Embed Size (px)
Citation preview

Supplement to March 2013
Supported by Alcon and ThromboGenicsJointly Sponsored by The Dulaney Foundation and Retina Today
Current treatment OptiOns
With articles byPravin U. Dugel, MDJay S. Duker, MDCarl D. Regillo, MD
fOr VitreOmaCular aDhesiOn anD maCular hOle
CME ACtivity

2 SupplEMEnt to rEtinA todAy MArCh 2013
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
Statement of needSymptomatic vitreomacular adhesion (VMA) is a condi-
tion in which the vitreous gel adheres in an abnormally strong manner to the retina. VMA can lead to vitreomacu-lar traction (VMT) and subsequent loss or distortion of visual acuity. Anomalous posterior vitreous detachment (PVD) is linked to several retinal disorders including macu-lar pucker, macular hole, age-related macular generation (AMD), macular edema, and retinal tears and detachment.
The incidence of VMA has been reported to be as high as 84% in cases of macular hole; 74% in VMT; and 56% in idiopathic epimacular membrane.1 The incidence of VMA in macular edema appears to depend on the severity of the underlying condition.2,3 In AMD, the rates vary3-12 but have been reported to be as high as 59% in exudative AMD.12
Currently, pars plana vitrectomy (PPV) is used to surgi-cally induce PVD and release the traction on the retina for selected cases. A vitrectomy procedure, however, is not without risk. Complications reported with standard PPV12-15 and more recently with small-gauge PPV16-20 include retinal detachment, retinal tears, endophthalmitis, and postopera-tive cataract formation. Additionally, PPV may result in incomplete separation, and it may potentially leave a nidus for vasoactive and vasoproliferative substances, or it may induce development of fibrovascular membranes. Further, as with any invasive surgical procedure, PPV introduces trauma to the vitreous and surrounding tissues.21,22
Data show that nonsurgical induction of PVD using ocri-plasmin, a vitreolysis agent, can offer the benefits of success-ful PVD while eliminating the risks associated with a surgical procedure. Pharmacologic vitreolysis has the following advantages over PPV: It induces complete separation, cre-ates a more physiologic state of the vitreomacular interface, prevents the development of fibrovascular membranes, is less traumatic to the vitreous, and is potentially prophylac-tic.21,22 Additionally, pharmacologic vitreolysis obviates the costs associated with surgery and allows earlier intervention, whereas surgery is reserved for more advanced cases. In 2 phase 3 studies, a single injection of ocriplasmin was shown to be safe and effective for PVD induction,23,24 providing further evidence that pharmacologic vitreolysis with ocri-plasmin may provide a safe and effective alternative to PPV for inducing PVD.
Retina specialists and other ophthalmologists must master insights on the pathogenesis of VMA, the role that VMA plays in various retinal pathologies, and the benefits of induced PVD vs anomalous PVD. Mastery includes knowl-edge of the clinical implications of VMA and the results of
recent clinical trials on both surgical and pharmacologic PVD induction, an understanding of vitreolysis agents and their differences, and the ability to identify patients who may benefit from PVD induction.
1. Koerner F, Garweg J. [Diseases of the vitreo-macular interface]. Klin Monbl Augenheilkd. 1999;214(5):305-310.2. Takahashi MK, Hikichi T, Akiba J, Yoshida A, Trempe CL. Role of the vitreous and macular edema in branch retinal vein occlu-sion. Ophthalmic Surg Lasers. 1997;28(4):294-299.3. Kado M, Jalkh AE, Yoshida A, et al. Vitreous changes and macular edema in central retinal vein occlusion. Ophthalmic Surg. 1990;21(8):544-549.4. Lambert HM, Capone A, Jr., Aaberg TM, et al. Surgical excision of subfoveal neovascular membranes in age-related macular degeneration. Am J Ophthalmol. 1992;113(3):257-2625. Weber-Krause B, Eckardt U. [Incidence of posterior vitreous detachment in eyes with and without age-related macular degeneration. An ultrasonic study]. Ophthalmologe. 1996;93(6):660-665.6. Ondes F, Yilmaz G, Acar MA, et al. Role of the vitreous in age-related macular degeneration. Jpn J Ophthalmol. 2000;44(1):91-93.7. Krebs I, Brannath W, Glittenberg C, et al. Posterior vitreomacular adhesion: a potential risk factor for exudative age-related macular degeneration? Am J Ophthalmol. 2007;144(5):741-746.8. Lee SJ, Lee CS, Koh HJ. Posterior vitreomacular adhesion and risk of exudative age-related macular degeneration: paired eye study. Am J Ophthalmol. 2009;147(4):621-626. e1.9. Robison CD, Krebs I, Binder S, et al. Vitreomacular adhesion in active and end-stage age-related macular degeneration. Am J Ophthalmol. 2009;148(1):79-82.10. Wheatley HM. Posterior vitreomacular adhesion and exudative age-related macular degeneration. Am J Ophthalmol. 2008;145(4):765; author reply: 766.11. Schmidt JC, Mennel S, Meyer CH, Kroll P. Posterior vitreomacular adhesion: a potential risk factor for exudative age-related macular degeneration. Am J Ophthalmol. 2008;145(6):1107; author reply: 1108.12. Mojana F, Cheng L, Bartsch DU, et al. The role of abnormal vitreomacular adhesion in age-related macular degeneration: spectral optical coherence tomography and surgical results. Am J Ophthalmol. 2008;146(2):218-227.13. Doft BH, Wisniewski SR, Kelsey SF, Groer-Fitzgerald S; Endophthalmitis Vitrectomy Study Group. Diabetes and postcataract extraction endophthalmitis. Curr Opin Ophthalmol. 2002;13(3):147-151.14. Doft BM, Kelsey SF, Wisniewski SR. Retinal detachment in the endophthalmitis vitrectomy study. Arch Ophthalmol. 2000;118(12):1661-1665.15. Wisniewski SR, Capone A, Kelsey SF, et al. Characteristics after cataract extraction or secondary lens implantation among patients screened for the Endophthalmitis Vitrectomy Study. Ophthalmology. 2000;107(7):1274-1282.16. Gupta OP, Weichel ED, Regillo CD, et al. Postoperative complications associated with 25-gauge pars plana vitrectomy. Ophthalmic Surg Lasers Imaging. 2007;38(4):270-275.17. Liu DT, Chan CK, Fan DS, Lam SW, Lam DS, Chan WM. Choroidal folds after 25 gauge transconjunctival sutureless vitrectomy. Eye. 2005;19(7):825-827.18. Scott IU, Flynn HW Jr, Dev S, et al. Endophthalmitis after 25-gauge and 20-gauge pars plana vitrectomy: incidence and outcomes. Retina. 2008;28(1):138-142.19. Kunimoto DY, Kaiser RS; Wills Eye Retina Service. Incidence of endophthalmitis after 20- and 25-gauge vitrectomy. Ophthalmology. 2007;114(12):2133-2137.20. Kaiser RS. Complications of sutureless vitrectomy and the findings of the Micro-Surgical Safety Task Force. Paper presented at: Retina Subspecialty Day, Annual Meeting of the American Academy of Ophthalmology; November 7-8, 2008; Atlanta, GA.21. de Smet MD, Gandorfer A, Stalmans P, et al. Microplasmin intravitreal administration in patients with vitreomacular traction scheduled for vitrectomy: the MIVI I trial. Ophthalmology. 2009;116(7):1349-1355. 22. Goldenberg DT, Trese MT. Pharmacologic vitreodynamics and molecular flux. Dev Ophthalmol. 2009;44:31-36. 23. Jumper J, Pakola S. The MIVI-007 trial. Phase 3 evaluation of single intravitreous injection of microplasmin or placebo for treatment of focal vitreomacular adhesion. Paper presented at: the American Society of Retina Specialists; August 31, 2010; Vancouver, BC.24. Packo K, Pakola S. The MIVI-006 trial. Phase 3 evaluation of single intravitreous injection of microplasmin or placebo for treatment of focal vitreomacular adhesion. Paper presented at: the American Society of Retina Specialists; August 31, 2010; Vancouver, BC.
target audienceThis certified CME activity is designed for retina spe-
cialists and general ophthalmologists involved in the management of patients with retinal disease.
Learning objectiveS – Upon completion of this activity, the participant
should be able to:
Release date: March 2013 Expiration date: March 2014Jointly sponsored by The Dulaney Foundation and Retina TodaySupported by an educational grant from Alcon and ThromboGenics
MArCh 2013 SupplEMEnt to rEtinA todAy 3
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
• Identify the key anatomic elements of the vitreous and the areas of vitreomacular adhesion
• Understand the normal progressive anatomic changes that occur in the vitreous over time
• Differentiate the various vitreous disease states associated with VMA
• Understand the use of OCT imaging in VMA dis-ease states
• Compare normal PVD vs anomalous PVD • Discuss the mechanism of action of pharmacologic
vitreolysis and delivery techniques• Discuss recent safety and efficacy data of pharma-
cologic vitreolysis agents used in VMA treatment Participants should read the CME activity in its entirety.
method of inStructionAfter reviewing the material, please complete the self-
assessment test, which consists of a series of multiple-choice questions. To answer these questions online and receive real-time results, please visit http://www.dulaney-foundation.org and click “Online Courses.” Upon com-pleting the activity and achieving a passing score of over 70% on the self-assessment test, you may print out a CME credit letter awarding 1 AMA PRA Category 1 Credit.™ The estimated time to complete this activity is 1 hour.
accreditation and deSignation This activity has been planned and implemented in
accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint sponsorship of the Dulaney Foundation and Retina Today. The Dulaney Foundation is accredited by the ACCME to provide continuing education for physicians. The Dulaney Foundation des-ignates this enduring material for a maximum of 1 AMA PRA Category 1 Credit.™ Physicians should claim only the credit commensurate with the extent of their participa-tion in the activity.
diScLoSureIn accordance with the disclosure policies of the
Dulaney Foundation and to conform with ACCME and US Food and Drug Administration guidelines, anyone in a position to affect the content of a CME activity is required to disclose to the activity participants (1) the existence of any financial interest or other relationships with the manufacturers of any commercial products/ devices or providers of commercial services and (2)
identification of a commercial product/device that is unlabeled for use or an investigational use of a product/ device not yet approved.
facuLty credentiaLSPravin U. Dugel, MD, is Managing Partner
of Retinal Consultants of Arizona in Phoenix; Clinical Associate Professor of Ophthalmology, Doheny Eye Institute, Keck School of Medicine at the University of Southern California, Los Angeles; and Founding Member of the Spectra Eye Institute in Sun City, AZ. He is a member of the Retina Today Editorial Board. He can be reached via email at [email protected].
Jay S. Duker, MD, is Director of the New England Eye Center and Professor and Chairman of the Department of Ophthalmology, Tufts University School of Medicine in Boston. He is a member of the Retina Today Editorial Board. Dr. Duker may be reached at [email protected].
Carl D. Regillo, MD, is the Director of the Retina Service of Wills Eye Institute and a Professor of Ophthalmology at Thomas Jefferson University in Philadelphia. He is a member of the Retina Today Editorial Board. He may be reached at [email protected].
facuLty/Staff diScLoSure decLarationS
Dr. Dugel states that he is a consultant for Alcon, AMO, ArcticDx, Ora, Regeneron, and ThromboGenics.
Dr. Duker states that he is a stockholder in Hemera Biosciences, Ophthotech, Paloma Pharmaceuticals, and EyeNettra; receives research support from OptoVue and Carl Zeiss Meditec; and is a consultant to EMD/Serono, Neovista, Novartis, Optos, QLT, and ThromboGenics.
Dr. Regillo states that he receives grant research support from Alimera, Allergan, Genentech, Glaxo Smith Kline, Ophthotech, Regeneron, ThromboGenics, Advanced Cell Technology, Johnson and Johnson, QLT, and Alcon. He is a consultant for Alimera, Alcon, Genentech, GlaxoSmithKline, and Regeneron.
All of those involved in the planning, editing, and peer review of this educational activity report no financial relationships.
4 SupplEMEnt to rEtinA todAy MArCh 2013
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
Pathophysiology of the Vitreomacular Interface
“The vitreous is like the appendix, it serves an important purpose in utero. After that it causes nothing but trouble.”
– Jay S. Duker, MD
Almost all vitreomacular interface (VMI) disease and pathology is the result of aging. There are 2 main events that occur with the vitreous as we age. The first is liquefaction, when pockets of
fluid develop within the vitreous cavity. Even autopsy specimens from children as young
as 4 years old show the beginning of the liquefaction of the vitreous, which proceeds slowly through life. Approximately 20% of the vitreous is liquefied by a person’s late teens, and by age 70, approximately 50% is liquefied. Despite this liquefaction, autopsy specimens on normal eyes show almost no posterior vitreous detachment in eyes younger than 60 years of age.
Along with this liquefaction process, there’s a pro-gressive age-related weakening of the adhesion (the molecular glue consisting of collagen, fibronectin, and laminin) between the posterior vitreous cortex, which is also commonly referred to as the posterior hyaloid, and the internal limiting membrane. After the age of 60, this weakness really becomes more evident, and, as the liquefaction increases, this can result in a posterior vitreous separation.
Mark Johnson, MD, who performed seminal research on the progression of posterior vitreous detachment (PVD) said in his paper in the American Journal of
Ophthalmology, “PVD is the most important event in the life of the human vitreous gel.”1
areaS of adheSionThere are 4 areas of the retina to which the vitreous is
most tightly adherent: the vitreous base, along large reti-nal vessels, the optic disc margin, and the macula. It adheres to the macula in 2 locations: along a 500 µm diameter circle, which is known as a foveolar attach-ment, or along a 1500 µm diameter circle, which is known
By Jay S. Duker, MD
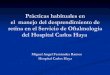
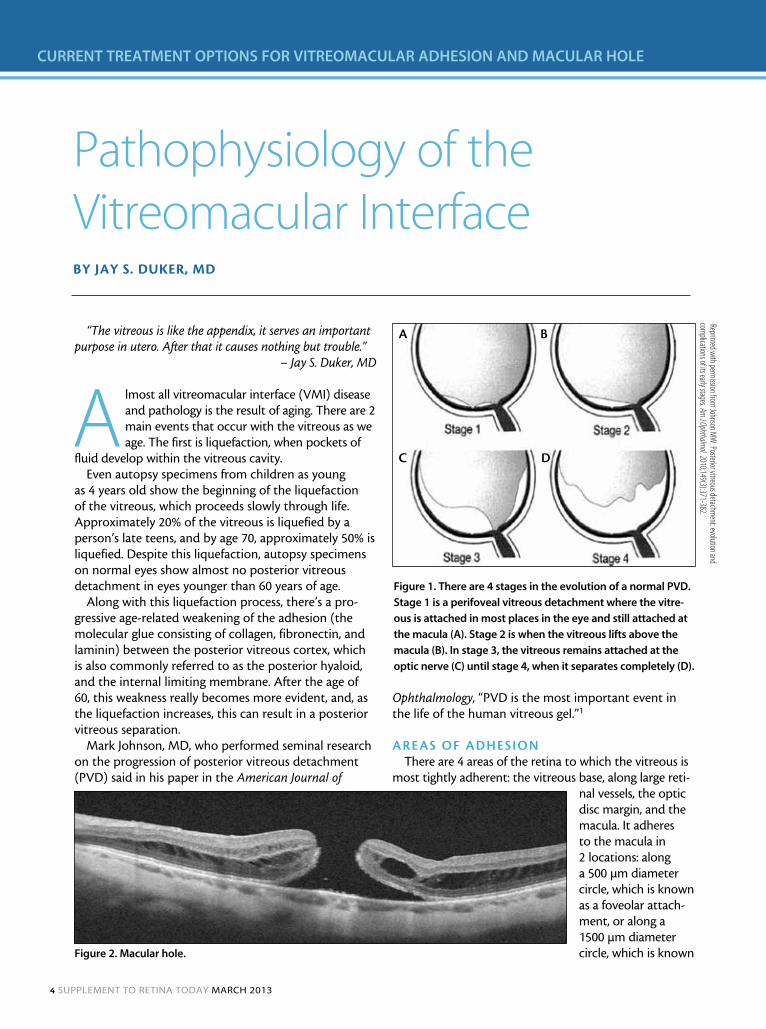
Figure 1. There are 4 stages in the evolution of a normal PVD.
Stage 1 is a perifoveal vitreous detachment where the vitre-
ous is attached in most places in the eye and still attached at
the macula (A). Stage 2 is when the vitreous lifts above the
macula (B). In stage 3, the vitreous remains attached at the
optic nerve (C) until stage 4, when it separates completely (D).
Reprinted with perm
ission from Johnson M
W. Posterior vitreous detachm
ent: evolution and com
plications of its early stages. Am J Ophthalm
ol. 2010;149(3):371-382.
a
c d
b
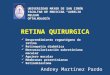
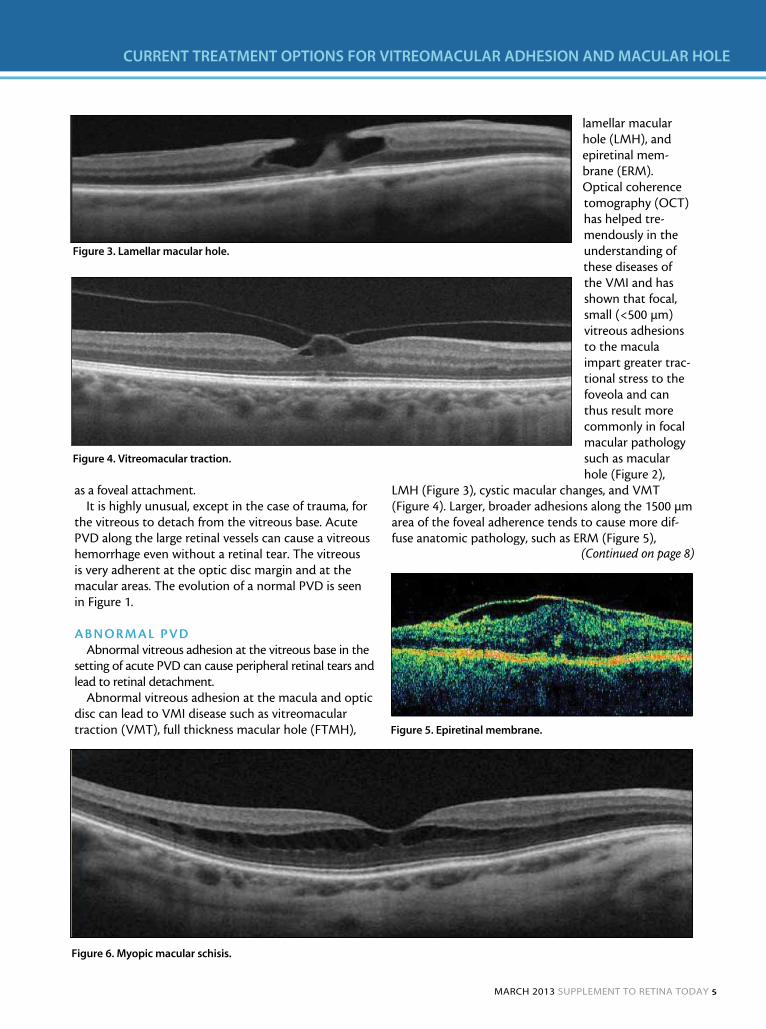
Figure 2. Macular hole.
MArCh 2013 SupplEMEnt to rEtinA todAy 5
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
as a foveal attachment. It is highly unusual, except in the case of trauma, for
the vitreous to detach from the vitreous base. Acute PVD along the large retinal vessels can cause a vitreous hemorrhage even without a retinal tear. The vitreous is very adherent at the optic disc margin and at the macular areas. The evolution of a normal PVD is seen in Figure 1.
abnormaL PvdAbnormal vitreous adhesion at the vitreous base in the
setting of acute PVD can cause peripheral retinal tears and lead to retinal detachment.
Abnormal vitreous adhesion at the macula and optic disc can lead to VMI disease such as vitreomacular traction (VMT), full thickness macular hole (FTMH),
lamellar macular hole (LMH), and epiretinal mem-brane (ERM). Optical coherence tomography (OCT) has helped tre-mendously in the understanding of these diseases of the VMI and has shown that focal, small (<500 µm) vitreous adhesions to the macula impart greater trac-tional stress to the foveola and can thus result more commonly in focal macular pathology such as macular hole (Figure 2),
LMH (Figure 3), cystic macular changes, and VMT (Figure 4). Larger, broader adhesions along the 1500 µm area of the foveal adherence tends to cause more dif-fuse anatomic pathology, such as ERM (Figure 5),
Figure 3. Lamellar macular hole.
Figure 4. Vitreomacular traction.
Figure 5. Epiretinal membrane.
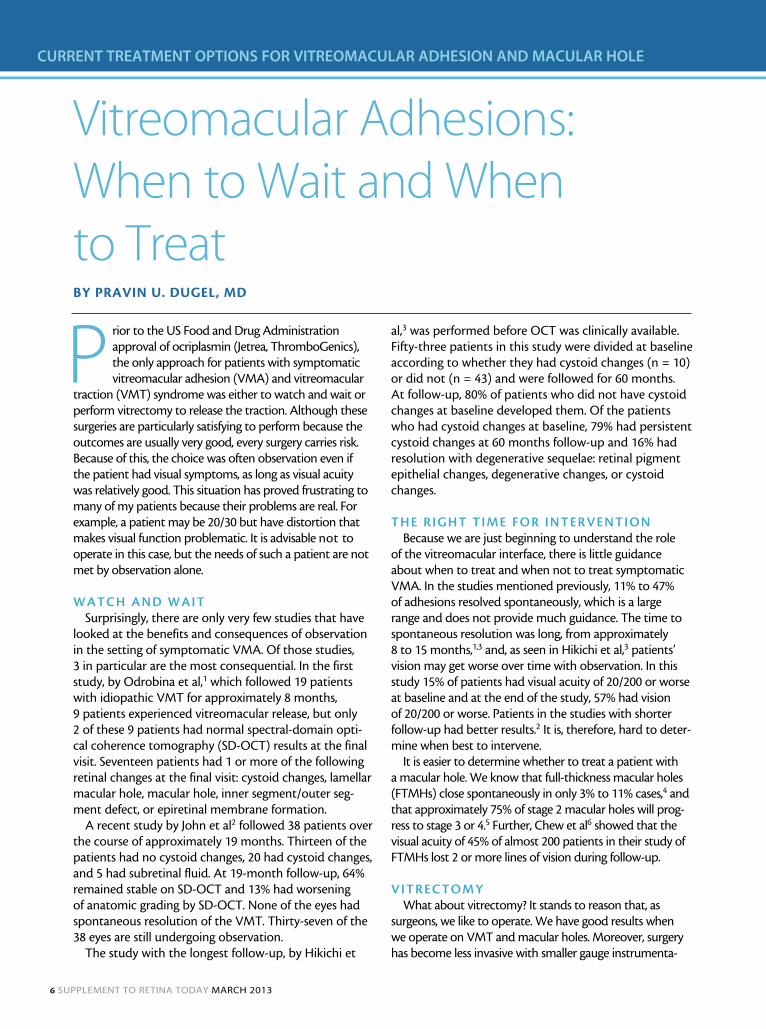
Figure 6. Myopic macular schisis.
(Continued on page 8)
6 SupplEMEnt to rEtinA todAy MArCh 2013
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
Vitreomacular Adhesions: When to Wait and When to TreatBy Pravin u. Dugel, MD
Prior to the US Food and Drug Administration approval of ocriplasmin (Jetrea, ThromboGenics), the only approach for patients with symptomatic vitreomacular adhesion (VMA) and vitreomacular
traction (VMT) syndrome was either to watch and wait or perform vitrectomy to release the traction. Although these surgeries are particularly satisfying to perform because the outcomes are usually very good, every surgery carries risk. Because of this, the choice was often observation even if the patient had visual symptoms, as long as visual acuity was relatively good. This situation has proved frustrating to many of my patients because their problems are real. For example, a patient may be 20/30 but have distortion that makes visual function problematic. It is advisable not to operate in this case, but the needs of such a patient are not met by observation alone.
Watch and WaitSurprisingly, there are only very few studies that have
looked at the benefits and consequences of observation in the setting of symptomatic VMA. Of those studies, 3 in particular are the most consequential. In the first study, by Odrobina et al,1 which followed 19 patients with idiopathic VMT for approximately 8 months, 9 patients experienced vitreomacular release, but only 2 of these 9 patients had normal spectral-domain opti-cal coherence tomography (SD-OCT) results at the final visit. Seventeen patients had 1 or more of the following retinal changes at the final visit: cystoid changes, lamellar macular hole, macular hole, inner segment/outer seg-ment defect, or epiretinal membrane formation.
A recent study by John et al2 followed 38 patients over the course of approximately 19 months. Thirteen of the patients had no cystoid changes, 20 had cystoid changes, and 5 had subretinal fluid. At 19-month follow-up, 64% remained stable on SD-OCT and 13% had worsening of anatomic grading by SD-OCT. None of the eyes had spontaneous resolution of the VMT. Thirty-seven of the 38 eyes are still undergoing observation.
The study with the longest follow-up, by Hikichi et
al,3 was performed before OCT was clinically available. Fifty-three patients in this study were divided at baseline according to whether they had cystoid changes (n = 10) or did not (n = 43) and were followed for 60 months. At follow-up, 80% of patients who did not have cystoid changes at baseline developed them. Of the patients who had cystoid changes at baseline, 79% had persistent cystoid changes at 60 months follow-up and 16% had resolution with degenerative sequelae: retinal pigment epithelial changes, degenerative changes, or cystoid changes.
the right time for interventionBecause we are just beginning to understand the role
of the vitreomacular interface, there is little guidance about when to treat and when not to treat symptomatic VMA. In the studies mentioned previously, 11% to 47% of adhesions resolved spontaneously, which is a large range and does not provide much guidance. The time to spontaneous resolution was long, from approximately 8 to 15 months,1,3 and, as seen in Hikichi et al,3 patients’ vision may get worse over time with observation. In this study 15% of patients had visual acuity of 20/200 or worse at baseline and at the end of the study, 57% had vision of 20/200 or worse. Patients in the studies with shorter follow-up had better results.2 It is, therefore, hard to deter-mine when best to intervene.
It is easier to determine whether to treat a patient with a macular hole. We know that full-thickness macular holes (FTMHs) close spontaneously in only 3% to 11% cases,4 and that approximately 75% of stage 2 macular holes will prog-ress to stage 3 or 4.5 Further, Chew et al6 showed that the visual acuity of 45% of almost 200 patients in their study of FTMHs lost 2 or more lines of vision during follow-up.
vitrectomyWhat about vitrectomy? It stands to reason that, as
surgeons, we like to operate. We have good results when we operate on VMT and macular holes. Moreover, surgery has become less invasive with smaller gauge instrumenta-
MArCh 2013 SupplEMEnt to rEtinA todAy 7
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
vitreomacular adhesion and vitreomacular traction With macular hole By Pravin U. Dugel, MD
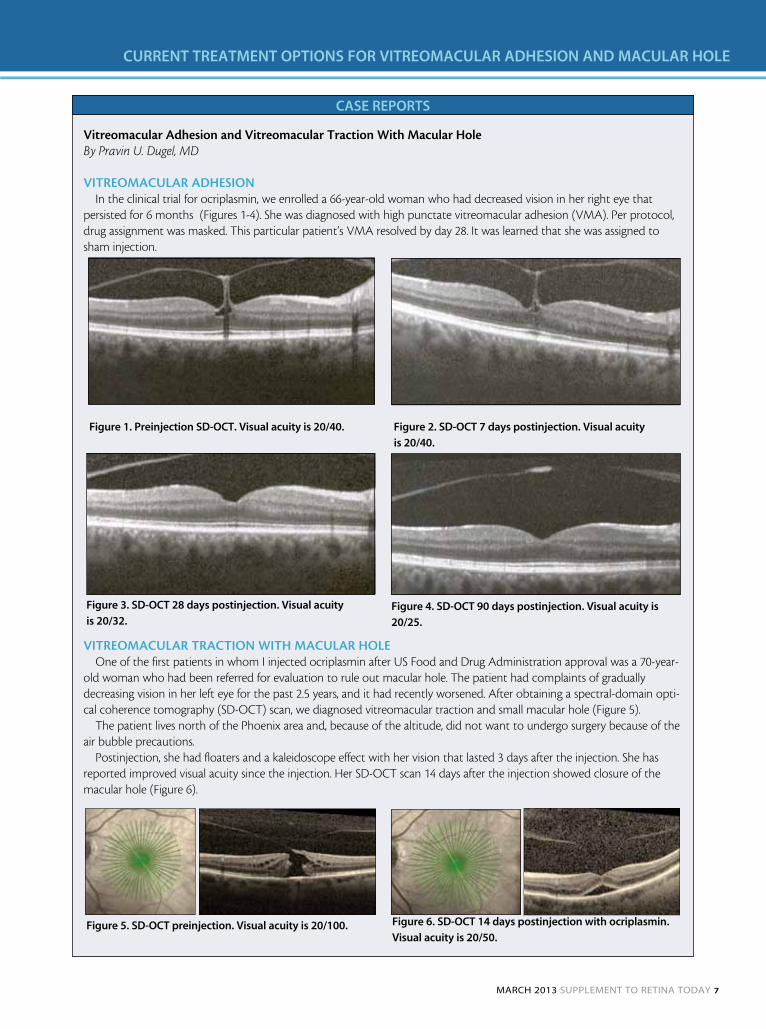
vitreomacuLar adheSionIn the clinical trial for ocriplasmin, we enrolled a 66-year-old woman who had decreased vision in her right eye that
persisted for 6 months (Figures 1-4). She was diagnosed with high punctate vitreomacular adhesion (VMA). Per protocol, drug assignment was masked. This particular patient’s VMA resolved by day 28. It was learned that she was assigned to sham injection.
vitreomacuLar traction With macuLar hoLeOne of the first patients in whom I injected ocriplasmin after US Food and Drug Administration approval was a 70-year-
old woman who had been referred for evaluation to rule out macular hole. The patient had complaints of gradually decreasing vision in her left eye for the past 2.5 years, and it had recently worsened. After obtaining a spectral-domain opti-cal coherence tomography (SD-OCT) scan, we diagnosed vitreomacular traction and small macular hole (Figure 5).
The patient lives north of the Phoenix area and, because of the altitude, did not want to undergo surgery because of the air bubble precautions.
Postinjection, she had floaters and a kaleidoscope effect with her vision that lasted 3 days after the injection. She has reported improved visual acuity since the injection. Her SD-OCT scan 14 days after the injection showed closure of the macular hole (Figure 6).
CASE REPoRTS
Figure 1. Preinjection SD-oCT. Visual acuity is 20/40. Figure 2. SD-oCT 7 days postinjection. Visual acuity
is 20/40.
Figure 3. SD-oCT 28 days postinjection. Visual acuity
is 20/32.Figure 4. SD-oCT 90 days postinjection. Visual acuity is
20/25.
Figure 5. SD-oCT preinjection. Visual acuity is 20/100. Figure 6. SD-oCT 14 days postinjection with ocriplasmin.
Visual acuity is 20/50.

8 SupplEMEnt to rEtinA todAy MArCh 2013
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
tion. Several studies have shown that surgery for VMT and macular hole is generally very effective and safe.7-11
However, surgery is not without risk. Risks with any vitrectomy procedure include retinal tears, detachments, endophthalmitis, and cataract formation in phakic patients. Additionally, patients who undergo surgery lose time from work and are inconvenienced by facedown positioning and restrictions on air travel because of a gas bubble.
deciSion-making in macuLar hoLe and vma/vmt
Now that we have ocriplasmin available, we have to decide whether to intervene surgically or pharmacologi-cally. The key to success with ocriplasmin lies in proper patient selection. Although ocriplasmin may have a wide application as a combination agent in chronic retinal diseases such as diabetic macular edema, retinal vein occlusion, and age-related macular degeneration, it is important to confine the use of this drug to only the 2 patient groups shown in the MIVI TRUST trials to have the greatest success: patients with VMA and a macular hole of 400 µm or less and patients with VMA and vitreo-macular adhesion of 1500 µm or less. If such patients are properly selected, the success rate with a single injection of ocriplasmin should be approximately 50%.
Pravin U. Dugel, MD, is Managing Partner of Retinal Consultants of Arizona in Phoenix; Clinical Associate Professor of Ophthalmology, Doheny Eye Institute, Keck School of Medicine at the University of Southern California, Los Angeles; and Founding Member of the Spectra Eye Institute in Sun City, AZ. He is a member of the Retina Today Editorial Board. Dr. Dugel states that he is a consultant for Alcon, AMO, ArcticDx, Ora, Regeneron, and ThromboGenics. He can be reached at [email protected].
1. Odrobina D, Michalewska Z, Michalewski J, Dzigielewski K, Nawrocki J. Long-term evaluation of vitreomacular traction disorder in spectral-domain optical coherence tomography. Retina. 2011;31(2):324-331.2. John VJ, Smiddy W, Flynn H. Natural clinical course of unoperated eyes with vitreomacular traction syndrome. Paper presented at: the Association for Research in Vision and Ophthalmology Annual Meeting. May 9, 2012; Fort Lauderdale, FL.3. Hikichi T, Yoshida A, Trempe CL. Course of vitreomacular traction syndrome. Am J Ophthalmol. 1995;119(1):55-61.4. American Academy of Ophthalmology Retina Panel. Preferred Practice Pattern® Guidelines. Idiopathic Macular Hole. San Francisco, CA: American Academy of Ophthalmology; 2008. http://www.aao.org/ppp.5. Kim JW, Freeman WR, Azen SP, el-Haig W, Klein DJ, Bailey IL. Prospective randomized trial of vitrectomy or observa-tion for stage 2 macular holes. Vitrectomy for Macular Hole Study Group. Am J Ophthalmol. 1996;121(6):605-614.6. Chew EY, Sperduto RD, Hiller R, et al. Clinical course of macular holes: the Eye Disease Case-Control Study. Arch Ophthalmol. 1999;117(2):242-246.7. Witkin AJ, Patron ME, Castro LC, et al. Anatomic and visual outcomes of vitrectomy for vitreomacular traction syndrome. Ophthalmic Surg Lasers Imaging. 2010 41(4):425-431.8. Larsson J. Vitrectomy in vitreomacular traction syndrome evaluated by ocular coherence tomography (OCT) retinal mapping. Acta Ophthalmol Scand. 2004;82(6):691-694.9. Rouhette H, Gastaud P. [Idiopathic vitreomacular traction syndrome. Vitrectomy results]. [Article in French] J Fr Ophtalmol. 2001;24(5):496-504.10. Ezra E, Gregor ZJ; Moorfields Macular Hole Study Ggroup Report No. 1. Surgery for idiopathic full-thickness macular hole: two-year results of a randomized clinical trial comparing natural history, vitrectomy, and vitrectomy plus autolo-gous serum: Moorfields Macular Hole Study Group. Report no. 1. Arch Ophthalmol. 2004;122(2):224-236.11. Mester V, Kuhn F. Internal limiting membrane removal in the management of full-thickness macular holes. Macula Surgery Web site. Available at: http://www.maculasurgery.com/MacularHole.htm.
traction macular detachments, and myopic macular schisis (Figure 6) In patients with diabetes, macular edema may occur as a result of hyaloidal thickening.
It is important to note that vitreomacular adhesion (VMA; Figure 7), in and of itself, is not a pathologic state. In fact, it resembles stage 1 PVD, shown in Figure 1. When a patient’s OCT looks like the image in Figure 7, the chances of a normal evolution of PVD are very good. VMT occurs, however, when focal retinal anatomic changes appear. At that point, the VMA may become symptomatic. It is in this setting that VMA can progress to retinal pathology, as seen in Figures 2 to 6.
SummaryVMA has been implicated as an initiating anatomic
configuration in a number of disease states including VMT, FTMH, LMH, and ERM. A better understanding of the identifying factors that might predict which eyes with VMA are prone to developing a disease of the VMI as apposed to merely progressing through the nonpathologic sequence of PVD will hopefully allow improved treatment of these con-ditions and better results for our patients.
Jay S. Duker, MD, is Director of the New England Eye Center and Professor and Chairman of the Department of Ophthalmology, Tufts University School of Medicine in Boston. He is a member of the Retina Today Editorial Board. He states that he is a stockholder in Hemera Biosciences, Ophthotech, Paloma Pharmaceuticals, and EyeNettra; receives research support from OptoVue and Carl Zeiss Meditec; and is a consultant to EMD/Serono, Neovista, Novartis, Optos, QLT, and ThromboGenics. Dr. Duker may be reached at [email protected].
1. Johnson MW. Posterior vitreous detachment: evolution and complications of its early stages. Am J Ophthalmol. 2010;149(3):371-382.
Figure 7. Vitreomacular adhesion.
VMA has been implicated as an initiating anatomic configuration in a number of
different disease states including VMT, FTMH, LMH, and ERM.
(Continued from page 5)
MArCh 2013 SupplEMEnt to rEtinA todAy 9
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
Ocriplasmin for the Treatment of Symptomatic Vitreomacular AdhesionBy Carl D. regillo, MD
Ocriplasmin (Jetrea, ThromboGenics) is a trun-cated form of human plasmin, made with recombinant DNA technology that targets fibronectin, laminin and collagen, among
other molecules. Ocriplasmin enhances vitreous lique-faction and promotes clean separation of the vitreous cortex from the internal limiting membrane.1
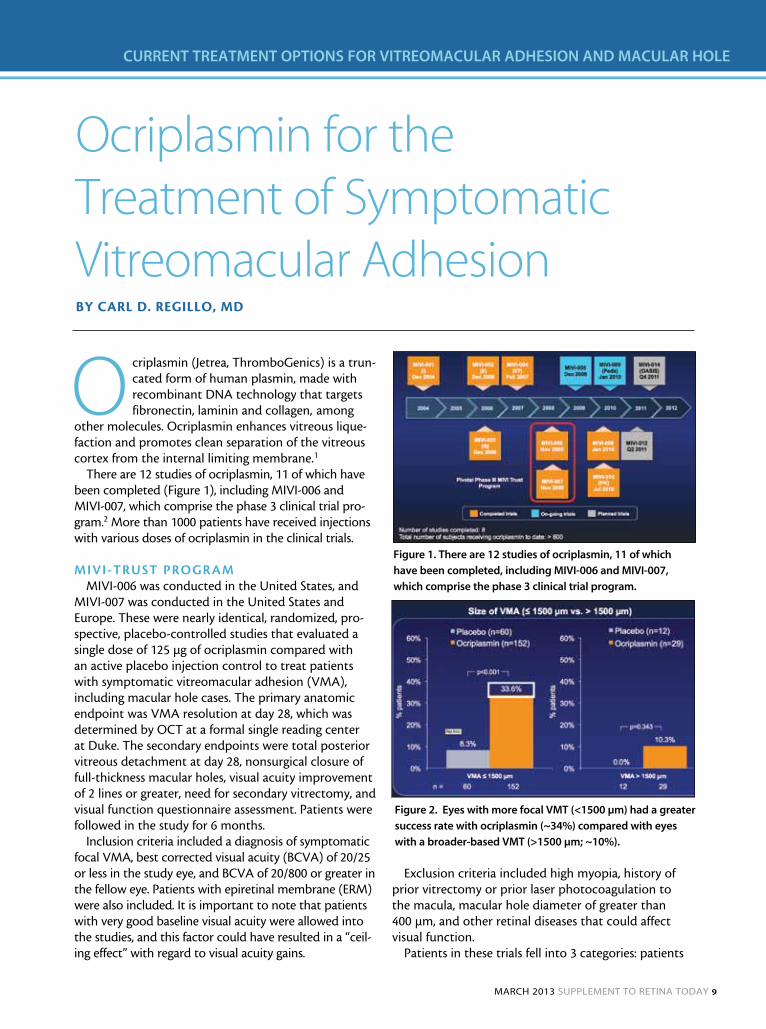
There are 12 studies of ocriplasmin, 11 of which have been completed (Figure 1), including MIVI-006 and MIVI-007, which comprise the phase 3 clinical trial pro-gram.2 More than 1000 patients have received injections with various doses of ocriplasmin in the clinical trials.
mivi-truSt Program MIVI-006 was conducted in the United States, and
MIVI-007 was conducted in the United States and Europe. These were nearly identical, randomized, pro-spective, placebo-controlled studies that evaluated a single dose of 125 µg of ocriplasmin compared with an active placebo injection control to treat patients with symptomatic vitreomacular adhesion (VMA), including macular hole cases. The primary anatomic endpoint was VMA resolution at day 28, which was determined by OCT at a formal single reading center at Duke. The secondary endpoints were total posterior vitreous detachment at day 28, nonsurgical closure of full-thickness macular holes, visual acuity improvement of 2 lines or greater, need for secondary vitrectomy, and visual function questionnaire assessment. Patients were followed in the study for 6 months.
Inclusion criteria included a diagnosis of symptomatic focal VMA, best corrected visual acuity (BCVA) of 20/25 or less in the study eye, and BCVA of 20/800 or greater in the fellow eye. Patients with epiretinal membrane (ERM) were also included. It is important to note that patients with very good baseline visual acuity were allowed into the studies, and this factor could have resulted in a “ceil-ing effect” with regard to visual acuity gains.
Exclusion criteria included high myopia, history of prior vitrectomy or prior laser photocoagulation to the macula, macular hole diameter of greater than 400 µm, and other retinal diseases that could affect visual function.
Patients in these trials fell into 3 categories: patients
Figure 1. There are 12 studies of ocriplasmin, 11 of which
have been completed, including MIVI-006 and MIVI-007,
which comprise the phase 3 clinical trial program.
Figure 2. Eyes with more focal VMT (<1500 µm) had a greater
success rate with ocriplasmin (~34%) compared with eyes
with a broader-based VMT (>1500 µm; ~10%).
10 SupplEMEnt to rEtinA todAy MArCh 2013
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
with vitreomacular traction (VMT) with no baseline macular hole and no baseline ERM, patients with macu-lar hole with or without ERM, and patients with ERM at baseline (ERM was not being treated; rather, VMA associated with ERM). All patients had VMA confirmed by optical coherence tomography (OCT).
reSuLtS: efficacyWith regard to the primary endpoint in the pooled
data from both phase 3 trials, 26.5% patients in the ocriplas-min group had VMA resolution at day 28 compared with 10.1% of patients in the placebo group.
VMT. In the pure VMT subgroup (no ERM or macular hole), there was a success rate of approximately 30% in the ocriplasmin arm compared with 7.7% in the placebo arm, a statistically significant difference. Eyes with more focal VMT (<1500 µm) had a greater success rate with ocriplasmin (~34%) compared with eyes with a broader-based VMT (>1500 µm; ~10%; Figure 2).
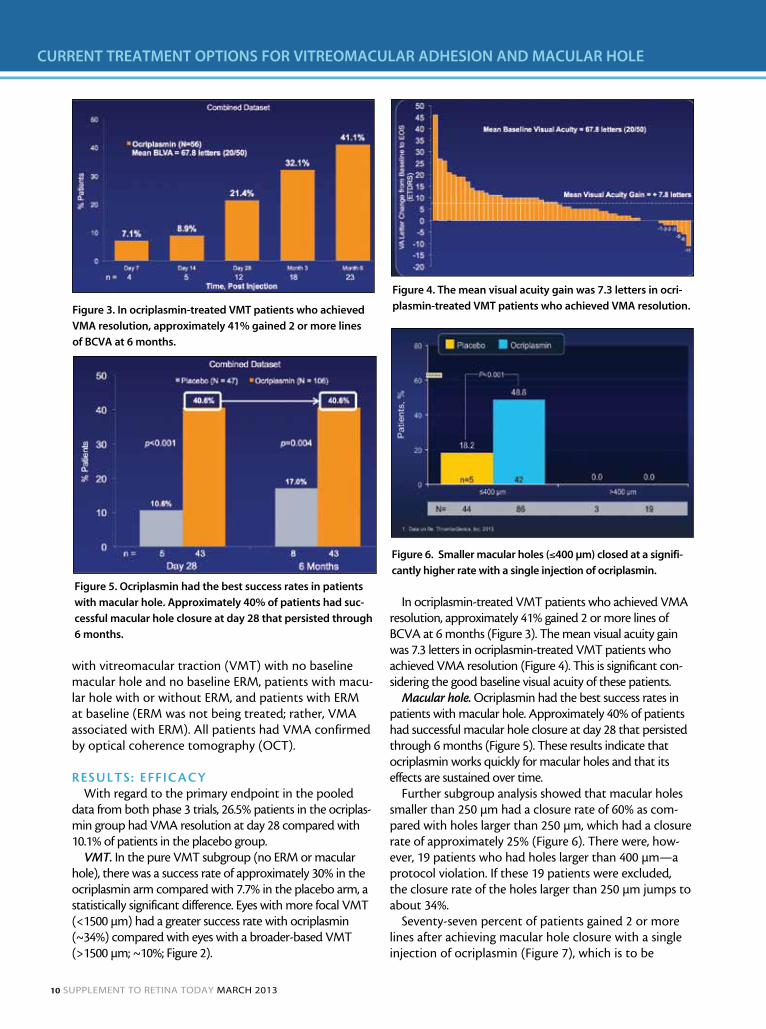
In ocriplasmin-treated VMT patients who achieved VMA resolution, approximately 41% gained 2 or more lines of BCVA at 6 months (Figure 3). The mean visual acuity gain was 7.3 letters in ocriplasmin-treated VMT patients who achieved VMA resolution (Figure 4). This is significant con-sidering the good baseline visual acuity of these patients.
Macular hole. Ocriplasmin had the best success rates in patients with macular hole. Approximately 40% of patients had successful macular hole closure at day 28 that persisted through 6 months (Figure 5). These results indicate that ocriplasmin works quickly for macular holes and that its effects are sustained over time.
Further subgroup analysis showed that macular holes smaller than 250 µm had a closure rate of 60% as com-pared with holes larger than 250 µm, which had a closure rate of approximately 25% (Figure 6). There were, how-ever, 19 patients who had holes larger than 400 µm—a protocol violation. If these 19 patients were excluded, the closure rate of the holes larger than 250 µm jumps to about 34%.
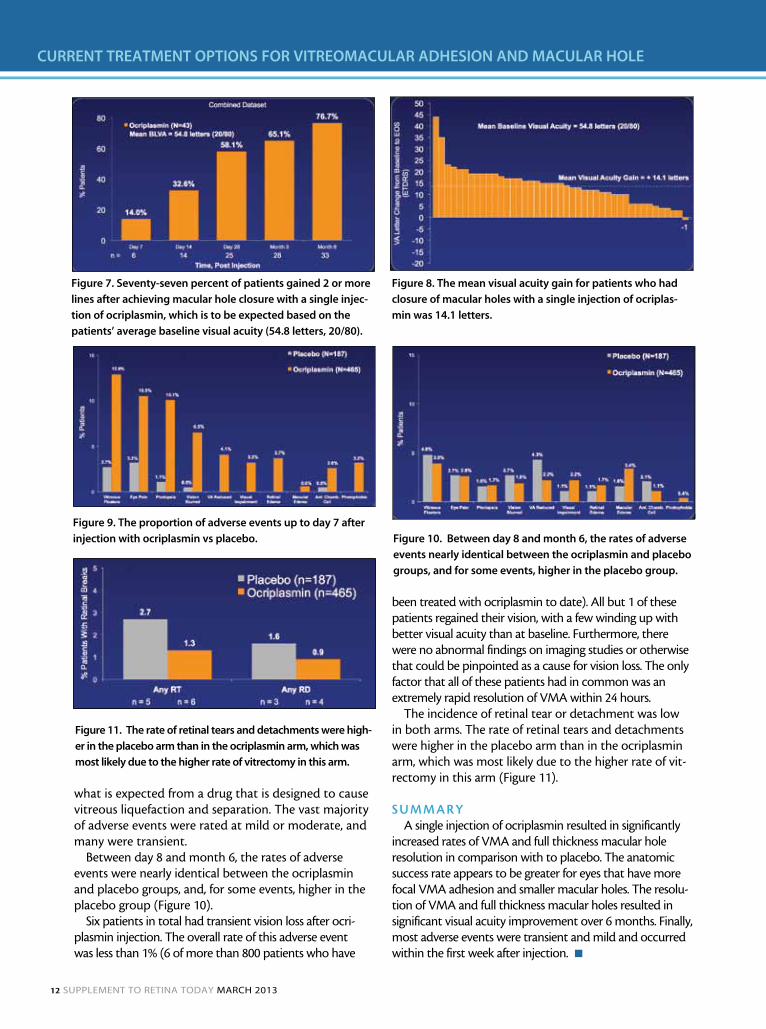
Seventy-seven percent of patients gained 2 or more lines after achieving macular hole closure with a single injection of ocriplasmin (Figure 7), which is to be
Figure 3. In ocriplasmin-treated VMT patients who achieved
VMA resolution, approximately 41% gained 2 or more lines
of BCVA at 6 months.
Figure 4. The mean visual acuity gain was 7.3 letters in ocri-
plasmin-treated VMT patients who achieved VMA resolution.
Figure 5. ocriplasmin had the best success rates in patients
with macular hole. Approximately 40% of patients had suc-
cessful macular hole closure at day 28 that persisted through
6 months.
Figure 6. Smaller macular holes (≤400 µm) closed at a signifi-
cantly higher rate with a single injection of ocriplasmin.
MArCh 2013 SupplEMEnt to rEtinA todAy 11
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
expected based on the patients’ average baseline visual acuity (54.8 letters, 20/80). The mean visual acuity gain for patients who had closure of macular holes with a single injection of ocriplasmin was 14.1 letters (Figure 8). One patient in the macular hole subgroup lost 1 let-ter of vision. The macular hole (387 µm) closed by day 7 and the patient also had pterygium, cortical cataract, cupping of optic disc, retinal pigment epithelial chang-es, vascular narrowing, and macular edema in the study eye at diagnosis.
ERM. In the clinical trials, ocriplasmin did not work well for patients with ERM. In patients who had some degree of ERM evident on OCT, the success rate overall was only about 8% to 9% compared with 1.5% in the placebo group.
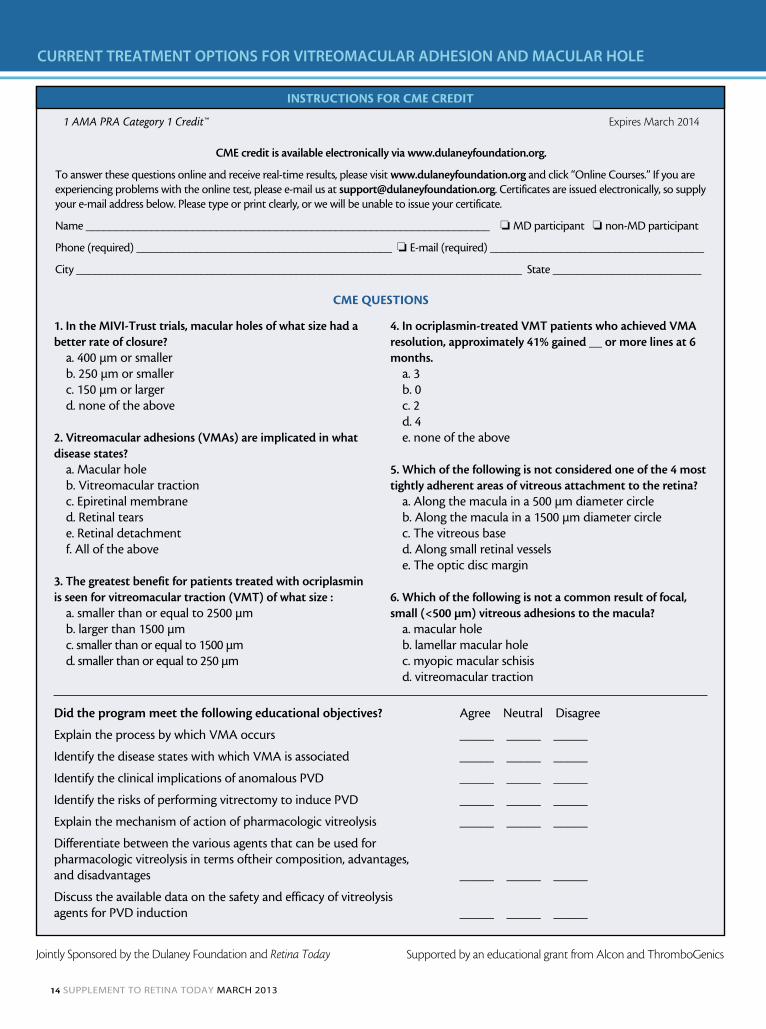
reSuLtS: SafetyFigure 9 shows the proportion of adverse events
up to day 7 after injection with ocriplasmin vs pla-cebo. There was a higher rate of adverse events in the ocriplasmin-treated eyes in all categories, but this is
vitreomacular tractionBy Carl D. Regillo, MD
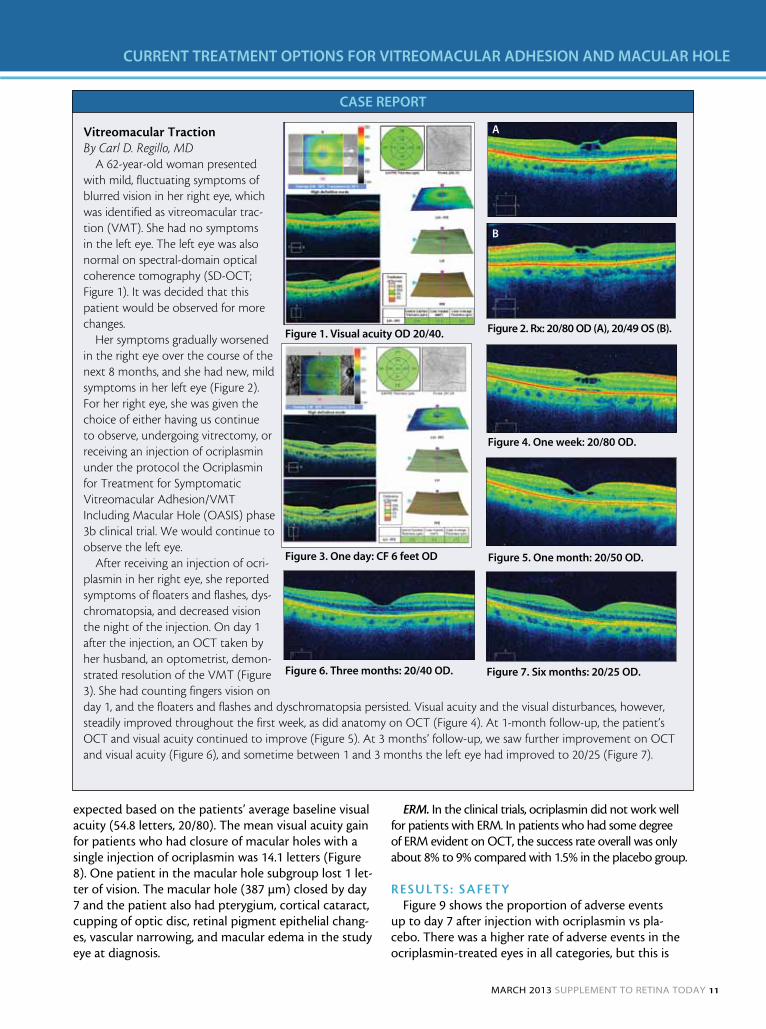
A 62-year-old woman presented with mild, fluctuating symptoms of blurred vision in her right eye, which was identified as vitreomacular trac-tion (VMT). She had no symptoms in the left eye. The left eye was also normal on spectral-domain optical coherence tomography (SD-OCT; Figure 1). It was decided that this patient would be observed for more changes.
Her symptoms gradually worsened in the right eye over the course of the next 8 months, and she had new, mild symptoms in her left eye (Figure 2). For her right eye, she was given the choice of either having us continue to observe, undergoing vitrectomy, or receiving an injection of ocriplasmin under the protocol the Ocriplasmin for Treatment for Symptomatic Vitreomacular Adhesion/VMT Including Macular Hole (OASIS) phase 3b clinical trial. We would continue to observe the left eye.
After receiving an injection of ocri-plasmin in her right eye, she reported symptoms of floaters and flashes, dys-chromatopsia, and decreased vision the night of the injection. On day 1 after the injection, an OCT taken by her husband, an optometrist, demon-strated resolution of the VMT (Figure 3). She had counting fingers vision on day 1, and the floaters and flashes and dyschromatopsia persisted. Visual acuity and the visual disturbances, however, steadily improved throughout the first week, as did anatomy on OCT (Figure 4). At 1-month follow-up, the patient’s OCT and visual acuity continued to improve (Figure 5). At 3 months’ follow-up, we saw further improvement on OCT and visual acuity (Figure 6), and sometime between 1 and 3 months the left eye had improved to 20/25 (Figure 7).
CASE REPoRT
Figure 1. Visual acuity oD 20/40. Figure 2. Rx: 20/80 oD (A), 20/49 oS (B).
Figure 4. one week: 20/80 oD.
Figure 5. one month: 20/50 oD.
Figure 6. Three months: 20/40 oD. Figure 7. Six months: 20/25 oD.
A
B
Figure 3. one day: CF 6 feet oD
12 SupplEMEnt to rEtinA todAy MArCh 2013
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
what is expected from a drug that is designed to cause vitreous liquefaction and separation. The vast majority of adverse events were rated at mild or moderate, and many were transient.
Between day 8 and month 6, the rates of adverse events were nearly identical between the ocriplasmin and placebo groups, and, for some events, higher in the placebo group (Figure 10).
Six patients in total had transient vision loss after ocri-plasmin injection. The overall rate of this adverse event was less than 1% (6 of more than 800 patients who have
been treated with ocriplasmin to date). All but 1 of these patients regained their vision, with a few winding up with better visual acuity than at baseline. Furthermore, there were no abnormal findings on imaging studies or otherwise that could be pinpointed as a cause for vision loss. The only factor that all of these patients had in common was an extremely rapid resolution of VMA within 24 hours.
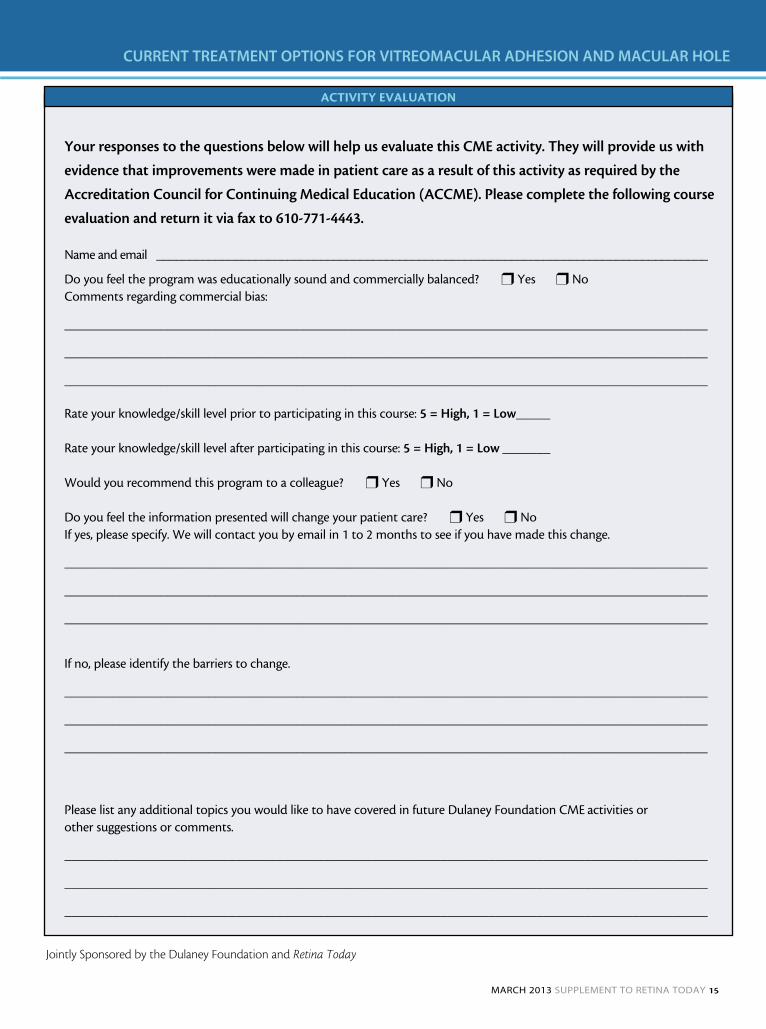
The incidence of retinal tear or detachment was low in both arms. The rate of retinal tears and detachments were higher in the placebo arm than in the ocriplasmin arm, which was most likely due to the higher rate of vit-rectomy in this arm (Figure 11).
SummaryA single injection of ocriplasmin resulted in significantly
increased rates of VMA and full thickness macular hole resolution in comparison with to placebo. The anatomic success rate appears to be greater for eyes that have more focal VMA adhesion and smaller macular holes. The resolu-tion of VMA and full thickness macular holes resulted in significant visual acuity improvement over 6 months. Finally, most adverse events were transient and mild and occurred within the first week after injection. n
Figure 7. Seventy-seven percent of patients gained 2 or more
lines after achieving macular hole closure with a single injec-
tion of ocriplasmin, which is to be expected based on the
patients’ average baseline visual acuity (54.8 letters, 20/80).
Figure 8. The mean visual acuity gain for patients who had
closure of macular holes with a single injection of ocriplas-
min was 14.1 letters.
Figure 9. The proportion of adverse events up to day 7 after
injection with ocriplasmin vs placebo. Figure 10. Between day 8 and month 6, the rates of adverse
events nearly identical between the ocriplasmin and placebo
groups, and for some events, higher in the placebo group.
Figure 11. The rate of retinal tears and detachments were high-
er in the placebo arm than in the ocriplasmin arm, which was
most likely due to the higher rate of vitrectomy in this arm.

MArCh 2013 SupplEMEnt to rEtinA todAy 13
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
dr. duker: Dr. Regillo, you have a lot of experience injecting ocriplasmin in the clinical trials and are well versed in the data. For whom do you think this drug is best suited?
dr. regillo: The data suggest that ocriplasmin works best in patients with focal, symptomatic, and progressive vitreomacular adhesion (VMA) and for patients with acute, small, full-thickness macular holes.
dr. duker: If you had a patient who presents with highly symptomatic vitreomacular traction (VMT) and 20/30 vision on the first visit, would you treat him or her, or would you wait?
dr. regillo: Perhaps.
dr. duker: How can I get you to go from, “perhaps” to, “Yes, I would definitely treat this patient”? What is your cut-off point from watch and wait?
dr. regillo: Let’s say the patient is 20/60 and symptom-atic and he or she says that the visual distortion began 3 months ago and is progressively getting worse. I would treat this patient with ocriplasmin.
dr. duker: What if a patient has been referred for an abnormal optical coherence tomography (OCT) scan that shows VMT, the patient has 20/25 vision and some distor-tion?
dr. regillo: I would be less inclined to treat this patient. Dr. Dugel’s article addressed the broad spectrum of sponta-neous resolution—11% to 40% in VMT—and I think that much of this variation is related to severity. When the VMT is mild, I think that there is a greater likelihood of spontane-
ous resolution. The studies with the longest follow-up for ocriplasmin, however, did not use OCT. Even so, I would make a prediction that the more severe the VMT, the less likely there will be spontaneous separation of the vitreous.
dr. duker: Do you think you or anyone can pick a priori patients who have VMA that will not progress to spontane-ous and clean separation?
dr. regillo: No. When a patient presents with early and mild VMA, it is not possible to predict its course.
dr. duker: What is your threshold for injecting a patient with a macular hole?
dr. regillo: Based on the data from the clinical trials, I will use ocriplasmin for full thickness macular holes that are 400 µm or less in size.
dr. duker: Will you watch these smaller holes initially?
dr. regillo: No. I will treat. The likelihood that macular holes will close spontaneously is low and the larger the hole is (up to 400 µm), the less likely spontaneous closure will occur.
dr. duker: For a retina specialist who is used to perform-ing intravitreal injections, is there anything unique about this drug that he or she should know about, or is this like any other injection that we do?
dr. regillo: Ocriplasmin is not a stable drug. It is shipped and stored frozen. When it is ready to be administered, it should be taken out of the freezer, defrosted, diluted, and then injected promptly. (See package insert for details.)
Q&A
Carl D. Regillo, MD, is the Director of the Retina Service of Wills Eye Institute and a Professor of Ophthalmology at Thomas Jefferson University in Philadelphia. He is a member of the Retina Today Editorial Board. Dr. Regillo states that he receives grant research support from Alimera, Allergan, Genentech, Glaxo Smith Kline, Ophthotech, Regeneron, ThromboGenics, Advanced Cell Technology,
Johnson & Johnson, QLT, and Alcon. He is a consultant for Alimera, Alcon, Genentech, GlaxoSmithKline, and Regeneron. He may be reached at [email protected].
1. Gandorfer A, Rohleder M, Sethi C, et al. Posterior vitreous detachment induced by microplasmin. Invest Ophthal-mol Vis Sci. 2004;45(2):641-647.2. Stalmans P, Benz MS, Gandorfer A, et al; MIVI-TRUST Study Group. Enzymatic vitreolysis with ocriplasmin for vitreomacular traction and macular holes. N Engl J Med. 2012;367(7):606-615.
14 SupplEMEnt to rEtinA todAy MArCh 2013
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
InstructIons for cME crEdIt
1. In the MIVI-Trust trials, macular holes of what size had a better rate of closure?
a. 400 µm or smallerb. 250 µm or smallerc. 150 µm or largerd. none of the above
2. Vitreomacular adhesions (VMAs) are implicated in what disease states?
a. Macular holeb. Vitreomacular tractionc. Epiretinal membraned. Retinal tearse. Retinal detachmentf. All of the above
3. The greatest benefit for patients treated with ocriplasmin is seen for vitreomacular traction (VMT) of what size :
a. smaller than or equal to 2500 µmb. larger than 1500 µmc. smaller than or equal to 1500 µmd. smaller than or equal to 250 µm
4. In ocriplasmin-treated VMT patients who achieved VMA resolution, approximately 41% gained __ or more lines at 6 months.
a. 3b. 0c. 2d. 4e. none of the above
5. Which of the following is not considered one of the 4 most tightly adherent areas of vitreous attachment to the retina?
a. Along the macula in a 500 µm diameter circleb. Along the macula in a 1500 µm diameter circlec. The vitreous based. Along small retinal vesselse. The optic disc margin
6. Which of the following is not a common result of focal, small (<500 μm) vitreous adhesions to the macula?
a. macular holeb. lamellar macular holec. myopic macular schisisd. vitreomacular traction
CME credit is available electronically via www.dulaneyfoundation.org.
To answer these questions online and receive real-time results, please visit www.dulaneyfoundation.org and click “Online Courses.” If you are experiencing problems with the online test, please e-mail us at [email protected]. Certificates are issued electronically, so supply your e-mail address below. Please type or print clearly, or we will be unable to issue your certificate.
Name ____________________________________________________________________ o MD participant o non-MD participant
Phone (required) ___________________________________________ o E-mail (required) ____________________________________
City ___________________________________________________________________________ State _________________________
1 AMA PRA Category 1 Credit™ Expires March 2014
Supported by an educational grant from Alcon and ThromboGenicsJointly Sponsored by the Dulaney Foundation and Retina Today
cME QuEstIons
did the program meet the following educational objectives? Agree Neutral Disagree
Explain the process by which VMA occurs _____ _____ _____
Identify the disease states with which VMA is associated _____ _____ _____
Identify the clinical implications of anomalous PVD _____ _____ _____
Identify the risks of performing vitrectomy to induce PVD _____ _____ _____
Explain the mechanism of action of pharmacologic vitreolysis _____ _____ _____
Differentiate between the various agents that can be used for pharmacologic vitreolysis in terms oftheir composition, advantages, and disadvantages _____ _____ _____
Discuss the available data on the safety and efficacy of vitreolysis agents for PVD induction _____ _____ _____
MArCh 2013 SupplEMEnt to rEtinA todAy 15
Current treatment OptiOns fOr VitreOmaCular adhesiOn and maCular hOle
Jointly Sponsored by the Dulaney Foundation and Retina Today
ActIvIty EvALuAtIon
Your responses to the questions below will help us evaluate this CME activity. They will provide us with
evidence that improvements were made in patient care as a result of this activity as required by the
Accreditation Council for Continuing Medical Education (ACCME). Please complete the following course
evaluation and return it via fax to 610-771-4443.
Name and email ____________________________________________________________________________________
Do you feel the program was educationally sound and commercially balanced? r Yes r NoComments regarding commercial bias:
______________________________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
Rate your knowledge/skill level prior to participating in this course: 5 = high, 1 = Low _____
Rate your knowledge/skill level after participating in this course: 5 = high, 1 = Low _______
Would you recommend this program to a colleague? r Yes r No
Do you feel the information presented will change your patient care? r Yes r NoIf yes, please specify. We will contact you by email in 1 to 2 months to see if you have made this change.
______________________________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
If no, please identify the barriers to change.
______________________________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
Please list any additional topics you would like to have covered in future Dulaney Foundation CME activities or other suggestions or comments.
______________________________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________