Embed Size (px)
DESCRIPTION
kbi white paper
Citation preview

White Paper
[KBI Antibacterial Hard Surface Disinfectant]
162-196 Innovation Drive, Winnipeg, Manitoba R3T 2N2 Tel: (204) 453-1301; Fax: (204) 474-7552; www.kanebiotech.com
White Paper on KBI Antibacterial Disinfectant
2
1.0 Introduction
For centuries, scientists thought infectious diseases were spread through the air or by direct person-to-person
contact. They believed the surrounding hard surfaces played little or no role.9 Until 1987, even the Centers for
Disease Control and the American Hospital Association focused on the spread of infection from one person to
another, thinking that flu infections were not spread from contaminated hard surfaces.9 Conventional strains
of the flu only lasted a few hours on hard surfaces. That thinking changed with the H1N1 pandemic as this virus
lives longer on hard surfaces than the typical flu, which survives just a few hours. Also, the bacterial pathogens
commonly isolated from hospital and food processing industry environment can survive on hard surfaces for
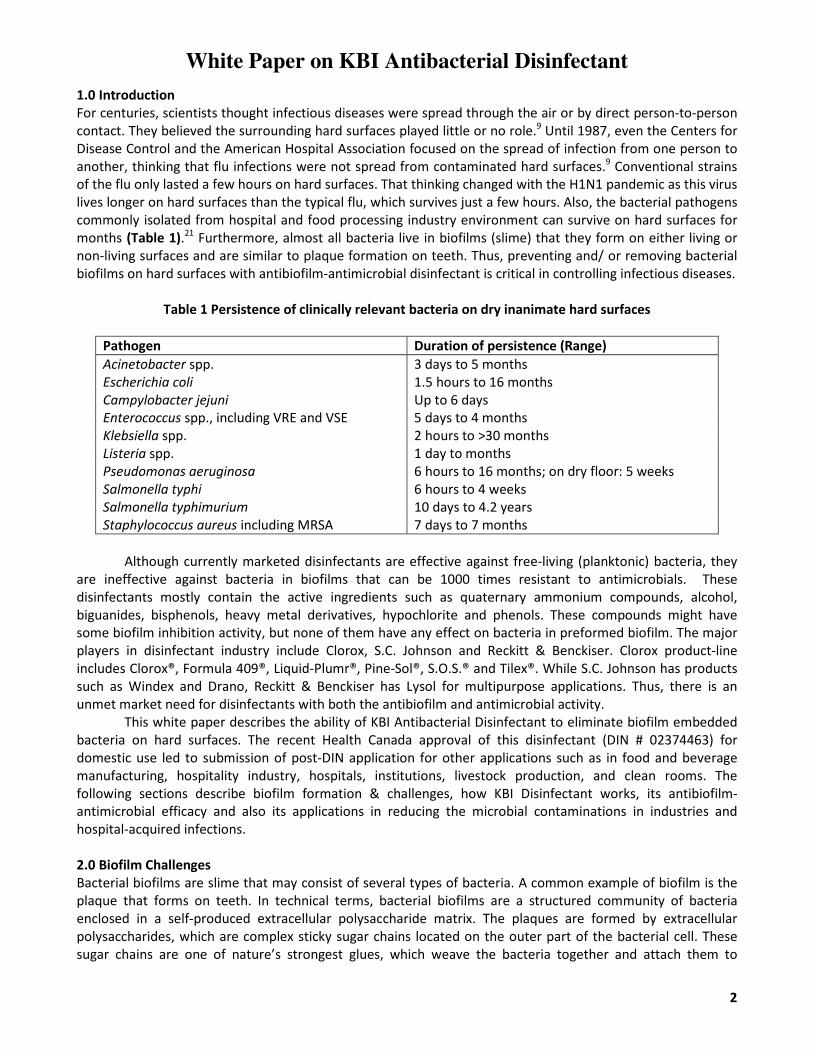
months (Table 1).21 Furthermore, almost all bacteria live in biofilms (slime) that they form on either living or
non-living surfaces and are similar to plaque formation on teeth. Thus, preventing and/ or removing bacterial
biofilms on hard surfaces with antibiofilm-antimicrobial disinfectant is critical in controlling infectious diseases.
Table 1 Persistence of clinically relevant bacteria on dry inanimate hard surfaces
Pathogen Duration of persistence (Range)
Acinetobacter spp. 3 days to 5 months
Escherichia coli 1.5 hours to 16 months
Campylobacter jejuni Up to 6 days
Enterococcus spp., including VRE and VSE 5 days to 4 months
Klebsiella spp. 2 hours to >30 months
Listeria spp. 1 day to months
Pseudomonas aeruginosa 6 hours to 16 months; on dry floor: 5 weeks
Salmonella typhi 6 hours to 4 weeks
Salmonella typhimurium 10 days to 4.2 years
Staphylococcus aureus including MRSA 7 days to 7 months
Although currently marketed disinfectants are effective against free-living (planktonic) bacteria, they
are ineffective against bacteria in biofilms that can be 1000 times resistant to antimicrobials. These
disinfectants mostly contain the active ingredients such as quaternary ammonium compounds, alcohol,
biguanides, bisphenols, heavy metal derivatives, hypochlorite and phenols. These compounds might have
some biofilm inhibition activity, but none of them have any effect on bacteria in preformed biofilm. The major
players in disinfectant industry include Clorox, S.C. Johnson and Reckitt & Benckiser. Clorox product-line
includes Clorox®, Formula 409®, Liquid-Plumr®, Pine-Sol®, S.O.S.® and Tilex®. While S.C. Johnson has products
such as Windex and Drano, Reckitt & Benckiser has Lysol for multipurpose applications. Thus, there is an
unmet market need for disinfectants with both the antibiofilm and antimicrobial activity.
This white paper describes the ability of KBI Antibacterial Disinfectant to eliminate biofilm embedded
bacteria on hard surfaces. The recent Health Canada approval of this disinfectant (DIN # 02374463) for
domestic use led to submission of post-DIN application for other applications such as in food and beverage
manufacturing, hospitality industry, hospitals, institutions, livestock production, and clean rooms. The
following sections describe biofilm formation & challenges, how KBI Disinfectant works, its antibiofilm-
antimicrobial efficacy and also its applications in reducing the microbial contaminations in industries and
hospital-acquired infections.
2.0 Biofilm Challenges
Bacterial biofilms are slime that may consist of several types of bacteria. A common example of biofilm is the
plaque that forms on teeth. In technical terms, bacterial biofilms are a structured community of bacteria
enclosed in a self-produced extracellular polysaccharide matrix. The plaques are formed by extracellular
polysaccharides, which are complex sticky sugar chains located on the outer part of the bacterial cell. These
sugar chains are one of nature’s strongest glues, which weave the bacteria together and attach them to

White Paper on KBI Antibacterial Disinfectant
3
surfaces. They start with an individual bacterial cell (also called free-living or planktonic cell) and these free-
living cells are the building blocks of biofilms (Figure 1). Bacterial cells attach to a hard surface using their gluey
extracellular polysaccharide structures. This is the first step in biofilm formation, followed by the bacterial cell-
cell attachment. This sequence of events leads to a highly structured and organized ecosystem that is self-
sustaining and provides a continuous source of contamination. Biofilms can form on any hard surfaces
including kitchen counter tops, hospital beds, food processing equipments, and cooling water towers.
Figure 1: Biofilm Formation
According to an estimate by the National Institute of Health (NIH, USA), about 80% of all human bacterial
infections are caused by biofilms.24 From a medical perspective, both commensal and pathogenic
microorganisms form biofilm-like conglomerates that are associated with the epithelial or endothelial lining;
embedded in the lung, intestinal or vaginal mucus layer; attached to the teeth or medical implant surfaces, or
formed intracellularly or formed on hard surfaces. Biofilm formation and persistence has profound
implications for the patient, because microorganisms growing as biofilms are 100-1000 times less susceptible
to antibiotics and host defenses than free-living bacteria. Biofilm-associated resistance could be attributed to
the following: (i) antimicrobials fail to penetrate beyond the surface layers of biofilm; (ii) antimicrobials may be
trapped and destroyed by enzymes in the biofilm matrix; (iii) presence of non-growing bacteria (persister cells)
against which antimicrobials are not active; (iv) expression of biofilm-specific genes; and (v) overexpression of
antimicrobial-destroying enzymes in response to hostile environmental conditions. Many biofilm infections are
notoriously difficult to resolve and they commonly manifest as chronic or recurrent infections. Biofilm
infections constitute a number of clinical challenges, including diseases involving uncultivable species, chronic
inflammation, impaired wound healing, and rapidly acquired antibiotic resistance.
3.0 How KBI Disinfectant Works
KBI Antibacterial Disinfectant contains synergistic antibiofilm-antimicrobial combination comprising
Chlorhexidine (CHX) and Sodium Metaperiodate (SMP). Both the compounds have a broad-spectrum
antimicrobial activity and sodium metaperiodate also has a broad-spectrum antibiofilm activity. When the
biofilm is disrupted by sodium metaperiodate, chlorhexidine rapidly kills bacteria embedded in biofilm on a
hard surface (Figure 2). While chlorhexidine kills bacteria by disrupting bacterial cell membrane, sodium
metaperiodate disrupts biofilms by oxidizing carbons bearing hydroxyl groups in polysaccharides, thereby
cleaving C-C bonds.38 When these two compounds are used in combination, sodium metaperiodate increases
the antimicrobial activity of chlorhexidine.15
Bacteria embedded
in a biofilm
Polysaccharide matrix
Bacteria embedded
in a biofilm
Polysaccharide matrix

White Paper on KBI Antibacterial Disinfectant
4
Figure 2: KBI Disinfectant in Action
4.0 Antibiofilm Efficacy of KBI Disinfectant
4.1 Synergistic Activity:
The synergistic antimicrobial and antibiofilm efficacy of Chlorhexidine (CHX) and Sodium Metaperiodate (SMP)
combination was tested against E. coli, and Pseudomonas aeruginosa growth and biofilm formation using a
standard 96-well crystal violet staining biofilm assay. Bacteria were grown in Tryptic Soy Broth (TSB) medium in
a 96-well microtiterplate in the absence and presence of CHX and SMP alone and combination (CHX+SMP). The
combination of CHX and SMP inhibited significantly more E. coli and P. aeruginosa growth and biofilm
compared to CHX or SMP alone (Figure 3).
SMP breaks down
polysaccharide
matrix releasing
biofilm embedded
bacteria
Bacteria
CHX kills bacteria
by rupturing cell
membrane
Polysaccharide matrix
Bacteria
SMP breaks down
polysaccharide
matrix releasing
biofilm embedded
bacteria
Bacteria
CHX kills bacteria
by rupturing cell
membrane
Polysaccharide matrix
Bacteria

White Paper on KBI Antibacterial Disinfectant
5
Figure 3: Synergistic Inhibitory Effect of Chlorhexidine (CHX) and Sodium Metaperiodate (SMP) Alone and in
Combination on Growth and Biofilm Formation of E. coli, and P. aeruginosa
4.2 Antibiofilm Activity:
Two different types of in vitro models such as Minimum Biofilm Eradication Concentration (MBEC™) Assay
(Innovotech, Edmonton, AB, Canada) and CDC biofilm reactor (CBR) Assay (BioSurface Technologies, Corp.,
Bozeman, MT) were used to evaluate the efficacy of KBI Antibacterial Disinfectant against Pseudomonas
aeruginosa biofilm. Both the assay methods are approved by the USA standard setting organization American
Society for Testing and Materials International (ASTM International) for evaluating antibiofilm activity of
disinfectant product on hard surfaces. While biofilm is formed under a low shear force using MBEC™ assay,
CBR assay represent biofilm formed under high shear force.1, 5
P. aeruginosa produced 4.46 log10 CFU/mm2 and 8.38 log10 CFU/cm2 biofilm on MBEC pegs (low shear
force) and in CDC biofilm reactor (high shear force), respectively. By using two different methods, we were
able to study the antibiofilm activity of disinfectants against biofilm produced under two different shear forces.
However, the MBEC assay of low shear biofilm may be more relevant to ‘Hard Surface’ disinfectants compared
to CDC Biofilm Reactor assay of high shear biofilm. Biofilm produced under high shear force was more robust
and therefore, it was more resistant to disinfectant treatment than biofilm formed under a low shear force.
While KBI Antibacterial Disinfectant killed 100% biofilm-embedded P. aeruginosa cells grown under a low
shear force, about 4 log reduction (more than 99.99% kill) was observed under high shear force (Figure 4).
When tested in comparison with commercially available Quaternary Ammonium Chloride (Quats) disinfectant
product, KBI Antibacterial Disinfectant was 10-100 times more effective in killing biofilm embedded P.
aeruginosa cells. Superior antibiofilm activity of KBI Antibacterial Disinfectant under both the assay conditions
could be attributed to antibiofilm compound sodium metaperiodate in the formulation.
Growth @ 600 nm Biofilm @ 630 nm
E. coli P. aeruginosa
0
20
40
60
80
100
120
Control CHX SMP CHX+SMP
Per
centa
ge
0
20
40
60
80
100
120
Control CHX SMP CHX+SMPP
erce
nta
ge
Growth @ 600 nm Biofilm @ 630 nmGrowth @ 600 nm Biofilm @ 630 nm
E. coli P. aeruginosa
0
20
40
60
80
100
120
Control CHX SMP CHX+SMP
Per
centa
ge
0
20
40
60
80
100
120
Control CHX SMP CHX+SMPP
erce
nta
ge

White Paper on KBI Antibacterial Disinfectant
6
Figure 4: Comparison of Antibiofilm Activity of KBI Disinfectant with a Commercial Product
4.3 Antimicrobial Activity:
The broad spectrum antimicrobial activity of KBI Disinfectant product is mainly due to chlorhexidine (Table 2).
Chlorhexidine is a membrane-active agent, causing protoplast and spheroplast lysis. At a higher concentration,
it causes precipitation of proteins and nucleic acids.
Table 2 Broad-Spectrum Antimicrobial Activity of Chlorhexidine6, 11, 16, 18, 25, 37
Bacteria Yeast/Fungi
• Candida albicans
• C. glabrata
• C. krusei
• C. parapsilosis
• C. tropicalis
• Aspergillus fumigatus
Virus
• Staphylococcus aureus
• Methicillin-resistant Staphylococcus aureus (MRSA)
• S. epidermidis
• Micrococcus luteus
• Streptococcus faecalis
• Neisseria sicca
• Klebsiella pneumoniae
• Aeromonas hydrophila
• Acinetobacter baumannii
• Citrobacter diversus
• Enterobacter cloacae
• Pseudomonas aeruginosa
• Proteus mirabilis
• Vancomycin-resistant Enterococci (VRE)
• Mycobacterium species (Bacteriostatic effect)
• Legionella pneumophila
• Escherichia coli O157:H7
• Listeria monocytogenes
• Salmonella spp.
• Campylobacter jejuni
• Herpes Simplex
• Influenza A
• Hepatitis B
0.001
0.15
0.004
0.031
0.001
0.01
0.1
1
10
100
% B
iofilm
MBEC Device (Low Shear Force) CBR (High Shear Force)
Control KBI Antibacterial Disinfectant Commercial Product (Quat)

White Paper on KBI Antibacterial Disinfectant
7
The antimicrobial activity of KBI Antibacterial Disinfectant was determined by Use-Dilution method as
described by Official Methods of Analysis of the Association of Official Analytical Chemists.2-4 The Use-Dilution
Method determines disinfectant activity for germicidal solutions. Staphylococcus aureus and Salmonella
choleraesuis are tested to support broad-spectrum disinfectant activity claims. Germicides that are intended
for use in hospitals or other health care facilities need to be tested against Pseudomonas aeruginosa.
Additional organisms that may be clinically significant are tested as an option. The Use-Dilution Method is a
qualitative carrier test. Stainless steel penicylinders are soaked for 15 minutes in a broth culture of the test
organism. The contaminated carriers are then removed and dried for approximately 30 minutes at 37ºC. This
now represents a nonporous, hard, inanimate surface contaminated with a dried film of bacteria. The
contaminated carriers are exposed to 10 ml of the KBI Antibacterial Disinfectant for 10 minutes at 20ºC. After
treatment; the carriers are removed from the disinfectant and placed in 10 ml subculture broth media
containing appropriate neutralizers. The subculture tubes are incubated 48 hours at 37ºC.
The tubes are examined for growth as determined by turbidity of the media. An effective disinfectant
for hospital use kills all the bacteria on 59 or 60 out of 60 carriers tested against S. aureus, S. choleraesuis and
P. aeruginosa (Table 2). For additional organisms, all the bacteria on 10 out of 10 carriers tested must be killed.
KBI disinfectant was effective in inhibiting pathogens including hospital related infections, medical device
associated infections, antibiotic resistant pathogens and food pathogens.
Table 2: Broad-Spectrum Activity of KBI Disinfectant
Number of Carriers Test Organism
Exposed Showing Growth
Staphylococcus aureus (ATCC 6538) 180 0
Pseudomonas aeruginosa (ATCC 15442) 180 0
Salmonella choleraesuis (ATCC 10708) 180 0
Escherichia coli O157:H7 20 0
E. coli (ATCC 25404) 20 0
Acinetobacter baumannii 20 0
Methicillin-resistant S. aureus (MRSA) 20 0
Vancomycin-resistant Enterococci (VRE) 20 0
Listeria monocytogenes 20 0
Klebsiella pneumoniae 20 0
Campylobacter jejuni (ATCC 33560) 20 0

White Paper on KBI Antibacterial Disinfectant
8
5.0 Market Applications
Home
Kitchen countertops
Kitchen sink
Dining table
Bath tub
Toilet seat
Athletic Facilities
Professional Team Sports
Collegiate Sports Facilities
High School Sports Facilities
Middle School Sports Facilities
Fitness Centers
Spas
Aquatic Centers and Swim Clubs
Athletic Training Centers
Educational Institutions
Pre-schools
Daycare Centers
Church Nurseries
Universities and Colleges
High Schools
Middle Schools
Elementary Schools
Kindergartens
Vocational Schools
Retreats and Conference
Centers
Healthcare
Hospitals
Emergency Rooms
Out Patient Surgery Centers
Physician Offices
Long Term Care Facilities
Physical Therapy Facilities
Chiropractic offices
Pharmacies
Hospice Centers
Home healthcare
Rehabilitation Facilities
Hospitality Industry
Hotels
Motels
Resorts
Restaurants
Food Industry
USDA Inspected Meat and
Poultry Plants
Snack Food Processing Plants
Dairy and Egg Plants
Beverage Plants
Breweries and Micro Breweries
Seafood Processing Plants
Frozen Pizza Plats
Animal Care
Veterinary Hospitals
Kennels
Animal Rescue Shelters
Other
Construction Companies
Banks
Museums
Hair and Beauty Salons
Barber Shops
Marine and Boat Facilities
Business Offices
Theaters
5.1 Domestic Applications:
The first comprehensive study was done by Finch et al.12 in which bacteria were isolated from numerous
surfaces throughout the home. The most notable result was that the kitchen sink was found to harbour large
numbers of Escherichia coli and Enterobacter spp., whereas toilet areas showed little evidence of
contamination with organisms of fecal origin. This study was followed by even larger investigation by Scott et
al.32 where the bacterial species and frequency of occurrence in 201 homes was reported. They found more
than 80% of the homes examined one or more species of Enterobacteria at wet sites such as kitchen sink, and
sink-U tube. The frequent occurrence of E. coli in high numbers in sink U-tubes (38.8 %) and on sink surfaces
(18.7 %) indicates that these organisms may be actively growing. It was established that potentially
enteropathogenic E. coli strains were present in the kitchen sink areas in 16 out of the 41 homes examined.
Scott et al.33 continued their research with an evaluation of phenolic disinfectant and hypochlorite disinfectant
in household kitchens. Results indicate that the disinfectant products showed substantial, but brief, reduction
in bacterial contamination. Josephson, et al.19 monitored eight locations within kitchen area. Almost all

White Paper on KBI Antibacterial Disinfectant
9
locations at all households exhibited contamination, with the sink and sponge samples exhibiting large
bacterial concentrations. The fecal coliform concentrations in sink and sponge samples were very high, with 63
and 67% of all samples being positive, respectively. In addition, data show that normal kitchens can easily be
contaminated with a variety of bacterial contaminants including fecal coliforms, E. coli, Salmonella, and
Campylobacter. The failure of the disinfectant products and very high frequency of isolating food pathogens
from wet areas such as kitchen sink and sink drain pipe could be attributed to biofilm formation, which acts as
a source of contamination.13 In addition, two separate studies indicate that food contact surfaces support
biofilm growth which acts as a source of cross contamination with E. coli and S. typhimurium.10, 29 Furthermore,
Neth, et al.27 demonstrated that the sanitizers and cleaning procedures failed to irradiate biofilm formed on
plastic cutting board. They have noticed moderate 10% reduction in bacterial load after sanitizing and cleaning
plastic cutting board. Several approaches have been developed to control microbial attachment; one approach
is the development of food contact materials incorporating antimicrobial compounds. Rodrigues, et al.31
evaluated Salmonella enterica Enteritidis adhesion and biofilm formation on regular and triclosan-impregnated
kitchen bench stones (silestones). Enumeration of adhered cells on granite, marble, stainless steel, and
silestones revealed that all materials were prone to bacterial colonization and no significant effect of triclosan
was found. The results of these studies and an increase in the outbreaks of food-borne diseases led to
realization of the need for disinfectants with antibiofilm activity.
5.2 Food Processing Industry
The presence of biofilms is common in food industry. Biofilms can exist on all types of surfaces in food
processing plants ranging from floors, walls, pipes and drains, and surfaces of equipment including stainless
steel, aluminum, nylon, Teflon, rubber, plastic, glass. Food contact surfaces such as conveyer belts,
pasteurizers, crevices, gaskets and dead spaces as well as areas that are hard to clean and sanitize, may
harbour biofilms. Also of concern is the potential of attachment of microorganisms on food surfaces, which
may affect the efficacy of interventions applied to carcasses, meat, produce or other foods to reduce
contamination.8 The attachment of the bacteria to the food product or the product contact surfaces leads to
serious hygienic problems and economic losses due to food spoilage. The United States Department of
Agriculture (USDA) estimates the costs associated with food borne illness to be about $5.5 billion to $22 billion
a year. This doesn’t include the billions lost every year due to spoiled product, which must be disposed or sold
as a lesser valued product. In addition to that, a number of reports have appeared on the persistence of
several food borne pathogens on food contact surfaces. For these reasons, it is considered that the presence of
biofilms in the food processing systems is a serious public health risk. Although many species of bacteria are
able to form biofilms in the food industry, the most important species in relation to food safety are listed
below.
Listeria monocytogenes:: A 2004 audit of food processing facilities by the USDA Food Safety and Inspection
Service reported that 27.8% of floors and drains sampled tested positive for Listeria, one of the common
illness-causing bacteria found in biofilm. L. monocytogenes is a hardy pathogen with ability to proliferate in
cold wet environments that are ideal for biofilm formation. In such close proximity to food preparation areas,
this creates a significant potential threat of cross contamination. The most prevalent strain of L.
monocytogenes (strain1/2c) found in food processing plants has good adhesion ability and requires only a
short contact time for attachment. Studies have shown that this pathogen can create a biofilm in slicers and
other steel utensils.20 This fact demonstrates the importance of this biofilm as a factor in cross-contamination.
The dairy industry has described the presence of Listeria in milk and dairy products which may be associated
with the emergence of clinical outbreaks. It has also been shown that milk protein remains in pipes reduces
bacteria, and have a possible inhibitory ability on the biofilm formation in its early stages. However, once
established, milk residues in pipes provide a source of nutrients and therefore favour the survival of the
biofilm.22 Based on recent estimates from the Centers for Disease Control and Prevention, the annual

White Paper on KBI Antibacterial Disinfectant
10
incidence of death caused by listeriosis is about eight times greater than mortality due to Escherichia coli
O157:H7 infections.26
Salmonella spp: The incidence of human pathogens on fresh produce is a serious concern in industrialized
countries. Salmonella spp. is one of the most commonly isolated pathogens associated with fresh produce
where preliminary FoodNet data on the incidence of food borne illness showed Salmonella at the top of the
overall incidence in the United States.28 Outbreaks of salmonellosis have been linked to a wide variety of fresh
produce including alfalfa sprouts, lettuce, fennel, cilantro, cantaloupes, unpasteurized orange juice, tomatoes,
melons, mango, celery and parsley.28, 29 Also, contamination of fruits and vegetables may occur at various
stages during production, harvest, processing, and transport. According to the research findings of the USDA
labs, Salmonella spp. in contact with solid inert surface and fresh cut fruits as well as vegetables are 4-5 times
more resistant than their free-living counterparts.14 Attached microorganisms (pathogens and spoilage
bacteria) are not easily removed by washing with water or antibacterial agents.
Escherichia coli: Escherichia coli O157:H7 is an important causative agent of severe gastrointestinal disease in
humans. E. coli O157:H7 causes the majority of sporadic and multi-person outbreaks of bloody diarrhea in the
U.S. E. coli O157:H7 infection is also responsible for most cases of hemolytic–uremic syndrome, a major cause
of acute renal failure in children. The pathogen has a low infection dose, as low as 10–100 organisms. The
Centers for Disease Control and Prevention (CDC) estimates that E. coli O157:H7 causes more than 70,000
illnesses and 60 deaths each year in the U.S.26 E. coli O157:H7 can persist in the farm environment, soil, water,
sediment, and animal carcasses. Healthy cows are known to be the major reservoir of E. coli O157:H7. This
pathogen is transmitted from contaminated cattle to farm water and soil through fecal contamination. A large
number of outbreaks of E. coli O157:H7 have been associated with the consumption of contaminated ground
beef and raw milk. There has also been an increase in E. coli O157:H7 outbreaks associated with produce
products, such as lettuce, apple cider, cantaloupe, and alfalfa sprouts in recent years.35 In 2006, multistate
outbreaks of E. coli O157:H7 infections through consumption of contaminated spinach and lettuce resulted in
199 illnesses in 26 states and 71 illnesses in 5 states, respectively.7 E. coli O157:H7 has shown the ability to
attach, colonize, and form biofilms on a variety of surfaces. In addition, E. coli O157:H7 is able to form biofilm
on produce including spinach, lettuce, Chinese cabbage, celery, leeks, basil, and parsley. E. coli O157:H7 that
had attached on the surface of stainless steel was able to transfer to meat, poultry, ready-to-eat deli, and
produce products.34 Strong attachment of the transferred pathogen on produce products (cantaloupe, lettuce,
carrot, and spinach) was detected (>103 CFU/cm2) even after washing these products with water. These
findings suggest the importance of biofilm formation by E. coli O157:H7 on food contact surfaces can be a
concern for efficient control of the pathogen particularly in produce products that require no heating or
cooking prior to consumption.
Campylobacter jejuni: Although Campylobacter does not multiply in food, its minimum infective dose is very
low, less than in any other pathogen. One of the mechanisms of survival of Campylobacter spp. in the
environment is the formation of biofilms. Campylobacter is capable of producing these biofilms in aquatic
media or stainless steel and glass surfaces. The ability of C. jejuni to develop biofilms faster under aerobic
conditions (20% O2) than in microaerophilic conditions (5% O2, 10% CO2), shows the capacity of this micro-
organism to adapt the conditions of the biofilm on their behalf, acting as a reservoir of viable cells.30 These
studies highlight the role of biofilms for the maintenance of Campylobacter in environments of processed
food, increasing the risk of contamination.
Bacillus spp: Bacillus spp. is found throughout dairy processing plants. Bacillus survives heat processing and
accumulates in pipelines and joints in the processing environment. If hot fluid continuously flows over a
surface for over 16 h, Bacillus and other bacteria that survive pasteurization process may form a biofilm.8

White Paper on KBI Antibacterial Disinfectant
11
One of the main problems of the food industry is represented by the survival of food borne pathogenic
or spoilage microorganisms due to an insufficient disinfection of surfaces or instruments that come in contact
with food. Biofilms formed on these surfaces are the main cause of contamination of the final product. Lee and
Frank23 found that L. monocytogenes adhering for 8 days were 100 times more resistant to hypochlorite
sanitizer than those adhering for only 4 days. In addition, biofilms formed on the raw meat surfaces and in
processing environment also offer considerable problems of cross contamination, disinfectant resistance and
post-processing contamination. These findings highlight the need for disinfectants that have both the
antimicrobial and antibiofilm activity for prevention and removal biofilms on hard surfaces or food contact
surfaces.
5.3 Hospital-Acquired Infections
The hospital-acquired (Nosocomial) infections are infections acquired from the hospitals as well as any other
health care facility such as nursing homes and health clinics. The importance of hospital-acquired infections
seems to have become better understood only in these past few decades. Hospital-acquired infections have
been a huge burden on the overall population. The US Centers for Disease Control and Prevention has
attributed hospital-acquired infections as the fourth leading cause of deaths after heart disease, cancer and
stroke. In the United States, about two million hospital-acquired infections occur every year leading to more
than $5 billion in added medical cost per annum.39
It is believed that the majority (80%) of health care infections are caused by the microbial flora that
patient bring with them to the health care facility.36 This micro-flora seems to be opportunistic to the new
environment and is able to take advantage of new routes that medical procedures offer including surgery,
implanted medical devices, and reusable medical devices. Other hospital-acquired infections (10% to 20%)
develop following contamination found within the health care environment including hospital bed, furniture,
clothing, toilets, air, water, and health care personnel. About 60–70% of hospital-acquired infections are
associated with some type of implanted medical device. It is estimated that over 5 million medical devices or
implants are used per annum in the U.S. alone. The worldwide production of biomedical devices and tissue
engineering-related materials is about $180 billion a year industry and expanding rapidly. Regardless of the
sophistication of the biomedical implant (catheters versus a three-dimensional stem cell-containing polymer
scaffold), all medical devices or tissue engineering constructs are susceptible to microbial colonization and
infection.
Antimicrobial resistance in bacteria including methicillin-resistant S. aureus (MRSA), vancomycin-
resistant Enterococci (VRE), and carbapenem resistant Klebsiella pneumoniae is also a major worldwide health
care issue. Particularly, MRSA infection kills ~19,000 hospitalized American patients annually, which is similar
to the number of deaths due to AIDS, tuberculosis, and viral hepatitis combined. A significant risk factor for
these healthcare associated infections is the extensive use of implanted prosthetic biomaterials for diagnostic
and therapeutic purposes, which can be colonized by staphylococci giving rise to device-related infections
involving biofilms. The challenge of staphylococcal biofilm infections is compounded by the existence of
multiple biofilm mechanisms in both S. aureus and S. epidermidis.
The elderly population and patient with weakened immune system are vulnerable to hospital-acquired
infections caused by Legionella pneumophila. Legionella pneumophila infection can cause Legionnaires'
disease and Pontiac fever, a severe form of pneumonia. The symptoms of Legionnaire's disease include
confusion, headache, diarrhoea, abdominal pain, fever, chills, and myalgia as well as a non-productive cough.
Pontiac fever is a milder flu-like illness without pneumonia. Each year, between 8,000 and 18,000 people are
hospitalized with Legionnaires' disease in the U.S. Mortality rate is reported to be 15-25%. Anyone can get
legionellosis, but the risk of developing Legionnaires' disease is greater for men who are middle aged and
older. The bacteria are found in water sources. They can multiply in stagnant water at certain temperatures
(between 25°C and 45°C). People become infected by breathing in droplets, mist or steam containing the
bacteria.

White Paper on KBI Antibacterial Disinfectant
12
In addition, mold is a major contributor of health care infections. The mold Candida species for
example, is the fourth leading cause of hospital-acquired blood stream infections in the US hospitals.17 Data
has shown that patients who acquire candidemia are likely to die during hospitalization as a result of the
infection.17 According to Gudlaugsson and associates, the prevention of health care infections caused by
Candida species should be a high priority for any health care facility.
6.0 References
1. American Society for Testing and Materials International (ASTM) Standard Test Method for Testing
Disinfectant Efficacy against Pseudomonas aeruginosa Biofilm using the MBEC Assay (Protocol # E2799-
11).
2. Association of Official Analytical Chemists AOAC Official Method 955.15 Testing Disinfectants against
Staphylococcus aureus.
3. AOAC Official Method 964.02 Testing Disinfectants against Pseudomonas aeruginosa.
4. AOAC Official Method 955.14 Testing Disinfectants against Salmonella choleraesuis.
5. ASTM Standard Test Method for Quantification of Pseudomonas aeruginosa Biofilm Grown with High
Shear and Continuous Flow using CDC Biofilm Reactor (Protocol # E2562-07).
6. Bernstein, D., Schiff, G., Schler, G., Prince, A., Feller, A., and Briner, W. (1990) In vitro virucidal
effectiveness of a 0.12% chlorhexidine gluconate mouthrinse. Journal of Dental Research 69, 874-876.
7. Centers for Disease Control and Prevention, (2006) Multistate outbreak of E. coli O157:H7 infections,
November–December 2006. Available from: http://www.cdc.gov/ecoli/2006/december/121406.htm.
8. Chmielewski, R.A.N, and Frank, J.F. (2003) Biofilm formation and control in food processing facilities.
Comprehensive Reviews in Food Science and Food Safety 2, 22-32.
9. Cozad, A., and Jones, R.D. (2003) Disinfection and the prevention of infectious disease. American Journal
of Infection Control 31, 243-254.
10. De Wit, J.C., Broekhuizen, G., and Kampelmacher, E.H (1979) Cross contamination during the preparation
of frozen chickens in the kitchen. Journal of Hygiene, Cambridge 83, 27-32.
11. Emilson, C.G. (1977) Susceptibility of various microorganisms to chlorhexidine. Scandinavian Journal of
Dental Research 85, 255-265.
12. Finch, J.E., Prince J., and Hawksworth, M (1978) A bacteriological survey of the domestic environment.
Journal of Applied Bacteriology 45, 357-364.
13. Furuhata, K., Ishizaki, N., and Fukuyama, M. (2010) Characterization of heterotrophic bacteria isolated
from the biofilm of a kitchen sink. Biocontrol Science 15, 21-25.
14. Gawande, P.V. and Bhagwat, A.A. (2002) Inoculation onto solid surfaces protects Salmonella spp. during
acid challenge: a model study using polyethersulfone membranes. Applied and Environmental
Microbiology 68, 86-92.
15. Gawande, P.V., LoVetri, K., Yakandawala, N., Romeo, T., Zhanel, G.G., Cvitkovitch, D.D., and Madhyastha,
S (2008) Antibiofilm activity of sodium bicarbonate, sodium metaperiodate and SDS combination against
dental unit waterline associated bacteria and yeast. Journal of Applied Microbiology 105: 986–992.
16. Griffiths, W., Favet, J., Eggimann, P., Auckenthaler, R., Peduzzi, R., Chevrolet, J.C., and Dommeyer, A.
Development of a chlorhexidine mouthwash for oro-pharyngeal decontamination (OPD) to be used in a
future clinical study in critically ill patients-1st communication. http://pharmacie.hug-
ge.ch/rd/posters/escp00_wg_des.pdf.
17. Gudlaugsson O., Gillespie, S., Lee, K., Berg, J.V., Hu, J., Messer, S., Herwaldt, L., Pfaller, M., and Diekema,
D. (2003) Attributed mortality of nosocomial candidemia, revisited. Clinical Infectious Diseases, 37, 1172-
1177.
18. Hiom, S.J., furr, J.R., Russell, A.D., and Dickinson, J.R. (1992) Effects of chlorhexidine diacetate on
Candida albicans, C. glabrata and Saccharomyces cerevisiae. Journal of Applied Bacteriology 72, 335-340.

White Paper on KBI Antibacterial Disinfectant
13
19. Josephson, K.L., Rubino J.R., and Pepper, I.L. (1997) Characterization and quantification of bacterial
pathogens and indicator organisms in household kitchens with and without the use of a disinfectant
cleaner. Journal of Applied Microbiology 83, 737-750.
20. Keskinen, L.A., Todd, E.C.D., and Ryser, E. (2008) Transfer of surface dried Listeria monocytogenes from
stainless steel knife blades to roast turkey breast. Journal of Food Protection 71, 176-181.
21. Kramer, A., Schwebke, I., and Kampf, G. (2006) How long do nosocomial pathogens persist on inanimate
surfaces? A systematic review. BMC Infectious Diseases 6,130.
22. Lee Wong, A.C. (1998). Biofilms in food processing environments. Journal of Dairy Science 81, 2765-2770.
23. Lee, S., and Frank, J.F. (1991) Inactivation of surface adherent Listeria monocytogenes using hypochlorite
and heat. Journal of Food Protection 54, 4-6.
24. Lewis, K. (2001) Riddle of biofilm resistance. Antimicrobial Agents Chemotherapy 45, 999–1007.
25. McDonnell, G., and Russell, A.D. (1999) Antiseptics and disinfectants: Activity, action, and resistance.
Clinical Microbiology Reviews 12, 147-179.
26. Mead, P.S., Slutsker, L., Dietz, V., McCaig, L.F., Bresee, J.S., Shapiro, C., Griffin, P.M., Tauxe, R.V., 1999.
Food-related illness and death in the United States. Emerging Infectious Diseases 5, 607–625.
27. Neth, K., Girard, D., and Albrecht, J. (2008) Determination of biofilm on plastic cutting boards. RURALS:
Review of Undergraduate Research in Agricultural and Life Sciences, University of Nebraska-Lincoln, 3,
Article 5.
28. Penteado, A. L. and Leitao, M. F. F. (2004) Growth of Salmonella Enteritidis in melon, watermelon and
papaya pulp stored at different times and temperatures. Food Control 15, 369-373.
29. Pui, C.F., Wong, W.C., Chai, L.C., Lee, H.Y., Tang, J.Y.H., Noorlis, A., Farinazleen, M.G., Cheah, Y.K., and
Son. R. (2011) Biofilm formation by Salmonella Typhi and Salmonella Typhimurium on plastic cutting
board and its transfer to dragon fruit. International Food Research Journal 18, 31-38.
30. Reuter, M., Mallett, A., Pearson, B.M., and van Vliet, A.H.M. (2010) Biofilm formation by Campylobacter
jejuni is increased under aerobic conditions. Applied and Environmental Microbiology 76, 2122-2128.
31. Rodrigues, D., Teixeira, P., Oliveira, R., and Azeredo, J. (2011) Salmonella enterica Enteritidis biofilm
formation and viability on regular and triclosan-impregnated bench cover materials. Journal of Food
Protection 74, 32-37.
32. Scott, E., Bloomfield, S.F., and Barlow, C.G. (1982) An investigation of microbial contamination in the
home. Journal of Hygiene, Cambridge 89, 279-293.
33. Scott, E., Bloomfield, S.F., and Barlow, C.G. (1984) Evaluation of disinfectants in the domestic
environment under ‘in use’ conditions. Journal of Hygiene, Cambridge 92, 193-203.
34. Silagyi, K., Kim, S.H., Lo M., and Wei, C.I. (2009) Production of biofilm and quorum sensing by Escherichia
coli O157:H7 and its transfer from contact surfaces to meat, poultry, ready-to-eat deli, and produce
products. Food Microbiology 26, 519-519.
35. Sivapalasingam, S., Friedman, C.R., Cohen, L., Tauxe, R.V., 2004. Fresh produce: a growing cause of
outbreaks of food borne illness in the United States, 1973 through 1997. Journal of Food Protection 67,
2342–2353.
36. Tilton, D. (2003). Nosocomial infections: diseases from within our doors. Retrieved May 15, 2005 from
http://www.nursingceu.com/NCEU/courses/nosocomial/.
37. Tortorano, A.M., Viviani, M.A., Biraghi, E., Rigoni, A.L., Prigitano, A., Grillot, R., and the EBGA Network
(2005) In vitro testing of fungicidal activity of biocides against Aspergillus fumigatus. Journal of Medical
Microbiology 54, 955-957.
38. Wang, X., Preston, J.F. III and Romeo, T. (2004) The pgaABCD locus of Escherichia coli promotes the
synthesis of a polysaccharide adhesin required for biofilm formation. Journal of Bacteriology 186, 2724–
2734.
39. Wenzel R.P. (2007) Health care-associated infections: Major issues in the early years of the 21st century.
Clinical Infectious Diseases 45 (Suppl 1), S85–S88.





























