-
IUD POSTPLACENTAIUDPOSTPLACENTA
Biran AffandiBiran Affandi
Kli ik R d S l hKlinik Raden
SalehDepartmentofObstetrics&Gynecology
F lt f M di i U i it f I d i
/FacultyofMedicine,UniversityofIndonesia/Cipto Mangunkusumo
GeneralHospital
kJakarta
Affandi B.IUDPostplacenta .Rapat Persiapan TOT
IUDPascapersalinan .BKKBNPusat ,Jakarta,28Desember 2010
-
Objectives:Objectives:1 T d t t
t1.Toupdatepostpartumcontraceptioncontraception
2 To review IUD2.ToreviewIUDPOSTPLACENTAPOSTPLACENTA
3.To discuss medical barriers3.TodiscussmedicalbarriersAffandi
B.IUDPostplacenta .Rapat Persiapan TOT IUDPascapersalinan
.BKKBNPusat ,Jakarta,28Desember 2010
-
MillenniumDevelopmentGoals1 E di d
h1.Eradicateextremepovertyandhunger2.Achieveuniversalprimaryeducation3.Promotegenderequality&empowerwomen4.Reducechildmortality5.Improvematernalhealth6.CombatHIV/AIDS,malaria&otherdiseases7.Ensureenvironmentalsustainability8.Develop
a global partnership for
development8.Developaglobalpartnershipfordevelopment
MDGs challenges are not newMDGs challenges are not new; what is
new is that they involve; what is new is that they involveMDGs
challenges are not newMDGs challenges are not new; what is new is
that they involve ; what is new is that they involve concrete,
timeconcrete, time--bound & quantitative bound &
quantitative targetstargets for action by 2015.for action by
2015.Affandi B.Kesehatan Reproduksi dan Upaya Kesehatan Maternaldi
Indonesia,QuoVadis?Orasi pada PITXVIIIPOGI,Jakarta,7Juli 2010
-
GOAL5ImproveMaternalHealth
TARGET6
Reducebythreequarters,between1990and
2015,thematernalmortalityratio
Affandi B.Kesehatan Reproduksi dan Upaya Kesehatan Maternaldi
Indonesia,QuoVadis?Orasi pada PITXVIIIPOGI,Jakarta,7Juli 2010
-
Maternalmortalityisanindicatorofgrossinequality,human rights
abuse andhumanrightsabuseanddevelopmentfailure.
Allmaternalhealthproblems
bl l harepreventableaslongasthegovernment pays attention
andgovernmentpaysattentionandprioritizesmaternalhealth.
Dr.S.T.Mathai,UNFPA,TheJakartaPost,13Jan.,2010
AffandiB.KesehatanReproduksidanUpayaKesehatanMaternaldiIndonesia,QuoVadis?OrasipadaPITXVIIIPOGI,Jakarta,7Juli2010
-
Ofthe11countriesthatcontributeto65l b l l d h fi
ipercenttoglobalmaternaldeath,fivearein
AsiancountriesincludingIndonesia,Bangladesh,Pakistan,IndiaandAfghanistan.Ahighmaternalmortalityrateisang
yindicatorofthestatusofpoorfunctioningofa countrys health system
including lack ofacountry
shealthsystemincludinglackofsupportiveandprotectivelegalandpolicyenvironmentenvironment.
Dr.S.T.Mathai,UNFPA,TheJakartaPost,13Jan.,2010
Affandi B.Kesehatan Reproduksi dan Upaya Kesehatan Maternaldi
Indonesia,QuoVadis?Orasi pada PITXVIIIPOGI,Jakarta,7Juli 2010
-
GOAL5ImproveMaternalHealthp
Target6:Reducebythreequarters,between
1990and2015,thematernalmortalityratio
Indicators:MaternalmortalityratioPercentageofbirthsattendedbyskilledg
yhealthpersonnelContraceptiveprevalencerate
AffandiB.PostpartumContraception&MedicalBarrier.DepartmentofObstetrics&Gynecology,UniversityofIndonesia,Jakarta,22Sept.2010
-
Threeprongedstrategytoreducingmaternalmortality
Family planning to ensure that every birth is
Familyplanningtoensurethateverybirthiswanted
Skilled care by a health professional with
Skilledcarebyahealthprofessionalwithmidwiferyskillsforeverypregnantwomand
i d hildbi thduringpregnancyandchildbirth
EmergencyObstetricCare(EmOC)toensuretimelyaccesstocareforwomenexperiencingcomplications.
UNFPA,2009p
AffandiB.PostpartumContraception&MedicalBarrier.DepartmentofObstetrics&Gynecology,UniversityofIndonesia,Jakarta,22Sept.2010
-
PERENCANAANKELUARGA
1.
Seorangwanitatelahdapatmelahirkan,segerasetelahiamendapathaidyangpertama(
h )(menarche)
2. Kesuburanseorangwanitaakanterusberlangsung,sampai mati haid
(menopause)sampaimatihaid(menopause)
3.
Kehamilandankelahiranyangterbaik,artinyarisikopalingrendahuntukibudananak,adalahp
g ,antara2035tahun
4. Persalinanpertamadankeduapalingrendahi ikrisikonya
5. Jarakantaraduakelahiransebaiknya24tahun
Affandi, 1984
Affandi
B.PostpartumContraception&MedicalBarrier.BuildingMomentumMDGs4&5,RSIABudiKemuliaan
,Jakarta,28Sept.2010
-
POLA PERENCANAAN KELUARGAPOLAPERENCANAANKELUARGA
FaseFase FaseFase FaseFase
M dM d M j kM j kMenundaMenundaKehamilanKehamilan
MenjarangkanMenjarangkanKehamilanKehamilan
TidakTidak HamilHamillagilagi
22 44
2020 3535
Affandi, 1984
Affandi
B.PostpartumContraception&MedicalBarrier.BuildingMomentumMDGs4&5,RSIABudiKemuliaan
,Jakarta,28Sept.2010
-
PEMILIHANKONTRASEPSIRASIONAL
FaseFase FaseFase FasFaseemenundamenundaKehamilanKehamilan
MenjarangkanMenjarangkanKehamilanKehamilan
TidakTidak hamilhamillagilagi
22 44
PilPil IUDIUD
IUDIUD SuntikanSuntikan
IUDIUD SuntikanSuntikan
SterilSteril IUDIUD
2020 3535 SederhanaSederhana SuntikanSuntikan ImplantImplant
SuntikanSuntikan MiniPilMiniPil PilPil ImplantImplant
SederhanaSederhana
SuntikanSuntikan MiniPilMiniPil PilPil ImplantImplant
SederhanaSederhana
ImplantImplant SuntikanSuntikan SederhanaSederhana
PilPilSederhanaSederhana SederhanaSederhana
SterilSterilAffandi, 1984
Affandi
B.PostpartumContraception&MedicalBarrier.BuildingMomentumMDGs4&5,RSIABudiKemuliaan
,Jakarta,28Sept.2010
-
CONTRACEPTIVEPREVALENCEINDONESIA 19702007INDONESIA,1970 2007
70
80
61 4 %
60
70
48 %
57 %60 % 61.4 %
40
50
20
3026 %
10
205 % (?)
01970 1980 1987 1997 2002 2007
Affandi
B.UnsafeAbortion:IndonesianExperience.1stInternationalCongressonWomenHealth&UnsafeAbortion,Bangkok,Thailand,2023January2010
-
CurrentContraceptiveUsersIndonesia March
2006Indonesia,March2006
METHODS USERS %METHODS USERS %
INJECTABLES 9 743 550 35 2INJECTABLES 9,743,550 35.2
PILLs 7,796,474 28.1
IUDs 5 218 196 18 8IUDs 5,218,196 18.8
IMPLANTABLES 3,156,705 11.4
STERILIZATION 1 515 406 5 5STERILIZATION 1,515,406 5.5
OTHERS 278,473 1.0
TOTAL 27 708 804 100 0TOTAL 27,708,804 100.0BKKBN, 2007
Affandi
B.UnsafeAbortion:IndonesianExperience.1stInternationalCongressonWomenHealth&UnsafeAbortion,Bangkok,Thailand
,2023January2010
-
BIRTHRATEBIRTHRATE
STILL HIGH ! ! !STILL HIGH ! ! !
4 5 5 Million/year4.5 5 Million/year
Affandi
B.UnsafeAbortion:IndonesianExperience.1stInternationalCongressonWomenHealth&UnsafeAbortion,Bangkok,Thailand
,2023January2010
-
FAKTAFAKTA1.PascasalinOVULASIdapatpterjadidalamwaktu21hari
2.PascakeguguranOVULASIdapatTERJADIdalamwaktu11hari
Affandi B.Kontrasepsi Terkini dan IUDPascaplasenta .Pertemuan
Koordinasi Peningkatan KBPascapersalinan di Rumah Sakit
,Makassar31Agustus 2010
Contraceptivechoicesforbreastfeedingwomen.JournalofFamilyPlanningandReproductiveHealthCare2004;30(3):181189
-
SimplifiedClassificationofEligibility( )Criteria(WHO)
AffandiB.PerkembanganKontrasepsi,TeknikPenapisandanKBPostpartum,BPMPPKB,Balikpapan,24Juni2010
-
12.Theuseofprogestogenonlymethodsinthefirst6weekspostpartumdoesnotappeartohaveanadversep
p ppeffectonbreastmilkvolume(GradeB).
13.Theuseofprogestogenonlymethodswhenb f di id 99% ffi (G d
)breastfeedingprovidesover99%efficacy(GradeB).
14.Theproblematicbleedingassociatedwithprogestogenonly methods
appears to be more acceptable than
thatonlymethodsappearstobemoreacceptablethanthatexperiencedbywomenwhoarenotbreastfeeding(GradeB).Aftercounselling,breastfeedingwomenmaychoosetouseaprogestogenonlymethodofcontraceptionbefore6
weeks postpartum if other contraceptive methods
are6weekspostpartumifothercontraceptivemethodsareunacceptable.
Contraceptivechoicesforbreastfeedingwomen.JournalofFamilyPlanningandReproductiveHealthCare2004;30:181189
Affandi
B.PostpartumContraception&MedicalBarrier.DepartmentofObstetrics&Gynecology,UniversityofIndonesia,Jakarta,
22Sept.2010
-
17.DMPAusebefore6weekspostpartumisnot usually recommended (Grade
C)notusuallyrecommended(GradeC).
18.TroublesomebleedingcanoccurwithDMPAuseintheearlypostpartumperiod(GradeC).
DMPAwillnotrequiretheinjectionuntilDay21postpartum,butiftheriskofimmediatesubsequentpregnancyishighitmaybegivenbeforethistime.
Contraceptive choices for breastfeeding women. Journal of Family
Planning and Reproductive Health Care 2004; 30:
181189Contraceptivechoicesforbreastfeedingwomen.JournalofFamilyPlanningandReproductiveHealthCare2004;30:181
189
Affandi
B.PostpartumContraception&MedicalBarrier.DepartmentofObstetrics&Gynecology,UniversityofIndonesia,Jakarta,
22Sept.2010
-
BreastfeedingwomenmaychoosetouseaprogestogenonlyimplantbeforeDay
28 without the need
forDay28withouttheneedforadditionalcontraceptiveprotection.
IMPLANTwillnotberequireduntilDay 28 postpartum, but if the risk
ofDay28postpartum,butiftheriskofimmediatesubsequentpregnancyishigh
it ma be gi en before this timehighitmaybegivenbeforethistime.
C i h i f b f di J l f il l i d d i H l h C 2004 30 181
189Contraceptivechoicesforbreastfeedingwomen.JournalofFamilyPlanningandReproductiveHealthCare2004;30:181189
Affandi
B.PostpartumContraception&MedicalBarrier.DepartmentofObstetrics&Gynecology,UniversityofIndonesia,Jakarta,
22Sept.2010
-
Statement,WHOGeneva,22Oct.2008:Progestinonlycontraceptiveuseduringlactation
1. Useofprogestinonlymethods,withtheexceptionofthel l b ll d d
flevonorgestrel
bearingIUD,isnotusuallyrecommendedforwomenwhoarelessthan6weekspostpartumandbreastfeeding,unlessothermoreappropriatemethodsareunavailableorunacceptable.
2.
Beyond6weekspostpartum,thereisnorestrictionfortheuseofprogestin
only contraceptive methods among
breastfeedingprogestinonlycontraceptivemethodsamongbreastfeedingwomen.
3. ThelevonorgestrelbearingIUDisnotusuallyrecommendedforth fi t
4 t t k l th i
tthefirst4postpartumweeks,unlessothermoreappropriatemethodsareunavailableorunacceptable.Beyond4weekspostpartum,thereisnorestrictiononitsuse.
Affandi
B.PostpartumContraception&MedicalBarrier.DepartmentofObstetrics&Gynecology,UniversityofIndonesia,Jakarta,
22Sept.2010
-
IUDCuAffandiB.PerkembanganKontrasepsi,TeknikPenapisandanKBPostpartum,BPMPPKB,Balikpapan,24Juni2010
-
ThepostpartuminsertionofIUDshasb f d l
danumberofadvantages,including
ease of insertion, availability of
skilledeaseofinsertion,availabilityofskilledpersonnelandappropriatef
ili i d i f hfacilities,andconvenienceforthewoman.
Practitionershavebeenconcernedaboutthepossibilityofhigherexpulsion,
infection and
perforationwww.fhi.org/en/rh/pubs/factsheets/iud_pp.htmexpulsion,infectionandperforationrates.Affandi
B.PostpartumContraception&MedicalBarrier.DepartmentofObstetrics&Gynecology,UniversityofIndonesia,Jakarta,
22Sept.2010
-
Postplacental (preferably within Postplacental
(preferablywithin10minutesafterexpulsionoftheplacenta)andimmediatepostpartum
insertion during
thepostpartuminsertionduringthefirstweekafterdelivery(butpreferablywithin48hours)areconvenient
effective and
safeconvenienteffectiveandsafetimestoinsertcopperIUDs.
Affandi B.Perkembangan Kontrasepsi,Teknik Penapisan dan
KBPostpartum,BPMPPKB,Balikpapan,24Juni 2010
{ManagingContraception20052007,page92}
-
Teknik Pemasangan AKDR
Affandi
B.PostpartumContraception&MedicalBarrier.DepartmentofObstetrics&Gynecology,UniversityofIndonesia,Jakarta,
22Sept.2010
-
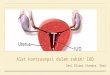
Fundal placement
ThewaytheIUDisinsertedismoreimportantthanthedesignofthedevice.Diff
i IUD l i b
DifferencesinIUDexpulsionratesbetweencentersparticipatinginthetrialsweregenerallygreaterthanexpulsion
rates for different IUDs;expulsionratesfordifferentIUDs;
FHIdatashowthatemphasisneedstobegiventothefundal placement of
the device.fundal placementofthedevice.
Theprovidershouldbeabletofeelthedevicethroughtheabdominalanduterinewallsatthetimeofinsertion.
Retrainingisnecessaryforthoseindividualswhoreporthighexpulsionrates
www.fhi.org/en/rh/pubs/factsheets/iud_pp.htmAffandi
B.PostpartumContraception&MedicalBarrier.DepartmentofObstetrics&Gynecology,UniversityofIndonesia,Jakarta,
22Sept.2010
-
Teknik Pemasangan AKDR
Affandi
B.PostpartumContraception&MedicalBarrier.DepartmentofObstetrics&Gynecology,UniversityofIndonesia,Jakarta,
22Sept.2010
-
Allowthewomantorest.Besureshegetscomplete
t tpostpartumcare.
P id i iProvidepostinsertioninstructionsinstructions.
-
ExpulsionExpulsion
Afterbirth,astheuterusreturnstonormalsize(involution),uterinecontractionsexpelretainedplacentalandbloodclotsandmayp
yhaveasimilareffectonanyforeignbodyintroduced into the
uterus.introducedintotheuterus.
IUDsinsertedwithin10minutesofplacental i h h l l i i
kexpulsionhaveamuchlowerexpulsionrisk
thanthoseinsertedlaterinthepostpartumperiod.
www.fhi.org/en/rh/pubs/factsheets/iud_pp.htm
Affandi
B.PostpartumContraception&MedicalBarrier.DepartmentofObstetrics&Gynecology,UniversityofIndonesia,Jakarta,
22Sept.2010
-
BarrierThatPreventContraceptiveSSuccess
Barriertoeffectivefamilyplanning services
Outcomewhenbarrierplanningservices areovercome
Accesstoservice
Contraceptivefpreference
Quality services Qualityservices
MAQExchangecurriculum(Online)MaximizingAccessandQualityinitiative,WashingtonDC,2001
Affandi
B.PostpartumContraception&MedicalBarrier.BuildingMomentumMDGs4&5,RSIABudiKemuliaan
,Jakarta,28Sept.2010
-
Medical barriersMedicalbarriersweredefinedas
"practices,derivedatp
,leastpartlyfromamedicalrationale,thatresultinascientifically
unjustifiablescientificallyunjustifiableimpedimentto,ordenialof,p ,
,contraception" SheltonJD,etal.Lancet,1992;340:13341335
Affandi B.Perkembangan Kontrasepsi,Teknik Penapisan dan
KBPostpartum,BPMPPKB,Balikpapan,24Juni 2010
-
MedicalBarriersthatrestrictfaccesstofamilyplanningservices
1 Provider bias When the provider is1.Providerbias
Whentheproviderisfororagainstaspecificmethod
2 O l t i ti li ibilit it
i2.Overlyrestrictiveeligibilitycriteria
Whocangetwhatcontraceptive
3.Unnecessaryprocesshurdles
Requirementsthat,fromtheuser'spointofview,makeitdifficulttoobtainacontraceptive
SheltonJD,etal.Lancet,1992;340:13341335
Affandi B.Perkembangan Kontrasepsi,Teknik Penapisan dan
KBPostpartum,BPMPPKB,Balikpapan,24Juni 2010
-
4.Inappropriatecontraindications Medical conditions that
restrict
theMedicalconditionsthatrestricttheuseofsomecontraceptives
5 Overly restrictive regulations 5.Overlyrestrictiveregulations
Nationallawsandclinicorhospitalregulationsregulations
6.Providerlimitation Whocanprovide what
methodprovidewhatmethod
7.Inappropriatemanagementofsideeffects Actions taken by
theeffects
Actionstakenbytheprovidertohelptheusertolerateacontraceptive method
Shelton JD et al Lancet 1992;340:13341335contraceptivemethod
Affandi B.Perkembangan Kontrasepsi,Teknik Penapisan dan
KBPostpartum,BPMPPKB,Balikpapan,24Juni 2010
SheltonJD,etal.Lancet,1992;340:1334 1335
-
ChecklistsReduceMedicalBarriers
Medicalbarriersoftenpreventclientsfromusingtheirdesiredmethodoffamilyplanning.
Thepregnancy,COC,DMPA,andIUDchecklistscaneffectivelyincreaseaccesstofamilyplanningwhilehelping
ensure client safetyhelpingensureclientsafety.
Introductionofchecklistsintoservicedeliverysettingsshouldincludecarefultrainingonhowtousethegchecklistsaswellasthemedicaleligibilitycriteriaonwhichtheyarebased.
Affandi B.Perkembangan Kontrasepsi,Teknik Penapisan dan
KBPostpartum,BPMPPKB,Balikpapan,24Juni 2010
-
Knowingisnotenough,wemustapplyWillingisnotenough,we
t dmustdoG hGoethe
Affandi
B.PostpartumContraception&MedicalBarrier.BuildingMomentumMDGs4&5,RSIABudiKemuliaan
,Jakarta,28Sept.2010