFICE PERSONNEL
LANGUAGE CODE LANGUAGE CODE LANGUAGE CODE LANGUAGE CODE LANGUAGE CODE
LANGUAGES INTERPRETED
LANGUAGE CODE LANGUAGE CODE LANGUAGE CODE LANGUAGE CODE
INTERPRETERSAVAILABLE?*
YES NO
LANGUAGES
DOES THIS OFFICE MEET ADA ACCESSIBILITY REQUIREMENTS?* YES NO
YES NO YES NODOES THIS SITE OFFER HANDICAPPED ACCESS FOR THE FOLLOWING
DOES THIS SITE OFFER OTHER SERVICES FOR THE DISABLED?*
ACCESSIBLE BY PUBLIC TRANSPORTATION?*
BUILDING?* YES NO
PARKING?* YES NO
RESTROOM?* YES NO
OTHER HANDICAPPED ACCESS
BUS* YES NO
SUBWAY* YES NO
REGIONAL TRAIN* YES NO
OTHER TRANSPORTATION ACCESS
TEXT TELEPHONY (TTY)* YES NO
AMERICAN SIGN LANGUAGE* YES NO
MENTAL/PHYSICAL IMPAIRMENTSERVICES*
YES NO
OTHER DISABILITY SERVICES
RADIOLOGYSERVICES? YES NO
DRAWINGBLOOD? YES NO
LABORATORYSERVICES? YES NO
ALLERGYINJECTIONS? YES NO
AGEAPPROPRIATEIMMUNIZATIONS?
YES NO
ALLERGY SKINTESTING? YES NO
FLEXIBLESIGMOIDOSCOPY?
YES NO
ROUTINE OFFICEGYNECOLOGY(PELVIC/PAP)?
YES NO
TYMPANOMETRY/ AUDIOMETRYSCREENING?
YES NO
ASTHMATREATMENT? YES NO
PHYSICALTHERAPY?
OSTEOPATHICMANIPULATION?
YES NO IV HYDRATION/TREATMENT?
YES NO CARDIACSTRESS TEST?
YES NO
IF YES, PROVIDE ACCREDITING/CERTIFYING PROGRAM(E.G., CLIA, COLA, MLE)
IF YES, PROVIDE X-RAYCERTIFICATION TYPE
IF YES, WHATCLASS/CATEGORYDO YOU USE?
IF YES, WHOADMINISTERS IT?
IS ANESTHESIAADMINISTERED INYOUR OFFICE?
YES NO
EKGS? YES NO
PULMONARYFUNCTIONTESTING?
YES NO YES NO
Does this location provide any of the following services?
LAST NAME FIRST NAME
CARE OF MINORLACERATIONS?
YES NO
TYPE OF PRACTICE(SELECT ONE ONLY)* SOLO PRACTICE SINGLE SPECIALTY GROUP MULTI-SPECIALTY GROUP
ADDITIONAL OFFICE PROCEDURES PROVIDED (INCLUDING SURGICAL PROCEDURES)
Accessibilities
Services
KAPER-1 (04/2009) Page 28
3104
Practice Location InformationSupplemental Form
Section 4 Practice Location Information - Page 5 of 5
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP. Std. App. v.5.0
Reprinted on 10/31/06
LOCATION* #
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
AdditionalPracticeLocation(Continued)
IMPORTANT
In the box provided,indicate to whichpractice location thispage belongs.
If you have additionalpartners/associates atTHIS location, use thePartner/AssociateSupplemental Form onpage 23. Photocopy asnecessary. Be certainto indicate the PracticeLocation Number at thetop of the page.
Code lists are found onpages 36-43. Enter theassociated 3-digit codein the space provided.
CoveringColleagues
Code lists are found onpages 36-43. Enter theassociated 3-digit codein the space provided.
If you have additionalcovering colleaguesthat are not partners atTHIS location, use theCovering ColleaguesSupplemental Form onpage 24. Photocopy asnecessary. Be certainto indicate the PracticeLocation Number at thetop of the page.
FIRST NAME
LAST NAME
FIRST NAME
LAST NAME
FIRST NAME
SPECIALTY CODE
M.I.
LIST ALL COVERING COLLEAGUES THAT ARE NOT PARTNERS/ASSOCIATES AT THIS PRACTICE
LIST ALL PARTNERS/ASSOCIATES AT THIS PRACTICE
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
M.I.
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
PROVIDER TYPE (CODE PG 36)
M.I.
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
M.I.
FIRST NAME
LAST NAME
FIRST NAME
SPECIALTY CODE COVERINGCOLLEAGUE(Y/N)?
M.I.
M.I.
SPECIALTY CODE
LAST NAME
FIRST NAME M.I.
SPECIALTY CODE
LAST NAME
FIRST NAME M.I.
SPECIALTY CODE
KAPER-1 (04/2009) Page 29
3105
Hospital AffiliationsSection 5
HospitalPrivileges
Use this form tocontinue listinghospitals where youcurrently haveprivileges.
If you need to reportadditional space forHospital Privileges,photocopy this page asneeded and submit asinstructed.
TIP Be certain youradmission percentagesadd up to 100% forcurrent hospitals.Otherwise, you willhave to correct thiserror.
Hospital Privileges (Current)Supplemental Form
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP. Std. App. v.5.0
Reprinted on 10/31/06
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
OTHER HOSPITAL
THIS SPACE HAS BEEN PURPOSELY LEFT BLANK
HOSPITAL NAME
DEPARTMENT NAME
NUMBER STREET SUITE/BUILDING
TELEPHONE
- -FAX
- -
FULL, UNRESTRICTEDPRIVILEGES?
ARE PRIVILEGESTEMPORARY?
YES NO
ADMITTING PRIVILEGE STATUS (E.G. NONE, FULL UNRESTRICTED, PROVISIONAL, TEMPORARY)
OF YOUR TOTAL ANNUALADMISSIONS, WHAT PERCENTAGEIS TO THIS HOSPITAL?
%
STATE ZIP CODECITY
YES NO
AFFILIATION START DATE
M M Y Y Y YAFFILIATION END DATE
M M Y Y Y Y
PLEASE EXPLAINTERMINATED AFFILIATION
DEPARTMENT DIRECTOR’S LAST NAME
DEPARTMENT DIRECTOR’S FIRST NAME M.I.
KAPER-1 (04/2009) Page 30
3106
Professional Liability Insurance CarrierSection 6
OtherProfessionalLiabilityInsuranceCarrier
List secondary /second layer / future orprevious carrier(s).
For second layercoverage list name ofhospital/organizationproviding coverage
OtherProfessionalLiabilityInsuranceCarrier
List secondary /second layer / future orprevious carrier(s).
For second layercoverage list name ofhospital/organizationproviding coverage
If you need additionalspace for InsuranceCoverage, photocopythis page as neededand submit asinstructed.
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE. NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Professional Liability Insurance CarrierSupplemental Form
SELF-INSURED? YES NO
CARRIER OR SELF-INSURED NAME
DO YOU HAVE UNLIMITED COVERAGEWITH THIS INSURANCE CARRIER?
YES NO
POLICY INCLUDES TAIL COVERAGE? YES NO
, ,$AMOUNT OF COVERAGE PER OCCURRENCE
, ,$AMOUNT OF COVERAGE AGGREGATE
POLICY NUMBER*
NUMBER* STREET* SUITE/BUILDING
EFFECTIVE DATE* EXPIRATION DATE
M M Y Y Y YM M Y Y Y Y TYPE OFCOVERAGE?*
INDIVIDUAL SHARED
STATE* ZIP CODE*CITY*
ORIGINAL EFFECTIVE DATE*
M M Y Y Y Y
SELF-INSURED? YES NO
CARRIER OR SELF-INSURED NAME
DO YOU HAVE UNLIMITED COVERAGEWITH THIS INSURANCE CARRIER?
YES NO
POLICY INCLUDES TAIL COVERAGE? YES NO
, ,$
AMOUNT OF COVERAGE PER OCCURRENCE, ,
$AMOUNT OF COVERAGE AGGREGATE
POLICY NUMBER*
NUMBER* STREET* SUITE/BUILDING
EFFECTIVE DATE* EXPIRATION DATE
M M Y Y Y YM M Y Y Y Y TYPE OFCOVERAGE?*
INDIVIDUAL SHARED
STATE* ZIP CODE*CITY*
ORIGINAL EFFECTIVE DATE*
M M Y Y Y Y
KAPER-1 (04/2009) Page 31
3107
Work HistorySection 7
Work HistorySupplemental Form
Work History
Use this form tocontinue listing workhistory.
If you need additionalspace for Work History,photocopy this page asneeded and submit asinstructed.
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
START DATECOUNTRY CODE
REASON FOR DEPARTURE (IF APPLICABLE)
END DATE
M M Y Y Y YM M Y Y Y Y
TELEPHONE
- -FAX
- -
PRACTICE / EMPLOYER NAME
NUMBER STREET SUITE/BUILDING
CITY STATE ZIP/POSTAL CODE
WORK HISTORY
START DATECOUNTRY CODE
REASON FOR DEPARTURE (IF APPLICABLE)
END DATE
M M Y Y Y YM M Y Y Y Y
TELEPHONE
- -FAX
- -
PRACTICE / EMPLOYER NAME
NUMBER STREET SUITE/BUILDING
CITY STATE ZIP/POSTAL CODE
WORK HISTORY
KAPER-1 (04/2009) Page 32
3108
Professional Training / Work History Gaps Section 7
Professional Training / Work History GapsSupplemental Form
ProfessionalTraining /Work HistoryGaps
Please explain anytime periods or gaps intraining or work historythat have occurredsince graduation fromprofessional schooland are longer thanthree month in durationor of a shorter durationif required by theorganization for whichyou are beingcredentialed.
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP. Std. App. v.5.0
Reprinted on 10/31/06
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
GAP START DATE GAP END DATE M M Y Y Y YM M Y Y Y Y
GAP START DATE GAP END DATE M M Y Y Y YM M Y Y Y Y
GAP START DATE GAP END DATE M M Y Y Y YM M Y Y Y Y
GAP START DATE GAP END DATE M M Y Y Y YM M Y Y Y Y
GAP START DATE GAP END DATE M M Y Y Y YM M Y Y Y Y
KAPER-1 (04/2009) Page 33
3109
Disclosure QuestionsSection 8
DisclosureQuestionsUse this form to reportany “Yes” response toone or more of theDisclosure Questionsin Section 8. Yourresponse should notexceed the spacesprovided.
Record the questionnumber in the firstcolumn, then yourexplanation in thesecond column.
If you need additionalspace to explain a Yesresponse, photocopythis page as neededand submit asinstructed.
QUESTION # EXPLANATION
QUESTION # EXPLANATION
QUESTION # EXPLANATION
Disclosure QuestionsSupplemental Form
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
KAPER-1 (04/2009) Page 34
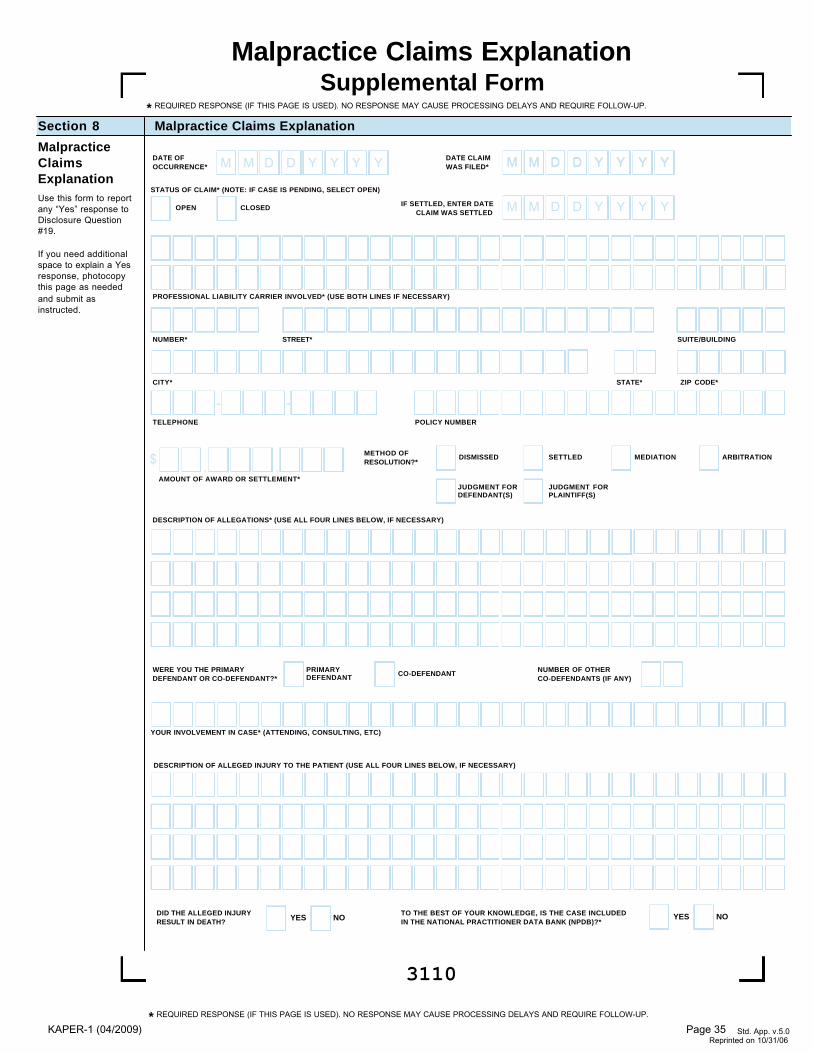
3110
Malpractice Claims ExplanationSection 8
MalpracticeClaimsExplanationUse this form to reportany “Yes” response toDisclosure Question#19.
If you need additionalspace to explain a Yesresponse, photocopythis page as neededand submit asinstructed.
Malpractice Claims ExplanationSupplemental Form
STATUS OF CLAIM* (NOTE: IF CASE IS PENDING, SELECT OPEN)
DESCRIPTION OF ALLEGATIONS* (USE ALL FOUR LINES BELOW, IF NECESSARY)
PROFESSIONAL LIABILITY CARRIER INVOLVED* (USE BOTH LINES IF NECESSARY)
NUMBER* STREET* SUITE/BUILDING
TELEPHONE
- -POLICY NUMBER
M M D D Y Y Y YDATE OFOCCURRENCE* M M D D Y Y Y YDATE CLAIM
WAS FILED*
M M D D Y Y Y Y
M M D D Y Y Y Y
IF SETTLED, ENTER DATECLAIM WAS SETTLED
, ,$AMOUNT OF AWARD OR SETTLEMENT*
METHOD OFRESOLUTION?*
DISMISSED SETTLED MEDIATION
CLOSEDOPEN
JUDGMENT FORPLAINTIFF(S)
ARBITRATION
JUDGMENT FORDEFENDANT(S)
WERE YOU THE PRIMARYDEFENDANT OR CO-DEFENDANT?*
PRIMARYDEFENDANT CO-DEFENDANT NUMBER OF OTHER
CO-DEFENDANTS (IF ANY)
YOUR INVOLVEMENT IN CASE* (ATTENDING, CONSULTING, ETC)
TO THE BEST OF YOUR KNOWLEDGE, IS THE CASE INCLUDEDIN THE NATIONAL PRACTITIONER DATA BANK (NPDB)?*
YES NODID THE ALLEGED INJURYRESULT IN DEATH?
DESCRIPTION OF ALLEGED INJURY TO THE PATIENT (USE ALL FOUR LINES BELOW, IF NECESSARY)
YES NO
STATE* ZIP CODE*CITY*
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
Std. App. v.5.0 Reprinted on 10/31/06
* REQUIRED RESPONSE (IF THIS PAGE IS USED). NO RESPONSE MAY CAUSE PROCESSING DELAYS AND REQUIRE FOLLOW-UP.
KAPER-1 (04/2009) Page 35
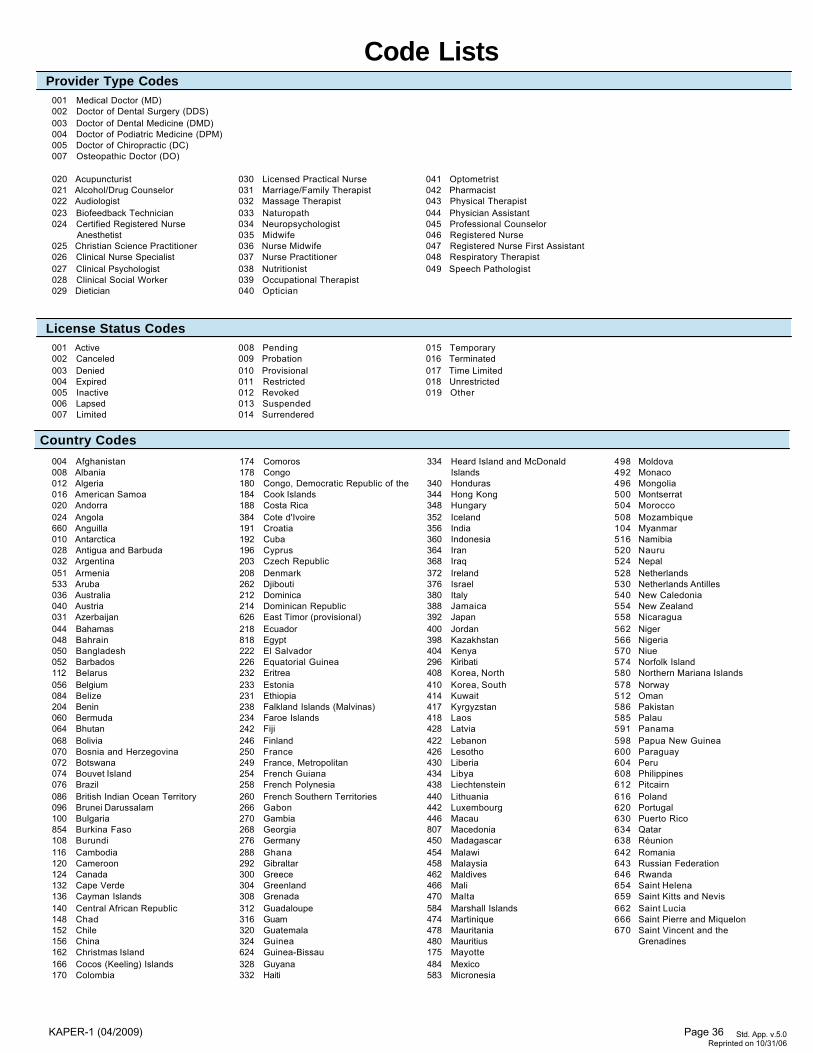
Code Lists
Std. App. v.5.0
Reprinted on 10/31/06
Provider Type Codes001 Medical Doctor (MD)002 Doctor of Dental Surgery (DDS)003 Doctor of Dental Medicine (DMD)004 Doctor of Podiatric Medicine (DPM)005 Doctor of Chiropractic (DC)007 Osteopathic Doctor (DO)
License Status Codes001 Active002 Canceled003 Denied004 Expired005 Inactive006 Lapsed007 Limited
008 Pending009 Probation010 Provisional011 Restricted012 Revoked013 Suspended014 Surrendered
015 Temporary016 Terminated017 Time Limited018 Unrestricted019 Other
020 Acupuncturist021 Alcohol/Drug Counselor022 Audiologist023 Biofeedback Technician 024 Certified Registered Nurse
Anesthetist025 Christian Science Practitioner 026 Clinical Nurse Specialist027 Clinical Psychologist028 Clinical Social Worker029 Dietician
030 Licensed Practical Nurse031 Marriage/Family Therapist 032 Massage Therapist033 Naturopath 034 Neuropsychologist035 Midwife036 Nurse Midwife 037 Nurse Practitioner038 Nutritionist039 Occupational Therapist040 Optician
041 Optometrist042 Pharmacist043 Physical Therapist 044 Physician Assistant045 Professional Counselor046 Registered Nurse047 Registered Nurse First Assistant048 Respiratory Therapist049 Speech Pathologist
Country Codes
004 Afghanistan008 Albania012 Algeria016 American Samoa020 Andorra024 Angola660 Anguilla010 Antarctica028 Antigua and Barbuda032 Argentina051 Armenia533 Aruba036 Australia040 Austria031 Azerbaijan044 Bahamas048 Bahrain050 Bangladesh052 Barbados112 Belarus056 Belgium084 Belize204 Benin060 Bermuda064 Bhutan068 Bolivia070 Bosnia and Herzegovina072 Botswana074 Bouvet Island076 Brazil086 British Indian Ocean Territory096 Brunei Darussalam100 Bulgaria854 Burkina Faso108 Burundi116 Cambodia120 Cameroon124 Canada132 Cape Verde136 Cayman Islands140 Central African Republic148 Chad152 Chile156 China162 Christmas Island166 Cocos (Keeling) Islands170 Colombia
174 Comoros178 Congo180 Congo, Democratic Republic of the 184 Cook Islands188 Costa Rica384 Cote d'Ivoire191 Croatia192 Cuba196 Cyprus203 Czech Republic208 Denmark262 Djibouti212 Dominica214 Dominican Republic626 East Timor (provisional)218 Ecuador818 Egypt222 El Salvador226 Equatorial Guinea232 Eritrea233 Estonia231 Ethiopia238 Falkland Islands (Malvinas)234 Faroe Islands242 Fiji246 Finland250 France249 France, Metropolitan254 French Guiana258 French Polynesia260 French Southern Territories266 Gabon270 Gambia268 Georgia276 Germany288 Ghana292 Gibraltar300 Greece304 Greenland308 Grenada312 Guadaloupe316 Guam320 Guatemala324 Guinea624 Guinea-Bissau328 Guyana332 Haiti
334 Heard Island and McDonald Islands
340 Honduras344 Hong Kong348 Hungary352 Iceland356 India360 Indonesia364 Iran368 Iraq372 Ireland376 Israel380 Italy388 Jamaica392 Japan400 Jordan398 Kazakhstan404 Kenya296 Kiribati408 Korea, North410 Korea, South414 Kuwait417 Kyrgyzstan418 Laos428 Latvia422 Lebanon426 Lesotho430 Liberia434 Libya438 Liechtenstein440 Lithuania442 Luxembourg446 Macau807 Macedonia450 Madagascar454 Malawi458 Malaysia462 Maldives466 Mali470 Malta584 Marshall Islands474 Martinique478 Mauritania480 Mauritius175 Mayotte484 Mexico583 Micronesia
498 Moldova492 Monaco496 Mongolia500 Montserrat504 Morocco508 Mozambique104 Myanmar516 Namibia520 Nauru524 Nepal528 Netherlands530 Netherlands Antilles540 New Caledonia554 New Zealand558 Nicaragua562 Niger566 Nigeria570 Niue574 Norfolk Island580 Northern Mariana Islands578 Norway512 Oman586 Pakistan585 Palau591 Panama598 Papua New Guinea600 Paraguay604 Peru608 Philippines612 Pitcairn616 Poland620 Portugal630 Puerto Rico634 Qatar638 Réunion642 Romania643 Russian Federation646 Rwanda654 Saint Helena659 Saint Kitts and Nevis662 Saint Lucia666 Saint Pierre and Miquelon670 Saint Vincent and the
Grenadines
KAPER-1 (04/2009) Page 36
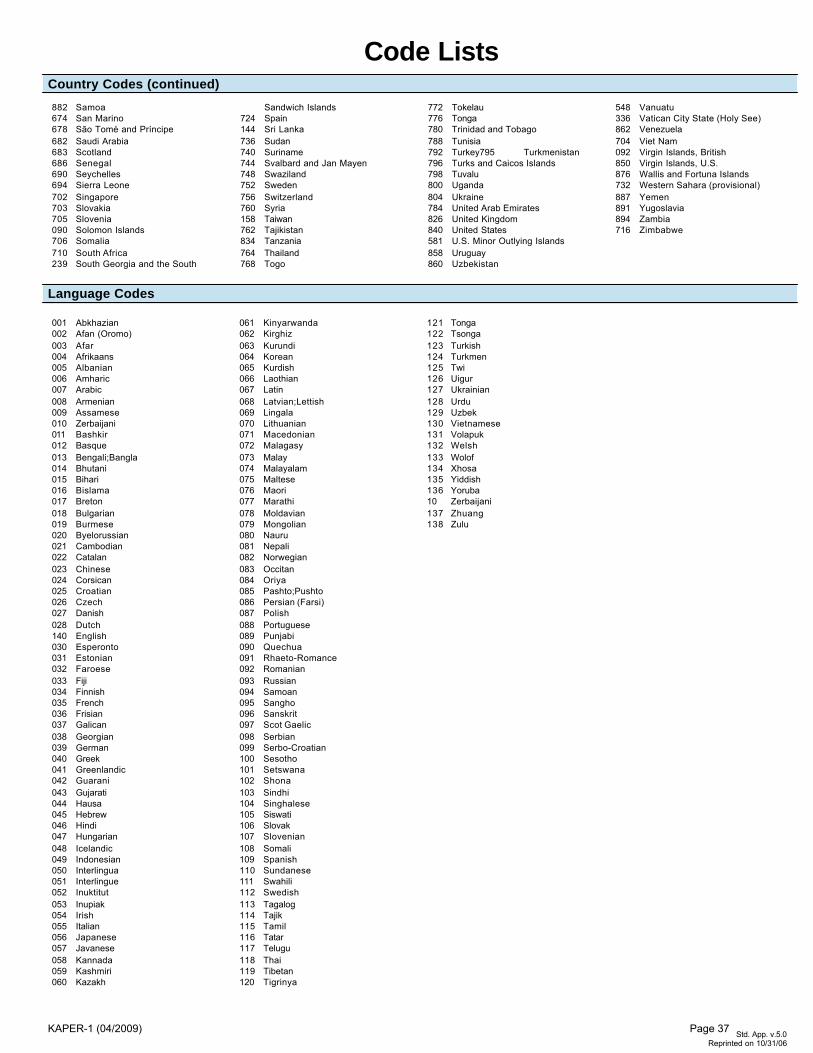
Code Lists
Language Codes
001 Abkhazian002 Afan (Oromo)003 Afar004 Afrikaans005 Albanian006 Amharic007 Arabic008 Armenian009 Assamese010 Zerbaijani011 Bashkir012 Basque013 Bengali;Bangla014 Bhutani015 Bihari016 Bislama017 Breton018 Bulgarian019 Burmese020 Byelorussian021 Cambodian022 Catalan023 Chinese024 Corsican025 Croatian026 Czech027 Danish028 Dutch140 English030 Esperonto031 Estonian032 Faroese033 Fiji034 Finnish035 French036 Frisian037 Galican038 Georgian039 German040 Greek041 Greenlandic042 Guarani043 Gujarati044 Hausa045 Hebrew046 Hindi047 Hungarian048 Icelandic049 Indonesian050 Interlingua051 Interlingue052 Inuktitut053 Inupiak054 Irish055 Italian056 Japanese057 Javanese058 Kannada059 Kashmiri060 Kazakh
061 Kinyarwanda062 Kirghiz063 Kurundi064 Korean065 Kurdish066 Laothian067 Latin068 Latvian;Lettish069 Lingala070 Lithuanian071 Macedonian072 Malagasy073 Malay074 Malayalam075 Maltese076 Maori077 Marathi078 Moldavian079 Mongolian080 Nauru081 Nepali082 Norwegian083 Occitan084 Oriya085 Pashto;Pushto086 Persian (Farsi)087 Polish088 Portuguese089 Punjabi090 Quechua091 Rhaeto-Romance092 Romanian093 Russian094 Samoan095 Sangho096 Sanskrit097 Scot Gaelic098 Serbian099 Serbo-Croatian100 Sesotho101 Setswana102 Shona103 Sindhi104 Singhalese105 Siswati106 Slovak107 Slovenian108 Somali109 Spanish110 Sundanese111 Swahili112 Swedish113 Tagalog114 Tajik115 Tamil116 Tatar117 Telugu118 Thai119 Tibetan120 Tigrinya
121 Tonga122 Tsonga123 Turkish124 Turkmen125 Twi126 Uigur127 Ukrainian128 Urdu129 Uzbek130 Vietnamese131 Volapuk132 Welsh133 Wolof134 Xhosa135 Yiddish136 Yoruba10 Zerbaijani137 Zhuang138 Zulu
Std. App. v.5.0 Reprinted on 10/31/06
882 Samoa674 San Marino678 São Tomé and Príncipe682 Saudi Arabia683 Scotland686 Senegal690 Seychelles694 Sierra Leone702 Singapore703 Slovakia705 Slovenia090 Solomon Islands706 Somalia710 South Africa239 South Georgia and the South
Sandwich Islands724 Spain144 Sri Lanka736 Sudan740 Suriname744 Svalbard and Jan Mayen748 Swaziland752 Sweden756 Switzerland760 Syria158 Taiwan762 Tajikistan834 Tanzania764 Thailand768 Togo
772 Tokelau776 Tonga780 Trinidad and Tobago788 Tunisia792 Turkey795 Turkmenistan796 Turks and Caicos Islands798 Tuvalu800 Uganda804 Ukraine784 United Arab Emirates826 United Kingdom840 United States581 U.S. Minor Outlying Islands858 Uruguay860 Uzbekistan
548 Vanuatu336 Vatican City State (Holy See)862 Venezuela704 Viet Nam092 Virgin Islands, British850 Virgin Islands, U.S.876 Wallis and Fortuna Islands732 Western Sahara (provisional)887 Yemen891 Yugoslavia894 Zambia716 Zimbabwe
Country Codes (continued)
KAPER-1 (04/2009) Page 37
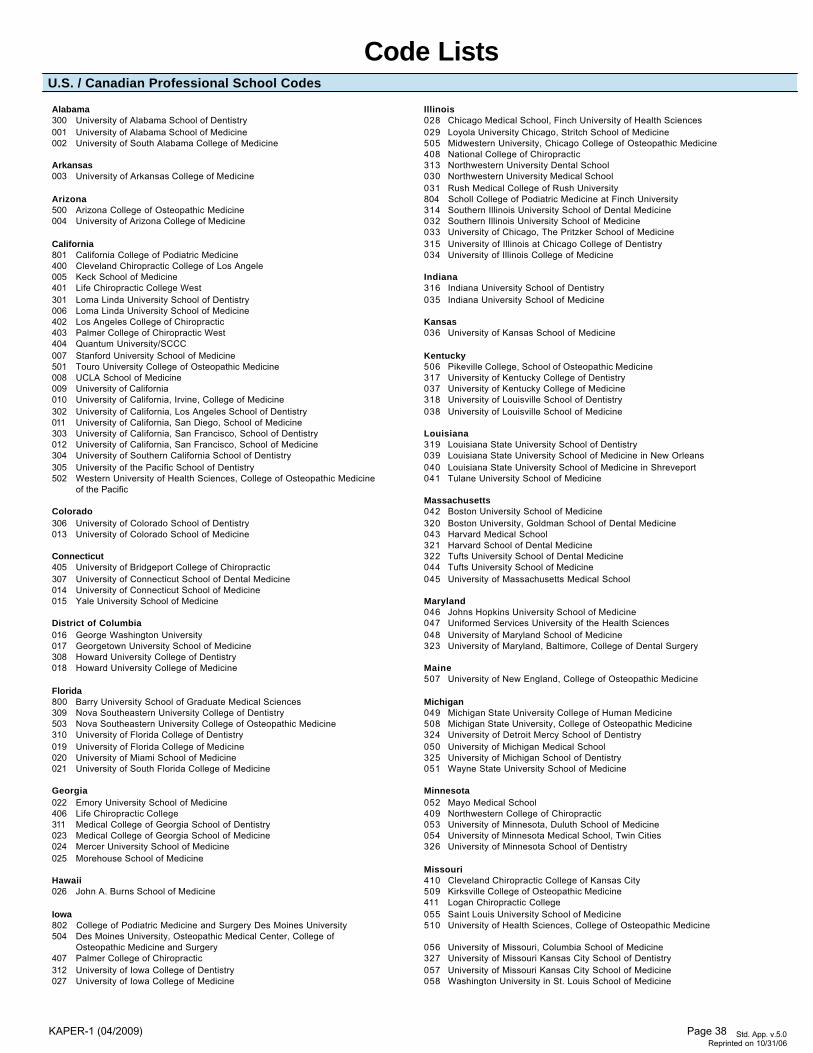
Code ListsU.S. / Canadian Professional School Codes
Alabama300 University of Alabama School of Dentistry001 University of Alabama School of Medicine002 University of South Alabama College of Medicine
Arkansas003 University of Arkansas College of Medicine
Arizona500 Arizona College of Osteopathic Medicine004 University of Arizona College of Medicine
California801 California College of Podiatric Medicine400 Cleveland Chiropractic College of Los Angele005 Keck School of Medicine401 Life Chiropractic College West301 Loma Linda University School of Dentistry006 Loma Linda University School of Medicine402 Los Angeles College of Chiropractic403 Palmer College of Chiropractic West404 Quantum University/SCCC007 Stanford University School of Medicine501 Touro University College of Osteopathic Medicine008 UCLA School of Medicine009 University of California010 University of California, Irvine, College of Medicine302 University of California, Los Angeles School of Dentistry011 University of California, San Diego, School of Medicine303 University of California, San Francisco, School of Dentistry012 University of California, San Francisco, School of Medicine304 University of Southern California School of Dentistry305 University of the Pacific School of Dentistry502 Western University of Health Sciences, College of Osteopathic Medicine
of the Pacific
Colorado306 University of Colorado School of Dentistry013 University of Colorado School of Medicine
Connecticut405 University of Bridgeport College of Chiropractic307 University of Connecticut School of Dental Medicine014 University of Connecticut School of Medicine015 Yale University School of Medicine
District of Columbia016 George Washington University017 Georgetown University School of Medicine308 Howard University College of Dentistry018 Howard University College of Medicine
Florida800 Barry University School of Graduate Medical Sciences309 Nova Southeastern University College of Dentistry503 Nova Southeastern University College of Osteopathic Medicine310 University of Florida College of Dentistry019 University of Florida College of Medicine020 University of Miami School of Medicine021 University of South Florida College of Medicine
Georgia022 Emory University School of Medicine406 Life Chiropractic College311 Medical College of Georgia School of Dentistry023 Medical College of Georgia School of Medicine024 Mercer University School of Medicine025 Morehouse School of Medicine
Hawaii026 John A. Burns School of Medicine
Iowa802 College of Podiatric Medicine and Surgery Des Moines University504 Des Moines University, Osteopathic Medical Center, College of
Osteopathic Medicine and Surgery 407 Palmer College of Chiropractic312 University of Iowa College of Dentistry027 University of Iowa College of Medicine
Illinois028 Chicago Medical School, Finch University of Health Sciences029 Loyola University Chicago, Stritch School of Medicine505 Midwestern University, Chicago College of Osteopathic Medicine408 National College of Chiropractic313 Northwestern University Dental School030 Northwestern University Medical School031 Rush Medical College of Rush University804 Scholl College of Podiatric Medicine at Finch University314 Southern Illinois University School of Dental Medicine032 Southern Illinois University School of Medicine033 University of Chicago, The Pritzker School of Medicine315 University of Illinois at Chicago College of Dentistry034 University of Illinois College of Medicine
Indiana316 Indiana University School of Dentistry035 Indiana University School of Medicine
Kansas036 University of Kansas School of Medicine
Kentucky506 Pikeville College, School of Osteopathic Medicine 317 University of Kentucky College of Dentistry037 University of Kentucky College of Medicine318 University of Louisville School of Dentistry038 University of Louisville School of Medicine
Louisiana319 Louisiana State University School of Dentistry039 Louisiana State University School of Medicine in New Orleans040 Louisiana State University School of Medicine in Shreveport041 Tulane University School of Medicine
Massachusetts042 Boston University School of Medicine320 Boston University, Goldman School of Dental Medicine043 Harvard Medical School321 Harvard School of Dental Medicine322 Tufts University School of Dental Medicine044 Tufts University School of Medicine045 University of Massachusetts Medical School
Maryland046 Johns Hopkins University School of Medicine047 Uniformed Services University of the Health Sciences048 University of Maryland School of Medicine323 University of Maryland, Baltimore, College of Dental Surgery
Maine507 University of New England, College of Osteopathic Medicine
Michigan049 Michigan State University College of Human Medicine508 Michigan State University, College of Osteopathic Medicine324 University of Detroit Mercy School of Dentistry050 University of Michigan Medical School325 University of Michigan School of Dentistry051 Wayne State University School of Medicine
Minnesota052 Mayo Medical School409 Northwestern College of Chiropractic053 University of Minnesota, Duluth School of Medicine054 University of Minnesota Medical School, Twin Cities326 University of Minnesota School of Dentistry
Missouri410 Cleveland Chiropractic College of Kansas City509 Kirksville College of Osteopathic Medicine 411 Logan Chiropractic College055 Saint Louis University School of Medicine510 University of Health Sciences, College of Osteopathic Medicine
056 University of Missouri, Columbia School of Medicine327 University of Missouri Kansas City School of Dentistry057 University of Missouri Kansas City School of Medicine058 Washington University in St. Louis School of Medicine
Std. App. v.5.0 Reprinted on 10/31/06
KAPER-1 (04/2009) Page 38
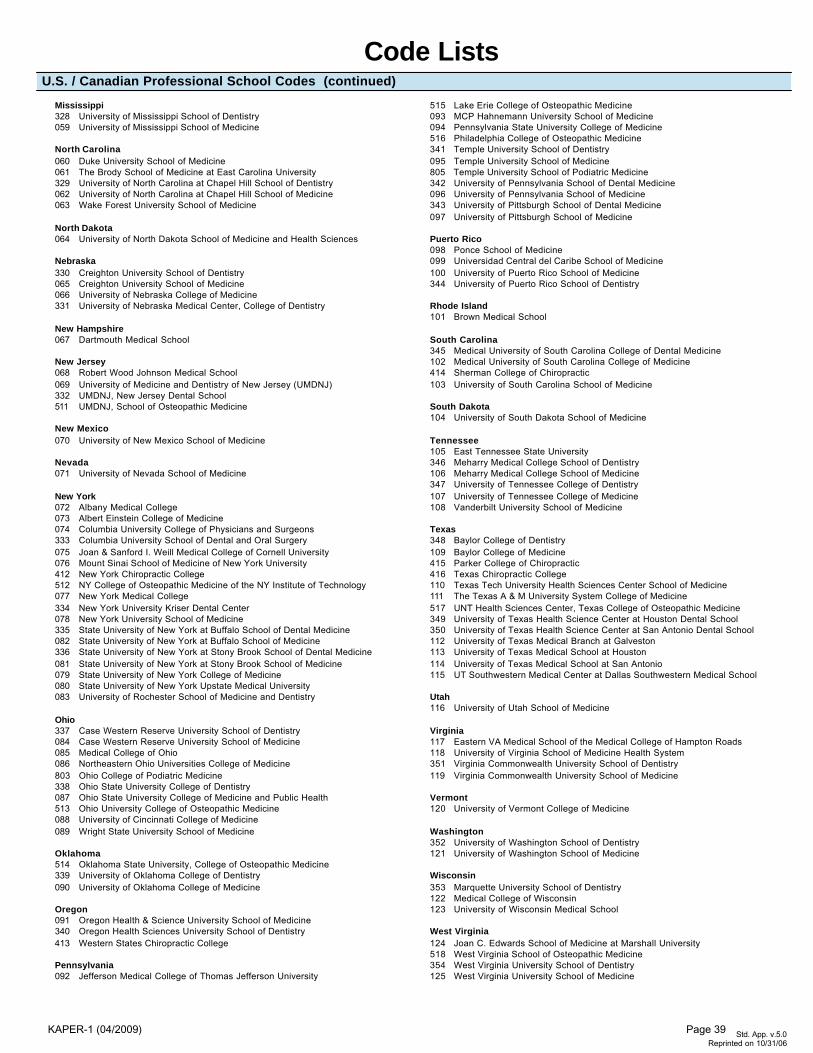
Mississippi328 University of Mississippi School of Dentistry059 University of Mississippi School of Medicine
North Carolina060 Duke University School of Medicine061 The Brody School of Medicine at East Carolina University329 University of North Carolina at Chapel Hill School of Dentistry062 University of North Carolina at Chapel Hill School of Medicine063 Wake Forest University School of Medicine
North Dakota064 University of North Dakota School of Medicine and Health Sciences
Nebraska330 Creighton University School of Dentistry065 Creighton University School of Medicine066 University of Nebraska College of Medicine331 University of Nebraska Medical Center, College of Dentistry
New Hampshire067 Dartmouth Medical School
New Jersey068 Robert Wood Johnson Medical School069 University of Medicine and Dentistry of New Jersey (UMDNJ)332 UMDNJ, New Jersey Dental School511 UMDNJ, School of Osteopathic Medicine
New Mexico070 University of New Mexico School of Medicine
Nevada071 University of Nevada School of Medicine
New York072 Albany Medical College073 Albert Einstein College of Medicine074 Columbia University College of Physicians and Surgeons333 Columbia University School of Dental and Oral Surgery075 Joan & Sanford I. Weill Medical College of Cornell University076 Mount Sinai School of Medicine of New York University412 New York Chiropractic College512 NY College of Osteopathic Medicine of the NY Institute of Technology077 New York Medical College334 New York University Kriser Dental Center078 New York University School of Medicine335 State University of New York at Buffalo School of Dental Medicine082 State University of New York at Buffalo School of Medicine336 State University of New York at Stony Brook School of Dental Medicine081 State University of New York at Stony Brook School of Medicine079 State University of New York College of Medicine080 State University of New York Upstate Medical University083 University of Rochester School of Medicine and Dentistry
Ohio337 Case Western Reserve University School of Dentistry084 Case Western Reserve University School of Medicine085 Medical College of Ohio086 Northeastern Ohio Universities College of Medicine803 Ohio College of Podiatric Medicine338 Ohio State University College of Dentistry087 Ohio State University College of Medicine and Public Health513 Ohio University College of Osteopathic Medicine088 University of Cincinnati College of Medicine089 Wright State University School of Medicine
Oklahoma514 Oklahoma State University, College of Osteopathic Medicine339 University of Oklahoma College of Dentistry090 University of Oklahoma College of Medicine
Oregon091 Oregon Health & Science University School of Medicine340 Oregon Health Sciences University School of Dentistry413 Western States Chiropractic College
Pennsylvania092 Jefferson Medical College of Thomas Jefferson University
515 Lake Erie College of Osteopathic Medicine093 MCP Hahnemann University School of Medicine094 Pennsylvania State University College of Medicine516 Philadelphia College of Osteopathic Medicine 341 Temple University School of Dentistry095 Temple University School of Medicine805 Temple University School of Podiatric Medicine342 University of Pennsylvania School of Dental Medicine096 University of Pennsylvania School of Medicine343 University of Pittsburgh School of Dental Medicine097 University of Pittsburgh School of Medicine
Puerto Rico098 Ponce School of Medicine099 Universidad Central del Caribe School of Medicine100 University of Puerto Rico School of Medicine344 University of Puerto Rico School of Dentistry
Rhode Island101 Brown Medical School
South Carolina345 Medical University of South Carolina College of Dental Medicine102 Medical University of South Carolina College of Medicine414 Sherman College of Chiropractic103 University of South Carolina School of Medicine
South Dakota104 University of South Dakota School of Medicine
Tennessee105 East Tennessee State University346 Meharry Medical College School of Dentistry106 Meharry Medical College School of Medicine347 University of Tennessee College of Dentistry107 University of Tennessee College of Medicine108 Vanderbilt University School of Medicine
Texas348 Baylor College of Dentistry109 Baylor College of Medicine415 Parker College of Chiropractic416 Texas Chiropractic College110 Texas Tech University Health Sciences Center School of Medicine111 The Texas A & M University System College of Medicine517 UNT Health Sciences Center, Texas College of Osteopathic Medicine 349 University of Texas Health Science Center at Houston Dental School350 University of Texas Health Science Center at San Antonio Dental School112 University of Texas Medical Branch at Galveston113 University of Texas Medical School at Houston114 University of Texas Medical School at San Antonio115 UT Southwestern Medical Center at Dallas Southwestern Medical School
Utah116 University of Utah School of Medicine
Virginia117 Eastern VA Medical School of the Medical College of Hampton Roads118 University of Virginia School of Medicine Health System351 Virginia Commonwealth University School of Dentistry119 Virginia Commonwealth University School of Medicine
Vermont120 University of Vermont College of Medicine
Washington352 University of Washington School of Dentistry121 University of Washington School of Medicine
Wisconsin353 Marquette University School of Dentistry122 Medical College of Wisconsin123 University of Wisconsin Medical School
West Virginia124 Joan C. Edwards School of Medicine at Marshall University518 West Virginia School of Osteopathic Medicine 354 West Virginia University School of Dentistry125 West Virginia University School of Medicine
U.S. / Canadian Professional School Codes (continued)
Code Lists
Std. App. v.5.0
Reprinted on 10/31/06KAPER-1 (04/2009) Page 39
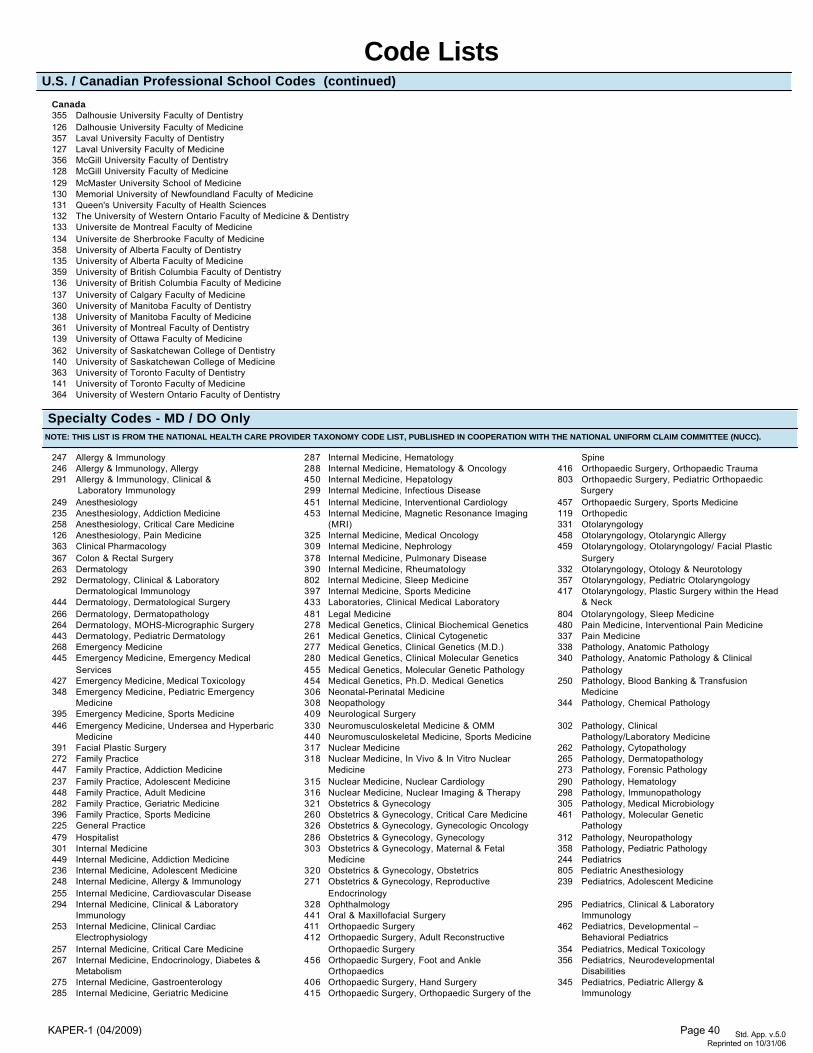
Canada355 Dalhousie University Faculty of Dentistry126 Dalhousie University Faculty of Medicine357 Laval University Faculty of Dentistry127 Laval University Faculty of Medicine356 McGill University Faculty of Dentistry128 McGill University Faculty of Medicine129 McMaster University School of Medicine130 Memorial University of Newfoundland Faculty of Medicine131 Queen's University Faculty of Health Sciences132 The University of Western Ontario Faculty of Medicine & Dentistry133 Universite de Montreal Faculty of Medicine134 Universite de Sherbrooke Faculty of Medicine358 University of Alberta Faculty of Dentistry135 University of Alberta Faculty of Medicine359 University of British Columbia Faculty of Dentistry136 University of British Columbia Faculty of Medicine137 University of Calgary Faculty of Medicine360 University of Manitoba Faculty of Dentistry138 University of Manitoba Faculty of Medicine361 University of Montreal Faculty of Dentistry139 University of Ottawa Faculty of Medicine362 University of Saskatchewan College of Dentistry140 University of Saskatchewan College of Medicine363 University of Toronto Faculty of Dentistry141 University of Toronto Faculty of Medicine364 University of Western Ontario Faculty of Dentistry
U.S. / Canadian Professional School Codes (continued)
Code Lists
Specialty Codes - MD / DO Only
247 Allergy & Immunology246 Allergy & Immunology, Allergy291 Allergy & Immunology, Clinical &
Laboratory Immunology249 Anesthesiology235 Anesthesiology, Addiction Medicine258 Anesthesiology, Critical Care Medicine126 Anesthesiology, Pain Medicine363 Clinical Pharmacology367 Colon & Rectal Surgery263 Dermatology292 Dermatology, Clinical & Laboratory
Dermatological Immunology444 Dermatology, Dermatological Surgery266 Dermatology, Dermatopathology264 Dermatology, MOHS-Micrographic Surgery443 Dermatology, Pediatric Dermatology268 Emergency Medicine445 Emergency Medicine, Emergency Medical
Services427 Emergency Medicine, Medical Toxicology348 Emergency Medicine, Pediatric Emergency
Medicine395 Emergency Medicine, Sports Medicine446 Emergency Medicine, Undersea and Hyperbaric
Medicine391 Facial Plastic Surgery272 Family Practice447 Family Practice, Addiction Medicine237 Family Practice, Adolescent Medicine448 Family Practice, Adult Medicine282 Family Practice, Geriatric Medicine396 Family Practice, Sports Medicine225 General Practice479 Hospitalist301 Internal Medicine449 Internal Medicine, Addiction Medicine236 Internal Medicine, Adolescent Medicine248 Internal Medicine, Allergy & Immunology255 Internal Medicine, Cardiovascular Disease294 Internal Medicine, Clinical & Laboratory
Immunology253 Internal Medicine, Clinical Cardiac
Electrophysiology257 Internal Medicine, Critical Care Medicine267 Internal Medicine, Endocrinology, Diabetes &
Metabolism275 Internal Medicine, Gastroenterology285 Internal Medicine, Geriatric Medicine
287 Internal Medicine, Hematology288 Internal Medicine, Hematology & Oncology450 Internal Medicine, Hepatology299 Internal Medicine, Infectious Disease451 Internal Medicine, Interventional Cardiology453 Internal Medicine, Magnetic Resonance Imaging
(MRI)325 Internal Medicine, Medical Oncology309 Internal Medicine, Nephrology378 Internal Medicine, Pulmonary Disease390 Internal Medicine, Rheumatology802 Internal Medicine, Sleep Medicine397 Internal Medicine, Sports Medicine433 Laboratories, Clinical Medical Laboratory481 Legal Medicine278 Medical Genetics, Clinical Biochemical Genetics261 Medical Genetics, Clinical Cytogenetic277 Medical Genetics, Clinical Genetics (M.D.)280 Medical Genetics, Clinical Molecular Genetics455 Medical Genetics, Molecular Genetic Pathology454 Medical Genetics, Ph.D. Medical Genetics306 Neonatal-Perinatal Medicine308 Neopathology409 Neurological Surgery330 Neuromusculoskeletal Medicine & OMM440 Neuromusculoskeletal Medicine, Sports Medicine317 Nuclear Medicine318 Nuclear Medicine, In Vivo & In Vitro Nuclear
Medicine315 Nuclear Medicine, Nuclear Cardiology316 Nuclear Medicine, Nuclear Imaging & Therapy321 Obstetrics & Gynecology260 Obstetrics & Gynecology, Critical Care Medicine326 Obstetrics & Gynecology, Gynecologic Oncology286 Obstetrics & Gynecology, Gynecology303 Obstetrics & Gynecology, Maternal & Fetal
Medicine320 Obstetrics & Gynecology, Obstetrics271 Obstetrics & Gynecology, Reproductive
Endocrinology328 Ophthalmology441 Oral & Maxillofacial Surgery411 Orthopaedic Surgery412 Orthopaedic Surgery, Adult Reconstructive
Orthopaedic Surgery456 Orthopaedic Surgery, Foot and Ankle
Orthopaedics406 Orthopaedic Surgery, Hand Surgery415 Orthopaedic Surgery, Orthopaedic Surgery of the
Spine416 Orthopaedic Surgery, Orthopaedic Trauma803 Orthopaedic Surgery, Pediatric Orthopaedic
Surgery457 Orthopaedic Surgery, Sports Medicine119 Orthopedic331 Otolaryngology458 Otolaryngology, Otolaryngic Allergy459 Otolaryngology, Otolaryngology/ Facial Plastic
Surgery332 Otolaryngology, Otology & Neurotology357 Otolaryngology, Pediatric Otolaryngology417 Otolaryngology, Plastic Surgery within the Head
& Neck804 Otolaryngology, Sleep Medicine480 Pain Medicine, Interventional Pain Medicine337 Pain Medicine338 Pathology, Anatomic Pathology340 Pathology, Anatomic Pathology & Clinical
Pathology250 Pathology, Blood Banking & Transfusion
Medicine344 Pathology, Chemical Pathology
302 Pathology, Clinical Pathology/Laboratory Medicine
262 Pathology, Cytopathology265 Pathology, Dermatopathology273 Pathology, Forensic Pathology290 Pathology, Hematology298 Pathology, Immunopathology305 Pathology, Medical Microbiology461 Pathology, Molecular Genetic
Pathology312 Pathology, Neuropathology358 Pathology, Pediatric Pathology244 Pediatrics805 Pediatric Anesthesiology 239 Pediatrics, Adolescent Medicine
295 Pediatrics, Clinical & Laboratory Immunology
462 Pediatrics, Developmental – Behavioral Pediatrics
354 Pediatrics, Medical Toxicology356 Pediatrics, Neurodevelopmental
Disabilities345 Pediatrics, Pediatric Allergy &
Immunology
Std. App. v.5.0 Reprinted on 10/31/06
NOTE: THIS LIST IS FROM THE NATIONAL HEALTH CARE PROVIDER TAXONOMY CODE LIST, PUBLISHED IN COOPERATION WITH THE NATIONAL UNIFORM CLAIM COMMITTEE (NUCC).
KAPER-1 (04/2009) Page 40
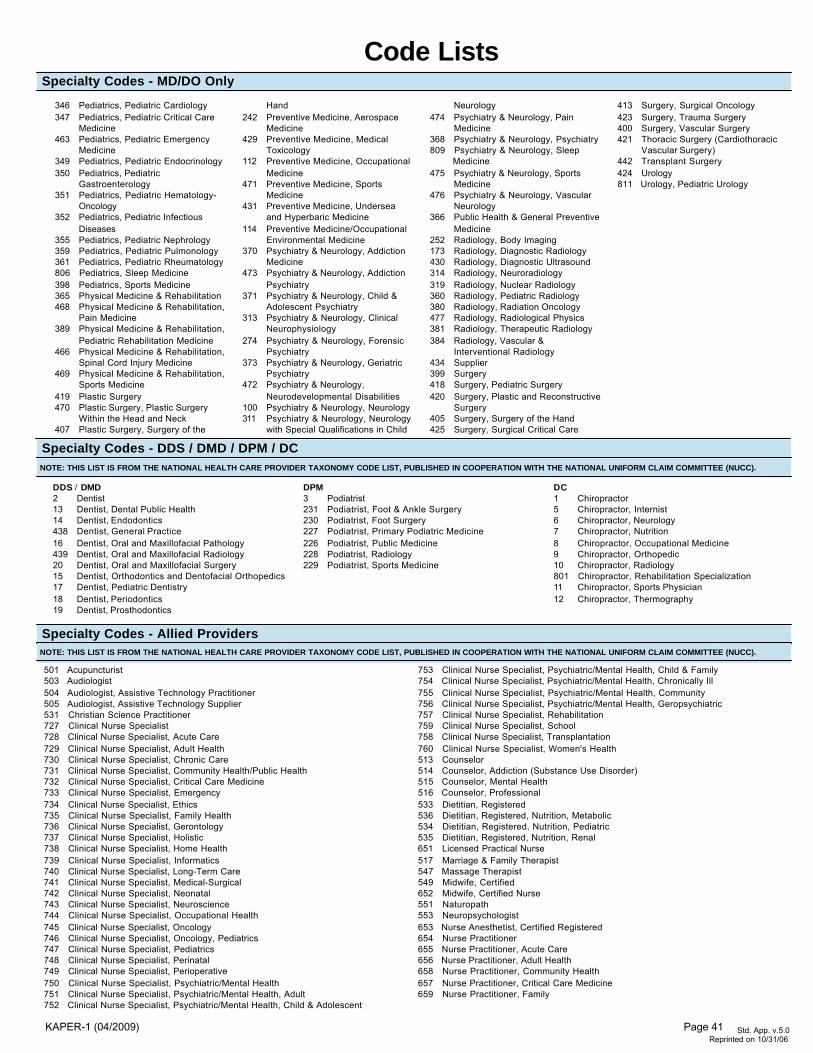
Specialty Codes - MD/DO Only
Code Lists
346 Pediatrics, Pediatric Cardiology347 Pediatrics, Pediatric Critical Care
Medicine463 Pediatrics, Pediatric Emergency
Medicine349 Pediatrics, Pediatric Endocrinology350 Pediatrics, Pediatric
Gastroenterology351 Pediatrics, Pediatric Hematology-
Oncology352 Pediatrics, Pediatric Infectious
Diseases355 Pediatrics, Pediatric Nephrology359 Pediatrics, Pediatric Pulmonology361 Pediatrics, Pediatric Rheumatology806 Pediatrics, Sleep Medicine398 Pediatrics, Sports Medicine365 Physical Medicine & Rehabilitation468 Physical Medicine & Rehabilitation,
Pain Medicine389 Physical Medicine & Rehabilitation,
Pediatric Rehabilitation Medicine466 Physical Medicine & Rehabilitation,
Spinal Cord Injury Medicine469 Physical Medicine & Rehabilitation,
Sports Medicine419 Plastic Surgery470 Plastic Surgery, Plastic Surgery
Within the Head and Neck407 Plastic Surgery, Surgery of the
Hand242 Preventive Medicine, Aerospace
Medicine429 Preventive Medicine, Medical
Toxicology112 Preventive Medicine, Occupational
Medicine471 Preventive Medicine, Sports
Medicine431 Preventive Medicine, Undersea
and Hyperbaric Medicine114 Preventive Medicine/Occupational
Environmental Medicine370 Psychiatry & Neurology, Addiction
Medicine473 Psychiatry & Neurology, Addiction
Psychiatry371 Psychiatry & Neurology, Child &
Adolescent Psychiatry313 Psychiatry & Neurology, Clinical
Neurophysiology274 Psychiatry & Neurology, Forensic
Psychiatry373 Psychiatry & Neurology, Geriatric
Psychiatry472 Psychiatry & Neurology,
Neurodevelopmental Disabilities100 Psychiatry & Neurology, Neurology311 Psychiatry & Neurology, Neurology
with Special Qualifications in Child
Neurology474 Psychiatry & Neurology, Pain
Medicine368 Psychiatry & Neurology, Psychiatry809 Psychiatry & Neurology, Sleep
Medicine475 Psychiatry & Neurology, Sports
Medicine476 Psychiatry & Neurology, Vascular
Neurology366 Public Health & General Preventive
Medicine252 Radiology, Body Imaging173 Radiology, Diagnostic Radiology430 Radiology, Diagnostic Ultrasound314 Radiology, Neuroradiology319 Radiology, Nuclear Radiology360 Radiology, Pediatric Radiology380 Radiology, Radiation Oncology477 Radiology, Radiological Physics381 Radiology, Therapeutic Radiology384 Radiology, Vascular &
Interventional Radiology434 Supplier399 Surgery418 Surgery, Pediatric Surgery420 Surgery, Plastic and Reconstructive
Surgery405 Surgery, Surgery of the Hand425 Surgery, Surgical Critical Care
413 Surgery, Surgical Oncology423 Surgery, Trauma Surgery400 Surgery, Vascular Surgery421 Thoracic Surgery (Cardiothoracic
Vascular Surgery)442 Transplant Surgery424 Urology811 Urology, Pediatric Urology
DDS / DMD2 Dentist13 Dentist, Dental Public Health14 Dentist, Endodontics438 Dentist, General Practice16 Dentist, Oral and Maxillofacial Pathology439 Dentist, Oral and Maxillofacial Radiology20 Dentist, Oral and Maxillofacial Surgery15 Dentist, Orthodontics and Dentofacial Orthopedics17 Dentist, Pediatric Dentistry18 Dentist, Periodontics19 Dentist, Prosthodontics
DPM3 Podiatrist231 Podiatrist, Foot & Ankle Surgery230 Podiatrist, Foot Surgery227 Podiatrist, Primary Podiatric Medicine226 Podiatrist, Public Medicine228 Podiatrist, Radiology229 Podiatrist, Sports Medicine
DC1 Chiropractor5 Chiropractor, Internist6 Chiropractor, Neurology7 Chiropractor, Nutrition8 Chiropractor, Occupational Medicine9 Chiropractor, Orthopedic10 Chiropractor, Radiology801 Chiropractor, Rehabilitation Specialization11 Chiropractor, Sports Physician12 Chiropractor, Thermography
Specialty Codes - Allied Providers
Specialty Codes - DDS / DMD / DPM / DC
501 Acupuncturist503 Audiologist504 Audiologist, Assistive Technology Practitioner505 Audiologist, Assistive Technology Supplier531 Christian Science Practitioner727 Clinical Nurse Specialist728 Clinical Nurse Specialist, Acute Care729 Clinical Nurse Specialist, Adult Health730 Clinical Nurse Specialist, Chronic Care731 Clinical Nurse Specialist, Community Health/Public Health732 Clinical Nurse Specialist, Critical Care Medicine733 Clinical Nurse Specialist, Emergency734 Clinical Nurse Specialist, Ethics735 Clinical Nurse Specialist, Family Health736 Clinical Nurse Specialist, Gerontology737 Clinical Nurse Specialist, Holistic738 Clinical Nurse Specialist, Home Health739 Clinical Nurse Specialist, Informatics740 Clinical Nurse Specialist, Long-Term Care741 Clinical Nurse Specialist, Medical-Surgical742 Clinical Nurse Specialist, Neonatal743 Clinical Nurse Specialist, Neuroscience744 Clinical Nurse Specialist, Occupational Health745 Clinical Nurse Specialist, Oncology746 Clinical Nurse Specialist, Oncology, Pediatrics747 Clinical Nurse Specialist, Pediatrics748 Clinical Nurse Specialist, Perinatal749 Clinical Nurse Specialist, Perioperative750 Clinical Nurse Specialist, Psychiatric/Mental Health751 Clinical Nurse Specialist, Psychiatric/Mental Health, Adult752 Clinical Nurse Specialist, Psychiatric/Mental Health, Child & Adolescent
753 Clinical Nurse Specialist, Psychiatric/Mental Health, Child & Family754 Clinical Nurse Specialist, Psychiatric/Mental Health, Chronically Ill755 Clinical Nurse Specialist, Psychiatric/Mental Health, Community756 Clinical Nurse Specialist, Psychiatric/Mental Health, Geropsychiatric757 Clinical Nurse Specialist, Rehabilitation759 Clinical Nurse Specialist, School758 Clinical Nurse Specialist, Transplantation760 Clinical Nurse Specialist, Women's Health513 Counselor514 Counselor, Addiction (Substance Use Disorder)515 Counselor, Mental Health516 Counselor, Professional533 Dietitian, Registered536 Dietitian, Registered, Nutrition, Metabolic534 Dietitian, Registered, Nutrition, Pediatric535 Dietitian, Registered, Nutrition, Renal651 Licensed Practical Nurse517 Marriage & Family Therapist547 Massage Therapist549 Midwife, Certified652 Midwife, Certified Nurse551 Naturopath553 Neuropsychologist653 Nurse Anesthetist, Certified Registered654 Nurse Practitioner655 Nurse Practitioner, Acute Care656 Nurse Practitioner, Adult Health658 Nurse Practitioner, Community Health657 Nurse Practitioner, Critical Care Medicine659 Nurse Practitioner, Family
NOTE: THIS LIST IS FROM THE NATIONAL HEALTH CARE PROVIDER TAXONOMY CODE LIST, PUBLISHED IN COOPERATION WITH THE NATIONAL UNIFORM CLAIM COMMITTEE (NUCC).
NOTE: THIS LIST IS FROM THE NATIONAL HEALTH CARE PROVIDER TAXONOMY CODE LIST, PUBLISHED IN COOPERATION WITH THE NATIONAL UNIFORM CLAIM COMMITTEE (NUCC).
Std. App. v.5.0 Reprinted on 10/31/06
KAPER-1 (04/2009) Page 41
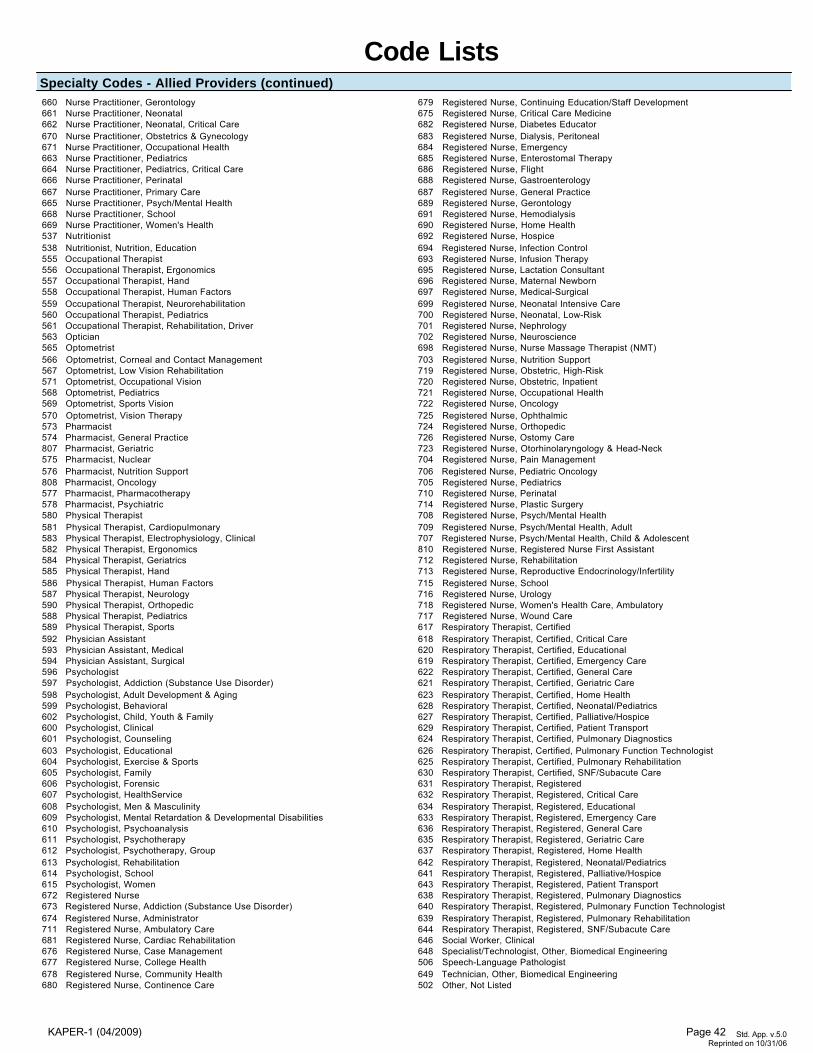
Code Lists
Std. App. v.5.0 Reprinted on 10/31/06
Specialty Codes - Allied Providers (continued) 660 Nurse Practitioner, Gerontology661 Nurse Practitioner, Neonatal662 Nurse Practitioner, Neonatal, Critical Care670 Nurse Practitioner, Obstetrics & Gynecology671 Nurse Practitioner, Occupational Health663 Nurse Practitioner, Pediatrics664 Nurse Practitioner, Pediatrics, Critical Care666 Nurse Practitioner, Perinatal667 Nurse Practitioner, Primary Care665 Nurse Practitioner, Psych/Mental Health668 Nurse Practitioner, School669 Nurse Practitioner, Women's Health537 Nutritionist538 Nutritionist, Nutrition, Education555 Occupational Therapist556 Occupational Therapist, Ergonomics557 Occupational Therapist, Hand558 Occupational Therapist, Human Factors559 Occupational Therapist, Neurorehabilitation560 Occupational Therapist, Pediatrics561 Occupational Therapist, Rehabilitation, Driver563 Optician565 Optometrist566 Optometrist, Corneal and Contact Management567 Optometrist, Low Vision Rehabilitation571 Optometrist, Occupational Vision568 Optometrist, Pediatrics569 Optometrist, Sports Vision570 Optometrist, Vision Therapy573 Pharmacist574 Pharmacist, General Practice807 Pharmacist, Geriatric575 Pharmacist, Nuclear 576 Pharmacist, Nutrition Support808 Pharmacist, Oncology577 Pharmacist, Pharmacotherapy578 Pharmacist, Psychiatric580 Physical Therapist581 Physical Therapist, Cardiopulmonary583 Physical Therapist, Electrophysiology, Clinical582 Physical Therapist, Ergonomics584 Physical Therapist, Geriatrics585 Physical Therapist, Hand586 Physical Therapist, Human Factors587 Physical Therapist, Neurology590 Physical Therapist, Orthopedic588 Physical Therapist, Pediatrics589 Physical Therapist, Sports592 Physician Assistant593 Physician Assistant, Medical594 Physician Assistant, Surgical596 Psychologist597 Psychologist, Addiction (Substance Use Disorder)598 Psychologist, Adult Development & Aging599 Psychologist, Behavioral602 Psychologist, Child, Youth & Family600 Psychologist, Clinical601 Psychologist, Counseling603 Psychologist, Educational604 Psychologist, Exercise & Sports605 Psychologist, Family606 Psychologist, Forensic607 Psychologist, HealthService608 Psychologist, Men & Masculinity609 Psychologist, Mental Retardation & Developmental Disabilities610 Psychologist, Psychoanalysis611 Psychologist, Psychotherapy612 Psychologist, Psychotherapy, Group613 Psychologist, Rehabilitation614 Psychologist, School615 Psychologist, Women672 Registered Nurse673 Registered Nurse, Addiction (Substance Use Disorder)674 Registered Nurse, Administrator711 Registered Nurse, Ambulatory Care681 Registered Nurse, Cardiac Rehabilitation676 Registered Nurse, Case Management677 Registered Nurse, College Health678 Registered Nurse, Community Health680 Registered Nurse, Continence Care
679 Registered Nurse, Continuing Education/Staff Development675 Registered Nurse, Critical Care Medicine682 Registered Nurse, Diabetes Educator683 Registered Nurse, Dialysis, Peritoneal684 Registered Nurse, Emergency685 Registered Nurse, Enterostomal Therapy686 Registered Nurse, Flight688 Registered Nurse, Gastroenterology687 Registered Nurse, General Practice689 Registered Nurse, Gerontology691 Registered Nurse, Hemodialysis690 Registered Nurse, Home Health692 Registered Nurse, Hospice694 Registered Nurse, Infection Control693 Registered Nurse, Infusion Therapy695 Registered Nurse, Lactation Consultant696 Registered Nurse, Maternal Newborn697 Registered Nurse, Medical-Surgical699 Registered Nurse, Neonatal Intensive Care700 Registered Nurse, Neonatal, Low-Risk701 Registered Nurse, Nephrology702 Registered Nurse, Neuroscience698 Registered Nurse, Nurse Massage Therapist (NMT)703 Registered Nurse, Nutrition Support719 Registered Nurse, Obstetric, High-Risk720 Registered Nurse, Obstetric, Inpatient721 Registered Nurse, Occupational Health722 Registered Nurse, Oncology725 Registered Nurse, Ophthalmic724 Registered Nurse, Orthopedic726 Registered Nurse, Ostomy Care723 Registered Nurse, Otorhinolaryngology & Head-Neck704 Registered Nurse, Pain Management706 Registered Nurse, Pediatric Oncology705 Registered Nurse, Pediatrics710 Registered Nurse, Perinatal714 Registered Nurse, Plastic Surgery708 Registered Nurse, Psych/Mental Health709 Registered Nurse, Psych/Mental Health, Adult707 Registered Nurse, Psych/Mental Health, Child & Adolescent810 Registered Nurse, Registered Nurse First Assistant712 Registered Nurse, Rehabilitation713 Registered Nurse, Reproductive Endocrinology/Infertility715 Registered Nurse, School716 Registered Nurse, Urology718 Registered Nurse, Women's Health Care, Ambulatory717 Registered Nurse, Wound Care617 Respiratory Therapist, Certified618 Respiratory Therapist, Certified, Critical Care620 Respiratory Therapist, Certified, Educational619 Respiratory Therapist, Certified, Emergency Care622 Respiratory Therapist, Certified, General Care621 Respiratory Therapist, Certified, Geriatric Care623 Respiratory Therapist, Certified, Home Health628 Respiratory Therapist, Certified, Neonatal/Pediatrics627 Respiratory Therapist, Certified, Palliative/Hospice629 Respiratory Therapist, Certified, Patient Transport624 Respiratory Therapist, Certified, Pulmonary Diagnostics626 Respiratory Therapist, Certified, Pulmonary Function Technologist625 Respiratory Therapist, Certified, Pulmonary Rehabilitation630 Respiratory Therapist, Certified, SNF/Subacute Care631 Respiratory Therapist, Registered632 Respiratory Therapist, Registered, Critical Care634 Respiratory Therapist, Registered, Educational633 Respiratory Therapist, Registered, Emergency Care636 Respiratory Therapist, Registered, General Care635 Respiratory Therapist, Registered, Geriatric Care637 Respiratory Therapist, Registered, Home Health642 Respiratory Therapist, Registered, Neonatal/Pediatrics641 Respiratory Therapist, Registered, Palliative/Hospice643 Respiratory Therapist, Registered, Patient Transport638 Respiratory Therapist, Registered, Pulmonary Diagnostics640 Respiratory Therapist, Registered, Pulmonary Function Technologist639 Respiratory Therapist, Registered, Pulmonary Rehabilitation644 Respiratory Therapist, Registered, SNF/Subacute Care646 Social Worker, Clinical648 Specialist/Technologist, Other, Biomedical Engineering506 Speech-Language Pathologist649 Technician, Other, Biomedical Engineering502 Other, Not Listed
KAPER-1 (04/2009) Page 42
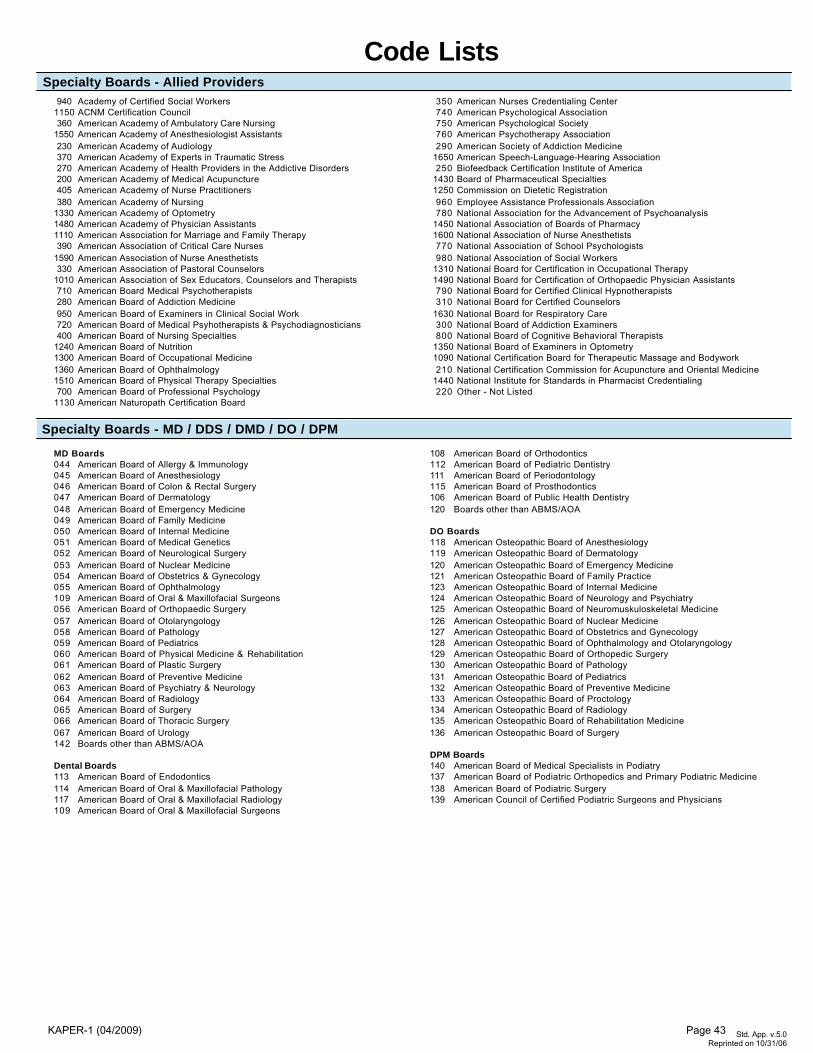
Code Lists
Specialty Boards - MD / DDS / DMD / DO / DPM
Specialty Boards - Allied Providers
MD Boards044 American Board of Allergy & Immunology045 American Board of Anesthesiology046 American Board of Colon & Rectal Surgery047 American Board of Dermatology048 American Board of Emergency Medicine049 American Board of Family Medicine050 American Board of Internal Medicine051 American Board of Medical Genetics052 American Board of Neurological Surgery053 American Board of Nuclear Medicine054 American Board of Obstetrics & Gynecology055 American Board of Ophthalmology109 American Board of Oral & Maxillofacial Surgeons056 American Board of Orthopaedic Surgery057 American Board of Otolaryngology058 American Board of Pathology059 American Board of Pediatrics060 American Board of Physical Medicine & Rehabilitation061 American Board of Plastic Surgery062 American Board of Preventive Medicine063 American Board of Psychiatry & Neurology064 American Board of Radiology065 American Board of Surgery066 American Board of Thoracic Surgery067 American Board of Urology142 Boards other than ABMS/AOA
Dental Boards113 American Board of Endodontics114 American Board of Oral & Maxillofacial Pathology117 American Board of Oral & Maxillofacial Radiology109 American Board of Oral & Maxillofacial Surgeons
108 American Board of Orthodontics112 American Board of Pediatric Dentistry111 American Board of Periodontology115 American Board of Prosthodontics106 American Board of Public Health Dentistry120 Boards other than ABMS/AOA
DO Boards118 American Osteopathic Board of Anesthesiology119 American Osteopathic Board of Dermatology120 American Osteopathic Board of Emergency Medicine121 American Osteopathic Board of Family Practice123 American Osteopathic Board of Internal Medicine124 American Osteopathic Board of Neurology and Psychiatry125 American Osteopathic Board of Neuromuskuloskeletal Medicine126 American Osteopathic Board of Nuclear Medicine127 American Osteopathic Board of Obstetrics and Gynecology128 American Osteopathic Board of Ophthalmology and Otolaryngology129 American Osteopathic Board of Orthopedic Surgery130 American Osteopathic Board of Pathology131 American Osteopathic Board of Pediatrics132 American Osteopathic Board of Preventive Medicine133 American Osteopathic Board of Proctology134 American Osteopathic Board of Radiology135 American Osteopathic Board of Rehabilitation Medicine136 American Osteopathic Board of Surgery
DPM Boards140 American Board of Medical Specialists in Podiatry137 American Board of Podiatric Orthopedics and Primary Podiatric Medicine138 American Board of Podiatric Surgery139 American Council of Certified Podiatric Surgeons and Physicians
Std. App. v.5.0
Reprinted on 10/31/06
940 Academy of Certified Social Workers1150 ACNM Certification Council360 American Academy of Ambulatory Care Nursing
1550 American Academy of Anesthesiologist Assistants230 American Academy of Audiology370 American Academy of Experts in Traumatic Stress270 American Academy of Health Providers in the Addictive Disorders200 American Academy of Medical Acupuncture405 American Academy of Nurse Practitioners380 American Academy of Nursing
1330 American Academy of Optometry1480 American Academy of Physician Assistants1110 American Association for Marriage and Family Therapy390 American Association of Critical Care Nurses
1590 American Association of Nurse Anesthetists330 American Association of Pastoral Counselors
1010 American Association of Sex Educators, Counselors and Therapists710 American Board Medical Psychotherapists280 American Board of Addiction Medicine950 American Board of Examiners in Clinical Social Work720 American Board of Medical Psyhotherapists & Psychodiagnosticians400 American Board of Nursing Specialties
1240 American Board of Nutrition1300 American Board of Occupational Medicine1360 American Board of Ophthalmology1510 American Board of Physical Therapy Specialties700 American Board of Professional Psychology
1130 American Naturopath Certification Board
350 American Nurses Credentialing Center740 American Psychological Association750 American Psychological Society760 American Psychotherapy Association290 American Society of Addiction Medicine
1650 American Speech-Language-Hearing Association250 Biofeedback Certification Institute of America
1430 Board of Pharmaceutical Specialties1250 Commission on Dietetic Registration960 Employee Assistance Professionals Association780 National Association for the Advancement of Psychoanalysis
1450 National Association of Boards of Pharmacy1600 National Association of Nurse Anesthetists770 National Association of School Psychologists980 National Association of Social Workers
1310 National Board for Certification in Occupational Therapy1490 National Board for Certification of Orthopaedic Physician Assistants790 National Board for Certified Clinical Hypnotherapists310 National Board for Certified Counselors
1630 National Board for Respiratory Care300 National Board of Addiction Examiners800 National Board of Cognitive Behavioral Therapists
1350 National Board of Examiners in Optometry1090 National Certification Board for Therapeutic Massage and Bodywork210 National Certification Commission for Acupuncture and Oriental Medicine
1440 National Institute for Standards in Pharmacist Credentialing220 Other - Not Listed
KAPER-1 (04/2009) Page 43
KAPER-1 (04/2009) Page 44
I
KAPER-1 (04/2009) Part B, Section 1
For Health Care Providers Desiring Initial Hospital or Health Care Facility Privileges
NOTE: Submission and approval of a pre-application for privileges may be required by a health care facility prior to the facility’s processing a completed KAPER-1 (04/2009), Part B, Section 1. Therefore, a provider desiring initial health care facility privileges is advised to contact the facility for information relating to any pre-application requirements.
KAPER-1 (04/2009) Page 45
Commonwealth of Kentucky Instructions - Form (04/2009), Part B, Section 1
A. Uniform Application for Evaluation (Credentialing) Form. Following is the form KAPER-1 (04/2009), Part B, Section 1, developed pursuant to KRS 304.17A-535(5) for evaluation (credentialing) of a health care provider. The form is available on the Web site of the Kentucky Department of Insurance at http://insurance.ky.gov. Prior to completing this form, a health care provider who desires initial evaluation (credentialing) by a hospital or health care facility is advised to contact that specific hospital or health care facility for information regarding submission of the complete KAPER-1 (04/2009), Part B, Section 1, and required attachments, as applicable and specified in item C of this instruction. B. Cover Letter. A cover letter, which is signed and dated by the health care provider who desires evaluation (credentialing) by a hospital or health care facility, requesting consideration of the complete KAPER-1 (04/2009), Part B, Section 1, and required attachments, as applicable and specified in item C of this instruction, may be required. C. Required Attachments. For a Physician, unless otherwise specified in this instruction, one (1) photocopy of each of the following supporting documents should be labeled and attached to the complete form KAPER-1 (04/2009), Part B, Section 1, in the following order: 1. Current medical, dental or professional license or evidence of licensure, as applicable (If medical, dental or other health care provider, including a psychologist, has applied for, but not received this license, a copy of the application for this license will be accepted until a copy of the license is available for submission.); 2. Current federal drug enforcement agency (DEA) certificate for each state of practice. (If medical, dental or other health care provider, including a psychologist, has applied for, but not received this number, a copy of the application for a DEA number will be accepted until the DEA number is available for submission.); 3. Current state substance registration certificate, if applicable. (If medical, dental or other health care provider, including a psychologist, has applied for but not received this certificate, a copy of the application for this certificate will be accepted until a copy of the state substance registration certificate is available for submission.); 4. Proof of current professional liability insurance, including name, inception and expiration dates and amount of coverage (If medical, dental or other health care provider, including a psychologist, has applied for but not received professional liability insurance, a photocopy of the application for professional liability insurance will be accepted until the proof of current professional liability insurance is available for submission.); 5. Board certification/eligibility verification information; 6. Curriculum vitae (All time periods from receipt of degree to present must be accounted for); 7. Current photograph; 8. Photo identification (ID). Additionally, photo ID should be presented in person at the hospital or health care organization where participation is desired; and 9. Separate pages or supplemental forms, if any, in page number order.
KAPER-1 (04/2009) Page 46
For an Allied Health Professional, unless otherwise specified in this instruction, one (1) photocopy of each of the following supporting documents should be labeled and attached to the complete form KAPER-1 (04/2009), Part B, Section 1, in the following order: 1. Current professional license or evidence of licensure (If multiple professional licenses are held by the allied health professional, a copy of each license and/or registration should be attached; for example, registered nurse (RN); 2. Current federal drug enforcement agency (DEA) certificate, if applicable for allied health professional specialty (If allied health professional has applied for but not been issued a DEA number, a copy of the application requesting this number may be submitted until a copy of the actual DEA number is available for submission.); 3. Current state substance registration certificate, if applicable (If allied health professional has applied for but not been issued a state substance registration certificate, a copy of the application requesting this certificate may be submitted until a copy of the actual certificate is available for submission.); 4. Statement of sponsoring health care provider (e.g., physician) or collaborative practice agreement, if applicable; 5. Proof of current professional liability insurance, including allied health professional name, inception and expiration date, and amount of coverage (If allied health professional has applied for but not been issued professional liability insurance, a copy of the application requesting coverage may be submitted until a copy of the approval of coverage is available for submission.); 6. Curriculum vitae or resume (All time periods from receipt of degree to present must be accounted for); 7. Current photograph; 8. Photo identification (ID). Additionally, photo ID should be presented in person at the hospital or health care organization where participation is desired; and 9. Separate pages or supplemental forms, if any, in page number order.
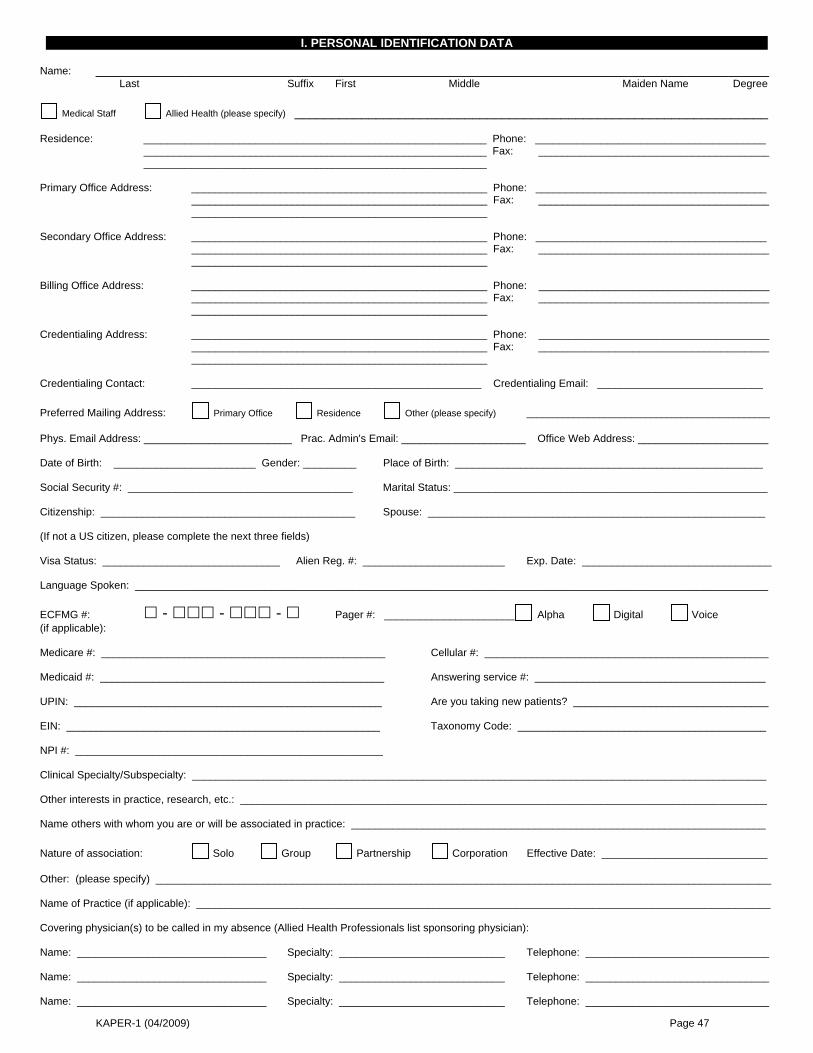
KAPER-1 (04/2009) Page 47
I. PERSONAL IDENTIFICATION DATA Name: ___________________________________________________________________________________________ Last Suffix First Middle Maiden Name Degree
Medical Staff Allied Health (please specify) ________________________________________________________________ Residence: __________________________________________________________ Phone: _______________________________________ __________________________________________________________ Fax: _______________________________________ __________________________________________________________ Primary Office Address: __________________________________________________ Phone: _______________________________________ __________________________________________________ Fax: _______________________________________ __________________________________________________ Secondary Office Address: __________________________________________________ Phone: _______________________________________ __________________________________________________ Fax: _______________________________________ __________________________________________________ Billing Office Address: __________________________________________________ Phone: _______________________________________ __________________________________________________ Fax: _______________________________________ __________________________________________________ Credentialing Address: __________________________________________________ Phone: _______________________________________ __________________________________________________ Fax: _______________________________________ __________________________________________________ Credentialing Contact: _________________________________________________ Credentialing Email: ____________________________ Preferred Mailing Address: Primary Office Residence Other (please specify) _______________________________________________ Phys. Email Address: _________________________ Prac. Admin's Email: _____________________ Office Web Address: ______________________ Date of Birth: ________________________ Gender: _________ Place of Birth: ____________________________________________________ Social Security #: ______________________________________ Marital Status: _____________________________________________________ Citizenship: ___________________________________________ Spouse: _________________________________________________________ (If not a US citizen, please complete the next three fields) Visa Status: ______________________________ Alien Reg. #: ________________________ Exp. Date: ________________________________ Language Spoken: ___________________________________________________________________________________________________________ ECFMG #: - - - Pager #: ______________________ Alpha Digital Voice (if applicable): Medicare #: ________________________________________________ Cellular #: ________________________________________________ Medicaid #: ________________________________________________ Answering service #: _______________________________________ UPIN: ____________________________________________________ Are you taking new patients? _________________________________ EIN: _____________________________________________________ Taxonomy Code: __________________________________________ NPI #: ____________________________________________________ Clinical Specialty/Subspecialty: _________________________________________________________________________________________________ Other interests in practice, research, etc.: _________________________________________________________________________________________ Name others with whom you are or will be associated in practice: ______________________________________________________________________ Nature of association: Solo Group Partnership Corporation Effective Date: ____________________________ Other: (please specify) ________________________________________________________________________________________________________ Name of Practice (if applicable): _________________________________________________________________________________________________ Covering physician(s) to be called in my absence (Allied Health Professionals list sponsoring physician): Name: ________________________________ Specialty: ____________________________ Telephone: _______________________________ Name: ________________________________ Specialty: ____________________________ Telephone: _______________________________ Name: ________________________________ Specialty: ____________________________ Telephone: _______________________________
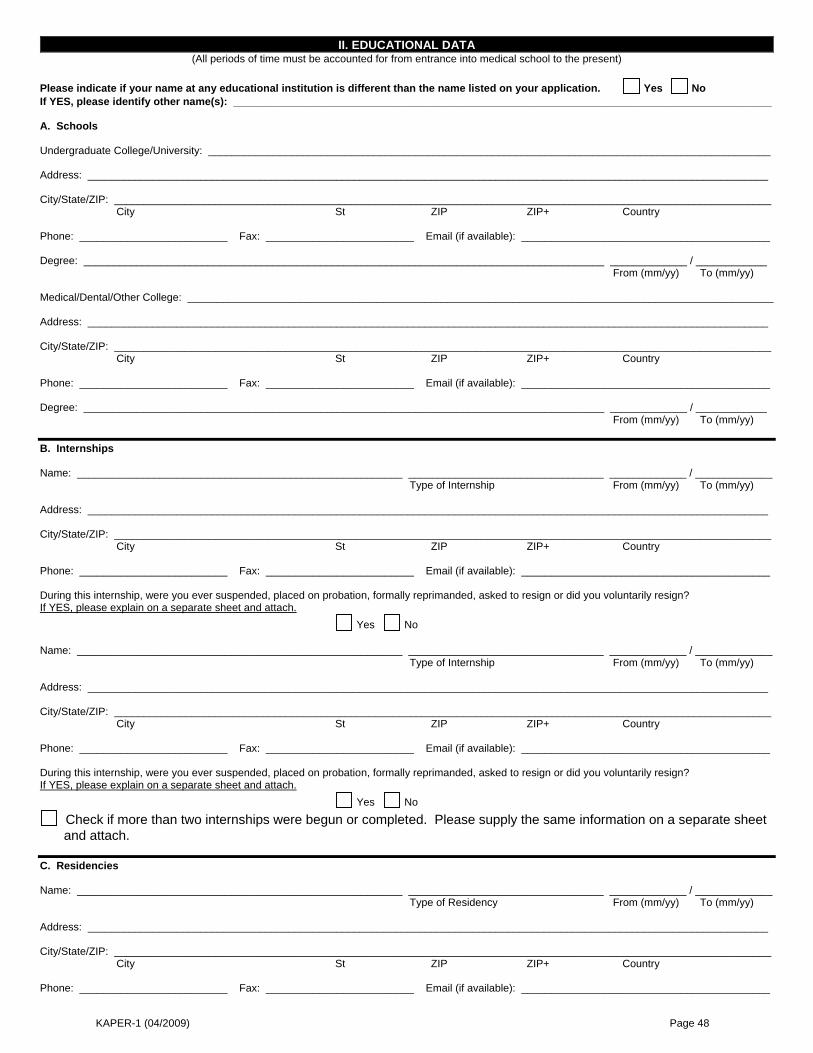
KAPER-1 (04/2009) Page 48
II. EDUCATIONAL DATA (All periods of time must be accounted for from entrance into medical school to the present)
Please indicate if your name at any educational institution is different than the name listed on your application. Yes No If YES, please identify other name(s): ___________________________________________________________________________________________ A. Schools Undergraduate College/University: _______________________________________________________________________________________________ Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________ Degree: ________________________________________________________________________________________ _____________ / ____________ From (mm/yy) To (mm/yy) Medical/Dental/Other College: ___________________________________________________________________________________________________ Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________ Degree: ________________________________________________________________________________________ _____________ / ____________ From (mm/yy) To (mm/yy) B. Internships Name: _______________________________________________________ _________________________________ _____________ / _____________ Type of Internship From (mm/yy) To (mm/yy) Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________ During this internship, were you ever suspended, placed on probation, formally reprimanded, asked to resign or did you voluntarily resign? If YES, please explain on a separate sheet and attach. Yes No Name: _______________________________________________________ _________________________________ _____________ / _____________ Type of Internship From (mm/yy) To (mm/yy) Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________ During this internship, were you ever suspended, placed on probation, formally reprimanded, asked to resign or did you voluntarily resign? If YES, please explain on a separate sheet and attach. Yes No
Check if more than two internships were begun or completed. Please supply the same information on a separate sheet and attach.
C. Residencies Name: _______________________________________________________ _________________________________ _____________ / _____________ Type of Residency From (mm/yy) To (mm/yy) Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________
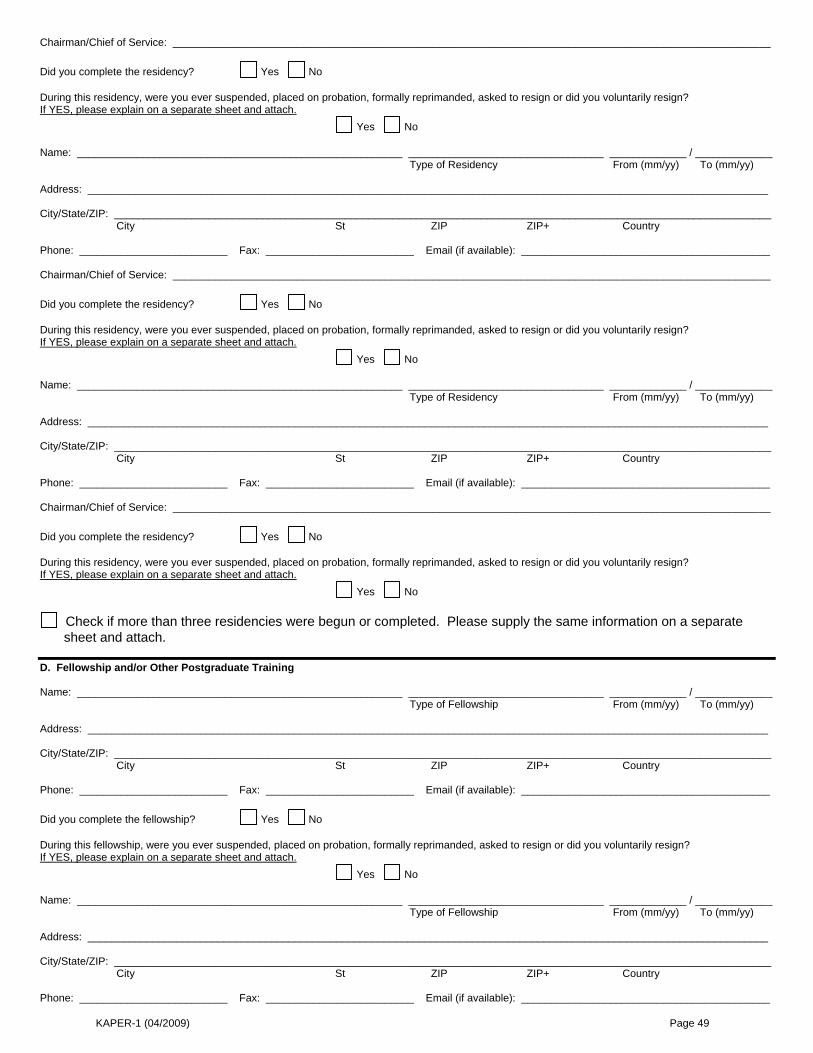
KAPER-1 (04/2009) Page 49
Chairman/Chief of Service: _____________________________________________________________________________________________________ Did you complete the residency? Yes No During this residency, were you ever suspended, placed on probation, formally reprimanded, asked to resign or did you voluntarily resign? If YES, please explain on a separate sheet and attach. Yes No Name: _______________________________________________________ _________________________________ _____________ / _____________ Type of Residency From (mm/yy) To (mm/yy) Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________ Chairman/Chief of Service: _____________________________________________________________________________________________________ Did you complete the residency? Yes No During this residency, were you ever suspended, placed on probation, formally reprimanded, asked to resign or did you voluntarily resign? If YES, please explain on a separate sheet and attach. Yes No Name: _______________________________________________________ _________________________________ _____________ / _____________ Type of Residency From (mm/yy) To (mm/yy) Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________ Chairman/Chief of Service: _____________________________________________________________________________________________________ Did you complete the residency? Yes No During this residency, were you ever suspended, placed on probation, formally reprimanded, asked to resign or did you voluntarily resign? If YES, please explain on a separate sheet and attach. Yes No
Check if more than three residencies were begun or completed. Please supply the same information on a separate sheet and attach.
D. Fellowship and/or Other Postgraduate Training Name: _______________________________________________________ _________________________________ _____________ / _____________ Type of Fellowship From (mm/yy) To (mm/yy) Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________ Did you complete the fellowship? Yes No During this fellowship, were you ever suspended, placed on probation, formally reprimanded, asked to resign or did you voluntarily resign? If YES, please explain on a separate sheet and attach. Yes No Name: _______________________________________________________ _________________________________ _____________ / _____________ Type of Fellowship From (mm/yy) To (mm/yy) Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________
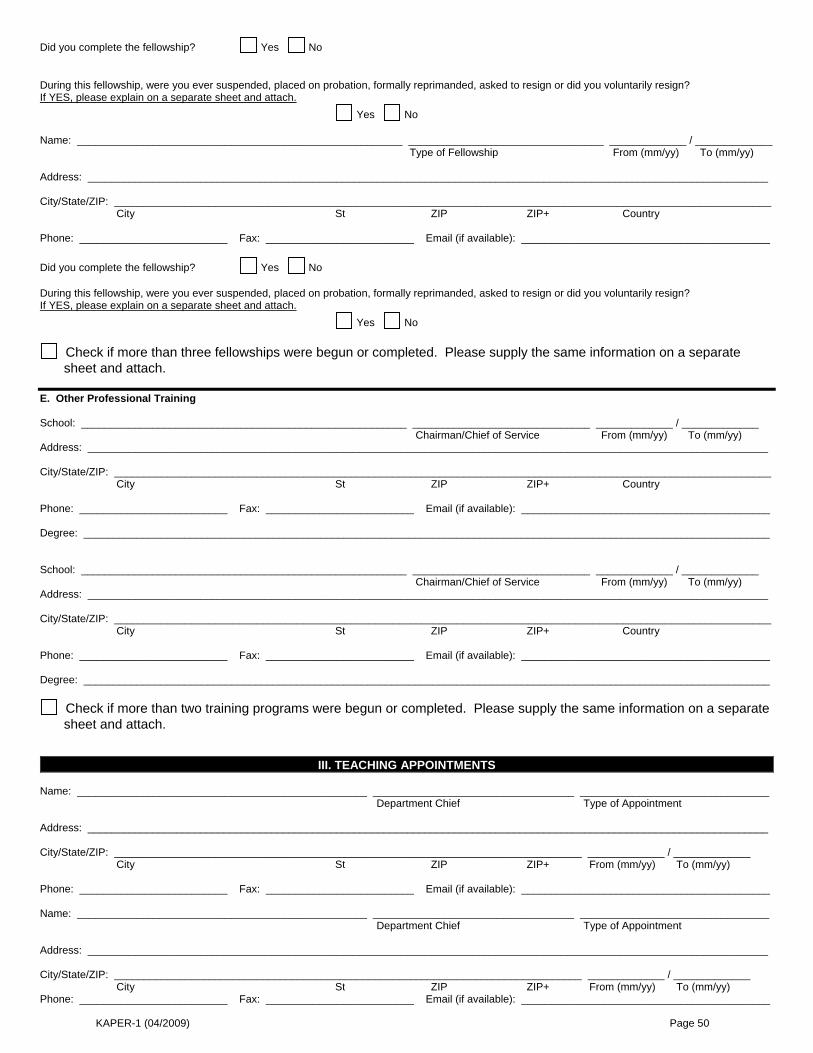
KAPER-1 (04/2009) Page 50
Did you complete the fellowship? Yes No During this fellowship, were you ever suspended, placed on probation, formally reprimanded, asked to resign or did you voluntarily resign? If YES, please explain on a separate sheet and attach. Yes No Name: _______________________________________________________ _________________________________ _____________ / _____________ Type of Fellowship From (mm/yy) To (mm/yy) Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________ Did you complete the fellowship? Yes No During this fellowship, were you ever suspended, placed on probation, formally reprimanded, asked to resign or did you voluntarily resign? If YES, please explain on a separate sheet and attach. Yes No
Check if more than three fellowships were begun or completed. Please supply the same information on a separate sheet and attach.
E. Other Professional Training School: _______________________________________________________ ______________________________ _____________ / _____________ Chairman/Chief of Service From (mm/yy) To (mm/yy) Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________ Degree: ____________________________________________________________________________________________________________________ School: _______________________________________________________ ______________________________ _____________ / _____________ Chairman/Chief of Service From (mm/yy) To (mm/yy) Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________ Degree: ____________________________________________________________________________________________________________________
Check if more than two training programs were begun or completed. Please supply the same information on a separate sheet and attach.
III. TEACHING APPOINTMENTS Name: _________________________________________________ __________________________________ ________________________________ Department Chief Type of Appointment Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________ _____________ / _____________ City St ZIP ZIP+ From (mm/yy) To (mm/yy) Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________ Name: _________________________________________________ __________________________________ ________________________________ Department Chief Type of Appointment Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________ _____________ / _____________ City St ZIP ZIP+ From (mm/yy) To (mm/yy) Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________
KAPER-1 (04/2009) Page 51
IV. POST-GRADUATE AND CONTINUING EDUCATION COURSES Have you participated in post-graduate/continuing education courses in the last three years? If YES, please supply an attached list and/or certificate of attendance.
YES NO List and/or certificates attached Do you have a cardio-pulmonary resuscitation certificate? CPR Yes No Date of Expiration ______________________
ACLS Yes No Date of Expiration ______________________
ATLS Yes No Date of Expiration ______________________
PALS Yes No Date of Expiration ______________________
NRP Yes No Date of Expiration ______________________
Please attach copies of all certificates.
V. LICENSURE INFORMATION List all current and past professional health care licenses held and attach copies of all active licenses. Allied Health Professionals: list all certifications. State: License #: Date Issued: Expiration Date: Status: License Obtained by:
KY State: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #2: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #3: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #4: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #5: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #6: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #7: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #8: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
If licensed in more than eight (8) states, please supply the same information on a separate sheet and attach.
VI. DRUG ENFORCEMENT ADMINISTRATION INFORMATION (DEA)
(This application cannot be processed without current Federal DEA Certificate for each state in which you practice) Federal DEA Certificate #: _________________________________________ Expiration: _______________________________________________ Federal DEA Certificate #: _________________________________________ Expiration: _______________________________________________
VII. STATE NARCOTICS REGISTRATION: CONTROLLED SUBSTANCE REGISTRATION (CSR)
Some states require additional CSR certificates. Attach copies of any additional CSR certificates you have. State: _____________________________________________________________________________________________________________________ Certificate #: ____________________________________________________ Expiration: _______________________________________________ State: _____________________________________________________________________________________________________________________ Certificate #: ____________________________________________________ Expiration: _______________________________________________
VIII. PROFESSIONAL LIABILITY DATA
(This application cannot be processed without proof of amount of professional liability) Name of Carrier: _____________________________________________________________________________________________________________ Address: ___________________________________________________________________________________________________________________ City: ________________________________________________ State: ______________________ ZIP: _____________________________ Policy #: ____________________________________________ Amount of Coverage: ________________________________________________
KAPER-1 (04/2009) Page 52
Date of Inception: _____________________________________ Date of Expiration: __________________________________________________ Name of Agency: _____________________________________________________________________________________________________________
CLAIMS MADE OCCURRENCE (Check One) Please list any other professional liability carriers you have used within the last five (5) years: _________________________________________________ ____________________________________________________________________________________________________________________________ Answer the following questions: 1. Has your professional liability insurance coverage been terminated by action of the insurance company? N/A Yes No
2. Have you been denied professional liability insurance coverage or been rated at a higher than average risk N/A Yes No class for your specialty?
3. Has your present professional liability insurance carrier excluded any specific procedures from your N/A Yes No coverage? 4. Have any professional liability suits or claims been filed against you? N/A Yes No
5. Have any professional liability suits or claims been filed against you which are presently pending? N/A Yes No
6. Have any judgments or settlements been made against you in professional liability cases? N/A Yes No
7. If applying to an Indiana facility, do you participate in the Indiana Patient Compensation Fund? N/A Yes No
8. If applying to a Virginia facility, do you participate in the Birth-related Neurological Injury Compensation Act? N/A Yes No If the answer is yes to any of the above questions, please explain the case(s) and the outcome(s) on the following Professional Liability Detail Sheet. Provide a full explanation including the name of the carrier, the date and specific information concerning any limitation, settlement or judgment.
PROFESSIONAL LIABILITY DETAIL SHEET
(Please copy this page if additional sheets are needed)
CHECK HERE IF NOT APPLICABLE Please fill in the following details for each pending or settled malpractice suit or claim you have experienced:
Pending Settled Date: ____________________________ List the allegations: ___________________________________________________________________________________________________________ ____________________________________________________________________________________________________________________________ Date of occurrence: ___________________________________________________________________________________________________________ Name of institution involved (i.e., hospital): _________________________________________________________________________________________ Name and address of insurance carriers involved: ___________________________________________________________________________________ Please supply the following details for each malpractice lawsuit in which you were a defendant, and which resulted in a jury award or court judgments against you. Title of the court case: _________________________________________________________________________________________________________ The court case number: ________________________________________________________________________________________________________ The venue of the case (place where court case took place, such as County District Court or Circuit Court): ______________________________________ ____________________________________________________________________________________________________________________________ Allegations listed in complaint: __________________________________________________________________________________________________ Date of incident leading to complaint: _____________________________________________________________________________________________ Place of incident: _____________________________________________________________________________________________________________ Name and address of malpractice insurance carrier: _________________________________________________________________________________ ____________________________________________________________________________________________________________________________ Amount of jury award or amount awarded by the court: _______________________________________________________________________________
KAPER-1 (04/2009) Page 53
IX. CERTIFICATION BY AMERICAN BOARD OF MEDICAL SPECIALTIES OR AMERICAN OSTEOPATHIC ASSOCIATION
(Allied Health Professional: list national certifications)
1. Are you board certified? Yes No (If not Board admissible, please explain on separate sheet and attach) 2. If yes, list full name of certifying board and date which you obtained certification/recertification:
_____________________________________________________________________________ Date: ____________________________ _____________________________________________________________________________ Date: ____________________________ _____________________________________________________________________________ Date: ____________________________ _____________________________________________________________________________ Date: ____________________________ _____________________________________________________________________________ Date: ____________________________
3. If you are not yet certified but have applied to a specialty board for examination, give the name of the board and date of application: _____________________________________________________________________________ Date: ____________________________
4. If status is one of eligibility, provide year when eligibility will terminate under rules of the specific board: _____________________________________ 5. List date of next required recertification (if applicable): ____________________________________________________________________________ 6. Have you ever been examined by a specialty board but failed to pass the exam? If yes, please explain. Yes No
X. INDIVIDUAL PRACTICE INFORMATION Please answer each of the following questions in full. If the answer to any question is "yes," please provide full explanation of the details on a separate sheet and attach. 1. Are there any actions that have been initiated or are any pending against you by any state licensing board? Yes No
Pending Resolved
2. Have you had any professional license or certification in any state that has ever been denied, limited, Yes No suspended, sanctioned, revoked, probated, voluntarily or involuntarily relinquished or not renewed?
3. Have you ever received notice of a proposed or actual exclusion (suspension, sanction, otherwise restricted) Yes No from any private health care program(s) or any health care program(s) funded in whole or in part by the state or federal government, including Medicare or Medicaid? If so, provide a detailed description of this matter, including the current status of your participation in such program(s).
4. Have you ever been the subject of an investigation by any private, federal or state agency concerning your N/A Yes No participation in any private, federal or state health insurance program?
5. Have your narcotics registration certificates ever been limited, suspended, revoked, voluntarily or N/A Yes No involuntarily surrendered or not renewed? 6. If applicable, is your federal (to include District of Columbia and territories of U.S.A.) and/or state narcotics N/A Yes No registration certificate being challenged? 7. Have you been named as a defendant or convicted of a felony or misdemeanor? Yes No
8. Have your employment, medical staff appointment or clinical privileges ever been voluntarily or involuntarily Yes No denied, suspended, diminished, revoked, limited or not renewed at any health care facility?
9. Have you ever withdrawn your application for appointment, reappointment, clinical privileges, or resigned Yes No from the medical staff of any health care facility before a decision was made by its governing board?
10. Have you ever been the subject of disciplinary proceedings or a focus review based on inappropriate Yes No quality of care at any hospital or health care facility?
11. Have you ever been denied membership or renewal thereof, or been subject to disciplinary or adverse Yes No action in any medical or professional organization?
XI. PERSONAL HEALTH STATUS Please answer each of the following questions in full. If the answer to any question is "yes," please provide full explanation of the details on the appropriate Explanation Sheet. 1. Do you currently have, or have you ever had any physical, mental, or emotional condition which impaired, or might Yes No reasonably be considered to impair, your ability to perform the procedures or provide the treatment for which you have requested clinical privileges or to meet the requirements of medical staff membership? 2. Have you ever been admitted to any hospital or been involved in a treatment program for any physical, mental or Yes No emotional condition which impaired or might reasonably be considered to impair, your ability to perform the procedures or provide the treatment for which you have requested clinical privileges or to meet the requirements of medical staff membership? 3. Do you currently have, or have you ever had a dependency on or abuse of the use of alcohol or drugs, or are you Yes No currently or have ever been involved in a treatment program for a dependency on or abuse of alcohol or drugs which impaired, or might reasonably be considered to impair, your ability to perform the procedures or provide the treatment for which you have requested clinical privileges or to meet the requirements of medical staff membership?
KAPER-1 (04/2009) Page 54
XII. PROFESSIONAL SOCIETIES Membership in local, state, or national medical societies Dates Name: _________________________________________________________________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: ____________________________________________________________________________________________________________ City: ________________________________________________ State: ______________________ ZIP: ______________________ Name: _________________________________________________________________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: ____________________________________________________________________________________________________________ City: ________________________________________________ State: ______________________ ZIP: ______________________ Name: _________________________________________________________________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: ____________________________________________________________________________________________________________ City: ________________________________________________ State: ______________________ ZIP: ______________________ Name: _________________________________________________________________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: ____________________________________________________________________________________________________________ City: ________________________________________________ State: ______________________ ZIP: ______________________ 1. I would like to use this application for membership in the __________________________________ County Medical Society and the KMA. A separate dues statement will be sent. 2. I am already a member of my local medical society. Please specify society: _____________________________________________________
XIII. PROFESSIONAL EMPLOYMENT AND AFFILIATIONS A. Employment List in chronological order all professional employment since completion of post-graduate education, starting with your current position. This includes all hospitals, corporations, military assignments, government agencies, group practices, other healthcare facilities or other types of activity. Complete addresses must be included. Date must be in MM/YY format. If you have a gap in employment of more than thirty (30) days, please explain on a separate page. "See CV" is not acceptable. Please attach additional sheets if more space is needed. Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________ Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________ Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________
KAPER-1 (04/2009) Page 55
Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________ B. Affiliations List in chronological order all professional affiliations since completion of post-graduate education, starting with your current position. This includes all hospitals, corporations, military assignments, government agencies, group practices, other healthcare facilities or other types of activity. Complete addresses must be included. Date must be in MM/YY format. If you have a gap in employment of more than thirty (30) days, please explain on a separate page. "See CV" is not acceptable. Please attach additional sheets if more space is needed. Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________ Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________ Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): _________________________________________ Reason for leaving: ________________________________________________________________________________________________________ Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________ Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________
KAPER-1 (04/2009) Page 56
XIV. PEER REFERENCES Name three physicians who have personal knowledge of your current clinical abilities, and ethical character, who will provide specific written comments on these matters upon request from Hospitals, Medical Societies, or Authorized Credentialing Services. The named individuals must have acquired the requisite knowledge through recent observation of your professional practice over a reasonable period of time, and at least one must have had organizational responsibility for your performance. The individuals should not be related to you by blood or marriage, training directors, partners/associates in your current group practice, or anyone with whom you have or anticipate having a financial relationship. Requested sources: practitioner in same specialty or practitioners with whom you have a referral pattern. If you recently completed training, you may use chief resident or other training colleague. Allied Health Professional should list their sponsoring physician, another physician and one peer from the same specialty as the applicant. Please note that you may be required to follow further directions of an individual hospital or facility in order to accommodate variations in medical staff bylaws. Reference: ________________________________________________________________________________________________________________ Address: _________________________________________________________________________________________________________________ City/St/ZIP: _____________________________________________________________________________ Country: ________________________ Phone: _________________________ Fax: _________________________ Email (if available): _________________________________________ Reference: ________________________________________________________________________________________________________________ Address: _________________________________________________________________________________________________________________ City/St/ZIP: _____________________________________________________________________________ Country: ________________________ Phone: _________________________ Fax: _________________________ Email (if available): _________________________________________ Reference: ________________________________________________________________________________________________________________ Address: _________________________________________________________________________________________________________________ City/St/ZIP: _____________________________________________________________________________ Country: ________________________ Phone: _________________________ Fax: _________________________ Email (if available): _________________________________________
KAPER-1 (04/2009) Page 57
XV. AUTHORIZATION AND RELEASE OF APPLICANT (HEALTHCARE FACILITY RELEASE)
(Please read carefully before signing) As a condition of applying for/accepting medical staff appointment or clinical privileges at the healthcare facilities listed in this application ("Hospital"), and whether or not my application is accepted, I acknowledge, consent, and agree as follows: A) I extend absolute immunity to, and release from all liability, the Hospital, its authorized representatives, and third parties (as defined in subsection C below), for any good faith communications, recommendations, disclosures or administrative action involving and pertaining to: (1) applications for appointment, reappointment or clinical privileges; (2) periodic reappraisals; (3) proceedings for suspension or reduction of clinical privileges or for denial or revocation of appointment, reappointment, or any other disciplinary action; (4) summary suspensions; (5) hearings and appellate reviews; (6) care evaluations; (7) utilization reviews; (8) any other healthcare facility, medical staff, department, service or committee activities; (9) my professional qualifications, credentials, clinical competence, character, mental or emotional stability, physical condition, ethics or behavior; and (10) any other matter that might directly or indirectly impact or reflect on my competence, on patient care or on the orderly operation of the Hospital. B) I will make myself available for interviews and acknowledge the burden of producing updated current information as to all questions on this application and such other information reasonably necessary to evaluate my qualifications. The Hospital and its authorized representatives may consult with and obtain information, including otherwise privileged or confidential information, from the Hospital's medical staff appointees and employees and from any third party bearing on my professional qualifications, all matters listed in subsection A, and any other matters bearing on my satisfaction of the criteria for reappointment to the medical staff. I authorize all persons and organizations having any knowledge of such matters to release said information to the Hospital or its authorized representatives upon request and I consent to the reporting of disciplinary information described below in section C. C) The term "Hospital and its authorized representatives" means the Hospital, its governing entity, persons who have any responsibility for or knowledge pertaining to the matters outlined in subsection A above, and authorized Centralized Verification Organization (CVO). The term "third party" means any individual, including a reappointee to the medical staff or other healthcare facilities, other physicians and health practitioners, government agencies, professional liability insurers, and other entities from whom or by whom the Hospital, authorized CVO, or other authorized representatives have requested or supplied information pertaining to matters in subsection A above. I acknowledge and agree that: (1) medical staff reappointment and clinical privileges are not a right; (2) applications and requests will be evaluated in accordance with prescribed procedures defined in the Hospital and medical staff bylaws, rules and regulations; (3) I shall be bound by the medical staff bylaws, rules and regulations, and corporate compliance programs, as amended from time to time, of hospitals to which I now and may subsequently apply; (4) I pledge to provide for continuous care for my patients in the hospital; (5) Hospital or its authorized representatives and third parties acting in their official capacities will notify authorized CVO and appropriate governmental agencies, boards or professional associations of disciplinary or professional action taken with respect to me if required to be reported to the Kentucky Medical Licensure Board by KRS 311.606 or if required to be reported by the authorized CVO, by medical staff bylaws, or by any other state or federal law; and (6) that this authorization, attestation and release is irrevocable for any period during which I am an applicant for or have medical staff privileges at Hospital, or, if later in time, for as long as Hospital may be under a duty to report information pursuant to the Health Care Quality Improvement Act of 1986. Pub. L. 99-660. I represent and warrant that at the time of this application and at all times while I maintain medical staff membership that (1) I am not nor have I ever been, excluded or suspended for any period of time whatsoever from participation in any state or federal health care program, including Medicare and Medicaid; (2) I have not been convicted under any state or federal law of any offense for which I could face mandatory exclusion from participation in any state or federal health care program, including Medicare and Medicaid; (3) I have not committed any act for which I may be permissibly excluded from participation in any state or federal health care program, including Medicare and Medicaid; (4) I do not hold, and have never held, a direct or indirect ownership or controlling interest of five percent (5%) or more in any entity that has been excluded or suspended for any period of time whatsoever from participation in any state or federal health care program, including Medicare and Medicaid, nor have I ever been an officer, director, agent, or managing employee of any such entity; and (5) I have never been convicted of a federal health care offense as defined in 18 U.S.C. § 24, including any theft, embezzlement, fraud, or other acts as prohibited therein with regard to any public or private health plan. I agree to notify Hospital immediately in the event I am unable to maintain one or more of these representations. D) Information and documents derived from or compiled in connection with matters listed in subsection A above, shall be privileged and confidential to the fullest extent permitted by law. Information contained in or attached to this application is accurate and complete to the best of my knowledge. Any misrepresentation, misstatement, or omission, whether intentional or not, may constitute cause for immediate rejection of this application and termination of any status or privilege granted in reliance upon it. Applicant's Signature: _______________________________________________________ Date: ________________________________
KAPER-1 (04/2009) Page 58
ACKNOWLEDGEMENT STATEMENT The following statement is required (by Medicare/Champus regulation) to be signed by each physician when he/she joins the Medical Staff. This must be signed and dated in the physician’s own handwriting using his/her legal signature (initials are not accepted). According to federal guidelines, stamped signatures and typed dates are not acceptable.
MEDICARE/CHAMPUS “Notice to physicians: Medicare/Champus payment to hospitals is based in part on each patient’s principle and secondary diagnoses and the major procedures performed on the patient, as attested to by the patient’s attending physician by virtue of his/her signature in the medical record. Anyone who misrepresents, falsifies, or conceals essential information required for payment of federal funds may be subject to fine, imprisonment or civil penalty under applicable federal law.” I certify that I have received the above statement. Signature: _________________________________________ Date: ___________ Type or Printed Name: ___________________________________________________
KAPER-1 (04/2009) Page 59
KAPER-1 (01/2009) Part B, Section 2
For Health Care Providers Desiring Reevaluation for Hospital or Health Care Facility Privileges
KAPER-1 (04/2009) Page 60
Commonwealth of Kentucky Instructions - KAPER-1 (01/2009), Part B, Section 2
A. Uniform Application for Reevaluation (Recredentialing) Form. Following is the KAPER-1 (01/2009), Part B, Section 2 developed pursuant to KRS 304.17A-545(5) for reevaluation (recredentialing) of health care providers. The form is available on the Web site of the Kentucky Department of Insurance at http://insurance.ky.gov. Prior to completing this form, a health care provider who desires reevaluation (recredentialing) by a hospital or health care facility is advised to contact that specific hospital or health care facility for information regarding submission of the complete KAPER-1 (01/2009), Part B, Section 2 and required attachments, as applicable and specified in item C of this instruction. B. Cover Letter. A cover letter, which is signed and dated by the provider, who desires reevaluation (recredentialing) by a hospital or health care facility, requesting consideration of the complete KAPER-1 (01/2009), Part B, Section 2 and required attachments, as applicable and specified in item C of this instruction, may be required. C. Required Attachments. Unless otherwise specified in this instruction, one (1) photocopy of each of the following supporting documents should be labeled and attached to the complete form KAPER-1 (01/2009), Part B, Section 2 in the following order: 1. Current medical, dental or professional license or evidence of licensure, as applicable; 2. Current federal drug enforcement agency (DEA) certificate for each state of practice; 3. Current state substance registration certificate, as applicable; 4. Proof of current professional liability insurance, including name, limits of liability and expiration dates. Additionally, if an affirmative response is entered for any question in Section VII of this section, provide a written explanation on an additional page of this attachment; 5. Proof of continuing medical education (CME) or continuing education unit (CEU) credits obtained in the past two (2) years; and 6. Separate pages, as applicable, in page number order.
KAPER-1 (04/2009) Page 61
I. PERSONAL IDENTIFICATION DATA Name: ___________________________________________________________________________________________ Last Suffix First Middle Maiden Name Degree
Medical Staff Allied Health (please specify) ________________________________________________________________ Residence: __________________________________________________________ Phone: _______________________________________ __________________________________________________________ Fax: _______________________________________ __________________________________________________________ Primary Office Address: __________________________________________________ Phone: _______________________________________ __________________________________________________ Fax: _______________________________________ __________________________________________________ Secondary Office Address: __________________________________________________ Phone: _______________________________________ __________________________________________________ Fax: _______________________________________ __________________________________________________ Billing Office Address: __________________________________________________ Phone: _______________________________________ __________________________________________________ Fax: _______________________________________ __________________________________________________ Credentialing Address: __________________________________________________ Phone: _______________________________________ __________________________________________________ Fax: _______________________________________ __________________________________________________ Credentialing Contact: _________________________________________________ Credentialing Email: ____________________________ Preferred Mailing Address: Primary Office Residence Other (please specify) _______________________________________________ Phys. Email Address: _________________________ Prac. Admin's Email: _____________________ Office Web Address: ______________________ Date of Birth: ________________________Gender: _________ Place of Birth: ____________________________________________________ Social Security #: ______________________________________ Marital Status: _____________________________________________________ Citizenship: ___________________________________________ Spouse: _________________________________________________________ (If not a US citizen, please complete the next three fields) Visa Status: ______________________________ Alien Reg. #: ________________________ Exp. Date: ________________________________ Language Spoken: ___________________________________________________________________________________________________________ ECFMG #: - - - Pager #: ______________________ Alpha Digital Voice (if applicable): Medicare #: ________________________________________________ Cellular #: ________________________________________________ Medicaid #: ________________________________________________ Answering service #: _______________________________________ UPIN: ____________________________________________________ Are you taking new patients? _________________________________ EIN: _____________________________________________________ Taxonomy Code: __________________________________________ NPI #: ____________________________________________________ Clinical Specialty/Subspecialty: _________________________________________________________________________________________________ Other interests in practice, research, etc.: _________________________________________________________________________________________ Name others with whom you are or will be associated in practice: ______________________________________________________________________ Nature of association: Solo Group Partnership Corporation Effective Date: ____________________________ Other: (please specify) ________________________________________________________________________________________________________ Name of Practice (if applicable): _________________________________________________________________________________________________ Covering physician(s) to be called in my absence (Allied Health Professionals list sponsoring physician): Name: ________________________________ Specialty: ____________________________ Telephone: _______________________________ Name: ________________________________ Specialty: ____________________________ Telephone: _______________________________ Name: ________________________________ Specialty: ____________________________ Telephone: _______________________________
KAPER-1 (04/2009) Page 62
II. TEACHING APPOINTMENTS Name: _________________________________________________ __________________________________ ________________________________ Department Chief Type of Appointment Address: ___________________________________________________________________________________________________________________ City/State/ZIP: _______________________________________________________________________________ _____________ / _____________ City St ZIP ZIP+ From (mm/yy) To (mm/yy) Phone: _________________________ Fax: _________________________ Email (if available): __________________________________________
III. POST-GRADUATE AND CONTINUING EDUCATION COURSES Have you participated in post-graduate/continuing education courses in the last two (2) years? If YES, please supply an attached list and/or certificate of attendance.
YES NO List and/or certificates attached Do you have a cardio-pulmonary resuscitation certificate? CPR Yes No Date of Expiration ______________________
ACLS Yes No Date of Expiration ______________________
ATLS Yes No Date of Expiration ______________________
PALS Yes No Date of Expiration ______________________
NRP Yes No Date of Expiration ______________________
Please attach copies of all certificates.
IV. LICENSURE INFORMATION List all current and past professional health care licenses held and attach copies of all active licenses. Allied Health Professionals: list all certifications. State: License #: Date Issued: Expiration Date: Status: License Obtained by:
KY State: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #2: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #3: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #4: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #5: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #6: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #7: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
State #8: _______ _____________ _____________ _____________ Active Inactive Exam Reciprocity
If licensed in more than eight (8) states, please supply the same information on a separate sheet and attach.
V. DRUG ENFORCEMENT ADMINISTRATION INFORMATION (DEA)
(This application cannot be processed without current Federal DEA Certificate for each state in which you practice) Federal DEA Certificate #: _________________________________________ Expiration: _______________________________________________ Federal DEA Certificate #: _________________________________________ Expiration: _______________________________________________
VI. STATE NARCOTICS REGISTRATION: CONTROLLED SUBSTANCE REGISTRATION (CSR)
Some states require additional CSR certificates. Attach copies of any additional CSR certificates you have. State: _____________________________________________________________________________________________________________________ Certificate #: ____________________________________________________ Expiration: _______________________________________________ State: _____________________________________________________________________________________________________________________ Certificate #: ____________________________________________________ Expiration: _______________________________________________
KAPER-1 (04/2009) Page 63
VII. PROFESSIONAL LIABILITY DATA Answer the following questions as they apply to the last two (2) years: 1. Has your professional liability insurance coverage been terminated by action of the insurance company? Yes No
2. Have you been denied professional liability insurance coverage or been rated at a higher than average risk Yes No class for your specialty?
3. Has your present professional liability insurance carrier excluded any specific procedures from our coverage? Yes No
4. Have any professional liability suits or claims been filed against you? Yes No
5. Have any professional liability suits or claims been filed against you which are presently pending? Yes No
6. Have any judgments or settlements been made against you in professional liability cases? Yes No
7. If applying to an Indiana facility, do you participate in the Indiana Patient Compensation Fund? N/A Yes No
8. If applying to a Virginia facility, do you participate in the Birth-related Neurological Injury Compensation Act? N/A Yes No If the answer is yes to any of the above questions, please explain the case(s) and the outcome(s) on the following Professional Liability Detail Sheet. Provide a full explanation including the name of the carrier, the date and specific information concerning any limitation, settlement or judgment.
PROFESSIONAL LIABILITY DETAIL SHEET
(Please copy this page if additional sheets are needed)
CHECK HERE IF NOT APPLICABLE Please fill in the following details for each pending or settled malpractice suit or claim you have experienced:
Pending Settled Date: ____________________________ List the allegations: ___________________________________________________________________________________________________________ ____________________________________________________________________________________________________________________________ Date of occurrence: ___________________________________________________________________________________________________________ Name of institution involved (i.e., hospital): _________________________________________________________________________________________ Name and address of insurance carriers involved: ___________________________________________________________________________________ Please supply the following details for each malpractice lawsuit in which you were a defendant, and which resulted in a jury award or court judgments against you. Title of the court case: _________________________________________________________________________________________________________ The court case number: ________________________________________________________________________________________________________ The venue of the case (place where court case took place, such as County District Court or Circuit Court): ______________________________________ ____________________________________________________________________________________________________________________________ Allegations listed in complaint: __________________________________________________________________________________________________ Date of incident leading to complaint: _____________________________________________________________________________________________ Place of incident: _____________________________________________________________________________________________________________ Name and address of malpractice insurance carrier: _________________________________________________________________________________ ____________________________________________________________________________________________________________________________ Amount of jury award or amount awarded by the court: _______________________________________________________________________________
KAPER-1 (04/2009) Page 64
VIII. CERTIFICATION BY AMERICAN BOARD OF MEDICAL SPECIALTIES OR AMERICAN OSTEOPATHIC ASSOCIATION
(Allied Health Professional: list national certifications) 1. Are you board certified? Yes No (If not Board admissible, please explain on separate sheet and attach) 2. If yes, list full name of certifying board and date which you obtained certification/recertification:
_____________________________________________________________________________ Date: ____________________________ _____________________________________________________________________________ Date: ____________________________ _____________________________________________________________________________ Date: ____________________________ _____________________________________________________________________________ Date: ____________________________ _____________________________________________________________________________ Date: ____________________________
3. If you are not yet certified but have applied to a specialty board for examination, give the name of the board and date of application: _____________________________________________________________________________ Date: ____________________________
4. If status is one of eligibility, provide year when eligibility will terminate under rules of the specific board: _____________________________________ 5. List date of next required recertification (if applicable): ____________________________________________________________________________ 6. Have you ever been examined by a specialty board but failed to pass the exam? If yes, please explain. Yes No
IX. INDIVIDUAL PRACTICE INFORMATION Please answer each of the following questions in full AS THEY PERTAIN TO THE LAST TWO YEARS. If the answer to any question is "yes," please provide full explanation of the details on a separate sheet and attach. 1. Are there any actions that have been initiated or are any pending against you by any state licensing board? Yes No
Pending Resolved
2. Have you had any professional license or certification in any state that has ever been denied, limited, Yes No suspended, sanctioned, revoked, probated, voluntarily or involuntarily relinquished or not renewed?
3. Have you ever received notice of a proposed or actual exclusion (suspension, sanction, otherwise restricted) Yes No from any private health care program(s) or any health care program(s) funded in whole or in part by the state or federal government, including Medicare or Medicaid? If so, provide a detailed description of this matter, including the current status of your participation in such program(s).
4. Have you ever been the subject of an investigation by any private, federal or state agency concerning your N/A Yes No participation in any private, federal or state health insurance program?
5. Have your narcotics registration certificates ever been limited, suspended, revoked, voluntarily or N/A Yes No involuntarily surrendered or not renewed? 6. If applicable, is your federal (to include District of Columbia and territories of U.S.A.) and/or state narcotics N/A Yes No registration certificate being challenged? 7. Have you been named as a defendant or convicted of a felony or misdemeanor? Yes No
8. Have your employment, medical staff appointment or clinical privileges ever been voluntarily or involuntarily Yes No denied, suspended, diminished, revoked, limited or not renewed at any health care facility?
9. Have you ever withdrawn your application for appointment, reappointment, clinical privileges, or resigned Yes No from the medical staff of any health care facility before a decision was made by its governing board?
10. Have you ever been the subject of disciplinary proceedings or a focus review based on inappropriate Yes No quality of care at any hospital or health care facility?
11. Have you ever been denied membership or renewal thereof, or been subject to disciplinary or adverse Yes No action in any medical or professional organization?
X. PERSONAL HEALTH STATUS Please answer each of the following questions in full AS THEY PERTAIN TO THE LAST TWO YEARS. If the answer to any question is "yes," please provide full explanation of the details on the appropriate Explanation Sheet. 1. Do you currently have, or have you ever had any physical, mental, or emotional condition which impaired, or might Yes No reasonably be considered to impair, your ability to perform the procedures or provide the treatment for which you have requested clinical privileges or to meet the requirements of medical staff membership? 2. Have you ever been admitted to any hospital or been involved in a treatment program for any physical, mental or Yes No emotional condition which impaired or might reasonably be considered to impair, your ability to perform the procedures or provide the treatment for which you have requested clinical privileges or to meet the requirements of medical staff membership? 3. Do you currently have, or have you ever had a dependency on or abuse of the use of alcohol or drugs, or are you Yes No currently or have ever been involved in a treatment program for a dependency on or abuse of alcohol or drugs which impaired, or might reasonably be considered to impair, your ability to perform the procedures or provide the treatment for which you have requested clinical privileges or to meet the requirements of medical staff membership?
KAPER-1 (04/2009) Page 65
XI. PROFESSIONAL EMPLOYMENT AND AFFILIATIONS A. Employment List in chronological order all professional employment within the past two (2) years, starting with your current position. This includes all hospitals, corporations, military assignments, government agencies, group practices, other healthcare facilities or other types of activity. Complete addresses must be included. Date must be in MM/YY format. If you have a gap in employment of more than thirty (30) days, please explain on a separate page. "See CV" is not acceptable. Please attach additional sheets if more space is needed. Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________ Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________ Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________ Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________ B. Affiliations List in chronological order all professional affiliations within the past two (2) years, starting with your current position. This includes all hospitals, corporations, military assignments, government agencies, group practices, other healthcare facilities or other types of activity. Complete addresses must be included. Date must be in MM/YY format. If you have a gap in employment of more than thirty (30) days, please explain on a separate page. "See CV" is not acceptable. Please attach additional sheets if more space is needed. Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________
KAPER-1 (04/2009) Page 66
Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________ Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________ Name: ________________________________________________ Department: __________________________ _____________ / _____________ From (mm/yy) To (mm/yy) Address: __________________________________________________________ Type of Privileges/Position: _______________________________ City/St/ZIP: _______________________________________________________________________________________________________________ City St ZIP ZIP+ Country Phone: _________________________ Fax: _________________________ Email (if available): ________________________________________ Reason for leaving: ________________________________________________________________________________________________________
XII. PEER REFERENCES Name two peers who have personal knowledge of your current clinical abilities, ethical character, who will provide specific written comments on these matters upon request from Hospitals, Medical Societies, or Authorized Credentialing Services. The named individuals must have acquired the requisite knowledge through recent observation of your professional practice over a reasonable period of time, and at least one must have had organizational responsibility for your performance. The individuals should not be related to you by blood or marriage, training directors, partners/associates in your current group practice, or anyone with whom you have or anticipate having a financial relationship. Requested sources: practitioner in same specialty or practitioners with whom you have a referral pattern. If you recently completed training, you may use chief resident or other training colleague. Allied Health Professional should list their sponsoring physician, another physician and one peer from the same specialty as the applicant. Please note that you may be required to follow further directions of an individual hospital or facility in order to accommodate variations in medical staff bylaws. Reference: ________________________________________________________________________________________________________________ Address: _________________________________________________________________________________________________________________ City/St/ZIP: _____________________________________________________________________________ Country: ________________________ Phone: _________________________ Fax: _________________________ Email (if available): _________________________________________ Reference: ________________________________________________________________________________________________________________ Address: _________________________________________________________________________________________________________________ City/St/ZIP: _____________________________________________________________________________ Country: ________________________ Phone: _________________________ Fax: _________________________ Email (if available): _________________________________________
KAPER-1 (04/2009) Page 67
XIII. AUTHORIZATION AND RELEASE OF APPLICANT (HEALTHCARE FACILITY RELEASE)
(Please read carefully before signing) As a condition of applying for/accepting medical staff appointment or clinical privileges at the healthcare facilities listed in this application ("Hospital"), and whether or not my application is accepted, I acknowledge, consent, and agree as follows: A) I extend absolute immunity to, and release from all liability, the Hospital, its authorized representatives, and third parties (as defined in subsection C below), for any good faith communications, recommendations, disclosures or administrative action involving and pertaining to: (1) applications for appointment, reappointment or clinical privileges; (2) periodic reappraisals; (3) proceedings for suspension or reduction of clinical privileges or for denial or revocation of appointment, reappointment, or any other disciplinary action; (4) summary suspensions; (5) hearings and appellate reviews; (6) care evaluations; (7) utilization reviews; (8) any other healthcare facility, medical staff, department, service or committee activities; (9) my professional qualifications, credentials, clinical competence, character, mental or emotional stability, physical condition, ethics or behavior; and (10) any other matter that might directly or indirectly impact or reflect on my competence, on patient care or on the orderly operation of the Hospital. B) I will make myself available for interviews and acknowledge the burden of producing updated current information as to all questions on this application and such other information reasonably necessary to evaluate my qualifications. The Hospital and its authorized representatives may consult with and obtain information, including otherwise privileged or confidential information, from the Hospital's medical staff appointees and employees and from any third party bearing on my professional qualifications, all matters listed in subsection A, and any other matters bearing on my satisfaction of the criteria for reappointment to the medical staff. I authorize all persons and organizations having any knowledge of such matters to release said information to the Hospital or its authorized representatives upon request and I consent to the reporting of disciplinary information described below in section C. C) The term "Hospital and its authorized representatives" means the Hospital, its governing entity, persons who have any responsibility for or knowledge pertaining to the matters outlined in subsection A above, and authorized Centralized Verification Organization (CVO). The term "third party" means any individual, including a reappointee to the medical staff or other healthcare facilities, other physicians and health practitioners, government agencies, professional liability insurers, and other entities from whom or by whom the Hospital, authorized CVO, or other authorized representatives have requested or supplied information pertaining to matters in subsection A above. I acknowledge and agree that: (1) medical staff reappointment and clinical privileges are not a right; (2) applications and requests will be evaluated in accordance with prescribed procedures defined in the Hospital and medical staff bylaws, rules and regulations; (3) I shall be bound by the medical staff bylaws, rules and regulations, and corporate compliance programs, as amended from time to time, of hospitals to which I now and may subsequently apply; (4) I pledge to provide for continuous care for my patients in the hospital; (5) Hospital or its authorized representatives and third parties acting in their official capacities will notify authorized CVO and appropriate governmental agencies, boards or professional associations of disciplinary or professional action taken with respect to me if required to be reported to the Kentucky Medical Licensure Board by KRS 311.606 or if required to be reported by the authorized CVO, by medical staff bylaws, or by any other state or federal law; and (6) that this authorization, attestation and release is irrevocable for any period during which I am an applicant for or have medical staff privileges at Hospital, or, if later in time, for as long as Hospital may be under a duty to report information pursuant to the Health Care Quality Improvement Act of 1986. Pub. L. 99-660. I represent and warrant that at the time of this application and at all times while I maintain medical staff membership that (1) I am not nor have I ever been, excluded or suspended for any period of time whatsoever from participation in any state or federal health care program, including Medicare and Medicaid; (2) I have not been convicted under any state or federal law of any offense for which I could face mandatory exclusion from participation in any state or federal health care program, including Medicare and Medicaid; (3) I have not committed any act for which I may be permissibly excluded from participation in any state or federal health care program, including Medicare and Medicaid; (4) I do not hold, and have never held, a direct or indirect ownership or controlling interest of five percent (5%) or more in any entity that has been excluded or suspended for any period of time whatsoever from participation in any state or federal health care program, including Medicare and Medicaid, nor have I ever been an officer, director, agent, or managing employee of any such entity; and (5) I have never been convicted of a federal health care offense as defined in 18 U.S.C. § 24, including any theft, embezzlement, fraud, or other acts as prohibited therein with regard to any public or private health plan. I agree to notify Hospital immediately in the event I am unable to maintain one or more of these representations. D) Information and documents derived from or compiled in connection with matters listed in subsection A above, shall be privileged and confidential to the fullest extent permitted by law. Information contained in or attached to this application is accurate and complete to the best of my knowledge. Any misrepresentation, misstatement, or omission, whether intentional or not, may constitute cause for immediate rejection of this application and termination of any status or privilege granted in reliance upon it. Applicant's Signature: _______________________________________________________ Date: ________________________________





























